Back to Journals » Clinical Interventions in Aging » Volume 21
Association of Glycated Hemoglobin (HbA1c) with Functional Outcomes After Endovascular Thrombectomy for Acute Ischemic Stroke
Authors Wang H, Tao D, Du J, Chen J, Xiao G
Received 24 September 2025
Accepted for publication 12 January 2026
Published 17 January 2026 Volume 2026:21 569850
DOI https://doi.org/10.2147/CIA.S569850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Huaishun Wang,1,* Dan Tao,2,* Junhao Du,1 Jie Chen,2 Guodong Xiao1
1Second Affiliated Hospital of Soochow University, Suzhou, 215004, People’s Republic of China; 2Fourth Affiliated Hospital of Soochow University, Suzhou, 215004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guodong Xiao, Email [email protected] Jie Chen, Email [email protected]
Background: The impact of chronic glycemic control, measured by glycated hemoglobin (HbA1c), on functional outcomes after endovascular thrombectomy (EVT) for acute large vessel occlusion (LVO) stroke remains to be fully elucidated.
Methods: We conducted a retrospective cohort study of 443 consecutive patients with anterior circulation LVO stroke who underwent EVT. Patients were categorized by HbA1c levels: low (< 6.0%), medium (6.0– 7.0%), and high (> 7.0%). The primary outcome was a poor functional outcome (modified Rankin Scale score 3– 6) at 3 months. The secondary outcome was symptomatic intracranial hemorrhage (sICH).
Results: Among the 443 patients, 229 (51.7%) had a poor functional outcome. Higher HbA1c levels were significantly associated with an increased risk of poor outcome after adjustment for confounders (P for trend = 0.013). When analyzed as a continuous variable, HbA1c showed a nonlinear relationship with poor outcome; risk increased with rising HbA1c until a threshold of 7.1%, after which the rate of increase attenuated. No significant association was found between HbA1c and sICH. Subgroup analysis revealed a significant interaction between HbA1c and thrombolysis (t-PA) administration (P for interaction = 0.042), indicating that the association between high HbA1c and poor outcome was more pronounced in patients who received t-PA.
Conclusion: Elevated HbA1c is independently associated with an increased risk of poor 3-month functional outcomes after EVT, with a risk threshold observed at 7.1%. These findings underscore the importance of long-term glycemic control in stroke management.
Keywords: HbA1c, endovascular thrombectomy, functional outcome, ischemic stroke, glycemic control
Introduction
Acute ischemic stroke (AIS) resulting from large vessel occlusion (LVO) represents one of the most devastating neurological emergencies, characterized by high morbidity and mortality rates.1 Endovascular thrombectomy (EVT) has revolutionized the management of these patients, offering significant improvements in functional outcomes by achieving rapid recanalization of occluded arteries.2–6 Despite successful restoration of blood flow, a substantial proportion of patients still experience poor functional recovery.
Hyperglycemia at admission is frequently observed in AIS patients and has been consistently associated with larger infarct volumes, heightened risk of hemorrhagic transformation, and poorer functional recovery.7 Stress-induced hyperglycemia, a physiological response to acute illness, may exacerbate ischemic injury through mechanisms such as increased oxidative stress, blood-brain barrier disruption, and impaired collateral circulation. Several studies have highlighted the detrimental effect of elevated blood glucose on stroke outcomes. For instance, hyperglycemia (defined as blood glucose ≥8 mmol/L) at admission, post-procedurally, or under fasting conditions has been independently linked to unfavorable outcomes.8,9 The triglyceride glucose index has also been proven to be related to the clinical prognosis of stroke patients.10 Moreover, glycated hemoglobin (HbA1c) has been identified as a significant predictor of complications such as symptomatic intracranial hemorrhage (sICH) and early neurological deterioration, particularly in non-diabetic patients.11,12 These findings suggest that acute glycemic excursions, rather than hyperglycemia alone, may play a pivotal role in worsening outcomes.
HbA1c has also garnered attention for its potential influence on post-EVT prognosis. HbA1c reflects the average blood glucose levels over the preceding two to three months and serves as a marker of long-term glucose regulation. Elevated HbA1c levels have been associated with microvascular and macrovascular complications, which may impair the brain’s capacity to recover from ischemic insult.13 In a secondary analysis of the RESCUE BT trial, patients with HbA1c >6.5% had significantly reduced likelihood of achieving good functional outcomes (modified Rankin Scale [mRS] 0–2) at 90 days and faced higher mortality risks.14
The relationship between HbA1c and outcomes may be further elucidated by considering the hemoglobin glycation index (HGI), which quantifies the discrepancy between observed HbA1c and that predicted by fasting blood glucose. Interestingly, this relationship appears to be U-shaped, with both low and high HGI values associated with increased risk of poor outcomes and early neurological deterioration.15 This complexity suggests that the interplay between acute and chronic glycemic control is multifaceted and may involve underlying physiological mechanisms such as insulin resistance and inflammatory pathways.
