Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Capecitabine versus Paclitaxel After CDK4/6 Inhibitor Progression in Hormone Receptor–Positive, HER2-Negative Metastatic Breast Cancer: A Real-World Study
Authors Birsin Z ![]() , Güren AK, Aliyev V, Guliyev M
, Güren AK, Aliyev V, Guliyev M ![]() , Jeral S, Cebeci S, Çerme E
, Jeral S, Cebeci S, Çerme E ![]() , Günaltılı M, Abbasov H
, Günaltılı M, Abbasov H ![]() , Çiçek E, Atak S, Sarı M
, Çiçek E, Atak S, Sarı M ![]() , Demirci NS, Alan Ö
, Demirci NS, Alan Ö ![]()
Received 24 January 2026
Accepted for publication 31 March 2026
Published 15 April 2026 Volume 2026:18 598598
DOI https://doi.org/10.2147/BCTT.S598598
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Zeliha Birsin,1 Ali Kaan Güren,2 Vali Aliyev,1 Murad Guliyev,1 Seda Jeral,1 Selin Cebeci,1 Emir Çerme,1 Murat Günaltılı,1 Hamza Abbasov,1 Ebru Çiçek,1 Süheyla Atak,1 Murat Sarı,2 Nebi Serkan Demirci,1 Özkan Alan1
1Department of Medical Oncology, Faculty of Medicine, Istanbul University-Cerrahpaşa, Istanbul, Turkey; 2Department of Medical Oncology, Faculty of Medicine, Marmara University, Istanbul, Turkey
Correspondence: Zeliha Birsin, Department of Medical Oncology, Faculty of Medicine, Istanbul University-Cerrahpaşa, Kocamustafapaşa Cd. No: 53, Fatih, Istanbul, 34098, Turkey, Tel +90 534 526 06 73, Email [email protected]
Background: Cyclin-dependent kinase 4/6 inhibitors (CDK4/6i) combined with endocrine therapy represent the standard first-line treatment for hormone receptor–positive (HR+), HER2-negative metastatic breast cancer. However, optimal chemotherapy selection after progression on CDK4/6i remains unclear. This study aimed to compare the clinical outcomes of capecitabine versus paclitaxel in a real-world post-CDK4/6i setting.
Methods: This retrospective two-center study included HR+/HER2− metastatic breast cancer patients who experienced disease progression after CDK4/6i therapy and subsequently received either capecitabine or paclitaxel. Paclitaxel was administered at a dose of 80 mg/m2 weekly, while capecitabine was given at 1000– 1250 mg/m2 twice daily on days 1– 14 of a 21-day cycle. Progression-free survival (PFS) and overall survival (OS) were analyzed using the Kaplan–Meier method and Cox regression analyses.
Results: A total of 115 patients were included, of whom 68 (59%) received capecitabine and 47 (41%) received paclitaxel. Baseline clinicopathological characteristics were comparable between the two groups. The median follow-up was 48.3 months. Median PFS was 5.45 months in the capecitabine group and 6.53 months in the paclitaxel group (p = 0.622). Median OS was 42.2 and 43.1 months, respectively (p = 0.299). Treatment type was not independently associated either PFS or OS. Visceral metastasis after CDK4/6i progression independently predicted shorter PFS (HR 1.62, p = 0.042), whereas higher tumor grade was associated with inferior OS (HR 1.82, p = 0.018). Treatment-related toxicities differed between regimens: paclitaxel was predominantly associated with neuropathy and hematologic toxicity, whereas capecitabine was primarily associated with hand–foot syndrome and gastrointestinal toxicity.
Conclusion: Capecitabine and paclitaxel demonstrated comparable efficacy after CDK4/6i progression, with no significant differences in PFS or OS. Given their distinct toxicity profiles, treatment selection should be individualized according to patient characteristics and tolerability.
Keywords: CDK4/6 inhibitors, post-CDK4/6 inhibitor treatment, hormone receptor–positive breast cancer, capecitabine, paclitaxel, real-world study
Introduction
Breast cancer is the most common malignancy among women and remains a leading cause of cancer-related mortality worldwide.1 It is a biologically heterogeneous disease composed of multiple subtypes with distinct molecular characteristics, clinical behaviors, and prognostic implications. In this context, recent studies have identified novel biomarkers associated with tumor biology, the tumor microenvironment, and clinical outcomes.2,3 Among the major molecular subtypes, hormone receptor–positive (HR+), HER2-negative breast cancer constitutes nearly 70% of all cases.4,5 In the metastatic setting, HR+/HER2– disease is primarily managed with endocrine therapy combined with cyclin-dependent kinase 4/6 inhibitors (CDK4/6i), which has become the established first-line standard of care.6,7 This treatment approach is supported by extensive evidence from large randomized clinical trials demonstrating marked improvements in progression-free and overall survival.8–10
Treatment decisions after progression on CDK4/6i remain challenging, as they require careful consideration of multiple clinical and biological factors. Available therapeutic options include endocrine therapy, targeted agents, chemotherapy, and antibody–drug conjugates (ADCs). Current guidelines recommend the use of targeted therapies—such as PI3K or AKT inhibitors,11,12 oral selective estrogen receptor degraders (SERDs) for ESR1-mutant disease,13,14 poly (ADP-ribose) polymerase (PARP) inhibitors for germline BRCA mutations.15,16 In addition, mTOR inhibitors such as everolimus17 and antibody–drug conjugates (ADCs) such as trastuzumab deruxtecan and sacituzumab govitecan are recommended in appropriate clinical subgroups.18–20 When determining treatment strategies after CDK4/6i progression, clinicians must consider the duration of benefit from prior CDK4/6i therapy, overall disease burden, and the patient’s clinical condition. Concurrently, several real-world issues—including financial toxicity, delays in obtaining biomarker results, and limited drug accessibility—further influence therapeutic decision-making.
Despite these considerations, chemotherapy remains one of the most frequently utilized treatment modalities in real world studies following progression on CDK4/6i,21–23 and pivotal CDK4/6i trials have reported post-progression chemotherapy use in approximately 20–50% of patients.24–26 However, to date, no randomized controlled trials have directly compared different chemotherapy regimens specifically in the post-CDK4/6i setting. Although several real-world studies have evaluated chemotherapy outcomes following CDK4/6 inhibitor progression, most have included heterogeneous treatment groups or broad regimen categories (eg, oral vs intravenous therapy), rather than direct comparisons between commonly used chemotherapy agents.27,28 As a result, evidence guiding the optimal selection of chemotherapy in this setting remains limited in routine clinical practice. Therefore, in this two-center study, we aimed to compare the effectiveness of capecitabine versus paclitaxel in patients with HR-positive/HER2-negative metastatic breast cancer who progressed after CDK4/6 inhibitor therapy.
