Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Association Between Vitamin D and Microvascular Changes in Early Diabetic Retinopathy in Patients with Type 2 Diabetes
Authors Wei Z ![]() , Wang K
, Wang K ![]() , Liu Y
, Liu Y ![]() , Liu P, Tang Y, Chen L
, Liu P, Tang Y, Chen L ![]() , Hou X
, Hou X ![]() , Yan F
, Yan F
Received 26 August 2025
Accepted for publication 31 October 2025
Published 8 November 2025 Volume 2025:18 Pages 4085—4095
DOI https://doi.org/10.2147/DMSO.S562924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Zichun Wei,1– 3,* Kewei Wang,1,2,* Yingqi Liu,1,2 Pan Liu,4 Yuqin Tang,5 Li Chen,1,2 Xinguo Hou,1,2 Fei Yan1,2
1Department of Endocrinology and Metabolism, Qilu Hospital of Shandong University, Jinan, 250012, People’s Republic of China; 2Shandong Provincial Key Laboratory of Spatiotemporal Regulation and Precision Intervention in Endocrine and Metabolic Diseases, Jinan, 250012, People’s Republic of China; 3University of Health and Rehabilitation Sciences Qingdao Hospital (Qingdao Municipal Hospital), Qingdao, 266071, People’s Republic of China; 4Department of Endocrinology, Tai’an City Central Hospital, Shandong, 271000, People’s Republic of China; 5Department of Endocrinology, Yiyuan County People’s Hospital, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fei Yan, Department of Endocrinology and Metabolism, Qilu Hospital of Shandong University, Jinan, 250012, People’s Republic of China, Tel +8618560088310, Email [email protected]
Purpose: Diabetic retinopathy (DR) is a prevalent microvascular complication of type 2 diabetes mellitus (T2DM). Current research indicates that the association between Vitamin D and diabetic retinopathy, particularly in the early stages, remains controversial. Therefore, we conducted this research to explore the correlation between vitamin D levels and microvascular alterations in nonproliferative diabetic retinopathy (NPDR) patients utilizing optical coherence tomography angiography (OCTA).
Patients and Methods: A cross-sectional analysis was conducted on 286 eyes from 150 subjects with NPDR, with or without diabetic retinopathy. All participants underwent OCTA examinations to assess retinal vessel density (VD), foveal avascular zone (FAZ) area, and retinal thickness. The relationships between vitamin D levels and OCTA-derived parameters were analyzed through multiple regression analyses.
Results: Our analysis revealed a notable decline in retinal vessel density linked to vitamin D deficiency. The superficial vascular complex and the deep vascular complex exhibited reduced vessel density associated with lower vitamin D levels. Additionally, an increase in parathyroid hormone levels significantly correlated with an enlargement of the FAZ area. Vitamin D deficiency was an independent factor in retinal microvascular pathology in T2DM, as evaluated by OCTA.
Conclusion: Individuals with T2DM and vitamin D deficiency were highly recommended to undergo regular ophthalmic screenings to monitor retinal health.
Keywords: diabetic retinopathy, optical coherence tomography angiography, vitamin D, parathyroid hormone, diabetes mellitus
Introduction
Diabetes mellitus (DM) is a rapidly expanding chronic condition with a projected global increase of 25% by 2030 and 51% by 2045.1 Among its various complications, diabetic retinopathy (DR) stands out as a significant ocular issue and the leading cause of blindness associated with DM.2 Effective screening for vascular abnormalities and proactive measures to prevent irreversible damage in high-risk patients are essential to alleviate the societal and financial burdens of DM.
The current diagnosis and treatment of DR often target advanced stages of the disease, where substantial microvascular damage has been presented.2 Histological investigations on human cadavers and animal models have demonstrated that pathologic alterations initiate many years prior to clinical symptoms manifest.3 A deeper comprehension of the pathogenesis of diabetic retinopathy necessitates the development of novel and more sensitive approaches for diagnosing, preventing, and treating the condition at an early stage. Optical coherence tomography angiography (OCTA) has emerged as a promising non-invasive technology that enables a reliable and quantitative microcirculation evaluation across distinct retinal capillary layers.4 OCTA has successfully evaluated various retinal and systemic vascular diseases, including diabetic retinopathy.5,6 Researchers have found that OCTA parameters are correlated with DR and can be used to identify preclinical stages of the disease by detecting early signs of retinal abnormalities.7–9
Vitamin D, known as “the sunshine hormone” for its structure and functions, plays a pivotal role in various physiological processes beyond just bone health.10 It influences cell proliferation, differentiation, apoptosis, immune function, inflammation, and vascular and metabolic functions.11–13 Recent research has increasingly focused on vitamin D’s role in non-traditional outcomes, particularly diabetes and its complications.14,15 Zoppini et al highlighted a strong association between low serum vitamin D levels and the presence of DR in type 2 diabetes patients.16 Alcubierre indicated that individuals with advanced DR exhibited lower serum vitamin D concentrations than those without DR.17 Moreover, vitamin D deficiency has been linked to a higher risk of proliferative diabetic retinopathy, although not with non-proliferative diabetic retinopathy.18,19 However, previous investigations have primarily relied on conventional fundoscopy and have focused on the association of vitamin D with advanced DR, often overlooking its role in the earliest microvascular changes within the retinal capillaries. In contrast, our study utilizes the high-resolution, layer-specific capabilities of OCTA to quantitatively assess both the superficial and deep capillary plexuses-a key methodological advancement-allowing for a more sensitive detection of subclinical alterations. Elucidating this relationship in NPDR is of significant clinical relevance, as serum vitamin D represents a readily measurable, low-cost biomarker. If proven to be a modifiable risk factor, it could open avenues for simple and cost-effective screening strategies and potential therapeutic interventions to prevent or delay the onset of DR. Therefore, this study aimed to examine the correlation between vitamin D levels and early retinal microvascular alterations, utilizing OCTA in patients both without diabetic retinopathy and with non-proliferative diabetic retinopathy.
