")
Back to Journals » Cancer Management and Research » Volume 14
Treatment Outcome and Safety of the TCX Regimen for Advanced Gastric Cancer: A Prospective Cohort Study
Authors Nguyen HT, Do KH , Le NB, Tran T
Received 3 August 2022
Accepted for publication 12 September 2022
Published 19 September 2022 Volume 2022:14 Pages 2825—2837
DOI https://doi.org/10.2147/CMAR.S384325
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Hieu Trong Nguyen,1 Kien Hung Do,2 Nguyen Ba Le,3 Thang Tran4
1Department of Medical Oncology 2, Hanoi Oncology Hospital, Hanoi, Vietnam; 2Department of Medical Oncology 1, National Cancer Hospital of Vietnam, Hanoi, Vietnam; 3Ha Thanh Hospital, Hanoi, Vietnam; 4Department of Medical Oncology 4, National Cancer Hospital of Vietnam, Hanoi, Vietnam
Correspondence: Hieu Trong Nguyen, Department of Medical Oncology 2, Hanoi Oncology Hospital, 42A Thanh Nhan, Thanh Nhan, Hai Ba Trung, Hanoi, Vietnam, Tel +84 983230112, Email [email protected]
Objective: To evaluate the outcome and safety of the paclitaxel, carboplatin, and capecitabine (TCX) regimen in patients with advanced gastric cancer.
Methods: Advanced gastric cancer patients received the TCX regimen for up to six cycles, which were 3 weeks apart. Paclitaxel (175 mg/m2) was given over a 3-hour infusion, followed by carboplatin in a 1-hour infusion on day 1. Capecitabine (850 mg/m2) was given orally twice daily from day 1 to day 14. Primary endpoints were progression-free survival (PFS) and overall survival (OS).
Results: Among 83 patients at stage IVa and IVb, the median PFS was 9.3 months; 6-month, 1-year, and 2-year PFS were 74.6%, 32.5%, and 14.4%, respectively. The median OS was 17.0 months; 6-month, 1-year, and 2-year OS were 97.5%, 68.7%, and 21.7%, respectively. In the multivariable Cox regression model, higher CEA was associated with poor OS. Common adverse events included hand-food syndrome (77.9%), peripheral neuropathy (63.2%), fatigue (68.7%), and nausea (54.2%).
Conclusion: The TCX regimen provided good survival and a better safety profile. More clinical trials are needed to confirm its treatment efficacy and safety, especially in comparison with other triplet regimens.
Keywords: paclitaxel, carboplatin, capecitabine, advanced gastric cancer, efficacy
Introduction
Gastric cancer is one of the most common cancers and the leading cause of death in Vietnam.1 Around 87% of patients with gastric cancer are diagnosed at late stages.2 While curative surgery (combined with chemotherapy as an adjuvant treatment) is effective in early-stage patients,3 it is often not possible in late-stage patients; even if it is possible, recurrence and metastasis after surgery are common.4 As a result, chemotherapy plays a key role at this stage. In addition to improving patient’s symptoms and quality of life, chemotherapy also improves survival. In a 2017 systematic review of chemotherapy for advanced gastric cancer, the hazard of death in patients receiving chemotherapy was one-third of that in patients receiving best supportive care.5 However, toxicity and efficacy should be considered when choosing any chemotherapy regimen.
Currently, no standard chemotherapy regimen has been globally approved for patients with advanced gastric cancer. Although the DCF (docetaxel, cisplatin and 5-fluorouracil) regimen has been found to improve survival and response rate, its hematological toxicities, such as febrile neutropenia, are common.6–15 The TCX (paclitaxel, carboplatin, and capecitabine) regimen was developed with aim to reduce the toxicity and improve tolerability while maintaining treatment efficacy. In particular, paclitaxel has been linked to lower severe hematological toxicity compared to docetaxel regimens.16–18 Carboplatin has been associated with less severe nausea/vomiting, thus is expected to improve tolerability and adherence.19–21 Capecitabine is preferred to continuous infusion of 5-FU because it is more convenient, less costly, and associated with less severe hematological toxicity, including neutropenia and neutropenia febrile.22 However, no trial has been conducted to investigate the efficacy of the TCX regimen on advanced gastric cancer patients, with the exception of two studies on metastatic distal esophageal cancer and esophagogastric junction cancer.23,24
In Vietnam, ECF (epirubicin, cisplatin, and 5-fluorouracil), EOX (epirubicin, oxaliplatin, and capecitabine), DCF (docetaxel, cisplatin, and 5-fluorouracil), and DCX (docetaxel, cisplatin, and capecitabine) are commonly used for cancer patients at the late stages. The TCX regimen has been introduced in Vietnam since 2016, but no studies have been done to describe its treatment outcome on advanced gastric cancer. Therefore, in this study, we aimed to evaluate the treatment outcome and safety of the TCX regimen on patients with advanced gastric cancer.
Materials and Methods
Study Design
A prospective cohort study was conducted from January 2016 to February 2020 at Hanoi Oncology Hospital on 83 patients diagnosed with advanced gastric cancer and received TCX regimen for at least 3 cycles.
Patient Eligibility
Eligible patients were those with histologically proven advanced gastric cancer (stage IVa/IVb according to the eighth American Joint Committee on Cancer (ACJJ) staging system for gastric carcinoma25 or metastatic cancer with a history of curative surgery) and an Eastern Cooperative Oncology Group Performance Status (ECOG PS) ≤2 who were planned to start TCX regimen within 4 weeks. Exclusion criteria were prior chemotherapy, HER2-positive gastric cancer, second cancer, a life expectancy of less than 3 months, altered mental status, absolute neutrophil count ≤1500 mm3, platelet count ≤100,000 mm3, insufficient liver function (total serum bilirubin >1.5 times the upper normal limit [UNL] or alanine transferase (ALT) >2.5 times or aspartate transferase (AST) >5 times the UNL in patients with liver metastasis), and insufficient renal function (serum creatinine level >1.25 mg/dl or creatinine clearance >60 mL/min). Figure 1 summarizes the screening, recruitment, and follow-up process of this study.
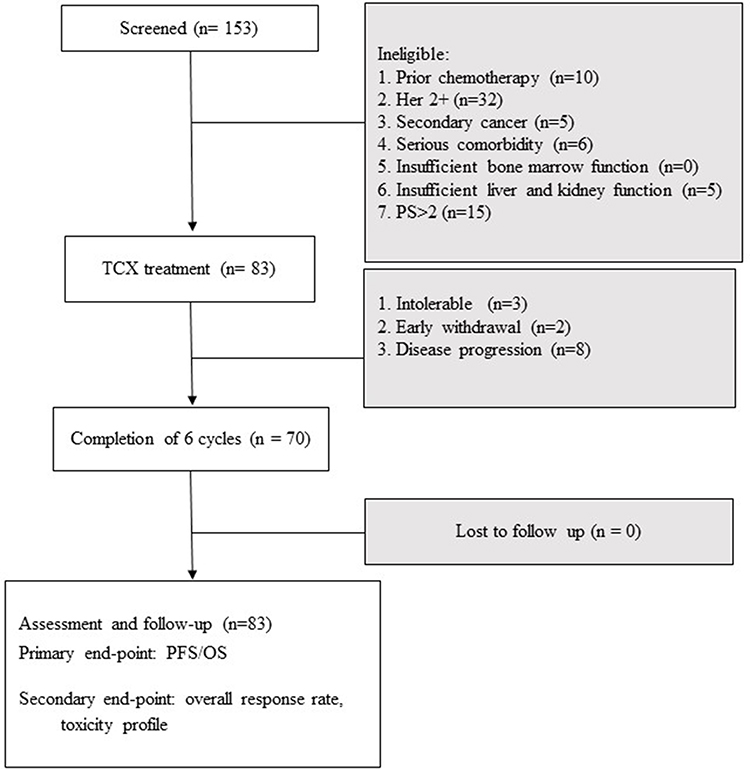 |
Figure 1 Study flow chart. |
Treatment Schedule
Participants would receive the TCX regimen which includes paclitaxel, carboplatin, and capecitabine for up to six cycles, repeated every 3 weeks. Paclitaxel (175 mg/m2) was given over a 3-hour infusion, followed by carboplatin (AUC 5) in a 1-hour infusion on day 1. Capecitabine (850 mg/m2) was given orally twice a day from day 1 to day 14. All patients received a routine supportive treatment plan that included hydration with normal saline (at least 3 L/24 hours), dexamethasone, and 5-HT3 antagonists. Granulocyte colony stimulating factor (G-CSF) was not routinely given, although it was used as secondary prophylaxis and in subsequent courses if severe neutropenia or febrile neutropenia occurred.
