Back to Journals » Psoriasis: Targets and Therapy » Volume 16
Bidirectional Associations Between Substance Abuse and Psoriasis: A Prospective Cohort Study
Authors Che X, Zhou J, Wang A, Guo J, Zhang C, Xiao Y
Received 2 August 2025
Accepted for publication 28 November 2025
Published 7 January 2026 Volume 2026:16 557781
DOI https://doi.org/10.2147/PTT.S557781
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Enzo Errichetti
Xuanlin Che,1– 3 Jiatong Zhou,1– 3 Anqi Wang,4 Jia Guo,1– 3 Chengcheng Zhang,5,6 Yi Xiao1– 3
1Department of Dermatology, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 2Hunan Engineering Research Center of Skin Health and Disease, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 3National Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 4Department of Dermatology, Third Hospital, Peking University, Beijing, People’s Republic of China; 5Department of Epidemiology and Biostatistics, School of Public Health, Guangdong Pharmaceutical University, Guangzhou, People’s Republic of China; 6Department of Social Medicine and Health Management, Xiangya School of Public Health, Central South University, Changsha, People’s Republic of China
Correspondence: Yi Xiao, Department of Dermatology, Xiangya Hospital, Central South University, 87 Xiangya Road, Changsha, Hunan, 410008, People’s Republic of China, Email [email protected] Chengcheng Zhang, Department of Epidemiology and Biostatistics, School of Public Health, Guangdong Pharmaceutical University, Guangzhou, People’s Republic of China, Email [email protected]
Background: Psoriasis and substance abuse remains a serious healthcare burden. However, associations between substance abuse and psoriasis have not been elucidated.
Objective: To evaluate the bidirectional associations between substance abuse and psoriasis.
Methods and Subjects: Based on the UK Biobank data, we conducted two prospective cohort studies to compare the risk of incident psoriasis in participants with versus without substance abuse (Cohort 1) and the risk of incident substance abuse in participants with versus without psoriasis (Cohort 2). Incident substance abuse (ICD: F10-F19) and psoriasis (ICD: L40) were primarily determined from hospital and primary care data, death registries and self-assessments.
Results: In Cohort 1, 4,097 of 454,245 developed psoriasis during follow-up. Baseline substance abuse was linked to an increased psoriasis risk (hazard ratio [HR]: 2.31, P< 0.001), notably in alcohol and tobacco users (HRs: 2.29 and 2.33, P< 0.001). Those with high genetic risk and substance abuse had the greatest psoriasis risk (HR: 5.19, P< 0.001). In Cohort 2, 25,176 out of 451,547 were diagnosed with substance abuse during follow-up. A notable association between baseline psoriasis and subsequent substance abuse (HR: 1.28, P< 0.001) was observed, slightly mediated by depression, anxiety, and sleep quality (1.7% to 3.4%; all P< 0.001). Sensitivity analyses showed consistent results.
Conclusion: Our findings identify bidirectional positive associations of substance abuse with psoriasis. This association is especially pronounced in those with both high genetic risk and alcohol or tobacco abuse. It is suggested that clinicians should consider alcohol or tobacco abuse among psoriasis patients to improve their life quality.
Plain Language Summary: What is already known about this topic?
Individual factors, like alcohol or tobacco consumption, have been reported to be associated with psoriasis risk. The bidirectional associations between the incidence of substance abuse and psoriasis remain unclear.
What does this article add to our knowledge?
Our findings emphasize a bidirectional positive relationship between substance abuse incidents and psoriasis. This association is especially pronounced in psoriasis patients with high genetic risk and in those who abuse alcohol and tobacco.
How does this study impact current management guidelines?
Our findings underscore the imperative of proactive measures against both psoriasis and substance abuse, especially concerning alcohol and tobacco.
Keywords: substance abuse, psoriasis, UK Biobank, bidirectional cohorts
Introduction
Psoriasis is a common, chronic, and inflammatory skin disease, which is characterized by dry, itchy, and raised skin plaques with silvery scales.1–3 Substance abuse pertains to the harmful use of psychoactive substances, such as alcohol, opioids, cannabinoids, sedatives, stimulants, hallucinogens, tobacco, and volatile solvents, frequently causing significant clinical distress.4–6 Substance abuse has been a thorny public health concern throughout human history.4,7 Evidence suggests a correlation between alcohol intake, smoking, and psoriasis risk.8–10 Several studies find that psoriasis may sustain drinking and smoking addition.11–13 Moreover, some studies have highlighted that opioid utilization is increasingly common among patients with psoriasis.14,15 Although “substance abuse” is a collective term, prior research has typically isolated individual factors, like alcohol or tobacco consumption, rather than holistically examining the interplay between substance abuse and psoriasis. Besides, nowadays researches involving substance abuse were difficult to control confounding factors.16 Therefore, this gap emphasizes the pressing need for large-scale prospective cohort studies to provide a comprehensive understanding of the bidirectional links between the incidence of substance abuse and psoriasis.
