Back to Journals » Journal of Inflammation Research » Volume 18
Blood Cell Count-Based Inflammatory Markers Exhibit Superior Association with Diabetic Peripheral Neuropathy Compared to Protein-Based Markers
Authors Ko FS, Wu TH, Su GY, Lin YH, Juan CC, Hwu CM ![]()
Received 21 February 2025
Accepted for publication 19 July 2025
Published 7 August 2025 Volume 2025:18 Pages 10609—10617
DOI https://doi.org/10.2147/JIR.S524220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Fu-Shun Ko,1 Tsung-Hui Wu,1,2 Guan-Yu Su,1,2 Yi-Hsiu Lin,3 Chi-Chang Juan,3,4 Chii-Min Hwu1,2
1Section of Endocrinology and Metabolism, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 2Faculty of Medicine, National Yang Ming Chiao Tung University College of Medicine, Taipei, Taiwan; 3Institutes of Physiology, College of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan; 4Department of Medical Research, Taipei Veterans General Hospital, Taipei, Taiwan
Correspondence: Chii-Min Hwu, Section of Endocrinology and Metabolism, Department of Medicine, Taipei Veterans General Hospital, 201, ShiPai Road Sec. 2, Chung-Cheng Build. 11F Room 522, Taipei, 112, Taiwan, Tel +886 2 2875 7516, Fax +886 2 2875 1429, Email [email protected]
Background: Diabetic peripheral neuropathy (DPN) is a prevalent and disabling complication of type 2 diabetes mellitus, contributing to poor quality of life and increased healthcare burden. Chronic low-grade inflammation has been proposed as a key contributor to the pathogenesis of DPN. While various inflammatory markers have been studied, their diagnostic utility remains unclear, particularly when comparing protein-based markers and blood cell count-derived ratios.
Objective: This study aimed to investigate whether blood cell count-based inflammatory markers, such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), are more strongly associated with DPN compared to protein-based markers, including interleukin-1 receptor antagonist (IL-1Ra) and high-sensitivity C-reactive protein (hsCRP).
Methods: In this cross-sectional study, 137 patients with type 2 diabetes were recruited. DPN was defined as a Michigan Neuropathy Screening Instrument (MNSI) score ≥ 2. All participants underwent physical examinations, questionnaire assessments, and laboratory evaluation of inflammatory markers.
Results: NLR was significantly elevated in the DPN group compared to controls (P < 0.05), while IL-1Ra and hsCRP levels showed no significant differences. Participants in the highest NLR tertile exhibited a higher DPN prevalence (19.0%) than those in the lowest tertile (8.8%). Multivariate linear regression identified NLR and HbA1c as independent predictors of MNSI scores.
Conclusion: Our findings demonstrate that the NLR, an inflammation-related marker derived from peripheral blood cell counts, is significantly associated with DPN, whereas protein-based markers did not demonstrate clear associations. These findings suggest that NLR may serve as a simple, cost-effective biomarker for identifying patients at risk for DPN. Further longitudinal studies are warranted to clarify causal relationships and evaluate its prognostic value.
Keywords: type 2 diabetes mellitus, diabetic peripheral neuropathy, inflammatory response, IL-1 receptor antagonist
Introduction
Diabetic peripheral neuropathy (DPN) is widely recognized as one of the most prevalent complications of diabetes, with epidemiological data suggesting that it affects approximately one-third to one-half of individuals diagnosed with this condition.1 Individuals with DPN face a significantly elevated risk of injuries, foot ulcers, and lower limb amputations, thereby imposing a considerable burden on diabetes management and healthcare systems.2 A widely accepted hypothesis concerning the pathogenesis of DPN posits that oxidative stress and inflammatory processes, driven by metabolic dysregulation, play a pivotal role in nerve damage.3 Despite decades of research, no definitive biomarker for DPN has been identified, highlighting the intricate interplay of multiple pathogenic mechanisms underlying its development.
Emerging evidence indicates that subclinical inflammation plays a critical role in the pathogenesis of DPN, contributing to its progression through complex inflammatory pathways.4,5 The inflammatory mechanisms underlying DPN involve the activation of the NF-κB and MAPK/JNK signaling pathways, the release of pro-inflammatory cytokines and chemokines, and the recruitment of circulating immune cells.4,5 Based on this “inflammation hypothesis”, inflammatory biomarkers have recently been proposed as potential diagnostic tools for DPN.5
A broad range of inflammatory markers has been investigated in relation to DPN, including cytokines, chemokines, immune receptors, and blood cell-derived indices.6 At the systemic protein level, interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and high-sensitivity C-reactive protein (hsCRP) have been linked to DPN development, whereas interleukin-1 receptor antagonist (IL-1Ra) and soluble intercellular adhesion molecule-1 (sICAM-1) have been associated with DPN progression but previous study showed the natural aging process itself increased IL-6 and hsCRP levels.5–8 Additionally, blood cell-derived markers, such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), have demonstrated promising potential as diagnostic indicators.9,10 The broad spectrum of inflammatory biomarkers associated with DPN suggests the involvement of multiple pathogenic pathways. A direct comparison between protein-based and blood cell-based inflammatory markers may provide further insight into their respective contributions to DPN pathophysiology.
