Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Relationship Between Liver Fibrosis and Increased Risk of Symptomatic Intracranial Hemorrhage in Ischemic Stroke Patients Undergoing Mechanical Thrombectomy
Authors Xu J, Zhang X ![]() , E Y, Wang W, Zhou J, Shi Y, Chen S
, E Y, Wang W, Zhou J, Shi Y, Chen S
Received 15 November 2023
Accepted for publication 15 January 2024
Published 18 January 2024 Volume 2024:20 Pages 101—108
DOI https://doi.org/10.2147/NDT.S450061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yu-Ping Ning
Jing Xu,* Xiaohao Zhang,* Yan E, Wei Wang, Junshan Zhou, Yanyan Shi, Shuaiyu Chen
Department of Neurology, Nanjing First Hospital, Nanjing Medical University, Nanjing, Jiangsu, 210000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanyan Shi; Shuaiyu Chen, Department of Neurology, Nanjing First Hospital, Nanjing Medical University, No. 68 Changle Road, Nanjing, Jiangsu Province, 210000, People’s Republic of China, Tel/Fax +86 02552271000, Email [email protected]; [email protected]
Background: Liver fibrosis has been reported to be associated with hematoma expansion and mortality in patients with intracerebral hemorrhage. This study aimed to detect the association between liver fibrosis and symptomatic intracranial hemorrhage (sICH) in ischemic stroke after mechanical thrombectomy (MT).
Methods: We retrospectively included patients with large artery occlusion in the anterior circulation and treated with MT at a single stroke center. The fibrosis-4 index (FIB-4) was used to assess the severity of liver fibrosis. sICH was diagnosed according to the Heidelberg Bleeding Classification criteria. Multivariate logistic regression and restricted cubic spline analysis were conducted to examine the relationship between liver fibrosis and sICH.
Results: Among the 578 patients (mean age, 70.1 years; 58.5% male) included in the study, 65 (11.2%) individuals were diagnosed with sICH. After adjusting for demographic characteristics and other potential confounders, a higher FIB-4 index was found to be independently associated with an increased risk of sICH (odds ratio: 1.306, 95% confidence interval: 1.127– 1.512, P=0.001). Similar results were obtained when analyzing FIB-4 as a categorical variable.
Conclusion: This study demonstrated that there is a significant association between FIB-4 and the risk of sICH in patients with acute ischemic stroke who underwent MT. Therefore, liver fibrosis could serve as a valuable parameter in monitoring the risk of sICH following MT.
Keywords: liver fibrosis, fibrosis-4 index, ischemic stroke, symptomatic intracranial hemorrhage, endovascular thrombectomy
Introduction
Ischemic stroke leads to a high prevalence of disability and mortality worldwide, especially in patients with cardioembolic stroke and atherothrombotic stroke.1–4 It has been confirmed that mechanical thrombectomy (MT) is a beneficial treatment for ischemic stroke patients who have suffered large artery occlusion.5 However, symptomatic intracranial hemorrhage (sICH) is a serious complication that can occur in ischemic stroke patients after MT treatment, leading to an increased risk of morbidity and mortality.6–8 Therefore, the early and accurate identification of sICH after MT is crucial for improving the prognosis.
Chronic liver diseases often lead to liver fibrosis, a condition characterized by the accumulation of extracellular matrix proteins.9 Nonalcoholic fatty liver disease (NAFLD) is an independent risk factor for cardiovascular disease, type 2 diabetes mellitus, and chronic kidney disease.10 Patients with nonalcoholic steatohepatitis, a progressive form of NAFLD characterized by hepatic inflammation and hepatocellular injury, are at a higher risk of developing progressive fibrosis.11 The fibrosis-4 index (FIB-4) is a noninvasive and practical tool for predicting liver fibrosis in patients with NAFLD,12 which is based on anthropometric measures and blood test results, making it easy to obtain. A prospective stroke cohort demonstrated that advanced liver fibrosis significantly correlated to a higher risk of long-term poor prognosis and stroke recurrence.13 Furthermore, a recent study in intracerebral hemorrhage reported that FIB-4 is associated with the size of hematoma at admission and its subsequent expansion.14 However, the relationship between liver fibrosis and sICH in ischemic stroke patients after MT treatment remains unclear.
