Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Association of Pegylated Liposomal Doxorubicin with Improved Overall Survival Compared with Epirubicin in Early-Stage Breast Cancer: A Population Based Study from Taiwan
Authors Chen YC ![]() , Cheng MC, Chen PH
, Cheng MC, Chen PH ![]() , Chung CH
, Chung CH ![]() , Chien WC, Dai MS, Chen JH, Huang TC
, Chien WC, Dai MS, Chen JH, Huang TC
Received 12 January 2026
Accepted for publication 28 April 2026
Published 3 June 2026 Volume 2026:18 595563
DOI https://doi.org/10.2147/BCTT.S595563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Yang-Chuan Chen,1 Min-Chi Cheng,2,3 Po-Huang Chen,2,3 Chi-Hsiang Chung,4– 6 Wu-Chien Chien,4– 8 Ming-Shen Dai,2,3 Jia-Hong Chen,2,3 Tzu-Chuan Huang2,3
1Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan; 2Division of Hematology and Oncology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan; 3Department of Oncology, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan; 4Department of Medical Research, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan; 5Graduate Institute of Public Health, College of Public Health, National Defense Medical University, Taipei, Taiwan; 6Taiwanese Injury Prevention and Safety Promotion Association (TIPSPA), Taipei, Taiwan; 7Graduate Institute of Life Sciences, College of Biomedical Sciences, National Defense Medical University, Taipei, Taiwan; 8Graduate Institute of Medical Sciences, College of Medicine, National Defense Medical University, Taipei, Taiwan
Correspondence: Tzu-Chuan Huang, Division of Hematology and Oncology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical University, 3F, No. 325, Section 2, Cheng-Kung Road, Neihu 114, Taipei, Taiwan, Tel +886-2-87923311, Email [email protected]
Purpose: Anthracycline-based regimens are a cornerstone of adjuvant therapy for early-stage breast cancer but are limited by cumulative cardiotoxicity. This study compared the effectiveness and cardiotoxicity of pegylated liposomal doxorubicin (Lipo-Dox) and epirubicin in women with early-stage, HER2-negative breast cancer using nationwide real-world data from Taiwan.
Patients and Methods: This population-based retrospective cohort study used Taiwan’s National Health Insurance Research Database to identify adult women with stage I–III, HER2-negative breast cancer treated with adjuvant anthracycline-based chemotherapy between 2006 and 2018. Propensity score matching (1:1) was performed to balance baseline characteristics, resulting in 1050 matched patients with a median follow-up of 6.05 years. Overall survival (OS), disease-free survival (DFS), and cardiotoxicity were analyzed using Cox proportional hazards models and Kaplan–Meier methods.
Results: Compared with epirubicin, Lipo-Dox was associated with significantly improved overall survival (adjusted hazard ratio 0.754, 95% CI 0.632– 0.899; P < 0.001). Survival benefits were consistent across 3-year, 5-year, and full follow-up analyses and demonstrated a dose-dependent relationship. Kaplan–Meier curves confirmed superior overall survival in the Lipo-Dox group (log-rank P < 0.001). No significant differences were observed between the two groups in disease-free survival or clinically diagnosed cardiac events.
Conclusion: In this nationwide propensity score–matched cohort, adjuvant Lipo-Dox was associated with sustained overall survival benefits without increased cardiotoxic risk compared with epirubicin. Lipo-Dox may represent a favorable anthracycline alternative, particularly for patients with cardiovascular comorbidities or elevated cardiotoxicity risk.
Keywords: breast cancer, pegylated liposomal doxorubicin, epirubicin, overall survival, cardiotoxicity
Introduction
Breast cancer remains the most frequently diagnosed malignancy among women worldwide, with an estimated 2.3 million new cases and 670,000 deaths in 2022.1 Notably, the study by Sung et al found that with dietary Westernization in younger generations, breast cancer incidence in recent Asian cohorts is converging with and even surpassing the historically high rates in the United States.2 While early-stage breast cancer demonstrates excellent outcomes with five-year survival rates exceeding 90% in countries with established screening programs and multidisciplinary care, optimizing systemic therapy—including chemotherapy, targeted agents, antibody–drug conjugates, and immunotherapies—further improves survival but adds treatment-related toxicities, making it essential to maximize cure rates while minimizing long-term morbidity.3
Anthracycline-based regimens have served as the therapeutic backbone for adjuvant and neoadjuvant breast cancer treatment for over three decades. Current evidence-based guidelines recommend combinations such as doxorubicin or epirubicin with cyclophosphamide followed by taxanes, which have consistently demonstrated significant improvements in disease-free survival and overall survival across multiple randomized controlled trials.4,5
However, conventional anthracyclines carry substantial risks of cumulative dose-dependent cardiotoxicity, presenting challenges in older patients, those with preexisting cardiovascular disease, or patients receiving concurrent trastuzumab-based therapy or thoracic radiotherapy.6–8 While epirubicin demonstrates a more favorable cardiac safety profile than doxorubicin, cardiotoxicity remains a notable concern, requiring careful cardiac monitoring and potentially compromising treatment delivery.9
Pegylated liposomal doxorubicin represents a significant pharmacological advancement designed to lessen doxorubicin-induced adverse effects.10,11 Through encapsulation of doxorubicin within polyethylene glycol-coated liposomes, this formulation exploits the enhanced permeability and retention effect characteristic of tumor vasculature, enabling preferential drug accumulation within malignant tissues while substantially reducing exposure to cardiac and bone marrow compartments.12 Extensive clinical experience has demonstrated that pegylated liposomal doxorubicin maintains antitumor efficacy comparable to conventional anthracyclines while markedly reducing cardiotoxicity and myelosuppression.13–17
The evolving recognition of pegylated liposomal doxorubicin’s favorable risk-benefit profile has influenced contemporary clinical practice guidelines.4,5 The 2022 European Society of Cardiology cardio-oncology guidelines, developed collaboratively with the European Hematology Association and European Society for Radio-therapy and Oncology, now explicitly recommend pegylated liposomal doxorubicin as the preferred anthracycline formulation for patients with established cardiovascular disease or elevated baseline cardiovascular risk.7,18
However, most comparative studies have enrolled predominantly Western populations, creating a knowledge gap for Asian patients. Zhang et al recently demonstrated higher anthracycline-related cardiotoxicity in Asian patients compared to other ethnic groups, with disparities persisting after multivariable adjustment.19 This suggests genetic or biological factors may influence treatment outcomes across ethnicities. These ethnic disparities may be partly attributable to pharmacogenomic differences, including genetic polymorphisms in drug-metabolizing enzymes (egcarbonyl reductases, UGT isoforms) and variations in cardiac susceptibility genes, which could differentially influence anthracycline pharmacokinetics and cardiotoxic risk across populations.
Beyond survival outcomes, real-world treatment selection also depends on tolerability, treatment completion rates, and quality of life considerations, which are particularly relevant when comparing anthracycline formulations in patients with significant comorbidities. Given these ethnic variations and Taiwan’s comprehensive healthcare system, region-specific data are crucial for optimizing treatment in Asian populations. However, comparative research on anthracycline formulations in Taiwanese breast cancer patients remains limited. We therefore conducted a population-based cohort study using Taiwan’s National Health Insurance Research Database to compare real-world effectiveness and safety of pegylated liposomal doxorubicin versus epirubicin in early-stage breast cancer, providing evidence to guide chemotherapy selection in Asian healthcare systems.
