Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Association Between Serum Vitamin D3 Levels and Diabetic Macular Edema in Patients with Type 2 Diabetes: A Retrospective Case-Control Study
Authors Al-latayfeh M ![]() , Shatnawi RA
, Shatnawi RA ![]() , Abu-Ain MS
, Abu-Ain MS ![]() , Alotaibi TM, Albazee E
, Alotaibi TM, Albazee E ![]() , Al-balawi M, Alnifise MH
, Al-balawi M, Alnifise MH
Received 17 December 2025
Accepted for publication 9 February 2026
Published 20 February 2026 Volume 2026:19 588850
DOI https://doi.org/10.2147/DMSO.S588850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Motasem Al-latayfeh,1,2 Raed A Shatnawi,1,2 Mohammad Saleh Abu-Ain,1,2 Talal Muteb Alotaibi,3 Ebraheem Albazee,4 Mohammed Al-balawi,5 Mohammad Hamd Alnifise6
1Department of Special Surgery, Faculty of Medicine, The Hashemite University, Zarqa, Jordan; 2Department of Ophthalmology, Prince Hamza Hospital, Amman, Jordan; 3General Surgery- General Surgery Department, KSA, Security Forces Hospital, Riyadh, Saudi Arabia; 4Otorhinolaryngology-Head and Neck Surgery, Kuwait Institute for Medical Specializations, Kuwait City, Kuwait; 5Internal Medicine Dept, King Fahad Specialist Hospital, Tabuk, Saudi Arabia; 6Primary Health Care Center, Qassim Health Cluster, Qassim Region, Saudi Arabia
Correspondence: Motasem Al-latayfeh, The Hashemite University, Tel +962797397711, Email [email protected]
Objective: To evaluate the association between serum vitamin D3 levels in patients with type two diabetes mellitus (T2DM) and diabetic macular edema (DME) taking into consideration other factors such as demographic, metabolic, and clinical confounders.
Methods: This retrospective case–control study included patients with T2DM attending a tertiary ophthalmology clinic. Cases were patients with clinical and OCT-confirmed DME. Controls had no DME. Patients with severe NPDR or higher stage were excluded. The study involved collecting several variables including age, sex, diabetes duration, HbA1c, BMI, smoking status, vitamin D3 levels, comorbidities, and vitamin D supplementation. Vitamin D3 was categorized into three groups: < 10, 10– 30, and > 30 ng/mL. Logistic regression was used to identify independent predictors of DME.
Results: A total of 332 participants were analyzed. A total of 184 control patients were compared to 148 DME patients. DME patients had significantly longer diabetes duration (12.91 y vs 17.21 y, p < 0.001 for Non-DME and DME groups respectively) and lower vitamin D3 levels (25.16 ng/mL vs 16.71 ng/mL, p < 0.001 for non DME and DME groups respectively). Vitamin D3 deficiency (< 10 ng/mL) was independently associated with increased odds of DME, whereas vitamin D3 sufficiency (> 30 ng/mL) was protective. Cigarette smoking, paradoxically, was found to be associated with lower odds for DME.
Conclusion: Vitamin D3 deficiency is associated with increased odds of DME. Interpretation should be cautious due to methodological limitations, including potential selection bias, unmeasured confounding, and lack of adjustment for diabetic retinopathy severity. Further research is required to explore further cause-effect relationship and effect of supplementation on the disease itself and response to treatment.
Keywords: type 2 diabetes mellitus, diabetic retinopathy, diabetic macular edema, Vitamin D3, smoking, risk factors, anti-VEGF
Introduction
Diabetic eye disease is a leading cause of vision loss worldwide.1 Diabetic retinopathy (DR) ranks as the 5th most common cause of preventable blindness and of visual impairment.2 Approximately, diabetic retinopathy affects one in three people with diabetes.3 A third of those with diabetic retinopathy are afflicted with vision-threatening retinopathy or diabetic macular edema.4 Diabetic macular edema (DME) can present at any stage of diabetic retinopathy and is characterized by retinal vessel leakage, decreased endothelial integrity, and exudative fluid accumulation in the macula.5 Chronic hyperglycemia within the context of inflammation and the advanced build-up of glycation end products contributes to the development of DME.6 Due to its rising prevalence relative to that of diabetes, the impact of DME is associated with substantial costs to any healthcare system.7
Diet and lifestyle choices are integral components of managing diabetes and its macro/micro-vascular complications.8 The entire spectrum of dietary components is composed of a myriad of factors, each with a unique association towards diabetic retinopathy and its associated complications. Of the many factors studied, vitamins show potential associations yet no concordance on exact mechanism and role in the development of diabetic retinopathy.
