Back to Journals » Psoriasis: Targets and Therapy » Volume 15
Beyond Skin Clearance: Personalized Strategies for DLQI Improvement in Psoriasis -Insights From a Shanghai Prospective Cohort
Authors Ma X ![]() , Xu Q
, Xu Q ![]() , Kuai L, Shen F, Duan Z
, Kuai L, Shen F, Duan Z ![]() , Gao X
, Gao X ![]() , Zhang R, Wang R
, Zhang R, Wang R ![]()
Received 22 April 2025
Accepted for publication 6 August 2025
Published 13 August 2025 Volume 2025:15 Pages 373—387
DOI https://doi.org/10.2147/PTT.S534881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Enzo Errichetti
Xin Ma,1,2,* Quanruo Xu,3,* Le Kuai,4,* Fanlingzi Shen,3 Zhen Duan,3 Xiangjin Gao,1 Rui Zhang,1 Ruiping Wang1,3
1Clinical Research Center, Shanghai Skin Diseases Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Department of Traditional Chinese Medicine, Shanghai Skin Diseases Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 3School of Public Health, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 4Department of Dermatology, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruiping Wang, Clinical Research Center, Shanghai Skin Diseases Hospital, School of Medicine, Tongji University, 1278 Baode Road, Jing’an District, Shanghai, 200443, People’s Republic of China, Email [email protected]
Introduction: Psoriasis is a chronic immune-mediated disease that significantly impacts patients clinically and psychologically. Physician-assessed severity measures, including Psoriasis Area and Severity Index (PASI), Body Surface Area (BSA), and Physician Global Assessment (PGA), often fail to capture patient-reported outcomes, particularly when clinical improvement and perceived quality-of-life gains are misaligned.
Purpose: To clarify the association between clinical improvements and Dermatology Life Quality Index (DLQI) outcomes, identify predictors of substantial DLQI improvement (≥ 90% reduction), and explore reasons for suboptimal DLQI responses in patients achieving skin clearance.
Methods: In this 12-week prospective study, 551 psoriasis patients were enrolled at Shanghai Skin Diseases Hospital. Data on demographics, clinical severity (PASI, BSA, and PGA), DLQI scores, and treatment modalities were collected. Logistic regression analyses were employed to assess the dose–response relationships between improvements in clinical parameters and DLQI reduction, and to identify factors of suboptimal DLQI improvement among patients achieving significant skin clearance.
Results: Median DLQI improved significantly (8.0 to 3.0) at week 12, with 24.1% of patients achieving ≥ 90% DLQI reduction. Strong dose-response associations existed between clinical severity improvements (PASI, BSA, PGA) and DLQI gains. PASI75 responders were significantly more likely to achieve substantial DLQI improvement (OR = 2.48, 95% CI: 1.51– 4.07). However, only 33.3% of PASI75 achievers reached ≥ 90% DLQI improvement. Early clinical response (as early as week 4) strongly predicted superior DLQI outcomes. Female sex, older age, lower baseline DLQI scores, and shorter disease duration were associated with achieving high skin clearance but suboptimal DLQI improvement.
Conclusion: Early clinical response effectively predicts substantial DLQI improvement, whereas demographic and disease-related factors help identify patients at risk for suboptimal quality-of-life gains despite significant skin clearance. These insights support personalized therapeutic strategies aimed at improving patient satisfaction beyond skin clearance alone.
Keywords: psoriasis, quality of life, biologic agents, cohort study
Introduction
Psoriasis is a chronic, immune-mediated inflammatory disorder that affects approximately 100 million individuals worldwide.1 It is characterized by well-demarcated, erythematous plaques with silvery scales and is frequently accompanied by pruritus, pain, and significant psycho-social distress.2 Beyond its dermatological manifestations, psoriasis is closely linked to cardiovascular disease, metabolic syndrome, and mood disorders, all of which further complicate disease management and intensify the overall patient burden.3 The disorder also imposes substantial socioeconomic costs, stemming from increased healthcare expenditures, lost productivity, and social isolation due to the stigma of visible lesions.4,5
Although recent therapeutic advances, particularly with biologic therapies, have markedly enhanced skin clearance, physician-reported measures6,7 such as the Psoriasis Area and Severity Index (PASI), Body Surface Area (BSA), and Physician Global Assessment (PGA) do not fully capture the broader impact on patients’ daily functioning and quality of life.8,9 To address this gap, the Dermatology Life Quality Index (DLQI) has emerged as a critical tool for evaluating the multidimensional burden of psoriasis. Compared to generic quality-of-life instruments such as the EQ-5D or SF-36, the DLQI demonstrates greater sensitivity to dermatology-specific changes and is therefore more suitable for evaluating treatment outcomes in psoriasis.10,11
Treatment targets have increasingly incorporated both physician and patient reported outcomes. PASI75 and PASI90 are widely accepted as objective benchmarks for treatment response,12–14 a ≥5-point improvement in DLQI has been proposed as a clinically meaningful threshold for patient-reported benefit.15 These dual endpoints have been adopted in European guidelines, which recommend continuing treatment when PASI improvement is 50–75% and DLQI ≤5, and suggest treatment adjustment if DLQI remains >5 despite clinical response.12,16 In clinical settings, these thresholds also guide therapeutic decision-making.17 According to Chinese guidelines, biologic therapies are indicated not only for patients with PASI ≥10, but also for those with substantial physical or psychological burden—as reflected by a DLQI >10—regardless of PASI level.18
Despite these advances, real-world studies have reported that some patients fail to achieve meaningful DLQI improvement even after substantial PASI reduction, highlighting a disconnect between clinical and patient-perceived outcomes.19 Factors such as residual lesions in visible areas, psychological distress, or unmet treatment expectations may contribute to this disparity.20 However, predictors of poor DLQI response remain insufficiently explored, limiting the implementation of individualized care strategies.