Materials and Methods
Study Design and Data Source
This population-based retrospective cohort study was designed to evaluate the comparative real-world effectiveness and safety of adjuvant pegylated liposomal doxorubicin-based versus epirubicin-based chemotherapy regimens in patients with early-stage breast cancer. The investigation utilized Taiwan’s National Health Insurance Research Database, specifically the Longitudinal Health Insurance Database, which contains comprehensive de-identified healthcare claims data encompassing over 99% of Taiwan’s population.
The study cohort included patients diagnosed between January 1, 2006, and December 31, 2018, with longitudinal follow-up extending through December 31, 2018. Patient observation commenced at treatment initiation and continued until death, withdrawal from the National Health Insurance system, or occurrence of predefined study endpoints. The investigation received approval from the Institutional Review Board of Tri-Service General Hospital, with informed consent requirements waived given the retrospective design and utilization of anonymized administrative data.
Study Population
The study population comprised women aged 20 years or older with newly diagnosed stage I–III breast cancer, classified according to International Classification of Diseases coding systems and linked with Taiwan Cancer Registry data. Eligible patients underwent mastectomy and initiated their first adjuvant chemotherapy regimen within three months following surgical intervention.
Patients were excluded from analysis if they demonstrated evidence of local recurrence or distant metastatic disease at adjuvant chemotherapy initiation, had prior diagnoses of melanoma or other malignancies within five years preceding breast cancer diagnosis (excluding cervical carcinoma in situ), experienced incomplete tracking or loss to follow-up within the database system, or possessed missing or corrupted medical record data that precluded adequate clinical assessment.
Additionally, patients with HER2-positive breast cancer were excluded to eliminate the confounding effect of HER2-targeted therapy on treatment outcomes. HER2 status was determined through linkage with Taiwan Cancer Registry data, which records HER2 positivity based on standard pathological assessment according to contemporary guidelines during the study period.
Treatment Group Definitions and Exposure Classification
A critical methodological consideration involves the indirect identification strategy necessitated by reimbursement policies during the study period. Pegylated liposomal doxorubicin was not directly covered by Taiwan’s National Health Insurance for adjuvant breast cancer treatment, requiring development of a proxy identification approach.
Treatment group classification utilized the following methodology based on sequential chemotherapy regimens:
Lipo-Dox-Based Group (Presumed Pegylated Liposomal Doxorubicin-Based)
This group comprised patients receiving sequential adjuvant chemotherapy with cyclophosphamide (C) followed by taxanes (T), without any corresponding insurance claims for epirubicin or conventional doxorubicin. To specifically distinguish this regimen from concurrent therapies like the TC protocol, eligibility was restricted to patients who initiated taxane treatment only after the completion of their cyclophosphamide course. This sequential C-T treatment pattern served as a surrogate marker for a Lipo-Dox-based regimen. The strategy is based on the rationale that pegylated liposomal doxorubicin was self-funded (and thus absent from claims data), while an anthracycline was the standard of care during the study period. Therefore, the absence of a billed anthracycline in this specific regimen was presumed to indicate out-of-pocket use of pegylated liposomal doxorubicin.
Epirubicin-Based Group (Epirubicin-Based Control)
This group consisted of patients who received a standard sequential regimen of epirubicin and cyclophosphamide, followed by taxanes. Consistent with the definition of sequential therapy used for the study cohort, patients initiated taxanes only after completing the epirubicin-cyclophosphamide phase of treatment.
The sequential treatment approach was defined as taxanes initiation occurring after documented completion of the cyclophosphamide-containing phase, typically with a treatment interval of 2–4 weeks between phases as per standard clinical protocols during the study period. Only patients meeting this sequential criteria were included in the analysis.
Propensity Score Matching and Bias Reduction
To address inherent selection bias and confounding variables characteristic of observational studies, rigorous one-to-one propensity score matching was implemented using logistic regression modeling. The propensity score estimation incorporated the following covariates: patient age at diagnosis, cancer stage, pre-existing comorbidities, and the inclusion date (ie, treatment initiation date).
Matching employed a nearest-neighbor algorithm with caliper width specification of 0.2 times the standard deviation of the logit-transformed propensity score. Post-matching covariate balance assessment utilized standardized mean differences, with values below 0.1 considered indicative of adequate balance between treatment groups.
Baseline Characteristics and Covariate Definitions
Comprehensive baseline characteristics were systematically assessed at or before the index treatment date. Patient age was analyzed as a continuous variable measured at breast cancer diagnosis. Cancer staging utilized the American Joint Committee on Cancer seventh and eighth edition criteria, categorizing patients into stages I, II, or III. Socioeconomic status was approximated through monthly income stratification based on insurance premium levels: less than NT$18,000, NT$18,000–34,999, and NT$35,000 or greater. Taiwan’s National Health Insurance is a mandatory social insurance program with income-based premiums, determined by the insured person’s occupation, income, and insured amount.
Healthcare delivery context was characterized by hospital level classification encompassing medical centers, regional hospitals, and local hospitals. Pre-existing comorbidity identification utilized International Classification of Diseases coding, encompassing diabetes mellitus, hypertension, depression, chronic kidney disease, congestive heart failure, chronic obstructive pulmonary disease, and hyperlipidemia, with specific diagnostic codes detailed in Supplement S1.
Outcome Definitions and Follow-Up Methodology
The clinical endpoints for this study were defined as follows:
- Primary Outcome: The primary endpoint was overall survival (OS), defined as the time from treatment initiation to death from any cause. Mortality data were ascertained through linkage with Taiwan’s National Death Registry.
- Secondary Outcomes: Secondary endpoints included:
- Disease-Free Survival (DFS): Defined as the time from treatment initiation to the first occurrence of local, regional, or distant breast cancer recurrence, or death from any cause, whichever occurred first.
- Cardiotoxicity: This was evaluated as a composite safety endpoint, encompassing the first diagnosis of acute myocardial infarction, ischemic heart disease, angina pectoris, cardiomyopathy, heart failure, or cardiac conduction disorders that occurred after the initiation of chemotherapy.
Statistical Analysis Framework
Baseline characteristic comparisons between matched treatment groups employed chi-square or Fisher’s exact tests for categorical variables and independent t-tests for continuous measures. Survival probability estimation utilized Kaplan-Meier methodology, with survival curve comparisons performed using Log rank testing.
Cox proportional hazards regression modeling calculated crude and adjusted hazard ratios with corresponding 95% confidence intervals for primary and secondary outcomes. Proportional hazards assumption verification employed Schoenfeld residual analysis. Multivariable models incorporated comprehensive adjustment for age, cancer stage, socioeconomic indicators, hospital characteristics, and pre-existing comorbidity profiles.
Subgroup analyses systematically examined treatment effects across diverse clinical and demographic strata to assess consistency of observed associations. Sensitivity analyses evaluated mortality outcomes across multiple follow-up intervals including three-year, five-year, and complete study period assessments. Cumulative anthracycline exposure was quantified using cumulative defined daily doses (cDDD), calculated based on the World Health Organization (WHO)-defined daily dose for doxorubicin equivalents (45 mg/m2/week). As body surface area (BSA) was unavailable in the National Health Insurance Research Database (NHIRD), dose normalization per m2 was not feasible. Patients were stratified into tertiles of cDDD (<33, 33–66, and ≥67) to facilitate dose–response analysis; these thresholds were derived empirically from the distribution of the study population rather than from predefined clinical cutoffs.
Statistical computations utilized SAS version 9.4 and R version 4.0.1, with statistical significance defined as two-sided P values less than 0.05.