In the current study, we utilized the UK Biobank database to execute two prospective cohort studies. We assessed the risk of developing psoriasis among participants with and without substance abuse, and vice versa. Our goal is to underscore the intertwined relationship between substance abuse and psoriasis, fostering heightened public cognizance and paving the way for timely clinical interventions.
Methods and Subjects
Study Design and Participant
Our study is derived from the UK Biobank (our application number #55257), which recruited over 500,000 people as a general cohort in 2006–2010 at 22 research centres across England, Scotland, and Wales. Recruitment was done by sending letters with address information. Ethical approval has been approved by the Northwest Multicentre Research Ethics Committee (Ref: 21/NW/0157). According to the item 1 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China: Research involving human subjects in the life sciences and medicine that utilises personal information data or biological samples may be exempted from ethical review under the following circumstances: provided it does not cause harm to human subjects, nor involve sensitive personal information or commercial interests. This exemption aims to reduce unnecessary burdens on researchers and facilitate the advancement of human-involved life science and medical research. Research conducted using publicly available data obtained lawfully, or data generated through observation without interfering with public conduct. Participants were asked to complete a questionnaire on a touch-screen, perform physical measurements, and complete a face-to-face interview with a trained nurse after signing an informed consent form. You can get more information about UK Biobank on the official website (https://www.ukbiobank.ac.uk/). Our variables of interest were primarily substance abuse and psoriasis.
We constructed two cohorts in this study. In Cohort 1, we excluded 10,904 participants with prevalent psoriasis and 37,220 with missing data on key covariates including education, ethnicity, Townsend deprivation index (TDI), physical activity, body mass index (BMI), and polygenic risk scores of psoriasis (PRSpso), and included 45,4245 participants to evaluate the association of substance abuse with incident psoriasis. In Cohort 2, we excluded 25,795 participants with prevalent substance abuse and 25,027 participants with missing data on key covariates, and included 451,547 participants for analysis of the association between psoriasis and incident substance abuse (Figure 1). The study was conducted in accordance with the Strengthening Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
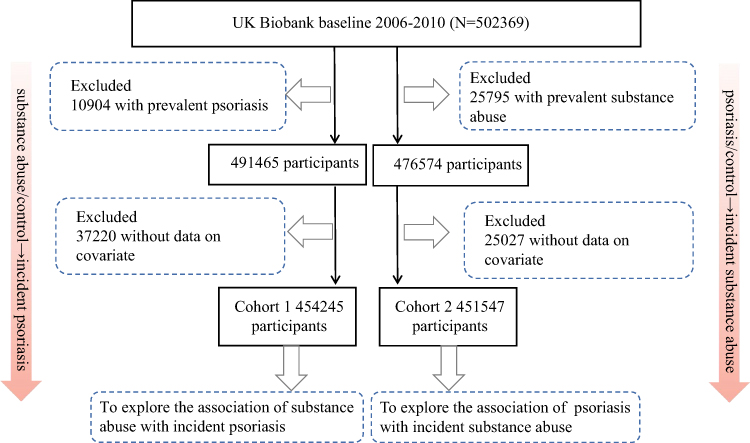 |
Figure 1 Participants selection. |
Ascertainment of Psoriasis
The diagnosis of psoriasis was primarily based on the patients’ hospital records. Linked primary care records were used as additional cases. Diagnoses were recorded using the International Classification of Diseases 10th Edition (ICD-10) coding system. The source of the participant’s psoriasis and date of first diagnosis can be downloaded from the first occurrence in UK Biobank.17 Psoriasis incidence was determined through linked hospital data until Oct 21, 2022, for England, Jul 31, 2021, for Scotland, Feb 28, 2018 for Wales. The follow-up endpoint date was determined by the date of first diagnosis, the date of death, the date of release, and the censoring date, whichever occurred first. We then calculated the time-to-event from the date of baseline recruitment to the follow-up endpoint date.