Materials and Methods
Study Design and Patient Inclusion Criteria
This retrospective, two-center study included patients with histopathologically confirmed hormone receptor–positive (HR+), HER2-negative de novo or recurrent metastatic breast cancer diagnosed between January 2014 and January 2024. Hormone receptor and HER2 status were evaluated according to the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines. Estrogen receptor (ER) and progesterone receptor (PR) positivity were defined as ≥1% nuclear staining, while HER2 negativity was defined as an immunohistochemistry (IHC) score of 0, 1+, or 2+ with a negative in situ hybridization (ISH) test.
Patients with either de novo or recurrent metastatic disease were included. Eligible patients had received CDK4/6 inhibitors as either first- or second-line therapy. Those treated with CDK4/6 inhibitors in the second-line setting had previously received endocrine monotherapy in the first-line setting, such as letrozole or tamoxifen. Only patients who developed documented disease progression while receiving CDK4/6 inhibitor therapy and subsequently received paclitaxel or capecitabine were included. Patients who discontinued CDK4/6 inhibitors due to toxicity or patient preference were not included in the study. Paclitaxel was administered at a dose of 80 mg/m2 weekly, whereas capecitabine was given orally at 1000–1250 mg/m2 twice daily on days 1–14 of a 21-day cycle. Chemotherapy was initiated shortly after radiologically confirmed disease progression on CDK4/6 inhibitor therapy according to routine clinical practice.
Patients were excluded if they had received any targeted therapy, including PI3K inhibitors, SERDs, mTOR inhibitors, antibody–drug conjugates (ADCs), or PARP inhibitors following CDK4/6 inhibitor treatment, had a second primary malignancy, had follow-up of less than one year, had an Eastern Cooperative Oncology Group performance status (ECOG PS) greater than 2, were younger than 18 years, or had missing key clinical or survival data.
Data Collection, Study Variables and Outcome Definitions
Clinical, pathological, and treatment-related data were obtained through a comprehensive review of archived patient records and institutional electronic medical records from both centers. Demographic variables (sex and age at metastatic diagnosis) and baseline clinical characteristics, including menopausal status and ECOG PS, were documented. Tumor-related features included histological type and grade, ER and PR expression, Ki-67 proliferation index, and HER2 status.
The pattern of metastatic presentation was classified as de novo or recurrent, and the presence of visceral metastasis at diagnosis and at progression after CDK4/6i therapy was recorded. Patients were considered endocrine–sensitive if they had de novo metastatic breast cancer or experienced disease recurrence more than 12 months after completion of adjuvant endocrine therapy.6 All other patients were classified as endocrine-resistant. Treatment-related variables included the line of therapy in which the CDK4/6i was administered (first or second line), the duration of CDK4/6i exposure, the chemotherapy agent received after CDK4/6i progression (paclitaxel or capecitabine), treatment response, progression status during this chemotherapy, and subsequent systemic therapies. Radiologic evaluations and treatment response assessments were generally performed at approximately 2–3-month intervals in accordance with routine clinical practice, although the exact timing was determined by the treating physician. Adverse events were retrospectively extracted from medical records and graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.29 Patient status at last follow-up (alive or deceased) was also documented.
The primary outcomes of the study were progression-free survival (PFS) and overall survival (OS). PFS was defined as the time from initiation of post-CDK4/6i chemotherapy to radiologic disease progression or death from any cause, whichever occurred first. OS was defined as the time from the diagnosis of metastatic breast cancer to death from any cause.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). The distribution of continuous variables was evaluated using the Shapiro–Wilk test as well as visual inspection of Q–Q plots and histograms. As none of the variables followed a normal distribution, continuous variables were summarized as medians with ranges and compared using non-parametric tests. Categorical variables were reported as frequencies and percentages. Group comparisons were conducted using the Mann–Whitney U-test for continuous variables and the Chi-square test or Fisher’s exact test, as appropriate, for categorical variables.
Progression-free survival (PFS) and overall survival (OS) were analyzed using the Kaplan–Meier method, and survival curves were compared using the Log rank test. Cox proportional hazards regression analysis was performed to identify factors associated with survival outcomes. Variables with p < 0.20 in univariate analysis or considered clinically relevant were included in the multivariable Cox regression model. Interaction analyses were performed to explore potential heterogeneity of treatment effects across clinically relevant subgroups. All statistical tests were two-sided, and a p-value ≤ 0.05 was considered statistically significant.
Ethical Considerations
The study was conducted in compliance with the principles of the Declaration of Helsinki. Due to the retrospective design, the requirement for informed consent was waived. Ethical approval for the study was obtained from the Institutional Review Board (IRB) of Istanbul University–Cerrahpaşa, Cerrahpaşa Faculty of Medicine (Approval No: 624/2025, dated October 3, 2025).
Results
Baseline Clinical, Demographic, and Treatment Characteristics
A total of 115 patients were included in the study cohort, of whom 68 (59%) received capecitabine and 47 (41%) received paclitaxel following progression on CDK4/6i therapy. The median age at metastatic diagnosis was 55 years (range, 27–85). Menopausal status, ER and PR expression levels, tumor grade, and HER2 scores were comparable between the capecitabine and paclitaxel groups, with no statistically significant differences observed (all p> 0.05). Ki-67 proliferation indices differed significantly between the treatment arms, with the paclitaxel group demonstrating higher proliferation indices compared with the capecitabine group (median 30% vs. 20%, p = 0.033). At the initiation of CDK4/6 inhibitor therapy, 72% of patients in the overall cohort had endocrine-sensitive disease, while 28% were classified as endocrine-resistant; notably, endocrine-sensitive disease was more frequent in the paclitaxel group at baseline (p=0.032).
At baseline, the proportions of patients with de novo metastatic disease, prior taxane exposure, first-line CDK4/6 inhibitor use, visceral metastasis, liver metastasis, and the number of metastatic sites were comparable between the two treatment groups (all p> 0.05).
At the time of data cutoff, 59% of the overall cohort had died, with comparable mortality rates between capecitabine (60%) and paclitaxel (57%) treatment arms (p=0.760). All findings are summarized in Table 1.