In this prospective study conducted at Shanghai Skin Diseases Hospital (2022–2024), we examined the association between early clinical improvements and quality-of-life outcomes in 551 patients with psoriasis. By integrating demographic, clinical, and treatment-related data, we aimed to identify key factors associated with substantial DLQI improvement and to clarify why some patients derive limited quality of life benefit despite achieving high skin clearance. These insights may inform personalized treatment strategies that address both visible symptoms and patient-centered needs.
Methods
Data Source and Study Population
This observational study was conducted at Shanghai Skin Diseases Hospital between 2022 and 2024. Patients with psoriasis were recruited from a prospectively established cohort, and all participants provided written informed consent. Eligible patients were aged ≥18 years with a clinical diagnosis of psoriasis vulgaris in accordance with global diagnostic and treatment guidelines. Exclusion criteria included planned relocation within one year, inability to provide informed consent, and the presence of significant neurological or psychiatric disorders. The study protocol was approved by the Institutional Ethical Review Board of Shanghai Skin Diseases Hospital (2022–25). We have registered this study in the Chinese clinical trial registry (ChiCTR2200066894), and performed it in line with the Declaration of Helsinki and STROBE guidelines.
Sample Size Calculation
In this study, we applied the sample size calculation formula n=[μα2× p(1-p)]/δ2 for observational study. We set p=30% for the ≥90% of PASI score reduction at week 12 compared to baseline, type I error α=0.05, the allowed error δ=15% of p, and a non-response rate of 10%, the sample size calculation result indicated that at least 445 psoriasis patients should be recruited. Ultimately, 551 psoriasis patients were successfully enrolled and completed the full 12-week follow-up, with no missing data for any key variables included in the final analysis.
Data Collection
Patients underwent a standardized physical examination during routine clinic visits, during which dermatologists assessed disease severity using PASI, PGA, and BSA. Simultaneously, structured questionnaires were used to collect detailed information on demographic characteristics (age, sex, marital status, education level, monthly income, and residency status), lifestyle factors (tobacco smoking, alcohol consumption, body mass index [BMI, kg/m²], and other relevant habits), and clinical assessments and medical history, including baseline psoriasis severity (evaluated by PASI, BSA, and PGA), quality of life (DLQI), disease duration, non-communicable disease comorbidities, and family history of psoriasis. Treatment information was also documented and patients were classified based on the therapy received. Follow-up assessments of PASI, BSA, and PGA were performed at weeks 4, 8, and 12, while DLQI was re-evaluated at week 12.
Definitions and Classifications
Psoriasis severity was evaluated using the PASI (range 0–72), BSA (percentage of affected skin), and PGA (scale 0–5), with higher scores indicating greater severity. Treatment response was defined as PASI75 for a ≥75% reduction and PASI90 for a ≥90% reduction from baseline. Quality of life was assessed with the DLQI, a 10-item questionnaire with scores ranging from 0 (no impairment) to 30 (maximum impairment), categorized as 0–1 (no impact), 2–5 (mild impact), 6–10 (moderate impact), and >10 (severe impact). Each question is scored on a four-point scale, reflecting the extent to which individual’s life quality is adversely affected by the skin condition: not at all/not relevant (0), a little (1), a lot (2), and very much (3). For subgroup analyses, patients were stratified by the percentage reduction in DLQI at week 12, and a reduction of at least 90% is considered optimal.
A smoker was defined as an individual who has consumed at least 100 cigarettes in their lifetime, while a drinker was defined as someone who consumed alcohol more than twice per week for at least six months. Disease duration was defined as the interval between psoriasis onset and the current investigation, categorized as <5, 5–10, or >10 years. A positive family history of psoriasis was defined as having at least one first-degree relative (parents, siblings, or children) with the disease. A medical history of non-communicable diseases (NCDs) was defined as the presence of at least one of the following: diabetes mellitus, hypertension, hyperlipidemia, hyperuricemia, coronary atherosclerotic heart disease, nonalcoholic fatty liver disease, tumors, or chronic renal insufficiency.
Additional variables were classified as follows: age (<35, 35–45, 46–60, and >60 years); education level (primary or lower, junior high, senior high, and college and above); monthly income (<3000, 3000–5000, 5001–10,000, and >10,000 RMB); residency status (urban or rural); and marital status (married, unmarried, or divorced/widowed/widower/others). BMI was calculated as weight (kg) divided by height (m²) and categorized as <23.9 kg/m² (low/normal), 24.0–28.0 kg/m² (overweight), and >28.0 kg/m² (obesity). Treatment modalities were grouped as follows: acitretin (25–50 mg daily), methotrexate (15–20 mg per week with folic acid supplementation), narrowband UVB (NB-UVB, 2–4 sessions per week), and biologic agents (ustekinumab, risankizumab, secukinumab).
Statistical Analysis
Data in this study was analyzed by applying the SAS 9.4. All variables were complete with no missing data. Normality testing was performed for continuous variables using the Shapiro–Wilk test. Variables that followed a normal distribution were presented as means ± standard deviations and compared using the Student’s t-test; otherwise, they were expressed as medians with interquartile ranges (IQRs) and compared using the Mann–Whitney U-test. Categorical variables were expressed as frequencies and percentages, with group comparisons conducted using the chi-square test. Logistic regression was performed to identify factors associated with achieving a ≥90% DLQI reduction, and odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Subgroup analyses were conducted to assess the differences by sex, age, and treatment modality. In this study, a two-tailed P value <0.05 was considered statistically significant.
Results
In this study, 551 psoriasis patients were enrolled (Table 1), including 417 males (75.7%) and 134 females (24.3%), with a mean age of 45.8 ± 18.2 years. Approximately 40% of participants had a college education or higher. About two-thirds resided in urban areas, and marital status varied significantly (P < 0.001), with 76.9% of females married compared to 66.2% of males. The overall mean BMI was 25.0 ± 3.9 kg/m², with males exhibiting a higher BMI (25.4 kg/m²) than females (23.8 kg/m²). Additionally, 51.2% of patients were smokers and they were predominantly males (62.6%), the NCD comorbidities were also more common in males (46.5% vs 30.6%). Measures of disease severity demonstrated sex-related differences: the overall median PASI was 11.4 (IQR: 8.0–16.8), with males scoring higher (12.0 vs 9.6); median BSA was 14.2% (IQR: 9.0–25.3), higher in males (15.0% vs 12.0%); and the median PGA was also higher in males (3.0 vs 2.0).
