Back to Journals » Infection and Drug Resistance » Volume 19
Case Report: Rare Multidrug-Resistant Enterobacter Cloacae Complicated by Invasive Pulmonary Aspergillosis in an Elderly Patient with Advanced Lung Adenocarcinoma Treated with Osimertinib
Authors Zhou M ![]() , Shi J, Cao C, Zhang C
, Shi J, Cao C, Zhang C ![]()
Received 23 January 2026
Accepted for publication 9 March 2026
Published 18 March 2026 Volume 2026:19 598530
DOI https://doi.org/10.2147/IDR.S598530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Meili Zhou, Jinli Shi, Chunyan Cao, Chengsen Zhang
Emergency Medical Center, Qingdao Central Hospital, University of Health and Rehabilitation Sciences, Qingdao, People’s Republic of China
Correspondence: Chengsen Zhang, Email [email protected]
Abstract: Osimertinib, a third-generation epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI), is the standard treatment for EGFR-mutated advanced non-small cell lung cancer (NSCLC). We report a rare case of multidrug-resistant (MDR) Enterobacter cloacae pneumonia complicated by invasive pulmonary aspergillosis (IPA) in a 75-year-old male with lung adenocarcinoma who had been receiving osimertinib for 8 months. Prompt susceptibility-guided therapy with polymyxin B plus tigecycline (for MDR bacteria) and voriconazole (for aspergillosis) achieved complete resolution, highlighting the importance of rapid microbiological diagnosis and targeted antimicrobials in this vulnerable population.
Keywords: osimertinib, multidrug-resistant enterobacter cloacae, invasive pulmonary aspergillosis, EGFR-TKI, opportunistic infection, lung adenocarcinoma
Introduction
Osimertinib is the preferred first-line therapy for EGFR-mutated advanced non-small cell lung cancer (NSCLC), offering superior efficacy and central nervous system penetration compared to earlier-generation TKIs.1 Patients with advanced NSCLC, particularly elderly individuals with multiple comorbidities, are at increased risk of opportunistic infections due to the underlying malignancy, chronic lung disease, and host immunosuppression. Targeted therapies such as osimertinib have been associated with reports of opportunistic infections in this population,2–5 although distinguishing the specific contribution of the drug from other predisposing risk factors is often challenging.
Multidrug-resistant (MDR) Enterobacter cloacae infections are uncommon in community settings but present significant therapeutic challenges due to extensive antimicrobial resistance.6 Co-infection with Aspergillus species further complicates management, particularly in elderly patients with malignancy and comorbidities7 Although isolated fungal or bacterial infections have been reported during osimertinib therapy,2,4 concurrent MDR Enterobacter cloacae pneumonia and invasive pulmonary aspergillosis remain exceedingly rare. This case highlights the importance of vigilance for opportunistic superinfections in this vulnerable patient population.
Case Summary
A 75-year-old male with a history of advanced EGFR-mutated lung adenocarcinoma (receiving osimertinib 80 mg daily for 8 months with good tumor control), bronchial asthma, emphysema, old cerebral infarction, mitral valve replacement, and atrial fibrillation (on warfarin) presented with a 3-day history of chest tightness, dyspnea, cough productive of purulent sputum, and fever (maximum 39.3°C).
Physical examination and initial investigations revealed signs of lower respiratory tract infection. Chest computed tomography demonstrated a right lower lobe mass with obstructive changes, multiple bilateral small nodules, mediastinal lymphadenopathy, left lower lobe consolidation, emphysema, cardiomegaly, and minimal bilateral pleural effusions with pleural thickening (Figure 1). Laboratory findings on admission showed leukocytosis with neutrophilia and elevated C-reactive protein (detailed in Table 1).