Ascertainment of Substance Abuse
Substance abuse determinations included mental and behavioural disorders caused by the use of alcohol, opioids, cannabinoids, sedatives or hypnotics, cocaine, other stimulants, hallucinogens, tobacco, volatile solvents or polydrug use, and use of other psychoactive substances, with ICD-10 coding F10-F19, respectively. The calculation of the incidence of substance abuse was similar to that of psoriasis.
Covariates
The data of sex, age, ethnicity, TDI, educational level, physical activity, smoking, alcohol consumption, BMI, and PRSpso were collected through an on-screen questionnaire at baseline survey. We selected these key covariates based on previous literature and complete and accurate records in the database we used.18,19 Ethnicity was categorized as white, mixed, Asian, black, Chinese, and other. TDI is an indicator of socioeconomic status, and higher scores represent worse living conditions. Smoking and alcohol consumption status were categorized into three categories: never, previous, and current. Ideal physical activity is defined as 75 minutes of vigorous exercise, 150 minutes of moderate-intensity exercise, 150 minutes of mixed (moderate and vigorous) exercise per week, or at least vigorous exercise once and moderate exercise at least five days a week. BMI was calculated as weight divided by squared height (kg/m2). In addition, we obtained PRSpso, which is widely used to estimate cumulative genetic risk for disease. PRSpso was constructed for all individuals from UK Biobank based on training data from external Genome-Wide Association Studies (GWAS), and the calculation was described in a previous study.20 PRSpso used in this study was obtained from UK Biobank (https://biobank.ndph.ox.ac.uk/ukb/field.cgi?id=26269). We then categorized the PRSpso into three groups based on quartiles: 1st for low genetic risk, 2nd to 3rd for intermediate risk, and 4th for high risk.
Mediation Variables
Symptoms of depression and anxiety were assessed using the Four-Item Patient Health Questionnaire (PHQ-4), and sleep quality was assessed using five sleep questions collected at baseline. Questions about depression symptoms included frequencies of 1) depressed mood and 2) lack of enthusiasm/interest; and anxiety symptoms included frequency of: 3) nervousness/restlessness, and 4) tiredness/sleepiness. Sleep quality questions included sleep duration, sleep type, insomnia, snoring, and daytime sleepiness, and the sleep quality score was summarised from five questions. Higher scores on depression and anxiety symptoms and sleep quality indicated greater severity.
