Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
An Unexpected Finding: Treatment History Associated with the Quality of Life in Chinese Patients with Port-Wine Stains
Authors Zhao Q, Liu L ![]() , Li X
, Li X ![]() , Yang L
, Yang L ![]() , Jiang X
, Jiang X ![]()
Received 30 May 2023
Accepted for publication 18 July 2023
Published 27 July 2023 Volume 2023:16 Pages 1969—1975
DOI https://doi.org/10.2147/CCID.S421296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Qian Zhao,1– 3,* Lian Liu,1,3,* Xiaoxue Li,1,3 Lihua Yang,1,3 Xian Jiang1,3
1Department of Dermatology, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China; 2Department of Medical Cosmetology, Chengdu Second People’s Hospital, Chengdu, Sichuan, 610021, People’s Republic of China; 3Laboratory of Dermatology, Clinical Institute of Inflammation and Immunology (CIII), Frontiers Science Center for Disease-Related Molecular Network, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xian Jiang, Department of Dermatology, West China Hospital, Sichuan University, 37 Guoxue Alley, Wuhou District, Chengdu, Sichuan, 610041, People’s Republic of China, Email [email protected]
Background: Port-wine stains (PWS) are predominantly located on the face and neck. Hence, PWS affect not only aesthetic appearance but may also cause psychological distress. However, very few studies have researched on the quality of life (QoL) in Chinese patients with PWS.
Aim: To evaluate QoL in patients with PWS.
Methods and Materials: Skindex-29 and Dermatology Life Quality Index (DLQI) were used to investigate the QoL of the patients with PWS and healthy controls.
Results: In total, 198 adults with PWS and 200 healthy controls were included. The scores of symptomatic, emotional and functional dimensions of Skindex-29 in the observational group were significantly higher as compared with the control group (P< 0.05). Female gender, lesion location and the treatment history (such as pulsed dye laser or photodynamic therapy) had a negative impact on the scores (emotional and functional dimensions) of the patients with PWS. The median DLQI score was 3 points in the observational group and 0 points in the control group (P< 0.05), and QoL of patients who had a history of previous treatments was diminished.
Conclusion: The QoL of patients with PWS is impaired. Patients’ QoL is negatively influenced by female gender, lesion location and treatment history. The Skindex-29 scale seems to be more applicable to the study of QoL of patients with PWS.
Keywords: port-wine stains, quality of life, Skindex-29, dermatology life quality index
Introduction
Port-wine stains (PWS) are congenital vascular malformations characterized by progressive dilatation of capillary and postcapillary venules in the skin, which affects 0.3% to 0.5% of the population.1 They typically manifest as pink to reddish, irregularly shaped and sized patches, which are mainly located on the face and/or neck. In some patients, the lesions gradually developed with increased thickness, and darker color over time. Thus, on the one hand, it will add difficulty to the treatment of PWS and on the other hand, it will result in further disfigurement.2
PWS affect not only aesthetic appearance but may also cause psychological distress to the patients. Over the last few decades, a dozen of articles have reported the psychological disabilities among patients with PWS.2–4 The tools used to assess quality of life include the Dermatology Life Quality Index (DLQI),5 Skindex-29 scale,6 Short Form-36 Health Survey (SF-36),7 Family Dermatology Life Quality Index and Children’s Dermatology Life Quality,8 etc. However, very few studies have researched on the quality of life (QoL) in Chinese patients with PWS. Among them, the Skindex-29 scale and DLQI have been widely applied to evaluate the patients’ quality of life (QoL) in dermatology.9,10
The Skindex-29 scale is a reliable, valid and convenient instrument to measure patients’ QoL. It consists of 30 items split into three subscales: symptoms, emotions, and functioning, which concerns respondents’ feelings over the past 4 weeks.11 The DLQI is a validated 10-item questionnaire for the QoL evaluation and follow-up of patients with dermatological diseases, regarding personal relationships, leisure, daily activities, and treatment.12 The DLQI is more centered on daily activities while Skindex-29 also measures emotions. Although the Skindex-29 scale and DLQI were utilized to measure QoL of PWS, there have been no studies combining Skindex-29 and DLQI to evaluate QoL of patients with PWS in China. Therefore, we used the Skindex-29 scale and DLQI to evaluate the QoL of patients with PWS, and to explore the influencing factors.
