Back to Journals » Patient Preference and Adherence » Volume 16
Caregiver Perspectives on Physiotherapy Treatment for Paediatric Burns in the United Arab Emirates
Authors Mohamed Muftah Alzaabi FS, Bairapareddy KC, Alaparthi GK ![]() , Hegazy F
, Hegazy F
Received 24 February 2022
Accepted for publication 19 May 2022
Published 17 June 2022 Volume 2022:16 Pages 1477—1486
DOI https://doi.org/10.2147/PPA.S363312
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Fatima Sultan Mohamed Muftah Alzaabi, Kalyana Chakravarthy Bairapareddy, Gopala Krishna Alaparthi, Fatma Hegazy
Physiotherapy, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates
Correspondence: Fatma Hegazy, Physiotherapy, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates, Email [email protected]
Background: Physiotherapy is an essential component of paediatric burn treatment. Children are admitted to the paediatric burn unit with their caregivers who play a vital role in supporting the child’s post-burn physiotherapy management.
Objective: The objective of the study is to determine caregivers’ attitudes on physiotherapy treatment for children with burns in the UAE. This study focused on the caregiver’s perspective on five important domains: caregiver’s knowledge, burden, attitude, adherence to physiotherapy exercise program, and caregiver’s satisfaction.
Methods: A descriptive cross-sectional study was conducted using self-administered questionnaire. Fifty caregivers were eligible to participate in the study. The analyses of the survey responses were done using SPSS software. Descriptive analysis and correlation statistics were used to present the data.
Results: The caregiver participants in the study reported to have reasonably good knowledge about the paediatric burns care (13.62 ± 3.49) and had a positive attitude towards the physiotherapy treatment provided to the children with the burn injuries (9.41 ± 1.56). The adherence to the prescribed exercise regimen of physiotherapy sessions was found to be good (11.88 ± 1.50) but were overburdened with the caregiving tasks (21.42 ± 11.62). The study demonstrated very high levels of satisfaction among the caregivers with the physiotherapy treatment sessions provided to the children (13.4 ± 1.83).
Conclusion: Caregiver attitude regarding physiotherapy management was overall positive; caregivers were well aware of the importance of physiotherapy and have reported high levels of satisfaction with the paediatric burn physiotherapy management.
Keywords: caregiver, burn, paediatric, physiotherapy, awareness, knowledge
Introduction
A burn is commonly defined as a primary injury to the skin or other organic tissue caused by heat, radiation, radioactivity, electricity, friction, smoke, or contact with combustible substances.1 Every year, more than 310,000 people die because of burn injuries,2 despite significant advancements in life support, antimicrobial therapy, and surgical methods.3 Pediatric burn victims are the most severely affected, accounting for approximately half of all burn casualties globally.4 In the UAE, 203 burn cases were reported in 2013, of which 25% victims were children under the age of five.5 With the goal of enhancing long-term functional outcomes, a multidisciplinary team approach is essential.6 A team of multidisciplinary health professionals focuses on enhancing long-term functional outcomes in hospitals in the UAE that have specialized pediatric burns care units.
The most prevalent cause of burn hospitalization in children is scalding due to hot water, and the second most common cause is flame burns. The most commonly burned anatomical regions were the extremities, followed by the abdomen, head, face, and chest.7 Burn injuries place a substantial financial burden on victims, families, and the society. Patients with burns may require numerous surgical procedures and may be hospitalized for an extended period of time. Burn victims experience many complications frequently, including pain, contractures, infections, and hypertrophic scarring. Burns can cause emotional and physical scars that last lifelong,8 which may have a long-term impact on children’s developmental, functional, psychological, and aesthetic status.9 Burn incidents present physical, financial, and emotional challenges for some children and caregivers, which may have life-altering consequences.5 As a result, the focus of research on pediatric burns has shifted over time from acute care and mortality reduction to post-burn health-related quality of life and functional rehabilitation.9
Changes in family dynamics that are unexpected and abrupt are stressful for caregivers and necessitate considerable changes in daily activities and duties. Caregivers have a vital role in assisting the routine healthcare rehabilitation of children with burn injuries, in addition to managing these changes.10 Physiotherapy has been a crucial intervention in burn management. Appropriate early-stage treatment, including mobilization, significantly minimizes the length of hospitalization and complications.11 Working in a multidisciplinary team, physiotherapists focus on patient and caregiver education, scar prevention, hypertrophic scar suppression, and restoration of the patient’s functional capacity, such as full range of motion, muscle strength, independent mobility, and activities of daily living.8,12 The involvement of caregivers in the healing process is crucial for children with burns. Involving a caregiver in an intervention program increased the likelihood of achieving goals and improving motor function in children with burns.13 The caregiver’s role was critical in the management of burns in children.14
Hospital exercise programs conducted in the absence of a physiotherapist, to sustain the therapeutic benefits of normal physiotherapy sessions, are an important aspect of continuous care for patients with burns. Caregivers’ compliance with hospital-based exercise programs may facilitate a better prognosis.8 Caregivers’ lack of awareness, lack of interest in physiotherapy management, poor adherence to the prescribed exercise program, and dissatisfaction with physiotherapy services have an impact on healing outcomes, which may hamper the success of exercise-based rehabilitation programs for pediatric patients with burns.15 Therefore, caregivers must be fully aware of the importance of physiotherapy in burn management.