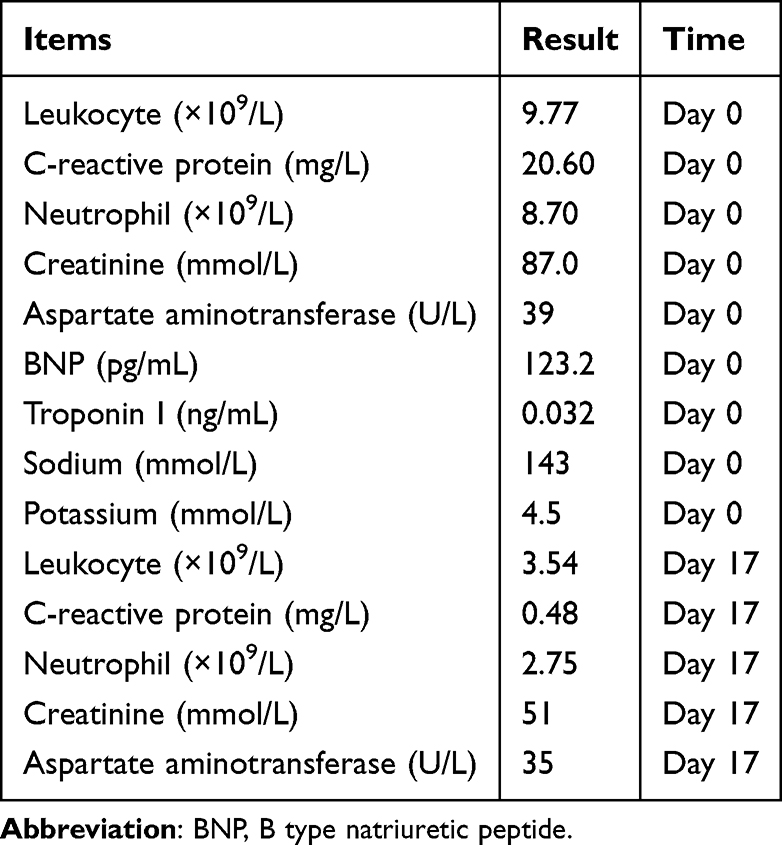 |
Table 1 Laboratory Results of the Patient |
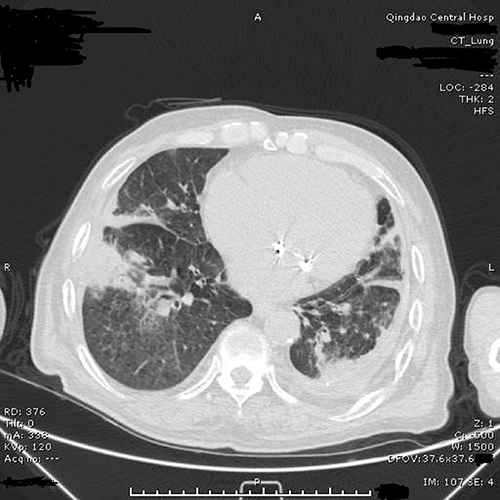 |
Figure 1 Representative chest computed tomography of the patient. |
Empirical intravenous oxacillin was initiated. After 3 days of persistent fever and worsening dyspnea, sputum culture grew multidrug-resistant Enterobacter cloacae, and Aspergillus DNA detection was positive. Subsequent fungal culture confirmed Aspergillus fumigatus. Microbiological identification and susceptibility results are summarized in Table 2.
 |
Table 2 Microbiological Identification and Antimicrobial Susceptibility Results of the Pathogens Isolated from Sputum |
The antimicrobial regimen was immediately changed to intravenous polymyxin B plus tigecycline for the bacterial infection and voriconazole for invasive pulmonary aspergillosis. Osimertinib was continued without interruption. Fever resolved within 3 days of the regimen switch, and dyspnea improved markedly. After 14 days of combination therapy, inflammatory markers normalized (Table 1), intravenous antibiotics were discontinued, and oral voriconazole was continued for one additional month. The patient was discharged in stable condition. At 1-month follow-up he remained free of recurrent fever, cough, sputum, or dyspnea. The clinical course and treatment timeline are summarized in Table 3.