The present study aims to contribute to this body of knowledge by examining the association between HbA1c levels and 3-month functional outcomes in patients receiving EVT for acute LVO stroke. By elucidating the role of chronic glycemic control in post-EVT recovery, this research may inform future clinical strategies aimed at optimizing metabolic management and improving overall prognosis in this vulnerable population.
Methods
Study Population and Setting
Between July 2017 and December 2024, consecutive patients who underwent MT for acute LVO were enrolled in this study in the Second Affiliated Hospital of Soochow University. The inclusion criteria for patients are as follows: Patients with acute AIS due to LVO in the anterior circulation confirmed by computed tomography angiography (CTA) or digital subtraction angiography (DSA), and those with a previous stroke score of no more than 1 point on the modified Rankin score (0–6 points). The exclusion criteria are as follows: (1) with acute vertebrobasilar artery occlusion, (2) patients without data of HbA1c, (3) a disability before the ischemic stroke; and severe concomitant diseases, (4) intracranial hemorrhage or arteriovenous malformations were confirmed by CT, (5) the ASPECT score obtained by preoperative CT is less than 6 points or (6) 3-month follow-up data is missing. Each MT therapy in this study was performed by a well-trained and experienced neurologist in accordance with the guidelines of the American Heart Association/American Stroke Association.16 All methods were carried out in accordance with relevant guidelines and regulations. Ninety-seven patients with acute vertebrobasilar artery occlusion were excluded, 67 patients without data of HbA1c and 3 patients lost to follow-up were excluded. Finally, 443 patients were entered into the final analysis of this study (Figure 1).
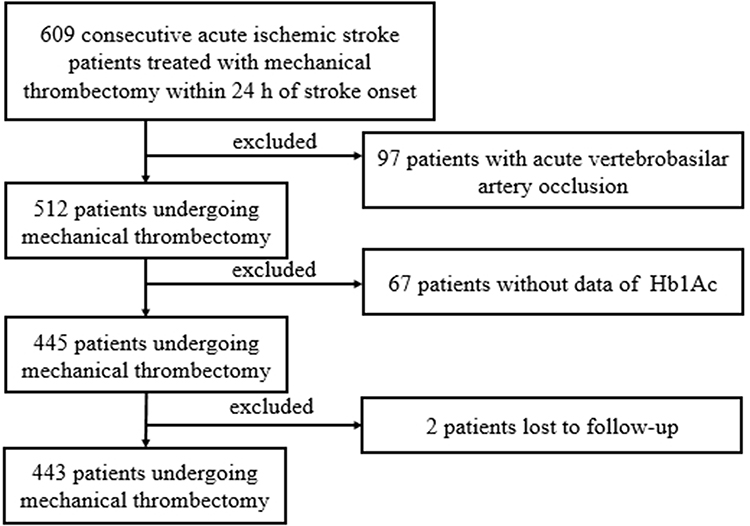 |
Figure 1 Flow diagram showing the patient selection process. |
Baseline Demographic and Clinical Information
Baseline characteristics, including demographics, stroke risk factors, admission National Institutes of Health Stroke Scale (NIHSS) scores, and Alberta Stroke Program Early Computed Tomography Score (ASPECTS). Laboratory parameters, including admission glucose and HbA1c levels, were also recorded. High HbA1c levels were defined as plasma levels exceeding 7.0%. Medium HbA1c levels was defined as plasma levels from 6.0% to 7.0%. Low HbA1c levels were defined as plasma levels below 6.0%. Additional laboratory data were documented according to previously established protocols. The procedure-related time was recorded.
Outcome Assessment
Follow-up was conducted by the trained neurologists who were blinded to the baseline information of patients by telephone or face-to-face visit. The primary outcome events were as follows: (1) poor functional outcome at 3-month (mRS ≥ 3 points), (2) symptomatic intracranial hemorrhage (sICH) occurred 24 hours after EVT.
Statistical Analysis
Continuous variables were appropriately expressed as means with standard deviation (SD) or medians with interquartile range (IQR) and were analyzed by 1-way ANOVA or Kruskal–Wallis test according to their normality of distribution. Categorical variables were presented as proportions and analyzed by the χ2 or Fisher exact tests. Binary logistic regression was used to estimate the risk of outcome events. After adopting stepwise regression to select the model combination with the smallest AIC, age, sex and admission SBP were included in the multivariate regression model in model 2.
Binary logistic regression was used to estimate the risk of poor prognosis and sICH. Odds ratios (OR) and 95% confidence intervals (CI) were calculated for each group. In model 1, we adjusted age and sex. We adopt stepwise regression to select the model combination with the smallest AIC. After eliminating the variables, the final variable we need to adjust is age, sex and admission systolic blood pressure (SBP) in model 2.
Two-sided P values of 0.05 were considered statistically significant. All statistics were conducted with SAS 9.4 software (SAS Institute Inc., Cary, NC). Figures were drawn by R software (R Development Core Team 2014, www.r-project.org).