Factors influencing caregivers during an exercise-based rehabilitation program for pediatric burn injuries must be identified.16 The study of caregivers’ knowledge of physiotherapy, attitude towards physiotherapy, adherence to the prescribed program, and satisfaction may aid in the development of a comprehensive education program for caregivers and, as a result, improve the success of pediatric burn rehabilitation programs. The objective of this study was to determine the caregivers’ basic knowledge and attitude towards physiotherapy-related management of pediatric burns, assess the caregiver burden, and adhere to the exercise program.
Materials and Methods
This was a descriptive, cross-sectional study conducted at the Latifah Women and Children Hospital in Dubai, UAE, which is one of the largest government hospitals in the UAE dedicated to women’s and children’s health and contains a large pediatric burn unit within the pediatric surgery ward. This study aimed to recruit all caregivers of children under the age of 13 years who were referred for post-burn physiotherapy management, spoke Arabic or English, and had a burn diagnosis, regardless of the year or etiology of the burn. Caregivers of patients with burns who spoke a different language as well as patients with burns who arrived at the rehabilitation center without a caregiver, were not included in the study.
Caregivers were recruited in two ways: those who came to the rehabilitation department for post-burn physiotherapy sessions were enrolled in the study after being informed about the study’s goal and procedure and signing a consent form, and those who came to the rehabilitation department for post-burn physiotherapy sessions were enrolled in the study after being informed about the study’s goal and procedure and signing a consent form. In addition, an online survey was used to contact the caregivers of pediatric patients with burns, whose contact information was obtained from the medical records department. Caregivers who answered the questions and were willing to participate in the study were enrolled. Twenty caregivers took part in the study while caring for the affected children in the hospital, and 30 caregivers took part in the study via an online survey. The standard guidelines have been followed for reporting this research work (Supplementary Table S1 - STROBE checklist).
Instrument
Relevant data were collected from caregivers using a self-administered questionnaire. Only Arabic and English were used to develop the questionnaire. The questionnaire was validated and approved by the Physiotherapy Department at the University of Sharjah’s Health Sciences College. Two physiotherapists, two pediatric burn specialists, and one health professional specializing in qualitative analysis were given the questionnaire in both languages for validation to improve the quality of the questionnaire. Following the reviewers’ recommendations, the five validators were asked to provide their final approval. The mean years of experience in the burn units for the content experts were 8 years with a standard deviation of 2.4. The content validators had an average of eight years’ experience working in a burn unit. On a four-point scale, experts were asked to rate the relevance of each question in the survey (1 = not relevant, 2 = slightly relevant, 3 = moderately relevant, and 4 = highly relevant). Item content validity indexes of >0.80 were approved as content valid, whereas I-CVIs of less than 0.80 were refined based on expert advice. The test-re-test approach with a one-week interval was used in a pilot study of ten caregivers for children with paediatric burns to establish feasibility. The kappa coefficient (k) of the closed-ended items was 0.81 to 1, indicating that the questionnaire was reliable.
The first portion of the questionnaire, which was filled out by the investigator, contained sociodemographic information about the caregiver, such as gender, age category, place of residence, education level, marital status, and relationship with the child. The five primary dimensions that determined caregivers’ perspectives on physiotherapy management are discussed in the second section. Caregivers’ knowledge, attitude toward physiotherapy management, burden, adherence to exercises, and caregiver satisfaction with post-physiotherapy burn management in the hospital were the domains studied. Each of the five sections was designed to provide very accurate answers; therefore, all questions had to be answered by the participants. The caregivers were recruited as per the selection criteria used in the study and all the participants were contacted during the three months of the study period. The selection bias was inevitable because the volunteers were chosen in one clinical facility. In the concluding section of the questionnaire, there was an open question regarding suggestions or comments.