Vitamin D3 (VitD3) has demonstrated anti-inflammatory, anti-angiogenic, and endothelial-stabilizing effects through modulation of VEGF signaling and inflammatory cytokines, mechanisms central to the pathogenesis of diabetic macular edema.6 Although several observational studies have linked VitD3 deficiency with diabetic retinopathy, evidence specifically examining its role in DME remains limited and inconsistent, partly due to heterogeneity in study design and methodology. Khater et al reported that VitD3 deficiency may influence the macular vascular density and size of foveal avascular zone (FAZ).9 Also, D’Angelo et al in their narrative review about the role of dietary supplements in DME suggested that vitamin D may help prevent DR through its anti-inflammatory and antiangiogenic effects.10
Given the high prevalence of VitD3 deficiency in Middle Eastern populations, including Jordan, understanding its role in diabetic retinal complications carries important regional public health implications.11 Given that, with the theoretical biological relationship between VitD3 status and retinal vascular integrity, this study aimed to evaluate whether serum VitD3 levels are associated with the presence of DME in patients with diabetes, while accounting for demographic, clinical, and metabolic covariates.
Methodology
This is a retrospective case-control study. It was conducted at a major tertiary center in Jordan. The study was approved by the Institutional Review Board at The Hashemite University in Jordan (IRB No 12/2020) and adhered to Declaration of Helsinki. Informed consent from patients was not obtained because it was waived by ethics committee since the study was a retrospective study and did not involve revealing any personal details of patients.
Selection of the study patients was based on chart documentation of DR, DME and optical coherence tomography (OCT) findings. DME group of patients was selected randomly from patients with DM who are visiting ophthalmology clinic, diagnosed with DME clinically and OCT Central Mean Thickness (CMT) >300 (on Optopol OCT machine, Optopol Inc. Poland), and currently being treated with anti-VEGF or scheduled to start anti-VEGF therapy. Control group included patients with DM with no documented DME based on OCT findings (CMT<=300). Central macular thickness was defined as the mean thickness within the central 1-mm ETDRS subfield measured by OCT. We excluded patients with documented severe non-proliferative DR or above or those whose reported VitD3 level was more than six months from the diagnosis of DME. Data collected for both groups included: age, sex, duration of DM, smoking status, body mass index (BMI), HgA1c level, VitD3 level, Cholesterol, and Triglycerides serum levels. Serum VitD3 measurements were obtained from medical records; detailed assay methodology was not consistently available due to the retrospective design. Associated comorbidities such as hypertension, chronic renal disease and hyperlipidemia were also recorded. Taking VitD3 supplements was noted. VitD3 level was recorded as absolute value and further all patients were categorized into three categories of VitD3 deficiency according to our laboratory standards: Deficient: VitD3 < 10 ng/mL, Insufficient: 10<=VitD3=<30 ng/mL, Sufficient: VitD3 > 30 ng/mL.
All data for both groups were recorded into an Excel sheet. SPSS statistical package 27 (IBM Corp, USA) was used to analyze the data. Statistical methods employed included descriptive statistics for both groups showing mean, and standard deviation for continuous variables, and frequencies for categorical variables. Cases with missing key variables were excluded, and no imputation methods were applied. Univariate and multivariate analysis were employed to study the effect of various factors on the development of DME in patients with DM with specific emphasis on role of VitD3 levels and VitD3 supplements. Model diagnostics included checks for multicollinearity and goodness-of-fit. Significance level was considered at p-value of 0.05.
Results
A total of 332 participants were included in the final analysis. Table 1 summarizes the demographic data for both groups. No significant age or sex differences were found between both groups. Also, there were no significant differences between groups in terms of diabetic control (HbA1c), BMI, and other medical comorbidities such as hypertension, renal diseases and hypercholesterolemia. However, patients with DME have longer duration of DM (12.91 y vs 17.21 y, p < 0.001 for Non-DME and DME groups, respectively). Smoking was more prevalent in non-DME patients (p < 0.001).