Statistical Analysis
The statistical package R software version 3.6.2 was used for static processing. Descriptive statistics methods mean ± standard deviation (SD) for continuous variables and numbers (percentages) for categorical variables were used for data processing, and differences between groups were tested using t-tests and chi-square tests. To assess the association between substance abuse and psoriasis, Cox proportional hazard regression models (both unadjusted and adjusted models) were used. We calculated hazard ratios (HR) and 95% confidence intervals (CI) from the model. P values less than 0.05 were considered statistically significant.
Results
Participant Characteristics of Two Cohorts
A total of 4,097 individuals developed psoriasis in Cohort 1 over a median follow-up period of 13.48 years (Table 1), and 25,176 participants were diagnosed with incident substance abuse in Cohort 2 over a median follow-up period of 13.42 years (Table S1). Compared to participants without psoriasis at baseline, the proportions of male, current or previous smokers, overweight or obese and mean age and TDI were higher in patients with psoriasis.
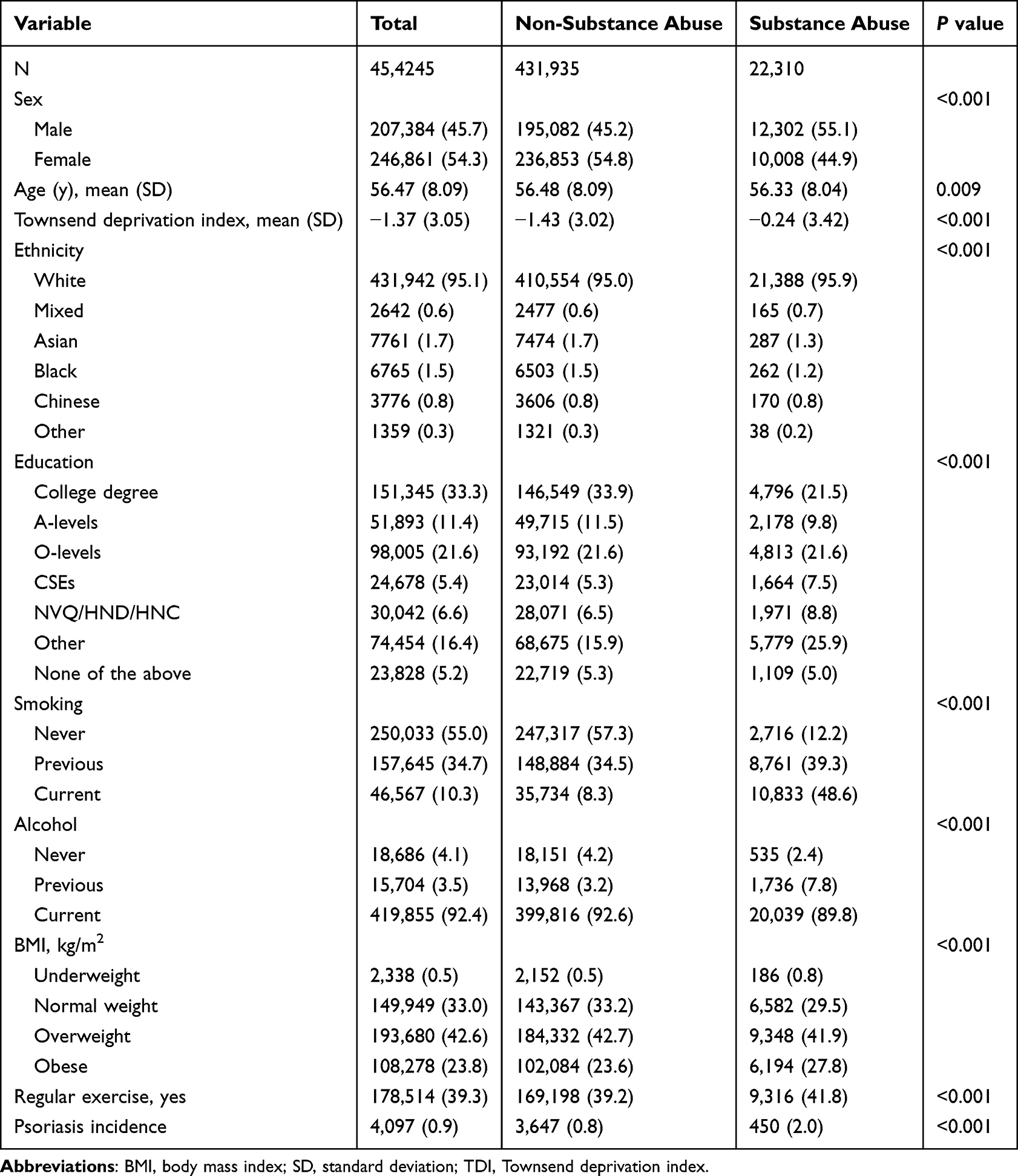 |
Table 1 Baseline Characteristic of the Participants in Cohort 1 |
Association of Prevalent Substance Abuse with Incident Psoriasis
In Cohort 1, we assessed the association of prevalent substance abuse with incident psoriasis. The crude HR for incident psoriasis was 2.47 (95% CI: 2.24 to 2.73) in participants with substance abuse at baseline compared to the non-exposure group (Figure 2). Substance abuse was significantly associated with psoriasis with an HR of 2.31 (95% CI: 2.09 to 2.57) after adjustments. For specific types of substance abuse, we found that alcohol (adjusted HR: 2.29; 95% CI: 1.82 to 2.88) and tobacco (adjusted HR: 2.33; 95% CI: 2.10 to 2.59) were associated with incident psoriasis. Furthermore, an additional 62% adjusted risk of incident psoriasis was also observed in participants with other types of substance abuse, although statistical significance was not reached due to the small sample size for this subgroup. The joint effects of high genetic risk and substance abuse were found, with an HR of 5.19 (95% CI: 4.37 to 6.15) for incident psoriasis compared with those with low genetic risk and no substance abuse (Figure 3). Consistent results were observed across subgroups by sex, age, TDI, and BMI (Figure S1).
