Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Glutathione S-Transferase M1/T1 Polymorphisms and Schizophrenia Risk: A New Method for Quality Assessment and a Systematic Review
Received 12 July 2022
Accepted for publication 28 November 2022
Published 7 January 2023 Volume 2023:19 Pages 97—107
DOI https://doi.org/10.2147/NDT.S376942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Hongzhou Liu,* Ying Xu,* Jie Peng
School of Clinical Medicine, The First Affiliated Hospital of Chengdu Medical College, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie Peng, Email [email protected]
Background: GST genes were reported to be involved in susceptibility to mental disorder. The results between deletions of GST genes and schizophrenia were inconclusive and confusing. Therefore, we performed this updated meta-analysis to outline the association using a new method for quality assessment.
Methods: Sixteen reported studies were selected, and the overall OR and 95% CI were calculated and analyzed by Review Manager 5.4 and STATE 12. The Newcastle-Ottawa Quality Assessment Scale (NOS) for case–control studies was rewritten to evaluate the quality of published studies, as there was no “Exposure” in these studies and other factors should be suggested to assess the quality.
Results: There was no significant association between deletions of GST genes and SZ risk (p > 0.05 in Random model). We also failed to find a significant relation between null genotypes and SZ risk in East Asian population. Based on further analysis of PCR methods, GSTM1 null was weakly associated with SZ risk in 8 studies using multiplex PCR (OR = 1.17, 95% CI = 1.00– 1.37, p = 0.05), but GSTT1 null was a protective factor for SZ risk (OR = 0.73, 95% CI = 0.56– 0.94, p = 0.02). When stratified by rewritten NOS stars and deductions, GSTM1 null was significantly associated with SZ risk in 9 studies with high quality (OR = 1.24, 95% CI = 1.08– 1.43, p = 0.002), and in 10 studies with no deductions (OR = 1.20, 95% CI = 1.05– 1.38, p = 0.007).
Conclusion: GSTM1 null genotype may be a genetic risk factor for SZ in studies using multiplex PCR and high-quality studies. However, GSTT1 null might be a protective factor. Besides, we provided a new method for quality assessment and it was useful and should be promoted in further analysis.
Keywords: glutathione S-transferase T1, GSTM1, polymorphism, schizophrenia, meta-analysis
Introduction
Schizophrenia (SZ) is a severe psychiatric disorder characterized by abnormal behavior and altered reality.1 The chronic psychotic symptoms have a profound impact on patients with SZ, and the average life expectancy is 10–20 years shorter than the general population.2 Despite the efforts of researchers, treatment for SZ remains limited, and the therapeutic targets have not expanded for decades.3 Our poor understanding of the neurobiological underlines of mental disorder results in limited treatment. Although many studies suggested that both genetic polymorphisms and environmental factors were implicated in the susceptibility and etiology of SZ, SZ was a highly heritable disease.4–6 Some GWAS studies with large participants probed that some genetic variants were related to SZ risk, including copy number variation (CNV) at 22q11.2.7,8 Therefore, null genotypes of glutathione S-transferases (GST) genes might be well suited for exploring the association with SZ.
Glutathione S-transferases (GSTs) are a family of Phase II metabolic isozymes, which code by glutathione S-transferase mu 1 (GSTM1), glutathione S-transferase theta-1 and theta-2 (GSTT1 and T2), glutathione S-transferase pi-1 (GSTP1), and glutathione S-transferase omega-1 (GSTO1).5 GSTM1 is located at 1p13.3, and GSTT1 is situated at 22q11.23. Deletion of the entire gene results in a lack of enzymatic activity and may cause upregulation of oxidative stress.4 Homozygous deletions of GSTM1 or GSTT1 have also been reported in various diseases, including SZ, cancer, and vascular disease.6,9,10
They are one of the key enzymes in the converting toxic compounds into hydrophilic metabolites for detoxification, and they play a crucial role in protecting neural cells from oxidative stress.6 GSTs are regarded as neuro-protective antioxidants, and some reported results showed that the GSTs levels were decreased in cerebrospinal fluid of SZ patients.11 This suggested that GSTs might be involved in the susceptibility and progression of SZ. Currently, a number of studies had found GSTM1 and GSTT1 polymorphisms to be associated with SZ risk, but some other studies were failed to find this association.12–27 Antioxidants impairment and oxidative damage could account for the positive results, while other enzymes completely reducing the effects of GST deletion might be responsible for the negative results. However, some studies showed that GSTM1 null genotype was reduced in SZ patients, and a protective effect of GSTT1 null genotype had also been observed. These results were confusing and required to re-analysis. Besides, case–control study about genetic polymorphisms needed to be assessed for quality using new methods. Therefore, we performed this meta-analysis on case–control studies using a new method for quality assessment. This was the first attempt to assess the quality of genetic study.
Materials and Methods
Search Strategy
PubMed and Chinese national knowledge infrastructure (CNKI) were selected and the keywords “schizophrenia”, “GSTT1”, “GSTM1”, “glutathione S-transferase”, “glutathione S-transferase T1”, “glutathione S-transferase M1”, and “polymorphism” were used for searching. All relevant studies from 1990 to March 2022 were included with no restriction.
Inclusion and Exclusion Criteria
All the studies should be complied with the following criteria: (1) The patients of studies must be schizophrenia; (2) The literatures should be the association studies included risk of SZ and GST genes; (3) Only case–control studies were considered; (4) The papers should provide sample size, OR values, and 95% CI or provide the related information such as genotype frequencies. Other studies would be excluded: (1) no healthy controls or case-only studies; (2) overlapped studies; (3) the articles are reviews; (4) studies without useful data, including genotype frequencies.
Study Selection and Data Extraction
According to pre-established criteria of inclusion and exclusion, a double-check procedure was performed to make sure the accuracy of the data entry. The following information was extracted from the studies and listed in Table 1: first author, published year, population, the data of total and exposure number in case and control groups. Other information was also collected and assessed by rewritten NOS in Supplementary Table S1, consisting of PCR method and PCR control, source of the controls, diagnostic criteria, subgroup analysis, age and gender of cases and controls, age of onset years, Hardy-Weinberg equilibrium (HWE) tests of CNVs, and deductions. Two reviewers were invited, and a standardized procedure was performed independently. Scores of studies were summarized in Supplementary Table S1.