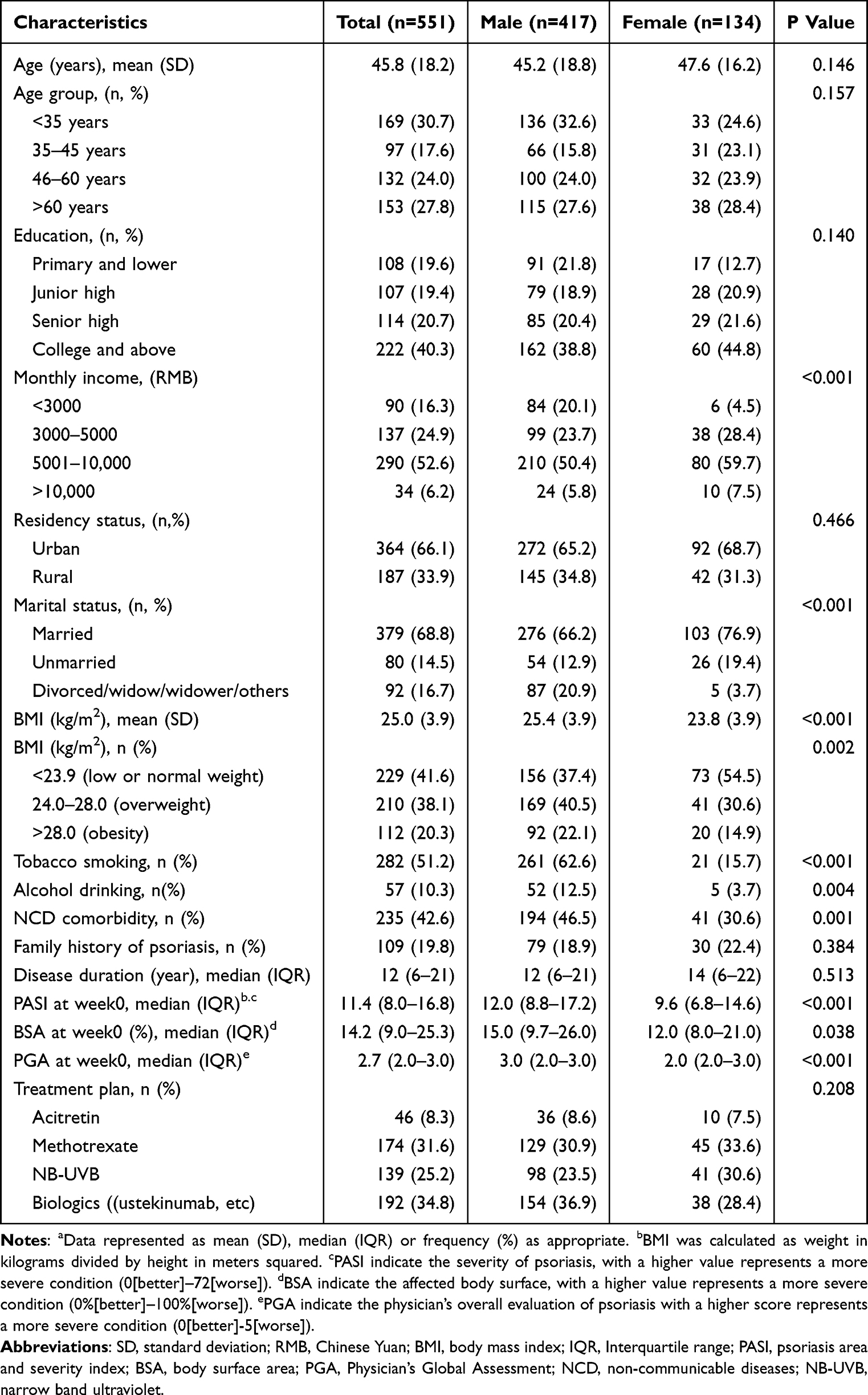 |
Table 1 The Baseline Characteristics of Patients with Psoriasis in Shanghaia |
Overall DLQI Improvement
At baseline, the median DLQI was 8.0 (IQR: 4.5–14.0), with no significant sex differences. After 12 weeks of treatment, the median DLQI significantly decreased to 3.0 (IQR: 1.0–7.0), with a mean reduction of 4.7 ± 6.3 points (Table 2). Initially, 68.1% of patients had DLQI scores in the higher ranges (6–10 and >10). By week 12, 37.0% had shifted to the 0–1 range, 29.9% to the 2–5 range, and only 11.1% remained in the >10 category. Moreover, 24.1% achieved a ≥90% reduction in DLQI, which was significantly more common in males (26.4%) than in females (17.2%; P = 0.030). Figure 1 illustrates a marked shift across each items of DLQI from baseline to week 12, with the greatest improvements observed in embarrassment/sadness (Q2) and sore, itchy, painful skin (Q1).
 |
Table 2 The Dermatology Life Quality Index (DLQI) Score Among Patients with Psoriasis in Shanghaia |
 |
Figure 1 Changes in the distribution of responses for the 10 DLQI items from baseline to week 12. Q1: Sore, itchy, painful skin; Q2: Embarrassment or self-consciousness; Q3: Impact on shopping or housework; Q4: Influence on clothing choices; Q5: Effect on social/leisure activities; Q6: Effect on sports/entertainment; Q7: Impact on work/study; Q8: Interpersonal problems; Q9: Sexual difficulties; Q10: Treatment difficulties. |
Early and Threshold‑Dependent Predictors of DLQI Improvement
In multivariable analyses (Table 3), both early clinical gains and attainment of key clearance thresholds robustly predicted ≥90% DLQI reduction at week 12. After adjusting for demographic and treatment factors (Model C), each one‑point decrease in PASI at week 4 increased the odds of substantial DLQI improvement by 6% (OR: 0.94; 95% CI: 0.91–0.98), strengthening to OR 0.90 (95% CI: 0.85–0.95) at week 8 and OR 0.78 (95% CI: 0.71–0.86) at week 12. Parallel dose–response trends were observed for BSA and PGA, indicating that even modest early reductions in skin severity forecast later quality‑of‑life benefits.