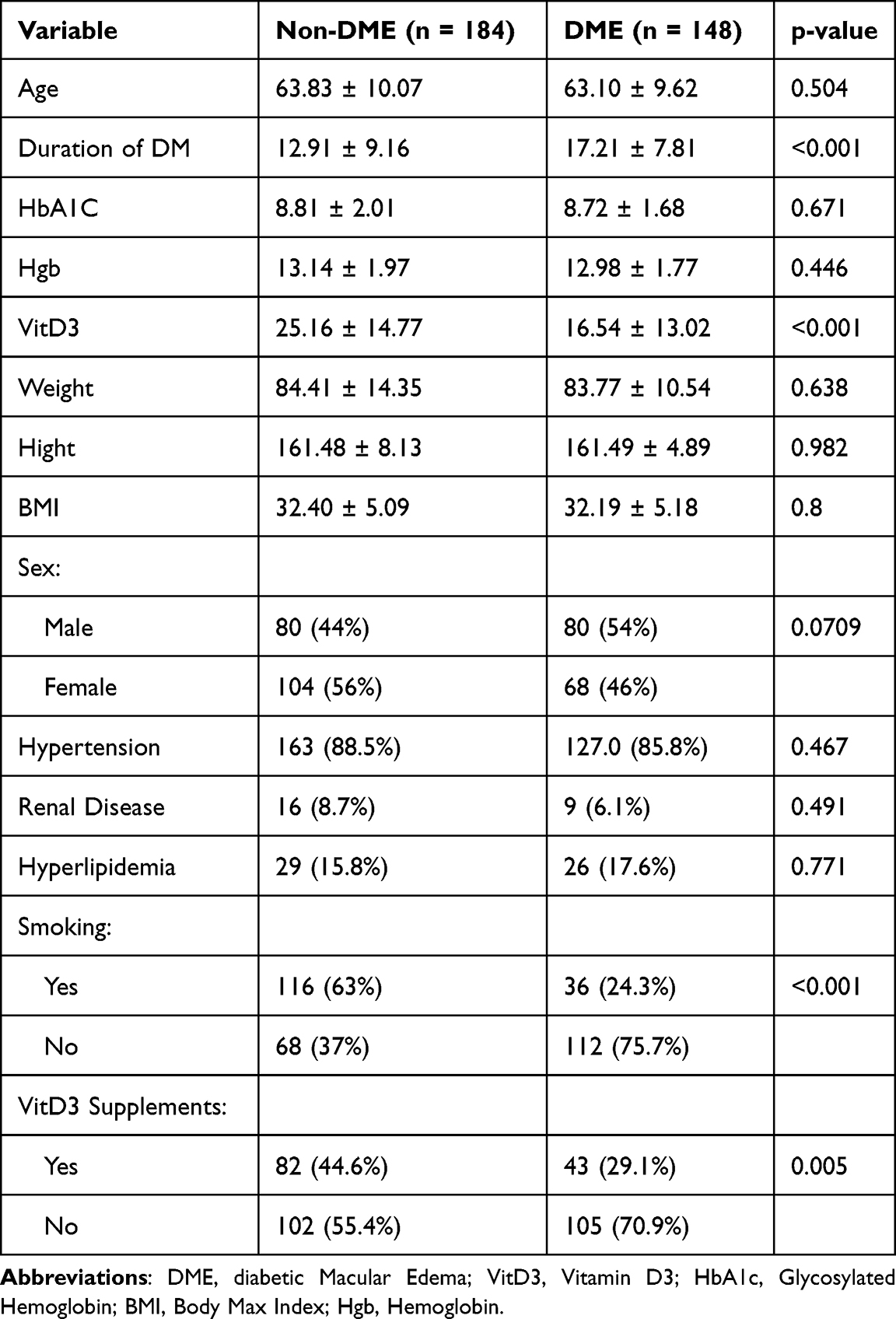 |
Table 1 Baseline Characteristics Stratified by DME Status |
Mean serum VitD3 level was significantly lower in DME patients compared to control group (25.16 ng/mL vs 16.71 ng/mL, p < 0.001 for non DME and DME groups respectively). In terms of VitD3 status category, there are more patients in non-DME groups with sufficient VitD3 levels compared to DME group (Figure 1).