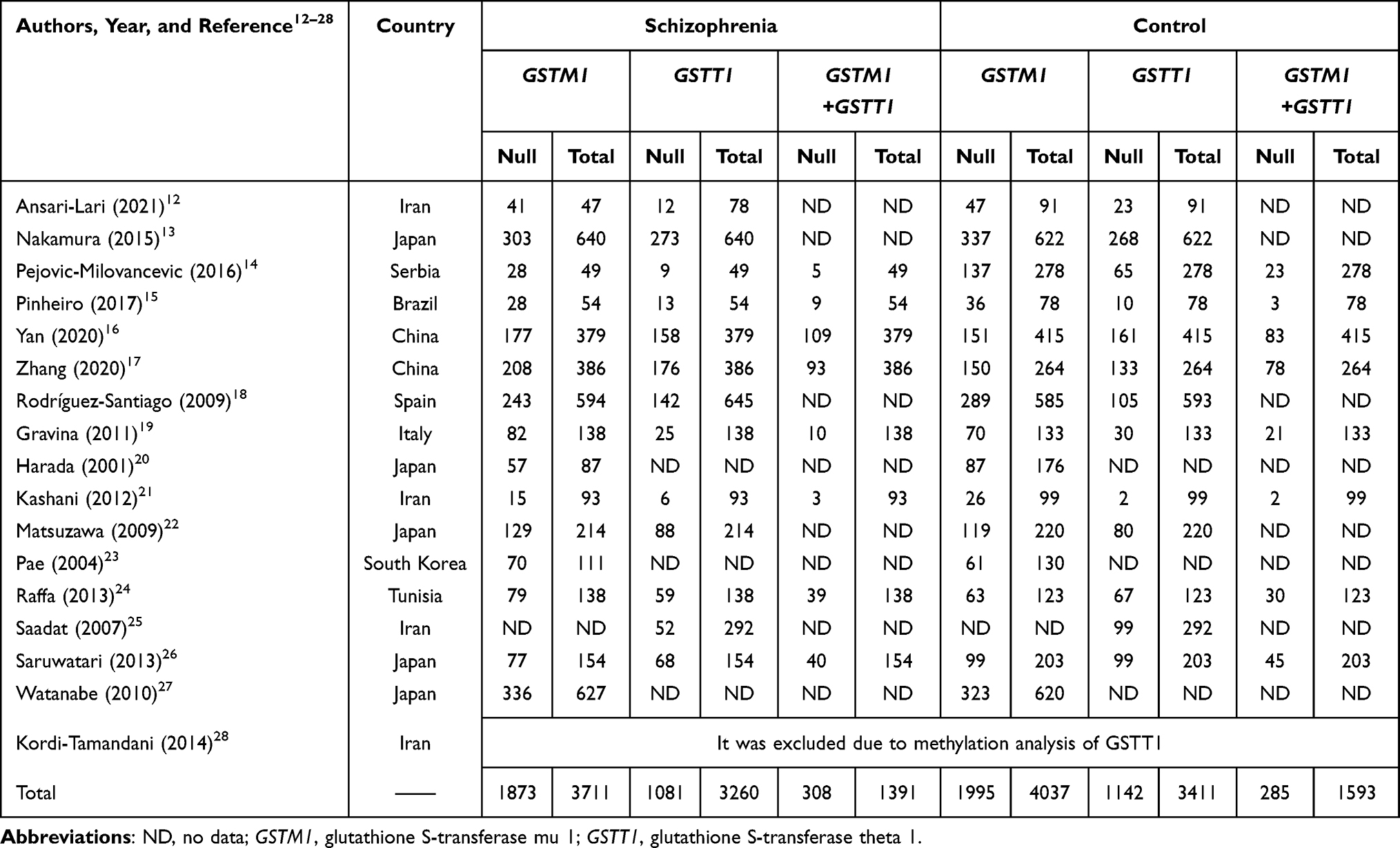 |
Table 1 Data Extraction of Eligible Studies Included in the Meta-Analysis |
Quality Assessment and Rewritten NOS
All studies were assessed using Newcastle-Ottawa quality assessment scale (NOS) rewritten by us in the Supplementary Table S2. The “Exposure” was deleted and items of “Methodology” and “Deductions” were added in rewritten NOS (reNOS). PCR methods, PCR controls, subgroup analysis, Hardy-Weinberg equilibrium (HWE), and age of onset years were included in item of “Methodology”. Deductions were defined by inconsistent data or incorrect descriptions, which would affect the quality score of studies. Studies with 6–10 stars or no deduction were indicated high-quality studies. The detail information and obtained stars of 16 studies were shown in the Supplementary Table S1.
Statistical Analysis Methods
Statistical analysis was done by using Review Manager 5.4 and STAT 12. Total OR and 95% CI were calculated to explore the strength of association between GSTM1/T1 null genotypes and schizophrenia. Q test was performed to check heterogeneity, and the heterogeneity was considered significant when p<0.10.4 The fixed effect model was used when p>0.10; otherwise, a random effect model was selected. Subgroup analysis was used to evaluate the source of bias. The funnel plot was used to detect publication bias. Egger’s test and Begg’s test were also selected to test publication bias. The sensitivity analysis was performed by deleting studies to assess the pooled results. All the tests were two-sided, and a p value of 0.05 for any test or model was considered to be statistically significant.
Results
Characteristics of Studies
According to the search strategy, 16 papers are selected in Figure 1. Fifteen studies included 3742 cases and 4037 controls were selected in GSTM1. Thirteen studies related to GSTT1 included 3260 cases and 3411 controls. The data extraction of studies is shown in Table 1 and Supplementary Table S1. Stratification of studies by ethnicity, PCR methods, total stars and deductions based on the rewritten NOS is summarized in Table 2.