Materials and Methods
Participants
Patients with PWS in our outpatient department were selected as the observational group during January 2019 and August 2020. Inclusion criteria were as follows: (1) The diagnosis of PWS was confirmed by 2 dermatologists; (2) Age ≥16 years old; (3) The patients could complete the questionnaire independently. Exclusion criteria were as follows: (1) Those patients with other skin diseases such as acne, rosacea, atopic dermatitis, etc; (2) Those patients with syndromes such as Sturge-Weber syndrome, Klippel Trenaunay syndrome, phakomatosis pigmentovascularis, etc; (3) Patients suffering from serious neurological and psychiatric diseases. The control group consisted of healthy individuals who underwent physical examination in the health management center of the same hospital within the same period. Some participants were treated with pulsed dye laser (PDL) or photodynamic therapy (PDT). And the total duration of the treatments for most of the patients was nearly 1 year. Each participants provided written informed consent, and the patients under 18 signed informed consent by their legal guardians.
Study Design
This was a descriptive observational case-control study and had been approved and reviewed by the Ethics Committee of West China Hospital. The study complies with the Helsinki declaration. The Clinical Trial Registration Number was ChiCTR1900028550. The QoL of patients and healthy individuals was investigated by the Skindex-29 scale and the DLQI. If the patients had some difficulties in understanding the questionnaire, the investigator provided an explanation.
The Skindex-29 scale is divided into 3 subdomains, which include symptomatic, emotional and functional dimensions.13 There are five alternative answers for each question, and the answers for each item (except for item 18) were converted into a linear score of 0–100 (never = 0, rarely = 25, sometimes = 50, often = 75, always = 100). The final score is the average score of all the answers. The higher the score on scale, the poorer the patients’ QoL.
The DLQI consists of 10 questions relating to symptoms and feelings, daily activities, leisure, work or study, personal relationships, and treatment history.14 Each question has 3 to 5 optional answers, and each question was scored from 0 to 3 points. The total score ranged from 0 to 30, and a higher score indicates a worse QoL. These scores are defined as follows: 0 to 1 = no impact; 2 to 5 = mild impact; 6 to 10 = moderate impact; 11 to 20 = severe impact; 21 to 30 = extremely severe impact.
Statistical Analysis
Microsoft Excel 2016 was used for data management, and Stata 15.0 software was applied for statistical analysis. Quantitative data were expressed as mean ± standard deviation (SD) or median (P25, P75), while enumeration data were expressed as case number and percentage. Rank sum test was used for grade data. Multiple linear regression analysis was used to explore the influencing factors, and the regression coefficient (β) and its standard error (SE) were used to express the factors. The test level α=0.05 (bilateral).
Results
Patient Characteristics
In total, 198 patients with PWS (age range: 16 to 61 years, mean age: 27.2 ± 8.63 years old; 73 male patients and 125 female patients) and 200 healthy controls (age range:16 to 58 years, mean age: 28.6 ± 9.21 years old; 73 male patients and 127 female patients) were included in the study. There was no statistically significant difference in age and gender between the two groups (P >0.05). As for the location, color and thickness of the lesions, the patients were divided into different groups (Table 1). In addition, patients were grouped according to whether they had received treatment or not.
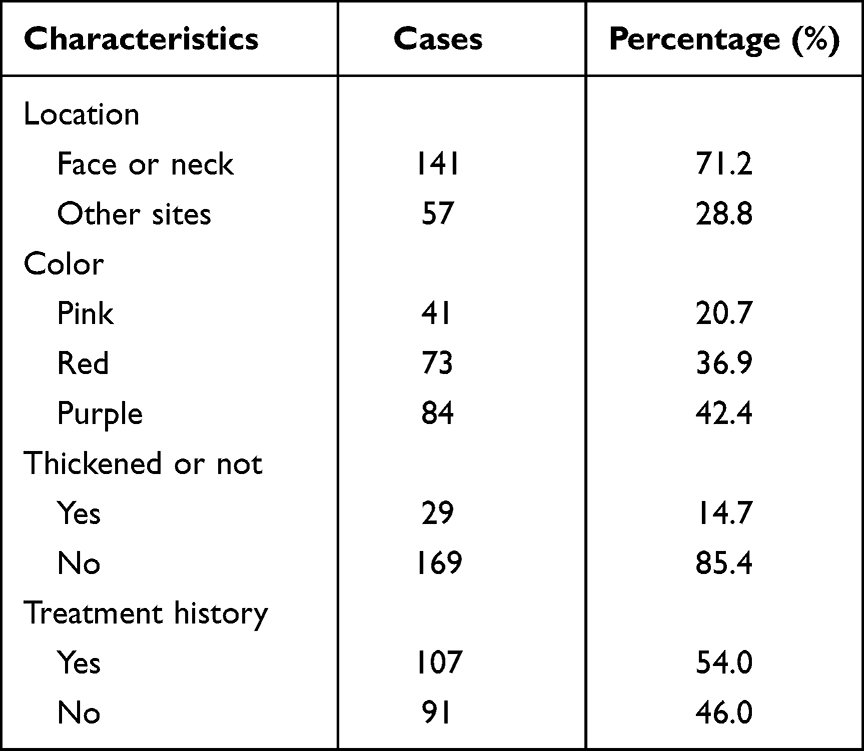 |
Table 1 Clinical Characteristics of Patients with PWS |
Skindex-29 Score in Patients with PWS and Healthy Controls
The median total score was 23.2 (8.62, 34.5) in the observational group, and 1.72 (0.0, 6.9) in the control group (P<0.001). The score of symptom dimension, emotion dimension and function dimension of Skindex-29 scale in the patient group were all higher than those in the control group (P<0.05) (Table 2). Thus, it was implied that the presence of PWS had a negative influence on QoL, especially from an emotional dimension.