Results
A total of 443 LVO patients were finally included with the mean age was 65±13 years old. Two hundred and fourteen patients had a good functional outcome and 229 patients had a poor functional outcome (Figure 2). The median baseline NIHSS score was 17.0 (13.0–20.0). Patients with low HbA1c were more likely to be young, male, lower median SBP and DBP, lower rate of diabetes mellitus, lower rate of hyperlipidemia, lower rate of atrial fibrillation, lower admission blood glucose level, good functional outcome and lower rate of sICH. Comparison of data of all patients is shown in Table 1.
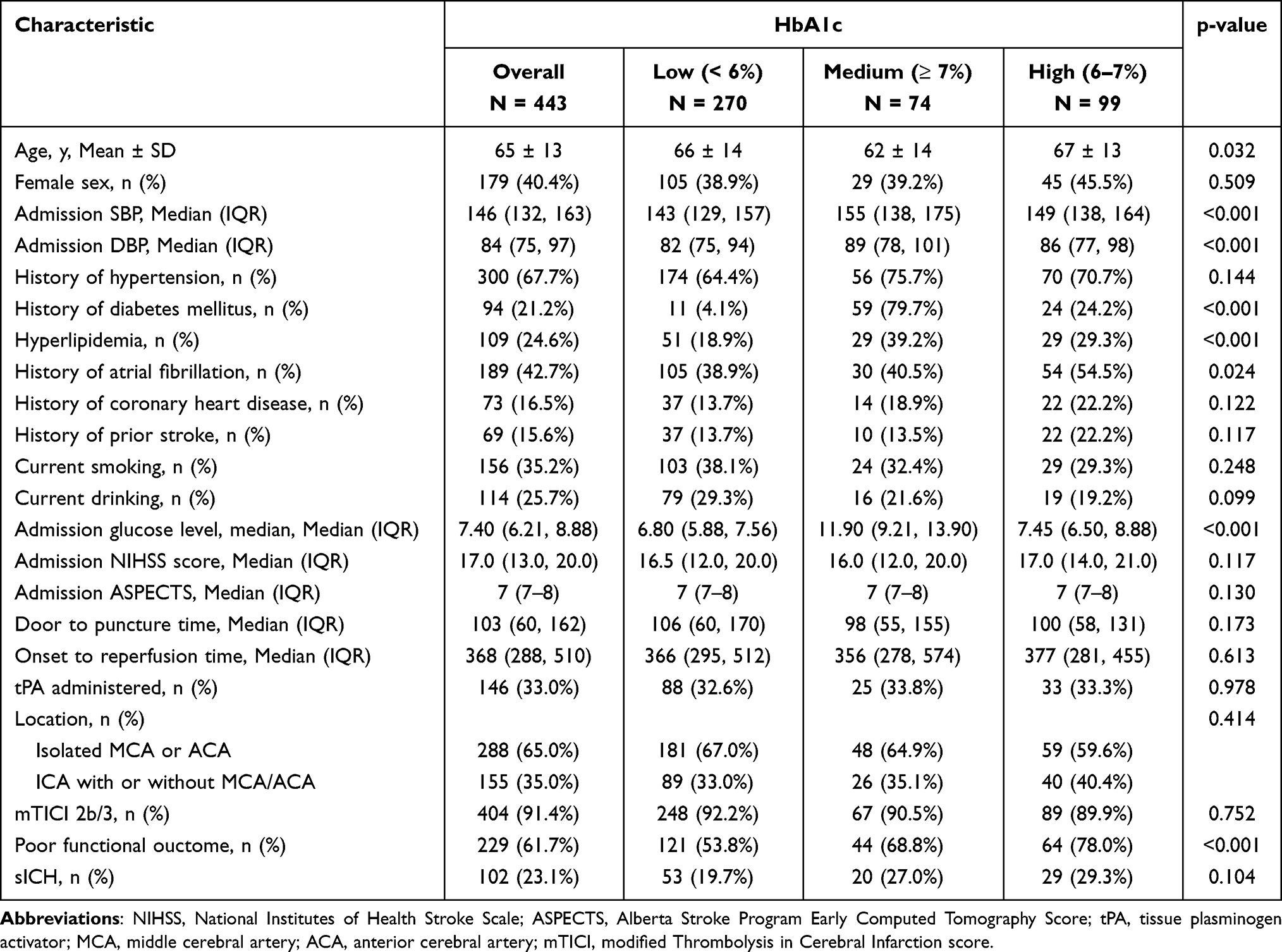 |
Table 1 Baseline Characteristics of Mechanical Thrombectomy Treated Acute Ischemic Stroke Patients |
 |
Figure 2 Distribution of mRS scores. |
Association of HbA1c with Outcomes
As shown in Table 2, taking HbA1c as an example, all patients were equally divided into three groups according to the level of HbA1c index, that is, HbA1c was used as a categorical variable to explore the association. In the logistic model, HbA1c was significantly associated poor functional outcome (P for trend = 0.002). After adjusting for age and sex, we could observe higher HbA1c increase the risk of poor outcome in model 1 (P for trend = 0.002). We adopt stepwise regression to select the model combination with the smallest AIC. After eliminating the variables, the final variable we need to adjust is age, sex and admission SBP in model 2. We could find higher HbA1c remain increasing the risk of poor functional outcome (P for trend = 0.013). When we explore the association between HbA1c and sICH, the risk of sICH increased with HbA1c increased. However, the association did not reach statistical significance in model 1 or model 2.