In this study, we aimed to investigate the associations between circulating inflammatory markers—including IL-1Ra, hsCRP, NLR, and PLR—and the presence of DPN in patients with type 2 diabetes. Through this analysis, we hope to identify a suitable biomarker for diagnosing DPN and gain further insight into its underlying mechanisms.
Methods
Subjects
In this study, we enrolled 137 ambulatory patients aged 50 years or older with a documented history of type 2 diabetes for more than 12 months from the diabetes clinic at Taipei Veterans General Hospital between January 2024 and December 2024. Patients were excluded if they had a diagnosis of type 1 diabetes, a history of alcohol abuse, known nerve damage of peripheral or central origin unrelated to diabetic neuropathy, or any medical condition deemed unsuitable for participation by the attending physician (including active infections, recent surgery and malignancy noted). The study protocol was approved by the hospital’s ethics committee, and written informed consent was obtained from all participants prior to enrollment. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Clinical Examination
Participants underwent anthropometric and blood pressure measurements at 8 AM following a 10- to 12-hour overnight fast. Body weight was measured to the nearest 0.1 kg, and height was recorded to the nearest millimeter. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m²). Seated blood pressure (BP) was measured using an automated BP monitor (HEM-7310, Omron Healthcare Inc., Kyoto, Japan). A structured questionnaire was administered by trained interviewers to collect demographic information and medical history. Following this, each participant underwent fasting blood sampling for the assessment of glucose, glycated hemoglobin (HbA1c), blood cell counts, and biochemical markers, including hsCRP and IL-1Ra levels.
Assessment of DPN
We used the Michigan Neuropathy Screening Instrument Physical Examination (MNSI-PE) protocol to evaluate DPN.11 This evaluation included an assessment of foot abnormalities (such as deformities, dry skin, calluses, infections, or fissures), the presence of foot ulceration, ankle reflexes, vibration perception using a tuning fork, and protective sensation testing with a 10-g monofilament. All neuropathic examinations were conducted by trained study nurses following a standardized operating procedure. DPN was diagnosed in patients with an MNSI-PE score of ≥2, as previously recommended in the literature,12 while those with scores below 2 were classified as controls.
Assays
Serum glucose and biochemical parameters were measured using commercial assay kits (Roche Diagnostics, Basel, Switzerland) in an automated blood chemistry analyzer (Roche-Hitachi 7180, Roche Diagnostics, Basel, Switzerland). Blood routine examinations primarily consists of complete blood counts (CBCs), which referred to the counts of the white blood cell (WBC), red blood cell (RBC), hemoglobin (Hb), platelet, neutrophil, monocyte, lymphocyte, eosinophil, and basophil. PLR and NLR were calculated using these counts. The estimated glomerular filtration rate (eGFR) was calculated using the simplified Modification of Diet in Renal Disease (MDRD) equation. Glycated hemoglobin (HbA1c) was analyzed using capillary electrophoresis. Serum IL-1Ra levels were determined by a solid-phase enzyme-linked immunosorbent assay (ELISA) (Quantikine, R&D Systems, Minneapolis, MN, USA), with a detection limit of 18.3 pg/mL. The intra-assay and inter-assay coefficients of variation (CVs) were 4.6% and 7.6%, respectively. High-sensitivity C-reactive protein (hsCRP) levels were measured using a turbidimetric method on an immunonephelometer (Beckman IMMAGE Nephelometer, Beckman Coulter, Fullerton, CA), with a measuring range of 0.15–1440 mg/L. Values below the detection limit were recorded as 0.14 mg/L. Blood cell counts were performed using an automated hematology analyzer (XN-3100, Sysmex, Kobe, Japan). All venous blood samples were drawn in the morning after an overnight fast and processed within one hour.