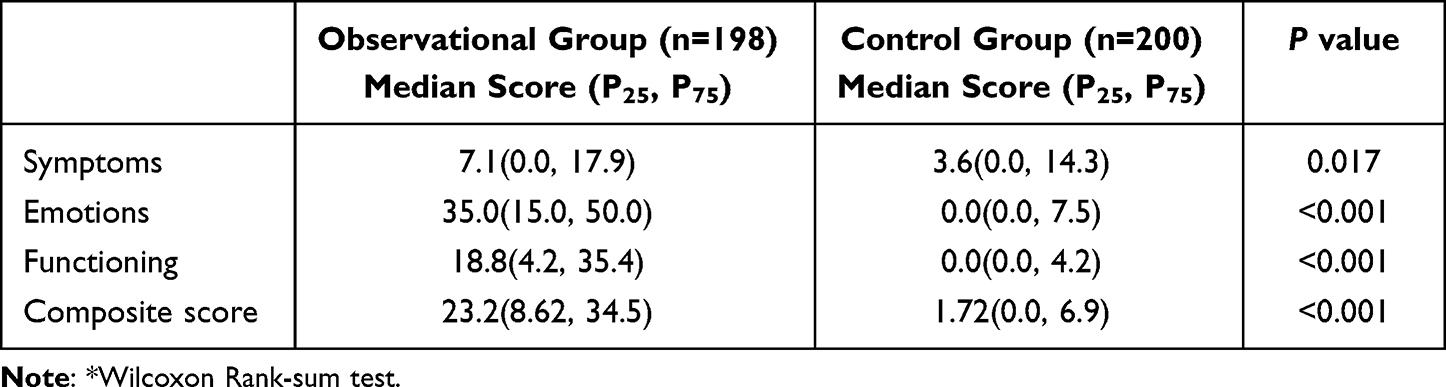 |
Table 2 Comparison of Skindex-29 Scale Scores Between the Two Groups* (Score) |
Multiple Linear Regression Analysis of Skindex-29 Scores
Multiple linear regression analysis of demographic measures in patients and healthy individuals are presented in Table 3. All of the scores (emotional, symptomatic, functional dimension and composite scores) in the observational group were all higher than the control group (P<0.05). Meanwhile, the scores of females were also all higher than those of males (P<0.05).
