Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Association of HTR1A Gene Polymorphisms with Efficacy and Plasma Concentrations of Atypical Antipsychotics in the Treatment of Male Patients with Schizophrenia
Authors Qin Y, Zhao J, Yang Y, Liu Y, Xiang H, Tong J, Huang C
Received 9 November 2023
Accepted for publication 24 January 2024
Published 30 January 2024 Volume 2024:20 Pages 185—193
DOI https://doi.org/10.2147/NDT.S449096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Ying Qin,1 Jingwen Zhao,1 Yong Yang,1 Yanjing Liu,1 Hui Xiang,2 Jingfeng Tong,3 Chengchen Huang3
1Department of Psychiatry, the Second People’s Hospital of Guizhou Province, Guiyang, 550004, People’s Republic of China; 2Department of Psychology, Guizhou Provincial People’s Hospital, Guiyang, 550002, People’s Republic of China; 3Shanghai Conlight Medical Laboratory, Co, Ltd, Shanghai, 200032, People’s Republic of China
Correspondence: Chengchen Huang, Shanghai Conlight Medical Laboratory Co, Ltd, Shanghai, People’s Republic of China, Email [email protected]
Purpose: We investigate the association of HTR1A rs10042486 and rs6295 with efficacy and plasma concentrations of atypical antipsychotics in the treatment of male patients with schizophrenia.
Patients and Methods: A total of 140 male patients diagnosed with schizophrenia who were treated with any single atypical antipsychotic between May 2020 and May 2022 were retrospectively included. Clinical symptoms were assessed using Positive and Negative Syndrome Scale (PANSS). All SNPs were typed using Agena Bioscience MassARRAY DNA mass spectrometry. Plasma concentrations of antipsychotics at week 3, 6 and 12 after treatment commence were analyzed using mass spectrometry.
Results: For efficacy of atypical antipsychotics, we observed no significant difference between HTR1A rs10042486, rs6295 and positive symptom improvement, where the patients with heterozygous mutant at the rs10042486 and rs6295 locus were superior to those with wild-type or homozygous mutant genotypes on negative symptom improvement, especially at 12 weeks of follow-up when the difference between genotypes at the rs6295 locus have statistical significance (P = 0.037). For plasma concentration, we found that quetiapine plasma concentrations were significantly lower in patients with mutation-heterozygous types than in wild-type and homozygous mutation genotypes at week 6. In contrast, higher plasma concentrations were found for mutant heterozygous than wild genotypes in the risperidone monotherapy analysis, and the difference among genotypes at the rs6295 locus was statistically significant at 6 weeks of follow-up.
Conclusion: The assessment of the correlation of genetic polymorphisms of HTR1A rs6295 and rs10042486 in male patients with schizophrenia with the monitoring of therapeutic drug concentrations and therapeutic efficacy provides a constructive foundation for the clinical individualization of antipsychotics, such as quetiapine and risperidone, which is important in selecting the dose of the medication and improving the improvement of negative symptoms.
Keywords: schizophrenia, HTR1A, polymorphism, plasma concentration, atypical antipsychotics, asian male patients
Introduction
Schizophrenia is a common (around 1% of the world’s population) chronic mental disorder that causes considerable distress and disability, with symptoms including hallucinations, delusions and behavioral disorders.1 For the treatment of schizophrenia, atypical antipsychotic drugs (also known as second-generation antipsychotics) are recommended as first-line agents and commonly used in clinics for their high efficacy and low adverse drug reactions.2–4 The mechanisms of antipsychotics are mainly based on the proposed neurotransmitter abnormality hypotheses explaining the biological background of schizophrenia, including dopamine, glutamic acid, and serotonin system (5-HT).5 Unlike typical antipsychotics, which predominantly focused on single receptor, atypical antipsychotics bind more receptors, including dopamine receptors and serotonin receptors.6,7 Numerous studies have revealed that altered 5-HT synthesis and metabolism, abnormalities in the levels of brain 5-HT1A and 5-HT2A receptors are associated with pathophysiology and efficacy in the treatment of schizophrenia.8–10 The 5-HT1A receptor encoded by HTR1A is one of the most abundant serotonin receptors in the central nervous system, and plays a crucial role in the regulation of mood, anxiety, and appetite by modulating serotonin activity.11 Studies have shown that the HTR1A gene induces neuronal inhibition and behavioral control in the central nervous system and is involved in the molecular mechanisms of schizophrenia.12 The transcriptional regulatory region’s rs6295 and rs10042486 locus have received the most attention.13,14 An Italian study showed that carriers of the rs6295 GG genotype had better reductions in negative symptoms after treatment with clozapine.15 However, studies on them in the treatment of schizophrenia were not comprehensive and the conclusions remained controversial. A meta-analysis showed that carriers of the C allele of the rs6295 polymorphism had significantly more improvement in negative symptoms compared to those carrying the G allele.16 Additionally, many studies have focused on the apparent relationship between HTR1A gene polymorphisms and antipsychotic efficacy in patients with schizophrenia17,18 and few studies exploring the associations between HTR1A gene polymorphisms and plasma concentrations of atypical antipsychotics.