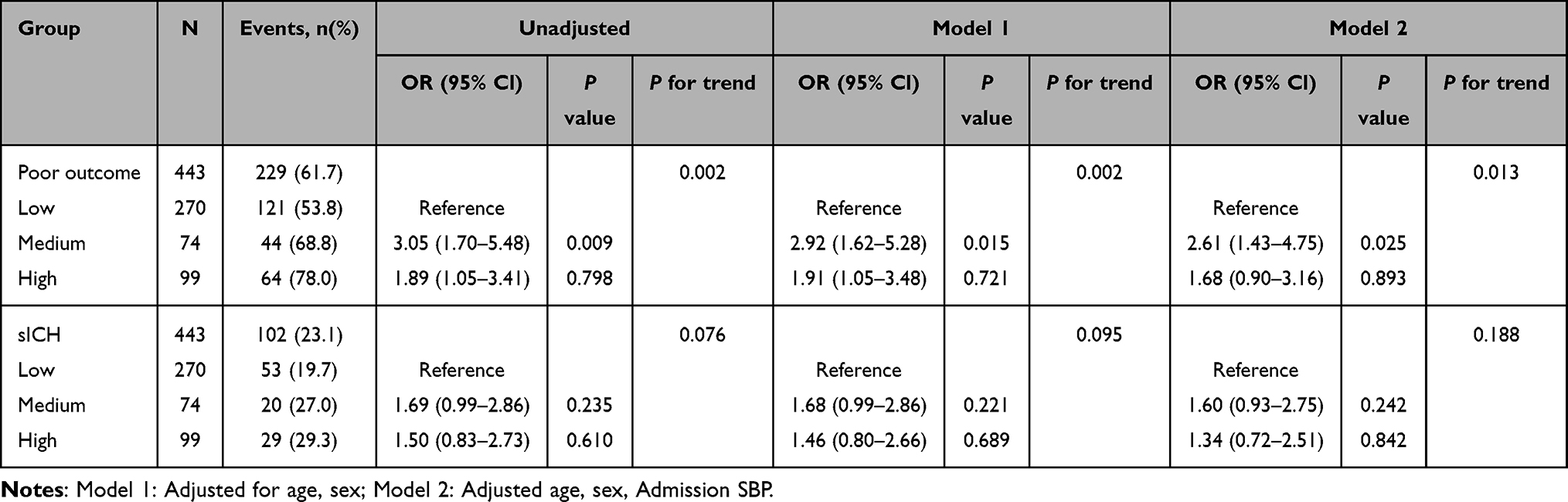 |
Table 2 The Association Between Groups and Endpoint Event (Poor Outcome and sICH) in MT-Treated Acute Ischemic Stroke Patients |
Taking HbA1c as a continuous variable, through the non-restrictive cubic spline model, we found that HbA1c shows a nonlinear association with patient prognosis. The association is similar to an “inverted U shape”. The break point of HbA1c was 7.1% (Figure 3).
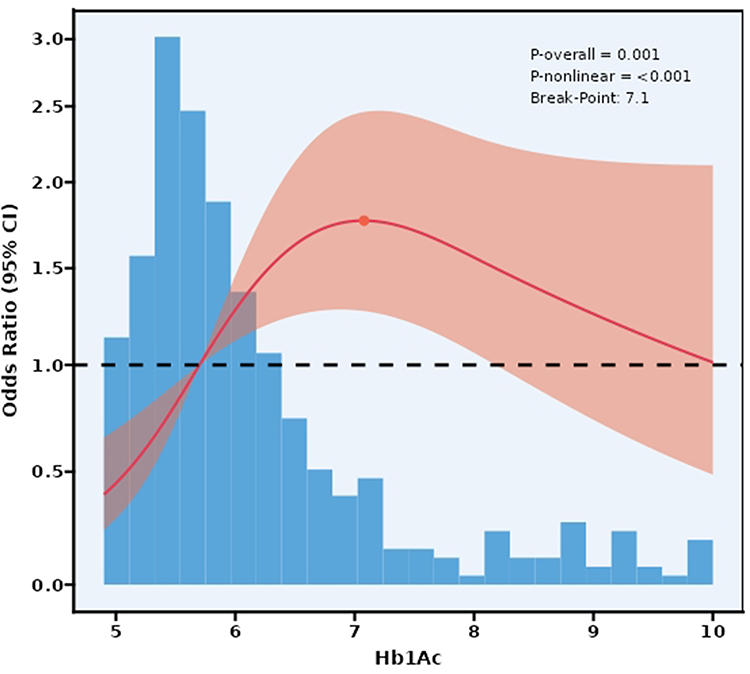 |
Figure 3 HbA1c as a continuous variable and the odds ratio of poor functional outcome (mRS 3–6) at 90 days. The association between HbA1c levels and clinical outcome, including the 95% CI, was analyzed. Data were modeled using a multivariable regression model with a RCS incorporating three knots, adjusted for covariates. The HbA1c level (7.1%) was used as the break point. The red solid line represents the adjusted odds ratio, while the red shaded area indicates the 95% CI bands. |
Subgroup Analysis for the Primary Outcome
In t-PA administered patients, HbA1c was associated with poor functional outcome (P = 0.009). However, we did not find significant association between HbA1c and poor functional outcome in non-t-PA administered patients. There is evidence that HbA1c and use of thrombolytic drugs have an interactive effect on poor functional outcome (P for interaction = 0.042). In patients without atrial fibrillation, HbA1c was associated with poor functional outcome (P = 0.024). This association has not been found in patients with atrial fibrillation. There is no evidence that HbA1c and history of atrial fibrillation have an interactive effect on poor functional outcome (P for interaction = 0.429). The above results could be seen from Figure 4.