Results
Study Population Selection
The patient selection process is detailed in the flowchart in Figure 1. From Taiwan’s Longitudinal Health Insurance Database (LHID) for the years 2006–2018, an initial 1,921,314 individuals were identified. After applying inclusion criteria—female patients with stage I–III breast cancer who initiated adjuvant chemotherapy with either a Lipo-Dox-based or Epirubicin-based regimen within three months post-mastectomy—2024 patients were deemed eligible. From this group, 573 patients were excluded due to factors such as recurrence or metastasis at the start of therapy, a history of other malignancies within five years, incomplete tracking data, or being younger than 20 years old. This resulted in a cohort of 1451 patients, of whom 525 had received a Lipo-Dox-based regimen and 926 had received an Epirubicin-based regimen.
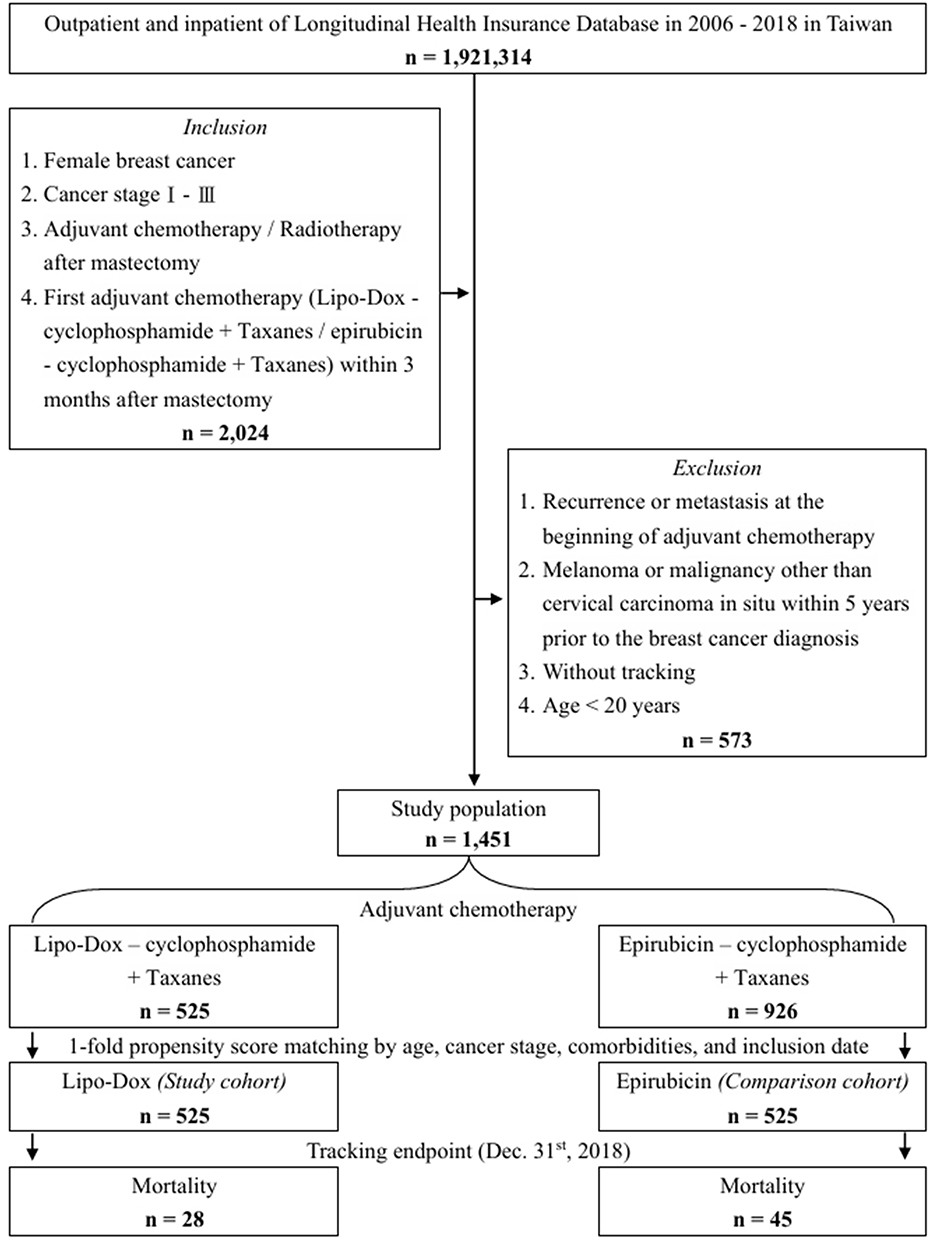 |
Figure 1 Flow diagram of study participant selection. Flow diagram illustrating the identification, screening, eligibility assessment, and 1:1 propensity score matching of patients with stage I–III breast cancer receiving adjuvant Lipo-Dox-based (Presumed Lipo-Dox + Cyclophosphamide + Taxanes) or Epirubicin-based (Epirubicin + Cyclophosphamide + Taxanes) chemotherapy. Patients were selected from Taiwan’s Longitudinal Health Insurance Database (LHID) from 2006 to 2017 and followed until December 31, 2018. Abbreviations: Lipo-Dox, liposomal doxorubicin. |
Propensity Score Matching and Baseline Characteristics
To minimize selection bias, we performed 1:1 propensity score matching (PSM) based on patient age, cancer stage, comorbidities, and the inclusion date. This matching process yielded a final analytical cohort of 1050 patients. The cohort was evenly divided, with 525 patients in the Lipo-Dox-based group (hereafter, the Lipo-Dox group) and 525 patients in the Epirubicin-based group (hereafter, the Epirubicin group).
The baseline demographic and clinical characteristics of the matched Lipo-Dox and Epirubicin cohorts are presented in Table 1. After propensity score matching, the two groups were well-balanced with respect to age (mean ± SD: 49.91 ± 18.82 years for Lipo-Dox vs. 49.98 ± 18.94 years for Epirubicin; P = 0.952), cancer stage (eg, Stage I: 47.43% in both groups; P = 0.999 for overall stage distribution), insurance premium levels (P = 0.825), the prevalence of individual comorbidities including diabetes mellitus (9.14% vs. 8.76%; P = 0.829), hypertension (10.67% vs. 11.24%; P = 0.767), depression (5.52% vs. 5.14%; P = 0.784), chronic kidney disease (5.33% vs. 5.71%; P = 0.787), congestive heart failure (2.29% vs. 1.90%; P = 0.830), chronic obstructive pulmonary disease (6.29% vs. 6.10%; P = 0.898), and hyperlipidemia (4.19% vs. 3.81%; P = 0.875), as well as the level of care (P = 0.916).