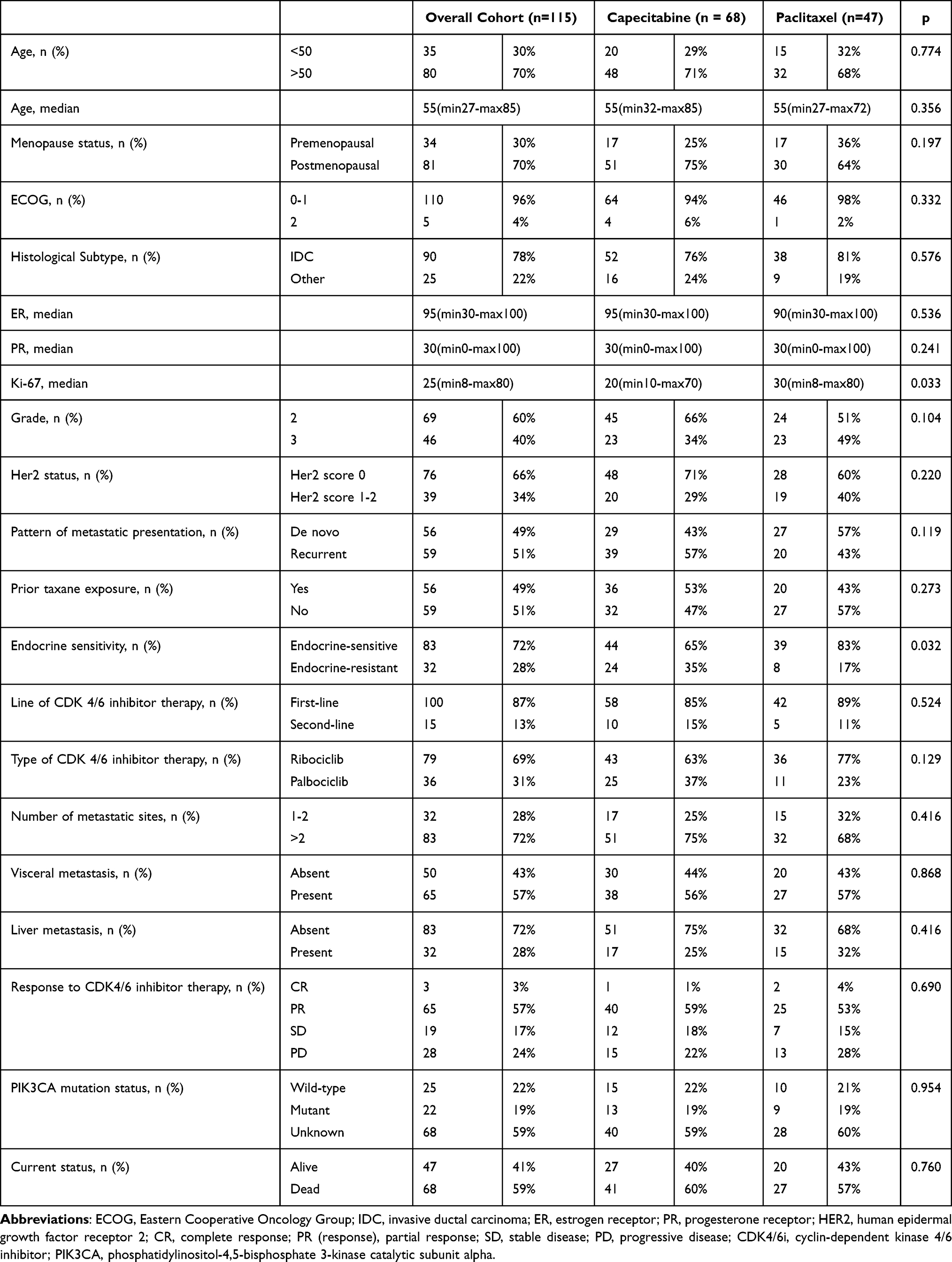 |
Table 1 Baseline Demographic and Clinicopathological Characteristics |
Post-CDK4/6i Treatment Response and Toxicity
Post-CDK4/6 inhibitor chemotherapy outcomes and toxicity data are presented in Table 2. Visceral metastasis at the time of CDK4/6i progression was present in 71% of the overall cohort, with comparable rates between the capecitabine and paclitaxel groups (69% vs. 74%, p = 0.533). The objective response rate (ORR) was 40% in the capecitabine group and 60% in the paclitaxel group, although this difference was not statistically significant (p = 0.089). The distribution of CDK4/6 inhibitor exposure duration (<12 vs ≥12 months) was comparable between the two treatment groups (52% vs 48%; p = 0.187).
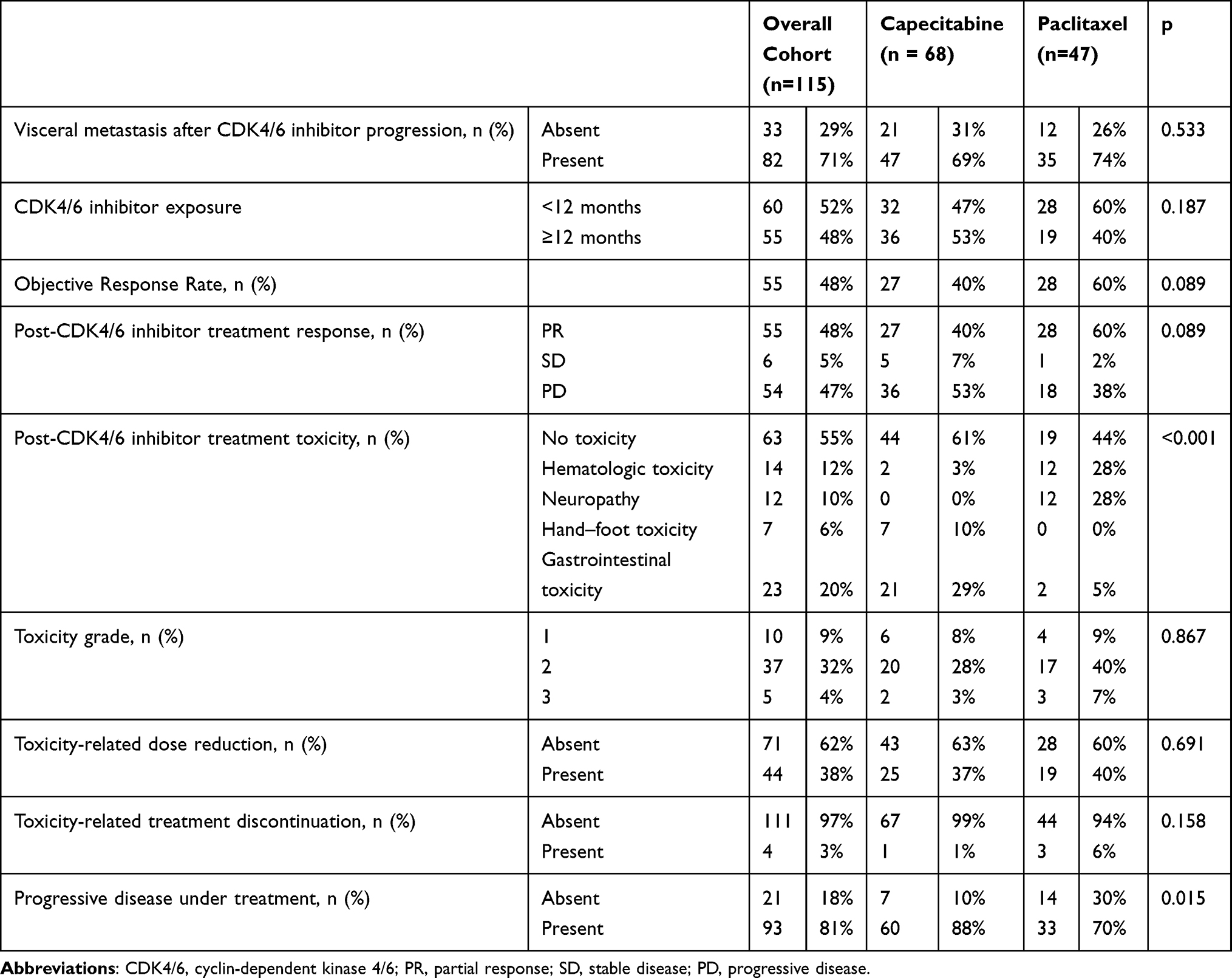 |
Table 2 Post-CDK4/6 Inhibitor Treatment Response and Toxicity |
Toxicity profiles differed markedly between treatments groups. Hematologic toxicity and peripheral neuropathy were more frequently observed in the paclitaxel group (28% and 28%, respectively). Hand–foot syndrome occurred exclusively in patients receiving capecitabine (10%), whereas gastrointestinal toxicity was significantly more common with capecitabine than paclitaxel (29% vs. 5%) (p<0.001). Treatment discontinuation due to toxicity occurred in 1 patient (1%) in the capecitabine group and 3 patients (6%) in the paclitaxel group, although this difference was not statistically significant (p = 0.158).