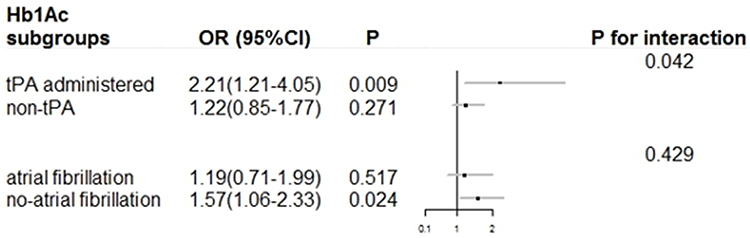 |
Figure 4 Subgroup analysis of HbA1c and poor functional outcome at 3-month. This figure illustrated the association between HbA1c and poor functional outcome at 3-month, analyzed across two patient subgroups: those who received tPA versus non-tPA, and those with atrial fibrillation versus those without atrial fibrillation. |
Discussion
This study provides a comprehensive analysis of the relationship between HbA1c index and clinical outcomes in patients with LVO stroke following EVT. Our findings indicate that when HbA1c is treated as a categorical variable, there is a significant trend towards increased risk of poor functional outcome at 3 months with rising HbA1c levels. More intriguingly, when analyzed as a continuous variable, HbA1c demonstrates a nonlinear, inverted U-shaped association with poor functional outcome, with a break point identified at 7.1%. However, we found no significant association between HbA1c levels and sICH. The interaction between HbA1c and intravenous thrombolysis (t-PA) is another pivotal observation: the adverse impact of elevated HbA1c on outcomes was exclusively pronounced in t-PA recipients.
The inverted U-shaped relationship with a peak risk at approximately 7.1% represents a novel finding in the context of thrombectomy outcomes. The identification of a 7.1% HbA1c threshold offers valuable clinical utility, particularly for pre-EVT risk stratification. Patients with HbA1c levels approaching or exceeding this cutoff should be recognized as high-risk candidates, warranting tailored management strategies. Preoperatively, this may include optimized glycemic control (when feasible before EVT) and enhanced vascular risk factor monitoring; postoperatively, close neurological surveillance and targeted metabolic interventions could help mitigate poor functional outcomes. This threshold is notably close to the conventional diagnostic cutoff for diabetes (6.5%) and the upper limit of prediabetes (5.7–6.4%),17 suggesting that the transition from prediabetes to established diabetes may represent a critical juncture in cerebrovascular pathophysiology. The increased risk observed at moderately elevated HbA1c levels (around 7.1%) rather than at extreme hyperglycemia may reflect the dual nature of glucose’s effects on cerebral tissue. At moderate elevations, hyperglycemia may exacerbate ischemic damage through multiple pathways including increased oxidative stress, inflammation, and endothelial dysfunction without triggering sufficient compensatory mechanisms.18,19 The finding that extreme hyperglycemia did not correspond to the highest risk of poor outcome suggests that other factors, including possibly more intensive glycemic management in known diabetic patients or alternative metabolic adaptations, might come into play at higher HbA1c levels.
A pivotal and novel aspect of our study is the significant interaction observed between HbA1c levels and intravenous thrombolysis. The strong association between high HbA1c and poor outcome was exclusively evident in the t-PA subgroup, suggesting that the presence of alteplase may potentiate the deleterious effects of chronic hyperglycemia. The mechanism for this interaction is likely rooted in the compounding effects of both conditions on blood-brain barrier integrity and the coagulation-fibrinolysis system. Chronic hyperglycemia induces endothelial inflammation and oxidative stress, rendering the blood-brain barrier more vulnerable.20 Intravenous thrombolytics like alteplase can further degrade the basal lamina and tight junctions, increasing blood-brain barrier permeability. This synergistic disruption significantly raises the risk of hemorrhagic transformation and severe cerebral edema, which are key drivers of neurological deterioration.21,22 Furthermore, hyperglycemia is known to promote a pro-thrombotic state and can induce resistance to thrombolytic agents, potentially leading to incomplete recanalization or early re-occlusion, thereby negating the benefits of EVT.23,24 This is corroborated by studies indicating that hyperglycemia modulates the efficacy and safety of thrombolytics, with some evidence suggesting that lower-dose thrombolysis might be safer in hyperglycemic patients due to reduced neuroinjury biomarker levels and hemorrhagic complications. Therefore, in patients receiving t-PA, the pre-existing endothelial vulnerability from high HbA1c is catastrophically exposed by the pharmacologic action of the thrombolytic drug, leading to markedly worse outcomes.