Toxicity of the treatment regimen was evaluated based on the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0.26 The TCX regimen would be temporarily discontinued if one of the following toxicities occurred: hematological toxicity (grade 3 or higher), non-hematological toxicity (grade 4), serum creatinine >120 µmol/L, and clinical deterioration (ECOG PS >2). Chemotherapy was continued when the patient’s condition improved (ECOG PS ≤2) and the toxic effects reduced to grade 2 or less. The treatment would be terminated if the patient did not improve within 2 weeks of supportive therapy. The subsequent treatment plan was decided by the treating physician based on the patient’s condition.
Assessments
Per routine practice, patients were clinically examined at baseline, before each treatment cycle, and after the end of treatment. Evaluations included physical examination, medical history, physical examination, complete blood cell count, serum creatinine and urea, liver enzymes (AST/ALT), tumor markers (CEA [Carcinoembryonic antigen] and CA 72–4 [cancer antigen 72–4]), and computed tomography (CT). A comprehensive assessment was conducted before initiation of chemotherapy, then every 3 weeks, except for tumor markers and CT (at baseline and the end of cycles 3 and 6).
After the end of treatment, patients were followed up every 3 months for disease progression. Follow-up was conducted until 2 years since the beginning of treatment, death, or loss-to-follow-up, whichever came first. All the information has been recorded in detail in patient’s medical charts.
For patients who did not return for follow-up, we called the patients or their family to ask for their current status (ie, whether they were alive, whether their cancer had progressed, and the date of these events if they had occurred).
Study Outcomes
Progression-free survival (PFS) and overall survival (OS) were two primary endpoints in this study. PFS was defined as the time since the initiation of TCX regimen to the first documented disease progression or death, whichever came first. Disease progression was defined as (1) an increase in the sum of the longest diameter of target lesions of ≥20% or at least 5 mm, compared with that of the initiation of the treatment and/or (2) the progression of non-targeted lesions; and/or (3) the appearance of one or more new lesions. OS was defined as the time since the initiation of TCX regimen to death, administrative censoring, or the last date the patient was known to be alive (often in patients who were lost to follow-up).
Secondary outcomes included clinical improvement, tumor response, and safety. Clinical improvement was measured by the presence or absence of symptoms and signs at the end of the treatment course compared to baseline evaluation. The measured symptoms and signs included fatigue, abdominal pain, early satiety, anorexia, dysphagia, nausea, vomiting, weight loss, pyloric stenosis, and gastrointestinal bleeding. Tumor response was evaluated using the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, which takes into account the responses in target and non-target lesions, as well as the formation of new lesions, in comparison to the prior evaluation. The elimination of all target and non-target lesions, normalization of tumor marker levels, and the absence of new lesions were considered complete response. A partial response was defined as a decrease in the sum of the longest diameter of target lesions by at least 30% compared to baseline, the persistence of one or more non-target lesions without progression and/or the maintenance of tumor marker levels above normal limits, and absence of new lesions.
Safety of the regimen was evaluated by the presence of grade 3/4 adverse events (AEs) using the definitions of adverse events in CTCAE version 4.0. The monitored adverse events included nausea, fatigue, stomatitis, diarrhea, allergy, phlebitis, hand-foot syndrome, peripheral neuropathy, anemia (hemoglobin <8.0 g/dL or transfusion indicated), leukopenia (white cell count <2000/μL), thrombocytopenia (platelet count <50,000/mm3), transaminitis (AST/ALT >100 UI/L), and hypercreatinemia (serum creatinine >300 mmol/L).
Sample Size
Sample size was calculated based on OS among esophagogastric cancer patients treated with TCX in a previous study.23 Assuming a 2-year OS of 30%, a margin of error of 10%, and a confidence level of 95%, the minimum sample size was 81 patients. Accounting for 8% loss-to-follow-up, we planned to recruit 88 patients.
Statistical Analysis
Demographic and personal characteristics of the study participants were summarized by frequency and percentage for categorical variables, and median and IQR range for continuous variables.
Kaplan-Meier method was used to estimate the survival endpoints. We would report 6-month, 1-year, and 2-year PFS and OS. The Cox proportional-hazards regression model was used to determine factors associated with the survival outcomes. The candidates for the regression models were selected on the theoretical basis through literature review and clinical experience; factors that were not selected based on theory but associated with the outcomes of interest in the univariable analysis might also be included in the models.
For the clinical improvement endpoints, we compared the presence of symptoms and signs at baseline and after the end of treatment course using McNemar’s test for paired dichotomous data. For the safety endpoints, AEs (any grade and grade 3/4) were reported for each cycle. Some AEs that were determined by the blood test results, such as anemia and hypercreatinemia, were recorded as continuous data. For these variables, we also examined the changes over cycles by the spaghetti plot and fitting generalized estimating equations.
All analyses were performed using Stata/BE 17 (StataCorp LLC, College Station, TX, US). An analysis with P-values of <0.05 was considered statistically significant.
Ethical Consideration
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Hanoi Medical University under decision No. 05/06012017 dated January 06, 2017. Informed consent was obtained from the patients before participating in the study. The investigators were responsible for protecting the privacy and confidentiality of patients as per Vietnam’s regulations and Good Clinical Practice.
Results
Participant Characteristics
A total of 83 patients were recruited in this study. At baseline, 77.1% were categorized as ECOG PS 0–1. Major metastatic sites were liver and peritoneum. Histopathologic types included moderately differentiated adenocarcinoma (37.3%), low differentiated adenocarcinoma (34.9%), and squamous cell carcinoma (27.7%) (Table 1).