Statistical Analysis
Data are expressed as mean (standard deviation), median (range) or number (%). NLR is calculated by dividing the number of neutrophils by the number of lymphocytes. PLR is measured by dividing the platelet count by the lymphocytes. Logarithmic transformation was used to reduce skewness of a measurement variable. The study patients were divided into two groups by status of DPN initially. Between-group differences in clinical and biochemical characteristics were compared by using χ2 tests and two-sample t tests. Then, we divided the patients into three groups by tertiles of the biomarker levels. The prevalence of DPN among different tertile groups was tested by χ2 tests. Odds ratios and 95% confidence intervals of risk for DPN among the patients were estimated from binary logistic regression analyses using the group without DPN as the reference (odds ratio = 1). Age, sex, BMI, systolic and diastolic BP, fasting glucose, HbA1c level, Log ALT, eGFR and diabetes duration were all included in the logistic regression models for adjustments.
Additionally, univariate and multivariate linear regression analyses were conducted to examine the associations between MNSI-PE scores and clinical parameters in this cohort. In the multivariate linear regression model, the MNSI-PE score was used as the dependent variable, while variables of interest were included as independent variables to assess their relative contributions to MNSI-PE scores. To achieve this, all potential determinants that demonstrated a univariate association with MNSI-PE scores (P < 0.05) were simultaneously included in the multivariate regression model. Statistical analyses were performed using IBM SPSS Statistics software (Version 25.0, IBM Corp., Armonk, NY, USA). A P value < 0.05 was considered statistically significant.
Results
This study included 54 patients with type 2 diabetes and DPN and 83 patients without DPN. The descriptive characteristics of the study participants, stratified by DPN status, are presented in Table 1. Patients with DPN exhibited significantly higher body mass index (BMI), fasting glucose, and glycated hemoglobin (HbA1c) levels compared to those without DPN. However, the two groups were comparable in terms of age, blood