Therefore, this study aimed to explore the association of liver fibrosis, as assessed by the FIB-4 index, with the presence of sICH in anterior circulation large vessel occlusive stroke after MT.
Methods
Study Population
We retrospectively collected patients with large vessel occlusion stroke after MT from Nanjing First Hospital from September 2019 to February 2023. The inclusion criteria for this study were as follows: (1) being 18 years of age or older; (2) having large artery occlusion in the internal carotid artery or middle cerebral artery; (3) undergoing MT treatment. The exclusion criteria included: (1) having a history of chronic viral hepatitis; (2) lacking complete clinical data for calculating the FIB-4 index; (3) having been diagnosed with a concomitant aneurysm, arteriovenous malformation, moyamoya disease, or hematological system diseases. This study was approved by the Ethics Committee of Nanjing First Hospital. All procedures performed in studies involving human participants were in accordance with the ethical standards of Nanjing First Hospital and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Due to its retrospective nature; patient consent was waived. Patient data was confidentiality maintained in Nanjing First Hospital.
Baseline Data Collection
We collected and analyzed the baseline data, including demographic characteristics, clinical data, procedure parameters, and laboratory data. The National Institutes of Health Stroke Scale (NIHSS) score was used to evaluate neurological impairment.15 Pre-treatment infarct volume was measured using the Alberta Stroke Program Early Computed Tomography Score (ASPECTS).16 The Trial of Org 10,172 in Acute Stroke Treatment (TOAST) classification was utilized to categorize stroke types.17 Procedural characteristics were also collected, which included whether intravenous thrombolysis was administered before MT, the time from onset to recanalization, successful reperfusion, and the procedural model used. Collateral status was assessed based on digital subtraction angiography using the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology grading system, with grades 0–1 indicating poor collateral status and grades 2–4 indicating moderate to excellent collateral status.18 Successful reperfusion was defined as a modified Thrombolysis in Cerebral Infarction score of 2b or 3.7
Calculation of FIB-4 Index
FIB-4 score is a well-validated and clinically established liver fibrosis index.19 The FIB-4 index is calculated using the formula: FIB-4 index = AST (IU/L) × age (years) / platelet count (10^9/L) × ALT (IU/L)^(1/2).20 Blood samples for all laboratory tests were obtained at 8 o’clock the following morning.
Definition of sICH
A follow-up brain computed tomography (CT) scan was usually performed 24–72 hours after each thrombectomy procedure. According to the Heidelberg Bleeding Classification criteria,21,22 sICH was diagnosed if the newly observed intracranial hemorrhage was correlated to any of the following conditions: (1) NIHSS score increased >4 points than that immediately before worsening; (2) NIHSS score increased >2 points in 1 category; (3) deterioration led to intubation, hemicraniectomy, external ventricular drain placement, or any other major interventions. In addition, the symptom deterioration could not be explained by causes other than the observed intracranial hemorrhage. Interpretation of all images was performed independently by two neurologists. In case of disagreement, a third reader (a board-certified neurologist) was consulted.
Statistical Analysis
For continuous variables, we reported the medians and interquartile ranges or means and standard deviations. The statistical analysis for continuous variables was performed using the Mann–Whitney U-test, t-test, Kruskal–Wallis test, or one-way analysis of variance, depending on appropriateness. For categorical variables, we presented the frequencies and percentages. The statistical analysis for categorical variables was conducted using the chi-square test or Fisher’s exact test. To assess the variables associated with the presence of sICH, binary logistic regression analysis was employed. In model 1, we adjusted for age and sex. In model 2, we further adjusted for baseline ASPECTS and poor collateral circulation. In model 3, we adjusted for age and sex, as well as all variables with a significance level of P < 0.1 in the univariate analysis. We also evaluated the pattern and magnitude of the association of FIB-4 with sICH using a logistic regression model with restricted cubic splines with 3 knots (at fifth, 50th, and 95th percentiles) adjusted for covariates included in model 3.23 All statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp, Armonk, NY, USA) and R software (version 4.3.1; Vienna, Austria).