Our findings align with and extend prior research, particularly the secondary analysis of the RESCUE BT trial.14 That study reported reduced good functional outcomes (mRS 0–2) at 90 days in patients with HbA1c >6.5%, consistent with our observation of increased adverse outcomes with elevated HbA1c. However, our research advances this understanding by identifying a specific 7.1% threshold and the nonlinear nature of the association, which was not previously elucidated. Furthermore, the RESCUE BT trial did not explore interactions with t-PA administration, a gap addressed by our subgroup analysis showing that the HbA1c-outcome association is amplified in t-PA recipients. While some studies have linked acute hyperglycemia to sICH, our focus on chronic glycemic control (via HbA1c) reveals no such association, emphasizing the distinct impacts of acute versus chronic dysglycemia on stroke complications.25 This discrepancy may be explained by the different temporal aspects of glycemic exposure—while acute hyperglycemia during the ischemic insult and reperfusion phase might directly influence blood-brain barrier integrity and hemorrhagic risk, chronic hyperglycemia as captured by HbA1c may exert its primary effects through different mechanisms, such as promoting atherosclerosis and impairing collateral circulation.26,27
The pathophysiological mechanisms underlying the observed association likely involve multiple interconnected pathways. Chronic hyperglycemia contributes to endothelial dysfunction, increased oxidative stress, and a proinflammatory state, all of which can exacerbate ischemic brain injury and impair recovery.28,29 The microvascular complications associated with prolonged hyperglycemia, including impaired cerebral autoregulation and reduced cerebrovascular reserve capacity, may render the brain more vulnerable to the ischemia-reperfusion injury that occurs with thrombectomy.25 Additionally, elevated HbA1c levels reflect not only chronic hyperglycemia but also increased protein glycation, which can directly affect vascular compliance and cerebral hemodynamics. The identification of 7.1% as a potential threshold is particularly interesting as it corresponds to a level where microvascular complications typically begin to manifest in diabetic patients,30,31 suggesting shared mechanisms between diabetic microangiopathy and vulnerability to ischemic brain injury.
When considering our findings in the context of previous literature, it appears that the relationship between glycemic control and stroke outcomes may be influenced by multiple factors including stroke subtype, treatment modality, and patient characteristics. Studies have shown that poor glycemic control is associated with various diabetes-related complications,32,33 and our study extends this understanding to the specific context of thrombectomy for LVO stroke. The lack of association between HbA1c and hemorrhagic transformation contrasts with findings related to acute hyperglycemia but is consistent with the concept that different aspects of dysglycemia may have distinct effects on various pathophysiological processes. This highlights the importance of considering both acute and chronic glycemic metrics when assessing risk in stroke patients.
Several limitations of this study should be acknowledged. The retrospective design introduces potential for unmeasured confounding, despite our efforts to adjust for known prognostic factors. Subgroup analyses may be underpowered. The sample size, while sufficient to detect the primary associations, may have limited power for subgroup analyses and for detecting more modest effects on secondary outcomes such as hemorrhagic transformation. The single-timepoint measurement of HbA1c may not fully capture the longitudinal glycemic control patterns that could influence outcomes. Additionally, we did not have detailed information on diabetes duration, specific treatments, or pre-stroke glycemic management strategies, which might modify the relationship between HbA1c and outcomes. The generalizability of our findings may be limited to populations with similar characteristics to our cohort, and validation in diverse populations is warranted.
The clinical implications of our findings are substantial. The identification of 7.1% as a potential risk threshold suggests that patients with HbA1c levels around this value may represent a high-risk group that could benefit from closer monitoring and possibly more aggressive management of vascular risk factors. The lack of association with hemorrhagic transformation may provide reassurance regarding the safety of thrombectomy in patients with elevated HbA1c. However, these implications should be considered tentative until confirmed by prospective studies. From a preventive perspective, our results underscore the importance of optimal glycemic control in the primary and secondary prevention of stroke, particularly in patients who might be candidates for thrombectomy should they experience an LVO stroke.
Conclusion
In conclusion, our study demonstrates that elevated HbA1c levels are associated with increased risk of poor functional outcome after thrombectomy for LVO stroke, with a nonlinear relationship that peaks at approximately 7.1%. This threshold may represent a critical point in the cerebrovascular complications of chronic hyperglycemia. In contrast, HbA1c was not significantly associated with symptomatic intracranial hemorrhage transformation. These findings enhance understanding of the complex relationship between chronic glycemic control and outcomes after thrombectomy and may help identify patients at increased risk who could benefit from tailored management strategies. This will need to be verified through multi-center prospective studies in the future.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to the datasets are owned by the institution only but are available from Guodong Xiao on reasonable request.