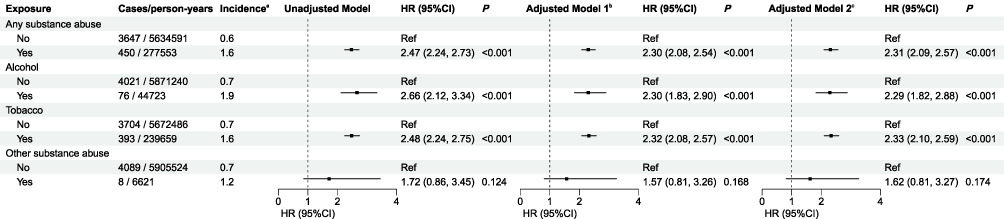 |
Figure 2 Association of substance abuse with the risk of incident psoriasis (Cohort 1). aPresented as events per 1000 person-years. bAdjusted for sex, age, ethnicity, Townsend deprivation score, educational level, physical activity, and body mass index. cAdditionally adjusted for polygenic risk scores. Abbreviations: CI, confidence interval; HR, hazard ratio. |
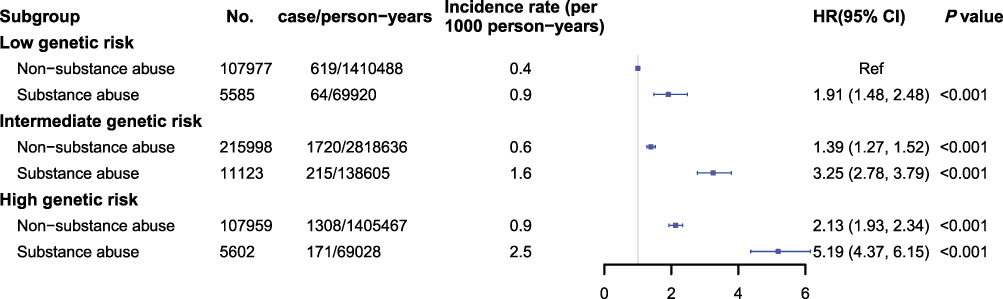 |
Figure 3 Joint effect of genetic risk and substance abuse on psoriasis incidence (Cohort 1). Adjusted for sex, age, ethnicity, Townsend deprivation score, educational level, physical activity, and body mass index. Abbreviations: CI, confidence interval; HR, hazard ratio. |
Association of Prevalent Psoriasis with Incident Substance Abuse
We further explored the association of prevalent psoriasis with incident substance abuse in Cohort 2 (Figure 4). After adjustments, a significant association of prevalent psoriasis with incident substance abuse was observed (HR: 1.28; 95% CI: 1.19 to 1.38). Besides, psoriasis was associated with incident alcohol abuse (HR: 1.41; 95% CI: 1.24 to 1.61) and incident tobacco abuse (HR: 1.24, 95% CI: 1.14, 1.34). Mediation analysis shows that symptoms of depression and anxiety and poor sleep quality mediated small proportions (1.7% to 3.4%; all P<0.001) of the total effect of psoriasis on substance abuse (Table S2). Consistent results were observed as above (Figure S2).
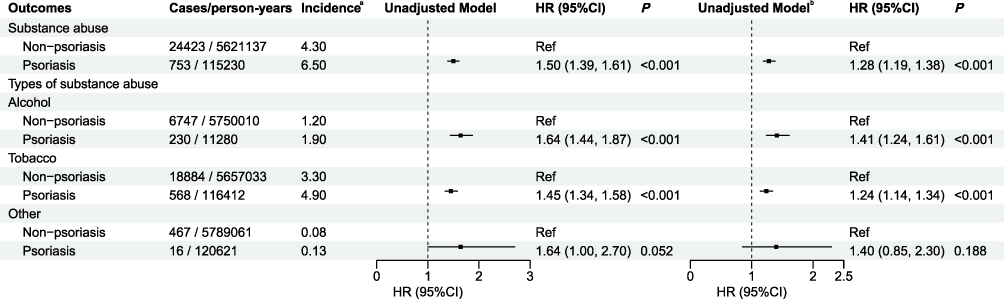 |
Figure 4 Association of psoriasis with the risk of incident substance abuse (Cohort 2). aPresented as events per 1000 person-years. bAdjusted for sex, age, ethnicity, Townsend deprivation index, educational level, physical activity, smoking status, alcohol status, and body mass index. Abbreviations: CI, confidence interval; HR, hazard ratio. |
Sensitivity Analysis
We performed sensitivity analyses to examine the robustness of the results. After excluding participants with less than two years of follow-up, the association of substance abuse with incident psoriasis was slightly attenuated but was consistent with the main findings in general (Table S3), while minimal change in the association of psoriasis with incident substance abuse was observed (Table S4). In the sensitivity analysis that excluded non-white populations, the association of substance abuse with psoriasis was barely changed (Tables S5 and S6).
Discussion
A significant association was found between prevalent substance abuse and incident psoriasis in our study. This association is especially pronounced in those with both high genetic risk and alcohol or tobacco abuse. Additionally, a marked positive correlation was observed between psoriasis and the incidence of substance abuse. Our results suggest an intricate relationship between substance abuse and psoriasis, offer new ideas for increased public awareness and prompt clinical interventions.