Ethical Consideration
The research ethics committee of the University of Sharjah reviewed and approved the study request on December 26, 2020, under reference number REC 20–12-14-01-S. The study proposal was reviewed and approved by the Dubai Health Authority’s Medical Education and Research Department on May 27, 2021 (reference number USRRC05-25/PG/2021). Following DHA clearance, permission was sought from the head of the rehabilitation department of Latifah Hospital to gain access to the patients’ medical records and contact information with the help of a senior physiotherapist.
Data Collection
All the information needed for this study was gathered using a self-administered questionnaire administered to caregivers of pediatric patients with burns who had been recommended by their surgeons for post-burn physiotherapy management. After signing the consent form, the participants were seated in the clinic’s rehabilitation department to complete a questionnaire that assessed the caregiver’s knowledge, burden, attitude, adherence to the exercise program, and satisfaction with physiotherapy services to determine their level of perspective. In addition, caregivers were recruited through an online survey. After taking their contact information from the medical records department, caregivers who agreed to participate in the study were enrolled.
Sample Size Estimation
Using a bivariate normal model of Exact tests, we needed a sample size of 50 people with a significance of 95% and an 80% power to detect a moderate correlation of 0.3 between exercise adherence and caregiver satisfaction. The sample size was calculated using G*Power (University of Kiel, Germany).
Data Analysis
SPSS version 22.0 was used to analyze the data. Descriptive statistics were used for patient characteristics, and percentages were calculated for the survey items. There were no missing data to report because all of the participants completed the questionnaire completely. For each component of the questionnaire, the data were reported as the mean and standard deviation as well as the percentage of respondents. The correlation of the survey items was determined using Spearman’s rho correlation coefficient test.
Results
Fifty caregivers were eligible to participate in the study, and 50 questionnaires were completed and analyzed. Table 1 presents the demographic characteristics of the participants. Female caregivers accounted for 74% of the total, whereas male caregivers accounted for 26%. The caregivers aged from 30–39 years, and more than half of them were in their mid-thirties. 68% of the caregivers lived in the city of Dubai, with the remainder hailing from other parts of the UAE. All the caregivers were married and lived with their spouses and children in the same house. Employed caregivers accounted for 58%, adding to the difficulty of caring for children with burns and limiting exercise compliance. The majority of caregivers were university graduates, which helped them to complete the survey swiftly, grasp the situation of the child, and communicate more effectively. The caregivers were all family members, with 70% of caregivers being the child’s biological mothers; 26%, biological fathers; and, 4%, other relatives. Forty % of the caregivers had more than three children at home, which increased their burden and stress” to enhance readability owing to other siblings’ obligations and responsibilities and making exercise compliance more difficult. The majority of the children who were burned were scalded, 20% were thermally burned, and the rest were chemically burned. There are no data on the type of inhalation burn damage.