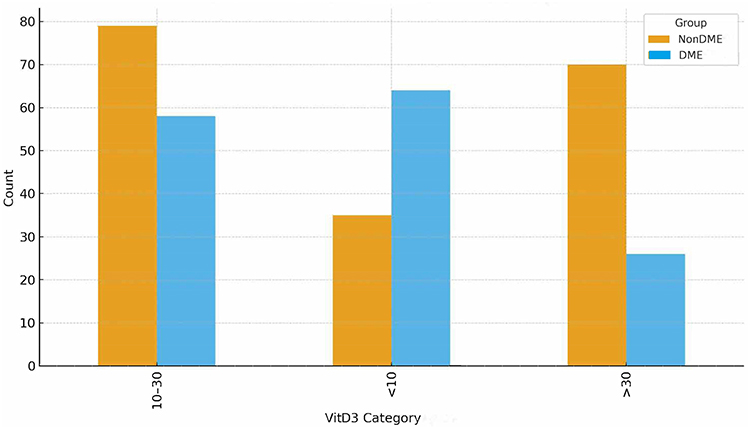 |
Figure 1 Frequency of patients with DME and no DME in different VitD3 serum level categories. |
In Univariate analysis, taking the VitD3 level 10–30 ng/mL as a reference group, VitD3 deficiency (<10 ng/mL) is associated with significant increase in the risk of DME (OR = 2.49; 95% CI = 1.46–4.56, p < 001). On the other hand, sufficient VitD3 level (>30 ng/mL) seems to be protective against DME (OR = 0.51; 95% CI = 0.29–0.89, p < 0.001) (Table 2). As VitD3 serum level increases from severe deficiency (<10) to moderate deficiency (10–30) to sufficiency (>30), the risk of DME decreases in a graded and statistically significant pattern.
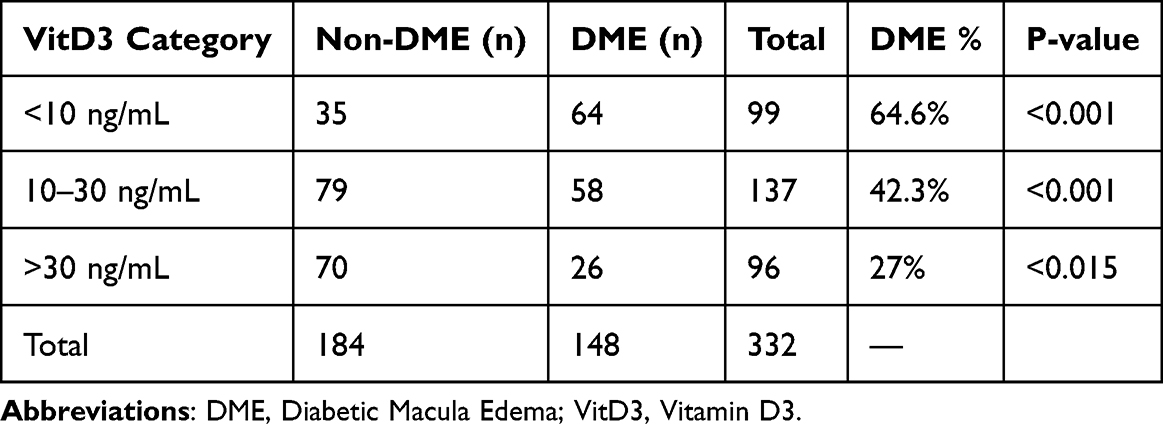 |
Table 2 VitD3 Category Distribution |
On multivariate analysis (Table 3), number of factors were possible predictive of DME including longer duration of DM (OR = 1.061; 95% CI = 1.031–1.091, p < 0.001) and VitD3 deficiency (OR = 2.506; 95% CI = 1.4–4.437, p < 0.001). Conversely, cigarette smoking (OR = 0.428; 95% CI = 0.201–0.912), VitD3 Sufficiency (OR = 0.527; 95% CI = 0.285–0.975, p = 0.04) were inversely associated with DME (Figure 2).