To this end, in this study, we first analyzed the relationship between HTR1A rs6295 and rs10042486 and efficacy of atypical antipsychotics in the treatment of male patients with schizophrenia. In addition, to better understand the possible mechanisms underlying this relationship, our secondary purpose was to evaluate the association of HTR1A rs6295 and rs10042486 with plasma concentration of atypical antipsychotics.
Materials and Methods
Participants
As a retrospective study, a total of 140 male patients with schizophrenia treated with any single atypical psychotropic and underwent a 12-week follow-up from May 2020 to May 2022 admitted to the Second People’s Hospital of Guizhou Province were enrolled in our study. All patients were assessed for the severity of disease at baseline and during treatment using the Positive and Negative Syndrome Scale (PANSS), including the PANSS positive, PANSS negative and PANSS general psychopathology subscales. Inclusion criteria: (i) fulfillment of the International Classification of Diseases 11th Revision (ICD-11) diagnostic criteria for schizophrenia, (ii) age between 18 and 60 years, (iii) no mix of antipsychotic medications 1 month prior to enrollment and (iv) PANSS score ≥ 60. Exclusion criteria: (i) heart, liver and kidney disease; (ii) alcohol dependence; (iii) epilepsy; (iv) diabetes mellitus; (v) none of the single or multiple serious side effects of monotherapy. Additionally, sociodemographic characteristics were recorded, including age, age at onset, marital status and educational levels. In this study, relapse was defined as the reappearance of clinically significant core symptoms of schizophrenia after remission or the relapse of a patient after an incomplete remission with “symptomatic exacerbation” or “worsening an increase of more than 25% in the PANSS score. This project was approved by the Ethics Committee of the Second People’s Hospital of Guizhou Province (No.2019–50) and the patients and their families provided informed consent.
Treatment
Patients were prescribed with 12-week of any one atypical antipsychotic drug administration, including quetiapine, risperidone, aripiprazole, olanzapine, clozapine, paliperidone, ziprasidone or amisulpride. For quetiapine monotherapy, the fumarate (AstraZeneca Pharmaceuticals Ltd., J20171029) was prescribed at an initial dose of 50 mg once daily. The dose was subsequently increased to 100 mg once daily after a few days, and then to 400 mg/day after 28 days of consistent usage. The dose adjustment during the 12-week treatment period was based on the patient’s condition. For patients receiving risperidone (Xi’an Janssen Pharmaceutical Co., Ltd, H20010310), the recommended initial dose is 1 mg. Within a week or so, the daily dosage can be gradually increased to 2–4 mg and may be further increased to 4 to 6 mg per day during the second week. The dose can be maintained or adjusted based on the individual’s response. In general, the optimal dose range is 2 to 6 mg per day, and the maximum daily dose should not exceed 10 mg. For the other antipsychotics, initiate the dose using an equivalent dose analogous to risperidone 1 mg or quetiapine 100 mg, and increase the measurement incrementally to the therapeutic dose according to the instructions for administration.
Sample Collection
During the study period, drug administration and blood collection time points were strictly controlled. Patients took the drugs at 20:00 on the night prior to the 3rd, 6th and 12th weeks of treatment at baseline. On the following day at 8:00 a.m., 5 mL of unanticoagulated blood of the enrollees (patients were in a fasting state) was drawn before drug administration. The blood was centrifuged at 2000 rpm for 5 min to separate plasma and blood cells, and 1 mL of each was taken according to the blood sample and dried blood film processing tutorials, separated to make dried blood films and promptly sent for genetic and plasma concentration testing. The remaining blood samples were saved for repeated testing after removing personal identification information using uniform code.
Genotyping
The testing method and experiments from nucleic acid extraction to final mass spectrometry analysis were conducted by Shanghai Conlight Medical Co., Ltd. Extraction of nucleic acids from collected samples was performed using total nucleic acid extraction kit (Conlight Medical) in strict accordance with the instructions. Genotyping for rs10042486 and rs6295 in HTR1A using matrix-assisted laser desorption ionization-time-of-flight mass spectrometry (MALDI-TOF MS). The results were analyzed with Typer 4.0 software (Agena Bioscience).
Plasma Concentrations Measurements
Therapeutical drug monitoring (TDM) was performed using a high-performance liquid chromatography and mass spectrometry instrument manufactured by Thermo Fisher (LC-MS, AB5500). The chromatographic column was a Kinetex-C18 with a particle size of 2.6 μm, a length and internal diameter of 100 mm × 3 mm, and a pore size of 100 Å. An electrospray ionization source was used, and positive ion multiple reaction monitoring was selected for analysis.
Treatment Efficacy Evaluation
In general, the rate of reduction in PANSS scores is the primary basis for evaluating the efficacy of psychiatric classifications, and a reduction in scores equal to or more than 50% is usually considered effective or responsive to treatment. In this study, we focused on the changes in the PANSS scale scores for positive symptoms, negative symptoms, and pathologic symptoms. Symptomatic treatment was considered effective or response at week 3, week 6, and week 12 follow-up when the positive symptom score, negative symptom score, and pathologic symptom score reduced by 50% or more from baseline. Calculated by subtracting the post-treatment score from the baseline score and dividing it by the baseline score.