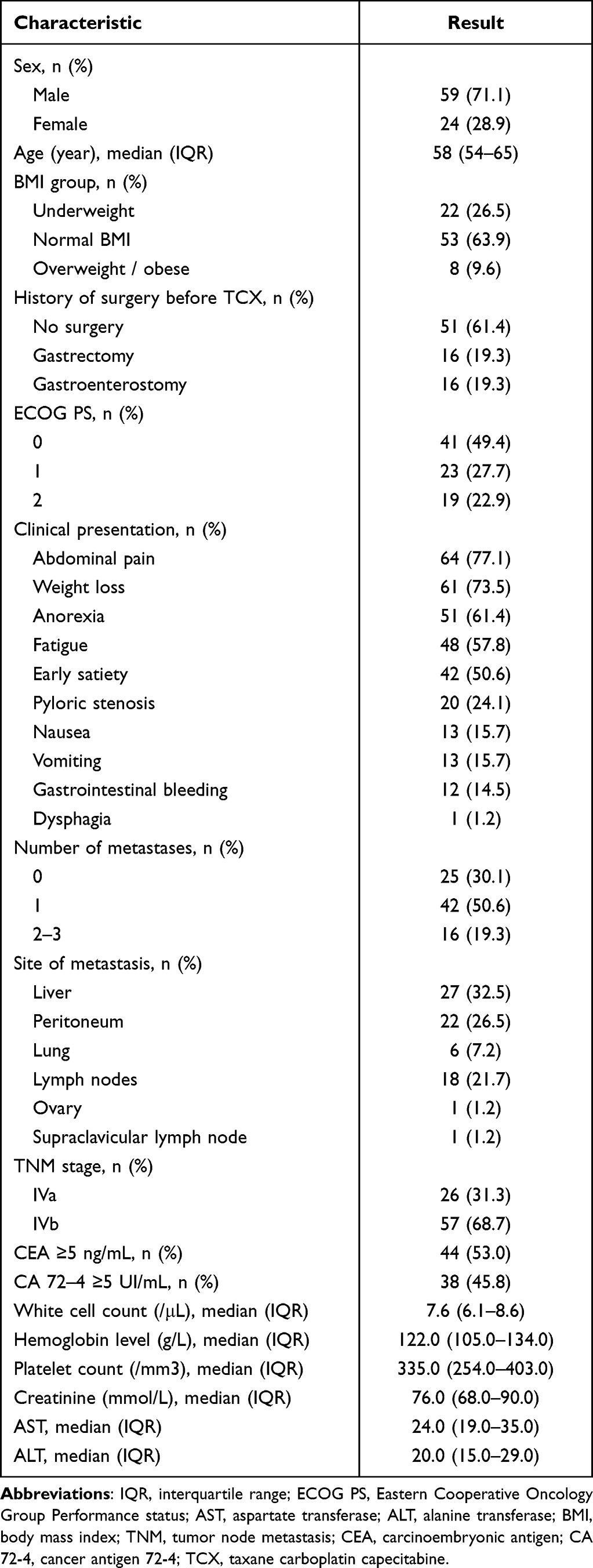 |
Table 1 Baseline Characteristics (n = 83) |
Survival
Median PFS was 9.3 months; 6-month, 1-year, and 2-year PFS were 74.6%, 32.5%, and 14.4%, respectively. Median OS was 17.0 months; 6-month, 1-year, and 2-year OS were 97.5%, 68.7%, and 21.7%, respectively (Figure 2). The median OS and PFS was significantly longer in patients with CEA <5ng/mL group compared to those with CEA ≥5ng/mL (OS: 20.5 months vs 12.9 months; log-rank p = 0.014; PFS: 11.8 months vs 8.0 months, log-rank p = 0.02) (Figure 3).
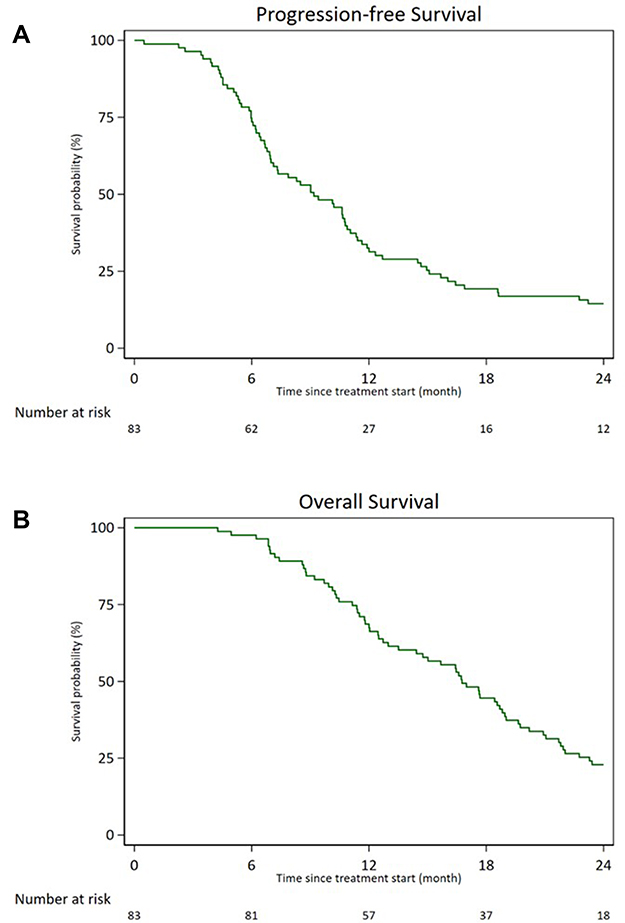 |
Figure 2 Kaplan-Meier estimates of (A) progression-free survival and (B) overall survival among the study participants (n = 83). |
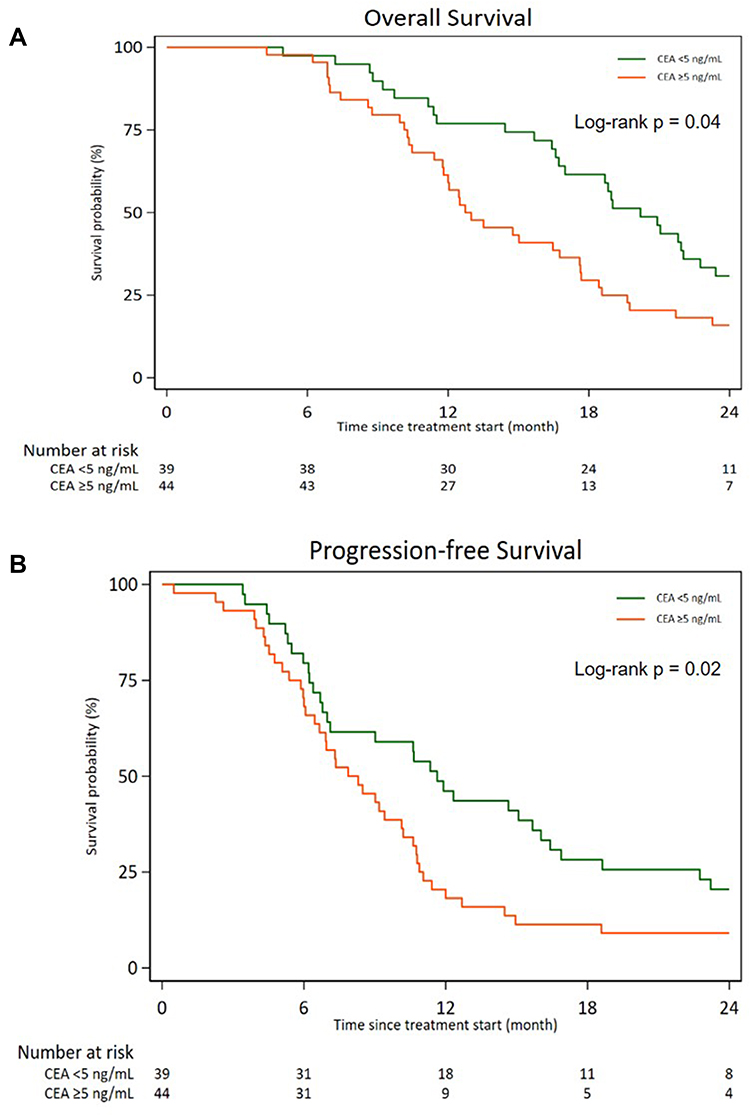 |
Figure 3 Kaplan-Meier estimates of (A) progression-free survival and (B) overall survival among the study participants, stratified by CEA levels (n = 83). |
In the univariate analysis, factors associated with PFS included CEA (≥5ng/mL versus <5ng/mL; HR = 1.75; 95% CI: 1.08–2.82), metastatic status (M1 versus M0; HR = 1.77; 95% CI: 1.05–2.97), TNM stage (IVb versus IVa; HR = 1.82; 95% CI: 1.07–3.10), and liver metastasis (HR = 1.78; 95% CI: 1.09–2.89), but none of these was significant in the multivariable Cox model (Table 2). For OS, CEA (≥5ng/mL versus <5ng/mL; HR = 1.86; 95% CI: 1.12–3.07) were found to be associated in the univariable analysis and remained significant in the Cox model (HR = 1.89; 95% CI: 1.13–3.17).