Result
Patient Characteristics
This study cohort consisted of 589 consecutive large vessel occlusive stroke patients who underwent MT. Six patients were excluded due to incomplete laboratory data for calculating the FIB-4 index, and 5 patients were excluded due to the presence of moyamoya disease, arteriovenous malformation, or hematological system diseases. Finally, 578 patients were analyzed, with a mean age of 70.8 years and 58.5% of the cohort being male. The median NIHSS score at admission was 14.0, and 37.2% of patients received intravenous thrombolysis. Poor collateral status was observed in 313 cases (51.2%). Successful recanalization was achieved in 530 patients (91.7%). According to the TOAST criteria, 281 patients (48.6%) were diagnosed with larger artery atherosclerotic stroke, 246 patients (42.6%) with cardio-embolism, and 51 patients (8.9%) with an undetermined etiology. The median ASPECTS score before treatment was 9.0, and the median FIB-4 score was 2.0. Additional demographic characteristics, clinical and laboratory data, neurological imaging data, and procedural characteristics stratified by FIB-4 quartiles can be found in Table S1. Patients with higher FIB-4 score were found to be older, more likely to suffer the cardioembolic stroke, hypertension, and coronary heart disease, and had a higher NIHSS score. Importantly, participants with higher FIB-4 score had an increased risk of sICH.
Association Between FIB-4 and sICH
According to the Heidelberg Bleeding Classification, 65 patients (11.2%) were classified as having a sICH within 72 hours after receiving MT treatment. In univariate analysis, it was found that patients with higher baseline ASPECTS score (median 8.0 versus 9.0; P = 0.007) were more likely to experience sICH. Furthermore, patients who developed sICH had a higher incidence of poor collateral status (67.7% versus 49.1%; P = 0.005). Additionally, patients with sICH had higher levels of fasting blood glucose (8.2 versus 7.1 mmol/L; P = 0.001) and FIB-4 score (2.6 versus 1.9; P = 0.003), as compared to those without sICH. These results are summarized in Table 1.
 |
Table 1 Clinical Characteristics of Study Participants According to Patients with and without sICH |
Table 2 demonstrated the results of multivariate regression analysis for FIB-4 index and sICH risk. In fully adjusted models, each unit increase in FIB-4 score was associated with a 30.6% (95% CI, 1.127−1.512, P = 0.001) increased ratio of sICH. Similar results were observed when the FIB-4 score was defined as a categorical variable. Furthermore, the restricted cubic spline suggested a strongly non-linear relationship between the FIB-4 index and risk of sICH after MT treatment (P for non-linearity = 0.012, Figure 1).
 |
Table 2 Multivariate Regression Analysis for FIB-4 and sICH |
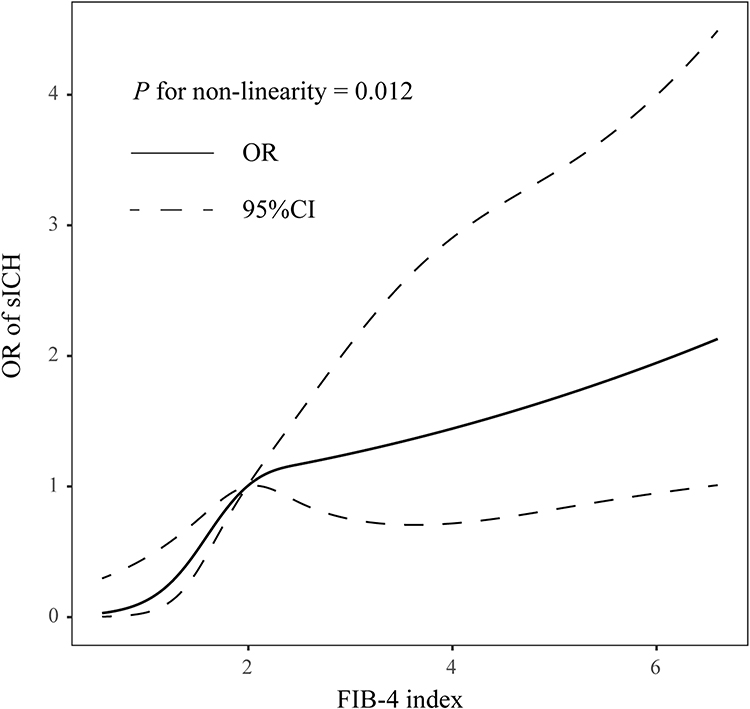 |
Figure 1 Restricted cubic spline evaluated the association between FIB-index and sICH in patients with large vessel occlusion after mechanical thrombectomy. The association was fitted with restricted cubic spline with 3 knots (at 5th, 50th, and 95th percentiles) adjusting for covariates including age and sex, as well as all variables with a significance level of P < 0.1 in the univariate analysis. |
Discussion