Among patients initially treated with capecitabine after CDK4/6 inhibition, 52.4% subsequently received paclitaxel, whereas 65.9% of those who initially received paclitaxel later received capecitabine. The use of other subsequent systemic therapies—including everolimus plus exemestane, fulvestrant, and platinum-based chemotherapy—was comparable between the two groups (Table S1).
Progression Free Survival Outcome
The median follow-up duration was 48.3 months (95% CI, 44.7–52.0). Median PFS was similar between the two groups: 5.45 months for capecitabine (95% CI, 3.51–7.39) and 6.53 months for paclitaxel (95% CI, 3.26–9.82), with no significant difference on Log rank testing (p = 0.622) (Figure 1).
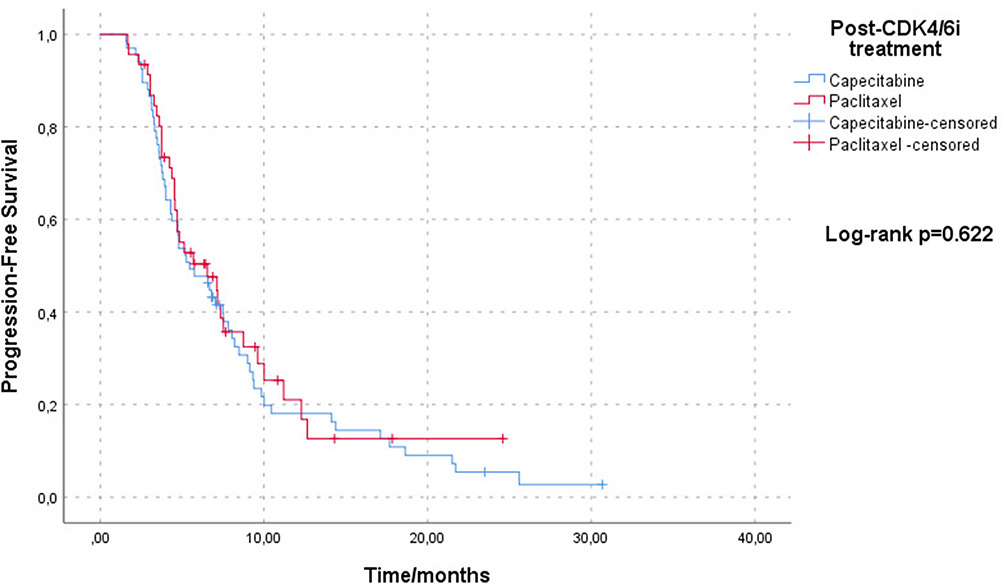 |
Figure 1 Progression-Free Survival According to Capecitabine and Paclitaxel. Kaplan–Meier curves showing progression-free survival (PFS) in patients treated with capecitabine or paclitaxel after progression on CDK4/6 inhibitor–based therapy. Tick marks indicate censored observations. |
In Cox regression analysis, treatment type was not significantly associated with PFS (HR 1.05, 95% CI 0.68–1.62; p = 0.822). Visceral metastasis at time of progression on CDK4/6 inhibitor therapy emerged as the only factor independently associated with inferior PFS (HR 1.62, 95% CI 1.01–2.57; p = 0.042), whereas no other clinical or pathological variables demonstrated a significant impact on PFS (Table 3).
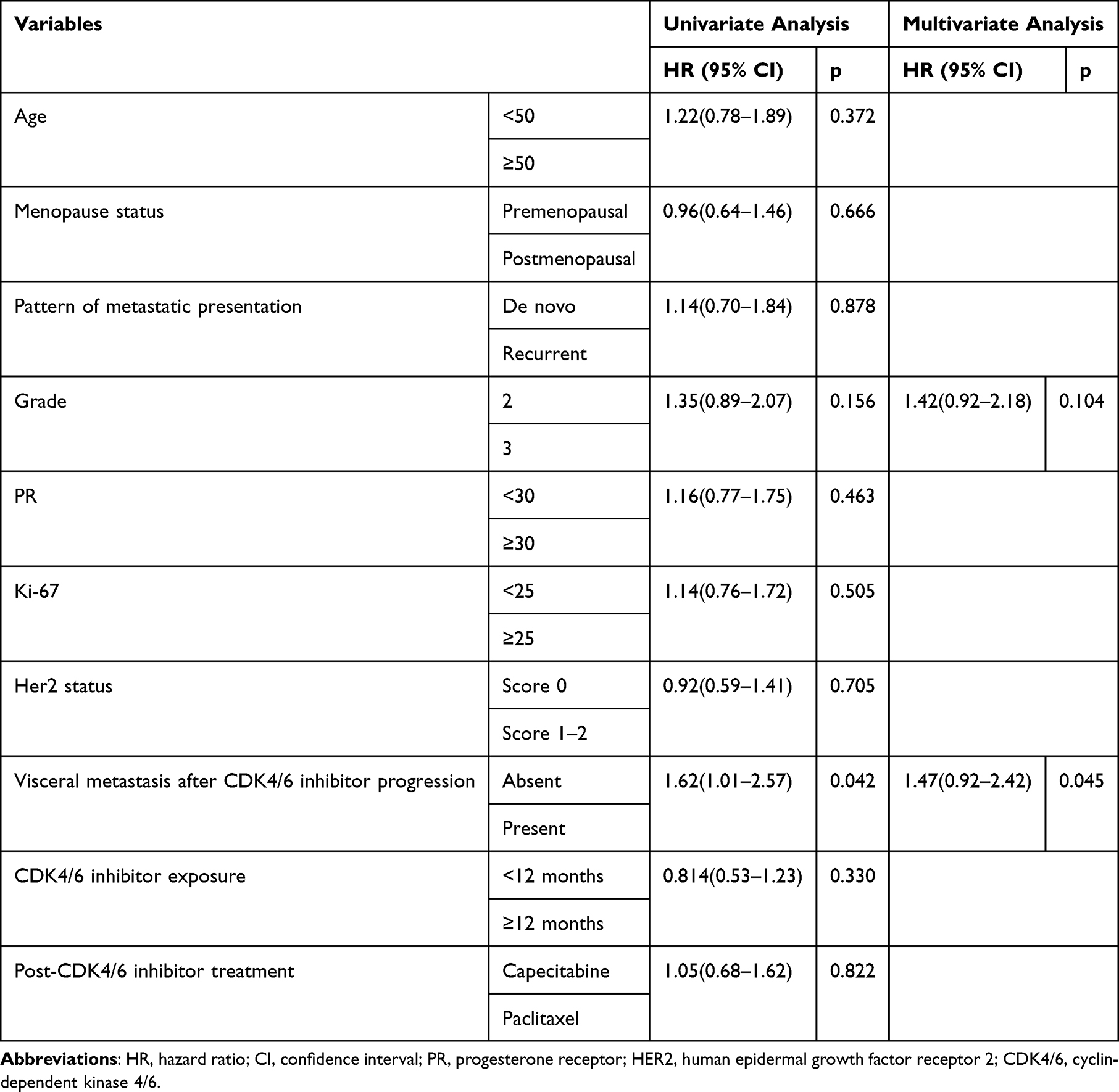 |
Table 3 Univariate and Multivariate Cox Regression Analysis for Progression-Free Survival in Patients with Metastatic HR-Positive HER2-Negative Breast Cancer |