Statistical Analyses
All data were statistically analyzed by applying SPSS 22.0 software, and measurement data were expressed as means and their 95% confidence intervals (95% CI). Hardy-Weinberg equilibrium was evaluated by comparing the observed and expected genotype distributions using the χ2 goodness-of-fit test. Allelic distributions and genotypes of HTR1A gene polymorphisms were tested using the χ2 test. The distributional differences between genotypes in the level of treatment effectiveness achieved by patients were analyzed using the Fisher-exact test for negative symptoms, positive symptoms, and pathologic symptoms. Comparison of psychotropic plasma concentration data between genotypes was performed by t-test for each follow-up period. Differences were considered statistically significant at P < 0.05, and withdrawal and shedding cases were not included in the statistical analysis.
Results
Study Population Characteristics and Hardy-Weinberg Equilibrium for Polymorphisms
A total of 140 male patients with schizophrenia were enrolled in this study. The socio-demographic characteristics of the included patients are listed in Table 1 with a mean age of 29.7 years (95% CI, 28.1–31.3) and the mean age at disease onset of 23.4 years (22.1–24.8). The majority of patients accepted elementary school and above education with 48.6% having a high school education or higher and were unmarried (79.3%). More than two-thirds of patients (72.1%) were in relapse. Over one-third of subjects (34.3%) were taking quetiapine and 22.9% were risperidone with the mean doses used in quetiapine and risperidone medicated patients being 540.4 mg/d and 4.7 mg/d; aripiprazole single-administration patients accounted for 13.6%, and the average dose used was 45.7 