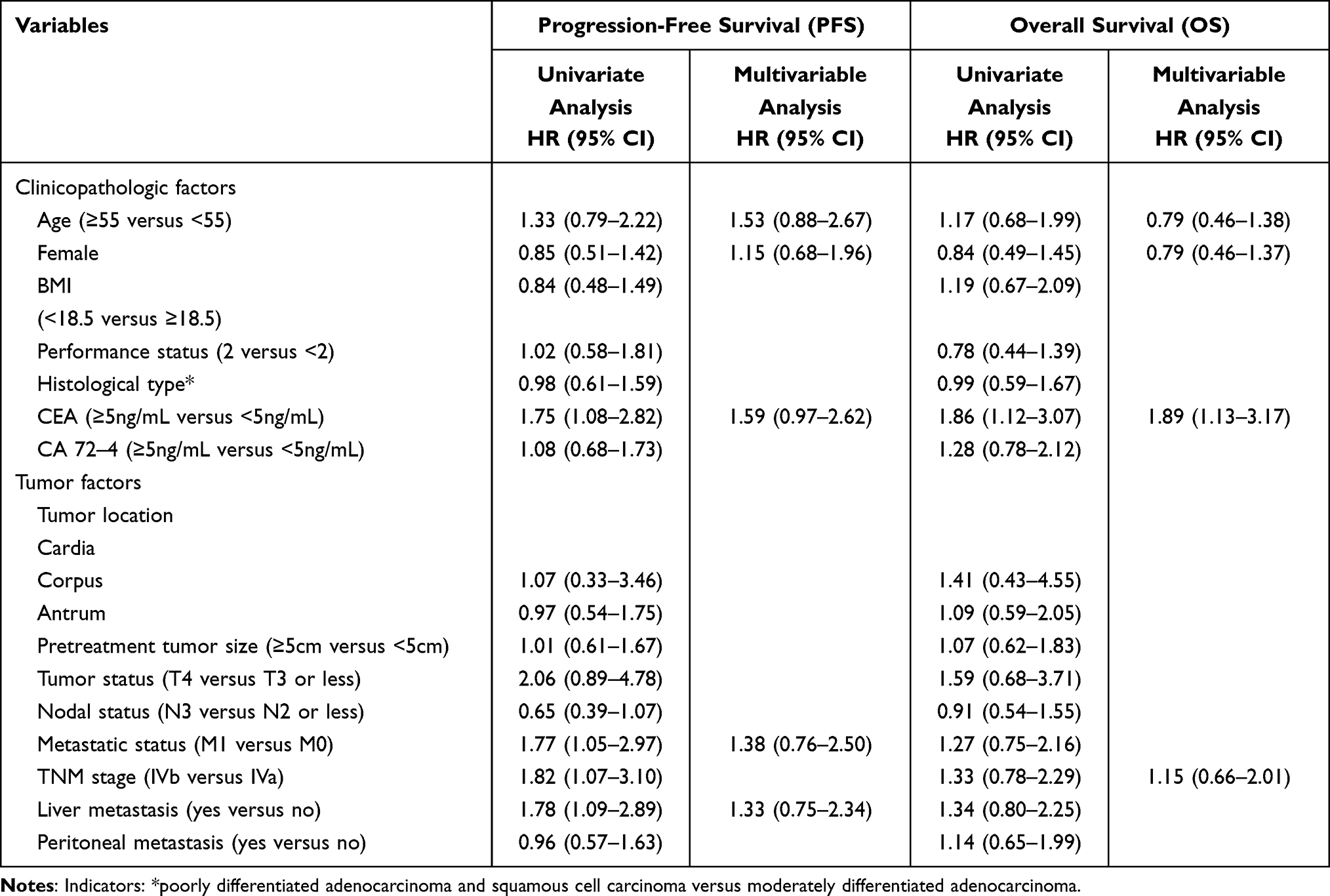 |
Table 2 Univariate and Multivariable Analysis of Factors Associated with Progression-Free Survival and Overall Survival Among the Study Participants (n = 83) |
Tumor Response and Clinical Improvement
A total of 466 TCX cycles were administered, and 70 out of 83 patients completed 6 cycles. Thirty-one patients (37.3%) had a partial response, and only four patients (4.8%) had a complete response. Eighteen patients (21.7%) had stable disease, while 30 patients (36.1%) had progressive disease (Table 3).
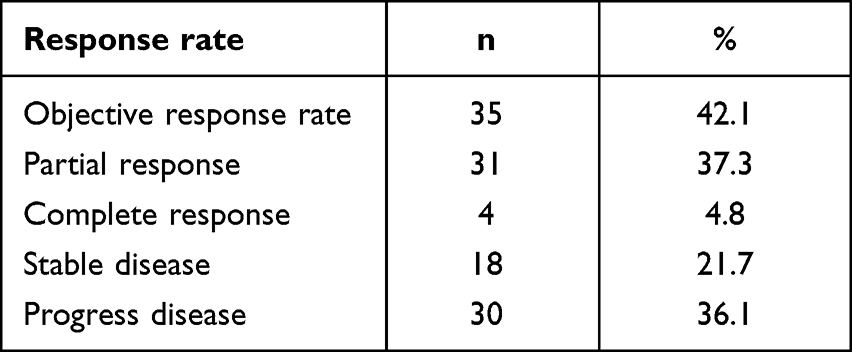 |
Table 3 Tumor Response Rate Among the Study Participants (n = 83) |
The prevalence of most of the signs and symptoms (including fatigue, abdominal pain, early satiety, poor eating, lose weight, pyloric stenosis and gastrointestinal bleeding) were reduced after the treatment course (Table 4). Fifteen patients were candidates for curative surgery after TCX chemotherapy, in which three patients refused to participate in the procedure and were treated with second-line chemotherapy. Twelve patients underwent curative surgery (gastrectomy with lymph node dissection) and for all these patients, R0 resection was achieved; and no viable tumors were detected in resected lymph nodes (ypN0).
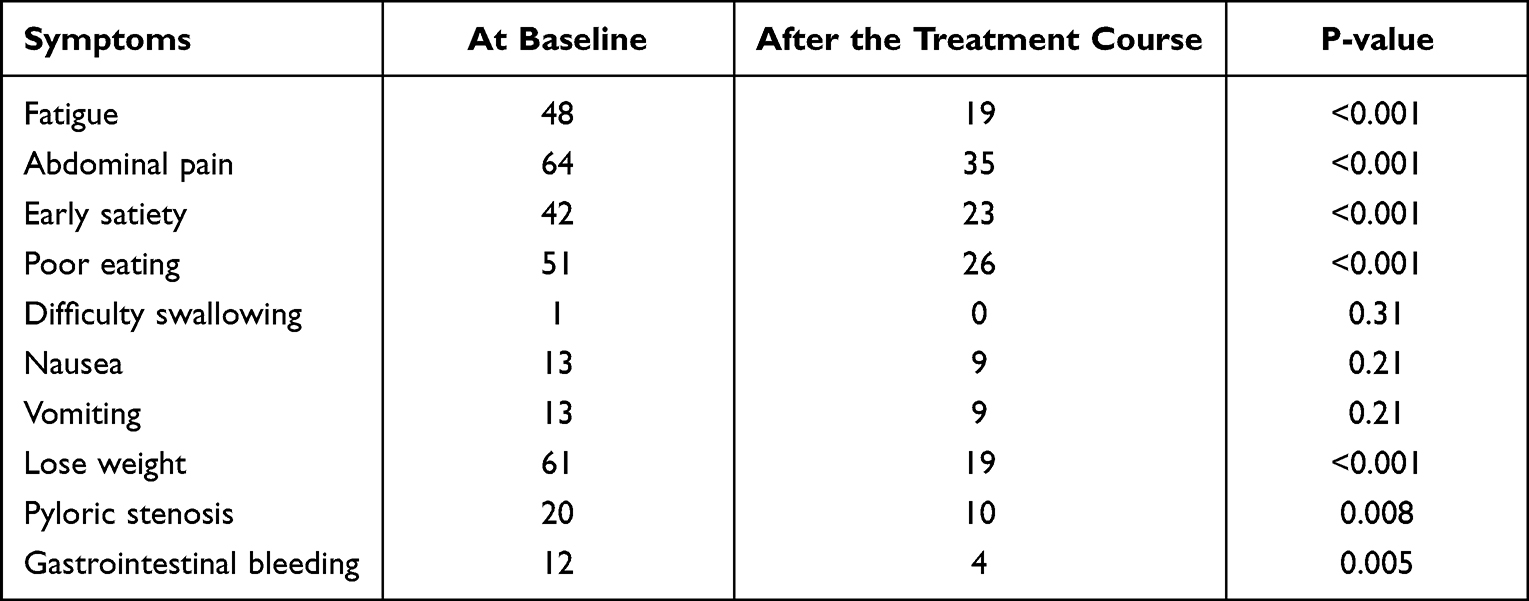 |
Table 4 Clinical Improvement Among the Study Participants (n = 83) |
Toxicity
The most common non-hematological toxicity was hand-foot syndrome (HFS) (77.9%), peripheral neuropathy (63.2%), fatigue (68.7%), and nausea (54.2%). Grade 3–4 fatigue was observed in only one patient. Although 27.1% suffered from grade 3–4 neutropenia, there was no patient experienced febrile neutropenia. Grade 3–4 anemia and thrombocytopenia only occurred in 2 (2.4%) and 1 (1.2%) patients, respectively (Table 5). No treatment-related deaths were observed during the course of treatment. Patients had two hospital admissions (median), and most were admitted for only 1 day. The major cause of hospital admissions was severe neutropenia, in which patients received G-CSF as a subsequent course (Table 6). A total of 10 treatment-related serious adverse effects (SAE) were observed in the study, resulting in hospitalization/prolonged hospital stay. Of these, three patients had elevated AST/ALT which required administration of reamberin or glutathione, six had both severe anemia and neutropenia which required blood transfusion and G-CSF, and one had severe anemia which required blood transfusion.