Materials and Methods
Study Subjects
This retrospective observational study involved 150 type 2 diabetes patients recruited from December 2023 to April 2024 at Qilu Hospital of Shandong University. All participants were of Han Chinese ethnicity and were recruited from the Shandong Province region of China. Eligible participants were those aged 18 years or older, diagnosed with type 2 diabetes according to WHO criteria. Exclusion criteria included: (1) presence of proliferative diabetic retinopathy; (2) a history of vitreous hemorrhage, retinal detachment, intraocular surgery (excluding cataract surgery), or ocular trauma; (3) previous treatment with anti-VEGF drugs or laser therapy; (4) other significant ocular conditions like glaucoma, vitreous diseases, amblyopia, or abnormalities in the optic nerve or cup/disc ratio; (5) severe systemic conditions other than diabetes mellitus like uncontrolled hypertension, malignant tumors, nephritis, or cerebrovascular disorders; (6) history of systemic surgery, thrombolysis therapy, or renal dialysis. The study was approved by the Ethics Committee of the Qilu Hospital of Shandong University (Approval No. KYLL-202311-026). Informed consent was obtained from all participants, and all methods were performed in accordance with the Declaration of Helsinki.
Clinical Assessment
All participants underwent a comprehensive evaluation that included a review of their medical history, a physical examination, routine biochemical tests., dilated color fundus photography, and extraction of study variables. These study variables encompassed various aspects, including demographics (age, sex), physical characteristics [body mass index (BMI), mean arterial pressure (MBP)], lifestyle factors (tobacco smoking, alcohol consumption), and serum markers (HbA1c, potassium, magnesium, creatinine, albumin, total calcium, and 25-OH-vitamin D3). The data for these variables were collected from the patient’s medical records, focusing on values obtained within the three months before their enrollment in the study (closest to the enrollment date). Serum levels of 25-OH-vitamin D3 and parathyroid hormone (PTH) were measured using enzyme-linked immunosorbent assay (ELISA). The reference ranges were 30–100 ng/mL for vitamin D and 15–65 pg/mL for PTH.
Based on the Endocrine Society guidelines, 25-OH-vitamin D3 levels were classified as follows: below 20 ng/mL indicated deficiency, 20 to 30 ng/mL suggested insufficiency, and 30 ng/mL or higher (≥ 75 nmol/L) was considered sufficient.20,21
Ophthalmic Assessment
For each eligible eye, two digital color fundus photographs were obtained and analyzed by seasoned physicians to reduce bias. The presence of DR was determined based on the defined characteristic lesions outlined by the Early Treatment Diabetic Retinopathy Study. Using a non-mydriatic Canon CR-2 camera, single-field 45° images centered on the macula were captured without dilating the pupils for all participants. The criteria for diagnosing DR required detecting at least one definitive microaneurysm and one retinal hemorrhage. DR severity was classified as either non-proliferative (NPDR) or proliferative (PDR).
The study employed a 6×6 mm macular angiogram using an SS OCT-A (BM-400K BMizar, TowardPi Medical Technology, Beijing, China) device. This device featured a swept-source vertical-cavity surface-emitting laser (VCSEL) operating at a wavelength of 1,060 nm and a scanning speed of 400,000 A-scans per second, providing a transverse resolution of 10 µm and an axial optical resolution of 3.8 µm. Each eye underwent scanning over a 6×6 mm area centered on the fovea. Vessel density (VD) was quantified as the ratio of pixels showing positive signal to total pixels within a defined area. The segmentation of retinal layers included the identification of the superficial vascular complex (SVC) spanning from the internal limiting membrane (ILM) to 10 µm above the inner plexiform layer (IPL), and the deep vascular complex (DVC) spanning from 10 µm above the IPL to 10 μm below the outer plexiform layer (OPL). Evaluation of the foveal avascular zone (FAZ) encompassed the region between the ILM and the OPL within the macular area, expressed in mm2. Specifically, the parafoveal region was defined as a 2.0 mm wide annulus extending outward from the 1.0 mm circle centered on the fovea, while the perifoveal region was characterized as a 3.0 mm wide annulus extending outward from the parafoveal area. Furthermore, the macular region, a 6×6 mm square centered on the fovea, was also analyzed, Figure 1. OCTA image quality was assessed based on signal strength, clarity, and the absence of significant artifacts. Images with a signal strength index (SSI) below 7, significant motion artifacts, poor centration, or segmentation errors were excluded from the analysis. For each participant, the right eye was preferentially analyzed. If the right eye image did not meet the quality standards, the left eye was used provided it satisfied all QC criteria. Based on these criteria, a total of 15 eyes from the initially recruited pool were excluded from the final analysis.
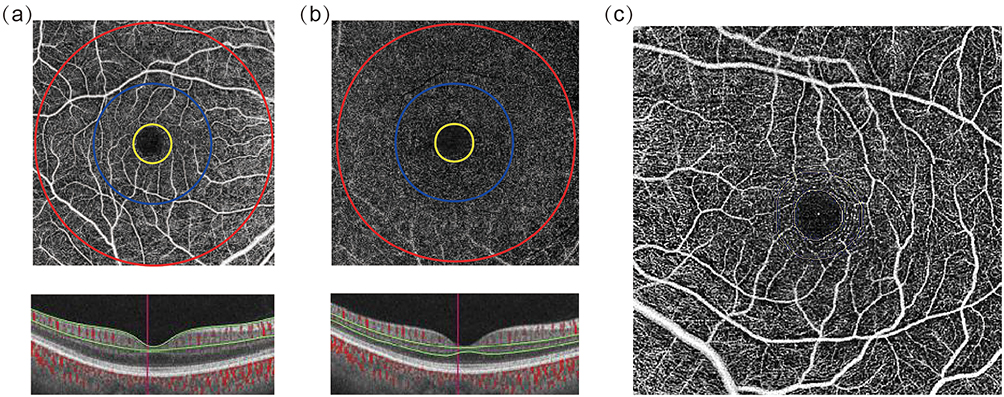 |
Figure 1 Quantitative measurement using OCTA in a healthy eye. (a) The OCTA images of the superficial vascular plexus (from ILM to 10 μm above IPL). Fovea: the region inside the yellow ring; parafovea: the region (ring diameter = 2 mm) between the yellow ring and red ring; perifovea: the region (ring diameter = 3 mm) between the red circle and blue circle. (b) The OCTA images of the deep vascular plexus (from 10 μm above IPL to 10 μm below OPL). (c) The area of the inner yellow circle is the FAZ area. |
Statistical Analysis
Statistical analyses were performed utilizing SPSS software (version 23; SPSS, Chicago, IL). Normality of data distribution was assessed using the Shapiro–Wilk test. Data were categorized based on their distribution: non-parametric variables were expressed as medians and interquartile ranges, while parametric variables were reported as means and standard deviations (SD). Differences between groups for normally distributed variables were assessed utilizing an independent-sample t-test, whereas the Mann–Whitney U-test was utilized for non-parametric variables. Differences in frequencies were analyzed utilizing the χ2 test or Fisher’s exact test, as appropriate. The relationships between clinical parameters and OCTA measurements were examined utilizing Spearman’s rank correlation test. Bonferroni correction was applied to correct P-values for multiple comparisons. Additionally, multiple linear regression was employed to explore the associations between indicators (independent variables) and OCTA measurements (dependent variables). Generally, only the right eye of each participant was analyzed; however, if OCTA images of the right eye were of poor quality, the left eye was examined instead. The significance level was set at P < 0.05.