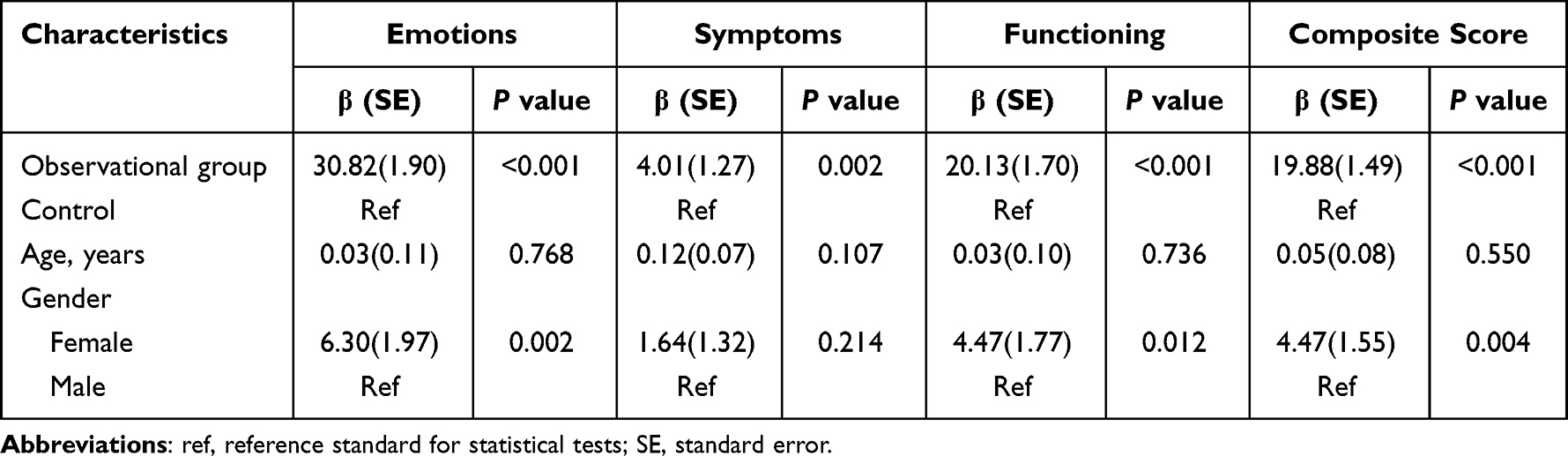 |
Table 3 Multiple Linear Regression Analysis of Skindex-29 Scores and Demographic Characteristics in the Two Groups |
Multiple linear regression analysis of clinical measures in patients are presented in Table 4. Females had more emotional (P<0.05) and functional (P<0.05) impairment in relation to their PWS than males. Meanwhile, the patients whose lesions were located on the face and neck had greater emotional (P<0.05) and functional (P<0.05) impairment than those whose lesions were on other sites. In the symptomatic dimension, the purple type had lower scores than those with pink lesions (P<0.05). Those who had a treatment history had higher scores on the emotion scale (P<0.05) and function scale (P<0.001). In addition, females (P<0.05), patients with facial and neck lesions (P<0.05) and those who had a treatment history (P<0.05) were associated with higher composite scores.
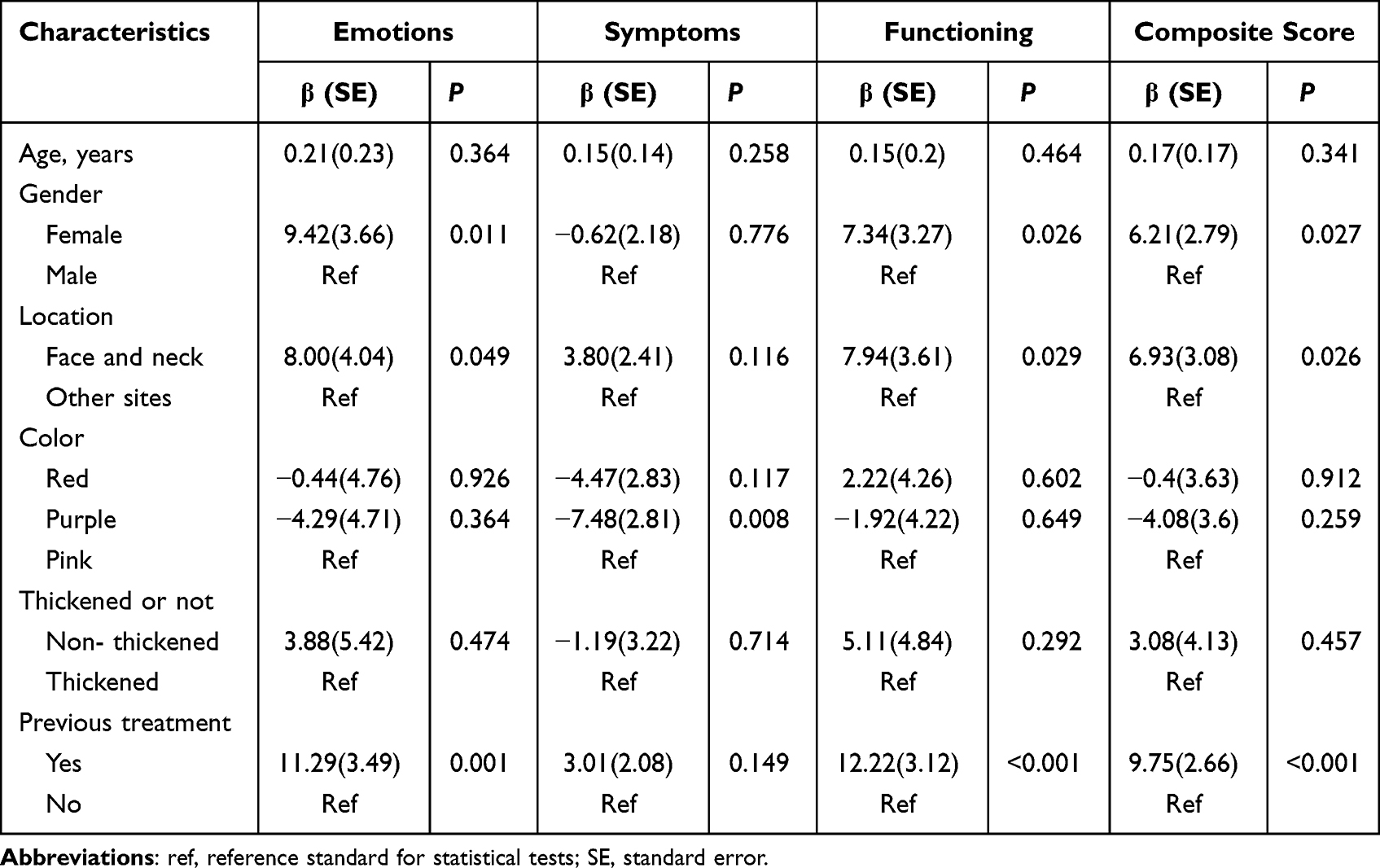 |
Table 4 Multiple Linear Regression Analysis of Skindex-29 Scores and Related Factors in the Observational Group |
DLQI Scores in in Patients with PWS and Healthy Controls