 |
Table 3 Treatment Effect Evaluation by PASI, BSA, PGA at week 4, week 8 and week 12 and Their Association with DLQI Score Deceased for at Least 90% at week 12 in Psoriasis Patients in Shanghai |
Achievement of clearance milestones further amplified this effect: by week 12, patients who reached PASI75 had 2.48‑fold higher odds of ≥90% DLQI reduction (95% CI: 1.51–4.07), those achieving PASI90 had 1.94‑fold greater odds (95% CI: 1.22–3.10), and patients with PGA 0/1 experienced a 2.44‑fold increase in the likelihood of substantial DLQI gains (95% CI: 1.48–4.04). Moreover, patients achieving PASI75 or PGA 0/1 as early as week 4 had over twice the odds of high DLQI reduction by week 12 (OR was 2.46 for PASI75 and 2.39 for PGA 0/1), underscoring the prognostic value of rapid skin clearance.
Dose–Response Patterns at Week 12 and Persistent DLQI Discordance
Dose–response analyses at week 12 (Table 4) demonstrated that greater clinical improvements corresponded to progressively higher odds of achieving ≥90% DLQI reduction. Compared with the lowest PASI change quartile, patients in the highest quartile (12.7–45.8 point reduction) had more than double the odds of substantial DLQI improvement (OR: 2.10; 95% CI: 1.21–3.65). Similar patterns were seen for BSA change (quartile 4, OR: 2.49; 95% CI: 1.37–4.52) and PGA change (quartile 4, OR: 3.61; 95% CI: 1.91–6.85). When evaluating percentage improvements, the top quartile of PASI reduction (76–100%) conferred a 6.70‑fold increase in odds (95% CI: 2.01–22.40), with comparable enhancements for BSA (OR: 4.75; 95% CI: 2.09–10.83) and PGA (OR: 5.33; 95% CI: 2.85–9.99). Nevertheless, notable discordance persisted: of the 54.4% of patients achieving PASI75 by week 12, only 33.3% attained ≥90% DLQI reduction, highlighting that significant clinical clearance does not guarantee commensurate improvements in quality of life and that additional patient‑centered factors must be addressed.
 |
Table 4 Dose–Response Evaluation Between Score Change of PASI, BSA, PGA at week 12 and the DLQI Score Deceased for at Least 90% at week 12 in Psoriasis Patients in Shanghai |
Determinants of DLQI Improvement Among Responders with ≥75% Skin Clearance
Table 5 summarizes patient characteristics stratified by DLQI reduction quartiles (0–25%, 26–50%, 51–75%, 76–100%) in those achieving ≥75% improvement in skin lesions. Among patients achieving PASI75, those in the highest DLQI reduction quartile (76–100%) were disproportionately male (83.5%), younger (mean age 41.1 years), and had longer disease duration (17.0 years) and higher baseline DLQI scores (11.0), while also being far more likely to receive biologic therapy (71.1%) compared with those in the lowest quartile. Parallel trends in the BSA and PGA subgroups reinforce that greater initial quality‑of‑life burden and access to advanced systemic treatments are key drivers of pronounced DLQI gains, even among patients with comparable clinical clearance.
 |
Table 5 Feature Comparison Between Different DLQI Score Decrease Percentage in Psoriasis Patients with at Least 75% Improvement in Skin Lesions Based on PASI, BSA, and PGA in Shanghai |
Demographic, Disease, and Treatment Predictors of DLQI Discordance
Figure 2 depicts adjusted odds ratios for failing to achieve ≥90% DLQI reduction despite clinical clearance. After controlling for treatment and baseline disease burden, female patients had substantially lower odds of optimal DLQI improvement than males, and patients aged 46–60 years (OR: 0.54) or >60 years (OR: 0.60) were similarly less likely to report major quality‑of‑life gains compared with those <35 years old. Married status was also associated with reduced odds, whereas single or divorced patients were over twice as likely to achieve ≥90% DLQI reduction (OR: 2.09; 95% CI: 1.27–3.44). Notably, higher socioeconomic status—reflected by education and monthly income—was linked to reduced likelihood of substantial DLQI gains (adjusted ORs <1).
 |
Figure 2 Forest Plot of Factors Associated with a ≥90% Reduction in DLQI at Week 12. The vertical line at odds ratio (OR)= 1 indicates no effect; points to the right suggest an increased likelihood, whereas points to the left suggest a decreased likelihood of reaching the DLQI improvement threshold. Bold italics indicate statistically significant differences. Abbreviations: CI, confidence interval; RMB, Chinese Yuan; NCD, non-communicable diseases; NB-UVB, narrowband ultraviolet B. |
Longer disease duration (>10 years) was positively associated with achieving ≥90% DLQI reduction, and biologic therapy conferred a more than three fold increase in odds compared with acitretin (OR: 3.73; 95% CI: 1.59–8.76). Consistent dose–response relationships between quartile improvements in PASI, BSA, and PGA and the probability of ≥90% DLQI reduction were observed across sex and treatment modalities (Figures S1–S3), with the strongest effect sizes in male patients and those receiving biologic agents. To further illustrate treatment-related differences, we compared DLQI outcomes across four treatment groups (Figure S4). Biologics showed the greatest benefit, with 39.6% of patients achieving ≥76% DLQI improvement, compared to 15.2% for acitretin.