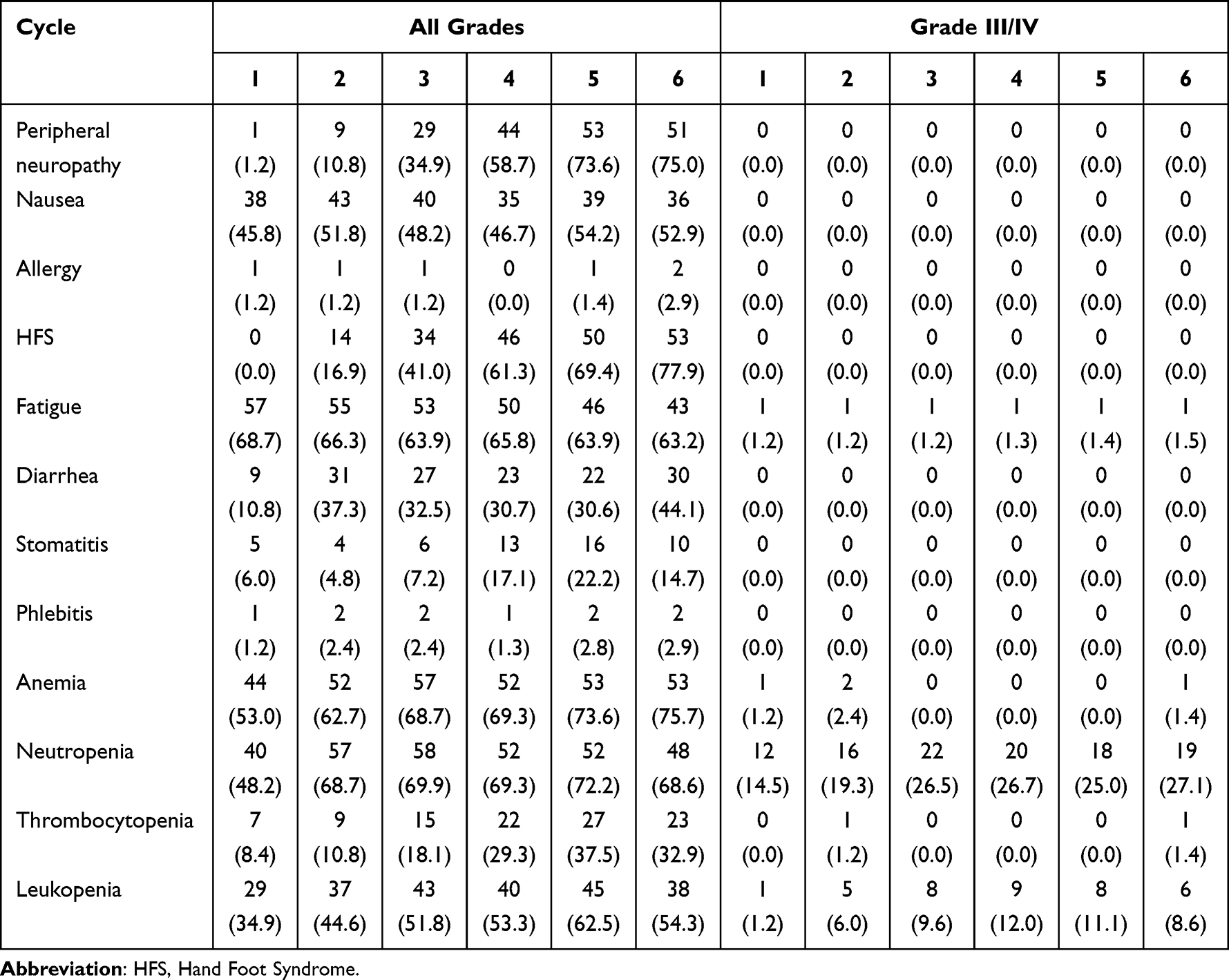 |
Table 5 Hematologic and Nonhematologic Toxicities (n = 83) |
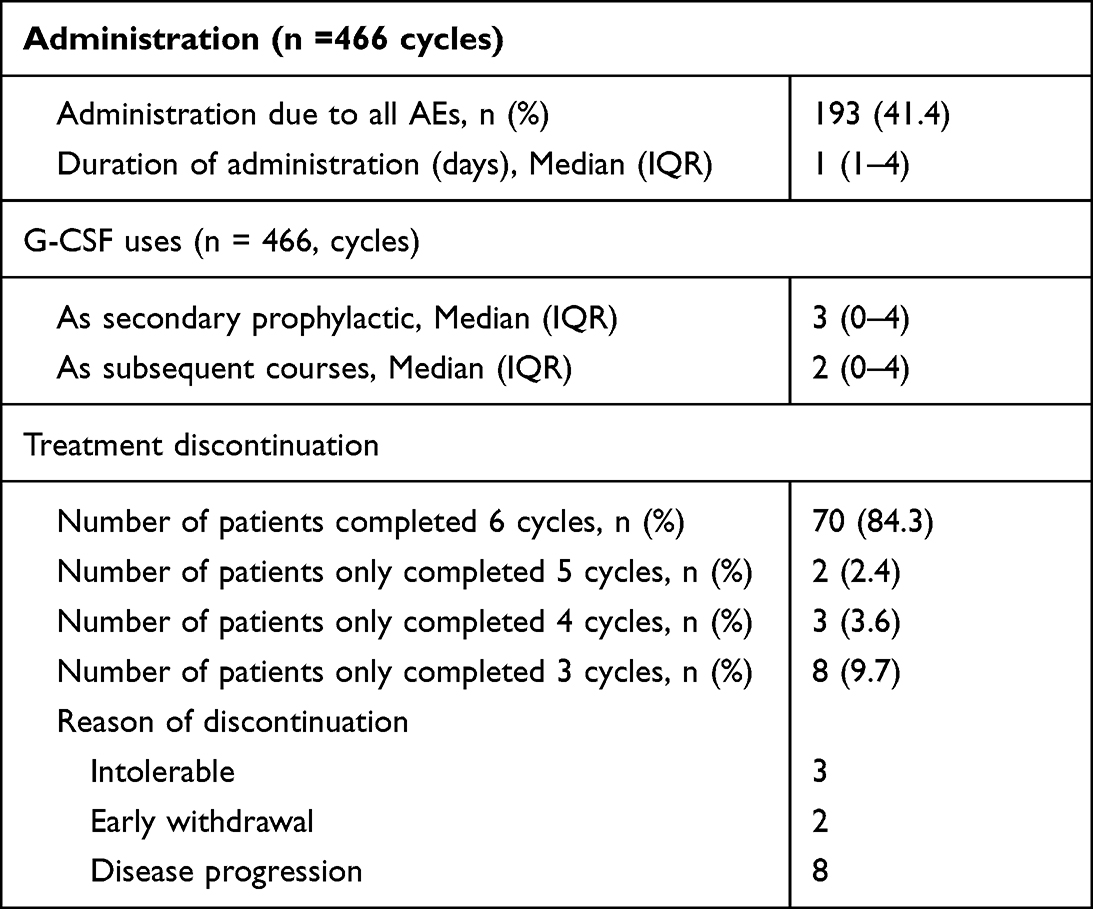 |
Table 6 Administration Due to AEs, G-CSF Uses and Treatment Discontinuation |
Discussion
In this study, we examined the treatment outcome and safety of the TCX regimen on patients with advanced gastric cancer. We found that the median PFS and OS were 9.3 months and 17.0 months, respectively, and the objective response rate (ORR) was 42.1%. The TCX regimen was relatively safe and tolerable, with the incidence of grade 3–4 neutropenia was 27.1% and the completion of 6 cycles in majority of the patients.