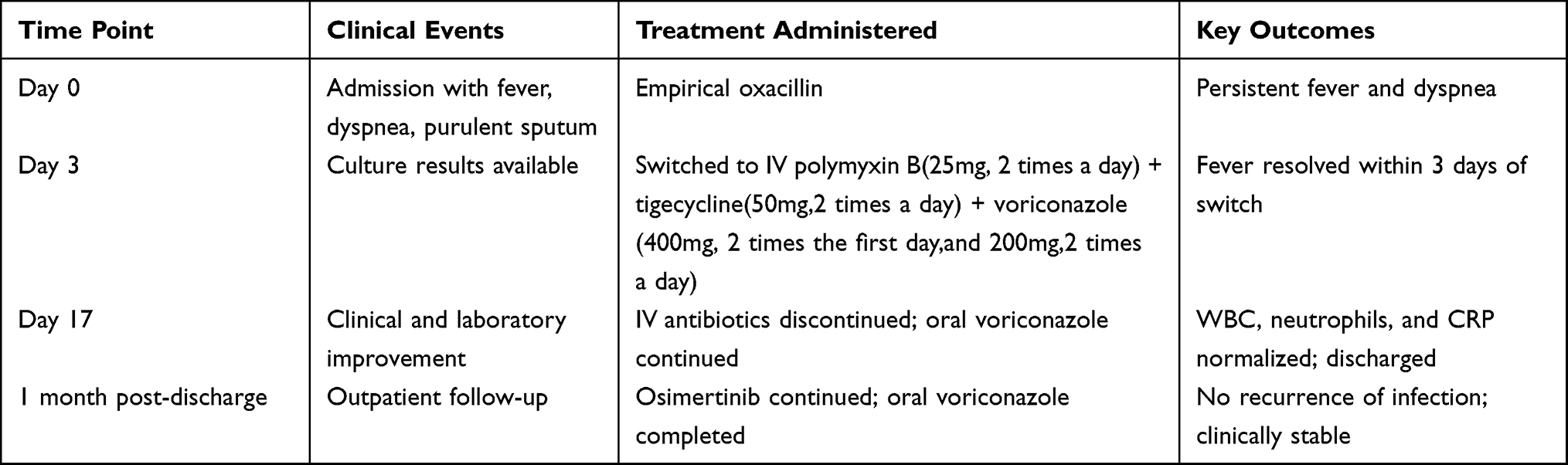 |
Table 3 Treatment Flowcharts and Clinical Course |
Discussion
This case illustrates a rare clinical presentation of multidrug-resistant (MDR) Enterobacter cloacae pneumonia complicated by invasive pulmonary aspergillosis (IPA) in a 75-year-old patient with advanced EGFR-mutated lung adenocarcinoma and multiple established host-related risk factors for opportunistic infection, including bronchial asthma, emphysema, old cerebral infarction, mitral valve replacement, and atrial fibrillation, while receiving osimertinib therapy for 8 months.
Opportunistic infections with both bacterial and fungal pathogens are well-recognized in patients with advanced lung cancer, primarily due to host-related risk factors such as advanced age, underlying malignancy, chronic structural lung disease, and cancer-associated immunosuppression. These established risk factors are the predominant contributors in the present case. The simultaneous occurrence of MDR E. cloacae and invasive aspergillosis is uncommon and presents significant diagnostic and therapeutic difficulties.
MDR Enterobacter cloacae infections are challenging to manage due to extensive antimicrobial resistance mechanisms, often leaving polymyxin B and tigecycline as the key treatment options.6 Concurrent invasive pulmonary aspergillosis in an immunocompromised host requires prompt initiation of effective antifungal therapy, with voriconazole remaining the first-line agent according to established guidelines.7
The favorable clinical response observed in this patient after targeted combination therapy underscores the importance of rapid microbiological diagnosis—including bacterial and fungal cultures as well as molecular testing—and prompt institution of susceptibility-guided treatment in complex cases. Clinicians caring for patients with advanced NSCLC should maintain a high index of suspicion for opportunistic and mixed infections when fever and pulmonary symptoms persist or worsen despite initial management.
Following successful treatment of the dual infection, osimertinib was continued at the same dose (80 mg daily) without interruption or dose reduction, as the patient had demonstrated excellent ongoing tumor control on imaging and had recovered fully from the infectious episode. This individualized decision was made jointly by the oncology and infectious-disease teams after weighing the clear benefit of continued targeted therapy against the resolved infection. In patients with advanced EGFR-mutated NSCLC who develop opportunistic infection while on osimertinib, continuation of EGFR-TKI therapy should be guided by tumor response, performance status, and overall risk–benefit assessment on a case-by-case basis.