Results
Baseline Characteristics of the Study Population
Our study enrolled 150 participants prospectively. The median age was 59 years, with an interquartile range from 50 to 65 years, and 36.7% (55 participants) were men. Participants had been diagnosed with type 2 diabetes for a median duration of 10 years, with an interquartile range of 5 to 18 years. Notably, 49.3% of the participants (74 individuals) exhibited vitamin D deficiency.
Table 1 presents the demographic and clinical characteristics of all patients, categorized by their vitamin D status. A comparison of patients with and without vitamin D deficiency revealed no significant differences in age, sex, duration of diabetes, HbA1c, MBP, FBG, HOMA-IR, Cr, TG, TC, and PTH. Patients with vitamin D deficiency displayed reduced vessel density in the SVC and DVC compared to those without vitamin D deficiency (all P < 0.005). However, the FAZ area and GCC thickness were comparable between these two groups.
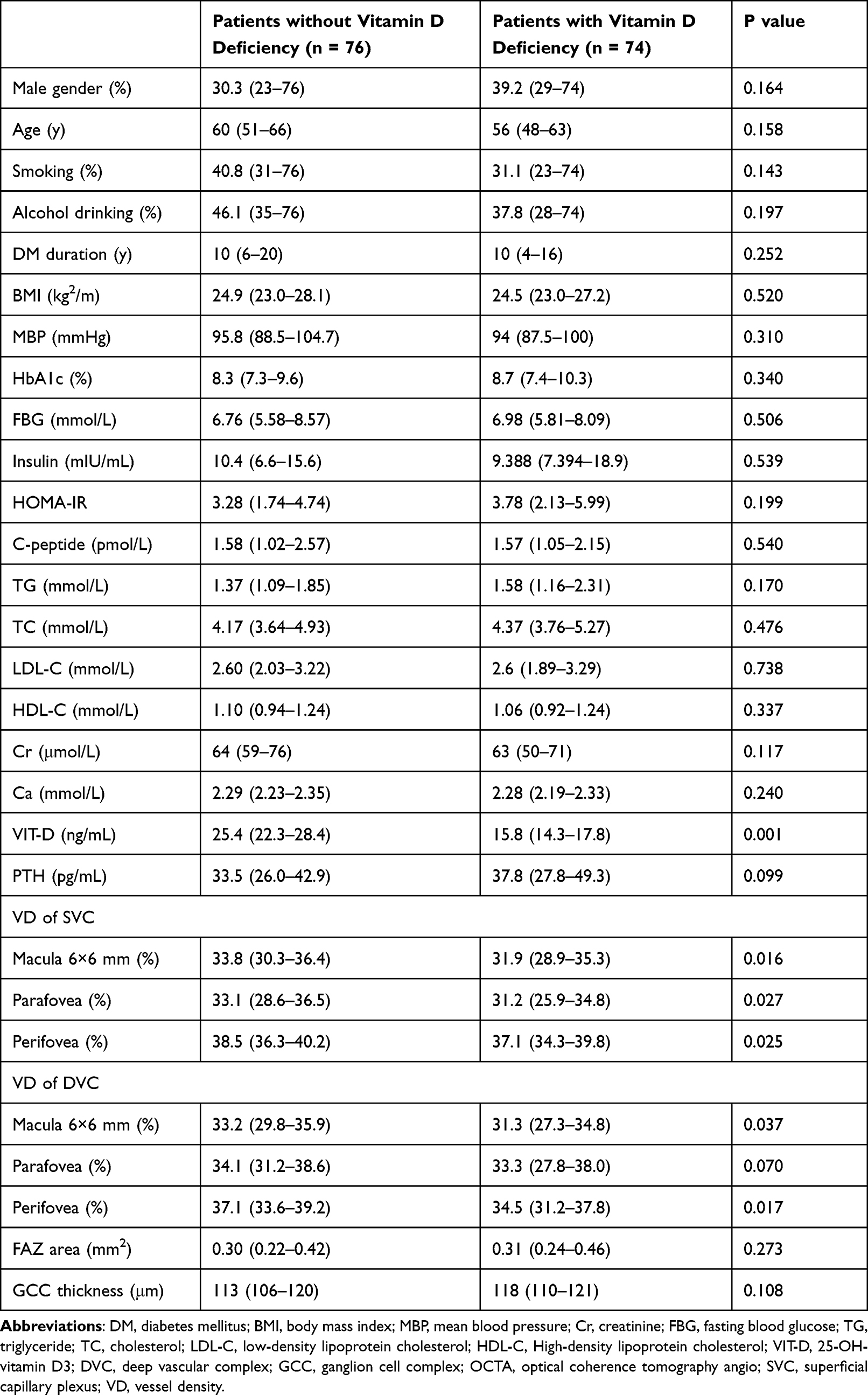 |
Table 1 Clinical Parameters in Different Study Groups |
Association of Clinical Data and OCTA Parameters
Table 2 displays the Spearman correlation coefficients between OCTA parameters and clinical data. Vitamin D exhibited positive associations with VD of SVC and DVC while displaying negative correlations with FAZ area (all P < 0.05). PTH levels were negatively correlated with the VD of the DVC (P < 0.05) and positively associated with the FAZ area. HOMA-IR showed a positive correlation with the macula 6×6 mm area of the DVC (r = 0.190, P = 0.022). HbA1C was positively associated with perifovea (r = 0.169, P = 0.045).