In subgroup analyses, no significant differences in PFS were observed between capecitabine and paclitaxel across all predefined clinical subgroups, including age, menopausal status, duration of prior CDK4/6 inhibitor therapy, and visceral disease involvement (Figure 2).
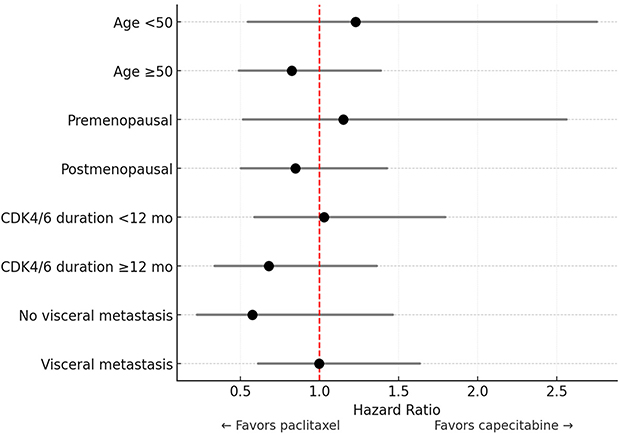 |
Figure 2 Subgroup Analysis of Progression-Free Survival. Forest plot showing hazard ratios for progression-free survival (PFS) comparing paclitaxel versus capecitabine across clinical subgroups. Left (<1) favors paclitaxel; right (>1) favors capecitabine. “mo” denotes months. |
Overall Survival Outcome
Median OS was similar between the two groups: 40.4 months for capecitabine (95% CI, 36.1–42.9) and 39.1 months for paclitaxel (95% CI, 27.3–48.8), with no significant difference on log-rank analysis (p = 0.299) (Figure 3).
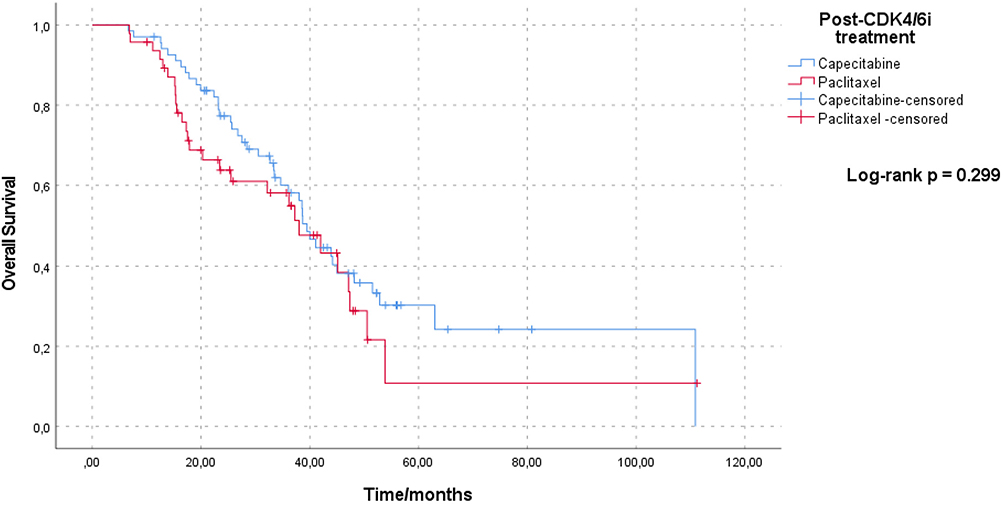 |
Figure 3 Overall Survival According to Capecitabine and Paclitaxel. Kaplan–Meier curves showing overall survival (OS) in patients treated with capecitabine or paclitaxel after progression on CDK4/6 inhibitor–based therapy. |
Consistent with these findings, Cox regression analysis demonstrated no association between treatment type and OS (HR 1.29, 95% CI 0.79–2.11; p = 0.301). In multivariate analysis, tumor grade emerged as the only independent predictor of OS (HR 1.82, 95% CI 1.10–3.01; p = 0.018), while endocrine sensitivity showed a trend towards significance but did not reach statistical significance (HR 1.62, 95% CI 0.99–2.63; p = 0.052). No other clinical and pathological variables were significantly associated with OS (Table 4).