In our study, we have found that liver fibrosis, as measured by the FIB-4 score, is an independent predictor of sICH in ischemic stroke patients who underwent MT treatment. This association remained even after adjusting for factors such as age, sex, pre-treatment ASPECTS, poor collateral status, baseline NIHSS score, successful reperfusion, stroke subtypes, and Fasting blood glucose levels.
Previous studies have demonstrated that a significant fibrous liver is associated with higher long-term mortality and recurrent events in patients who have suffered from ischemic stroke or transient ischemic attacks.13 These studies have used the FIB-4 index to evaluate liver fibrosis and have consistently reported similar findings. A previous study found that clinically silent liver fibrosis, evaluated by the FIB-4 index, is an independent risk factor for unfavorable outcomes after thrombectomy.20 In addition, FIB-4 score values were also related to sICH after intravenous thrombolysis, specifically among patients with a high probability of advanced hepatic fibrosis.24 While the relationship between FIB-4 and sICH has been confirmed in our study, the underlying mechanism is still unknown. However, based on existing literature, liver fibrosis has been shown to contribute to endothelial dysfunction, hypercoagulable state, and systemic inflammation.25–27 Furthermore, NAFLD has been associated with lipidosis, which may contribute to increased carotid intimal medial thickness and the prevalence of carotid plaques.28,29 These adverse factors contribute to an increased risk of sICH. Firstly, liver cirrhosis can cause abnormal coagulation, predisposing patients to bleeding and an increased risk of subarachnoid and intracranial hemorrhage.30 Secondly, hepatocyte-derived extracellular vesicles can promote endothelial inflammation, leading to blood-brain barrier dysfunction and exacerbating neuronal injury after ischemic insults.31,32 Thirdly, NAFLD is often associated with atherogenic dyslipidemia characterized by increased serum triglyceride levels, increased small, dense LDL particles, and decreased HDL cholesterol, as well as Type 2 Diabetes, which can lead to artery fragility and vascular rupture.33–35 However, further investigations are needed to fully understand the underlying mechanisms that link liver fibrosis to the occurrence of sICH in ischemic stroke patients after EVT.
Within our study population, 11.2% of patients were diagnosed with sICH within 72 hours after MT, according to the Heidelberg Bleeding Classification criteria. This rate is slightly higher than what has been reported in randomized controlled trials,5 and the rate observed in the North American Solitaire Stent Retriever Acute Stroke registry (9.9%).36 This indicates that Chinese ischemic stroke patients were more prevalent. Additionally, we identified several other factors that were associated with sICH after MT. These factors include pre-treatment ASPECTS, poor collateral status, and fasting blood glucose levels. Previous studies have shown that age, baseline stroke severity, high blood pressure, high baseline glucose levels, Hs-CRP levels, pre-treatment ASPECT score, NIHSS ≥15.5 at 24 hours post-stroke, and longer onset to treatment delays are also associated with sICH.22,37–39 However, we did not find age, baseline stroke severity, high blood pressure, or Hs-CRP levels to be significant factors in our study. These discrepancies may be due to differences in study populations, sample sizes, types of strokes, the degree of high blood pressure control, and the definitions and timing of determining sICH.