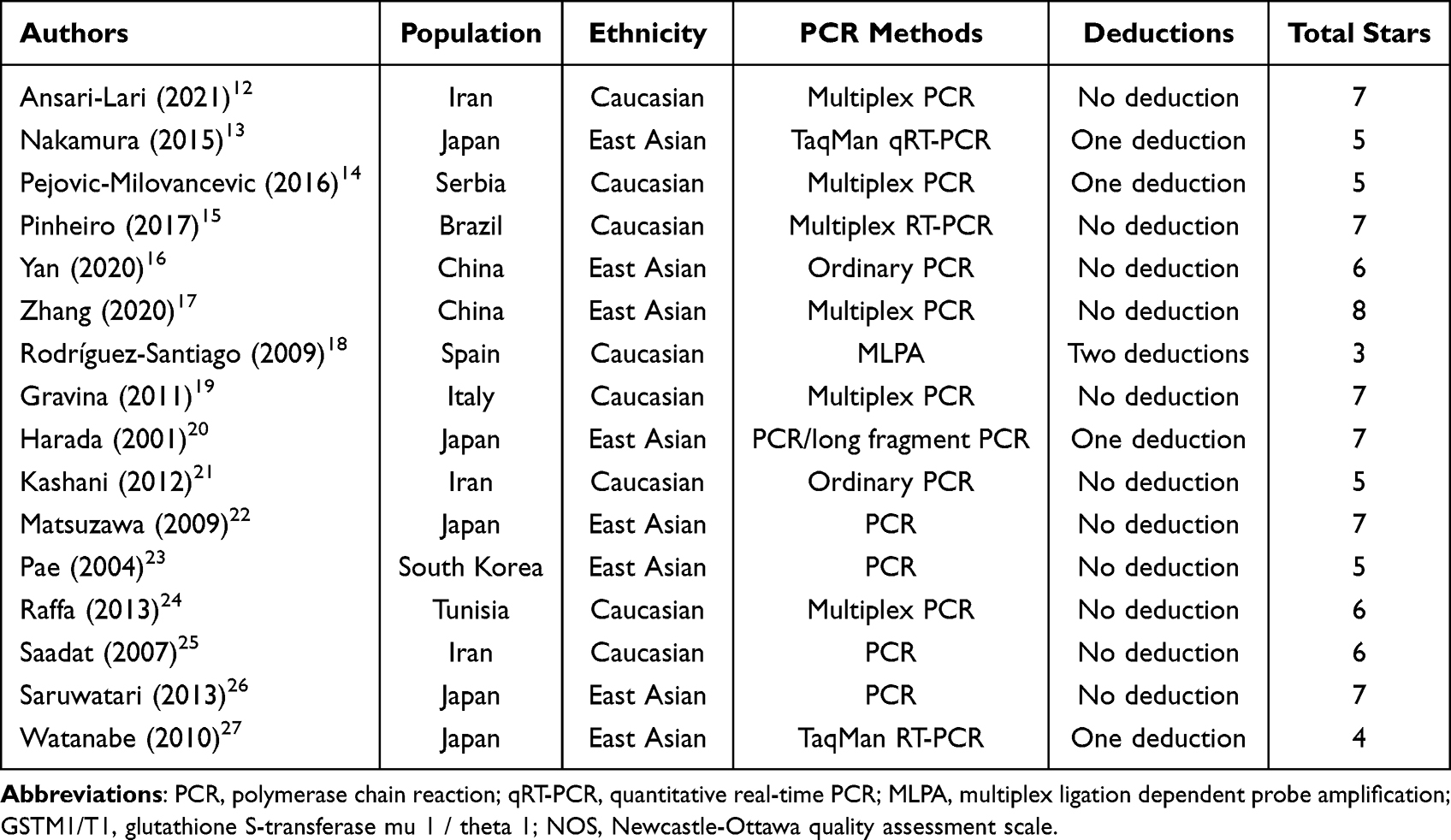 |
Table 2 Stratification of Studies by Ethnicity, PCR Methods, Total Stars and Deductions Based on the Rewritten NOS |
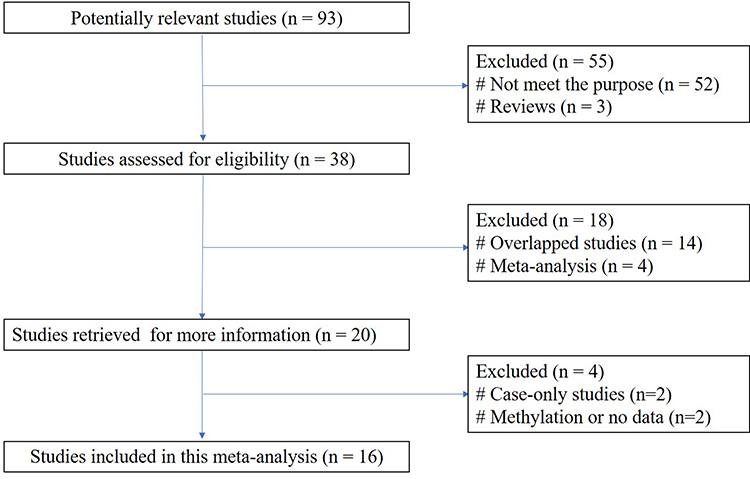 |
Figure 1 A flow diagram of the study selection process. |
Overall Results of Meta-Analysis
The overall results of heterogeneity assessed with Q test and I2 statistic are shown in Figure 2. The random-effect methods were selected due to p < 0.05 of Q test or I2 > 50%. As shown in Figure 2, there were no significant associations between deletions of GSTM1/T1 and SZ. Publication bias was investigated using funnel plot, and the shape of the funnel plot was symmetrical. The result of Egger’s test was p = 0.117, and Begg’s test was p = 0.073. No publication bias was observed in this meta-analysis. The sensitivity analysis performed by deleting studies showed that there were no changes in the overall results. This indicated that the bias had few effects on the overall results and the conclusion was robust.
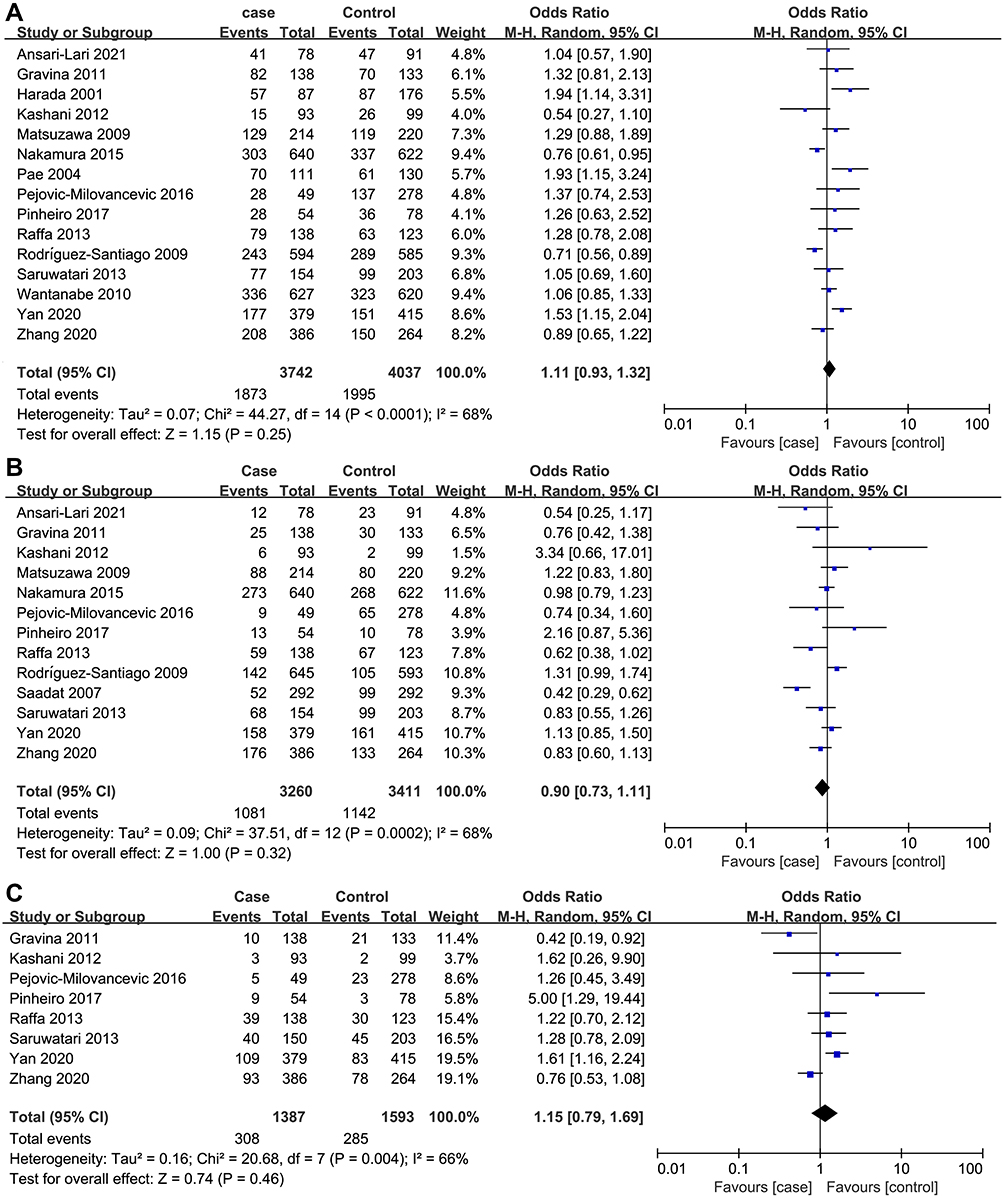 |
Figure 2 Forest plot of overall studies. (A) Analysis of null genotype vs present genotype of GSTM1. P = 0.25 [Overall OR = 1.11, 95% CI = (0.93–1.32)]. (B) Analysis of null genotype vs present genotype of GSTT1. P = 0.32 [Overall OR = 0.90, 95% CI = (0.73–1.11)]. (C) Analysis of null genotype vs present genotype of GSTM1 + GSTT1. P = 0.46 [Overall OR = 1.16, 95% CI = (0.79–1.69)]. |
Subgroup Results of Ethnicity
Stratification of studies by ethnicity is performed in Table 3. The results of East Asian were (OR = 1.19, 95% CI = 0.94–1.49, p = 0.15) for GSTM1 null, (OR = 0.99, 95% CI = 0.87–1.13, p = 0.89) for GSTT1 null and (OR = 1.16, 95% CI = 0.71–1.89, p = 0.56) for both deletions of GSTM1 and GSTT1 as shown in Table 3. No significant association was found in subgroup analysis of ethnicity. This result changed the inherent thinking that different races might provide diversity and race might not play an important role in this meta-analysis. Funnel plot and Egger’s test were used for evaluation of the publication bias, and no publication bias was observed (p > 0.05).