Discussion
Psoriasis poses significant challenges for both patients and society due to its chronic nature and multifaceted impact. This burden underscores the necessity of proactive treatment strategies that not only target disease severity but also improve patients’ overall quality of life. While physician-reported measures such as PASI, BSA, and PGA are effective in evaluating skin clearance, they do not adequately reflect the broader functional and psychological impact of the disease.21,22 This disconnect emphasizes the importance of understanding patients’ treatment expectations and aligning therapeutic strategies with their individual goals through shared decision-making. In this study, we systematically collected comprehensive data on clinical severity (using PASI, BSA, and PGA) and patient-reported quality of life (DLQI), along with detailed demographic, lifestyle, and treatment information. Our findings highlight that integrating objective clinical indicators with patient-level characteristics and treatment choices can more accurately enhance quality of life and help achieve meaningful therapeutic outcomes.
Previous studies have shown that although changes in PASI and DLQI are moderately correlated, the PASI response alone does not reliably reflect improvements in quality of life.11,19 Our results builds on these findings by demonstrating a robust dose–response relationship between improvements in objective clinical measures (PASI, BSA, and PGA) and DLQI reductions, though this relationship was not entirely linear. The most pronounced quality-of-life benefits occur in patients who achieved near-complete skin clearance, corresponding to the 76–100% improvement range in clinical indicators. Notably, patients achieving a PASI improvement of 75% were over six times more likely to experience a ≥90% reduction in DLQI, with similar thresholds observed for both BSA and PGA. This finding aligns with previous work,23 suggesting that a PASI75 response represents a critical benchmark for meaningful patient-perceived benefits, while improvements below this threshold are substantially less influential. In other words, relying solely on PASI may underestimate overall benefits if the improvement does not reach this critical level. Conversely, the DLQI provides a more patient-centered assessment by capturing the broader impact of psoriasis on daily life.24 However, beyond a certain point—typically PASI90-additional improvements in PASI yield diminishing returns in DLQI.25 Notably, our findings highlight the potential of DLQI as a dynamic tool for early treatment guidance. Patients lacking early PASI response were much less likely to achieve meaningful DLQI improvement, suggesting that concurrent monitoring of DLQI can help identify non-responders and inform timely treatment adjustments to optimize outcomes.
Furthermore, our study underscores the prognostic value of early clinical response. Reductions in PASI, BSA, and PGA as early as week 4 were predictive of achieving a ≥90% DLQI improvement by week 12, with patients achieving PASI75 early being over twice as likely to experience marked quality-of-life gains. Similar associations were observed at weeks 8 and 12. These results echo previous studies that early treatment responses are strong predictors of long-term outcomes, particularly in patients receiving biologics.26 For example, early improvements at weeks 4 and 6 with ixekizumab have been shown to predict PASI75 achievement at week 12 with over 90% accuracy.27 Furthermore, the optimal thresholds for achieving a DLQI score of 0 or 1 were identified as a PASI75 achievement rate for ixekizumab and a PASI 50 achievement rate for ustekinumab at week 4.28 Overall, our findings underscore that early and sustained clinical improvements are associated with meaningful quality-of-life improvement over the 12-week period.
Subgroup analyses revealed that sex significantly influenced DLQI outcomes, with male patients more likely to achieve ≥90% DLQI improvement, especially when substantial PASI, BSA, or PGA gains were observed. Prior studies have shown that while female patients often present with lower clinical severity,29,30 they report greater psychological distress,31 reduced quality-of-life,29 higher treatment expectations,32 and an increased incidence of drug-related adverse events and drug-related discontinuation rates.33 In contrast, greater disease burden in male patients is often linked to higher BMI,34 more comorbidities,35 and lifestyle factors such as smoking and alcohol use.36,37 These sex-based differences may also reflect broader sociocultural influences—such as gender norms, stigma, and healthcare access—that vary by region and ethnicity.38,39 These findings underscore the need for sex-specific and culturally informed management strategies, and suggest that global psoriasis policies should consider local social contexts alongside biological differences to optimize patient-centered care.32,33
In this study, age and marital status further modulated the likelihood of optimal DLQI response. Younger patients generally exhibited better improvements, potentially attributable to fewer comorbidities, shorter disease duration, and higher treatment adherence.40,41 Similarly, unmarried or divorced/widowed individuals showed higher rates of DLQI improvement. This may reflect greater autonomy and fewer caregiving responsibilities, which could enhance treatment adherence. In contrast, married patients may experience greater psychosocial strain related to household or caregiving duties, negatively impacting treatment outcomes and perceived quality of life.42,43
Our findings further suggested that patients with higher education and higher monthly income tended to correlate with a lower likelihood of achieving ≥90% DLQI improvement. This apparent paradox may stem from multiple factors. First, individuals with lower income and less educational attainment tended to present with higher disease activity and more extensive skin involvement;44 our previous researches suggested that patients with higher baseline DLQI scores experienced greater improvements in quality of life. Second, highly educated patients may express lower satisfaction, potentially due to more realistic or cautious treatment expectations,45 which could influence the overall treatment outcomes and satisfaction. Furthermore, high-income individuals may experience increased stress and anxiety,46 which are factors known to negatively impact the treatment outcomes and satisfaction.45 Consequently, clinicians should engage in discussions about realistic outcomes tailored to the patient’s level of understanding. Ensuring that all patients maintain accurate expectations may enhance treatment engagement and overall satisfaction.
Treatment modality emerged as a key determinant of DLQI improvement. Patients receiving biologics consistently achieved the largest quality-of-life gains across all quartiles of PASI, BSA, and PGA improvement, reflecting their rapid and durable efficacy.47,48 Meanwhile, conventional therapies such as methotrexate and NB-UVB still provided meaningful DLQI improvement in select patients, highlighting their relevance as cost-effective options, particularly in resource-limited settings.49 Notably, real-world data suggest methotrexate may outperform other traditional agents in terms of long-term survival and tolerability, making it a viable option when biologics are inaccessible.50 However, treatment response is not uniform. Factors such as male sex, NCD comorbidities, alcohol consumption, and lack of prior biologic exposure were associated with suboptimal outcomes for both methotrexate and acitretin users, suggesting the need for careful patient stratification.50 Real-world data from Japan and Germany further support the long-term value of biologics, showing better adherence, reduced healthcare burden, and improved persistence despite variations in access.51,52 These insights underscore the need to move beyond severity-driven decisions and adopt multidimensional treatment strategies—guided by early clinical response, psychosocial burden, and cost-effectiveness—to achieve equitable, patient-centered psoriasis care.