There are several limitations in our study. Firstly, an important limitation is the lack of information on whether the patients had pre-existing liver fibrosis or other factors that may have influenced its development, such as infections. Additionally, due to the nature of our study design, we were unable to establish a causal relationship between FIB-4 and sICH. Furthermore, we did not record the potential impact of medications such as statins on liver function. Lastly, our study was conducted in a single center and focused on a specific population of stroke patients, which limits the applicability and generalizability of our findings.
In conclusion, the current analysis demonstrated that FIB-4 is a risk factor for sICH in acute ischemic stroke patients who undergo EM treatment. These findings suggest that evaluating liver fibrosis using FIB-4 may serve as an effective parameter for monitoring the occurrence of sICH following MT. Further studies with large sample sizes are needed to assess these associations comprehensively, which may help to identify patients at high risk of sICH and open the way to the proposal of new therapeutic options for sICH after EVT treatment.
Data Sharing Statement
The raw data that support the findings of this study are available on request from the corresponding author., without undue reservation.
Funding
There is no funding to report.
Disclosure
All the authors declare that there is no conflict of interest.
References
1. Tu W, Zhao Z, Yin P, et al. Estimated Burden of Stroke in China in 2020. JAMA Network Open. 2023;6(3):e231455. doi:10.1001/jamanetworkopen.2023.1455
2. Arboix A, Oliveres M, Massons J, Pujades R, Garcia-Eroles L. Early differentiation of cardioembolic from atherothrombotic cerebral infarction: a multivariate analysis. Eur J Neurol. 1999;6(6):677–683. doi:10.1046/j.1468-1331.1999.660677.x
3. Çinar T, Hayiroğlu Mİ, Selçuk M, et al. Evaluation of electrocardiographic P wave parameters in predicting long-term atrial fibrillation in patients with acute ischemic stroke. Arq Neuropsiquiatr. 2022;80(9):877–884. doi:10.1055/s-0042-1755322
4. Hayıroğlu Mİ, Çınar T, Selçuk M, et al. The significance of the morphology-voltage-P-wave duration (MVP) ECG score for prediction of in-hospital and long-term atrial fibrillation in ischemic stroke. J Electrocardiol. 2021;69:44–50. doi:10.1016/j.jelectrocard.2021.09.006
5. Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723–1731. doi:10.1016/S0140-6736(16)00163-X
6. Zhang X, Xie Y, Wang H, et al. Symptomatic Intracranial Hemorrhage After Mechanical Thrombectomy in Chinese Ischemic Stroke Patients: the ASIAN Score. Stroke. 2020;51(9):2690–2696. doi:10.1161/STROKEAHA.120.030173
7. Zhang X, Yuan K, Wang H, et al. Nomogram to Predict Mortality of Endovascular Thrombectomy for Ischemic Stroke Despite Successful Recanalization. J Am Heart Assoc. 2020;9(3):e014899. doi:10.1161/JAHA.119.014899
8. Zhang X, Zhou F, Wang W, et al. Levels of adhesion molecules and clinical outcomes in patients with ischemic stroke after mechanical thrombectomy. Front Neurol. 2022;13:1024162. doi:10.3389/fneur.2022.1024162
9. Shah A, Lydecker A, Murray K, et al. Comparison of noninvasive markers of fibrosis in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2009;7(10):1104–1112. doi:10.1016/j.cgh.2009.05.033
10. Adams L, Anstee Q, Tilg H, Targher G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut. 2017;66(6):1138–1153. doi:10.1136/gutjnl-2017-313884