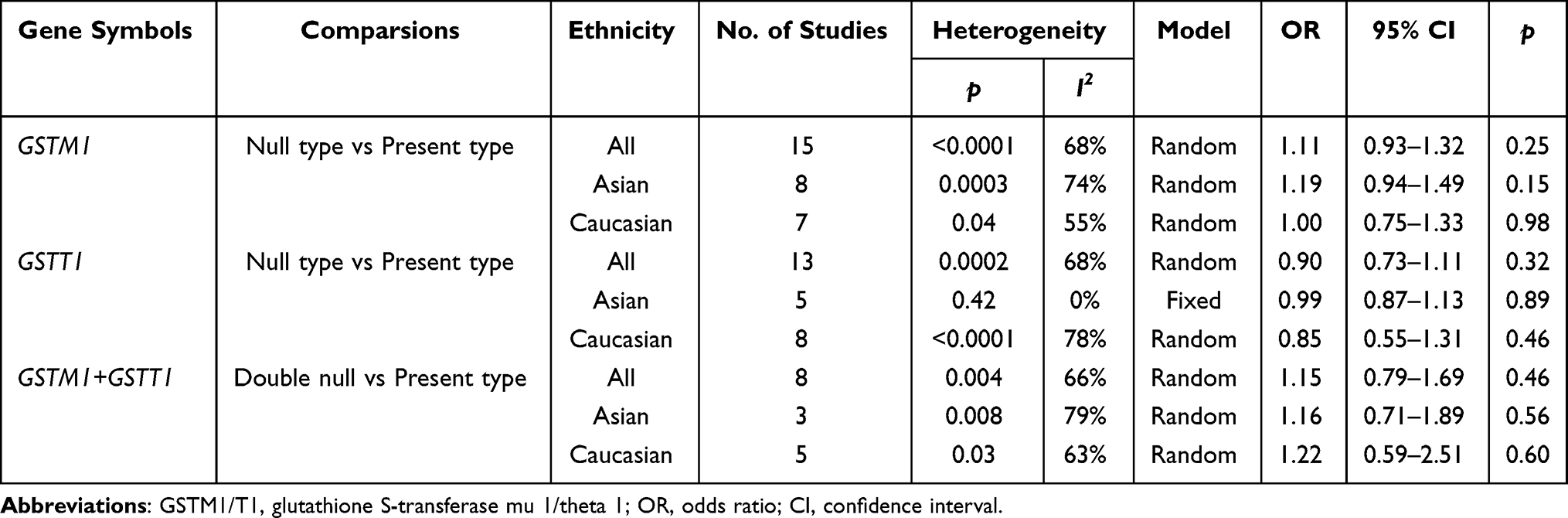 |
Table 3 Overall Analysis and Subgroup Analysis of Ethnicity |
Subgroup Results of PCR Methods
PCR method was not the criteria for quality assessment, but it was interesting to perform a sub-analysis due to judgement of genotype with same methods. However, the results should be interpreted carefully. Stratification of studies by PCR methods is performed in Table 4. When stratified for PCR methods of Multiplex PCR as shown in Table 4, GSTM1 null genotype showed weak association with risk of SZ (OR = 1.17, 95% CI = 1.00–1.37, p = 0.05). p = 0.05 should be interpreted with caution. Usually, we should re-analyze with a larger sample size, but this was a meta-analysis and difficult to re-analyze. We preferred to find a weak association in this section, and the positive results were more interesting. Surprisingly, there was a significant association between GSTT1 null genotype and the decreased risk of SZ (OR = 0.73, 95% CI = 0.56–0.94, p = 0.02). These results indicated that the GST genes played different roles in SZ patients and combination of GSTM1 null and GSTT1 present should be further researched. Besides, double null showed no relation with SZ in subgroup analysis of multiplex PCR (p > 0.05), but significant association was observed in subgroup analysis of other methods (OR = 1.73, 95% CI = 1.27–2.36, p = 0.0006). This positive result should be carefully interpreted due to only 3 included studies, and it might not be representative. As mentioned above, no publication bias was observed (p > 0.05).