Previous studies had reported alcohol and tobacco intake on the risk of psoriasis. On the one hand, various findings suggested that smoking is an independent risk factor for the development of psoriasis.21,22 Jonathan et al utilized prospectively collected tobacco exposure data and revealed that prenatal exposure to tobacco exhibited a dose-response relationship with increased susceptibility to pediatric psoriasis, indicating a potential causal role of smoking in the pathogenesis of psoriasis.23 Lately, a Mendelian randomization study has further verified the causal relationship between smoking on psoriasis risk.9 On the other hand, as early as 1990, there was a retrospective study identified that alcohol is a risk factor for psoriasis.11 However, there are also some inconsistent findings.9,24,25 Hence, the available evidence is insufficient to establish alcohol consumption as a definitive risk factor for psoriasis.26 In our large-scale prospective cohort study, we confirm that alcohol abuse is a risk factor for the development of psoriasis. In addition to those, all previous studies have focused on analyzing the impact of a separate factor rather than comprehensively assessing the influence of substance abuse. Our research showed the joint effects of substance abuse to be a risk factor for the incidence of psoriasis. Therefore, early intervention of the disorder or behaviour of substance abuse, especially alcohol and tobacco abuse, could be an effective way to reduce incident psoriasis in the real-world setting. Besides smoking and alcohol, our findings indicate that there is an additional 62% adjusted risk of developing psoriasis associated with other forms of substance abuse, although no statistical significance was observed due to the small subgroup sample size. Previous studies have indicated that genes of the endogenous opioid system may be involved in the inflammatory dysregulation seen in psoriasis,27 suggesting that other forms of substance abuse, such as opioids and hallucinogens, could etiologically influence the initiation of psoriasis.
Moreover, our cohort 2 is the first to utilize a prospective cohort to reveal the relationship between psoriasis and the incidence of substance abuse behaviours as a whole, as well as the specific incidences of alcohol and tobacco abuse. Several prevalence studies are consistent with our results. Prior research has consistently shown that smoking and alcohol abuse are notably more prevalent among patients with psoriasis. For instance, a small-scale cross-sectional study conducted in 2007 found that patients with psoriasis exhibited addictive behaviours, including alcohol and tobacco abuse.13 Besides, another cross-sectional online survey in Germany also finds that there is a higher prevalence of daily smoking and alcohol dependency in individuals with psoriasis.28 We also detect the potential mediating effect of psychological symptoms and sleep quality on the impact of psoriasis on substance abuse. Previously, an amount of evidence revealed that patients with psoriasis often suffer from a psychosocial burden because of stigmatization or its comorbidities such as depression and anxiety.29–31 This might contribute to psychiatric pathology and substance abuse.32 However, the aspect that deviates from the anticipated expectations is that the mediation analysis displayed that depression symptoms, anxiety symptoms, or poor sleep quality all partially only mediated a very small part of the total effect of the association between psoriasis and incident substance abuse. More possible reasons mediating this behaviour change needed further research. It seems that there is a vicious positive feedback loop between psoriasis and substance abuse, indicating early intervention of psoriasis and substance abuse is necessary. As dermatologists, it is incumbent upon us to promptly identify and intervene in the early stages of psoriasis and substance abuse.
There are still some limitations to consider. First, the majority of participants in the UK Biobank were of European ancestry, which may limit the generalizability of the findings to populations with different backgrounds. Second, the symptoms of depression and anxiety, as well as sleep quality in this study, were self-reported, which could affect the accuracy of the information. Despite these limitations, this research has notable strengths. To our knowledge, it is the first large-scale prospective cohort study to report the bidirectional associations between substance abuse and psoriasis. It provides a higher level of evidence than previous retrospective studies.
Conclusion
Our findings highlight the importance of proactive measures against both psoriasis and alcohol or tobacco abuse. Early intervention of alcohol or tobacco abuse might effectively reduce incident psoriasis, though population information from other continents are needed in the future.
Abbreviations:
TDI, Townsend deprivation index; BMI, Body mass index; PRSpso, Polygenic risk scores of psoriasis; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; ICD-10, International Classification of Diseases 10th edition; GWAS, Genome-Wide Association Studies; SD, Standard deviation; PHQ-4, Four-Item Patient Health Questionnaire; HRs, Hazard ratios; CI, Confidence interval.
Data Sharing Statement
The data is available upon application at the UK Biobank’s official site.
Author Statement
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Xuanlin Che, Jiatong Zhou contributed equally as the first authors. Anqi Wang, Jia Guo, Chengcheng Zhang and Yi Xiao contributed equally as the senior authors.