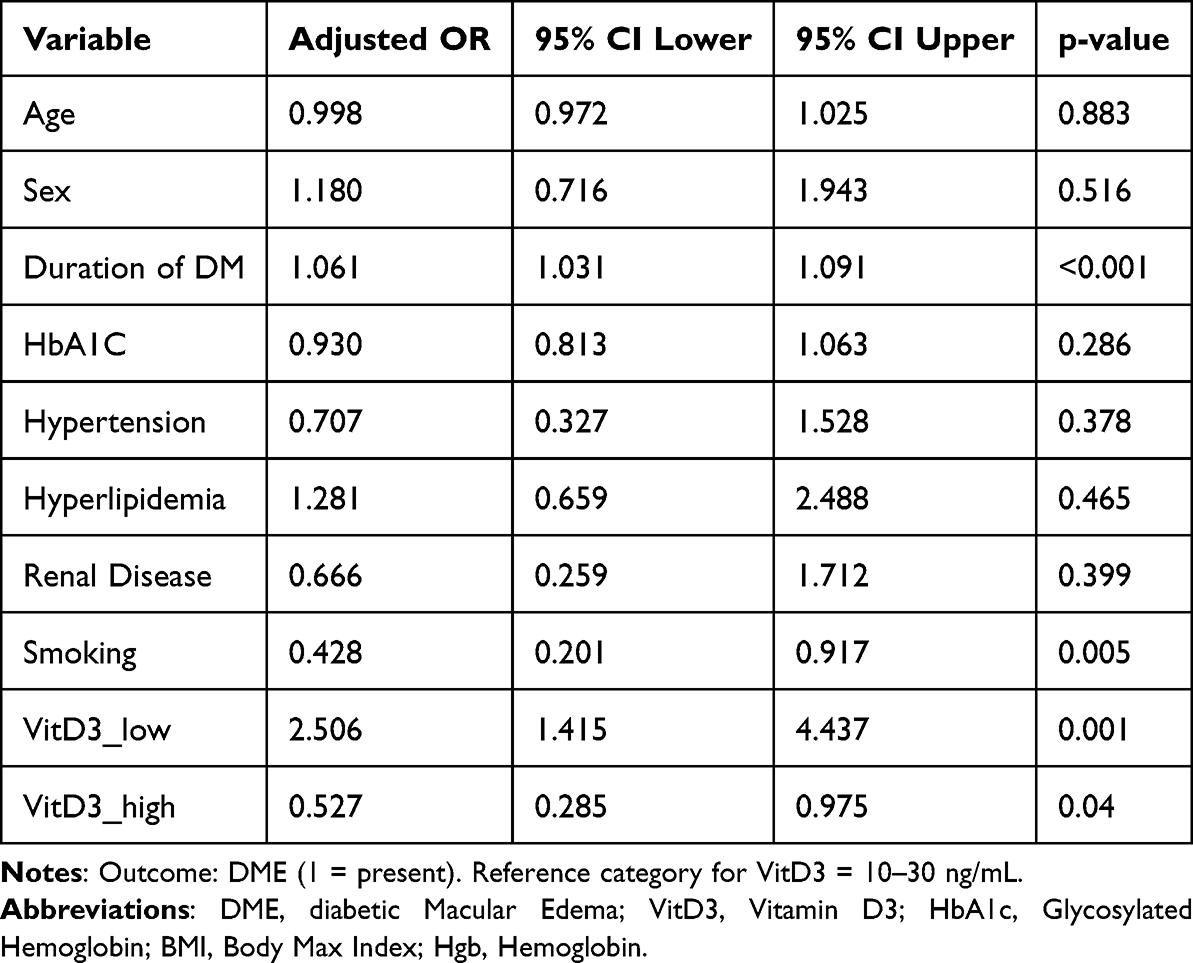 |
Table 3 Multivariate Logistic Regression for Different DME Risk Factors |
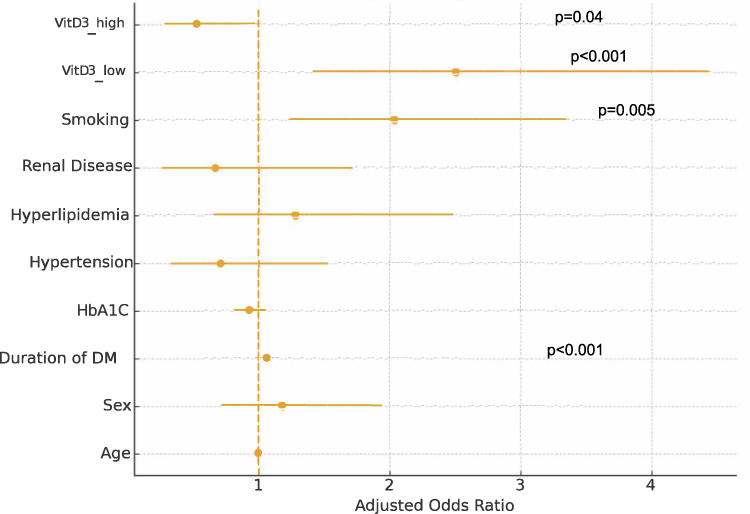 |
Figure 2 Forest plot for different risk factors of DME in multiple regression model. |
Discussion
Our study represents the largest Middle Eastern cohort upon which an exploration of the role of an important dietary constituent, VitD3 (calcitriol), in the development of DME. In short, we found that VitD3 deficiency is strongly associated with DME on both univariate and multivariate models. Other factors associated with DME included duration of DM. On the other hand, appropriate VitD3 levels and cigarette smoking could be protective against the disease.