The survival outcomes in our study appear to be higher than that of other doublet and triplet chemotherapy regimens. For first-line doublet regimens, PFS did not exceed 6 months (3.7–6.0 months) and OS did not exceed 1 year (8.6–10.5 months).12,27,28 For triplet regimens, survival was longer (PFS 5.0–7.4 months and OS 8.9–11.2 months) but still lower than in our study.12,29–32 Among these, docetaxel-containing three-drug regimens increased response rates; however, the benefits of docetaxel-containing three-drug combinations (DCF and FLOT) were outweighed by their toxicity.5 Due to concerns about toxicity, the National Comprehensive Cancer Network has recently removed the DCF regimen from the recommendation for first-line treatment for metastatic or locally advanced cancer, and suggested that dose-modified or other DCF modifications should be utilized as an alternative.33 Based on this point, TCX was used in this study with the expectation to retain the same effectiveness while reducing the toxicity and increasing the tolerability of the regimen, thus, could be more suitable for the physical condition of patients with advanced gastric cancer. Although studies have yet to confirm the superiority of paclitaxel over docetaxel, there was evidence that suggests the difference in toxicity between these two, in monotherapy as well as combined regimens. Specifically, a 2006 study in South Korea showed that the PF (paclitaxel and 5-fluorouracil) regimen had fewer serious adverse effects than that of the DF (docetaxel and 5-fluorouracil) regimen.17 In another study, neutropenia was more common in the DFL (docetaxel, 5-fluorouracil and leucovorin) regimen than that of the PFL regimen (paclitaxel, 5-fluorouracil and leucovorin) (71% versus 62%).18 A Phase III clinical trial in 449 patients with metastatic breast cancer demonstrated a higher incidence of hematological and non-hematological toxicity in the docetaxel group compared to paclitaxel.16 Despite its limited efficacy in esophageal and gastric cancer, with the single agent response rate of 5–10%,34–36 carboplatin was associated with less severe nausea/vomiting and thus might improve tolerability and adherence. Thus, the use of carboplatin in the combination of docetaxel, carboplatin and fluorouracil was recommended as category 2B in the recent NCCN guidelines.33 The introduction of oral capecitabine into the treatment regimen to replace the continuous infusion of 5-FU has demonstrated clinical benefits. The Real-2 multicenter clinical trial found that 5-FU infusion and capecitabine had similar effectiveness.29 This substitution not only reduced the hematological toxicity as previously reported,27,37,38 but also eliminated the requirement for hospitalization, as a central venous access device was no longer required. As expected, the ORR in our study were comparable to those of the DCF and its modification regimens (42.1% vs 25%–48.7%)9,14,39–42 while the toxicity profile was more favorable.
In our study, higher CEA was associated with poor OS and PFS. As a membrane protein, CEA was associated with cell–cell adhesion and junction.43 CEA has sialofucosylated glycoforms that act as selectin ligands and aid the metastasis of colon cancer cells.44–47 In a retrospective cohort study that included 1596 gastric cancer patients, CEA was associated with chemokine signaling and immunology regulation, especially T cells and Th cells,48 which have previously been shown to have a role in mediating cancer metastasis process.49–51 Because CEA is involved in tumor metastasis, it may be linked to the prognosis of gastric cancer. In a meta-analysis that included 14,651 patients, increased pretreatment serum CEA levels nearly doubled the risk of mortality in patients with gastric cancer.52 In a study on 615 Chinese patients with advanced gastric cancer, a CEA level of ≥8 ng/mL was associated with higher death risk compared to that of <8 ng/mL, and therefore, CEA has been incorporated into a prognostic scoring model for mortality risk stratification.53 However, because other studies have indicated otherwise,54–58 CEA is not considered an independent predictor for patients with gastric cancer, and curative approach should not be tailored based on CEA level.25 However, the difference in mortality among levels of CEA should be considered by treating physicians, as patients could benefit from more intensive regimens (such as docetaxel-containing triplet regimen).
Our study reported a better safety profile of the TCX regimen. No patient died from treatment-related events. Non-hematologic and hematologic toxicities, albeit frequent, were mild and required neither intervention nor treatment discontinuation. Anemia is a common adverse effect in gastric cancer patients on chemotherapy. In addition to the adverse effect caused by the chemotherapy itself, anemia can also be aggravated by many factors such as gastrointestinal bleeding before admission, malnutrition, and vitamin B12 deficiency.59 Only 27.1% of our patients had severe neutropenia (grade 3–4 AE), and no patient experienced febrile neutropenia. This incidence was much lower than that of a study on CF/DCF regimens (57% in patients treated with CF and 82% in DCF). Also, in this study, the incidence of febrile neutropenia was 29% and 12% in the DCF and CF arms, respectively, and treatment-related infections were the main cause of death in both arms.12 A meta-analysis that included 482 randomized participants in three studies have reported the rate of treatment‐related deaths (6.2%) and treatment discontinuation due to toxicity (17%) in patients treated with taxane‐platinum‐fluoropyrimidine combinations.5 DCX (docetaxel, cisplatin and capecitabine), a modified regimen of DCF, had varied incidence of severe neutropenia and febrile neutropenia across studies (16–62% for severe neutropenia and 4.5–19% for febrile neutropenia).37,38,60 Substituting docetaxel with paclitaxel, as well as the introduction of oral capecitabine as an alternative to intravenous 5-FU, may play a role in alleviating hematological toxicity, as shown in previous studies.16–18,37,38,60
To our knowledge, this is the first prospective cohort study evaluating the efficacy and toxicity of TCX regimen in patients with advanced stage cancer. The relatively small sample size, short follow-up period, and lack of a control group were the main disadvantages of this study. The results of our study need validating by prospective, randomized controlled clinical trials comparing TCX and other chemotherapy regimens in the treatment of advanced gastric cancer with a large number of participants.
Conclusions
The TCX regimen provided good survival and a better safety profile. Clinical trials are needed to confirm its treatment efficacy and safety, especially in comparison with other triplet regimens.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pham T, Bui L, Kim G, Hoang D, Tran T, Hoang M. Cancers in Vietnam – burden and control efforts: a narrative scoping review. Cancer Control. 2019;26(1):1073274819863802. doi:10.1177/1073274819863802
2. Van Thuan T, Anh PT, Van Tu D. Cancer control in Vietnam: where are we? Cancer Control. 2016;99. Available from http://www.cancercontrol.info/cc2016/cancer-control-in-vietnam-where-we-are/.