pressure, diabetes duration, estimated glomerular filtration rate (eGFR), and alanine aminotransferase (ALT) levels. The median (range) values of neutrophil, lymphocyte, and platelet counts in the group without diabetic peripheral neuropathy (DPN) were 3.60 (4.79), 1.64 (5.63), and 227 (283) × 10³/μL, respectively, whereas in the group with DPN, the corresponding values were 4.08 (9.76), 1.50 (2.95), and 224 (412) × 10³/μL, respectively. A significant difference was observed in blood cell-derived inflammatory markers, with log-transformed NLR [Log (NLR)] being significantly higher in the DPN group (P = 0.001). In contrast, protein-based inflammatory markers, including IL-1Ra and hsCRP, did not differ significantly between the two groups (Table 2).
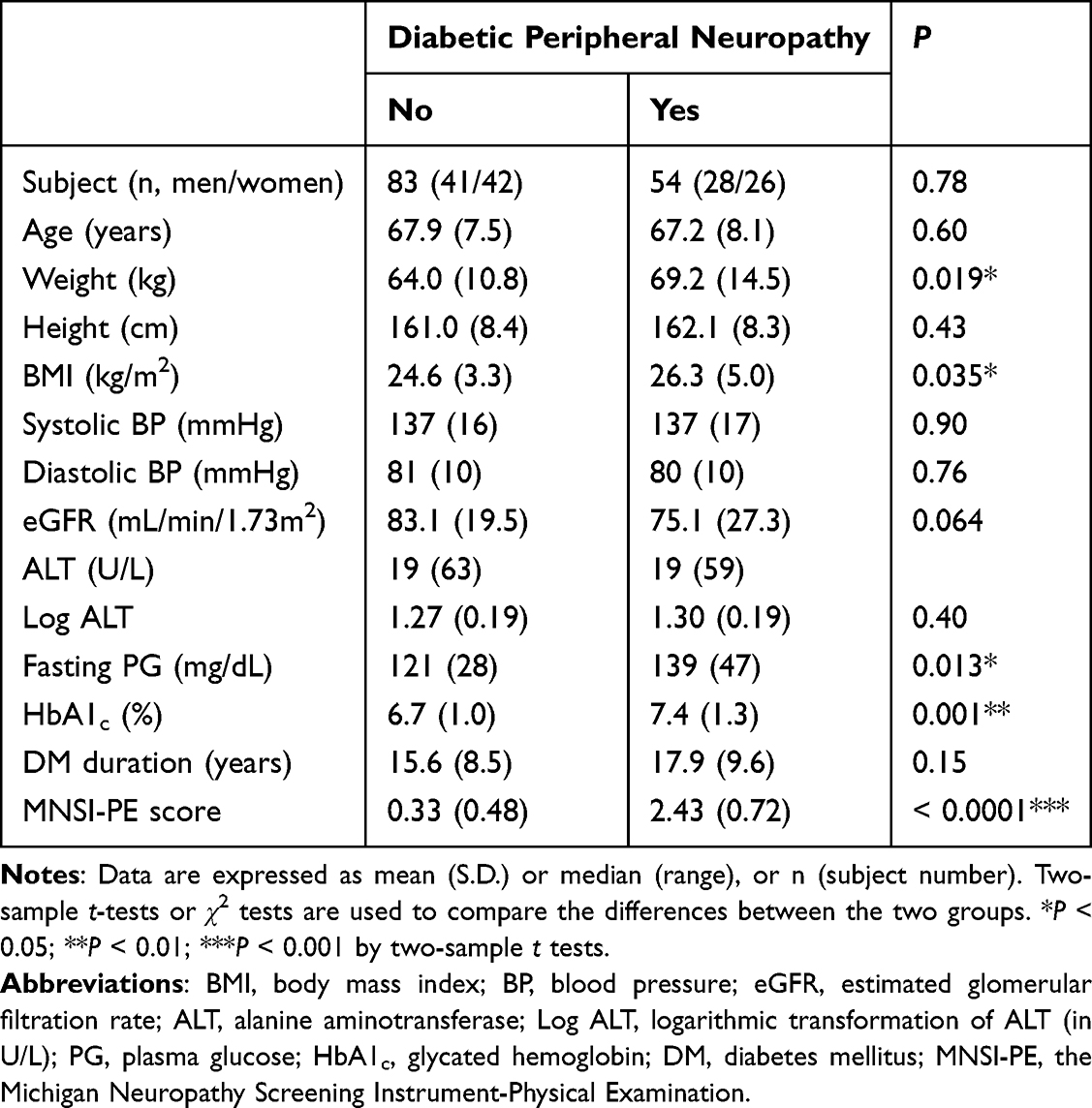 |
Table 1 Descriptive Characteristics of the Study Participants by Status of Diabetic Peripheral Neuropathy |
 |
Table 2 Markers of Inflammation in Type 2 Diabetes Patients with or Without Diabetic Peripheral Neuropathy |
The prevalence of DPN, stratified by tertiles of inflammatory markers, is presented in Figure 1. A significant difference in DPN prevalence was observed among patients with varying levels of NLR, as determined by χ²-tests. However, no significant differences were detected among the tertile groups for PLR, IL-1Ra and hsCRP. To further evaluate the association between inflammatory markers and DPN risk, logistic regression analyses were conducted. Patients with different levels of NLR exhibited significantly different risks of DPN, both before and after adjusting for potential confounders. In contrast, no significant association was found between PLR, IL-1Ra or hsCRP levels and DPN risk (Table 3).
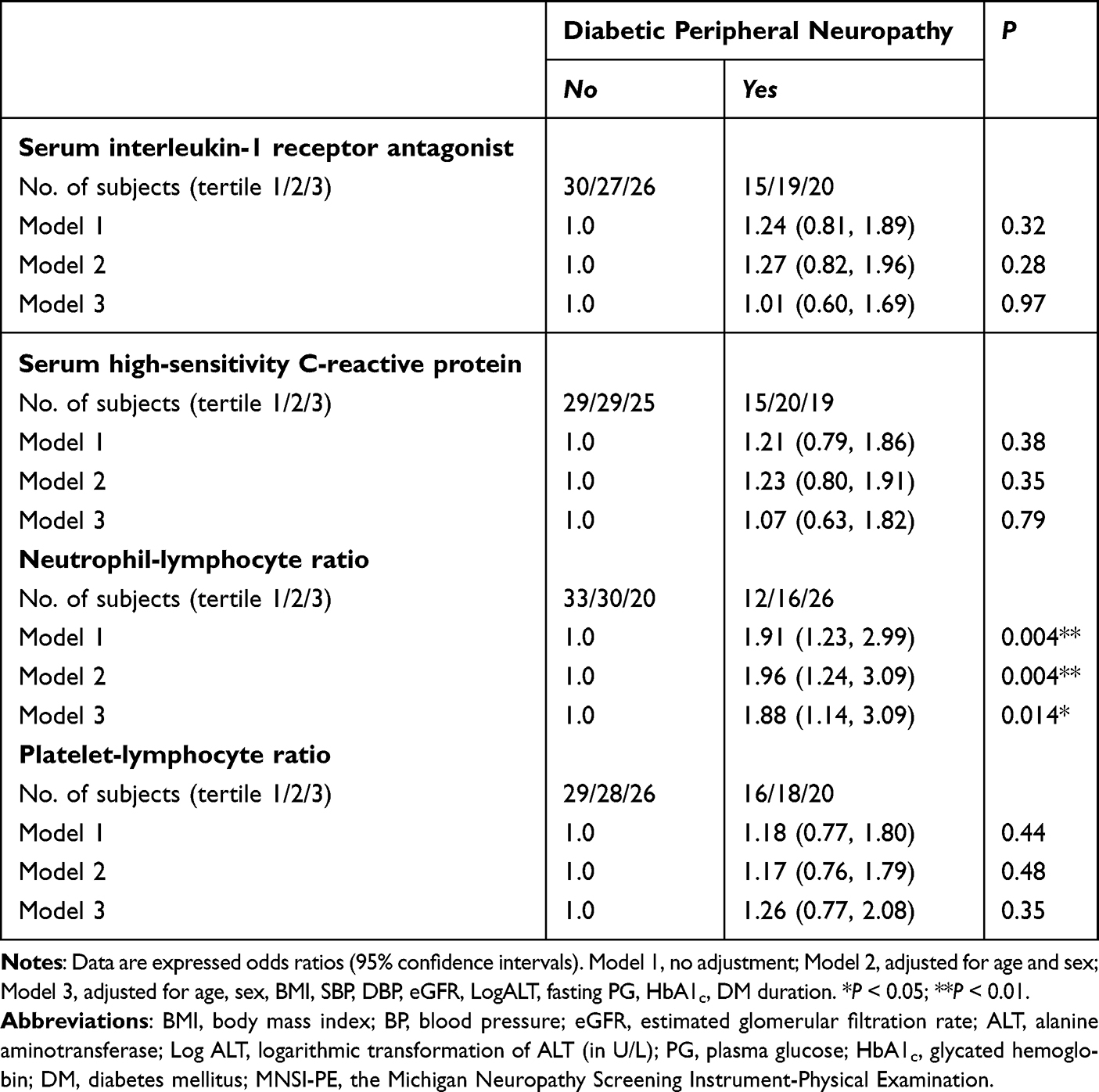 |
Table 3 Logistic Regression Analysis of Diabetic Peripheral Neuropathy (Yes vs No) in the Association with Markers of Inflammation (Grouped Into Tertiles According to Inflammatory Marker Levels) in Patients with Type 2 Diabetes Mellitus (n = 137) |
 |