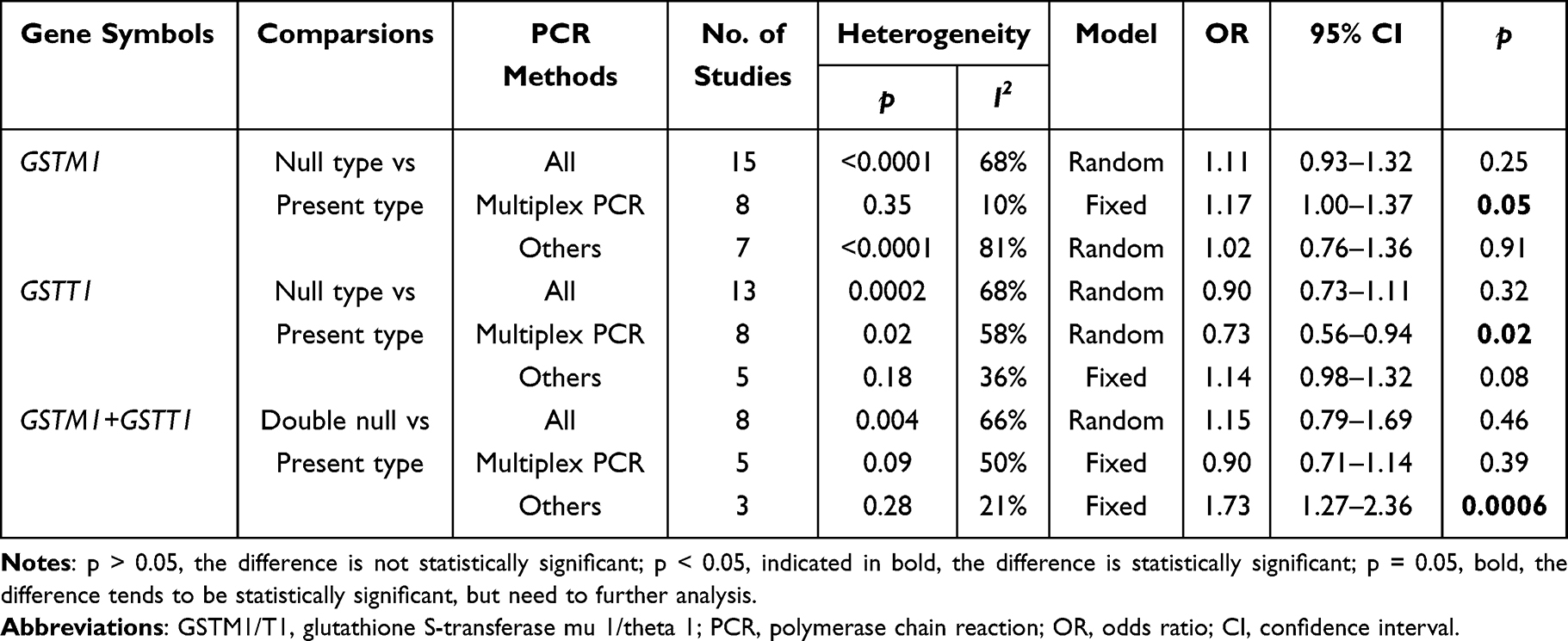 |
Table 4 Overall Analysis and Subgroup Analysis of PCR Methods |
Subgroup Results of NOS Stars and Deductions
Meta-analysis was an evidence-based method using reported studies, and study quality was a very important factor for making a conclusion. Therefore, we re-written the NOS scale for quality assessment and conducted the sub-analysis. The subgroup results of studies with 6–10 stars are listed in Table 5. GSTM1 null genotype showed a significant association with risk of SZ (OR = 1.24, 95% CI = 1.08–1.43, p = 0.002). This result revealed that we should pay more attention to the quality of studies and new assessment scale was needed for evaluation. However, there was no significant association between GSTT1 null genotype and SZ risk (p > 0.05), and double null genotypes also had no association with SZ (p > 0.05).
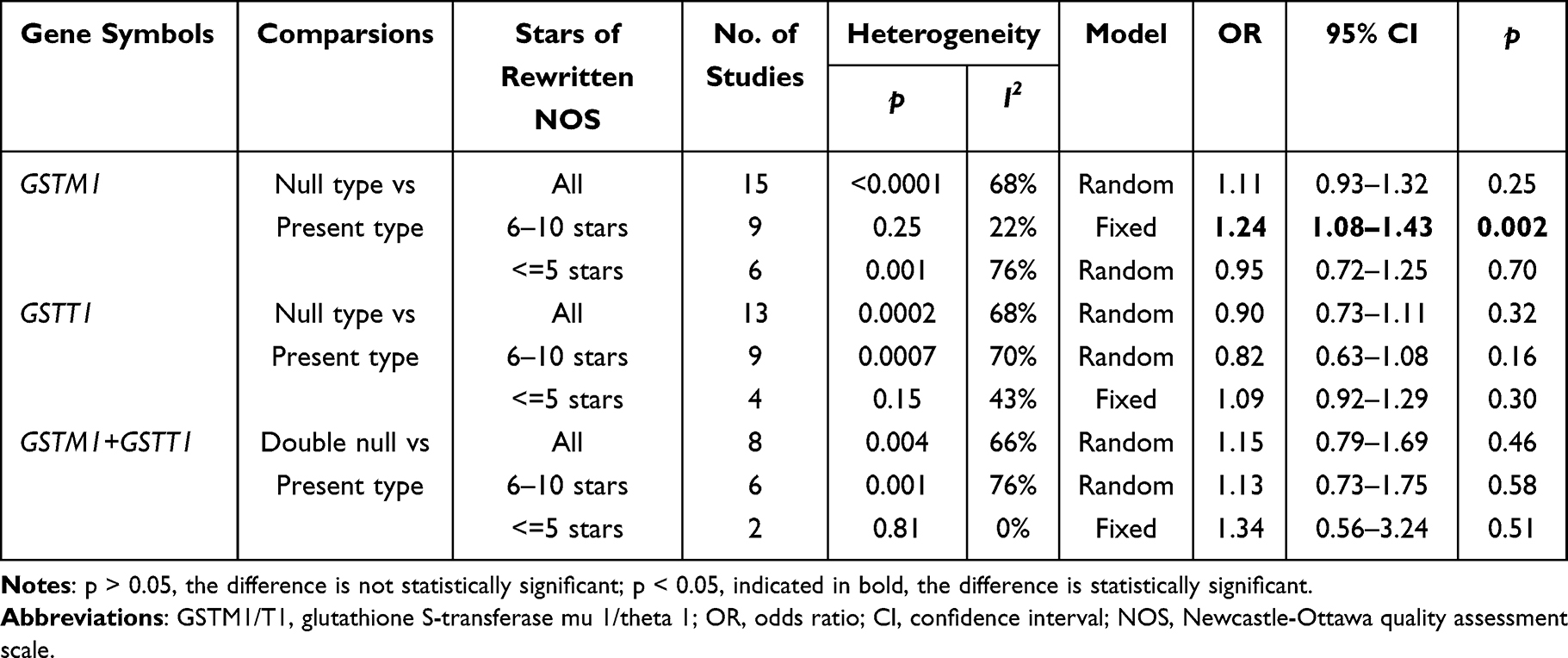 |
Table 5 Overall Analysis and Subgroup Analysis of Stars Obtained from NOS |
When stratified by no deductions as shown in Table 6, GSTM1 null genotype also showed significant association with risk of SZ (OR = 1.20, 95% CI = 1.05–1.38, p = 0.007). This result was consistent with subgroup analysis of high-quality studies in Table 5. Not surprisingly, GSTT1 null genotype was not related with SZ (p > 0.05), and double null genotypes were also not found to be associated with SZ (p > 0.05). Moreover, no publication bias was observed (p > 0.05).