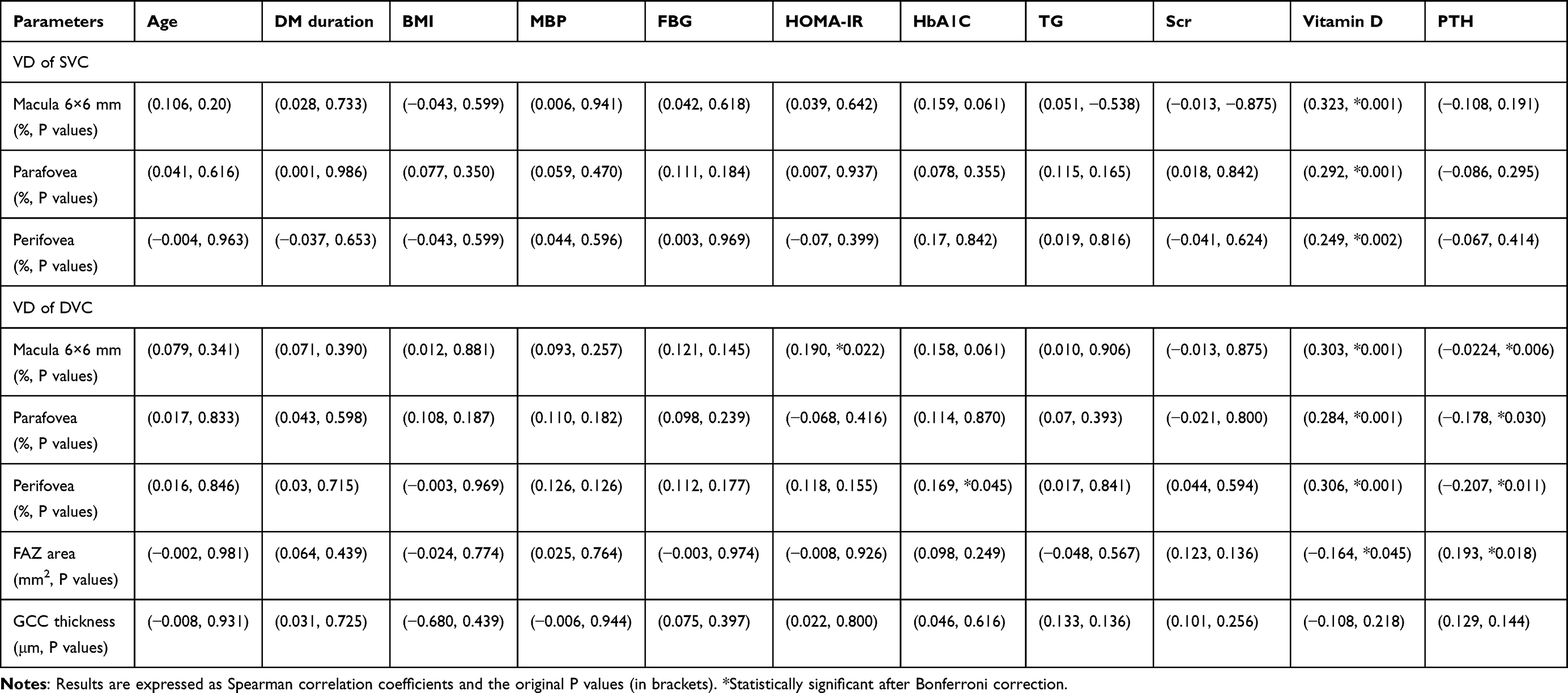 |
Table 2 Spearman Correlation Coefficients Between the OCTA Parameters and Clinical Data |
Multiple Linear Regression Analysis of OCTA Parameters
The multiple linear regression analyses indicated a correlation between higher Vitamin D levels and increased vessel density within the SVC and DVC across the macula’s 6×6 mm parafoveal and perifoveal areas (all P < 0.05, Table 3). Furthermore, a negative association was observed between Vitamin D levels and FAZ area (β = −0.005, P = 0.017, Table 3). However, no significant association was found between Vitamin D levels and GCC thickness. The multiple linear regression analyses also demonstrated an association between PTH levels and FAZ area (β = 0.002, P = 0.040, Table 4). Conversely, no significant association was found between PTH levels and vessel density of SVC and DVC (Table 4).