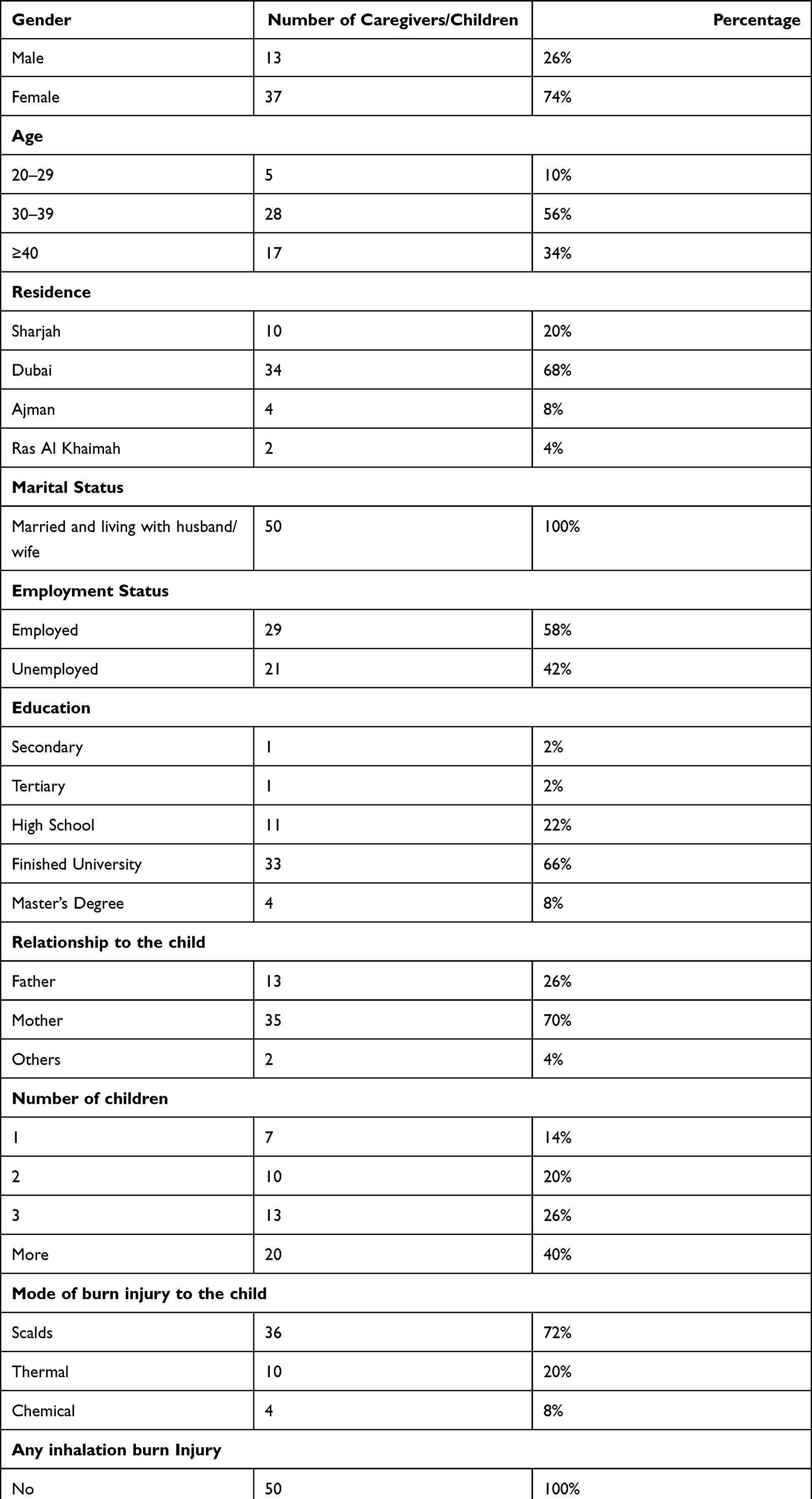 |
Table 1 Demographic Characteristic of Caregiver Participants |
For each caregiver, the total score for each of the survey’s primary domains (knowledge, attitude toward physiotherapy, caregiver burden, caregiver experience, and exercise adherence) was calculated. For the total scores, the survey findings for all domains were expressed as means and standard deviations. The total score of one domain was matched with the scores of the other domains to determine whether there was any correlation (Table 2).
 |
Table 2 Descriptive Statistics for Total Scores of Each Domain in the Questionnaire |
The participants were examined for their knowledge of the first aid offered to children in the event of a burn injury and their grasp of physiotherapy. The domain score in the participants ranged from 0 to 21 (minimum 6, maximum 21) with 11 questions in the knowledge domain. With a mean score of 13.62 (SD 3.49), the caregivers in the study reported having a reasonably excellent understanding. Caregivers attitudes toward physiotherapy after a burn injury were evaluated. A low score reflected a negative attitude towards physiotherapy. The caregivers who took part in the study had a good attitude toward physiotherapy, with a mean score of 9.41 (SD 1.56).
