Back to Journals » Clinical Interventions in Aging » Volume 21
Association Between Pulmonary Function, Respiratory Muscle Strength and Cognitive Function in Chinese Community-Dwelling Older Adults
Authors He Z, Cheng G, Li S, Zhao F, Fei H, Zeng Y, Yi S
Received 22 August 2025
Accepted for publication 11 December 2025
Published 8 January 2026 Volume 2026:21 559130
DOI https://doi.org/10.2147/CIA.S559130
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Zhichao He,1,* Guirong Cheng,1,2,* Shiyue Li,3,* Feibo Zhao,1 Haishi Fei,1 Yan Zeng,1,2 Shengzhong Yi4
1Brain Science and Advanced Technology Institute, School of Medicine, Wuhan University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 2Geriatric Hospital Affiliated to Wuhan University of Science and Technology, Wuhan University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 3Department of Orthopedics, The Second Affiliated Hospital of Air Force Medical University, Xian, Shaanxi, People’s Republic of China; 4Hubei, Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shengzhong Yi, Hubei, Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Zhuodaoquan South Road, Hongshan District, Wuhan, 430079, People’s Republic of China, Email [email protected] Yan Zeng, Brain Science and Advanced Technology Institute, School of Medicine, Wuhan University of Science and Technology, West Huangjiahu Road, Hongshan District, Wuhan, 430065, People’s Republic of China, Email [email protected]
Purpose: Decline in pulmonary function (PF) and respiratory muscle strength (RMS) is influenced by environmental and genetic factors and is inconsistently linked to cognitive outcomes. This study explores the associations between PF, RMS, and cognitive function among community-dwelling older adults in China, analyzing interactions with APOE Ɛ4 and the mediating effect of serum total bilirubin.
Patients and Methods: About 1,081 Hubei Memory and Aging Cohort (HMACS) participants underwent PF (PEF, FEV1 and FVC), RMS (MIP and MEP) assessment, cognitive tests, APOE genotyping, and bilirubin measurement. Multivariate logistic regression and general linear regression were used to analyze associations.
Results: Among 1,081 participants (mean age 70.52 ± 5.55 years), 26.1% had cognitive impairment. Lower PF and RMS scores were associated with cognitive impairment. Higher comprehensive PF (c-PF) and RMS indices protected against cognitive impairment (eg, c-PF: OR = 0.482– 0.609, P < 0.05; MEP: OR = 0.464, P = 0.005). PF and RMS indices correlated positively with global cognition, memory, language, and executive function. Sex differences were noted, with males (n = 449, 41.5%) showing associations between MIP/MEP and global cognition, memory, and language, while females (n = 632, 58.5%) showed broader associations. APOE Ɛ4 status (n = 330) did not affect these associations. Serum total bilirubin levels (n = 977) correlated with pulmonary and cognitive function but did not mediate the associations.
Conclusion: PF (especially PEF) and RMS (especially MEP) indices are significantly associated with cognitive function and impairment in older adults, independent of APOE Ɛ4 status. These findings provide biomarkers for assessing cognitive health risk and a basis for interventions targeting PF and RMS to preserve cognitive function.
Keywords: pulmonary function, respiratory muscle strength, cognitive impairment, cross-sectional study, older adults
Introduction
Pulmonary function (PF) and respiratory muscle strength (RMS)—key respiratory indicators—decline with aging or disease, showing asynchronous reductions in forced vital capacity (FVC), forced expiratory volume in one second (FEV1) and peak expiratory flow (PEF), and are co-regulated by environmental and genetic factors.1,2
Existing studies link PF to cognition, with shared risks including aging, hypertension, cardiovascular disease, frailty, and smoking.3–5 European cohorts confirm poor baseline PF raises dementia and cognitive impairment risks,6–8 but conclusions remain controversial, potentially due to genetic (eg, APOE Ɛ4) and environmental interactions.9,10 Chinese community studies are limited: while PF correlates with global cognition,3,11 most focus on single indicators (eg, PEF, FEV1), lacking systematic analysis of PF/RMS with cognitive impairment or domain-specific decline. Thus, multi-indicator PF/RMS decline associations with cognitive outcomes in older adults need clarification.
The PF-cognition link may involve systemic inflammation, cerebral hypoperfusion from chronic hypoxia, microvascular damage, and brain atrophy.5,6 Total bilirubin, an endogenous antioxidant, may mediate this via free radical scavenging (protecting pulmonary tissue)12,13 and inhibiting oxidative stress/inflammation (alleviating neuronal damage);14,15 Reduced total bilirubin is linked to cognitive decline and stroke risk,16,17 supporting potential mediation.
Current cognitive impairment biomarkers have limitations: invasive cerebrospinal fluid markers,18–20 variable-sensitivity blood markers, costly/complex neuroimaging, and non-standardized extracellular vesicles.21 In contrast, PF/RMS indices are non-invasive, convenient, and reflect systemic health, addressing gaps in large-scale screening, long-term monitoring, and primary care—offering new insights for early cognitive impairment warning.
This study explores associations between PF (PEF, FEV1 and FVC), RMS (MIP and MEP), and cognitive impairment/function in Chinese community-dwelling older adults, analyzing APOE Ɛ4 interactions and total bilirubin mediation.