This study has several limitations. First, the observational design precludes definitive causal inferences between clinical improvements and DLQI outcomes. Second, as all patients were recruited from a single tertiary care center, the generalizability of our findings may be limited. Third, potential residual confounding factors including the unmeasured socioeconomic or behavioral variables may have influenced DLQI outcomes among psoriasis patients and should be addressed in future studies. Lastly, the relatively short follow-up period of 12 weeks may not fully capture the long-term sustainability of quality-of-life improvements. Future multi-center studies with extended follow-up and randomized designs are warranted to validate and expand upon these findings.
Conclusion
This study demonstrates that early and sustained clinical improvement strongly predicts meaningful DLQI gains in psoriasis patients. Integrating patient characteristics, treatment modality, and early PASI response enables better identification of those likely to benefit from targeted strategies. While conventional therapies remain important, broader access to biologics—particularly for those with high DLQI burden—may offer greater long-term value. Routine DLQI monitoring in the early treatment phase can help guide timely adjustments, ensuring that both skin and quality-of-life goals are achieved.
Data Sharing Statement
The data for this study are available upon request from the corresponding author. The request should state the title and aim of the research for which the data are requested.
Ethics Approval and Informed Consent
The study was approved by the Institutional Ethical Review Board of Shanghai Skin Diseases Hospital (2022–25) and registered in the Chinese clinical trial registry (ChiCTR2200066894). We performed this study in line with the Declaration of Helsinki and STROBE guidelines.
Acknowledgments
We thank the dermatologists in Shanghai Skin Disease Hospital for data collection.
Funding
This study was supported by the Clinical Research Plan of SHDC (SHDC2024CRX032), the Clinical Research Program of Shanghai Municipal Health Commission (202240371), Intelligence Fund of Shanghai Skin Diseases Hospital (2021KYQD01), Shanghai Key Discipline Construction Project of Traditional Chinese Medicine (SHZYYZDXK-2024104), Youth Talent Promotion Project of China Association of Traditional Chinese Medicine (2024–2026) Category B (2024-QNRC2-B04), Health Young Talents of Shanghai Municipal Health Commission (2022YQ026), Youth Medical Talents–Specialist Program of Shanghai “Rising Stars of Medical Talents” Youth Development Program.
Disclosure
All authors report no conflicts of interest in this work.
References
1. WHO. Global report on psoriasis. 2016.
2. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
3. Takeshita J, Grewal S, Langan SM. Psoriasis and comorbid diseases. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
4. Mehrmal S, Uppal P, Nedley N, Giesey RL, Delost GR. The global, regional, and national burden of psoriasis in 195 countries and territories, 1990 to 2017: a systematic analysis from the Global Burden of Disease Study 2017. J Am Acad Dermatol. 2021;84(1):46–52. doi:10.1016/j.jaad.2020.04.139
5. Trettin B, Feldman SR, Andersen F, Danbjørg DB, Agerskov H. A changed life: the life experiences of patients with psoriasis receiving biological treatment. Br J Dermatol. 2020;183(3):516–523. doi:10.1111/bjd.18876
6. Puzenat E, Bronsard V, Prey S. What are the best outcome measures for assessing plaque psoriasis severity? A systematic review of the literature. J Eur Acad Dermatol Venereol. 2010;24(s2):10–16. doi:10.1111/j.1468-3083.2009.03562.x
7. Walsh JA, McFadden M, Woodcock J. Product of the Physician Global Assessment and body surface area: a simple static measure of psoriasis severity in a longitudinal cohort. J Am Acad Dermatol. 2013;69(6):931–937. doi:10.1016/j.jaad.2013.07.040
8. Nicolescu AC, Ionescu M-A, Constantin MM. Psoriasis Management Challenges Regarding Difficult-to-Treat Areas: therapeutic Decision and Effectiveness. Life. 2022;12(12):2050. doi:10.3390/life12122050
9. Ogbechie-Godec O, Azarchi S, Lee J, Cohen DE, Neimann A, Nagler AR. Validated patient-reported outcome measurements for psoriasis may not reflect patients’ current preferences. J Am Acad Dermatol. 2019;80(5):1445–1447.e4. doi:10.1016/j.jaad.2018.09.019
10. Sampogna F, Tabolli S, Söderfeldt B, Axtelius B, Aparo U, Abeni D. Measuring quality of life of patients with different clinical types of psoriasis using the SF‐36. Br J Dermatol. 2006;154(5):844–849. doi:10.1111/j.1365-2133.2005.07071.x
11. Herédi E, Rencz F, Balogh O. Exploring the relationship between EQ-5D, DLQI and PASI, and mapping EQ-5D utilities: a cross-sectional study in psoriasis from Hungary. Eur J Health Econ. 2014;15(S1):111–119. doi:10.1007/s10198-014-0600-x
12. Belinchón Romero I, Dauden E, Ferrándiz Foraster C, González-Cantero Á, Carrascosa Carrillo JM. Therapeutic goals and treatment response evaluation in moderate to severe psoriasis: an experts opinion document. Ann Med. 2021;53(1):1727–1736. doi:10.1080/07853890.2021.1986637
13. Gisondi P, Talamonti M, Chiricozzi A. Treat-to-Target Approach for the Management of Patients with Moderate-to-Severe Plaque Psoriasis: consensus Recommendations. Dermatol Ther. 2021;11(1):235–252. doi:10.1007/s13555-020-00475-8