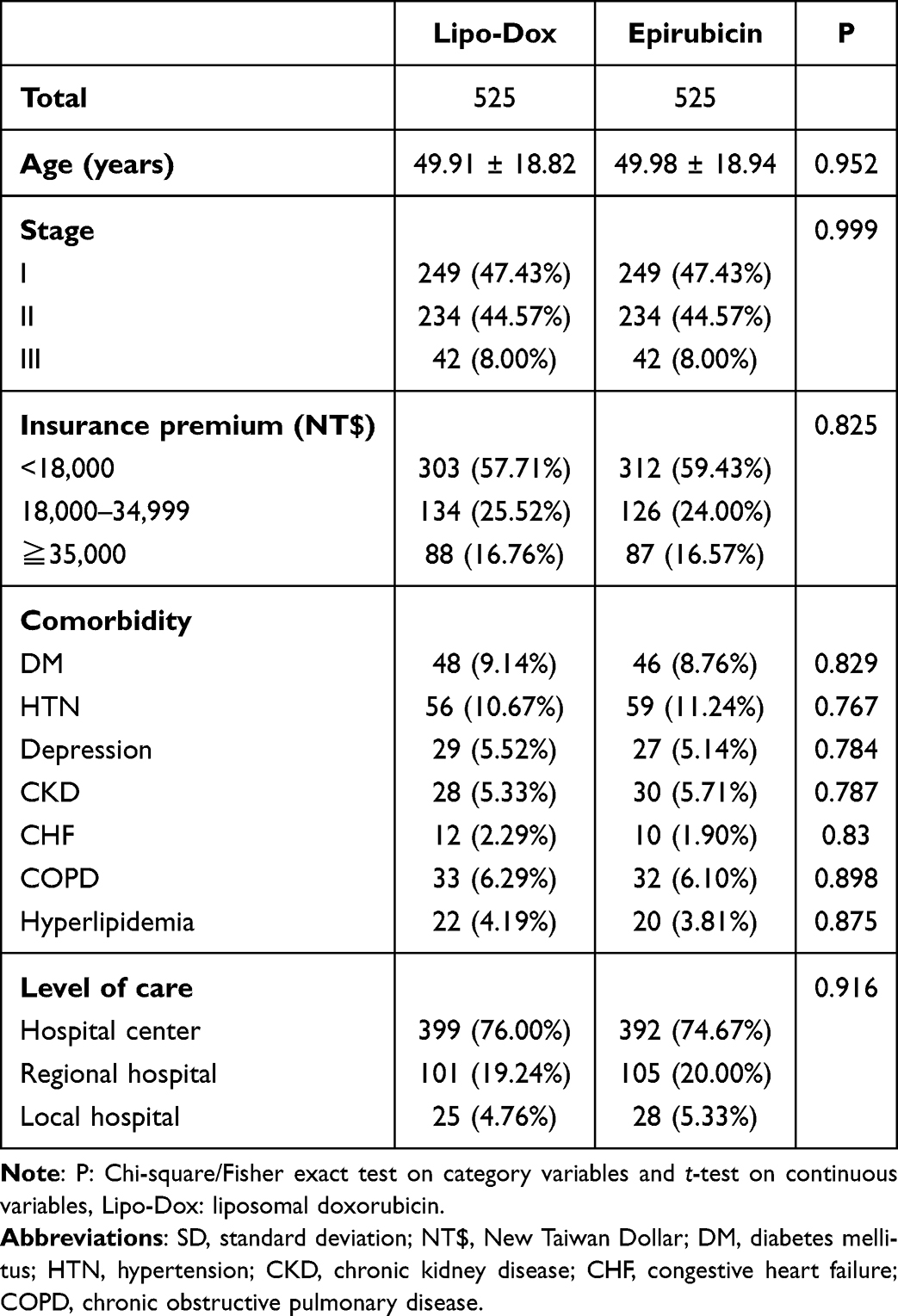 |
Table 1 Baseline Characteristics of the Study Population Stratified by Treatment Group |
Details regarding follow-up duration are provided in Supplement S2. For the matched cohort, the mean (± SD) follow-up duration was 6.13 ± 3.04 years for the Lipo-Dox group and 6.10 ± 2.98 years for the Epirubicin group. The overall mean follow-up duration for the total matched cohort was 6.12 ± 3.01 years, with a median follow-up of 6.05 years.
Survival Outcomes
Kaplan-Meier survival analysis for overall survival is presented in Figure 2. Patients in the Lipo-Dox group demonstrated significantly better overall survival compared to those in the Epirubicin group (log-rank P < 0.001).
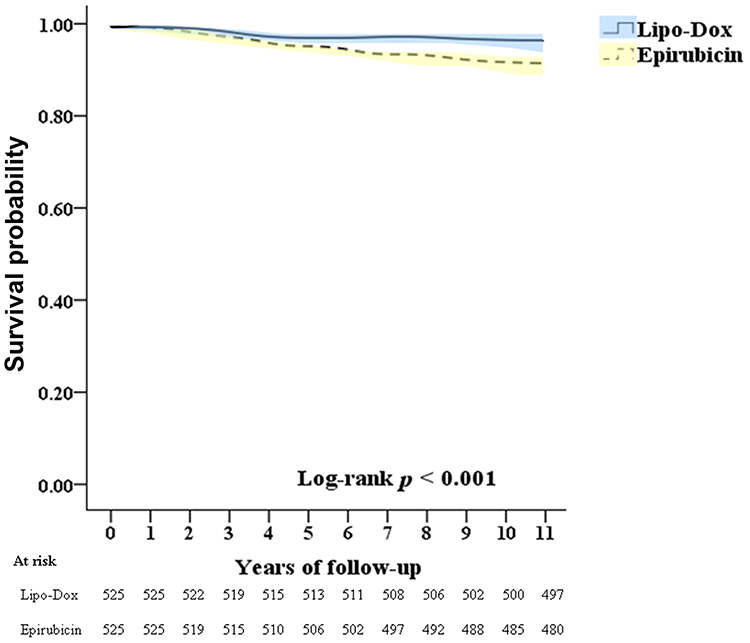 |
Figure 2 Kaplan-Meier curves for overall survival. Kaplan-Meier estimates of overall survival for patients with stage I–III breast cancer treated with adjuvant Lipo-Dox-based therapy versus Epirubicin-based therapy after 1:1 propensity score matching (n = 1,050). Shaded areas represent 95% confidence intervals. The number-at-risk table is displayed below the x-axis. The P-value was determined by the Log rank test. |
The primary and secondary clinical outcomes are summarized in Table 2. For the primary outcome of overall survival (all-time mortality), a total of 28 deaths (10.30 per 100,000 person-years, PYs) occurred in the Lipo-Dox group, compared to 45 deaths (13.92 per 100,000 PYs) in the Epirubicin group. After adjusting for covariates, the Lipo-Dox group was associated with a significantly lower risk of all-time mortality compared to the Epirubicin group (aHR 0.754, 95% CI 0.632–0.899; P < 0.001). In the unmatched cohort, a total of 28 deaths occurred in the Lipo-Dox group (10.30 per 100,000 person-years [PYs]) and 77 deaths in the epirubicin group (13.51 per 100,000 PYs). Lipo-Dox was associated with a lower risk of all-cause mortality compared with epirubicin (adjusted hazard ratio [aHR] 0.775, 95% confidence interval [CI] 0.645–0.906; P = 0.003). Kaplan–Meier curves for overall survival in the unmatched cohort are presented in Supplementary S3.