mg/d; olanzapine single-administration patients accounted for 11.4%, and the average dose was 24.3 mg/d; clozapine single-administration patients accounted for 3.6%, and the average dose was 135 mg/d, paliperidone single-administration patients accounted for 9.3%, and the average dose was 8.5 mg/d, and ziprasidone single-administration 2.9% of patients with a mean dose of 105 mg/d, and amisulpride monotherapy 2.1% of patients with a mean dose of 466.7 mg/d. The detailed baseline characteristics of the study cohort are presented in Supplementary Table 1. All SNPs were in Hardy-Weinberg equilibrium (P = 0.855 for rs10042486, and P = 0.947 for rs6295) (Table 2).
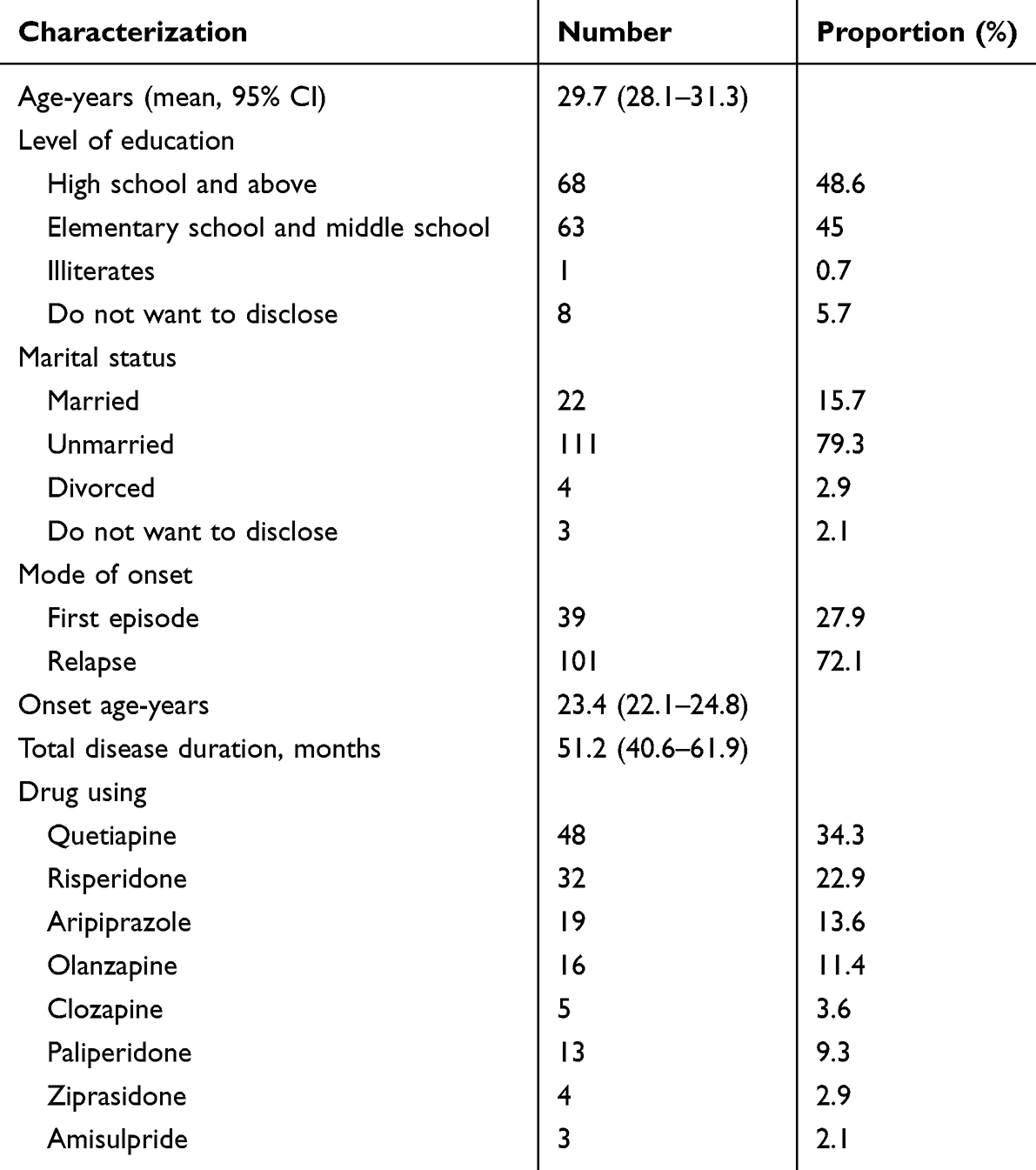 |
Table 1 Characterizations of Study Population |
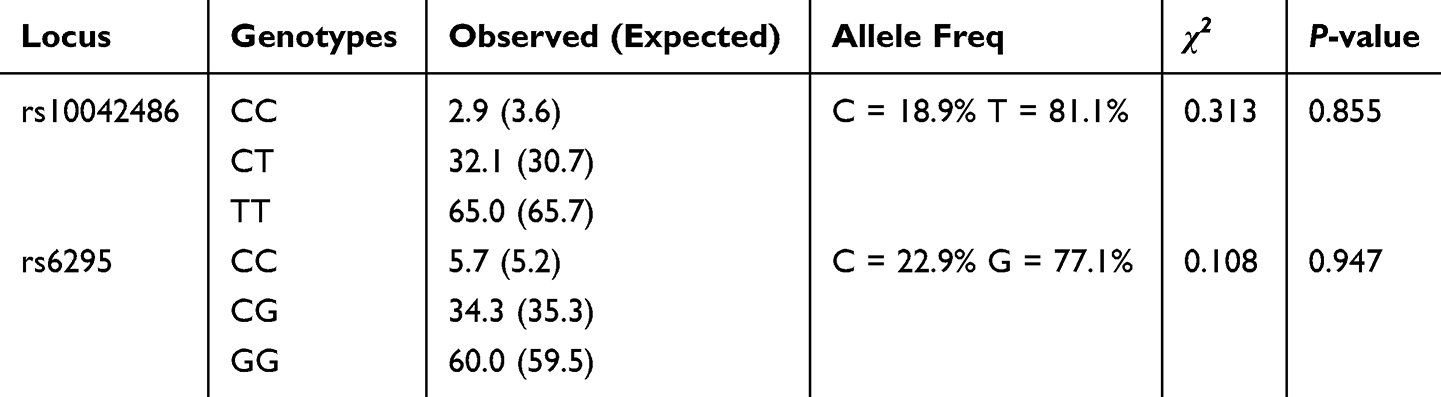 |
Table 2 Genotype Distribution of the HTR1A Gene and the Hardy-Weinberg Equilibrium Testing |
Relationship Between Polymorphisms of HTR1A and Response to Treatment
In order to investigate the association of treatment efficacy with rs6295 and rs10042486 within HTR1A, we evaluated the severity of symptoms of the patients using PANSS scale. The difference in PANSS scores between genotypes of rs6295 and rs10042486 was not statistically significant from baseline to 12 weeks of follow-up (Supplementary Table 2). In addition, there were no significant differences between genotypes of HTR1A rs6295 and rs10042486 with regard to efficacy assessed by PANSS except for rs6295 at week 12 posttreatment when evaluated by PANSS negative subscale (Table 3). Particularly, patients with the CG genotype (83.3%) in the rs6295 locus, compared to those with the CC and GG genotypes, exhibit more response rate in negative symptoms after 12 weeks of treatment (P = 0.037) (Table 3).