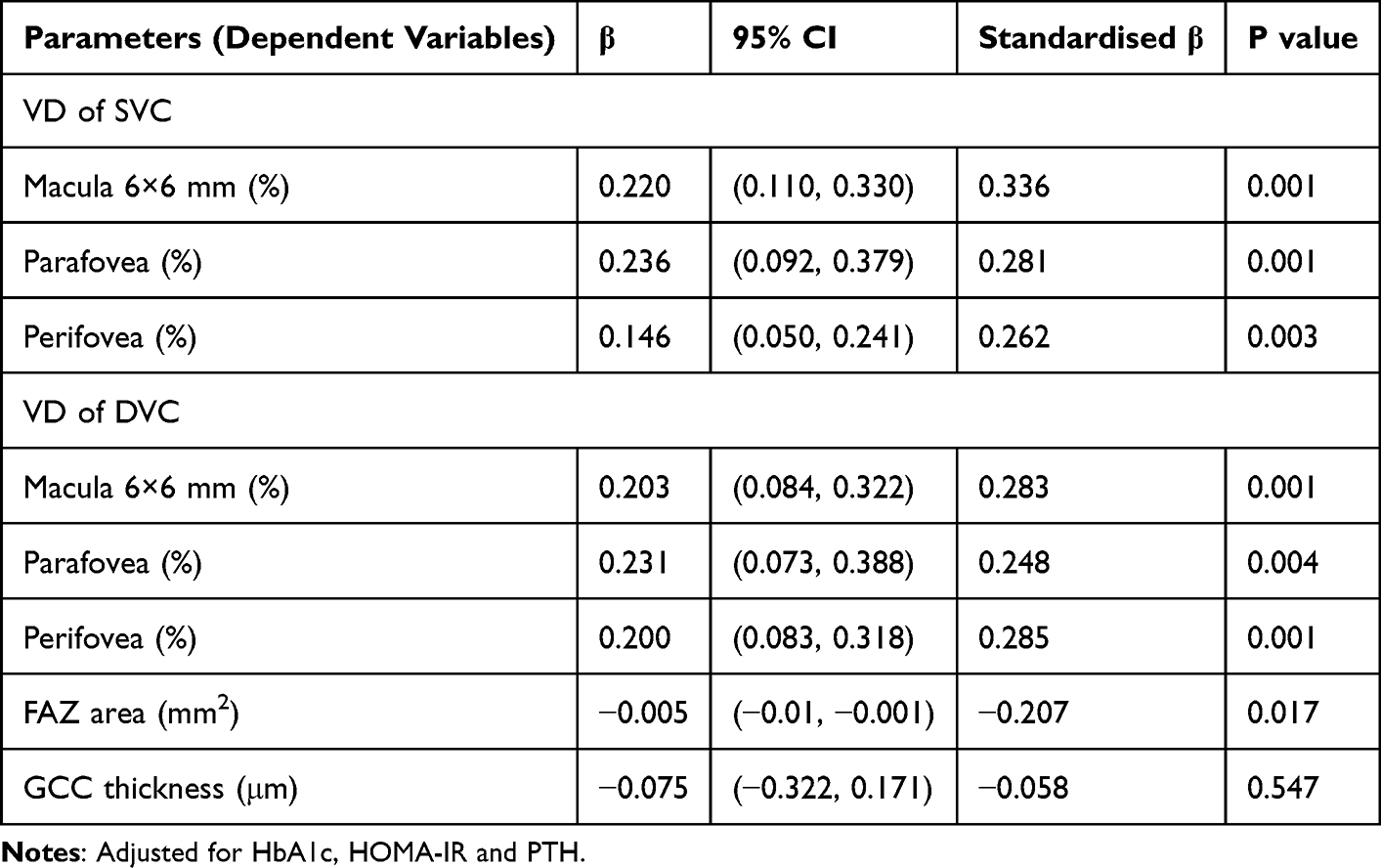 |
Table 3 Multiple Regression Models of Vitamin D with OCTA Parameters (Dependent Variables) |
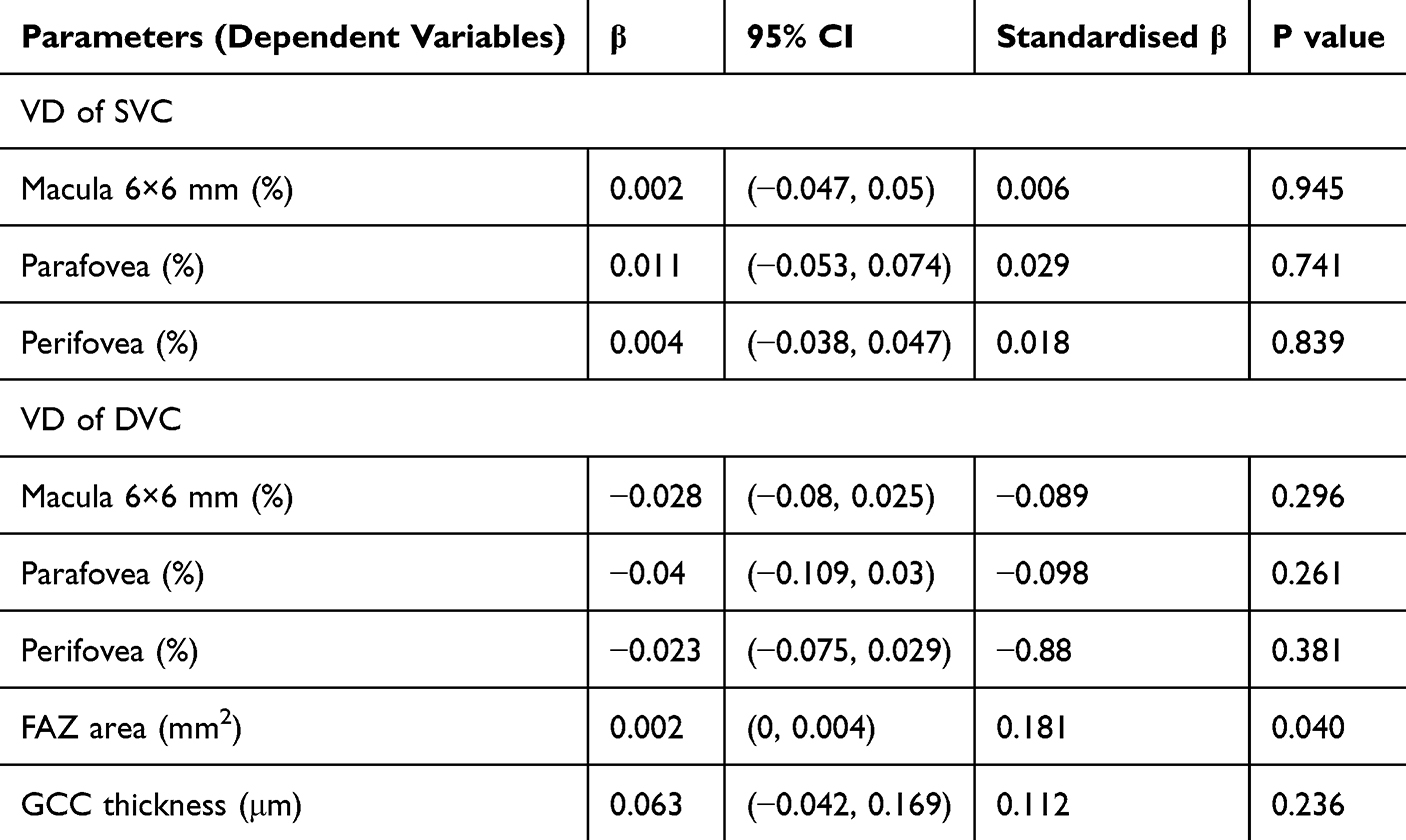 |
Table 4 Multiple Regression Models of PTH with OCTA Parameters (Dependent Variables) |
Discussion
This research explored the links between clinical data and retinal microvascular alterations as assessed by OCTA in the early stage of diabetic retinopathy. Our analysis revealed a notable decrease in retinal vessel density associated with vitamin D deficiency. Specifically, reduced density in the SVC and DVC correlated with lower vitamin D levels. Moreover, we identified an inverse association between vitamin D levels and the FAZ area. Elevated PTH levels were significantly associated with increased FAZ area within the retina. This investigation represents the initial comprehensive analysis of the connection between retinal structure, capillary density, and vitamin D and PTH levels in individuals diagnosed with type 2 diabetes.