Ethics Approval and Consent to Participate
The study protocols were approved by the ethics committees of Second Affiliated Hospital of Soochow University, Soochow University (approval No.JD-LK2024112-l01) and was exempt from the requirement for informed consent due to its retrospective design. All patient data were de-identified and anonymized to protect confidentiality prior to analysis.
Acknowledgments
We thank the study participants, their relatives, and the clinical staff for their support and contribution to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Suzhou Strengthening Health through Science and Education Project (grant: QNXM2024012).
Disclosure
The authors declare that they have no competing interests and the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
References
1. Wade SS, Michael HL, Joey DE, et al. Significance of large vessel intracranial occlusion causing acute ischemic stroke and TIA. Stroke. 2009;40(12). doi:10.1161/STROKEAHA.109.561787
2. Olvert AB, Puck SSF, Debbie B, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2014;372(1). doi:10.1056/NEJMoa1411587
3. Tudor GJ, Angel C, Erik C, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 2015;372(24). doi:10.1056/NEJMoa1503780
4. Mayank G, Andrew MD, Bijoy KM, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372(11). doi:10.1056/NEJMoa1414905
5. Bruce CVC, Peter JM, Timothy JK, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372(11). doi:10.1056/NEJMoa1414792
6. Jeffrey LS, Mayank G, Alain B, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 2015;372(24). doi:10.1056/NEJMoa1415061
7. Kazumi K, Yuki S, Yasuyuki I, et al. Admission hyperglycemia and serial infarct volume after t-PA therapy in patients with and without early recanalization. J Neurol Sci. 2011;307. doi:10.1016/j.jns.2011.05.021
8. Ao Q, Longyi Z, Shuang T, Wenli X. Association between hyperglycemia and unfavorable outcome in patients with successful thrombectomy for acute ischemic stroke: a single-center study. BMC Neurol. 2025;25(1). doi:10.1186/s12883-025-03456-7
9. Rinkel LA, Nguyen TT, Guglielmi V, et al. High admission glucose is associated with poor outcome after endovascular treatment for ischemic stroke. Stroke. 2020;51(11):3215–10. doi:10.1161/STROKEAHA.120.029944
10. Bukke SP, Pathange BB, Nelluri KD, et al. Association of triglyceride glucose index with clinical outcomes in ischemic stroke: a retrospective study. BMC Neurol. 2024;24(1). doi:10.1186/s12883-024-03257-9
11. Jie G, Xiangliang C, Qing H, Mengmeng G, Ye H, Gelin X. Stress hyperglycemia is associated with unfavorable outcomes after mechanical thrombectomy in patients with acute ischemic stroke. Brain Sci. 2025;15(4). doi:10.3390/brainsci15040456
12. Andrea R, Peter UH, Peter DS, et al. Glycosylated hemoglobin A1 predicts risk for symptomatic hemorrhage after thrombolysis for acute stroke. Stroke. 2013;44(8). doi:10.1161/STROKEAHA.111.000123
13. Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–412. doi:10.1136/bmj.321.7258.405
14. Fei G, Xiaolin T, Linyu L, et al. Association of admission HbA1c levels and clinical outcomes in patients with large vessel occlusion following endovascular treatment: a secondary analysis of RESCUE BT trial. Clin Intervent Aging. 2025;20. doi:10.2147/CIA.S465214
15. Nan J, Xiao-Xi L. Impact of hemoglobin glycation index on prognosis in critical patients with acute ischemic stroke: a retrospective cohort study using MIMIC-IV 2.2 database. Sci Rep. 2025;15(1). doi:10.1038/s41598-025-1743-2
16. William JP, Alejandro AR, Teri A, et al. 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3). doi:10.1161/STR.0000000000000158
17. Tainayah WT, Obidiugwu Kenrik D, Maher Y, et al. Identifying pre-diabetes ‘hotspots’ in Northern California using geospatial analysis: opportunities to target diabetes prevention strategies and improve health equity. BMJ Open. 2025;14(12). doi:10.1136/bmjopen-2024-103456
18. Ivana T, Gordana S, Š M, Lea O, Mario L. Increased renal resistive index as a marker of early stage of diabetic nephropathy in normoalbuminuric children with type 1 diabetes mellitus. Acta Clin Croat. 2025;63(1). doi:10.20471/acc.2025.63.01.06
19. Ryosuke T, Motoki F, Takeru O, et al. Hyperglycemia enhances excessive superoxide anion radical generation, oxidative stress, early inflammation, and endothelial injury in forebrain ischemia/reperfusion rats. Brain Res. 2009;1309. doi:10.1016/j.brainres.2009.10.014