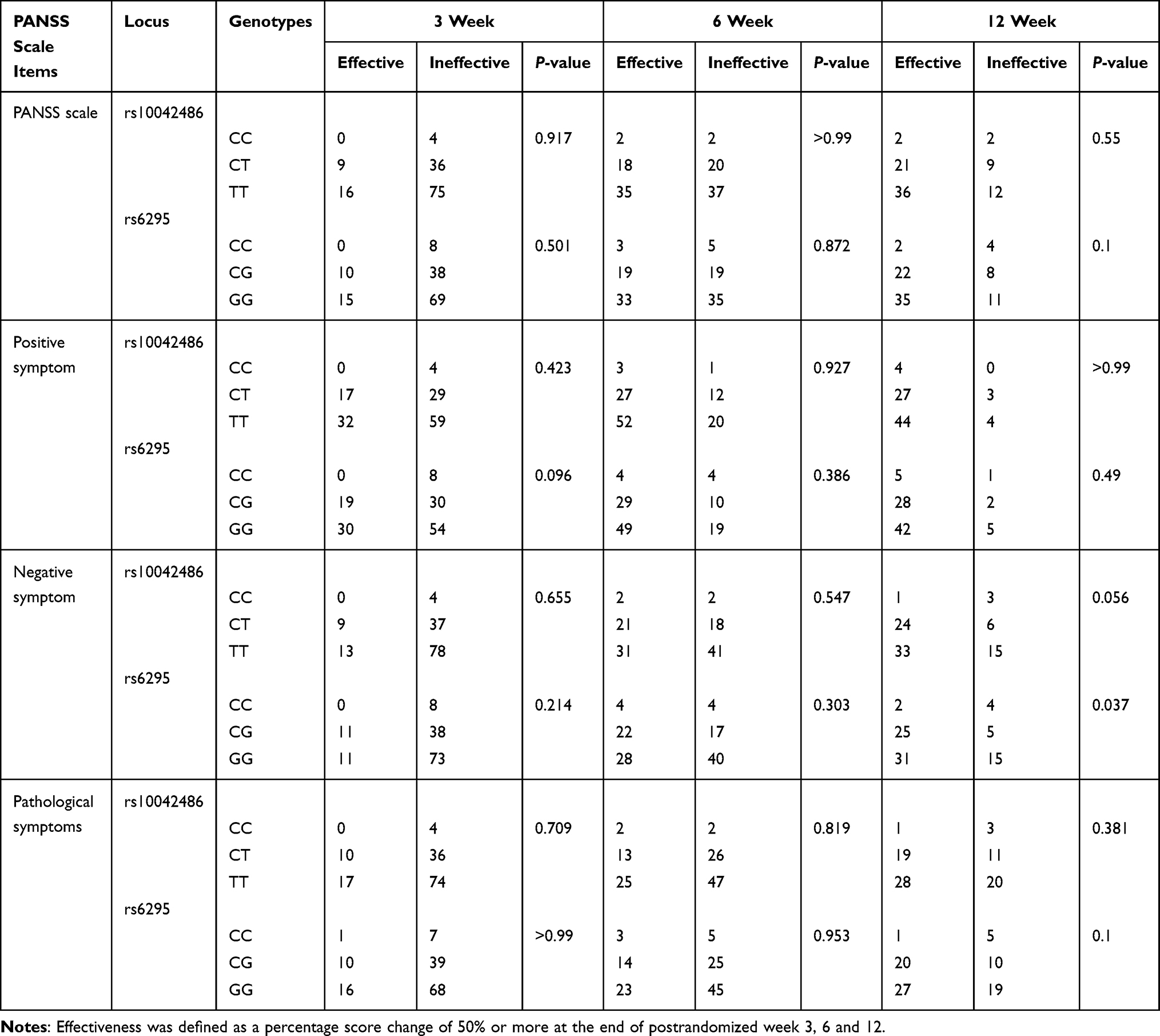 |
Table 3 Treatment Efficacy at 3, 6, and 12 Weeks for Each HTR1A Genotype Based on PANSS Total and Subscale Analyses |
Association of Plasma Concentration Changes in Quetiapine and Risperidone with HTR1A Polymorphisms
Wild-type and heterozygous mutant genotypes receiving quetiapine monotherapy had decreased plasma concentrations at weeks 6 and 12 compared with postrandomized week 3. In contrast, heterozygous mutations showed an alternating trend from decreasing to increasing. Plasma concentrations of the TT genotype at rs10042486 locus were significantly higher than those of the CT genotype at postrandomized week 6 (t = 3.126, P = 0.005). Similarly, the rs6295 locus GG genotype had significantly higher plasma concentrations than the CG genotype (t = 2.877, P = 0.008). However, there were no statistically significant differences between the genotypes at weeks 3 and 12 of treatment.
In patients receiving risperidone monotherapy, plasma concentrations in patients with the wild-type genotype showed a decreasing and then increasing pattern, whereas those patients with the mutant homozygous showed an increasing trend from week 3 to week 12. At the end of week 6, plasma concentrations were lower in the wild type than in the mutant heterozygous and homozygous mutant genotypes. There was no statistically significant difference in plasma concentrations between genotypes at the rs10042486 locus and a statistically significant difference in plasma concentration between genotypes at the rs6295 locus (t = 2.113, P = 0.048) (Table 4).