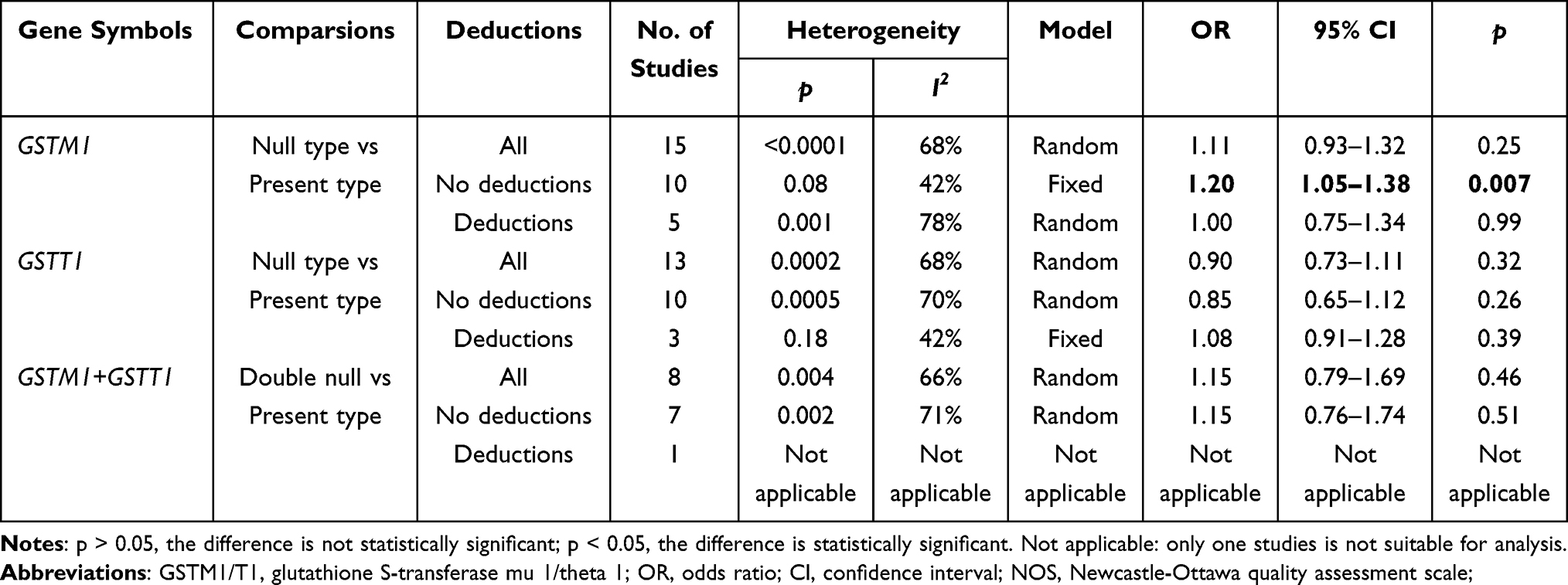 |
Table 6 Overall Analysis and Subgroup Analysis of Deductions Assessed Using Rewritten NOS |
Discussion
In our study, no significant association was observed between GSTM1/T1 null genotypes and SZ risk using a meta-analysis of total population. Further stratified analysis by ethnicity also suggested that deletions of GSTM1/T1 had no clear association with increased susceptibility to SZ. However, subgroup analysis of multiplex PCR revealed that GSTM1 null genotype had a weak association with risk of SZ. Interestingly, GSTT1 null genotype significantly reduced SZ risk in studies using multiplex PCR. When stratified by re-NOS stars and deductions, GSTM1 null was significantly associated with risk of SZ in high-quality studies. These results indicated that the quality of studies and methods of research should be paid more attention in further meta-analysis.
Up to now, some studies have evaluated the association between genetic deletion of GST genes and risk of SZ using meta-analysis.4–6,27 However, these published results remain conflicting and an updated meta-analysis is necessary for further assessment. Watanabe et al found a weak significant association between GSTM1 null genotype and SZ risk in Asian population.27 A significant association was also reported by Cai et al between GSTM1 null genotype and risk of SZ, but GSTT1 null genotype was related to the decreased risk of SZ.5 In another meta-analysis reported by Kim et al, they failed to find the association between GST genes and SZ. Subgroup analysis based on ethnicity showed that GSTM1 polymorphism had a weak association with SZ risk in East Asian population.4 Huang et al also reported that GSTM1 deletion was significantly associated with SZ.6 However, the literature included and data extraction were not consistent in these reported studies. Especially, the quality of included studies was not assessed. To identify them, we performed this updated meta-analysis using new method to re-analyze the association and provide new insight and improving perspective for further research.
As we all known, the distribution of GSTM1/T1 deletion is various in different populations. Nelson et al found that the frequency of GSTT1 null genotype was 64% in Asian, 28% in Caucasian, and 22% in African American population.28,29 Therefore, stratification of studies by ethnicity was usually used in meta-analysis. However, we failed to find the association between GST genes and risk of SZ in Asian population. These results suggested that subgroup analysis of ethnicity might be out of magic and other assessment methods of studies should be promoted. In the present studies, we performed stratified analysis of studies by PCR methods and rewritten NOS. When subgroup analysis of multiplex PCR, GSTM1 null showed a weak association with SZ risk, but GSTT1 null was a protective factor. These inconsistent results were interesting and needed to be interpreted with caution. The reason might be that the same PCR method used in the studies would be comparable and the judgement of genotype was less arbitrariness.
The quality assessment of reported studies was the highlights of this study. As shown in Supplementary Table S2, the NOS was rewritten and some important criteria were added for evaluation, including methodology domain and deduction domain. Deductions were defined by inconsistent data or incorrect descriptions, which would affect the quality score of studies. The detailed information was listed in the Supplementary Table S1. Meta-analysis was an evidence-based method using reported studies, and study quality was very important for making a conclusion. Therefore, we re-written the NOS scale for quality assessment and conducted the sub-analysis. The subgroup analysis of studies obtained 6–10 stars revealed that GSTM1 null genotype was significantly associated with risk of SZ. The result indicated that GSTM1 null was related to SZ risk in high-quality studies. Moreover, in studies with no deductions, GSTM1 null also showed a significant association with risk of SZ. The same conclusions were reached, and the consistent results were also indicated that study quality was very important and needed to be assessed. However, quality assessment of studies was missing and ignored in the reported meta-analysis. These results were very interesting and suggested that the included studies needed to be assessed for quality in further meta-analysis. Our study provided a new quality assessment method with the ability to discover potential associations.
The deficiency of GST enzymes causes by deletions of GSTM1/T1 could lead to the reduction of Glutathione (GSH).30–32 GSH is an important antioxidant, which detoxifies reactive oxygen species (ROS) in the central nervous system, and thus plays an important role in protecting neural tissues.33,34 GSH levels were significantly decreased in cerebrospinal fluid of SZ patients and proton magnetic resonance spectroscopy revealed a significant reduction of GSH in the medial prefrontal cortex of schizophrenic patients, suggesting that GSH-related enzyme deficiency might play a vital role in risk and etiology of schizophrenia.11,32 Besides, dysregulation of glutathione metabolism was reported to be associated with brain inflammation in psychiatric disorders.35,36 GSTM1 null genotype might increase risk of SZ through brain inflammation induced by enzyme inactivity.35–37
GST genes were widely present in human body and were abundant in the kidney, liver, and lung.36–38 In addition, GSTM1 and GSTP1 were detected in both human and rodent brains.39 Notably, GSTM1 was also suggested that it is one of the most abundant proteins in astrocytes.40 However, the result showed that GSTT1 null might be a protective factor. This result should be interpreted with caution and the reason should be further research. It indicated that GST genes played different roles in SZ patients and combination of GSTM1 null and GSTT1 present should be further discussed.