Diabetic retinopathy represents a significant microvascular complication of type 2 diabetes with potentially severe consequences, including proliferative retinopathy and vision loss. Timely screening is crucial for early detection to prevent the progression to advanced stages of the disease. OCTA emerges as a promising non-invasive technology that offers a reproducible and quantitative assessment of the microcirculation within different layers of the retina.22–24 Numerous clinical studies have demonstrated the utility of OCTA in identifying diabetic retinopathy at earlier stages than traditional clinical examination methods. Patients with diabetes, even in the absence of apparent retinopathy signs, have been found to exhibit lower retinal VD on OCTA compared to non-diabetic individuals.4,25 Multiple studies have indicated significant associations between diabetic retinopathy progression and specific OCTA metrics, including an enlarged FAZ area, reduced FAZ circularity and decreased VD in the SVC and DVC.26,27 The findings presented are primarily derived from cross-sectional studies. Sun et al investigated the utility of OCTA in predicting the progression of DR. The results demonstrated that the metrics for VD and FD at the DVC were correlated with the risks of DR progression. In contrast, metrics at the SVC did not show the same associations. These results highlight the significance of OCTA in identifying early macular microvascular changes in diabetic retinopathy.
Vitamin D has been suggested to play a crucial role in ocular health through its impact on various physiological processes. The presence of the VDR in the retina and human retinal endothelial cells underscores its potential influence on ocular function.28 Research has demonstrated that vitamin D can modulate peripheral and microvessel circulation by regulating the renin-angiotensin system and enhancing endothelial cell-mediated vasodilatation.29 The protective role of vitamin D in retinal microvascular health may be mediated through multiple pathways. First, vitamin D exerts anti-inflammatory effects by suppressing pro-inflammatory cytokines and inhibiting nuclear factor kappa-B (NF-κB) signaling. Second, it enhances endothelial function by promoting nitric oxide synthesis and reducing oxidative stress. Third, vitamin D modulates the renin-angiotensin system, thereby mitigating angiotensin II–induced vasoconstriction and endothelial dysfunction. Additionally, the presence of vitamin D receptors in retinal endothelial cells supports a direct role in maintaining vascular integrity. These mechanisms collectively suggest that vitamin D deficiency may exacerbate microvascular damage in diabetes, highlighting its potential as a modifiable risk factor in early DR. Evidence indicated that vitamin D may lower the risk of developing open-angle glaucoma by enhancing ocular blood flow, a process intricately linked to endothelial function and the renin-angiotensin system.30 Recent research has highlighted a strong link between vitamin D deficiency and an increased risk of proliferative diabetic retinopathy, but such an association did not exist for nonproliferative diabetic retinopathy.9,18 This study investigated the association between vitamin D levels and retinal microvascular alterations, as assessed by OCTA, in diabetic patients with non-proliferative diabetic retinopathy. It should be noted that our findings of a significant association contrast with some previous reports that have found no clear link between vitamin D and diabetic retinopathy. Such discrepancies could stem from methodological differences, including variations in OCTA acquisition settings, segmentation techniques, or the assays used to measure vitamin D levels.
This discrepancy may be attributed to sensitivity of the assessment tool. Previous studies relied on clinical grading of DR based on fundus photography, which detects relatively late-stage structural lesions. In contrast, our use of OCTA allows for the quantification of subtle, preclinical microvascular changes in the capillary networks that are not visible on fundoscopy. Our findings revealed that diabetic patients with vitamin D deficiency exhibited decreased vessel density in SVC and DVC compared to those without a deficiency in vitamin D. We also found that lower vessel density in the SVC and DVC was linked to reduced levels of vitamin D in diabetic eyes. Furthermore, we observed a negative correlation between vitamin D levels and the area of the FAZ. These findings suggest that vitamin D deficiency could be a potential biomarker for the early detection of diabetic retinopathy. This study extends current knowledge by demonstrating, through high-resolution OCTA, that vitamin D deficiency is associated with reduced vessel density in both the superficial and deep retinal vascular plexuses in NPDR patients. This layer-specific analysis suggests that vitamin D may exert a generalized protective effect on the retinal microvasculature, detectable even before advanced retinopathic changes occur.
Parathyroid hormone is a systemic hormone crucial for regulating calcium, phosphate, and vitamin D levels, thereby playing a significant role in mineral metabolism and bone turnover. The wide-ranging effects of parathyroid hormone are mediated through the PTH1R, which is broadly distributed throughout the body, exhibiting higher expression levels in the bone and kidney.31,32 Interestingly, PTH1R has also been identified in the myocardium and vasculature, indicating potential links to cardiovascular diseases. Research has shown that even normal-range elevated PTH levels are associated with an increased cardiovascular risk, independent of other risk factors.33,34 Gambardella showed that PTH could induce mitochondrial reactive oxygen species (ROS) production and increase intracellular calcium (Ca2+) accumulation in endothelial cells, leading to oxidative stress and severe cellular injury. This endothelial damage could compromise capillary integrity and promote apoptosis, potentially contributing to capillary dropout and FAZ enlargement in the retina.31 Consistent with previous findings, our research revealed significant correlations between PTH levels and the area of the FAZ. However, our analysis revealed no significant correlations between PTH levels and VD in the SVC and DVC.
No significant correlations were observed between diabetes-related factors, such as duration of diabetes and recent HbA1c levels, and the OCTA parameters examined in the study. This finding is unexpected, as these variables are commonly linked to the risk and advancement of diabetic retinopathy in previous literature. However, this outcome may be due to the pre-clinical nature of the patient population in our study. In our investigation, these variables may exhibit a slight connection with microvascular changes that can be discerned through advanced imaging modalities like OCTA.