14. Baker C, Mack A, Cooper A. Treatment goals for moderate to severe psoriasis: an A ustralian consensus. Aust J Dermatology. 2013;54(2):148–154. doi:10.1111/ajd.12014
15. de Ruiter CC, Rustemeyer T. Biologics Can Significantly Improve Dermatology Life Quality Index (DLQI) in Psoriatic Patients: a Systematic Review. PTT. 2022;12:99–112. doi:10.2147/PTT.S356568
16. Mrowietz U, Kragballe K, Reich K. Definition of treatment goals for moderate to severe psoriasis: a European consensus. Arch Dermatol Res. 2011;303(1):1–10. doi:10.1007/s00403-010-1080-1
17. Mermin D, Boursault L, Milpied B, Taieb A, Ezzedine K, Seneschal J. DLQI as a major criterion for introduction of systemic agents in patients with mild psoriasis. Acad Dermatol Venereol. 2016;30(11):1961–1964. doi:10.1111/jdv.13803
18. XJ Zhang, Wang G, FR Zhang, et al. Guideline for the diagnosis and treatment of psoriasis in China (2023 edition). Chin J Dermatol. 2023;56:573–625. doi:10.35541/cjd.20220839
19. Maul J-T, Maul LW, Didaskalu JA. Correlation between Dermatology Life Quality Index and Psoriasis Area and Severity Index in Patients with Psoriasis: a Cross- sectional Global Healthcare Study on Psoriasis. Acta Derm Venereol. 2024;104:adv20329. doi:10.2340/actadv.v104.20329
20. Muslimani MA, Bolcato V, Silvestri A, Brazzelli V. Psoriatic patients undergoing long‐term therapy with biologics: impact of residual localization of psoriasis on quality of life in an Italian clinical setting. Dermatologic Therapy. 2020;33:1. doi:10.1111/dth.14337
21. Kimball AB, Krueger G, Woolley JM. The dermatology life quality index (DLQI) provides qualitatively different information from the pasi. J Am Acad Dermatol. 2004;50(3):P156. doi:10.1016/j.jaad.2003.10.547
22. Yu N, Peng C, Zhou J. Measurement properties of the patient global assessment numerical rating scale in moderate-to-severe psoriasis. Br J Dermatol. 2023;189(4):437–446. doi:10.1093/bjd/ljad188
23. Mattei PL, Corey KC, Kimball AB. Psoriasis Area Severity Index (PASI) and the Dermatology Life Quality Index (DLQI): the correlation between disease severity and psychological burden in patients treated with biological therapies. Acad Dermatol Venereol. 2014;28(3):333–337. doi:10.1111/jdv.12106
24. Puig L, Thom H, Mollon P, Tian H, Ramakrishna GS. Clear or almost clear skin improves the quality of life in patients with moderate‐to‐severe psoriasis: a systematic review and meta‐analysis. Acad Dermatol Venereol. 2017;31(2):213–220. doi:10.1111/jdv.14007
25. Edson‐Heredia E, Banerjee S, Zhu B. A high level of clinical response is associated with improved patient‐reported outcomes in psoriasis: analyses from a Phase 2 study in patients treated with ixekizumab. Acad Dermatol Venereol. 2016;30(5):864–865. doi:10.1111/jdv.13032
26. Strober B. Biologic therapy for psoriasis: early response implies future success. Br J Dermatol. 2013;169(6):1178–1179. doi:10.1111/bjd.12726
27. Zhu B, Edson-Heredia E, Cameron GS. Early clinical response as a predictor of subsequent response to ixekizumab treatment: results from a Phase II study of patients with moderate-to-severe plaque psoriasis. Br J Dermatol. 2013;169(6):1337–1341. doi:10.1111/bjd.12610
28. Puig L, Zhu B, Burge R. Early Treatment Targets for Predicting Long-term Dermatology Life Quality Index Response in Patients with Moderate-to- Severe Plaque Psoriasis: a Post-hoc Analysis from a Long-term Clinical Study. The Journal of Clinical and Aesthetic Dermatology. 2020;13(10):18–22.
29. Guillet C, Seeli C, Nina M, Maul LV, Maul J-T. The impact of gender and sex in psoriasis: what to be aware of when treating women with psoriasis. Int J Women Dermatol. 2022;8(2):e010. doi:10.1097/JW9.0000000000000010
30. Hägg D, Sundström A, Eriksson M, Schmitt-Egenolf M. Severity of Psoriasis Differs Between Men and Women: a Study of the Clinical Outcome Measure Psoriasis Area and Severity Index (PASI) in 5438 Swedish Register Patients. Am J Clin Dermatol. 2017;18(4):583–590. doi:10.1007/s40257-017-0274-0
31. Napolitano M, Mastroeni S, Fania L. Sex‐ and gender‐associated clinical and psychosocial characteristics of patients with psoriasis. Clin Exp Dermatol. 2020;45(6):705–711. doi:10.1111/ced.14218
32. Maul JT, Navarini AA, Sommer R. Gender and age significantly determine patient needs and treatment goals in psoriasis – a lesson for practice. Acad Dermatol Venereol. 2019;33(4):700–708. doi:10.1111/jdv.15324
33. Verardi F, Maul LV, Borsky K. Sex differences in adverse events from systemic treatments for psoriasis: a decade of insights from the Swiss Psoriasis Registry (SDNTT). Acad Dermatol Venereol. 2024;38(4):719–731. doi:10.1111/jdv.19730
34. Norden A, Rekhtman S, Strunk A, Garg A. Risk of psoriasis according to body mass index: a retrospective cohort analysis. J Am Acad Dermatol. 2022;86(5):1020–1026. doi:10.1016/j.jaad.2021.06.012
35. Salihbegovic E, Kurtalic S, Omerkic E. Comorbidity in Men with Psoriasis. Med Arch. 2021;75(1):31. doi:10.5455/medarh.2021.75.31-34
36. Armstrong AW, Harskamp CT, Dhillon JS, Armstrong EJ. Psoriasis and smoking: a systematic review and meta‐analysis. Br J Dermatol. 2014;170(2):304–314. doi:10.1111/bjd.12670
37. Choi J, Han I, Min J. Dose‐response analysis between alcohol consumption and psoriasis: a systematic review and meta‐analysis. J Deutsche Derma Gesell. 2024;22:641–652.