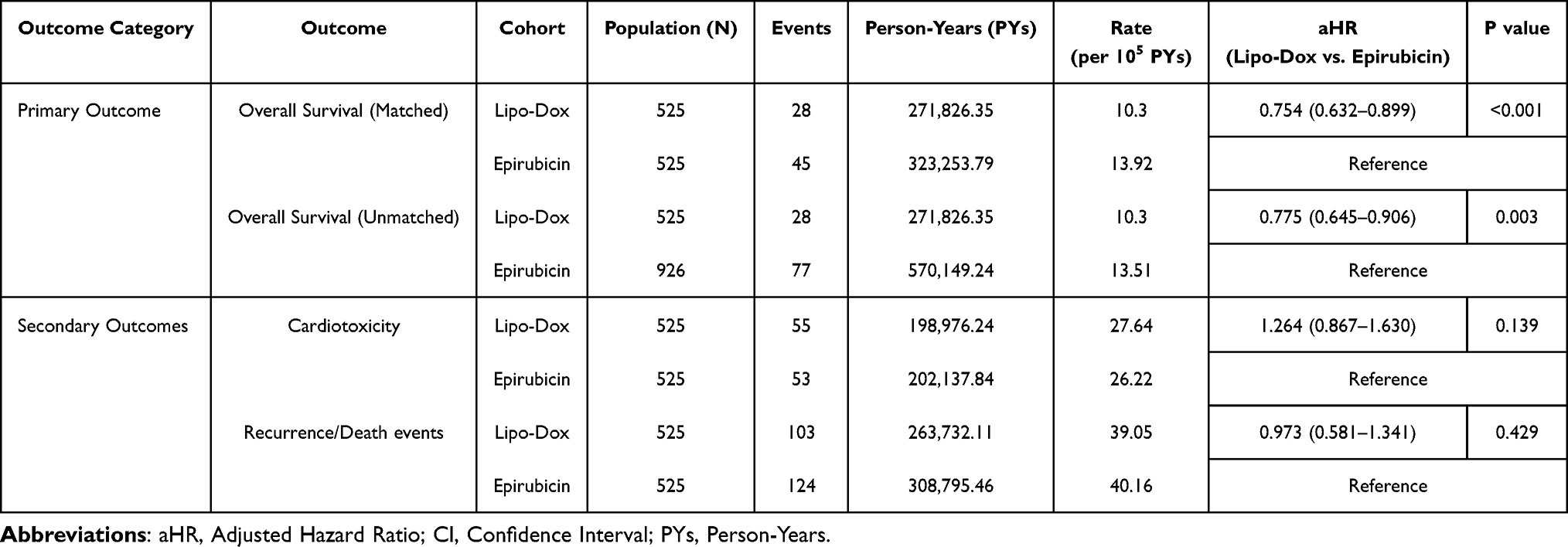 |
Table 2 Primary and Secondary Outcomes Comparing Lipo-Dox versus Epirubicin Adjuvant Chemotherapy |
For secondary outcomes, the incidence rate of cardiotoxicity was 27.64 per 100,000 PYs in the Lipo-Dox group (55 events) and 26.22 per 100,000 PYs in the Epirubicin group (53 events). There was no statistically significant difference in the risk of cardiotoxicity between the two groups (aHR 1.264, 95% CI 0.867–1.630; P = 0.139). The incidence rate of disease-free survival events (breast cancer recurrence or death) was 39.05 per 100,000 PYs in the Lipo-Dox group (103 events) and 40.16 per 100,000 PYs in the Epirubicin group (124 events). No significant difference in DFS was observed between the Lipo-Dox and Epirubicin groups (aHR 0.973, 95% CI 0.581–1.341; P = 0.429). Kaplan-Meier curves for cardiotoxicity and disease-free survival (DFS) are presented in Supplementary S4. No statistically significant differences were observed between groups in either cardiotoxicity or DFS (log-rank P > 0.05).
Sensitivity Analyses
Sensitivity analyses evaluating the adjusted hazard ratios for mortality at different follow-up durations are detailed in Supplement S5. The Lipo-Dox group consistently showed a lower risk of mortality compared to the Epirubicin group across these time points: for 3-year mortality, the aHR was 0.816 (95% CI 0.724–0.937; P = 0.018); for 5-year mortality, the aHR was 0.779 (95% CI 0.672–0.913; P = 0.007); and for all-time mortality (consistent with the primary analysis), the aHR was 0.754 (95% CI 0.632–0.899; P < 0.001). These findings indicate that the observed survival benefit with Lipo-Dox was robust across different follow-up assessments.
Subgroup Analyses for Overall Survival
Subgroup analyses for overall survival were performed to evaluate the consistency of the treatment effect of Lipo-Dox versus Epirubicin across various prespecified clinical and demographic strata. The observed survival benefit associated with the Lipo-Dox group was generally consistent across most subgroups examined, including those defined by cancer stage, insurance premium levels, common comorbidities, and hospital level of care. While the magnitude of the effect varied slightly between sub-groups, the direction of the adjusted hazard ratios predominantly favored the Lipo-Dox group. Detailed results for all subgroups, including specific adjusted hazard ratios and 95% confidence intervals, are presented in Figure 3.
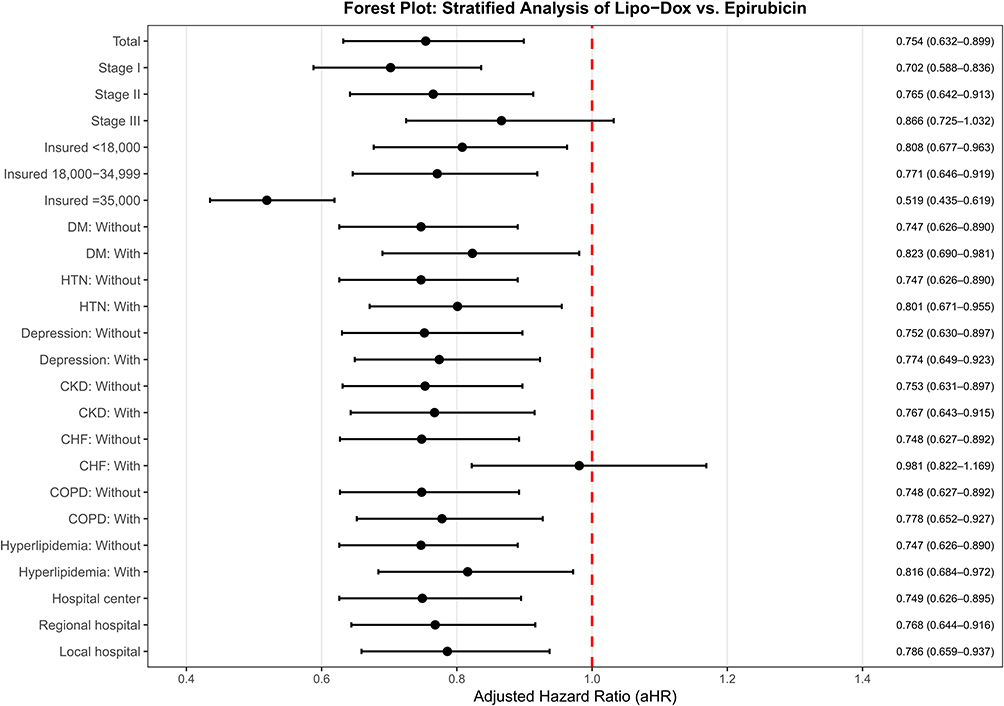 |
Figure 3 Subgroup analysis of overall survival: Lipo-Dox versus Epirubicin across clinical and demographic strata. Forest plot showing adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) for overall survival, comparing the Lipo-Dox-based (Study) cohort with the Epirubicin-based (Comparison) cohort across various patient subgroups. Hazard ratios were adjusted for age, cancer stage, monthly income level, level of care, and pre-existing comorbidities (diabetes mellitus, hypertension, depression, chronic kidney disease, congestive heart failure, chronic obstructive pulmonary disease, and hyperlipidemia) unless the variable itself was used for stratification. Abbreviations: aHR, adjusted hazard ratio; CI, confidence interval; DM, diabetes mellitus; HTN, hypertension; CKD, chronic kidney disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease. |
Factors Associated with Overall Survival
Results from the multivariable Cox regression analysis for factors associated with overall survival are presented in Table 3. After adjusting for other covariates, treatment with Lipo-Dox (vs. Epirubicin) remained significantly associated with improved overall survival (aHR 0.754, 95% CI 0.632–0.899; P < 0.001). Other factors significantly associated with an increased risk of mortality included older age (aHR per year increase 1.174, 95% CI 1.025–1.372; P = 0.026), more advanced cancer stage (Stage III vs. Stage I: aHR 1.477, 95% CI 1.282–1.996; P < 0.001), and the presence of comorbidities such as diabetes mellitus (aHR 2.501, 95% CI 1.972–3.452; P < 0.001), hypertension (aHR 2.653, 95% CI 2.013–3.684; P < 0.001), depression (aHR 1.986, 95% CI 1.782–3.044; P < 0.001), chronic kidney disease (aHR 1.830, 95% CI 1.435–2.684; P < 0.001), congestive heart failure (aHR 1.792, 95% CI 1.488–2.697; P < 0.001), chronic obstructive pulmonary disease (aHR 1.343, 95% CI 1.068–1.897; P = 0.002), and hyperlipidemia (aHR 1.540, 95% CI 1.275–2.430; P < 0.001). Patients with higher insurance premiums (≥NT$35,000 vs. <NT$18,000: aHR 0.670, 95% CI 0.483–1.001; P = 0.051) showed a trend towards better survival, though not reaching statistical significance for the highest category in this model. Treatment at a hospital center (vs. local hospital: aHR 0.786, 95% CI 0.629–0.901; P < 0.001) or regional hospital (vs. local hospital: aHR 0.842, 95% CI 0.735–0.977; P = 0.019) was associated with better overall survival.