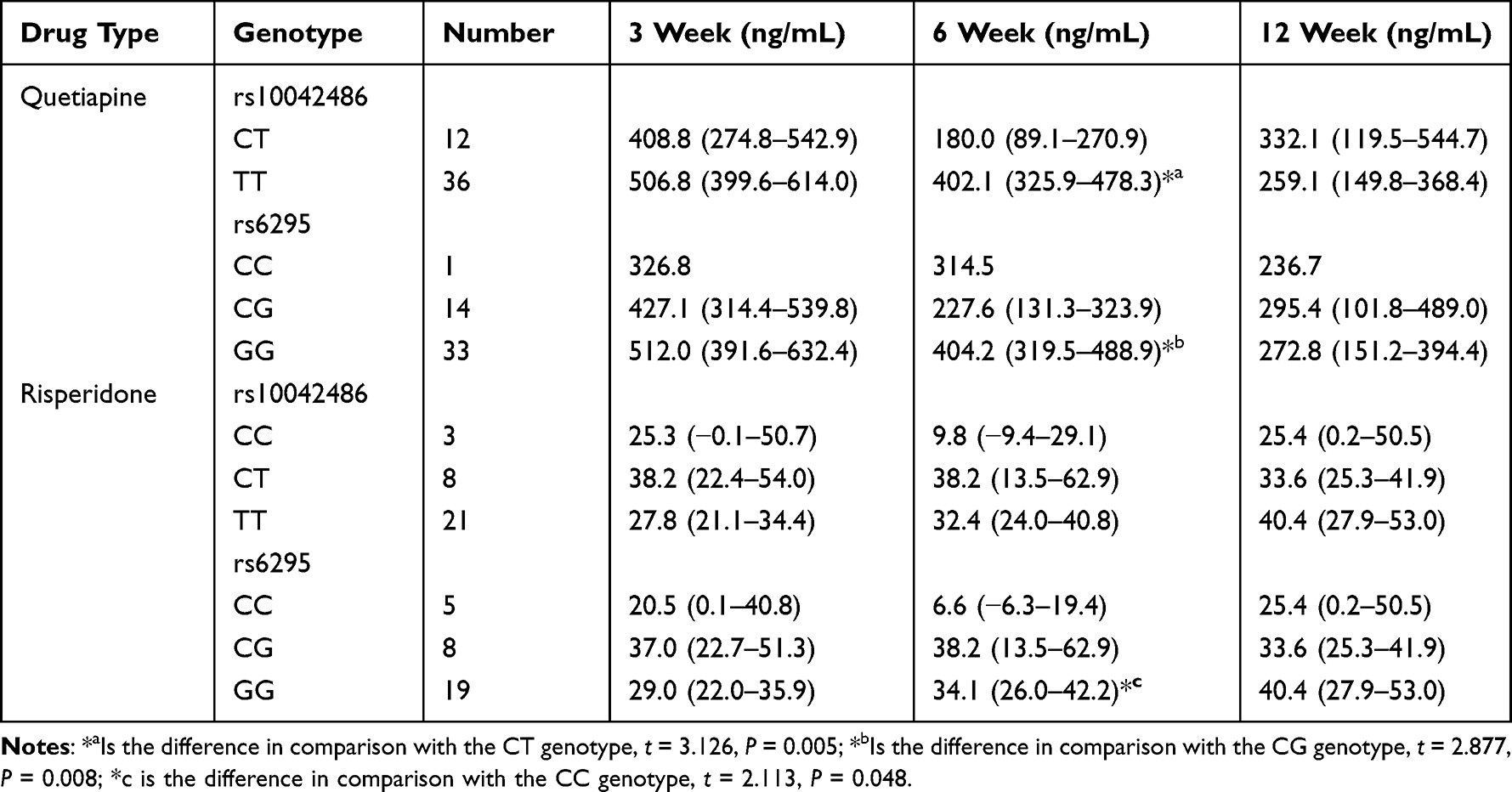 |
Table 4 Plasma Concentrations of Quetiapine and Risperidone After 3, 6, and 12 Weeks in Patients with Different Genotypes of the HTR1A |
Discussion
To our knowledge, this study is the first to report differences in risperidone plasma concentrations and treatment response in subjects with heterozygous or homozygous mutations in HTR1A. First, we found that the distribution of genotypes at the rs10042486 and rs6295 locus of the HTR1A gene conformed to Hardy-Weinberg equilibrium. The differences between genotypes were not statistically significant (P > 0.05), which means that the population studied was genetically balanced and representative of the population. In addition, the genotypes of the rs10042486 locus and the rs6295 locus were predominantly homozygous mutant, accounting for 65.0% and 60.0%, respectively, which is similar to the results of a previous study.14 Among the genotypes associated with improvement of negative symptoms, mutation heterozygosity showed the best improvement (Table 3). Previous studies have shown that polymorphisms in the HTR1A gene may affect the efficacy and side effects of antipsychotic drugs.16,19 Genetic polymorphisms in drug-metabolising enzymes and drug targets influence drug response, possibly by affecting pharmacokinetics, which may include absorption, distribution, metabolism and elimination of the drug; and pharmacodynamics, which is the therapeutic response of the drug target to the drug.20–22 Therefore, the detection of HTR1A genotype could be helpful in assessing the risk and efficacy of medication at the early stage of medication administration.
Accurate selection of drug and dose is a challenge due to variations in individual genotypes, as patients may experience a variety of side effects such as drowsiness, dizziness, weight gain, insomnia, and tremor with the same dose.23–25 Regular monitoring of plasma concentrations and dosage adjustments of drugs can help to reduce side effects in patients.26 In the present study, we found that HTR1A polymorphisms significantly affected the plasma concentrations of quetiapine versus risperidone, especially at week 6 after monotherapy. This suggests that when taking quetiapine or risperidone as a monoadministration, patients need to be regularly monitored for changes in plasma concentrations, especially in the sixth week of treatment, in order to prevent the occurrence of toxicity due to high plasma concentrations in carriers of the TT phenotype at the rs10042486 locus and the GG phenotype at the rs6295 locus, or plasma concentrations lower than the therapeutic reference concentration range occurring in carriers of the CC phenotype at the rs10042486 locus and the CC genotype at the rs6295 locus.