Figure 1 Prevalence of diabetic peripheral neuropathy (DPN) among type 2 diabetes patients by tertiles of circulating levels of inflammatory markers. DPN was diagnosed if a participant scored ≥ 2 on the Michigan Neuropathy Screening Instrument-Physical Examination. There were significant differences in prevalence of DPN among patients with different levels of NLR by χ2 tests; however, the significant differences could not be detected among the PLR, the IL1-Ra and the hsCRP tertile groups. (A) IL-1Ra (interleukin-1 receptor antagonist): No significant difference in DPN prevalence across tertiles (χ² = 1.08, P = 0.58). (B) hsCRP (high-sensitivity C-reactive protein): No significant difference across tertiles (χ² = 0.82, P = 0.66). (C) NLR (neutrophil-to-lymphocyte ratio): A significant trend was observed, with increasing DPN prevalence from Tertile 1 to Tertile 3 (χ² = 9.11, P = 0.010*). (D) PLR (platelet-to-lymphocyte ratio): No significant difference in DPN prevalence (χ² = 0.60, P = 0.74). *P < 0.05. Abbreviations: IL1-Ra, interleukin-1 receptor antagonist; hsCRP; high-sensitivity C-reactive protein; NLR, neutrophil-lymphocyte ratio; PLR, platelet-lymphocyte ratio. |
The results of the univariate and multivariate linear regression analyses, with MNSI-PE score as the dependent variable, are presented in Table 4. Fasting glucose, HbA1c, eGFR, and Log(NLR) were identified as significant univariate correlates and were simultaneously included in the multivariate model to assess their relative contributions to MNSI-PE scores. In the final model, HbA1c and Log(NLR) remained significantly associated with MNSI-PE scores, while fasting glucose and eGFR did not retain statistical significance. The multivariate model collectively accounted for 15% of the variance in MNSI-PE scores (P < 0.0001).
 |
Table 4 Univariate and Multivariate Linear Regression Analyses of Clinical Parameters in Association with the Michigan Neuropathy Screening Instrument-Physical Examination Score (as the Dependent Variable) in Patients with Type 2 Diabetes (n = 137) |
Discussion
Our findings indicate that an inflammatory marker derived from blood cell counts, namely NLR, exhibit a significant association with DPN. Conversely, protein-based markers such as IL-1Ra and hs-CRP do not demonstrate a clear relationship with DPN. This study is among the few to investigate the intricate association between circulating inflammatory biomarkers and DPN in individuals with type 2 diabetes.