There are some limitations in this meta-analysis. First, only case–control studies were included in this meta-analysis, which would cause publication bias. However, funnel plot, Egger’s test and Begg’s test showed that publication bias was negligible. Second, GSTM1 null and GSTT1 null were antithetical in subgroup analysis of multiplex PCR and should be interpreted with caution. Some detailed information might be important for this conflicted result. However, it was hard for collecting the information. Third, heterogeneity is difficult to rule out and risk of bias is difficult to assess. It may be determined by confounding factors, such as control selection, methods, and missing data (arising from reporting biases). However, the information is hard to evaluate completely.
This study is a meta-analysis to investigate the relationship between GSTM1/T1 deletions and susceptibility to SZ. We found that GSTM1 null was associated with SZ risk in studies using multiplex PCR. The significant association was also observed between GSTM1 null and SZ risk in high-quality studies. Besides, we provided a new method for quality assessment and it should be promoted in further analysis. To confirm this result, further studies with larger sample size are required to provide more precise evidence.
Data Sharing Statement
All the data used to support the findings of this study are included within the article.
Registration Information
The review was not registered.
Review Protocol
A protocol was not prepared.
PRISMA 2020 Statement
This systematic review adherence to the PRISMA 2020 guidelines.
Acknowledgments
The authors are thankful to Dr. Pei Ma (Center for Gene Diagnosis, Zhongnan Hospital of Wuhan University) and Tianrong Yang (School of Clinical Medicine, The First Affiliated Hospital of Chengdu Medical College) for their advice on meta-analysis.
Funding
This research was supported by foundation of the First Affiliated Hospital of Chengdu Medical College (CYFY-GQ49), the program of Wuhan Municipal Health Commission (WX20C32), the Natural Science Foundation of Sichuan Province (2022NSFSC1514), and the program of Chengdu Medical College (CYZYB22-17).
Disclosure
The authors declare no conflict of interest.
References
1. Carter CJ. Schizophrenia susceptibility genes converge on interlinked pathways related to glutamatergic transmission and long-term potentiation, oxidative stress and oligodendrocyte viability. Schizophr Res. 2006;86(1–3):1–14. doi:10.1016/j.schres.2006.05.023
2. Charlson FJ, Ferrari AJ, Santomauro DF, et al. Global epidemiology and burden of schizophrenia: findings from the global burden of disease study 2016. Schizophr Bull. 2018;44(6):1195–1203. doi:10.1093/schbul/sby058
3. Ermakov EA, Dmitrieva EM, Parshukova DA, et al. Oxidative stress-related mechanisms in Schizophrenia pathogenesis and new treatment perspectives. Oxid Med Cell Longev. 2021;2021:8881770. doi:10.1155/2021/8881770
4. Kim SK, Kang SW, Chung JH, et al. Genetic polymorphisms of glutathione-related enzymes (GSTM1, GSTT1, and GSTP1) and Schizophrenia risk: a meta-analysis. Int J Mol Sci. 2015;16(8):19602–19611.
5. Cai L, Cai MH, Wang MY, et al. Meta-analysis-based preliminary exploration of the connection between ATDILI and Schizophrenia by GSTM1/T1 gene polymorphisms. PLoS One. 2015;10(6):e0128643. doi:10.1371/journal.pone.0128643
6. Huang T, Liu CL, Li LL, et al. A new method for identifying causal genes of schizophrenia and anti-tuberculosis drug-induced hepatotoxicity. Sci Rep. 2016;6:32571. doi:10.1038/srep32571
7. Lam M, Chen CY, Li Z, et al. Comparative genetic architectures of schizophrenia in East Asian and European populations. Nat Genet. 2019;51(12):1670–1678. doi:10.1038/s41588-019-0512-x
8. Warland A, Kendall KM, Rees E, et al. Schizophrenia-associated genomic copy number variants and subcortical brain volumes in the UK Biobank. Mol Psychiatry. 2020;25(4):854–862. doi:10.1038/s41380-019-0355-y
9. Minina VI, Soboleva OA, Glushkov AN, et al. Polymorphisms of GSTM1, GSTT1, GSTP1 genes and chromosomal aberrations in lung cancer patients. J Cancer Res Clin Oncol. 2017;143(11):2235–2243. doi:10.1007/s00432-017-2486-3
10. Bhat MA, Gandhi G. Association of GSTT1 and GSTM1 gene polymorphisms with coronary artery disease in North Indian Punjabi population: a case-control study. Postgrad Med J. 2016;92(1094):701–706. doi:10.1136/postgradmedj-2015-133836
11. Do KQ, Trabesinger AH, Kirsten-Krüger M, et al. Schizophrenia: glutathione deficit in cerebrospinal fluid and prefrontal cortex in vivo. Eur J Neurosci. 2000;12(10):3721–3728. doi:10.1046/j.1460-9568.2000.00229.x
12. Ansari-Lari M, Zendehboodi Z, Masoudian M, et al. Additive effect of glutathione S-transferase T1 active genotype and infection with Toxoplasma gondii for increasing the risk of schizophrenia. Nord J Psychiatry. 2021;75(4):275–280. doi:10.1080/08039488.2020.1843711
13. Nakamura T, Ohnuma T, Hanzawa R, et al. Associations of common copy number variants in glutathione S-transferase mu 1 and D-dopachrome tautomerase-like protein genes with risk of schizophrenia in a Japanese population. Am J Med Genet B Neuropsychiatr Genet. 2015;168(7):630–636. doi:10.1002/ajmg.b.32347
14. Pejovic-Milovancevic MM, Mandic-Maravic VD, Coric VM, et al. Glutathione S-transferase deletion polymorphisms in early-onset psychotic and bipolar disorders: a case-control study. Lab Med. 2016;47(3):195–204. doi:10.1093/labmed/lmw017
15. Pinheiro DS, Santos RDS, de Brito RB, et al. GSTM1/GSTT1 double-null genotype increases risk of treatment-resistant schizophrenia: a genetic association study in Brazilian patients. PLoS One. 2017;12(8):e0183812. doi:10.1371/journal.pone.0183812
16. Yan C, Duan L, Fu C, et al. Association Between Glutathione S-Transferase (GST) polymorphisms and Schizophrenia in a Chinese Han Population. Neuropsychiatr Dis Treat. 2020;16:479–487. doi:10.2147/NDT.S235043
17. Zhang X, Yang J, Liu X, et al. Glutathione S-transferase gene polymorphisms (GSTT1 and GSTM1) and risk of schizophrenia: a case-control study in Chinese Han population. Medicine. 2020;99(36):e21918. doi:10.1097/MD.0000000000021918