11. Heyens L, Busschots D, Koek G, Robaeys G, Francque S. Liver Fibrosis in Non-alcoholic Fatty Liver Disease: from Liver Biopsy to Non-invasive Biomarkers in Diagnosis and Treatment. Front Med Lausanne. 2021;8:615978. doi:10.3389/fmed.2021.615978
12. Chalasani N, Younossi Z, Lavine J, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2018;67(1):328–357. doi:10.1002/hep.29367
13. Baik M, Nam H, Heo J, et al. Advanced Liver Fibrosis Predicts Unfavorable Long-Term Prognosis in First-Ever Ischemic Stroke or Transient Ischemic Attack. Cerebrovasc Dis. 2020;49(5):474–480. doi:10.1159/000510436
14. Parikh N, Kamel H, Navi B, et al. Liver Fibrosis Indices and Outcomes After Primary Intracerebral Hemorrhage. Stroke. 2020;51(3):830–837. doi:10.1161/STROKEAHA.119.028161
15. Sucharew H, Khoury J, Moomaw C, et al. Profiles of the National Institutes of Health Stroke Scale items as a predictor of patient outcome. Stroke. 2013;44(8):2182–2187. doi:10.1161/STROKEAHA.113.001255
16. Barber P, Demchuk A, Zhang J, Buchan A. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet. 2000;355(9216):1670–1674. doi:10.1016/S0140-6736(00)02237-6
17. Adams HJ, Bendixen B, Kappelle L, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24(1):35–41. doi:10.1161/01.STR.24.1.35
18. Zaidat OO, Yoo AJ, Khatri P, et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement. Stroke. 2013;44(9):2650–2663. doi:10.1161/STROKEAHA.113.001972
19. Sterling R, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43(6):1317–1325. doi:10.1002/hep.21178
20. Fandler-Höfler S, Stauber R, Kneihsl M, et al. Non-invasive markers of liver fibrosis and outcome in large vessel occlusion stroke. Ther Adv Neurol Disord. 2021;14:17562864211037239. doi:10.1177/17562864211037239
21. von Kummer R, Broderick JP, Campbell BC, et al. The Heidelberg Bleeding Classification: classification of Bleeding Events After Ischemic Stroke and Reperfusion Therapy. Stroke. 2015;46(10):2981–2986. doi:10.1161/STROKEAHA.115.010049
22. Hao Y, Yang D, Wang H, et al. Predictors for Symptomatic Intracranial Hemorrhage After Endovascular Treatment of Acute Ischemic Stroke. Stroke. 2017;48(5):1203–1209. doi:10.1161/STROKEAHA.116.016368
23. Durrleman S, Simon R. Flexible regression models with cubic splines. Stat Med. 1989;8(5):551–561. doi:10.1002/sim.4780080504
24. Norata D, Lattanzi S, Broggi S, Rocchi C, Bartolini M, Silvestrini M. Liver fibrosis-4 score predicts outcome of patients with ischemic stroke undergoing intravenous thrombolysis. Front Neurol. 2023;14:1103063. doi:10.3389/fneur.2023.1103063
25. du Plessis J, van Pelt J, Korf H, et al. Association of Adipose Tissue Inflammation With Histologic Severity of Nonalcoholic Fatty Liver Disease. Gastroenterology. 2015;149(3):635–48.e14. doi:10.1053/j.gastro.2015.05.044
26. Verrijken A, Francque S, Mertens I, et al. Prothrombotic factors in histologically proven nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Hepatology. 2014;59(1):121–129. doi:10.1002/hep.26510
27. Jiang F, Chen Q, Wang W, Ling Y, Yan Y, Xia P. Hepatocyte-derived extracellular vesicles promote endothelial inflammation and atherogenesis via microRNA-1. J Hepatol. 2020;72(1):156–166. doi:10.1016/j.jhep.2019.09.014
28. Weng S, Zhou J, Chen X, Sun Y, Mao Z, Chai K. Prevalence and factors associated with nonalcoholic fatty pancreas disease and its severity in China. Medicine. 2018;97(26):e11293. doi:10.1097/MD.0000000000011293
29. Beer S, Babel J, Martin N, Blank V, Wiegand J, Karlas T. Non-invasive assessment of steatohepatitis indicates increased risk of coronary artery disease. PLoS One. 2023;18(9):e0286882. doi:10.1371/journal.pone.0286882