38. Bray JK, Cline A, McMichael AJ, Feldman SR. Differences in healthcare barriers based on racial and/or ethnic background for patients with psoriasis. J Dermatological Treat. 2021;32(6):590–594. doi:10.1080/09546634.2019.1687824
39. Mazurkiewicz N, Krefta J, Lipowska M. Attitudes Towards Appearance and Body-Related Stigma Among Young Women With Obesity and Psoriasis. Front Psychiatry. 2021;12:1. doi:10.3389/fpsyt.2021.788439
40. Sampogna F, Chren MM, Melchi CF, Pasquini P, Tabolli S, Abeni D. Age, gender, quality of life and psychological distress in patients hospitalized with psoriasis. Br J Dermatol. 2006;154(2):325–331. doi:10.1111/j.1365-2133.2005.06909.x
41. Trettel A, Spehr C, Körber A, Augustin M. The impact of age on psoriasis health care in Germany. Acad Dermatol Venereol. 2017;31(5):870–875. doi:10.1111/jdv.14115
42. Sharma D, Jilani AQ, Sharma P. Determinants and Correlates of Depression in Psoriasis Patients: does Marital Adjustment Play a Role? Ind J Private Psychiatry. 2024;18(2):75–79. doi:10.5005/jp-journals-10067-0159
43. Wu M, Zeng S, Zhang Y. Disease Burden and Coping Strategies of Spouses of Patients with Psoriasis: a Qualitative Study. JMDH. 2024;17:1653–1662. doi:10.2147/JMDH.S458075
44. Gilkey T, Lampley N, Salvator A, Padmanabhan A. 51395 Socioeconomic Status Correlates with Increased Use of Biologic Treatments and Improved Outcomes in Psoriasis Patients. J Am Acad Dermatol. 2024;91(3):AB315. doi:10.1016/j.jaad.2024.07.1255
45. Bishop MD, Mintken P, Bialosky JE, Cleland JA. Factors shaping expectations for complete relief from symptoms during rehabilitation for patients with spine pain. Physiother Theory Pract. 2019;35(1):70–79. doi:10.1080/09593985.2018.1440676
46. Akkiraju K, Rao ND. Higher income is associated with greater life satisfaction, and more stress. Commun Psychol. 2025;3(1):27. doi:10.1038/s44271-025-00210-z
47. Jung S, Suh D, Lee S-M. Factors Associated with Treatment Satisfaction in Korean Patients with Psoriasis. PPA. 2024;18:2093–2105. doi:10.2147/PPA.S485512
48. Thomas SE, van den Reek JMPA, Seyger MMB, de Jong EMGJ. How to define a ‘super-responder’ to biologics in psoriasis studies. Br J Dermatol. 2023;189(5):621–622. doi:10.1093/bjd/ljad280
49. McCoy T, Natarelli N, Pan A, Shakhbazova A, Sivamani RK, Chambers CJ. Systematic review and estimated cost‐efficacy of biologics compared with narrowband ultraviolet B light for the treatment of moderate to severe psoriasis and atopic dermatitis. Int J Dermatology. 2023;62(8):986–999. doi:10.1111/ijd.16677
50. Alabas OA, Mason KJ, Yiu ZZN. Effectiveness and persistence of Acitretin, ciclosporin, fumaric acid esters and methotrexate for patients with moderate-to-severe psoriasis: a cohort study from BADBIR. Br J Dermatol. 2023;188(5):618–627. doi:10.1093/bjd/ljad004
51. Miyazaki C, Masuda J, Rodriguez-Rey MD. Real-world biologic treatment patterns and healthcare resource utilization in psoriasis patients using an insurance claims database in Japan. J Dermatological Treat. 2024;35:2. doi:10.1080/09546634.2023.2299598
52. Pinter A, Schulte M, Kossack N, Pignot M, Schultze M, Feldhus A. Real-world psoriasis treatment patterns and disease burden in Germany, with a focus on biologics and apremilast: data from a German statutory health insurance database. Journal of Medical Economics. 2025;28(1):207–220. doi:10.1080/13696998.2025.2452054
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psoriatic Foot Involvement is the Most Significant Contributor to the Inconsistency Between PASI and DLQI: A Retrospective Study from China
Yang J, Hu K, Li X, Hu J, Tan M, Zhang M, Chen J, Kuang Y
Clinical, Cosmetic and Investigational Dermatology 2023, 16:443-451
Published Date: 15 February 2023
An Unexpected Finding: Treatment History Associated with the Quality of Life in Chinese Patients with Port-Wine Stains
Zhao Q, Liu L, Li X, Yang L, Jiang X
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1969-1975
Published Date: 27 July 2023
Psoriasis: Prevalence, Clinical Variants and Quality of Life, Among Patients Attending the Skin Clinic at Mbarara Regional Referral Hospital, Uganda
Lubwama H, Mulyowa GK, Mirembe SK, Katungi TJ, Male M
Psoriasis: Targets and Therapy 2025, 15:117-126
Published Date: 2 April 2025
Predictors of Quality of Life in Psoriasis Patients: Insights from a Cross-Sectional Study
Walniczek P, Ponikowska M, Kolarczyk EB, Spaleniak P, Mróz-Kijowska K, Czapla M, Uchmanowicz I
Psoriasis: Targets and Therapy 2025, 15:163-174
Published Date: 24 April 2025
Challenges Psoriasis and Its Impact on Quality of Life: Challenges in Treatment and Management
Ponikowska M, Vellone E, Czapla M, Uchmanowicz I
Psoriasis: Targets and Therapy 2025, 15:175-183
Published Date: 1 May 2025