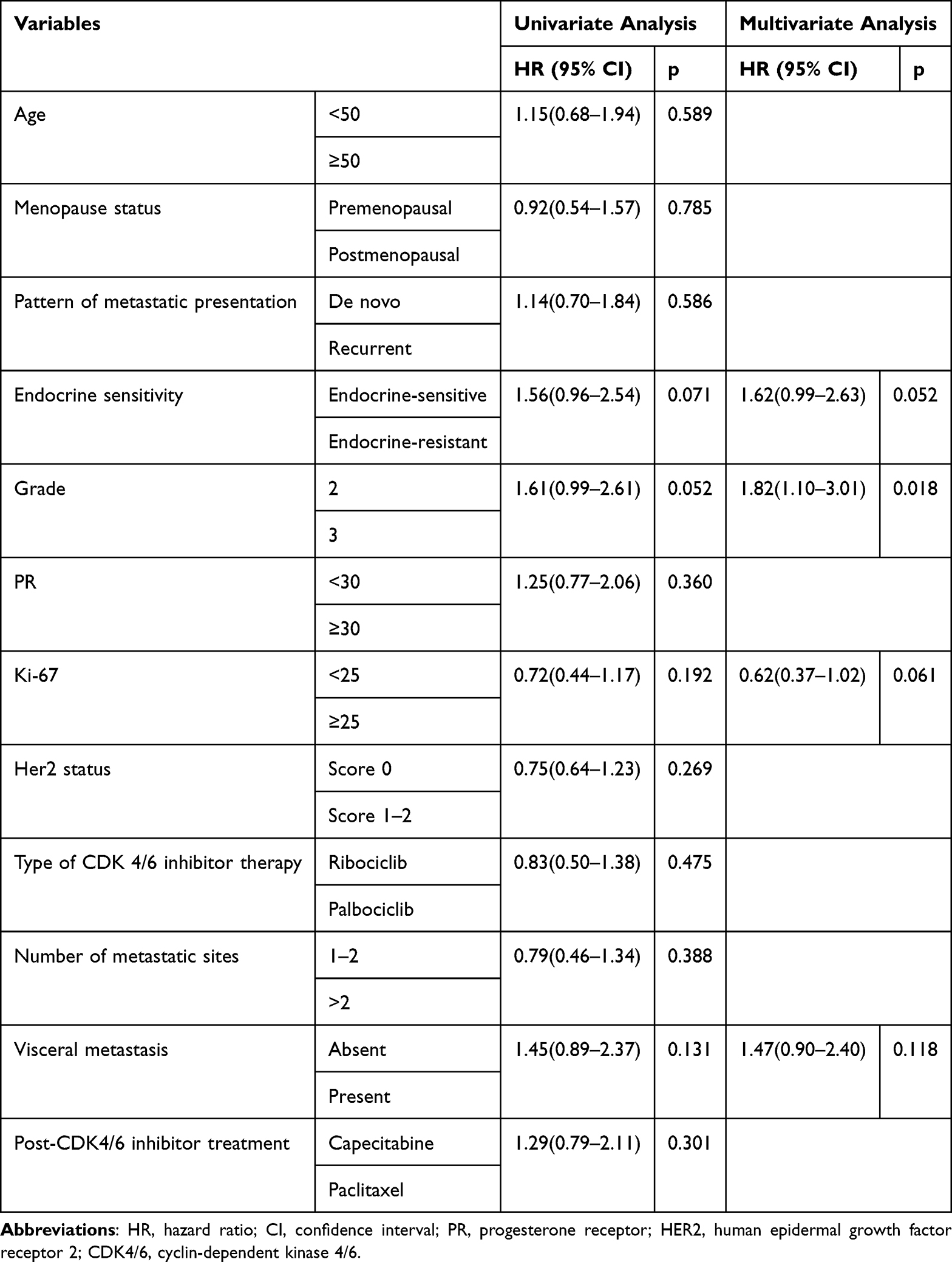 |
Table 4 Univariate and Multivariate Cox Regression Analysis for Overall Survival in Patients with Metastatic HR-Positive HER2-Negative Breast Cancer |
Subgroups analyses of OS showed no treatment-specific benefit favoring either capecitabine or paclitaxel across age groups, menopausal status, duration of prior CDK4/6 inhibitor exposure, or visceral metastasis status (Figure 4).
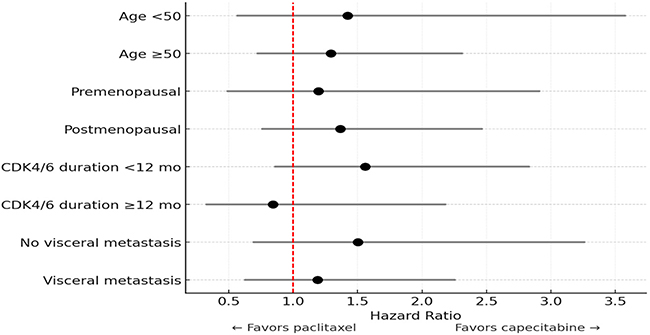 |
Figure 4 Subgroup Analysis of Overall Survival. Forest plot showing hazard ratios for overall survival (OS) comparing paclitaxel versus capecitabine across clinical subgroups. Left (<1) favors paclitaxel; right (>1) favors capecitabine. “mo” denotes months. |
Discussion
In this two-center retrospective study, we compared capecitabine and paclitaxel as post-CDK4/6i treatment options for patients with HR+/HER2− metastatic breast cancer. Our findings indicate that capecitabine and paclitaxel demonstrated comparable clinical activity in the post-CDK4/6i setting. PFS did not differ between the two treatment groups (log-rank p = 0.622), and OS was likewise similar (log-rank p = 0.299). Cox regression analyses further confirmed that treatment type was not associated with PFS or OS, while the presence of visceral metastasis predicted shorter PFS and higher tumor grade was associated with poorer OS.
The introduction of CDK4/6 inhibitors has fundamentally reshaped the therapeutic landscape for HR+/HER2− advanced and metastatic breast cancer.6,7 Following disease progression on CDK4/6 inhibitor–based first-line therapy, international guidelines recommend comprehensive molecular profiling—including gBRCA, ESR1, AKT, PI3K, and PTEN alterations—to inform optimal second-line treatment selection and identify patients who may benefit from targeted therapeutic strategies.6,7 For patients who demonstrate endocrine resistance and lack targeted treatment options due to the absence of actionable molecular alterations, systemic chemotherapy remains an appropriate and clinically justified therapeutic approach. Consistent with this treatment framework, major CDK4/6 inhibitor trials have reported heterogeneous patterns of subsequent chemotherapy use. Notably, across these trials, paclitaxel and capecitabine have consistently been the most commonly used chemotherapy agents in the post-progression setting;30,31 however, a direct and systematic comparison of their relative efficacy has not been well characterized.
Previous real-world and clinical studies assessing chemotherapy outcomes following first-line CDK4/6 inhibitor treatment have reported median PFS values generally falling within the range of approximately 4 to 7 months.27,32,33 Similarly, in our study, median PFS was comparable between treatment groups, with 5.45 months for capecitabine and 6.53 months for paclitaxel. Michel et al27 evaluated 215 patients who progressed after first-line CDK4/6 inhibitor therapy and subsequently received chemotherapy, reporting capecitabine as the most commonly used regimen, followed by taxane-based combinations, capecitabine plus bevacizumab, single-agent taxanes, and anthracycline-containing treatments. Importantly, their analysis showed that the choice of chemotherapy did not significantly influence PFS or OS. Consistent with these observations, capecitabine also emerged as the most frequently administered agent in our cohort, and similarly, we found no significant differences in PFS or OS between patients receiving capecitabine and those treated with paclitaxel.