20. Xiaoxue T, Yuzhao Z, Fei L, Tianzhuang H, Yuegao L. Predicting early hematoma enlargement in spontaneous intracerebral hemorrhage: hypocalcemia, hyperglycemia, and CT signs. J Stroke Cerebrovasc Dis. 2025;34(10). doi:10.1016/j.jstrokecerebrovasdis.2025.107228
21. Philipp H, Prateeka K, Anthony N, et al. Admission hyperglycemia effect on symptomatic intracranial hemorrhage in tenecteplase versus alteplase before large vessel occlusion stroke thrombectomy. J Neurol. 2024;271(12). doi:10.1007/s00415-024-12725-0
22. Huang P, Yi XY. Predictive role of admission serum glucose, baseline NIHSS score, and fibrinogen on hemorrhagic transformation after intravenous thrombolysis with alteplase in acute ischemic stroke. Eur Rev Med Pharmacol Sci. 2023;27(20). doi:10.26355/eurrev_202310_34483
23. Huihui L, Aoming J, Yuesong P, et al. Efficacy and safety of intravenous tenecteplase versus alteplase in treating acute ischemic stroke with diabetes and admission hyperglycemia. J Am Heart Assoc. 2024;13(20). doi:10.1161/JAHA.124.034996
24. Rui L, N TN, Pengfei X, et al. Effects of admission hyperglycemia and intravenous thrombolysis allocation in acute basilar artery occlusion after endovascular treatment: analysis of the ATTENTION registry. Neurotherapeutics. 2024;21(1). doi:10.1007/s13311-023-01442-7
25. Kunxin L, Wenlong Z, Quanhong W, et al. A cross-sectional study on the correlation between internal cerebral vein asymmetry and hemorrhagic transformation following endovascular thrombectomy. Front Neurol. 2025;15. doi:10.3389/fneur.2025.1529876
26. Xavier R, Sergio -R-R, Belén O, et al. Glycated hemoglobin and subclinical atherosclerosis in people without diabetes. J Am Coll Cardiol. 2021;77(22). doi:10.1016/j.jacc.2021.03.31
27. Weimin C, Jun X, Xiao W, et al. Association between triglyceride-glucose index and all-cause mortality in critically ill patients with ischemic stroke: analysis of the MIMIC-IV database. Cardiovasc Diabetol. 2023;22(1). doi:10.1186/s12933-023-02041-w
28. Keisuke M, Takahiko I, Sou S, et al. Diabetes mellitus aggravates hemorrhagic transformation after ischemic stroke via mitochondrial defects leading to endothelial apoptosis. PLoS One. 2014;9(8). doi:10.1371/journal.pone.0103818
29. Peng Y, Ling W, Hao Y, Wei S, Ping H. Acute hyperglycemia exacerbates neuroinflammation and cognitive impairment in sepsis-associated encephalopathy by mediating the ChREBP/HIF-1α pathway. Eur J Med Res. 2024;29(1). doi:10.1186/s40001-024-02129-3
30. Nathan DM, Genuth S, Lachin J, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14). doi:10.1056/NEJM199309303291401
31. Lily A, Nasrin A, B GD, et al. Long-term follow-up of intensive glycaemic control on renal outcomes in the Veterans Affairs Diabetes Trial (VADT). Diabetologia. 2017;61(2). doi:10.1007/s00125-017-4473-2
32. Rury RH, Sanjoy KP, Angelyn M, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15). doi:10.1056/NEJMoa0806470
33. Giovanni S, Eugenio R, Rosaria C, Annunziata L. Long-term HbA1c variability and macro-/micro-vascular complications in type 2 diabetes mellitus: a meta-analysis update. Acta Diabetol. 2023;60(6). doi:10.1007/s00592-023-02037-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel Metabolic Score for Insulin Resistance and Symptomatic Intracranial Hemorrhage in Ischemic Stroke Patients After Endovascular Thrombectomy
Chen S, E Y, Zhang X, Wei B, Wang S, Xu Z, Gong P, Xie Y, Qin C, Zhang Y
Neuropsychiatric Disease and Treatment 2023, 19:321-328
Published Date: 5 February 2023
Diabetes Mellitus and Its Therapy in Brunei Darussalam – A Critical Revisit
Muhammad Haskani NH, Ming LC, Dhaliwal JS, Wee DVT, Goh BH, Ali M, Shaharuddin S, Goh KW, Goh HP
Patient Preference and Adherence 2023, 17:1131-1136
Published Date: 22 April 2023
Relationship Between Liver Fibrosis and Increased Risk of Symptomatic Intracranial Hemorrhage in Ischemic Stroke Patients Undergoing Mechanical Thrombectomy
Xu J, Zhang X, E Y, Wang W, Zhou J, Shi Y, Chen S
Neuropsychiatric Disease and Treatment 2024, 20:101-108
Published Date: 18 January 2024
Endovascular Thrombectomy for Acute Ischemic Stroke in Indonesia: Challenging and Strategic Planning
Rilianto B, Kurniawan RG, Rajab NM, Prasetyo BT
Neuropsychiatric Disease and Treatment 2024, 20:621-630
Published Date: 21 March 2024
Frequent Self-Monitoring Blood Glucose Correlated to Better Medication Adherence and Glycemic Control in Children with Type 1 Diabetes Mellitus
Rochmah N, Soetjipto S, Faizi M, Hisbiyah Y, Perwitasari RK, Fedora K, Rosyidah LN, Endarko E, Kuswanto D, Rini EA
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2203-2209
Published Date: 4 June 2024