The DLQI scores of PWS patients and healthy controls ranged from 0 to 25 and from 0 to 10, respectively. The DLQI scores of PWS patients were mainly distributed from 0 to 1 (34.3%) and from 2 to 5 (33.8%). The median DLQI score was 3 points and 0 points in the observational and control groups, respectively. In conclusion, it suggested that PWS had a mild effect on QoL. The difference in DLQI scores between the two groups was statistically significant (P<0.001) (Table 5). Multiple linear regression analysis of DLQI scores and clinical characteristics in the observational group are shown in Table 6. It showed that after controlling for other variables, the DLQI scores of patients with PWS were affected by treatment history, and those who had received treatment scored higher than those who had not (P<0.05).
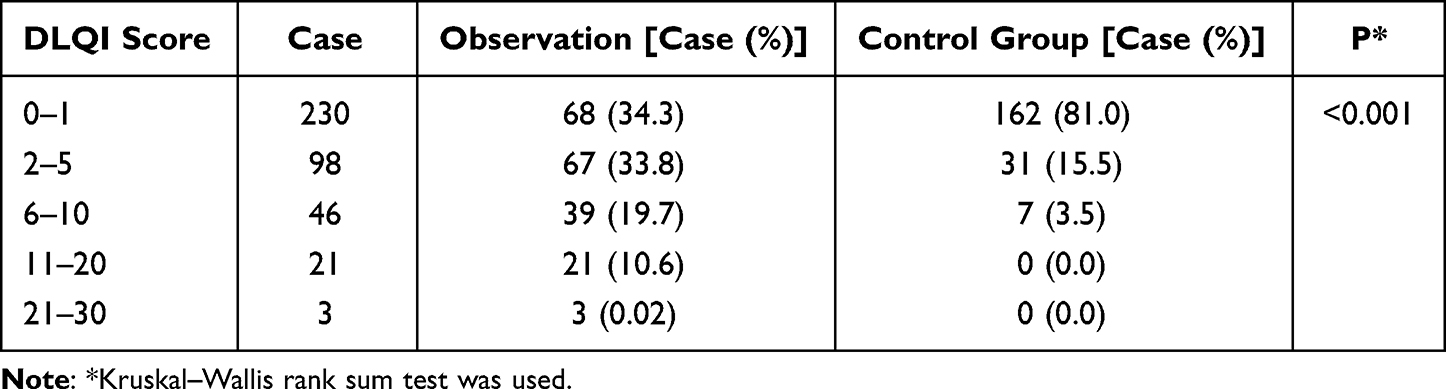 |
Table 5 Comparison of DLQI Scores Between the Two Groups |
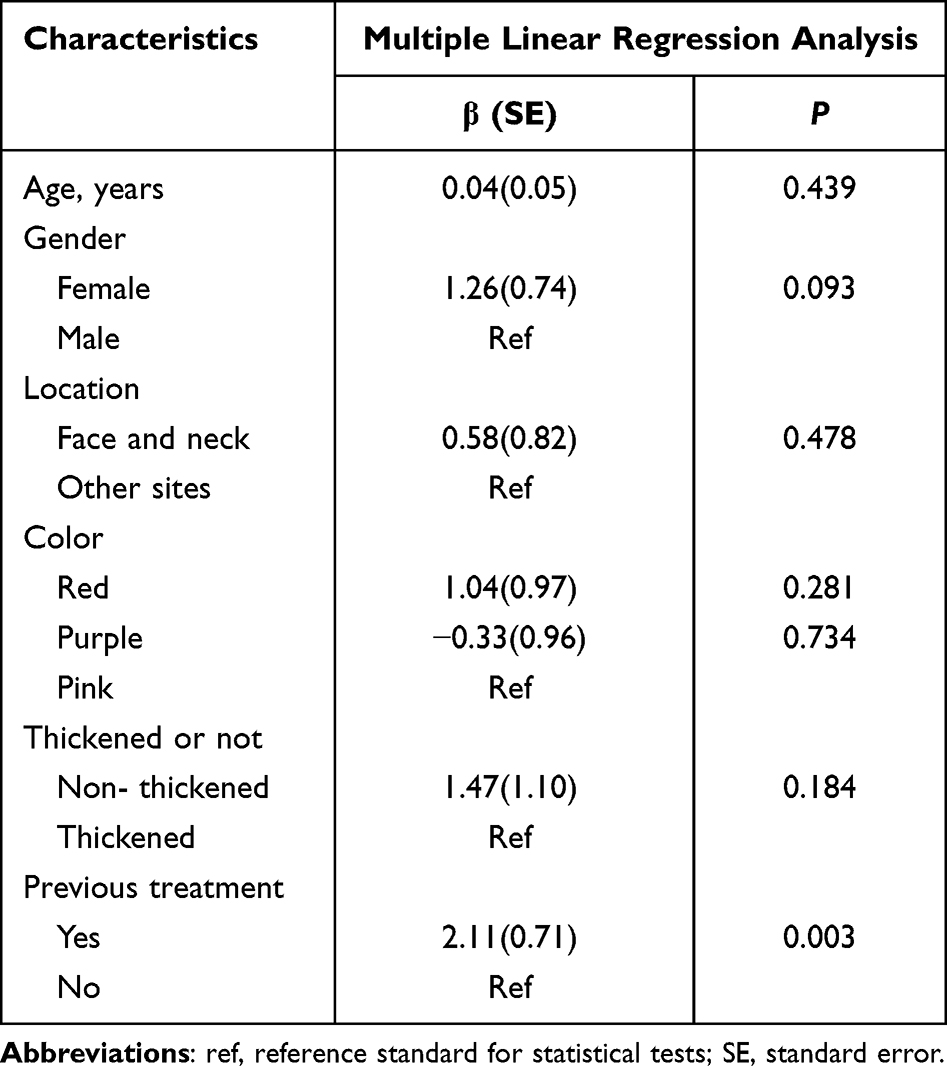 |
Table 6 Linear Regression Analysis of DLQI Scores and Related Factors in the Observational Group |
Discussion
The scores of symptomatic, emotional and functional dimensions of Skindex-29 in the observational group were significantly higher as compared with the control group. Of these, patients were most severely impaired on emotional dimension (35.0). Our finding was similar with the result of a previous study that the emotion domain was most significantly influenced.6 The median DLQI score was 3 points in the observational group and 0 points in the control group. Meanwhile, in another study, the median DLQI score was 5 points.5 These findings from the DLQI revealed the QoL of patients were mildly impacted. In conclusion, both of the subscales showed that the QoL of patients with PWS was indeed impaired as compared with the control group.
Among the Skindex-29 scale, females reported significantly higher scores from emotional and functional dimensions, especially the emotional section in this study. In reality, similar findings were reported in other dermatological conditions such as acne,15 psoriasis,16 keratinocyte carcinomas17 and vitiligo.18 In addition, Hagen et al also found that females had more emotional and symptomatic impairment in relation to PWS than males.6 This was probably due to the fact that females had greater attention to cosmetic defects and aesthetic orientation as expected. It should be noted that the sex differences in impact on QoL of patients with PWS should be taken into account by clinicians.