Caregiver burden was measured using 12 items, with a total score ranging from 0 to 52, and the caregivers of pediatric patients with burns in this study had a minimum score of 0 and a maximum score of 52, with a mean value of 21.42 (11.62), indicating low-to-moderate burden. The caregivers in this study stated that adherence to the suggested exercise schedule of physiotherapy sessions was good, with a mean score of 11.88 (1.50). Caregivers’ satisfaction with the physiotherapy treatment sessions delivered to the children was very good, with a mean value of 13.42 (1.83), whereas the maximum possible score for this domain was 14. A correlation analysis was conducted among the domain scores. There was a weak, but significant, relationship between exercise adherence and caregiver satisfaction (r-0.32, p=0.09), demonstrating that better exercise adherence improved caregiver satisfaction. Similarly, caregiver burden showed a weak negative correlation with caregiver satisfaction, indicating that a reduced caregiver load is related to a greater level of satisfaction with physiotherapy treatment. (Table 3).
 |
Table 3 Correlation Between the Total Scores of the Domains in the Questionnaire |
The recommendations of the treating physician were the caregiver’s preferred source of information for the treatment of their children with burn injuries (96%) (Figure 1). 86% of caregivers reported adhering to the specified exercise routine (Figure 2). The primary reasons for noncompliance with the exercise program were caregivers’ dislike of the child crying during therapy, lack of change in the child’s physical health status, uncooperative children, and lack of time for the caregiver to provide the therapy (Figure 3).
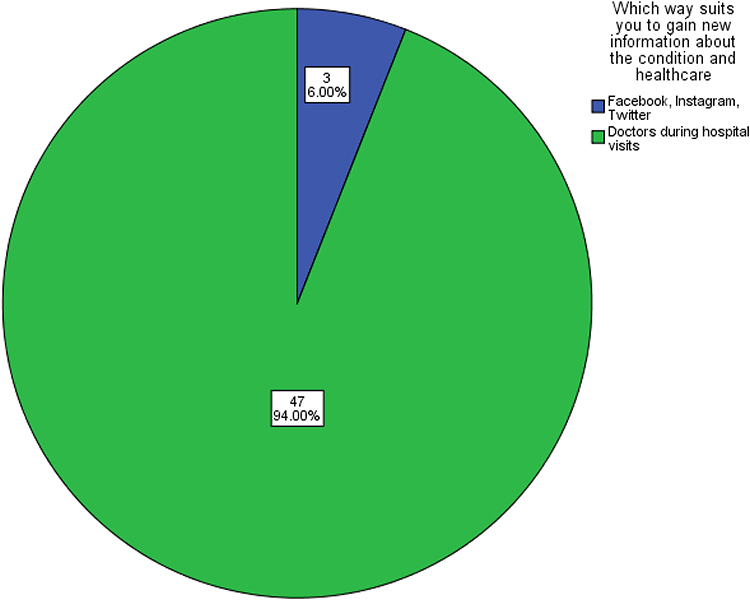 |
Figure 1 Pie chart showing source of information caregivers prefer. |
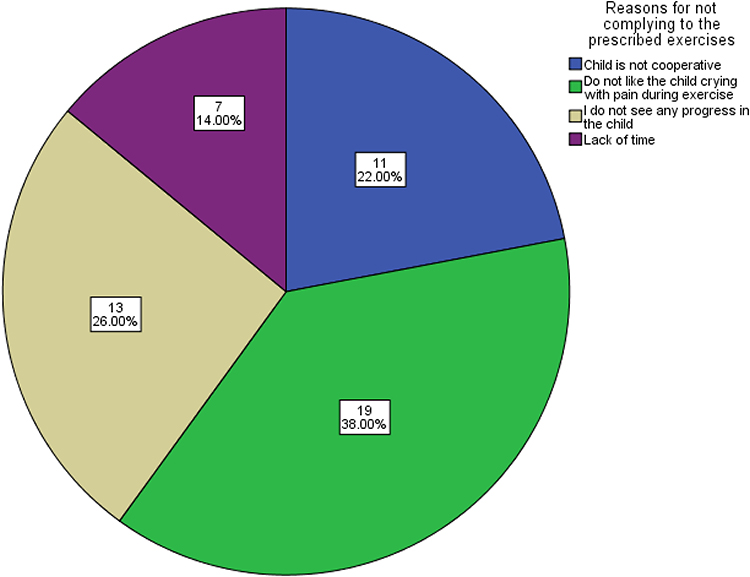 |
Figure 2 Pie chart showing the reasons for not complying to the prescribed exercises. |
 |
Figure 3 Pie chart showing the percentage of caregivers compliant to the prescribed number of sessions. |
Discussion
The main goal of this study was to determine the level of perspective of caregivers in the UAE towards physiotherapy treatment for children with burns by examining five major domains: caregiver knowledge, burden, attitude, adherence to physiotherapy exercise, and caregiver satisfaction with physiotherapy service. According to the data obtained from the survey, caregivers had a good level of understanding and awareness of the importance of physiotherapy in children with burns. Compared to men, women made up for the majority of caregivers in the survey. Majorly, the biological mothers of the children with burns provided care while the child was hospitalized and after discharge; this reflects the sociocultural background of the UAE, where mothers are typically responsible for the children’s care and family issues, whereas fathers are responsible for providing financial support to the family. Similar findings were observed in other countries.8 Two studies performed in Zimbabwe8 and India7 described the same socio-demographic features of caregivers; the caregivers sampled for this study were relatively young, with the majority aged 30–39 years, and the caregivers had more than three children at home.17
Caregivers in this study indicated that physiotherapy was helpful in the overall management of burns, leading to proper healing of the burn wound without problems, which supports findings from the literature that physiotherapy is an essential aspect of the entire burn care process.18 The most common type of burn injury was scalding due to hot water, as was the case in most of the literature on burns and the current investigation.19,20 All children with burns in this study were given an exercise regimen that comprised a mix of active and passive joint range of motion exercises, muscle stretching, strengthening, and soft tissue manipulation. According to findings from a study conducted in the United States, heterogeneity in physiotherapy treatment for children with burns resulted in proper wound healing without any problems. The caregivers reported being well informed about the recommended fitness program and its advantages.12