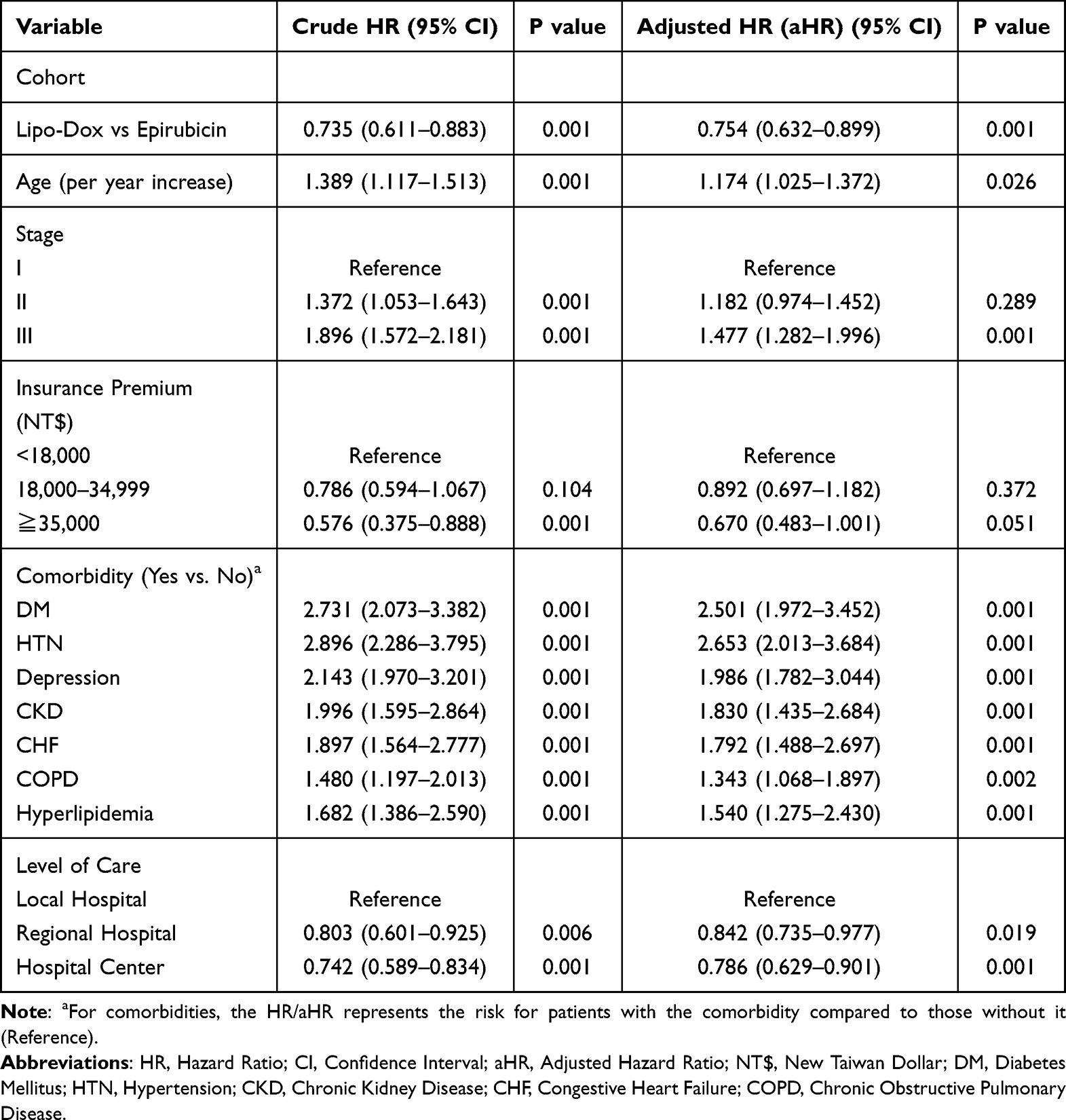 |
Table 3 Multivariable Cox Regression Analysis of Factors Associated with Overall Survival |
Overall Survival by Lipo-Dox Cumulative Defined Daily Dose (cDDD)
The association between Lipo-Dox treatment and mortality, stratified by the cumulative defined daily dose (cDDD) of Lipo-Dox received by patients in the Lipo-Dox group (compared to the Epirubicin group), is presented in Supplement S6. The overall adjusted hazard ratio for mortality comparing Lipo-Dox to Epirubicin was 0.754 (95% CI 0.632–0.899; P < 0.001). When stratified by Lipo-Dox cDDD, patients receiving <33 cDDD had an aHR of 0.863 (95% CI 0.725–1.029; P = 0.184). Those receiving 33–66 cDDD of Lipo-Dox showed an aHR of 0.816 (95% CI 0.684–0.973; P < 0.001), and patients receiving ≥67 cDDD of Lipo-Dox had an aHR of 0.586 (95% CI 0.490–0.698; P < 0.001) compared to the Epirubicin group, suggesting a potential dose-dependent benefit with higher cumulative doses of Lipo-Dox. In contrast, the Epirubicin group showed relatively stable mortality rates across cDDD tertiles, with no comparable dose-response pattern (Supplement S3, Table).
Discussion
In this comprehensive, population-based cohort study, we observed an association between adjuvant therapy with Lipo-Dox and improved overall survival compared to epirubicin for patients with early-stage breast cancer. Our analysis indicated a 24.6% relative reduction in the hazard of all-cause mortality with the Lipo-Dox-based regimen, an association that remained consistent across various patient subgroups. These findings raise the possibility that liposomal anthracycline formulation may be linked to better long-term outcomes in a real-world setting, though the underlying mechanisms for this observation require careful consideration.
Interpretation of the Overall Survival Benefit
The clinical implications of our findings may be most relevant for patients with early-stage breast cancer who also have significant comorbidities. In our analysis, the association between Lipo-Dox and improved overall survival was consistent across most subgroups, a finding of particular importance for patients with pre-existing conditions. For this population, where the balance between therapeutic efficacy and treatment-related toxicity is especially critical, a regimen with a more favorable tolerability profile could plausibly translate into better long-term outcomes.