Prevention of recurrence in similar high-risk patients (elderly individuals with advanced lung cancer, chronic lung disease, and multiple comorbidities) relies primarily on heightened clinical vigilance, prompt microbiological evaluation of any new or worsening respiratory symptoms, and close multidisciplinary collaboration between oncology and infectious-disease specialists. Specific prophylactic antimicrobial strategies (antibacterial or antifungal) cannot be recommended on the basis of a single case observation. Larger prospective studies are needed to better define infection risks, optimal management, and potential preventive approaches in this population.
This report has several important limitations inherent to single-case descriptions. As a single observation, it cannot establish any causal relationship between osimertinib and the dual opportunistic infection. Invasive pulmonary aspergillosis cannot be definitively attributed to osimertinib, and the possibility of Aspergillus colonization rather than true invasive disease—driven primarily by the patient’s underlying advanced malignancy, structural lung disease, and multiple comorbidities—cannot be excluded. These uncertainties highlight the need for cautious interpretation of the findings and reinforce that larger, prospective studies are required to better characterize infection risks in this population.
We share the hope that the early disclosure of relevant larger-scale clinical research results will help further improve and optimize existing clinical diagnosis and treatment strategies for opportunistic infections in this vulnerable population.
Conclusion
This case suggests that clinicians should maintain awareness of possible severe or mixed infections in elderly patients with advanced lung cancer receiving targeted therapy and should pursue early microbiological evaluation when clinical deterioration occurs. However, this single observation does not establish osimertinib as a direct cause of opportunistic infection and does not support routine screening or prophylactic strategies. The findings represent a hypothesis-generating clinical alert rather than a basis for changes in standard management. Further studies are warranted to better characterize infection risks in this population.
Ethics
The case was approved for publication by the ethics committee of Qingdao Central Hospital, University of Health and Rehabilitation Sciences, approval number: KY202602601.
Patient Consent
Informed consent was obtained from the patient for publication of this case report.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest.
References
1. Soria JC, Ohe Y, Vansteenkiste J. et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–5.
2. Hamada Y, Motegi T, Kuramoto K, et al. Pulmonary Cryptococcosis During Osimertinib Treatment for EGFR L858R-Mutant Lung Adenocarcinoma: a Case Report. Cureus. 2025;17(5):e12345.
3. Reinwald M. Risk of infection associated with targeted therapies for solid organ and hematological malignancies. Ther Adv Med Oncol. 2021;13:1758835921991841.
4. Takechi H, Endoh H, Hata Y, et al. Osimertinib-induced lymphocytopenia and pneumocystis jirovecii pneumonia. Pulmonology. 2022;28(5):402–404.
5. Morelli T, Fujita K, Redelman-Sidi G, et al. Infections due to dysregulated immunity: an emerging complication of cancer immunotherapy. Thorax. 2022;77(3):304–311.
6. Tamma PD. IDSA 2024 Guidance on the Treatment of Antimicrobial Resistant Gram-Negative Infections. Clin Infect Dis. 2024;2024:ciae403.
7. Patterson TF, Denning DW, Fishman JA, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;63(4):e1–e60.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Osimertinib for an Advanced NSCLC Patient with Two Common EGFR Mutations and a Concomitant MET Exon 14 Skipping Mutation: A Case Report
Liu Z, Song P, Zhou L, Ji D, Shen H, Dong H, Feng X
Cancer Management and Research 2023, 15:645-650
Published Date: 12 July 2023
Abnormally Activated MNX1 Promotes Tumor Growth and Osimertinib Resistance and Predicts Survival in EGFR-Mutant Lung Adenocarcinoma
Gu W, Gan J, Liu P, Lai J, Liu C, Zhang G, Shi C, Jiang Q, Qiu F
Drug Design, Development and Therapy 2025, 19:11411-11431
Published Date: 20 December 2025
Acquired BRAF-AGK Fusion Following Osimertinib Plus Savolitinib in EGFR-Mutated MET-Amplified Non-Small-Cell Lung Cancer: Durable Response to Gefitinib and Trametinib in a Case Report
Lee AF, Wu SY
OncoTargets and Therapy 2026, 19:605699
Published Date: 3 June 2026