VitD3 has demonstrated several vital roles across both in-vivo and in-vitro studies. The literature showcases a number of VitD3-related roles such as lowering reactive oxygen species and modulating VEGF expression in retinal cells, preventing glucose-mediated cell damage, and acting as an inhibitor of retinal neovascularization.12–14 Several studies have shown that patients with diabetes are already at a higher risk of VitD3 deficiency compared to their non-diabetic counterparts. In fact, VitD3 deficiency was associated with higher rates of complications among such patients, mainly the development of diabetic retinopathy and its severe variants.15
Nonetheless, the generalized association between VitD3 and diabetic retinopathy is still inconclusive. While some studies support the gradient relationship between levels of VitD3 and worse retinopathy severities,16 others failed to observe such an association nor were able to associate VitD3 deficiency to classical factors of diabetic retinopathy.15 While certain meta-analyses have reached an accord on the negative effect of low serum VitD3 on patients with diabetes, the quality of available evidence is subpar to say the least.17–20
Interestingly, while Lae Kim et al had failed to find a significant difference in serum VitD3 among patients with DME and controls; they were able to demonstrate significant differences in VitD3 in the aqueous humor, particularly higher for patients with DME.21 This finding implies that the localized levels of VitD3 may represent organ ischemia. Moreover, aqueous humor VitD3 was not correlated with serum vitD3 in that same study. These findings support the notion that serum VitD3 may not be a true marker of concurrent ocular deprivation as the eye itself can produce VitD3 while also the blood–brain barrier limits the transmission of VitD3 to the eyes.21 Thus, localized VitD3 levels may not depend on its systemic counterparts.22 Interestingly, Karimi et al found that serum VitD3 levels demonstrate an inverse relationship with HbA1c levels, which implies an indirect effect on VitD3 on the risk factors of diabetic retinopathy or its more severe complications, mainly DME.22
Diabetic retinopathy has two sets of risk factors: modifiable and non-modifiable. Those modifiable include hyperglycemia, metabolic syndrome and its constituents, and hypertension. On the other hand, non-modifiable risk factors include sex, duration of diabetes, ethnicity, puberty, pregnancy among others.23 Many of these factors are shared directly with DME. Within our case-control, in addition to lower serum VitD3 level, we demonstrated that duration of DM is still a major risk factor for DME. This is pathologically sound as longer duration of DM corresponds to an increased amount of hyperglycemia-induced retinal damage.24 This is further support by the observation which shows that tight glycemic control halts the progression of retinopathy and reduces its risk by nearly half.25 However, both factors retained statistical significance on multivariate analysis which may indicate that they might be independent of each other as a predictive factor of DME.
On the other hand, cigarette smoking and higher serum level of VitD3 were possible protective factors against DME. The relationship between smoking and DME is not well understood. Several analyses of the Wisconsin Epidemiologic Study of Diabetic Retinopathy failed to provide consistent conclusions regarding the impact of smoking with regard to progression of diabetic retinopathy.26 Thomson et al reported a protective role of smoking against DME in a large cohort.27 Possible mechanisms by which smoking may decrease the risk for DME may involve inhibition of the secretion of VEGF and subsequent endothelial cell migration as shown by several studies.28 Although cigarette smoking was statistically associated with lower odds of DME, this counterintuitive finding should be interpreted with extreme caution and does not imply a protective clinical effect. Residual confounding and selection bias are likely contributors.
This paper contains several limitations which include: Retrospective design, moderate sample size, an outpatient hospital-based sample, probability for selection bias, loose inclusion criteria, missing data for medications and other clinical variables, control and target groups may not be fully matched in terms of all clinical characteristics, measurement errors may have been introduced when measuring VitD3 or other laboratory measures, and finally, lack of account for dietary habits and other forms of VitD3 production. However, it highlights important relationship between VitD3 levels and risk of DME, which may warrant further evaluation by more robust and community scale studies.
Conclusion
VitD3 deficiency is associated with increased odds of diabetic macular edema. While the findings are clinically relevant, they must be interpreted cautiously due to methodological limitations. Further research is warranted to clarify causality and determine whether VitD3 supplementation may influence DME development or treatment outcomes. The observed association between smoking and reduced odds of DME should not be interpreted as protective and warrant cautious interpretation.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data is not publicly available because it contains information that could compromise the privacy of research participants.
Author Contributions
Motasem Al-latayfeh: Main author, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review and editing.
Raed Shatnawi: co-author, Conceptualization, Methodology, Visualization, Writing the original draft, Writing – review and editing.
Mohammad Abu-Ain: co-author, Conceptualization, Methodology, Visualization, Writing the original draft, Writing – review and editing.
Talal Muteb Alotaibi: co-author, Conceptualization, Data curation, Investigation, Methodology, Validation, Visualization, Writing the original draft.