White cell count and its components are well-established inflammatory markers that are readily available and cost-effective to measure. NLR reflects the dynamic interplay between innate immunity (neutrophils) and the adaptive cellular immune response (lymphocytes) in various pathological states and disease conditions.13 In a systematic review and meta-analysis, Shahrabi et al reported that individuals with DPN exhibited significantly higher NLR levels compared to those without DPN (standardized mean difference = 0.61; 95% CI = 0.40–0.81, p < 0.001). The pooled positive likelihood ratio, negative likelihood ratio, and diagnostic odds ratio of NLR for DPN were 2.30 (95% CI = 1.71–3.09), 0.45 (95% CI = 0.30–0.67), and 5.06 (95% CI = 3.16–8.12), respectively.9 Consistent with these findings, the present study also demonstrated that patients with DPN had significantly higher NLR levels than those without DPN (Table 2). Furthermore, the prevalence of DPN in the highest NLR tertile was more than twice that of the lowest tertile (Figure 1). Notably, among the circulating inflammatory markers examined, NLR exhibited the strongest association with DPN in this study. These findings highlight NLR as a distinct inflammatory biomarker for DPN, suggesting its potential utility as a clinical tool for the early detection of DPN in patients with type 2 diabetes.
PLR is another blood cell-based inflammatory marker that warrants attention. An elevated PLR reflects variations in platelet and lymphocyte counts in response to inflammation, platelet activation, and prothrombotic states.14 In recent years, PLR has emerged as a valuable inflammatory marker for assessing various inflammatory conditions, cardiovascular diseases, and diabetes-related complications. A cross-sectional study conducted in Japan demonstrated that PLR may serve as a marker for high-risk diabetic foot and diabetic foot ulcer in patients with type 2 diabetes.15 Chen et al compared the predictive performance of PLR and NLR for incident DPN in a cohort comprising both type 1 and type 2 diabetes patients. Their findings suggested that while PLR effectively predicted DPN in type 1 diabetes, it was not a reliable predictor for type 2 diabetes.10 Similarly, Li et al analyzed the associations between blood cell ratios and DPN in a cohort of 1058 patients with type 2 diabetes. Their results indicated that NLR, but not PLR, was significantly associated with DPN risk.16 In this study, a marginal difference in Log (PLR) between the two groups was initially observed (P = 0.075, Table 2). However, this association was rendered statistically non-significant upon application of alternative analytical approaches (Table 3 and Table 4). These results indicate that the observed relationship between PLR and DPN is likely confounded by other factors, thereby limiting the potential of PLR as an independent biomarker for diabetic peripheral neuropathy in individuals with type 2 diabetes.
Serum hsCRP is widely recognized as a prototypical and commonly used marker of inflammation and has been linked to the development of DPN.17 Doupis et al reported that patients with diabetes and DPN exhibited higher hsCRP levels than those without DPN, even after adjustments for age, sex, and medication use.18 Additionally, data from a large cohort study with a one-year follow-up indicated that hsCRP levels exceeding 2.5 mg/L could predict neuropathic complications in individuals with type 2 diabetes.19 However, the natural aging process itself increased hsCRP levels.8 Similarly, Herder et al found that serum concentrations of IL-1Ra were positively associated with the presence of DPN and higher MNSI scores.20 However, findings from the InCHIANTI study did not support a significant association between serum IL-1Ra levels and peripheral nerve conduction.21 In a separate study, Herder et al previously reported that elevated circulating levels of hsCRP and IL-1Ra were associated with a higher risk of DPN over a 6.5-year period in the population-based KORA F4/FF4 cohort study. Nonetheless, after extensive adjustments for clinical parameters, the associations between hsCRP, IL-1Ra, and incident DPN were no longer significant.22–24 Consistent with these findings, the present study did not identify a significant association between serum protein-based markers (hsCRP and IL-1Ra) and DPN, both before and after adjustments (Table 3). The inconsistent findings across studies raise concerns regarding the reliability of hsCRP and IL-1Ra as biomarkers for DPN.7,25
There were limitations of the present study. First, it lacked peripheral neurophysiological test results. However, numerous studies in the literature have utilized MNSI to assess DPN, making it a reasonable choice for this study, particularly given the sample size of over 100 patients. Second, caution is warranted when generalizing these findings to other ethnic groups, as all participants in this study were of Chinese ethnicity. Third, lipid levels and the use of medications such as statins, antihypertensive agents, or antiplatelet drugs, may influence systemic inflammatory parameters and potentially confound biomarker-based associations and our statistical model did not include these variables. Additionally, the cross-sectional study design precludes the establishment of a causal relationship between DPN and inflammatory markers. However, a longitudinal follow-up of these patients is currently underway to address this limitation.