Funding
This work was supported by the National Natural Science Foundation of China (82103737), the National Key Research and Development Program of China (2021YFF1201205), the National Natural Science Funds for Distinguished Young Scholars (82225039), and Huxiang Youth Talent Program (2022RC1014).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JP. Psoriasis. Lancet. 2021;397(10281):1301–9 doi:10.1016/S0140-6736(20)32549-6
2. Conrad C, Gilliet M. Psoriasis: from pathogenesis to targeted therapies. Clin Rev Allergy Immunol. 2018;54(1):102–113. doi:10.1007/s12016-018-8668-1
3. Greb JE, Goldminz AM, Elder JT, et al. Psoriasis. Nat Rev Dis Primers. 2016;2(1):16082. doi:10.1038/nrdp.2016.82
4. Frances RJ. Substance abuse. JAMA. 1991;265(23):3171–3172. doi:10.1001/jama.1991.03460230121039
5. McLellan AT. Substance misuse and substance use disorders: why do they matter in healthcare? Transac Amer Clin Climatolog Assoc. 2017;128:112–130.
6. Loftis JM, Huckans M. Substance use disorders: psychoneuroimmunological mechanisms and new targets for therapy. Pharmacol Ther. 2013;139(2):289–300. doi:10.1016/j.pharmthera.2013.04.011
7. Lo TW, Yeung JWK, Tam CHL. Substance abuse and public health: a multilevel perspective and multiple responses. Int J Environ Res Public Health. 2020;17(7):2610. doi:10.3390/ijerph17072610
8. Gerdes S, Zahl VA, Weichenthal M, Mrowietz U. Smoking and alcohol intake in severely affected patients with psoriasis in Germany. Dermatology. 2010;220(1):38–43. doi:10.1159/000265557
9. Wei J, Zhu J, Xu H, et al. Alcohol consumption and smoking in relation to psoriasis: a Mendelian randomization study. British J dermatol. 2022;187(5):684–691. doi:10.1111/bjd.21718
10. Lee EJ, Han KD, Han JH, Lee JH. Smoking and risk of psoriasis: a nationwide cohort study. J Am Acad Dermatol. 2017;77(3):573–575. doi:10.1016/j.jaad.2017.04.015
11. Poikolainen K, Reunala T, Karvonen J, Lauharanta J, Kärkkäinen P. Alcohol intake: a risk factor for psoriasis in young and middle aged men? BMJ. 1990;300(6727):780–783. doi:10.1136/bmj.300.6727.780
12. McAleer MA, Mason DL, Cunningham S, et al. Alcohol misuse in patients with psoriasis: identification and relationship to disease severity and psychological distress. British J dermatol. 2011;164(6):1256–1261. doi:10.1111/j.1365-2133.2011.10345.x
13. Zink A, Herrmann M, Fischer T, et al. Addiction: an underestimated problem in psoriasis health care. J Euro Acad Dermatol Venereol. 2017;31(8):1308–1315. doi:10.1111/jdv.14204
14. Taylor MT, Noe MH, Horton DB, Barbieri JS. Trends in opioid prescribing at outpatient visits for psoriasis and psoriatic arthritis. British J Dermatol. 2021;185(1):200–201. doi:10.1111/bjd.19865
15. Noe MH, Shin DB, Wehner MR, Margolis DJ, Gelfand JM. Opioid prescribing in adults with and without psoriasis. J Am Acad Dermatol. 2020;83(6):1777–1779. doi:10.1016/j.jaad.2020.03.080
16. Larsson SC, Butterworth AS, Burgess S. Mendelian randomization for cardiovascular diseases: principles and applications. Eur Heart J. 2023;44(47):4913–4924. doi:10.1093/eurheartj/ehad736
17. Saklatvala JR, Hanscombe KB, Mahil SK, et al. Genetic validation of psoriasis phenotyping in UK biobank supports the utility of self-reported data and composite definitions for large genetic and epidemiological studies. J investigat dermatol. 2023;143(8):1598–1601.e1510. doi:10.1016/j.jid.2023.02.010
18. Shen M, Xiao Y, Jing D, et al. Associations of combined lifestyle and genetic risks with incident psoriasis: a prospective cohort study among UK Biobank participants of European ancestry. J Am Acad Dermatol. 2022;87(2):343–350. doi:10.1016/j.jaad.2022.04.006
19. Budu-Aggrey A, Brumpton B, Tyrrell J, et al. Evidence of a causal relationship between body mass index and psoriasis: a mendelian randomization study. PLoS Med. 2019;16(1):e1002739. doi:10.1371/journal.pmed.1002739
20. Thompson DJ, Wells D, Selzam S, et al. UK biobank release and systematic evaluation of optimised polygenic risk scores for 53 diseases and quantitative traits. Paper presented at: medRxiv. 2022.