Ebraheem Albazee: co-author, Conceptualization, Data curation, Investigation, Methodology, Validation, Visualization, Writing the original draft.
Mohammed Ahmed Al-balawi: co-author, Conceptualization, Data curation, Investigation, Methodology, Validation, Visualization, Writing the original draft.
Mohammad Hamad Alnifise: co-author, Conceptualization, Data curation, Investigation, Methodology, Validation, Visualization, Writing the original draft.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors report no conflicts of interest in this study.
References
1. Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82(11):844–8.
2. Steinmetz JD, Bourne RRA, Briant PS. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the global burden of disease study. Lancet Glob Health. 2021;9(2):e144–60. doi:10.1016/S2214-109X(20)30489-7
3. Shah J, Cheong ZY, Tan B, Wong D, Liu X, Chua J. Dietary intake and diabetic retinopathy: a systematic review of the literature. Nutrients. 2022;14(23):5021. doi:10.3390/nu14235021
4. Yau JWY, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diab Care. 2012;35(3):556–564. doi:10.2337/dc11-1909
5. Tan GS, Cheung N, Simó R, Cheung GCM, Wong TY. Diabetic macular oedema. Lancet Diab Endocrinol. 2017;5(2):143–155. doi:10.1016/S2213-8587(16)30052-3
6. Fekri S, Soheilian M, Roozdar S, Abtahi SH, Nouri H. The effect of vitamin D supplementation on the outcome of treatment with bevacizumab in diabetic macular edema: a randomized clinical trial. Int Ophthalmol. 2022;42(11):3345–3356. doi:10.1007/s10792-022-02333-2
7. Graue-Hernandez EO R-D-L-P-D, Hernandez-Jimenez S, Aguilar-Salinas CA, Kershenobich-Stalnikowitz D, Jimenez-Corona A, Jimenez-Corona A. Prevalence and associated risk factors of diabetic retinopathy and macular oedema in patients recently diagnosed with type 2 diabetes. BMJ Open Ophthalmol. 2020;5(1)e000304. doi:10.1136/bmjophth-2019-000304
8. Evert AB, Dennison M, Gardner CD, et al. Nutrition therapy for adults with diabetes or prediabetes: a consensus report. Diab Care. 2019;42(5):731–754. doi:10.2337/dci19-0014
9. Khater AA, Elmohamady MN, Badr TI, et al. Relation between vitamin D deficiency and diabetic maculopathy. Sci Rep. 2025;15(1):23922. doi:10.1038/s41598-025-08941-z
10. D’Angelo A, Lixi F, Vitiello L, Gagliardi V, Pellegrino A, Gianaccare G. The role of diet and oral supplementation for the management of diabetic retinopathy and diabetic macular edema: a narrative review. BioMed Res Int. 2025;2025:Article6654976. doi:10.1155/bmri/6654976
11. El-Khateeb M, Khader Y, Batieha A, et al. Vitamin D deficiency and associated factors in Jordan. Sage Open Med. 2019:7. doi:10.1177/2050312119876151.
12. Lu L, Lu Q, Chen W, Li J, Li C, Zheng Z. Vitamin D3 protects against diabetic retinopathy by inhibiting high-glucose-induced activation of the ROS/TXNIP/NLRP3 inflammasome pathway. J Diab Res. 2018;2018:8193523. doi:10.1155/2018/8193523
13. Lazzara F, Longo AM, Giurdanella G, et al. Vitamin D3 preserves blood retinal barrier integrity in an in vitro model of diabetic retinopathy. Front Pharmacol. 2022;13:971164. doi:10.3389/fphar.2022.971164
14. Albert DM, Scheef EA, Wang S, et al. Calcitriol is a potent inhibitor of retinal neovascularization. Invest Ophthalmol Vis Sci. 2007;48(5):2327–2334. doi:10.1167/iovs.06-1210
15. Ruamviboonsuk V, Grzybowski A. The roles of vitamins in diabetic retinopathy: a narrative review. J Clin Med. 2022;11(21):6490. doi:10.3390/jcm11216490
16. Ashinne B, Rajalakshmi R, Anjana RM, et al. Association of serum vitamin D levels and diabetic retinopathy in Asian Indians with type 2 diabetes. Diab Res Clin Pract. 2018;139:308–313. doi:10.1016/j.diabres.2018.02.040