This hypothesis is indirectly supported by our observation of a dose-response relationship, wherein higher cumulative doses of Lipo-Dox were associated with a greater survival benefit. This suggests that the ability to maintain adequate dose intensity—which is often challenging in vulnerable patients but may be more achievable with a better-tolerated agent—is linked to improved survival. While our findings are exploratory, they raise the possibility that the therapeutic advantages of liposomal formulation might be most pronounced in patients whose clinical status makes them more susceptible to the toxicities of conventional chemotherapy.
Importantly, in the analysis of the unmatched cohort, the survival benefit associated with Lipo-Dox remained directionally consistent with the primary propensity score–matched results, suggesting that the observed advantage is not solely attributable to the matching process or the associated reduction in sample size. Nevertheless, without propensity score matching, estimates are more susceptible to baseline imbalances and confounding by indication, and the magnitude of the treatment effect should therefore be interpreted with caution. Taken together, the concordance between matched and unmatched analyses provides complementary evidence that the observed survival benefit is unlikely to represent an artifact of the PSM approach and may instead reflect a genuine treatment effect.
Cardiotoxicity Considerations and Study Limitations
The lack of a significant difference in cardiotoxicity likely reflects the limited sensitivity of claims-based data in detecting subclinical cardiac dysfunction. In contrast, prior studies have demonstrated the cardioprotective advantage of Lipo-Dox through systematic cardiac monitoring.6,20,21 Given these methodological differences, our null finding (aHR 1.264, P = 0.139) should be interpreted as no significant difference in clinically diagnosed cardiac events, rather than equivalence in cardiac safety profiles between the two formulations.
Comparison with Existing Literature
Our study’s findings must be interpreted within the context of the existing literature, particularly recent studies from Asian cohorts. Notably, our observation of a significant overall survival advantage with the Lipo-Dox regimen contrasts with the findings of several other key studies that reported comparable survival outcomes. For instance, in a large retrospective study of 1471 Chinese patients, Hu et al found no significant differences in overall or disease-free survival between Lipo-Dox-based and epirubicin-based regimens.17 Similarly, the prospective, randomized Phase II trial by Tseng et al in a Taiwanese cohort concluded that both regimens yielded comparable long-term efficacy, with no statistically significant differences in 5-year DFS or OS rates.15 This conclusion was echoed in a randomized controlled trial by Tang et al, which also demonstrated that 5-year DFS and OS did not differ significantly when comparing a Lipo-Dox-based regimen to conventional doxorubicin.22
The discrepancy between our real-world findings and the results from these studies warrants careful consideration. One possible explanation is the difference between a population-based setting and the more controlled environment of prospective clinical trials, where factors like treatment tolerability and dose intensity may have a more pronounced impact in routine practice. Another possibility is that a modest survival benefit may only become statistically apparent in a very large cohort with extended follow-up, such as ours. However, as a retrospective analysis, the potential for residual or unmeasured confounding factors remains a key concern. For example, patients who were capable of affording out-of-pocket Lipo-Dox may have differed in characteristics that could independently influence survival. It is important to mention that our propensity score matching and multivariable models did account for proxies of socioeconomic status (insurance premium levels) and the level of care (hospital type). Nevertheless, the potential for residual confounding from unmeasured variables, such as health literacy or social support, cannot be entirely dismissed. Therefore, our finding of an OS advantage could be considered hypothesis-generating and requires further long-term prospective studies to validate.
A notable finding is the apparent discordance between the significant OS benefit and the absence of a significant DFS difference. This pattern suggests that Lipo-Dox may not confer greater direct antitumor efficacy compared to epirubicin, consistent with prior randomized trials. However, the OS advantage may reflect favorable long-term effects such as better tolerability enabling completion of planned treatment cycles, reduced cumulative organ toxicity facilitating more effective management of subsequent therapies upon recurrence, or potentially favorable immunomodulatory effects. This discordance underscores the importance of evaluating long-term survival outcomes beyond traditional efficacy endpoints.
Study Strengths and Methodological Rigor
This study has several methodological strengths that enhance the validity of its findings. Its primary strength is the use of Taiwan’s National Health Insurance Research Database, a comprehensive, population-based source that ensures a high degree of representativeness and minimizes the selection bias inherent in single-institution studies. This large Asian cohort is particularly noteworthy, as it begins to address a critical knowledge gap in a literature dominated by research on Western populations, where pharmacogenomic and toxicity profiles may differ. To ensure methodological rigor, we implemented propensity score matching, which effectively balanced baseline characteristics between the treatment groups and substantially reduced confounding bias. Finally, the extended follow-up period, with a median observation time exceeding six years, provided a mature dataset for assessing long-term survival outcomes.
Study Limitations and Methodological Considerations
Despite its strengths, this study has several limitations that must be considered when interpreting the findings. The primary methodological limitation is the indirect identification of the Lipo-Dox cohort, a surrogate-based strategy necessitated by re-imbursement policies. A potential misclassification concern involves patients who received a TC (docetaxel-cyclophosphamide) regimen without any anthracycline. Our sequential C-then-T identification pattern could theoretically capture these patients. However, during the study period, anthracycline-based sequential regimens were the standard of care in Taiwan, and TC was infrequently used for early-stage breast cancer. Nevertheless, this represents an inherent limitation of our surrogate identification approach.
Furthermore, like all analyses of administrative claims data, our study lacked granular clinical information such as patient performance status, precise chemotherapy dosing, and treatment adherence patterns. While HER2 status was available for cohort selection, the absence of detailed molecular subtyping, such as hormone receptor status, precluded more specific biomarker-stratified analyses. This limits the generalizability of our findings across molecular subtypes, as the prognostic and therapeutic implications differ substantially between triple-negative breast cancer and HR-positive/HER2-negative disease. Although propensity score matching was used to balance numerous covariates, the potential for residual confounding from unmeasured factors, particularly socioeconomic influences not fully captured by insurance premium data, cannot be entirely excluded. Patients who self-funded Lipo-Dox may possess higher health literacy, better nutritional status, and greater access to comprehensive supportive care. While our propensity score model included insurance premium levels as a proxy for socioeconomic status, this variable may not fully capture the broader “wealth effect” that could independently influence survival outcomes. Lastly, the study period of 2006–2018 may not fully reflect contemporary clinical practice, especially regarding advances in supportive care and cardiac monitoring protocols.
Clinical Implications and Future Directions
While our findings require cautious interpretation, they may hold particular relevance for the treatment of patients with early-stage breast cancer who also present with significant comorbidities. The consistent association with improved survival observed across various subgroups, including those with pre-existing conditions, suggests that Lipo-Dox could be considered a relevant therapeutic option for this higher-risk population. In these patients, for whom treatment tolerability and the mitigation of long-term toxicity are paramount, the potentially favorable safety profile of a liposomal formulation might contribute to better overall outcomes. Therefore, when selecting an anthracycline, clinicians might consider Lipo-Dox as a potential alternative, especially for patients with an elevated cardiovascular risk or a high comorbidity burden. This consideration would align with contemporary cardio-oncology guidelines. Decisions regarding this off-label, self-funded treatment in Taiwan should, however, remain individualized, balancing the potential benefits against the financial burden on the patient.
To build upon these findings, several future research avenues are warranted. Further prospective studies with systematic cardiac monitoring, along with pharmacogenomic investigations in Asian populations, may help clarify the safety profile of Lipo-Dox and potential ethnic differences in anthracycline-related toxicity. Formal cost-effectiveness analyses and long-term survivorship studies focusing on quality of life would be essential to inform healthcare policy regarding reimbursement and to fully understand the overall therapeutic value of liposomal formulation.