In contrast to our study, Berton Giachetti et al28 evaluated 506 patients with HR+/HER2– metastatic breast cancer who progressed on CDK4/6 inhibitor–based endocrine therapy. Following progression, 43.7% received ET-based treatment and 56.3% received chemotherapy; among those receiving chemotherapy, 63% were treated with oral regimens—predominantly capecitabine—while 37% received intravenous regimens, most commonly taxane-based therapies. Oral chemotherapy was associated with a longer median PFS compared with intravenous chemotherapy (6.89 vs. 5.44 months); however, this PFS benefit did not translate into a statistically significant OS advantage in the overall cohort. A significant OS difference was observed only among patients with visceral metastases, in whom intravenous chemotherapy was associated with poorer survival outcomes. In our cohort, although PFS was numerically longer in the paclitaxel group, no statistically significant differences were observed between the paclitaxel and capecitabine groups. Moreover, subgroup analyses in our study did not confirm the findings of Berton Giachetti et al,28 as no significant differences were detected across any subgroup. Consistent with the findings of Berton Giachetti et al,28 Bender et al33 also reported a median PFS of 7.1 months among patients treated with capecitabine after progression on CDK4/6 inhibitor–based endocrine therapy. In our cohort, the median PFS for patients receiving capecitabine was 5.45 months, which is in line with the findings reported by Michel et al27 for single-agent capecitabine (median PFS: 5.1 months). The modest differences in PFS observed across these studies may be attributable to variations in patient population characteristics, prior treatment exposure, and disease burden.
In our cohort, paclitaxel and capecitabine demonstrated comparable PFS and OS outcomes, suggesting that efficacy alone may not be the primary determinant when selecting between these agents. However, toxicity differences remain clinically relevant. Notably, three patients in the paclitaxel group were unable to continue maintenance therapy due to treatment-related neuropathy. Paclitaxel-associated peripheral neuropathy and hematologic toxicity can be managed with dose modifications, regular hematologic monitoring, and supportive care.34 In contrast, capecitabine-related hand–foot syndrome may be alleviated with moisturizing strategies, avoidance of mechanical stress, and dose adjustments, while gastrointestinal toxicity is generally manageable with antiemetic and antidiarrheal treatments.35 Taken together, these toxicity considerations highlight that treatment selection in routine clinical practice should incorporate not only efficacy but also toxicity profiles, patient comorbidities, treatment tolerability, and individual patient preferences.
While our findings are largely consistent with previous reports, the present study provides a more focused comparison between commonly used chemotherapy agents—specifically capecitabine and paclitaxel—in the post-CDK4/6 inhibitor setting, thereby offering clinically relevant insights for treatment selection in routine practice.
Our study has several limitations. First, its retrospective design introduces an inherent risk of bias. Furthermore, treatment allocation was not randomized and may have been influenced by physician preference and patient characteristics, introducing potential selection bias. As this was a two-center study conducted over a long study period, variations in clinical practice and treatment decision-making may also have influenced the results. Additionally, the relatively small sample size may limit the statistical power and generalizability of the findings. No formal sample size or power calculation was performed due to the retrospective nature of the study, and the study may be underpowered to detect small differences, particularly in subgroup analyses. Molecular data were also incomplete, as PIK3CA, ESR1, and BRCA mutation status were unknown for most patients, precluding a comprehensive assessment of the potential impact of these alterations on chemotherapy outcomes. These molecular alterations may influence chemotherapy sensitivity and tolerability, and their absence limits the interpretation of treatment response in this cohort. In addition, adverse events were collected retrospectively from medical records, which may have led to underreporting of some toxicities.
Conclusion
In this two-center retrospective study, capecitabine and paclitaxel demonstrated comparable clinical efficacy in the post-CDK4/6 inhibitor setting, with no significant differences in PFS or OS. Subgroup analyses also showed no treatment specific differences between the two agents. Given their differing toxicity profiles, treatment selection in routine clinical practice should take into account patient comorbidities, treatment tolerability, and individual patient preferences. Larger prospective studies are needed to confirm these findings and better guide treatment decisions in this context.
Institutional Review Board Statement
This retrospective study was approved by the Ethics Committee of Istanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine (Approval No: 624/2025, dated October 3, 2025). The study was conducted in accordance with the principles of the Declaration of Helsinki and the Good Clinical Practice Guidelines of the Turkish Medicines and Medical Devices Agency.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Informed Consent Statement
The requirement for informed consent was waived due to the retrospective nature of the study and the use of de-identified data, as approved by the Ethics Committee of Istanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that there are no conflicts of interest related to this study.
References
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–13. doi:10.3322/caac.21820
2. Wang J, Wang Y, Ma H, et al. CLIC6’s role in cancer: from broad analysis to breast cancer validation. Front Oncol. 2025;15. doi:10.3389/fonc.2025.1667589
3. Aimaiti X, Wang Y, Ismtula D, et al. Bystin is a prognosis and immune biomarker: from pan-cancer analysis to validation in breast cancer. Breast Cancer. 2025;17:755–779. doi:10.2147/bctt.S537429
4. Howlader N, Altekruse SF, Li CI, et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. 2014;106(5). doi:10.1093/jnci/dju055
5. Matutino A, Joy AA, Brezden-Masley C, Chia S, Verma S. Hormone receptor-positive, HER2-negative metastatic breast cancer: redrawing the lines. Curr Oncol. 2018;25(Suppl 1):S131–s41. doi:10.3747/co.25.4000
6. Gennari A, André F, Barrios CH, et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol. 2021;32(12):1475–1495. doi:10.1016/j.annonc.2021.09.019