18. Rodriguez-Santiago B, Brunet A, Sobrino B, et al. Association of common copy number variants at the glutathione S-transferase genes and rare novel genomic changes with schizophrenia. Mol Psychiatry. 2010;15(10):1023–1033. doi:10.1038/mp.2009.53
19. Gravina P, Spoletini I, Masini S, et al. Genetic polymorphisms of glutathione S-transferases GSTM1, GSTT1, GSTP1 and GSTA1 as risk factors for schizophrenia. Psychiatry Res. 2011;187:454–456. doi:10.1016/j.psychres.2010.10.008
20. Harada S, Tachikawa H, Kawanishi Y. Glutathione S-transferase M1 gene deletion may be associated with susceptibility to certain forms of schizophrenia. Biochem Biophys Res Commun. 2001;281(2):267–271. doi:10.1006/bbrc.2001.4347
21. Kashani FL, Kordi-Tamandani DM, Sahranavard R, et al. Analysis of glutathione S-transferase genes polymorphisms and the risk of schizophrenia in a sample of Iranian population. Neuron Glia Biol. 2012;7:199–203. doi:10.1017/S1740925X12000130
22. Matsuzawa D, Hashimoto K, Hashimoto T, et al. Association study between the genetic polymorphisms of glutathione-related enzymes and schizophrenia in a Japanese population. Am J Med Genet B Neuropsychiatr Genet. 2009;150B:86–94. doi:10.1002/ajmg.b.30776
23. Pae CU, Yu HS, Kim JJ, et al. Glutathione S-transferase M1 polymorphism may contribute to schizophrenia in the Korean population. Psychiatr Genet. 2004;14:147–150. doi:10.1097/00041444-200409000-00005
24. Raffa M, Lakhdar R, Ghachem M, et al. Relationship between GSTM1 and GSTT1 polymorphisms and schizophrenia: a case-control study in a Tunisian population. Gene. 2013;512:282–285. doi:10.1016/j.gene.2012.10.031
25. Saadat M, Mobayen F, Farrashbandi H. Genetic polymorphism of glutathione S-transferase T1: a candidate genetic modifier of individual susceptibility to schizophrenia. Psychiatry Res. 2007;153:87–91. doi:10.1016/j.psychres.2006.03.024
26. Saruwatari J, Yasui-Furukori N, Kamihashi R, et al. Possible associations between antioxidant enzyme polymorphisms and metabolic abnormalities in patients with schizophrenia. Neuropsychiatr Dis Treat. 2013;9:1683–1698. doi:10.2147/NDT.S52585
27. Watanabe Y, Nunokawa A, Kaneko N, et al. A case-control study and meta-analysis of association between a common copy number variation of the glutathione S-transferase mu 1 (GSTM1) gene and schizophrenia. Schizophr Res. 2010;124:236–237. doi:10.1016/j.schres.2010.08.001
28. Kordi-Tamandani DM, Mojahed A, Sahranavard R, et al. Association of glutathione s-transferase gene methylation with risk of schizophrenia in an Iranian population. Pharmacology. 2014;94(3–4):179–182. doi:10.1159/000368083
29. Legge SE, Santoro ML, Periyasamy S, Okewole A, Arsalan A, Kowalec K. Genetic architecture of schizophrenia: a review of major advancements. Psychol Med. 2021;51(13):2168–2177. doi:10.1017/S0033291720005334
30. Chowdari KV, Bamne MN, Nimgaonkar VL. Genetic association studies of antioxidant pathway genes and schizophrenia. Antioxid Redox Signal. 2011;15(7):2037–2045. doi:10.1089/ars.2010.3508
31. Upthegrove R, Khandaker GM. Cytokines, oxidative stress and cellular markers of inflammation in Schizophrenia. Curr Top Behav Neurosci. 2020;44:49–66.
32. Fraguas D, Díaz-Caneja CM, Ayora M, et al. Oxidative stress and inflammation in first-episode psychosis: a systematic review and meta-analysis. Schizophr Bull. 2019;45(4):742–751. doi:10.1093/schbul/sby125
33. Naveen AT, Adithan C, Padmaja N, et al. Glutathione S-transferase M1 and T1 null genotype distribution in South Indians. Eur J Clin Pharmacol. 2004;60(6):403–406. doi:10.1007/s00228-004-0779-3
34. Ayano G, Tesfaw G, Shumet S. The prevalence of schizophrenia and other psychotic disorders among homeless people: a systematic review and meta-analysis. BMC Psychiatry. 2019;19(1):370. doi:10.1186/s12888-019-2361-7
35. Kim E, Keskey Z, Kang M, et al. Validation of oxidative stress assay for schizophrenia. Schizophr Res. 2019;212:126–133. doi:10.1016/j.schres.2019.07.057
36. Kano SI, Choi EY, Dohi E, et al. Glutathione S-transferases promote proinflammatory astrocyte-microglia communication during brain inflammation. Sci Signal. 2019;12(569):eaar2124. doi:10.1126/scisignal.aar2124
37. Buosi P, Borghi FA, Lopes AM, et al. Oxidative stress biomarkers in treatment-responsive and treatment-resistant schizophrenia patients. Trends Psychiatry Psychother. 2021;43(4):278–285. doi:10.47626/2237-6089-2020-0078
38. Nestsiarovich A, Obyedkov V, Kandratsenka H, et al. Disorganization at the stage of schizophrenia clinical outcome: clinical-biological study. Eur Psychiatry. 2017;42:44–48. doi:10.1016/j.eurpsy.2016.12.011
39. Al Nimer F, Strom M, Lindblom R, et al. Naturally occurring variation in the glutathione-S-transferase 4 gene determines neurodegeneration after traumatic brain injury. Antioxid Redox Signal. 2013;18(7):784–794. doi:10.1089/ars.2011.4440
40. Sharma K, Schmitt S, Bergner CG, et al. Cell type- and brain region-resolved mouse brain proteome. Nat Neurosci. 2015;18:1819–1831. doi:10.1038/nn.4160
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Paliperidone Palmitate versus Risperidone Long-Acting Injectable in Patients with Schizophrenia: A Meta-Analysis of Efficacy and Safety
Zhao M, Qin B, Mao Y, Zhang Y, Zhao R, Wang A, Wang H, Zhao J, Wang C
Neuropsychiatric Disease and Treatment 2023, 19:749-757
Published Date: 5 April 2023
A Meta-Analysis on the Efficacy of Acupuncture as an Adjuvant Therapy for Schizophrenia
Huang C, Zhang P, Dong Y, Chang R, Lao J, Li Z, Lan D
Neuropsychiatric Disease and Treatment 2023, 19:2381-2400
Published Date: 7 November 2023
Association of HTR1A Gene Polymorphisms with Efficacy and Plasma Concentrations of Atypical Antipsychotics in the Treatment of Male Patients with Schizophrenia
Qin Y, Zhao J, Yang Y, Liu Y, Xiang H, Tong J, Huang C
Neuropsychiatric Disease and Treatment 2024, 20:185-193
Published Date: 30 January 2024
Lack of Efficacy of Simvastatin Adjunctive Therapy for Patients with Schizophrenia: A Meta-Analysis of Randomized Controlled Trials
Chen J, Yuan Y, Hu Y, Liang L
Neuropsychiatric Disease and Treatment 2024, 20:1667-1675
Published Date: 6 September 2024