Approximately two-thirds of PWS occur on the face. Moreover, some lesions gradually thicken and darken with age, and the lesions located on the face are difficult to cover through clothing or make-up.8 These factors would spontaneously lead to social embarrassment and self-stigma. In our study, among the Skindex-29 scale, the patients whose lesions were located on the face and neck had greater emotional and functional impairment than those on other sites.6 Besides, Hagen et al revealed that QoL in patients with facial PWS was impacted.8 Hence, early management and treatment are critical for these patients.
An unexpected finding was observed in the present study. The data from the Skindex-29 scale and the DLQI revealed that previous treatments had a negative impact on the QoL of patients with PWS. According to these results, there are still numerous problems associated with the treatment of PWS. The reasons for the finding might be as follows: (1) although pulsed dye laser (PDL) is still the gold standard for the treatment of PWS, complete clearance is achieved in less than 10% of patients by PDL;19 (2) after PDL treatment, the recurrence rate of these lesions between 16% and 50% in patients, further aggravating their distress;20 (3) whether laser or photodynamic therapy, multiple treatment sessions are usually required and it would increase their financial burden; (4) those patients who were cured would not return (selection bias). A previous study has demonstrated that a minority of patients was dissatisfied with PDL therapy, and our study also showed that previous treatments had a negative impact on the QoL of patients with PWS.21 In conclusion, with these therapeutic limitations, the patients that experienced treatments were negatively impacted in their QoL. Therefore, early prevention and selecting the correct treatments of PWS are still important. New and effective treatments are urgently needed.
In our study, the Skindex-29 scale and the DLQI were utilized to evaluate the QoL of patients with PWS. We found that for females, PWS on the face and neck, and treatment history influenced the QoL from the Skindex-29 scale. However, we just found that treatment history influenced the QoL on the DLQI, and prior research has pointed out that female gender and thickened type were the main factors influencing the DLQI scores.5 Therefore, we speculate that the Skindex-29 scale might be more sensitive and accurate than the DLQI in this study. Compared with the DLQI, the Skindex-29 scale could detect significant differences among the dimensions of symptoms, emotion and function, suggesting that the Skindex-29 scale has a stronger detection ability than the DLQI. Previous studies have reported similar results.22 Although the DLQI is more convenient than the Skindex-29 scale, Skindex-29 might be more applicable to the study for the QoL in patients with PWS.
Our study aimed at the patients over 16 years old. Since PWS usually presents at birth and does not regress spontaneously, it is necessary to investigate the quality of life of patients with PWS and their families at all ages in the future. Besides, more long-term studies will be helpful in assessing the impact of PDL or PDT therapy on patients’ QoL.
The present study still has some limitations. First, it is a single center study with a limited sample size (selection bias). Second, sufficient details about previous treatments were not included. Therefore, more prospective studies are needed.
Conclusion
In conclusion, our study emphasizes that the QoL of patients with PWS is impaired. And patients’ QoL is negatively affected by female gender, lesion location and treatment history. Female patients with PWS who had treatment history should be taken into consideration by clinicians in the management and appropriate support should be provided.
Data Sharing Statement
The corresponding author will share the study protocol and all data collected with this study upon reasonable request for one year after publication of this manuscript.
Acknowledgments
This study was supported by grants from National Natural Science Foundation of China (Grant No. 82003373 and 82073473), the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYJC21036).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jacobs AH, Walton RG. The incidence of birthmarks in the neonate. Pediatrics. 1976;58(2):218–222. doi:10.1542/peds.58.2.218
2. Lanigan SW, Cotterill JA. Psychological disabilities amongst patients with port wine stains. Br J Dermatol. 1989;121(2):209–215. doi:10.1111/j.1365-2133.1989.tb01800.x
3. van der Horst CM, de Borgie CA, Knopper JL, et al. Psychosocial adjustment of children and adults with port wine stains. Br J Plast Surg. 1997;50(6):463–467. doi:10.1016/S0007-1226(97)90335-0
4. Wanitphakdeedecha R, JNC N, Yan C, et al. Quality of life and psychological effects of port-wine stain: a review of literature. Clin Cosmet Investig Dermatol. 2021;14:681–690. doi:10.2147/CCID.S315804
5. Wang J, Zhu YY, Wang ZY, et al. Analysis of quality of life and influencing factors in 197 Chinese patients with port-wine stains. Medicine. 2017;96(51):e9446. doi:10.1097/MD.0000000000009446
6. Hagen SL, Grey KR, Korta DZ, et al. Quality of life in adults with facial port-wine stains. J Am Acad Dermatol. 2017;76(4):695–702. doi:10.1016/j.jaad.2016.10.039
7. Schiffner R, Brunnberg S, Hohenleutner U, et al. Willingness to pay and time trade-off: useful utility indicators for the assessment of quality of life and patient satisfaction in patients with port wine stains. Br J Dermatol. 2002;146(3):440–447. doi:10.1046/j.1365-2133.2002.04613.x
8. Neumann R, Leonhartsberger H, Knobler R, et al. Immunohistochemistry of port-wine stains and normal skin with endothelium-specific antibodies PAL-E, anti-ICAM-1, anti-ELAM-1, and anti-factor VIIIrAg. Arch Dermatol. 1994;130(7):879–883. doi:10.1001/archderm.1994.01690070073011
9. Joseph A, Prasad S, Hynan LS, et al. Differences in quality of life in patients with cutaneous lupus erythematosus with varying income levels. Lupus. 2021;30(6):972–980. doi:10.1177/0961203321999724
10. Bregnhoj A, Thuesen KKH, Emmanuel T, et al. HSP90 inhibitor RGRN-305 for oral treatment of plaque type psoriasis: efficacy, safety and biomarker results in an open-label proof-of-concept study. Br J Dermatol. 2021;186(5):861–874.