Conclusion
Our findings demonstrate that the neutrophil-to-lymphocyte ratio (NLR), an inflammation-related marker derived from peripheral blood cell counts, is significantly associated with diabetic peripheral neuropathy (DPN). In contrast, protein-based inflammatory markers such as interleukin-1 receptor antagonist (IL-1Ra) and high-sensitivity C-reactive protein (hsCRP) do not show a clear association with DPN. The underlying biological mechanisms responsible for these associations merit further investigation.
Acknowledgments
This work was supported by the National Science and Technology Council, Taiwan (NSTC113-2314-B-075-007-) and the Taipei Veterans General Hospital (V113C-166, V114C-177).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ang L, Mizokami-Stout K, Eid SA, et al. The conundrum of diabetic neuropathies-past, present, and future. J Diab Complications. 2022;36(11):108334. doi:10.1016/j.jdiacomp.2022.108334
2. ElSayed NA, McCoy RG, Aleppo G, American Diabetes Association Professional Practice Committee. Retinopathy, neuropathy, and foot care: standards of care in diabetes-2025. Diabetes Care. 2025;48(Supplement 1):S252–S265. doi:10.2337/dc25-S012
3. Pop-Busui R, Boulton AJ, Feldman EL, et al. Diabetic neuropathy: a position statement by the American diabetes association. Diabetes Care. 2017;40(1):136–154. doi:10.2337/dc16-2042
4. Cheng Y, Chen Y, Li K, et al. How inflammation dictates diabetic peripheral neuropathy: an enlightening review. CNS Neurosci Ther. 2024;30:e14477.
5. Bönhof GJ, Herder C, Strom A, Papanas N, Roden M, Ziegler D. Emerging biomarkers, tools, and treatments for diabetic polyneuropathy. Endocr Rev. 2019;40(1):153–192. doi:10.1210/er.2018-00107
6. Panou T, Gouveri E, Papazoglou D, Papanas N. The role of novel inflammation-associated biomarkers in diabetic peripheral neuropathy. Metabol Open. 2024;24:100328. doi:10.1016/j.metop.2024.100328
7. Hussain S, Yadav SS, Sawlani KK, et al. Evaluating pro- and anti-inflammatory biomarkers for predicting type 2 diabetes mellitus in the geriatric population and correlation with clinical and biochemical parameters. Cureus. 2025;17(1):e77896. doi:10.7759/cureus.77896
8. Milan-Mattos JC, Anibal FF, Perseguini NM, et al. Effects of natural aging and gender on pro-inflammatory markers. Braz J Med Biol Res. 2019;52(9):e8392. doi:10.1590/1414-431X20198392
9. Rezaei Shahrabi A, Arsenault G, Nabipoorashrafi SA, et al. Relationship between neutrophil to lymphocyte ratio and diabetic peripheral neuropathy: a systematic review and meta-analysis. Eur J Med Res. 2023;28(1):523. doi:10.1186/s40001-023-01479-8
10. Chen M, Zhu Y, Wang J, Wang G, Wu Y. The predictive value of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio levels of diabetic peripheral neuropathy. J Pain Res. 2021;14:2049–2058. doi:10.2147/JPR.S304595
11. Herman WH, Pop-Busui R, Braffett BH, et al. DCCT/EDIC Research Group. Use of the Michigan neuropathy screening instrument as a measure of distal symmetrical peripheral neuropathy in type 1 diabetes: results from the diabetes control and complications trial/epidemiology of diabetes interventions and complications. Diabet Med. 2012;29(7):937–944. doi:10.1111/j.1464-5491.2012.03644.x
12. Fateh HR, Ghasemi M, Ghasemi S, et al. Correlation of Michigan neuropathy screening instrument, United Kingdom screening test and electrodiagnosis for early detection of diabetic peripheral neuropathy. Diabetol Metab Syndr. 2016;8:36. doi:10.1186/s13098-016-0151-7
13. Zahorec R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl Lek Listy. 2021;122(7):474–488. doi:10.4149/BLL_2021_078
14. Gasparyan AY, Ayvazyan L, Mukanova U, Yessirkepov M, Kitas GD. The platelet-to-lymphocyte ratio as an inflammatory marker in rheumatic diseases. Ann Lab Med. 2019;39(4):345–357. doi:10.3343/alm.2019.39.4.345