The observed correlation between vitamin D deficiency and early microvascular impairment, measured via OCTA, indicates that serum vitamin D levels may serve as a useful biomarker for stratifying T2DM patients according to their risk of developing diabetic retinopathy. While our findings do not support a causal relationship, they highlight the need to explore the potential of vitamin D supplementation in slowing DR progression. Existing mechanistic studies offer plausible pathways: vitamin D has been shown to suppress retinal neovascularization in experimental models, attenuate the transcriptional activity of hypoxia-inducible factor-1 (HIF-1), and downregulate matrix metalloproteinase (MMP) expression—all key processes implicated in DR pathogenesis.35 These collective insights strengthen the justification for a rigorously designed, randomized, placebo-controlled clinical trial to evaluate whether vitamin D supplementation can mitigate the initiation or advancement of diabetic retinopathy.
It should be noted that our findings of a significant association contrast with some previous reports that have found no clear link between vitamin D and diabetic retinopathy. Such discrepancies could stem from methodological differences, including variations in OCTA acquisition settings, segmentation techniques, or the assays used to measure vitamin D levels.
The current study has several limitations. Firstly, its retrospective nature precludes the ability to establish causality. Secondly, all participants were hospitalized in a specific geographical area, thereby limiting the extrapolation of the findings to more diverse populations. Thirdly, the sample size, while adequate for initial correlation analyses, may be underpowered to detect subtle relationships, especially in subgroup comparisons (eg, between different stages of NPDR). The lack of a pre-specified sample size calculation is a limitation. Future longitudinal studies with larger, prospectively recruited cohorts are needed to confirm and extend our findings. Lastly, a small field of view (6 mm x 6 mm) in OCT angiography may not fully represent the entire retinal circulation.
Conclusion
In conclusion, our study revealed a link between vitamin D deficiency and reduced retinal microvascular parameters assessed through OCTA in the early stage of diabetic retinopathy. These findings emphasize the importance of promoting regular ophthalmic screenings for vitamin D-deficient individuals.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Author Contributions
ZW and KW contributed equally to this work and should be considered co-first authors. ZW and KW contributed to the conceptualization. YL, PL, and YT conducted formal analysis. LC conducted the data curation. XH contributed to the supervision and visualization. FY contributed to writing - original draft and funding acquisition. FY and KW contributed to the review and editing. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study received funding from the National Natural Science Foundation of China (grant number 81800736), National Natural Science Foundation of China (NSFC) Regional Innovation and Development Joint Fund (grant number U24A20374), China Endocrine and Metabolic Talent Research Project (grant number 2023-N-03-09), and Shandong Provincial Natural Science Foundation (grant number ZR2023MH049).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
2. Simo R, Stitt AW, Gardner TW. Neurodegeneration in diabetic retinopathy: does it really matter? Diabetologia. 2018;61(9):1902–1912. doi:10.1007/s00125-018-4692-1
3. Seyyar SA, Tiskaoglu NS, Tokuc EO, et al. Is serum vitamin D associated with diabetic retinopathy and its severity or with diabetes itself ? Clin Exp Optom. 2023;106(6):612–618. doi:10.1080/08164622.2022.2090232
4. Simonett JM, Scarinci F, Picconi F, et al. Early microvascular retinal changes in optical coherence tomography angiography in patients with type 1 diabetes mellitus. Acta Ophthalmol. 2017;95(8):e751–e755. doi:10.1111/aos.13404
5. Sun Z, Yang D, Tang Z, et al. Optical coherence tomography angiography in diabetic retinopathy: an updated review. Eye. 2021;35(1):149–161. doi:10.1038/s41433-020-01233-y
6. Elnahry AG, Noureldine AM, Abdel-Kaderi AA, et al. Optical coherence tomography angiography biomarkers predict anatomical response to bevacizumab in diabetic macular edema. Diabet Metabo Syndro Obes Targets Therapy. 2022;15:395–405. doi:10.2147/DMSO.S351618
7. Xu F, Li Z, Yang X, et al. Assessment of choroidal structural changes in patients with pre- and early-stage clinical diabetic retinopathy using wide-field SS-OCTA. Front Endocrinol. 2022;13:1036625. doi:10.3389/fendo.2022.1036625
8. Sun Z, Tang F, Wong R, et al. OCT angiography metrics predict progression of diabetic retinopathy and development of diabetic macular edema: a prospective study. Ophthalmology. 2019;126(12):1675–1684. doi:10.1016/j.ophtha.2019.06.016
9. Yuan M, Wang W, Kang S, et al. Peripapillary microvasculature predicts the incidence and development of diabetic retinopathy: an SS-OCTA study. Am J Ophthalmol. 2022;243:19–27. doi:10.1016/j.ajo.2022.07.001
10. Pittas AG, Jorde R, Kawahara T, et al. Vitamin D supplementation for prevention of type 2 diabetes mellitus: to D or not to D? J Clin Endocrinol Metab. 2020;105(12):3721–3733. doi:10.1210/clinem/dgaa594
11. Heaney RP. Vitamin D in health and disease. Clin J Am Soc Nephrol. 2008;3(5):1535–1541. doi:10.2215/CJN.01160308
12. Plum LA, DeLuca HF. Vitamin D, disease and therapeutic opportunities. Nat Rev Drug Discov. 2010;9(12):941–955. doi:10.1038/nrd3318
13. Wang SQ, Gao HN, Zhang MM, et al. High apolipoprotein B/apolipoprotein A1 is associated with vitamin D deficiency among type 2 diabetes patients. Diabet Metab Syndro Obes. 2024;17:2357–2369. doi:10.2147/DMSO.S465391