Conclusion
In this large, population-based cohort study, adjuvant chemotherapy with Lipo-Dox was associated with improved overall survival compared to an epirubicin-based regimen in patients with early-stage breast cancer. This association was notably consistent across subgroups, including in patients with multiple comorbidities where the balance between efficacy and safety is crucial. However, this survival advantage was not accompanied by a significant difference in disease-free survival, and the study’s design limited the assessment of subclinical cardiotoxicity. Therefore, our findings should be considered hypothesis-generating and interpreted with caution. These real-world data suggest that Lipo-Dox may be a reasonable therapeutic consideration for selecting patients, particularly those with a high comorbidity burden. Further prospective research is warranted to validate this potential survival benefit and to better characterize the agent’s long-term risk-benefit profile.
Institutional Review Board Statement
This study was deemed exempt from review by the Tri-Service General Hospital Institutional Review Board (approval number: A202505204) due to the use of de-identified data. This study was conducted in accordance with the Declaration of Helsinki.
Data Sharing Statement
Study data are available from the corresponding author upon reasonable request. Taiwan’s National Health Insurance Research Database was accessed through institutional license. All data were de-identified and handled in compliance with data protection and privacy regulations.
Informed Consent Statement
This study used de-identified data from the Ministry of Health and Welfare’s National Health Insurance Research Database (NHIRD). Individual identities cannot be identified. It is a low-risk secondary data analysis without clinical intervention.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. World Health Organization. Breast Cancer [Fact sheet]. World Health Organization. 2025.
2. Sung H, Rosenberg PS, Chen WQ, et al. Female breast cancer incidence among Asian and Western populations: more similar than expected. J Natl Cancer Inst. 2015;107(7). doi:10.1093/jnci/djv107
3. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–14. doi:10.3322/caac.21820
4. Loibl S, André F, Bachelot T, et al. Early breast cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2024;35(2):159–182. doi:10.1016/j.annonc.2023.11.016
5. National Comprehensive Cancer N. NCCN clinical practice guidelines in oncology: breast cancer. 2025. National Comprehensive Cancer Network. Available from: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf.
6. Lyon AR, López-Fernández T, Couch LS, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43(41):4229–4361. doi:10.1093/eurheartj/ehac244
7. Zhang M, Yang H, Xu C, Jin F, Zheng A. Risk factors for anthracycline-induced cardiotoxicity in breast cancer treatment: a meta-analysis. Front Oncol. 2022;12:899782. doi:10.3389/fonc.2022.899782
8. Gil-Gil MJ, Bellet M, Bergamino M, et al. Long-term cardiac safety and survival outcomes of neoadjuvant pegylated liposomal doxorubicin in elderly patients or prone to cardiotoxicity and triple negative breast cancer. final results of the multicentre phase II CAPRICE study. Front Oncol. 2021;11:645026. doi:10.3389/fonc.2021.645026
9. Yamaguchi N, Fujii T, Aoi S, Kozuch PS, Hortobagyi GN, Blum RH. Comparison of cardiac events associated with liposomal doxorubicin, epirubicin and doxorubicin in breast cancer: a Bayesian network meta-analysis. Eur J Cancer. 2015;51(16):2314–2320. doi:10.1016/j.ejca.2015.07.031
10. Gabizon A, Shmeeda H, Barenholz Y. Pharmacokinetics of pegylated liposomal Doxorubicin: review of animal and human studies. Clin Pharmacokinet. 2003;42(5):419–436. doi:10.2165/00003088-200342050-00002
11. Gabizon AA, Patil Y, La-Beck NM. New insights and evolving role of pegylated liposomal doxorubicin in cancer therapy. Drug Resist Updat. 2016;29:90–106. doi:10.1016/j.drup.2016.10.003
12. Barenholz Y. Doxil®--the first FDA-approved nano-drug: lessons learned. J Control Release. 2012;160(2):117–134. doi:10.1016/j.jconrel.2012.03.020
13. Zhang J, Jiang H, Zhang J, et al. Effectiveness and safety of pegylated liposomal doxorubicin versus epirubicin as neoadjuvant or adjuvant chemotherapy for breast cancer: a real-world study. BMC Cancer. 2021;21(1):1301. doi:10.1186/s12885-021-09050-6
14. Hung CC, Yang Y, Tsai IC, Hsu CY, Liu CH, Yang JR. The efficacy of pegylated liposomal doxorubicin-based neoadjuvant chemotherapy in breast cancer: a retrospective case-control study in Taiwan. Biochem Res Int. 2020;2020:5729389. doi:10.1155/2020/5729389
15. Tseng LM, Chen FM, Chen ST, et al. Comparison of the efficacy, safety, and quality of life of pegylated liposomal doxorubicin-cyclophosphamide versus epirubicin-cyclophosphamide in patients with early-stage HER2-negative breast cancer: a prospective, randomized, multicenter, phase II study. Oncol Res Treat. 2024;47(10):484–495. doi:10.1159/000540369
16. Rafiyath SM, Rasul M, Lee B, Wei G, Lamba G, Liu D. Comparison of safety and toxicity of liposomal doxorubicin vs. conventional anthracyclines: a meta-analysis. Exp Hematol Oncol. 2012;1(1):10. doi:10.1186/2162-3619-1-10
17. Hu W, Lv K, Teng R, et al. Pegylated liposomal doxorubicin versus epirubicin as adjuvant therapy for stage I-III breast cancer. Front Genet. 2021;12:746114. doi:10.3389/fgene.2021.746114
18. Lien MY, Liu LC, Wang HC, et al. Safety and efficacy of pegylated liposomal doxorubicin-based adjuvant chemotherapy in patients with stage I-III triple-negative breast cancer. Anticancer Res. 2014;34(12):7319–7326.
19. Zhang L, Song J, Hanif W, et al. Racial and ethnic disparities in cardiotoxicity in patients with cancer treated with anthracyclines. J Am Heart Assoc. 2025;14(7):e037780. doi:10.1161/jaha.124.037780
20. Oikonomou EK, Kokkinidis DG, Kampaktsis PN, et al. Assessment of prognostic value of left ventricular global longitudinal strain for early prediction of chemotherapy-induced cardiotoxicity: a systematic review and meta-analysis. JAMA Cardiol. 2019;4(10):1007–1018. doi:10.1001/jamacardio.2019.2952
21. Cil T, Kaplan AM, Altintas A, Akin AM, Alan S, Isikdogan A. Use of N-terminal pro-brain natriuretic peptide to assess left ventricular function after adjuvant doxorubicin therapy in early breast cancer patients: a prospective series. Clin Drug Investig. 2009;29(2):131–137. doi:10.2165/0044011-200929020-00007
22. Tang L, He M, Geng C, et al. Pegylated liposomal doxorubicin + cyclophosphamide followed by taxane as adjuvant therapy for early-stage breast cancer: a randomized controlled trial. Oncologist. 2025;30(6). doi:10.1093/oncolo/oyaf101
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics and Survival Outcomes of Patients with De Novo Metastatic Breast Cancer
Almasri H, Erjan A, Abudawaba H, Ashouri K, Mheid S, Alnsour A, Abdel-Razeq H
Breast Cancer: Targets and Therapy 2022, 14:363-373
Published Date: 29 October 2022
Clinical Value of Cardiac Troponin I in Assessing Anthracycline-Induced Cardiotoxicity in Postoperative Breast Cancer Patients
Li H, Li X, Tang S
Breast Cancer: Targets and Therapy 2026, 18:580515
Published Date: 23 January 2026