15. Mineoka Y, Ishii M, Hashimoto Y, Yamashita A, Nakamura N, Fukui M. Platelet to lymphocyte ratio correlates with diabetic foot risk and foot ulcer in patients with type 2 diabetes. Endocr J. 2019;66(10):905–913. doi:10.1507/endocrj.EJ18-0477
16. Li J, Wang X, Jia W, et al. Association of the systemic immuno-inflammation index, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio with diabetic microvascular complications. Front Endocrinol. 2024;15:1367376. doi:10.3389/fendo.2024.1367376
17. Stanimirovic J, Radovanovic J, Banjac K, et al. Role of C-reactive protein in diabetic inflammation. Mediators Inflamm. 2022;2022:3706508. doi:10.1155/2022/3706508
18. Doupis J, Lyons TE, Wu S, Gnardellis C, Dinh T, Veves A. Microvascular reactivity and inflammatory cytokines in painful and painless peripheral diabetic neuropathy. J Clin Endocrinol Metab. 2009;94(6):2157–2163. doi:10.1210/jc.2008-2385
19. Aryan Z, Ghajar A, Faghihi-Kashani S, Afarideh M, Nakhjavani M, Esteghamati A. Baseline high-sensitivity C-reactive protein predicts macrovascular and microvascular complications of type 2 diabetes: a population-based study. Ann Nutr Metab. 2018;72(4):287–295. doi:10.1159/000488537
20. Herder C, Bongaerts BW, Rathmann W, et al. Association of subclinical inflammation with polyneuropathy in the older population: KORA F4 study. Diabetes Care. 2013;36(11):3663–3670. doi:10.2337/dc13-0382
21. Di Iorio A, Cherubini A, Volpato S, et al. Markers of inflammation, vitamin E and peripheral nervous system function: the InCHIANTI study. Neurobiol Aging. 2006;27(9):1280–1288. doi:10.1016/j.neurobiolaging.2005.07.004
22. Herder C, Kannenberg JM, Huth C, et al. Proinflammatory cytokines predict the incidence and progression of distal sensorimotor polyneuropathy: KORA F4/FF4 study. Diabetes Care. 2017;40(4):569–576. doi:10.2337/dc16-2259
23. Toronto Diabetic Neuropathy Expert Group, Tesfaye S, Boulton AJM, Dyck PJ, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care. 2010;33(10):2285–2293. doi:10.2337/dc10-1303
24. Herder C, Lankisch M, Ziegler D, et al. Subclinical inflammation and diabetic polyneuropathy: MONICA/KORA survey F3 (Augsburg, Germany). Diabetes Care. 2009;32(4):680–682. doi:10.2337/dc08-2011
25. Hussain G, Rizvi SA, Singhal S, et al. Serum levels of TNF-α in peripheral neuropathy patients and its correlation with nerve conduction velocity in type 2 diabetes mellitus. Diabetes Metab Syndr. 2013;7(4):238–242. doi:10.1016/j.dsx.2013.02.005
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Increased Systemic Immune-Inflammation Index Was Associated with Type 2 Diabetic Peripheral Neuropathy: A Cross-Sectional Study in the Chinese Population
Li J, Zhang X, Zhang Y, Dan X, Wu X, Yang Y, Chen X, Li S, Xu Y, Wan Q, Yan P
Journal of Inflammation Research 2023, 16:6039-6053
Published Date: 11 December 2023
Association of HbA1c Variability with Vibrating Perception Threshold in Middle-Aged and Elderly Patients with Type 2 Diabetes Mellitus: A Retrospective Cohort Study
Ding J, Shi Q, Dong L, Su H, Du Y, Pan T, Zhong X
Diabetes, Metabolic Syndrome and Obesity 2024, 17:193-202
Published Date: 10 January 2024
Lower Free Triiodothyronine is a Risk Factor of Diabetic Peripheral Neuropathy in Patients with Type 2 Diabetes Mellitus
Chen Y, Sun L, Chen M, Zhang H, Song B, Wang H, Jiang A, Zhang L, Li S, Wang J, Wang W, Zhang H
Diabetes, Metabolic Syndrome and Obesity 2024, 17:4407-4415
Published Date: 25 November 2024
Causal Central Network Remodeling in Diabetic Neuropathy: An Integrated MR-fMRI Study
Li X, Gao L
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2753-2765
Published Date: 9 August 2025
J-Shaped Relationship Between Visceral Fat Area and Large-Nerve Fiber Dysfunction Estimated by Vibration Perception Threshold in Type 2 Diabetes: A Cross-Sectional Study
Tang D, Gu X, Xuan Y, Liu Q, Lu L
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2935-2943
Published Date: 20 August 2025