14. Maddaloni E, Cavallari I, Napoli N, et al. Vitamin D and Diabetes Mellitus. Front Horm Res. 2018;50:161–176.
15. Mao R, Zhou G, Jing D, et al. Vitamin D status, Vitamin D receptor polymorphisms, and the risk of incident rosacea: insights from Mendelian randomization and cohort study in the UK biobank. Nutrients. 2023;16(1):15. doi:10.3390/nu16010015
16. Zoppini G, Galletti A, Targher G, et al. Lower levels of 25-hydroxyvitamin D 3 are associated with a higher prevalence of microvascular complications in patients with type 2 diabetes. BMJ Open Diabetes Res Care. 2015;3(1):e000058. doi:10.1136/bmjdrc-2014-000058
17. Alcubierre N, Valls J, Rubinat E, et al. Vitamin D deficiency is associated with the presence and severity of diabetic retinopathy in type 2 diabetes mellitus. J Diabetes Res. 2015;2015:374178. doi:10.1155/2015/374178
18. Navaei S, Nazemi S, Emamian MH, et al. Vitamin D deficiency and diabetic retinopathy risk. J Fr Ophtalmol. 2023;46(7):737–741. doi:10.1016/j.jfo.2023.01.024
19. Yuan J, Zhou JB, Zhao W, et al. Could vitamin D be associated with proliferative diabetic retinopathy? Evidence from pooling studies. Horm Metab Res. 2019;51(11):729–734. doi:10.1055/a-1010-6449
20. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–1930. doi:10.1210/jc.2011-0385
21. Guarnotta V, Di Gaudio F, Giordano C. Vitamin D deficiency in cushing’s disease: before and after its supplementation. Nutrients. 2022;15(1):14. doi:10.3390/nu15010014
22. Jia Y, Bailey ST, Wilson DJ, et al. Quantitative optical coherence tomography angiography of choroidal neovascularization in age-related macular degeneration. Ophthalmology. 2014;121(7):1435–1444. doi:10.1016/j.ophtha.2014.01.034
23. Waheed NK, Rosen RB, Jia Y, et al. Optical coherence tomography angiography in diabetic retinopathy. Prog Retin Eye Res. 2023;97:101206. doi:10.1016/j.preteyeres.2023.101206
24. Chua J, Sim R, Tan B, et al. Optical coherence tomography angiography in diabetes and diabetic retinopathy. J Clin Med. 2020;10(1):9. doi:10.3390/jcm10010009
25. Durbin MK, An L, Shemonski ND, et al. Quantification of retinal microvascular density in optical coherence tomographic angiography images in diabetic retinopathy. JAMA Ophthalmol. 2017;135(4):370–376. doi:10.1001/jamaophthalmol.2017.0080
26. Johannesen SK, Viken JN, Vergmann AS, et al. Optical coherence tomography angiography and microvascular changes in diabetic retinopathy: a systematic review. Acta Ophthalmol. 2019;97(1):7–14. doi:10.1111/aos.13859
27. Lee H, Lee M, Chung H, et al. Quantification of retinal vessel tortuosity in diabetic retinopathy using optical coherence tomography angiography. Retina. 2018;38(5):976–985. doi:10.1097/IAE.0000000000001618
28. Zhan D, Zhao J, Shi Q, et al. 25-hydroxyvitamin D3 inhibits oxidative stress and ferroptosis in retinal microvascular endothelial cells induced by high glucose through down-regulation of miR-93. BMC Ophthalmol. 2023;23(1):22. doi:10.1186/s12886-022-02762-8
29. de la Guia-Galipienso F, Martinez-Ferran M, Vallecillo N, et al. Vitamin D and cardiovascular health. Clin Nutr. 2021;40(5):2946–2957. doi:10.1016/j.clnu.2020.12.025
30. Huynh B, Shah P, Sii F, et al. Low systemic vitamin D as a potential risk factor in primary open-angle glaucoma: a review of current evidence. Br J Ophthalmol. 2021;105(5):595–601. doi:10.1136/bjophthalmol-2020-316331
31. Gambardella J, De Rosa M, Sorriento D, et al. Parathyroid hormone causes endothelial dysfunction by inducing mitochondrial ROS and specific oxidative signal transduction modifications. Oxid Med Cell Longev. 2018;2018(1):9582319. doi:10.1155/2018/9582319
32. Wannamethee SG, Welsh P, Papacosta O, et al. Elevated parathyroid hormone, but not vitamin D deficiency, is associated with increased risk of heart failure in older men with and without cardiovascular disease. Circ Heart Fail. 2014;7(5):732–739. doi:10.1161/CIRCHEARTFAILURE.114.001272
33. Hagstrom E, Hellman P, Larsson TE, et al. Plasma parathyroid hormone and the risk of cardiovascular mortality in the community. Circulation. 2009;119(21):2765–2771. doi:10.1161/CIRCULATIONAHA.108.808733
34. Pascale AV, Finelli R, Giannotti R, et al. Vitamin D, parathyroid hormone and cardiovascular risk: the good, the bad and the ugly. J Cardiovasc Med. 2018;19(2):62–66. doi:10.2459/JCM.0000000000000614
35. Gverovic Antunica A, Znaor L, Ivanković M, et al. Vitamin D and diabetic retinopathy. Int J Mol Sci. 2023;24(15):12014. doi:10.3390/ijms241512014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association of Axial Length with Macular Microvascular Changes in Chinese Diabetic Retinopathy Patients
Zhang Q, Yang L, Xu X, Lan X, Wang Z, Sun Y, Fu S, Xiong Y
International Journal of General Medicine 2022, 15:3895-3902
Published Date: 8 April 2022
Prevalence and Factors Associated with Diabetic Retinopathy among Adult Diabetes Patients in Southeast Ethiopia: A Hospital-Based Cross-Sectional Study
Sahiledengle B, Assefa T, Negash W, Tahir A, Regasa T, Tekalegn Y, Mamo A, Teferu Z, Solomon D, Gezahegn H, Bekele K, Zenbaba D, Tasew A, Desta F, Regassa Z, Feleke Z, Kene C, Tolcha F, Gomora D, Dibaba D, Atlaw D
Clinical Ophthalmology 2022, 16:3527-3545
Published Date: 20 October 2022
Psychometric Impact of Diabetic Retinopathy-Induced Visual Impairment: A Hospital-Based Study, Al Buraimi, Sultanate of Oman
Vankudre GS, Mohamed ZD, Ayyappan JP, Alrasheed SH
Clinical Optometry 2025, 17:3-10
Published Date: 13 January 2025
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025
Central Macular Thickness and Foveal Avascular Zone are Indicators of Early Diabetic Retinopathy
Wei Q, Wang W, Qiu Q
Clinical Ophthalmology 2025, 19:3505-3514
Published Date: 22 September 2025