The differences in plasma concentrations between HTR1A genotypes were probably due to mutations at the rs6295 and rs10042486 locus resulting in reduced gene activity or defective post-receptor signalling, which led to the drug plasma concentrations to be increased. Whether the difference in plasma concentration between genotypes was responsible for the difference in negative symptom improvement was not further explored in this study. Previous studies have focused on the effects of metabolism or toxicity-related genes on patient efficacy or side effects, and few studies have focused on the influence of responsive genes on plasma concentrations.27,28 Analysis of HTR1A gene polymorphisms may help to stratify different subgroups of patients with psychiatric disorders (especially those with significant negative symptoms) and thus provide targeted individualised treatment.
In conclusion, this study found for the first time that polymorphisms at the rs10042486 and rs6295 loci of the HTR1A gene may be associated with efficacy and plasma concentrations in male schizophrenic patients. There are still many limitations of this study, such as small sample size and unsystematic grouping of medication regimens, which restricted us from further analysing the pattern of plasma concentration changes in patients and the most suitable single medication regimen for patients based on genetic polymorphisms.
Abbreviations
PANSS, The Positive and Negative Syndrome Scale; ICD-11, The International Classification of Diseases 11th Revision; MALDI-TOF MS, Matrix-assisted laser desorption ionization-time-of-light mass spectrometry; TDM, Therapeutical drug monitoring; LC-MS, Liquid chromatography and mass spectrometry instrument; CI, Confidence intervals.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and was approved by the ethics committee of clinical trial ethics committee of the Second People’s Hospital of Guizhou Province. Written informed consent was obtained from all individuals included in the study.
Acknowledgments
The authors wish to thank Shanghai Conlight Medical Co., Ltd. for technical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by Science and Technology Fund Project of Guizhou Provincial Health Committee gzwkj 2022-066 and Guizhou Provincial Key Technology R&D Program [2020]4Y064.
Disclosure
Jingfeng Tong and Chengchen Huang are affiliated with Shanghai Conlight Medical Co., Ltd. The authors declare no other conflicts of interest in this work.
References
1. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)
2. Weyant C, Brandeau ML, Basu S. Personalizing Medical Treatment Decisions: integrating Meta-analytic Treatment Comparisons with Patient-Specific Risks and Preferences. Med Decis Mak. 2019;39(8):998–1009. doi:10.1177/0272989X19884927
3. Dev R, Li J, Zhang D, et al. An economic evaluation of a mobile text messaging intervention to improve mental health care in resource-poor communities in China: a cost-effectiveness study. BMC Health Serv Res. 2020;20(1):989. doi:10.1186/s12913-020-05855-6
4. Nayak R, Rosh I, Kustanovich I, Stern S. Mood Stabilizers in Psychiatric Disorders and Mechanisms Learnt from In Vitro Model Systems. Int J Mol Sci. 2021;22(17):9315. doi:10.3390/ijms22179315
5. Guan F, Lin H, Chen G, et al. Evaluation of association of common variants in HTR1A and HTR5A with schizophrenia and executive function. Sci Rep. 2016;6(1):38048. doi:10.1038/srep38048
6. Ng IS, Chua J, Lui Y, Tan L, Teo DS. Approach to acute psychosis in older adults. Singapore Med J. 2023;64(6):391. doi:10.4103/singaporemedj.SMJ-2022-150
7. Lodge D, Perez S. New approaches to the management of schizophrenia: focus on aberrant hippocampal drive of dopamine pathways. Drug Des Devel Ther. 2014;887. doi:10.2147/DDDT.S42708
8. Chilmonczyk Z, Bojarski A, Pilc A, Sylte I. Functional Selectivity and Antidepressant Activity of Serotonin 1A Receptor Ligands. Int J Mol Sci. 2015;16(8):18474–18506. doi:10.3390/ijms160818474
9. Haleem DJ. 5-HT1A receptor-dependent control of nigrostriatal dopamine neurotransmission in the pharmacotherapy of Parkinson’s disease and schizophrenia. Behav. Pharmacol. 2015;26:45–58. doi:10.1097/FBP.0000000000000123
10. Mlambo R, Liu J, Wang Q, Tan S, Chen C. Receptors Involved in Mental Disorders and the Use of Clozapine, Chlorpromazine, Olanzapine, and Aripiprazole to Treat Mental Disorders. Pharmaceuticals. 2023;16(4):603. doi:10.3390/ph16040603