3. Nakajima T, Nishi M. Surgery and adjuvant chemotherapy for gastric cancer. Hepatogastroenterology. 1989;36(2):79–85.
4. Jung JJ, Cho JH, Shin S, Shim YM. Surgical treatment of anastomotic recurrence after gastrectomy for gastric cancer. Korean J Thorac Cardiovasc Surg. 2014;47(3):269–274. doi:10.5090/kjtcs.2014.47.3.269
5. Wagner AD, Syn NL, Moehler M, et al. Chemotherapy for advanced gastric cancer. Cochrane Database Syst Rev. 2017;8:CD004064. doi:10.1002/14651858.CD004064.pub4
6. Li B, Chen L, Luo HL, Yi FM, Wei YP, Zhang WX. Docetaxel, cisplatin, and 5-fluorouracil compared with epirubicin, cisplatin, and 5-fluorouracil regimen for advanced gastric cancer: a systematic review and meta-analysis. World J Clin Cases. 2019;7(5):600–615. doi:10.12998/wjcc.v7.i5.600
7. Kilickap S, Yalcin S, Ates O, Tekuzman G. The first line systemic chemotherapy in metastatic gastric carcinoma: a comparison of docetaxel, cisplatin and fluorouracil (DCF) versus cisplatin and fluorouracil (CF); versus epirubicin, cisplatin and fluorouracil (ECF) regimens in clinical setting. Hepatogastroenterology. 2011;58(105):208–212.
8. Babu KG, Chaudhuri T, Lakshmaiah KC, et al. Efficacy and safety of first-line systemic chemotherapy with epirubicin, cisplatin plus 5-fluorouracil and docetaxel, cisplatin plus 5-fluorouracil regimens in locally advanced inoperable or metastatic gastric or gastroesophageal junction adenocarcinoma: a prospective Phase II study from South India. Indian J Cancer. 2017;54(1):47–51. doi:10.4103/ijc.IJC_168_17
9. Roth AD, Fazio N, Stupp R, et al. Docetaxel, cisplatin, and fluorouracil; docetaxel and cisplatin; and epirubicin, cisplatin, and fluorouracil as systemic treatment for advanced gastric carcinoma: a randomized phase II trial of the Swiss Group for Clinical Cancer Research. J Clin Oncol. 2007;25(22):3217–3223. doi:10.1200/JCO.2006.08.0135
10. Teker F, Yilmaz B, Kemal Y, Kut E, Yucel I. Efficacy and safety of docetaxel or epirubicin, combined with cisplatin and fluorouracil (DCF and ECF), regimens as first line chemotherapy for advanced gastric cancer: a retrospective analysis from Turkey. Asian Pac J Cancer Prev. 2014;15(16):6727–6732. doi:10.7314/APJCP.2014.15.16.6727
11. Shah MA, Janjigian YY, Stoller R, et al. Randomized multicenter phase II study of modified docetaxel, cisplatin, and fluorouracil (DCF) versus DCF plus growth factor support in patients with metastatic gastric adenocarcinoma: a study of the US gastric cancer consortium. J Clin Oncol. 2015;33(33):3874–3879. doi:10.1200/JCO.2015.60.7465
12. Van Cutsem E, Moiseyenko VM, Tjulandin S, et al. Phase III study of docetaxel and cisplatin plus fluorouracil compared with cisplatin and fluorouracil as first-line therapy for advanced gastric cancer: a report of the V325 study group. J Clin Oncol. 2006;24(31):4991–4997. doi:10.1200/JCO.2006.06.8429
13. Chen XL, Chen XZ, Yang C, et al. Docetaxel, cisplatin and fluorouracil (DCF) regimen compared with non-taxane-containing palliative chemotherapy for gastric carcinoma: a systematic review and meta-analysis. PLoS One. 2013;8(4):e60320. doi:10.1371/journal.pone.0060320
14. Wang J, Xu R, Li J, et al. Randomized multicenter phase III study of a modified docetaxel and cisplatin plus fluorouracil regimen compared with cisplatin and fluorouracil as first-line therapy for advanced or locally recurrent gastric cancer. Gastric Cancer. 2016;19(1):234–244. doi:10.1007/s10120-015-0457-4
15. Tebbutt NC, Cummins MM, Sourjina T, et al. Randomised, non-comparative phase II study of weekly docetaxel with cisplatin and 5-fluorouracil or with capecitabine in oesophagogastric cancer: the AGITG ATTAX trial. Br J Cancer. 2010;102(3):475–481. doi:10.1038/sj.bjc.6605522
16. Jones SE, Erban J, Overmoyer B, et al. Randomized phase III study of docetaxel compared with paclitaxel in metastatic breast cancer. JCO. 2005;23(24):5542–5551. doi:10.1200/JCO.2005.02.027
17. Park SH, Lee WK, Chung M, et al. Paclitaxel versus docetaxel for advanced gastric cancer: a randomized phase II trial in combination with infusional 5-fluorouracil. Anticancer Drugs. 2006;17(2):225–229. doi:10.1097/00001813-200602000-00015
18. Chon HJ, Rha SY, Im CK, et al. Docetaxel versus paclitaxel combined with 5-FU and leucovorin in advanced gastric cancer: combined analysis of two phase II trials. Cancer Res Treat. 2009;41(4):196–204. doi:10.4143/crt.2009.41.4.196
19. Jiang J, Liang X, Zhou X, Huang R, Chu Z. A meta-analysis of randomized controlled trials comparing carboplatin-based to cisplatin-based chemotherapy in advanced non-small cell lung cancer. Lung Cancer. 2007;57(3):348–358. doi:10.1016/j.lungcan.2007.03.014
20. du Bois A, Lück HJ, Meier W, et al. A randomized clinical trial of cisplatin/paclitaxel versus carboplatin/paclitaxel as first-line treatment of ovarian cancer. J Natl Cancer Inst. 2003;95(17):1320–1329. doi:10.1093/jnci/djg036
21. Ozols RF, Bundy BN, Greer BE, et al. Phase III trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel in patients with optimally resected stage III ovarian cancer: a gynecologic oncology group study. J Clin Oncol. 2003;21(17):3194–3200. doi:10.1200/JCO.2003.02.153
22. Chintala L, Vaka S, Baranda J, Williamson SK. Capecitabine versus 5-fluorouracil in colorectal cancer: where are we now? Oncol Rev. 2011;5(2):129–140. doi:10.4081/oncol.2011.129
23. Ruoff CA, Hong B, Kaplan BH, Pollack S. Single-center experience with paclitaxel (T), carboplatin (C), and capecitabine (X) in the treatment of advanced esophagogastric cancer. JCO. 2013;31(4_suppl):116. doi:10.1200/jco.2013.31.4_suppl.116
24. Hosein PJ, Ray N, Anthony LB, et al. Paclitaxel, carboplatin, and capecitabine (TCX) with and without radiation in locally advanced and metastatic distal esophageal and esophagogastric junction cancer: a single-center retrospective review. JCO. 2015;33(3_suppl):197. doi:10.1200/jco.2015.33.3_suppl.197
25. Common Terminology Criteria for Adverse Events (CTCAE). 2009:79.
26. Kang YK, Kang WK, Shin DB, et al. Capecitabine/cisplatin versus 5-fluorouracil/cisplatin as first-line therapy in patients with advanced gastric cancer: a randomised phase III noninferiority trial. Ann Oncol. 2009;20(4):666–673. doi:10.1093/annonc/mdn717
27. Seo BG, Oh SY, Lee DM, et al. A phase II study of paclitaxel and cisplatin as salvage therapy for patients with advanced or metastatic gastric cancer. Cancer Res Treat. 2007;39(1):6–9. doi:10.4143/crt.2007.39.1.6
28. Cunningham D, Starling N, Rao S, et al. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N Engl J Med. 2008;358(1):36–46. doi:10.1056/NEJMoa073149
29. Webb A, Cunningham D, Scarffe JH, et al. Randomized trial comparing epirubicin, cisplatin, and fluorouracil versus fluorouracil, doxorubicin, and methotrexate in advanced esophagogastric cancer. J Clin Oncol. 1997;15(1):261–267. doi:10.1200/JCO.1997.15.1.261
30. Al-Batran SE, Hartmann JT, Probst S, et al. Phase III trial in metastatic gastroesophageal adenocarcinoma with fluorouracil, leucovorin plus either oxaliplatin or cisplatin: a study of the Arbeitsgemeinschaft Internistische Onkologie. J Clin Oncol. 2008;26(9):1435–1442. doi:10.1200/JCO.2007.13.9378
31. Dank M, Zaluski J, Barone C, et al. Randomized phase III study comparing irinotecan combined with 5-fluorouracil and folinic acid to cisplatin combined with 5-fluorouracil in chemotherapy naive patients with advanced adenocarcinoma of the stomach or esophagogastric junction. Ann Oncol. 2008;19(8):1450–1457. doi:10.1093/annonc/mdn166
32. Ajani JA, D’Amico TA, Bentrem DJ, et al. Gastric cancer, version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20(2):167–192.