30. Van Dyken P, Lacoste B. Impact of Metabolic Syndrome on Neuroinflammation and the Blood-Brain Barrier. Front Neurosci. 2018;12:930. doi:10.3389/fnins.2018.00930
31. Targher G, Day C, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med. 2010;363(14):1341–1350. doi:10.1056/NEJMra0912063
32. Çinier G, Hayıroğlu Mİ, Kolak Z, et al. The value of C-reactive protein-to-albumin ratio in predicting long-term mortality among HFrEF patients with implantable cardiac defibrillators. Eur J Clin Invest. 2021;51(8):e13550. doi:10.1111/eci.13550
33. Speliotes E, Massaro J, Hoffmann U, et al. Fatty liver is associated with dyslipidemia and dysglycemia independent of visceral fat: the Framingham Heart Study. Hepatology. 2010;51(6):1979–1987. doi:10.1002/hep.23593
34. Nseir W, Shalata A, Marmor A, Assy N. Mechanisms linking nonalcoholic fatty liver disease with coronary artery disease. Dig Dis Sci. 2011;56(12):3439–3449. doi:10.1007/s10620-011-1767-y
35. Duan W, Shi R, Yang F, et al. FSTL3 partially mediates the association of increased nonalcoholic fatty liver disease fibrosis risk with acute myocardial infarction in patients with type 2 diabetes mellitus. Cardiovasc Diabetol. 2023;22(1):297. doi:10.1186/s12933-023-02024-x
36. Zaidat O, Castonguay A, Gupta R, et al. North American Solitaire Stent Retriever Acute Stroke registry: post-marketing revascularization and clinical outcome results. J Neurointerv Surg. 2014;6(8):584–588. doi:10.1136/neurintsurg-2013-010895
37. van der Steen W, van der Ende NAM, van Kranendonk KR, et al. Determinants of Symptomatic Intracranial Hemorrhage After Endovascular Stroke Treatment: a Retrospective Cohort Study. Stroke. 2022;53(9):2818–2827. doi:10.1161/STROKEAHA.121.036195
38. Venditti L, Chassin O, Ancelet C, et al. Pre-procedural predictive factors of symptomatic intracranial hemorrhage after thrombectomy in stroke. J Neurol. 2021;268(5):1867–1875. doi:10.1007/s00415-020-10364-x
39. Csecsei P, Tarkanyi G, Bosnyak E, et al. Risk analysis of post-procedural intracranial hemorrhage based on STAY ALIVE Acute Stroke Registry. J Stroke Cerebrovasc Dis. 2020;29(7):104851. doi:10.1016/j.jstrokecerebrovasdis.2020.104851
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Associated with Liver Fibrosis in Chinese Patients with Type 2 Diabetes Mellitus and Non-Alcoholic Fatty Liver Disease
Luo Y, Wang C, Zhang T, He X, Hao J, Shen A, Zhao H, Chen S, Ren L
International Journal of General Medicine 2023, 16:293-302
Published Date: 24 January 2023
A Novel Metabolic Score for Insulin Resistance and Symptomatic Intracranial Hemorrhage in Ischemic Stroke Patients After Endovascular Thrombectomy
Chen S, E Y, Zhang X, Wei B, Wang S, Xu Z, Gong P, Xie Y, Qin C, Zhang Y
Neuropsychiatric Disease and Treatment 2023, 19:321-328
Published Date: 5 February 2023
The Relationship Between Neuron-Specific Enolase and Clinical Outcomes in Patients Undergoing Mechanical Thrombectomy
Peng Q, Chen W, E Y, Deng Y, Xu Z, Wang S, Fu X, Wei B, Wang M, Hou J, Zhang Y, Duan R
Neuropsychiatric Disease and Treatment 2023, 19:709-719
Published Date: 4 April 2023
A Novel Nomogram to Predict Symptomatic Intracranial Hemorrhage in Ischemic Stroke Patients After Intravenous Thrombolysis
Jiang Z, Xu D, Li H, Wu X
Therapeutics and Clinical Risk Management 2023, 19:993-1003
Published Date: 29 November 2023
Endovascular Thrombectomy for Acute Ischemic Stroke in Indonesia: Challenging and Strategic Planning
Rilianto B, Kurniawan RG, Rajab NM, Prasetyo BT
Neuropsychiatric Disease and Treatment 2024, 20:621-630
Published Date: 21 March 2024