11. Riga MS, Lladó-Pelfort L, Artigas F, Celada P. The serotonin hallucinogen 5-MeO-DMT alters cortico-thalamic activity in freely moving mice: regionally-selective involvement of 5-HT1A and 5-HT2A receptors. Neuropharmacology. 2018;142:219–230. doi:10.1016/j.neuropharm.2017.11.049
12. Filip M, Bader M. Overview on 5-HT receptors and their role in physiology and pathology of the central nervous system. Pharmacol Rep. 2009;61(5):761–777. doi:10.1016/S1734-1140(09)70132-X
13. Asad S, Nikamo P, Gyllenberg A, et al. HTR1A a Novel Type 1 Diabetes Susceptibility Gene on Chromosome 5p13-q13. PLoS One. 2012;7(5):e35439. doi:10.1371/journal.pone.0035439
14. Takekita Y, Fabbri C, Kato M, et al. HTR1A Gene Polymorphisms and 5-HT1A Receptor Partial Agonist Antipsychotics Efficacy in Schizophrenia. J Clin Psychopharmacol. 2015;35(3):220–227. doi:10.1097/JCP.0000000000000304
15. Bosia M, Lorenzi C, Pirovano A, et al. COMT Val158Met and 5-HT1A-R −1019 C/G polymorphisms: effects on the negative symptom response to clozapine. Pharmacogenomics. 2015;16(1):35–44. doi:10.2217/pgs.14.150
16. Takekita Y, Fabbri C, Kato M, et al. HTR1A Polymorphisms and Clinical Efficacy of Antipsychotic Drug Treatment in Schizophrenia: a Meta-Analysis. Int J Neuropsychopharmacol. 2016;19(5):pyv125. doi:10.1093/ijnp/pyv125
17. Yoshikawa A, Li J, Meltzer HY. A functional HTR1A polymorphism, rs6295, predicts short-term response to lurasidone: confirmation with meta-analysis of other antipsychotic drugs. Pharmacogenomics J. 2020;20(2):260–270. doi:10.1038/s41397-019-0101-5
18. Mössner R, Schuhmacher A, Kühn KU, et al. Functional serotonin 1A receptor variant influences treatment response to atypical antipsychotics in schizophrenia. Pharmacogenet Genomics. 2009;19(1):91–94. doi:10.1097/FPC.0b013e328311a917
19. De Deurwaerdère P, Di Giovanni G. Serotonin in Health and Disease. Int J Mol Sci. 2020;21(10):3500. doi:10.3390/ijms21103500
20. Zhong X, Tong X, Ju Y, Du X, Li Y. Interpersonal Factors in the Pharmacokinetics and Pharmacodynamics of Voriconazole: are CYP2C19 Genotypes Enough for Us to Make a Clinical Decision? Curr Drug Metab. 2018;19(14):1152–1158. doi:10.2174/1389200219666171227200547
21. Amalinei C. Current Knowledge and Novel Therapeutic Approaches Based on Pharmacokinetics and Pharmacodynamics in Stress-Induced Pathology. Medicina. 2022;58(7):839. doi:10.3390/medicina58070839
22. Franczyk B, Rysz J, Gluba-Brzózka A. Pharmacogenetics of Drugs Used in the Treatment of Cancers. Genes. 2022;13(2):311. doi:10.3390/genes13020311
23. Johnson BO, Orji G, Johnson OO, et al. Rebound Catatonia Associated With Injectable Paliperidone. Cureus. 2023. doi:10.7759/cureus.40478
24. Efron D, Dale RC. Tics and Tourette syndrome. J Paediatr Child Health. 2018;54(10):1148–1153. doi:10.1111/jpc.14165
25. Sugawara Kikuchi Y, Shimizu T. Aripiprazole for the treatment of psychotic symptoms in patients with dementia with Lewy bodies: a case series. Neuropsychiatr Dis Treat. 2019;15:543–547. doi:10.2147/NDT.S189050
26. Xu X, Li S, Luan X, et al. Sensitivity enhancement of a Cu (II) metal organic framework-acetylene black-based electrochemical sensor for ultrasensitive detection of imatinib in clinical samples. Front Chem. 2023:11. doi:10.3389/fchem.2023.1191075
27. Zhang L, Brown SJ, Shan Y, et al. CYP2D6 Genetic Polymorphisms and Risperidone Pharmacokinetics: a Systematic Review and Meta‐analysis. Pharmacotherapy. 2020;40(7):632–647. doi:10.1002/phar.2434
28. Jukic MM, Smith RL, Haslemo T, Molden E, Ingelman-Sundberg M. Effect of CYP2D6 genotype on exposure and efficacy of risperidone and aripiprazole: a retrospective, cohort study. Lancet Psychiatry. 2019;6(5):418–426. doi:10.1016/S2215-0366(19)30088-4
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Switching Clozapine to Cariprazine in Three Patients with Persistent Symptoms of Schizophrenia: A Case Series
Duque-Yemail JD, Avila JC
Neuropsychiatric Disease and Treatment 2022, 18:1433-1440
Published Date: 13 July 2022
Glutathione S-Transferase M1/T1 Polymorphisms and Schizophrenia Risk: A New Method for Quality Assessment and a Systematic Review
Liu H, Xu Y, Peng J
Neuropsychiatric Disease and Treatment 2023, 19:97-107
Published Date: 7 January 2023