33. Sternberg C, Kelsen D, Dukeman M, Leichman L, Carboplatin: HR. A new platinum analog in the treatment of epidermoid carcinoma of the esophagus. Cancer Treat Rep. 1985;69(11):1305–1307.
34. Queisser W, Preusser P, Mross KB, et al. Phase II evaluation of carboplatin in advanced esophageal carcinoma. A trial of phase I/II study group of the Association for Medical. Oncology of the German Cancer Society. Oncol Res Treat. 1990;13:190–193.
35. Mannell A, Winters Z. Carboplatin in the treatment of esophageal cancer. S Afr Med J. 1989;76(5):213–214.
36. Polyzos A, Felekouras E, Karatzas T, et al. Modified docetaxel-cisplatin in combination with capecitabine as first-line treatment in metastatic gastric cancer: a phase II study. Anticancer Res. 2012;32(9):4151–4156.
37. Bilici A, Selcukbiricik F, Demir N, Oven Ustaalioglu BB, Dikilitas M, Yildiz O. Modified docetaxel and cisplatin in combination with capecitabine (DCX) as a first-line treatment in HER2-negative advanced gastric cancer. Asian Pac J Cancer Prev. 2014;15(20):8661–8666. doi:10.7314/APJCP.2014.15.20.8661
38. Dong L, Li J, Lou XP, et al. Comparison of short-term efficacy and safety of TIROX and DCF regimens for advanced gastric cancer. J Int Med Res. 2014;42(3):737–743. doi:10.1177/0300060513510657
39. Sadighi S, Mohagheghi MA, Montazeri A, Sadighi Z. Quality of life in patients with advanced gastric cancer: a randomized trial comparing docetaxel, cisplatin, 5-FU (TCF) with epirubicin, cisplatin, 5-FU (ECF). BMC Cancer. 2006;6(1):274. doi:10.1186/1471-2407-6-274
40. Thuss-Patience PC, Kretzschmar A, Repp M, et al. Docetaxel and continuous-infusion fluorouracil versus epirubicin, cisplatin, and fluorouracil for advanced gastric adenocarcinoma: a randomized phase II study. J Clin Oncol. 2005;23(3):494–501. doi:10.1200/JCO.2005.02.163
41. Ajani JA, Moiseyenko VM, Tjulandin S, et al. Clinical benefit with docetaxel plus fluorouracil and cisplatin compared with cisplatin and fluorouracil in a phase III trial of advanced gastric or gastroesophageal cancer adenocarcinoma: the V-325 study group. J Clin Oncol. 2007;25(22):3205–3209. doi:10.1200/JCO.2006.10.4968
42. Beauchemin N, Arabzadeh A. Carcinoembryonic antigen-related cell adhesion molecules (CEACAMs) in cancer progression and metastasis. Cancer Metastasis Rev. 2013;32(3–4):643–671. doi:10.1007/s10555-013-9444-6
43. Thomas SN, Zhu F, Schnaar RL, Alves CS, Konstantopoulos K. Carcinoembryonic antigen and CD44 variant isoforms cooperate to mediate colon carcinoma cell adhesion to E- and L-selectin in shear flow. J Biol Chem. 2008;283(23):15647–15655. doi:10.1074/jbc.M800543200
44. Konstantopoulos K, Thomas SN. Cancer cells in transit: the vascular interactions of tumor cells. Annu Rev Biomed Eng. 2009;11(1):177–202. doi:10.1146/annurev-bioeng-061008-124949
45. Thomas SN, Tong Z, Stebe KJ, Konstantopoulos K. Identification, characterization and utilization of tumor cell selectin ligands in the design of colon cancer diagnostics. Biorheology. 2009;46(3):207–225. doi:10.3233/BIR-2009-0534
46. Benchimol S, Fuks A, Jothy S, Beauchemin N, Shirota K, Stanners CP. Carcinoembryonic antigen, a human tumor marker, functions as an intercellular adhesion molecule. Cell. 1989;57(2):327–334. doi:10.1016/0092-8674(89)90970-7
47. Cai Q, Zhou W, Li J, et al. Association of preoperative serum carcinoembryonic antigen and gastric cancer recurrence: a large cohort study. J Cancer. 2021;12(2):397–403. doi:10.7150/jca.47899
48. Thommen DS, Schumacher TNT. T Cell dysfunction in cancer. Cancer Cell. 2018;33(4):547–562. doi:10.1016/j.ccell.2018.03.012
49. Knochelmann HM, Dwyer CJ, Bailey SR, et al. When worlds collide: th17 and Treg cells in cancer and autoimmunity. Cell Mol Immunol. 2018;15(5):458–469. doi:10.1038/s41423-018-0004-4
50. Lambert AW, Pattabiraman DR, Weinberg RA. Emerging biological principles of metastasis. Cell. 2017;168(4):670–691. doi:10.1016/j.cell.2016.11.037
51. Deng K, Yang L, Hu B, Wu H, Zhu H, Tang C. The prognostic significance of pretreatment serum CEA levels in gastric cancer: a meta-analysis including 14651 patients. PLoS One. 2015;10(4):e0124151. doi:10.1371/journal.pone.0124151
52. Ma T, Wu Z, Zhang X, et al. Development and validation of a prognostic scoring model for mortality risk stratification in patients with recurrent or metastatic gastric carcinoma. BMC Cancer. 2021;21(1):1326. doi:10.1186/s12885-021-09079-7
53. Nakajima K, Ochiai T, Suzuki T, et al. Impact of preoperative serum carcinoembryonic antigen, CA 19-9 and alpha fetoprotein levels in gastric cancer patients. Tumour Biol. 1998;19(6):464–469. doi:10.1159/000030038
54. Ucar E, Semerci E, Ustun H, Yetim T, Huzmeli C, Gullu M. Prognostic value of preoperative CEA, CA 19-9, CA 72-4, and AFP levels in gastric cancer. Adv Ther. 2008;25(10):1075–1084. doi:10.1007/s12325-008-0100-4
55. Duraker N, Celik AN. The prognostic significance of preoperative serum CA 19-9 in patients with resectable gastric carcinoma: comparison with CEA. J Surg Oncol. 2001;76(4):266–271. doi:10.1002/jso.1044
56. Gaspar MJ, Arribas I, Coca MC, Díez-Alonso M. Prognostic value of carcinoembryonic antigen, CA 19-9 and CA 72-4 in gastric carcinoma. Tumour Biol. 2001;22(5):318–322. doi:10.1159/000050633
57. Ychou M, Duffour J, Kramar A, Gourgou S, Grenier J. Clinical significance and prognostic value of CA72-4 compared with CEA and CA19-9 in patients with gastric cancer. Dis Markers. 2000;16(3–4):105–110. doi:10.1155/2000/595492
58. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
59. Gilreath JA, Stenehjem DD, Rodgers GM. Diagnosis and treatment of cancer-related anemia: diagnosis and treatment of cancer-related anemia. Am J Hematol. 2014;89(2):203–212. doi:10.1002/ajh.23628
60. Kang YK, Ryu MH, Yoo C, et al. Phase I/II study of a combination of docetaxel, capecitabine, and cisplatin (DXP) as first-line chemotherapy in patients with advanced gastric cancer. Cancer Chemother Pharmacol. 2011;67(6):1435–1443. doi:10.1007/s00280-010-1444-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.