In a previous study conducted in Australia,21 caregivers reported feelings of distress, guilt, blame, and the parental need for information and support, whereas the current study found that caregivers had a favorable attitude towards physiotherapy treatment. In this study, the majority of the caregivers were employed, which contributed to the burden of caring for a burned child, in contrast to other findings from previous studies where the majority of the caregivers were unemployed, which improved their ability to care for the child with burns.8,22 Caregivers reported a low-to-moderate burden of caring for children with burns, according to the current study, with caregivers accepting responsibility for wound care, changing wound dressings, and involving the child with burns in a home exercise program. Contrastingly, caregivers experienced moderate-to-high burden in another study.23
In the current study, caregiver satisfaction with physiotherapy services was quite high, with caregivers complimenting the physiotherapists’ professional behavior and the fact that the child was in good hands.8 The majority of caregivers reported that physiotherapists described their treatment procedures to them and provided them with sufficient justification and reasons for their treatment technique choices. Another study in South Africa found that 50% of caregivers were dissatisfied and unhappy with their child’s pain treatment, the fit of the recommended pressure garment, and the child’s psychosocial results and service.24
During hospital visits, almost all caregivers in this study opted to learn new information about the condition and healthcare from doctors, as opposed to caregivers in a previous study in Singapore, who preferred to learn new information from family members, relatives, and the media.25 For caregivers of children with burns, the transition from hospital to home is difficult because they must restore the child’s feeling of normalcy following the burn episode. As soon as the caregiver arrives at home, he or she must assume the position of a professional healthcare provider by following the care plan and routines. One of the challenges caregivers face at home is adhering to an exercise routine. In a recent study, caregivers were successful in adhering to the number of exercise sessions prescribed by the physiotherapist; however, most of those who were unsuccessful reported that they were unable to adhere to the prescribed exercise program because of the child’s unwillingness to cooperate and because they did not like seeing their child cry during exercise sessions. This is in contrast to a study conducted in the United Kingdom, where nearly half of the participants failed to adhere to an exercise program at home due to the emotional and psychological impact of the burn incident and the presence of other responsibilities at home.10
Nearly half of the participants in this study failed to adhere to an exercise program at home because of the emotional and psychological impact of the burn incident and the presence of their responsibilities toward other siblings. These findings show that the caregivers in our study were well-informed about the importance of physiotherapy in the treatment of children with burns. In a recent study, the majority of caregivers failed to carry out the exercise program prescribed by the therapist because the child always cried during the physiotherapy session. This indicates that physiotherapy is uncomfortable and painful for some children due to the nature of the treatment methods, such as passive range of motion and stretching exercises, both of which are required in the post-burn exercise program.26
Unfortunately, no research has been undertaken in the UAE on the importance of physiotherapy management in children with burn injuries or on parents’ or caregivers’ attitudes or knowledge of physiotherapy treatment in children with burn injuries. In the UAE, there have been limited investigations of pediatric burn epidemiology. The caregivers’ perspective was evaluated in this study using five categories, resulting in a lengthy and time-consuming questionnaire. Despite consenting to receiving the form and online survey, the majority of the caregivers did not complete it for unspecified reasons. Many caregivers of pediatric burn victims had changed their contact information, making it difficult for us to reach them. Due to the COVID-19 pandemic, some caregivers who attended post-burn physiotherapy sessions were reluctant to travel to the hospital for fear of contracting the virus, resulting in a decline in the number of research participants. Because of the unsatisfactory hospital experience, a few caregivers declined to participate in the study.