17. Yuan J, Zhou JB, Zhao W, et al. Could Vitamin D be associated with proliferative diabetic retinopathy? Evidence from pooling studies. Horm Metab Res. 2019;51(11):729–734. doi:10.1055/a-1010-6449
18. Zhang J, Upala S, Sanguankeo A. Relationship between vitamin D deficiency and diabetic retinopathy: a meta-analysis. Can J Ophthalmol. 2017;52 Suppl 1:S39–44. doi:10.1016/j.jcjo.2017.09.026
19. Luo BA, Gao F, Qin LL. The association between Vitamin D deficiency and diabetic retinopathy in type 2 diabetes: a meta-analysis of observational studies. Nutrients. 2017;9:307. doi:10.3390/nu9030307
20. Xiong R, Yuan Y, Zhu Z, et al. Micronutrients and diabetic retinopathy: evidence from the national health and nutrition examination survey and a meta-analysis. Am J Ophthalmol. 2022;238:141–156. doi:10.1016/j.ajo.2022.01.005
21. Kim KL, Moon SY, Noh HM, Park SP, Kim YK. Serum and aqueous humor vitamin D levels in patients with diabetic macular edema. Graefe’s Arch Clin Exp Ophthalmol. 2019;257(6):1191–1198. doi:10.1007/s00417-019-04305-2
22. Karimi S, Movafaghi V, Arabi A, Shahraki T, Safi S. Effects of oral Vitamin D supplement therapy on clinical outcomes of intravitreal bevacizumab in diabetic macular edema. J f Ophthalm Vision Res. 2021;16(1):34–41. doi:10.18502/jovr.v16i1.8249
23. Ting DSW, Cheung GCM, Wong TY. Diabetic retinopathy: global prevalence, major risk factors, screening practices and public health challenges: a review. Clin Exp Ophthalmol. 2016;44(4):260–277. doi:10.1111/ceo.12696
24. Klein R, Klein BE, Moss SE, Davis MD, DeMets DL. The Wisconsin epidemiologic study of diabetic retinopathy. III. Prevalence and risk of diabetic retinopathy when age at diagnosis is 30 or more years. Arch Ophthalmol. 1984;102(4):527–532. doi:10.1001/archopht.1984.01040030405011
25. Shurter A, Genter P, Ouyang D, Ipp E. Euglycemic progression: worsening of diabetic retinopathy in poorly controlled type 2 diabetes in minorities. Diab Res Clin Pract. 2013;100(3):362–367. doi:10.1016/j.diabres.2013.03.018
26. Varma R, Bressler NM, Doan QV, et al. Prevalence of and risk factors for diabetic macular edema in the United States. JAMA Ophthalmol. 2014;132(11):1334–1340. doi:10.1001/jamaophthalmol.2014.2854
27. Thomson KB, Khalid SI, Sabherwal N, Heiferman MJ. Association between tobacco smoking and the development of diabetic macular edema. J Vitreoretin Dis. 2024;8(6):651–657. PMID: 39554620; PMCID: PMC11562456. doi:10.1177/24741264241269479
28. Michaud SÉ, Dussault S, Groleau J, Haddad P, Rivard A. Cigarette smoke exposure impairs VEGF-induced endothelial cell migration: role of NO and reactive oxygen species. J Mol Cell Cardiol. 2006;41(2):275–284. doi:10.1016/j.yjmcc.2006.05.004
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relationship Between Risk Factors and Macular Thickness in Patients with Early Diabetic Retinopathy
Wei Q, Qiu W, Liu Q, Jiang Y
International Journal of General Medicine 2022, 15:6021-6029
Published Date: 5 July 2022
The Economic Burden of Diabetic Retinopathy in Jordan: Cost Analysis and Associated Factors
Al-Dwairi RA, Aleshawi A, Abu-zreig L, Al-Shorman W, Al Beiruti S, Alshami AO, Allouh MZ
ClinicoEconomics and Outcomes Research 2024, 16:161-171
Published Date: 15 March 2024
Brolucizumab versus Aflibercept in Patients with Diabetic Macular Edema: A Meta-Analysis of Randomized Controlled Trials
Justino LB, Justino GB, Graffunder FP, Binotti WW, Khodor A, Caranfa JT
Clinical Ophthalmology 2024, 18:3679-3690
Published Date: 10 December 2024
Outcomes of Anti-VEGF Therapy in Eyes with Diabetic Macular Edema, Vein Occlusion-Related Macular Edema, and Neovascular Age-Related Macular Degeneration: A Systematic Review
Aldokhail LS, Alhadlaq AM, Alaradi LM, Alaradi LM, AlShaikh FY
Clinical Ophthalmology 2024, 18:3837-3851
Published Date: 17 December 2024
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025