11. Vasquez D, Aguirre DC, Sanclemente G. Construct validity and responsiveness of the Colombian version of Skindex-29. Br J Dermatol. 2019;181(4):770–777. doi:10.1111/bjd.17742
12. Xiao Y, Huang X, Jing D, et al. Assessment of the Dermatology Life Quality Index (DLQI) in a homogeneous population under lifetime arsenic exposure. Qual Life Res. 2018;27(12):3209–3215. doi:10.1007/s11136-018-1969-2
13. Chren MM. The Skindex instruments to measure the effects of skin disease on quality of life. Dermatol Clin. 2012;30(2):231–+. doi:10.1016/j.det.2011.11.003
14. Lewis V, Finlay AY. 10 years experience of the Dermatology Life Quality Index (DLQI). J Investig Dermatol Symp Proc. 2004;9(2):169–180. doi:10.1111/j.1087-0024.2004.09113.x
15. Berg M, Lindberg M. Possible gender differences in the quality of life and choice of therapy in acne. J Eur Acad Dermatol Venereol. 2011;25(8):969–972. doi:10.1111/j.1468-3083.2010.03907.x
16. Sampogna F, Chren MM, Melchi CF, et al. Age, gender, quality of life and psychological distress in patients hospitalized with psoriasis. Br J Dermatol. 2006;154(2):325–331. doi:10.1111/j.1365-2133.2005.06909.x
17. Sampogna F, Paradisi A, Iemboli ML, et al. Sex differences in health-related quality of life in patients with keratinocyte carcinomas. Acta Derm Venereol. 2021;101(4):adv00439. doi:10.2340/00015555-3736
18. Sawant NS, Vanjari NA, Khopkar U. Gender differences in depression, coping, stigma, and quality of life in patients of vitiligo. Dermatol Res Pract. 2019;2019:6879412. doi:10.1155/2019/6879412
19. Lanigan SW. Port-wine stains unresponsive to pulsed dye laser: explanations and solutions. Br J Dermatol. 1998;139(2):173–177. doi:10.1046/j.1365-2133.1998.02351.x
20. Michel S, Landthaler M, Hohenleutner U. Recurrence of port-wine stains after treatment with the flashlamp-pumped pulsed dye laser. Br J Dermatol. 2000;143(6):1230–1234. doi:10.1046/j.1365-2133.2000.03893.x
21. Hansen K, Kreiter CD, Rosenbaum M, et al. Long-term psychological impact and perceived efficacy of pulsed-dye laser therapy for patients with port-wine stains. Dermatol Surg. 2003;29(1):49–55. doi:10.1046/j.1524-4725.2003.29010.x
22. Fernandez-Penas P, Jones-Caballero M, Espallardo O, et al. Comparison of Skindex-29, dermatology life quality index, psoriasis disability index and medical outcome study short form 36 in patients with mild to severe psoriasis. Br J Dermatol. 2012;166(4):884–887. doi:10.1111/j.1365-2133.2012.10806.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Beyond Skin Clearance: Personalized Strategies for DLQI Improvement in Psoriasis -Insights From a Shanghai Prospective Cohort
Ma X, Xu Q, Kuai L, Shen F, Duan Z, Gao X, Zhang R, Wang R
Psoriasis: Targets and Therapy 2025, 15:373-387
Published Date: 13 August 2025