Limitations of the Study
The questionnaire was not translated into any languages other than English. Given the UAE’s huge expatriate population, a study of caregiver perspectives utilizing questionnaires in many languages might be more relevant. The pandemic situation altered the caregivers’ opinions, and the questionnaire must have contained some items about caregiver burden during the ongoing pandemic situation.
Conclusion
The majority of caregivers of children with burns had a good awareness of the role of physiotherapy in post-burn treatment and a favorable attitude toward physiotherapy provided in hospitals. Although most caregivers were successful in adhering to the physiotherapist’s recommended home exercise routine, and nearly all caregivers indicated a high level of satisfaction with the hospital’s physiotherapy services, caregiver burden was reported to be moderate to severe.
Consent
All participants provided informed consent in accordance with the Declaration of Helsinki.
Funding
The authors declare that no funding was received for the study.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Khazaei S, Shirani F, Afshari M, et al. Etiology and outcome of burns in Hamadan, Iran: a registry-based study. Arch Trauma Res. 2019;8(3):144–148. doi:10.4103/atr.atr_47_19
2. Forjuoh S, Gielen A. Chapter 4. Burns. In: Peden M, Oyegbite K, OzanneSmith J, et al., editors. World Report on Child Injury and Prevention. Geneva: World Health Organization; 2008:79–98.
3. Stachowski M, Kondela-Cebulski P. Physical therapists in burn care: role and staffing patterns. Phys Ther. 1983;63(7):1091–1095. doi:10.1093/ptj/63.7.1091
4. Dissanaike S, Rahimi M. Epidemiology of burn injuries: highlighting cultural and socio-demographic aspects. Int Rev Psychiatry. 2009;21(6):505–511. doi:10.3109/09540260903340865
5. Grivna M, Eid HO, Abu-Zidan FM. Epidemiology of burns in the United Arab Emirates: lessons for prevention. Burns. 2014;40(3):500–505. doi:10.1016/j.burns.2013.08.010
6. Ohgi S, Gu S. Pediatric burn rehabilitation: philosophy and strategies. Burn Trauma. 2013;1:73–79. doi:10.4103/2321-3868.118930
7. Grivna M, Barss P, El-Sadig M. Epidemiology and prevention of child injuries in the United Arab Emirates: a report for SafeKids Worldwide. J Med. 2008:1–44.
8. Peck MD. Epidemiology of burns throughout the world. Part I: distribution and risk factors. Burns. 2011;37(7):1087–1100. doi:10.1016/j.burns.2011.06.005
9. Chiwaridzo M, Zinyando VJ, Dambi JM, Kaseke F, Munambah N, Mudawarima T. Perspectives of caregivers towards physiotherapy treatment for children with burns in Harare, Zimbabwe: a cross-sectional study. Burns Trauma. 2016;1:4.
10. Atiyeh B, Janom HH. Physical rehabilitation of pediatric burns. Ann Burns Fire Disasters. 2014;27(1):37.
11. Andrews N, Jones LL, Moiemen N, Calvert M, Kinghorn P, Litchfield I; PEGASUS Study Group. Below the surface: parents’ views on the factors that influence treatment adherence in paediatric burn scar management—A qualitative study. Burns. 2018;44(3):626–635. doi:10.1016/j.burns.2017.09.003
12. Sözen İ, Güldoğan CE, Yastı AÇ. Etiology of childhood burns and parental awareness in Turkey. Turkish J Surgery. 2016;32(3):168.