21. Armstrong AW, Harskamp CT, Dhillon JS, Armstrong EJ. Psoriasis and smoking: a systematic review and meta-analysis. British J Dermatol. 2014;170(2):304–314. doi:10.1111/bjd.12670
22. Williams HC. Smoking and psoriasis. BMJ. 1994;308(6926):428–429. doi:10.1136/bmj.308.6926.428
23. Groot J, Nybo Andersen AM, Blegvad C, Pinot de Moira A, Skov L. Prenatal, infantile, and childhood tobacco exposure and risk of pediatric psoriasis in the Danish national birth Cohort offspring. J Am Acad Dermatol. 2020;83(6):1625–1632. doi:10.1016/j.jaad.2019.09.038
24. Dai YX, Wang SC, Chou YJ, et al. Smoking, but not alcohol, is associated with risk of psoriasis in a Taiwanese population-based cohort study. J Am Acad Dermatol. 2019;80(3):727–734. doi:10.1016/j.jaad.2018.11.015
25. Li W, Chan AA, Han J, Chlebowski RT, Lee DJ. Alcohol and smoking cessation as potential modulators for smoking-associated psoriasis risk in postmenopausal women: the women’s health initiative. Ame J Clin Dermatol. 2023;24(2):325–332. doi:10.1007/s40257-022-00750-8
26. Brenaut E, Horreau C, Pouplard C, et al. Alcohol consumption and psoriasis: a systematic literature review. J Euro Acad Dermatol Venereol. 2013;27(Suppl 3):30–35. doi:10.1111/jdv.12164
27. Loite U, Raam L, Reimann E, et al. The expression pattern of genes related to melanogenesis and endogenous opioids in psoriasis. Int J Mol Sci. 2021;22(23). doi:10.3390/ijms222313056
28. Schielein MC, Tizek L, Schuster B, et al. Always online? Internet addiction and social impairment in psoriasis across Germany. J Clin Med. 2020;9(6):1818. doi:10.3390/jcm9061818
29. EclinicalMedicine. The burden of psoriasis: a call for awareness. EClinicalMedicine. 2021;38:101114. doi:10.1016/j.eclinm.2021.101114
30. Strober B, Gooderham M, de Jong E, et al. Depressive symptoms, depression, and the effect of biologic therapy among patients in psoriasis longitudinal assessment and registry (PSOLAR). J Am Acad Dermatol. 2018;78(1):70–80. doi:10.1016/j.jaad.2017.08.051
31. Adesanya EI, Matthewman J, Schonmann Y, et al. Factors associated with depression, anxiety and severe mental illness among adults with atopic eczema or psoriasis: a systematic review and meta-analysis. British J Dermatol. 2023;188(4):460–470. doi:10.1093/bjd/ljac132
32. Hayes J, Koo J. Psoriasis: depression, anxiety, smoking, and drinking habits. Dermatologic Therapy. 2010;23(2):174–180. doi:10.1111/j.1529-8019.2010.01312.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cutaneous Adverse Events After COVID-19 Vaccination
Weschawalit S, Pongcharoen P, Suthiwartnarueput W, Srivilaithon W, Daorattanachai K, Jongrak P, Chakkavittumrong P
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1473-1484
Published Date: 8 June 2023
Increased Risk of Dermatomyositis in Patients with Psoriasis: A Retrospective Cohort Study
Chen M, Tian N, Cui R, Zhang H, Wang Q, Tong Q, Chen Z, Wang YH, Wei JC, Dai SM
ImmunoTargets and Therapy 2025, 14:139-149
Published Date: 1 March 2025
Psoriasis Increases the Risk of ANCA Associated Vasculitis: Insights from A Propensity Score-Matched Study
Cui R, Wang Q, Kang ZJ, Du Y, Chen M, Wang YH, Wei JC, Dai S
ImmunoTargets and Therapy 2025, 14:1087-1095
Published Date: 26 September 2025
Global Trends and Future Predictions of Psoriasis Burden: Insights from the GBD 2021 Study
Gu X, Wang X, Bin Y, Xue R, Zhu G
Psoriasis: Targets and Therapy 2025, 15:569-580
Published Date: 24 December 2025