7. Al Sukhun S, Temin S, Barrios CH, et al. Systemic treatment of patients with metastatic breast cancer: ASCO resource-stratified guideline. JCO Glob Oncol. 2024;10:e2300285. doi:10.1200/go.23.00285
8. Lu YS, Im SA, Colleoni M, et al. Updated overall survival of ribociclib plus endocrine therapy versus endocrine therapy alone in pre- and perimenopausal patients with HR+/HER2- advanced breast cancer in MONALEESA-7: a Phase III randomized clinical trial. Clin Cancer Res. 2022;28(5):851–859. doi:10.1158/1078-0432.Ccr-21-3032]
9. Sledge GW Jr, Toi M, Neven P, et al. The effect of abemaciclib plus fulvestrant on overall survival in hormone receptor-positive, ERBB2-negative breast cancer that progressed on endocrine therapy-MONARCH 2: a randomized clinical trial. JAMA Oncol. 2020;6(1):116–124. doi:10.1001/jamaoncol.2019.4782
10. Cristofanilli M, Rugo HS, Im S-A, et al. Overall survival with palbociclib and fulvestrant in women with HR+/HER2− ABC: updated exploratory analyses of PALOMA-3, a double-blind, Phase III randomized study. Clin Cancer Res. 2022;28(16):3433–3442. doi:10.1158/1078-0432.Ccr-22-0305
11. André F, Ciruelos E, Rubovszky G, et al. Alpelisib for PIK3CA -mutated, hormone receptor–positive advanced breast cancer. N Engl J Med. 2019;380(20):1929–1940. doi:10.1056/NEJMoa1813904
12. Rugo HS, Oliveira M, Howell SJ, et al. Capivasertib and fulvestrant for patients with hormone receptor-positive advanced breast cancer: characterization, time course, and management of frequent adverse events from the phase III CAPItello-291 study. ESMO Open. 2024;9(9):103697. doi:10.1016/j.esmoop.2024.103697
13. Bidard F-C, Kaklamani VG, Neven P, et al. Elacestrant (oral selective estrogen receptor degrader) versus standard endocrine therapy for estrogen receptor–positive, human epidermal growth factor receptor 2–negative advanced breast cancer: results from the randomized phase III EMERALD trial. J Clin Oncol. 2022;40(28):3246–3256. doi:10.1200/jco.22.00338
14. Bidard F-C, Mayer EL, Park YH, et al. First-line camizestrant for emerging ESR1 -mutated advanced breast cancer. N Engl J Med. 2025;393(6):569–580. doi:10.1056/NEJMoa2502929
15. Litton JK, Rugo HS, Ettl J, et al. Talazoparib in patients with advanced breast cancer and a germline BRCA mutation. N Engl J Med. 2018;379(8):753–763. doi:10.1056/NEJMoa1802905
16. Robson M, Im S-A, Senkus E, et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N Engl J Med. 2017;377(6):523–533. doi:10.1056/NEJMoa1706450
17. Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor–positive advanced breast cancer. N Engl J Med. 2012;366(6):520–529. doi:10.1056/NEJMoa1109653
18. Rugo HS, Bardia A, Tolaney SM, et al. TROPiCS-02: a Phase III study investigating sacituzumab govitecan in the treatment of HR+/HER2- metastatic breast cancer. Future Oncol. 2020;16(12):705–715. doi:10.2217/fon-2020-0163
19. Modi S, Jacot W, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9–20. doi:10.1056/NEJMoa2203690
20. Bardia A, Hu X, Dent R, et al. Trastuzumab deruxtecan after endocrine therapy in metastatic breast cancer. N Engl J Med. 2024;391(22):2110–2122. doi:10.1056/NEJMoa2407086
21. Choong GM, Liddell S, Ferre RAL, et al. Clinical management of metastatic hormone receptor-positive, HER2-negative breast cancer (MBC) after CDK 4/6 inhibitors: a retrospective single-institution study. Breast Cancer Res Treat. 2022;196(1):229–237. doi:10.1007/s10549-022-06713-1
22. Read SH, Quignot N, Kapso-Kapnang R, et al. Treatment patterns of patients with HR+/HER2- metastatic breast cancer receiving CDK4/6 inhibitor-based regimens: a cohort study in the French nationwide healthcare database. Breast Cancer Res Treat. 2024;204(3):579–588. doi:10.1007/s10549-023-07201-w
23. Sawaki M, Muramatsu Y, Togo K, Iwata H. Real-world treatment patterns of subsequent therapy after palbociclib in patients with advanced breast cancer in Japan. Breast. 2023;70:1–7. doi:10.1016/j.breast.2023.05.006
24. Rugo HS, Im S-A, Joy AA, et al. Effect of palbociclib plus endocrine therapy on time to chemotherapy across subgroups of patients with hormone receptor‒positive/human epidermal growth factor receptor 2‒negative advanced breast cancer: post hoc analyses from PALOMA-2 and PALOMA-3. Breast. 2022;66:324–331. doi:10.1016/j.breast.2022.11.005
25. Im S-A, Lu Y-S, Bardia A, et al. Overall survival with ribociclib plus endocrine therapy in breast cancer. N Engl J Med. 2019;381(4):307–316. doi:10.1056/NEJMoa1903765
26. Johnston S, O’Shaughnessy J, Martin M, et al. Abemaciclib as initial therapy for advanced breast cancer: MONARCH 3 updated results in prognostic subgroups. NPJ Breast Cancer. 2021;7(1):80. doi:10.1038/s41523-021-00289-7
27. Michel LL, Ziegler P, Kreis P, et al. Prognostic impact of the choice of chemotherapy after first-line CDK4/6 inhibitor therapy in patients with metastatic hormone receptor-positive, HER2-negative breast cancer. Eur J Cancer. 2025;227:115689. doi:10.1016/j.ejca.2025.115689
28. Berton Giachetti PPM, Morganti S, Gandini S, et al. Survival following CDK4/6 inhibitor therapy for hormone receptor-positive, ERBB2-negative metastatic breast cancer. JAMA Network Open. 2025;8(2):e2461067. doi:10.1001/jamanetworkopen.2024.61067
29. Diagnosis NCIDoCT. CTCAE and Adverse Event Reporting 2025 [Available from: https://dctd.cancer.gov/research/ctep-trials/for-sites/adverse-events.
30. Hortobagyi GN, Stemmer SM, Burris HA, et al. Overall survival with Ribociclib plus letrozole in advanced breast cancer. N Engl J Med. 2022;386(10):942–950. doi:10.1056/NEJMoa2114663
31. Finn RS, Martin M, Rugo HS, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016;375(20):1925–1936. doi:10.1056/NEJMoa1607303
32. Martin JM, Handorf EA, Montero AJ, Goldstein LJ. Systemic therapies following progression on first-line CDK4/6-inhibitor treatment: analysis of real-world data. Oncologist. 2022;27(6):441–446. doi:10.1093/oncolo/oyac075
33. Bender L, Pflumio C, Trensz P, et al. Capecitabine efficacy after cycline-dependent-kinase 4/6 inhibitor plus endocrine therapy in metastatic hormone receptor-positive breast cancer. Cancer Treat Res Commun. 2023;36:100738. doi:10.1016/j.ctarc.2023.100738]
34. Mahmoud AMAS, El Said NO, Shash E, Ateyya H. Prevention of paclitaxel-induced peripheral neuropathy: literature review of potential pharmacological interventions. Future J Pharm Sci. 2024;10(1):67. doi:10.1186/s43094-024-00638-w
35. Saif MW, Katirtzoglou NA, Syrigos KN. Capecitabine: an overview of the side effects and their management. Anticancer Drugs. 2008;19(5):447–464. doi:10.1097/CAD.0b013e3282f945aa
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Outcome and Safety of the TCX Regimen for Advanced Gastric Cancer: A Prospective Cohort Study
Nguyen HT, Do KH, Le NB, Tran T
Cancer Management and Research 2022, 14:2825-2837
Published Date: 19 September 2022