13. Celis MM, Suman OE, Huang TT, Yen P, Herndon DN. Effect of a supervised exercise and physiotherapy program on surgical interventions in children with thermal injury. J Burn Care Rehabil. 2003;24(1):57–61. doi:10.1097/00004630-200301000-00014
14. Rone-Adams SA, Stern DF, Walker V. Stress and compliance with a home exercise program among caregivers of children with disabilities. Pediatric Physical Therapy. 2004;16(3):140–148. doi:10.1097/01.PEP.0000136006.13449.DC
15. Enns J, Gawaziuk JP, Khan S, et al. Mental and physical health outcomes in parents of children with burn injuries as compared with matched controls. J Burn Care Res. 2016;37(1):e18–e26. doi:10.1097/BCR.0000000000000309
16. Fairaq A. Population Awareness and Attitude towards First Aid in Burn in Makkah Al-Mukarramah, Saudi Arabia–A Cross Sectional Study. J Pharmaceutical Res Int. 2021;22–29. doi:10.9734/jpri/2021/v33i24B31438
17. Mudawarima T, Chiwaridzo M, Jelsma J, Grimmer K, Muchemwa FC. A systematic review protocol on the effectiveness of therapeutic exercises utilised by physiotherapists to improve function in patients with burns. Syst Rev. 2017;6(1):1–7. doi:10.1186/s13643-017-0592-6
18. Pai MS, Kumar V, Janthosh PP, Sundeep PT. Socio-demographic characteristics of mothers of hospitalised children in surgical wards. Int J Curr Res. 2015;7(9):20676–20679.
19. Cen Y, Chai J, Chen H, Chen J, Guo G, Han C; Chinese Burn Association. Guidelines for burn rehabilitation in China. Burns Trauma. 2015:3:547.
20. Outwater AH, Ismail H, Mgalilwa L, Temu MJ, Mbembati NA. Burns in Tanzania: morbidity and mortality, causes and risk factors: a review. Int J Burns Trauma. 2013;3(1):18.
21. Burd A, Yuen C. A global study of hospitalized paediatric burn patients. Burns. 2005;31(4):432–438. doi:10.1016/j.burns.2005.02.016
22. Lernevall LS, Moi AL, Cleary M, Kornhaber R, Dreyer P. Support needs of parents of hospitalised children with a burn injury: an integrative review. Burns. 2020;46(4):771–781. doi:10.1016/j.burns.2019.04.021
23. Remera JM Perceptions among caregivers and physiotherapists on the importance of chest physiotherapy in asthmatic children attending hospitals in Kigali, Rwanda. Doctoral dissertation, University of the Western Cape.
24. Rimmer RB, Bay RC, Alam NB, et al. Measuring the burden of pediatric burn injury for parents and caregivers: informed burn center staff can help to lighten the load. J Burn Care Res. 2015;36(3):421–427. doi:10.1097/BCR.0000000000000095
25. Parbhoo A. Primary Caregivers’ Evaluation of a Burns Rehabilitation Programme at the Red Cross Childrens’ Hospital. Stellenbosch University; 2005. Doctoral dissertation, Stellenbosch.
26. Thein MM, Lee BW, Bun PY. Knowledge, attitude and practices of childhood injuries and their prevention by primary caregivers in Singapore. Singapore Med J. 2005;46(3):122.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge and Awareness of Non-Technical Skills Over the Course of an Educational Program in Nursing - A Repeated Cross-Sectional Study
Wevling A, Olsen BF, Nygaard AM, Heiberg T
Advances in Medical Education and Practice 2023, 14:31-41
Published Date: 10 January 2023
Knowledge and Attitude of Pediatric Nurses in Saudi Arabia Regarding Child Abuse
Alharbi HF, Moussa FL
Journal of Multidisciplinary Healthcare 2023, 16:2057-2069
Published Date: 20 July 2023
Awareness and Knowledge of Adverse Effects of Topical Corticosteroids Among the General Population in Jeddah, Saudi Arabia
Roblah TM, Baabdullah AM
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3065-3075
Published Date: 26 October 2023
Ethical Awareness and Practices Among Emergency Department Personnel in Riyadh’s Tertiary Hospitals: A Cross-Sectional Analysis
Al-Wathinani AM, AlHokair AA, Almeshari AZ, Alsaqri FS, Aldaihan FM, Alrumeh AS, AlOtaibi AA, Alkanhal IA, Aljuaid M, Albusair MK, Alluhayb AA, Goniewicz K
Risk Management and Healthcare Policy 2024, 17:677-688
Published Date: 23 March 2024
Radiologic Technology Students’ Perceptions on Adoption of Artificial Intelligence Technology in Radiology
Arif WM
International Journal of General Medicine 2024, 17:3129-3136
Published Date: 16 July 2024