Methods
Study Design and Participants
Data were from the Hubei Memory and Aging Cohort Study (HMACS; ChiCTR1800019164), established in 2018 to investigate cognitive impairment prevalence, risk/protective factors in community-dwelling older adults (design/assessment details reported previously).22 For cohort establishment, urban participants were recruited by randomly selecting 4 districts in the Wuhan metropolitan area of Hubei Province and then 31 neighborhoods within these districts, while rural participants were from 4 randomly selected townships in Dawu County (a remote mountain area) and 48 villages under these townships, and all eligible participants were identified from the electronic health records (EHRs) of local hospitals and health centers and met the following a priori inclusion criteria: 1) registered residents in the sampled neighborhoods/villages with valid EHRs; 2) aged ≥65 years; 3) no prior diagnosis of dementia; 4) no medical records of schizophrenia, major depressive disorder, or life-threatening diseases; 5) able to complete physical and cognitive examinations. Residents living in nursing homes or psychiatric hospitals were excluded. PF testing was added in May 2023.
Of 1,820 initial participants, 739 were excluded based on strict, a priori defined eligibility criteria to ensure data quality and analytical validity (Figure S1 for detailed exclusion workflow). The primary exclusion criteria were: (1) age < 65 years (n = 97; consistent with gerontological definitions of “older adults,” our study focused on participants ≥65 years); (2) non-cooperation with PF assessment (n = 198); (3) severe hearing/visual impairment (n = 122, which would compromise the validity of cognitive and PF measurements); and (4) other reasons (n = 32). Among the remaining 1,371 participants who completed the baseline interview, 290 were further excluded due to incomplete neuropsychological data (n = 116), repeated/unreliable PF data (n = 141), or poor coordination during PF testing (n = 33). Ultimately, 1,081 participants were included in the final analysis.
To evaluate potential selection bias, we compared baseline characteristics—including age, sex, educational attainment, physical activity levels, and chronic conditions—between included (n = 1,081) and excluded (n = 739) participants. No statistically significant differences were observed across all variables (all p > 0.05), with detailed comparisons provided in Table S1.
This study was conducted in compliance with the Declaration of Helsinki. All procedures involving human participants were approved by the Medical Ethics Committee of Wuhan University of Science and Technology (Approval No.201845), and written informed consent was obtained from each participant prior to enrollment.
Measurements
Assessment of PF
PF was measured by trained physicians using a calibrated portable spirometer (X2210205000420 X2, SecG Medical Equipment Co., Ltd.) with three flow and volume settings. All assessments strictly adhered to the 2005 ATS/ERS international standards for spirometry. Participants sat with pinched noses, using a disposable mouthpiece: after 2 calm breaths, they inhaled deeply and exhaled continuously at maximum speed/force for ≥6 seconds. The test was repeated at least twice (a third if differences exceeded 5%).
PF predicted values were calculated via Global Lung Initiative 2012 equations,23 accounting for sex, age, height, weight, and ethnicity; values <80% of predicted were abnormal. The comprehensive PF (c-PF) index was the mean of z-scores for PEF, FEV1, and FVC and higher values indicate better function.
Assessment of RMS
MIP and MEP were measured via a calibrated portable RMS meter (MicroRPM, CareFusion, USA; flow sensor, accuracy ± 3%). Assessments followed the 2019 ATS/ERS guidelines for respiratory muscle testing: Participants sat with a disposable mouthpiece and nose clip. MIP was the maximum value from maximal inhalation (≥2 seconds) after calm exhalation to functional residual capacity; MEP was the maximum from maximal exhalation (≥2 seconds) after deep inhalation to total lung capacity. Each was measured at least 3 times (1-minute intervals), with the maximum valid value used. Valid measurements required a pressure plateau ≥1 second and ≤10% difference between the two highest values. Inter-rater reliability was evaluated via duplicate assessments of 50 randomly selected participants by two trained physicians, yielding an intraclass correlation coefficient (ICC) of 0.92, confirming high reliability.
Results were reported as absolute values (cmH2O) and % predicted (GLI-2012 Southeast Asia equations).24 MIP < 60 cmH2O (or <80% predicted) indicated inspiratory dysfunction; MEP < 100 cmH2O (or <70% predicted) indicated expiratory dysfunction. The comprehensive RMS (c-RMS) index was the mean of MIP and MEP z-scores; higher values reflect better function.
Assessment of Neuropsychological and Diagnosis of Cognitive Impairment
Neurologists and trained medical postgraduates conducted standardized face-to-face assessments, including four subdomains and global cognitive function: memory (Auditory Verbal Learning Test), language (30-item Boston Naming Test, Animal Fluency Test), executive function (Trail Making Test A/B), and attention (Digit Span Test), global cognitive function was calculated as the mean of the four subdomains z-scores.
Cognitive impairment (MCI and dementia) was diagnosed per Chinese expert consensus.25 MCI followed Petersen criteria;26 dementia adhered to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria, confirmed via three steps: initial diagnosis by cognitive experts, review by data-collecting physicians, and final adjudication by senior neurologists.27
Test for APOE Ɛ Genotyping
APOE Ɛ genotyping was performed using the MassARRAY iPLEX Gold system (Agena Bioscience, Inc). After clinical sample collection, DNA was extracted per standard protocols. Following PCR amplification, shrimp alkaline phosphatase (SAP) treatment removed excess deoxynucleoside triphosphates. Extension primers and iPLEX mixture were added to complete extension. After desalination, products were loaded onto chip plates for mass spectrometric analysis.
Biochemical and Hematological Biomarkers
Measured biomarkers included: inflammatory-related (leukocyte count; neutrophil, monocyte, lymphocyte, basophil, eosinophil percentages and absolute counts; high-sensitivity C-reactive protein; platelet count, volume distribution width, plateletcrit); erythrocyte-related (hematocrit, red blood cell count, mean corpuscular volume, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration); liver function-related (alanine aminotransferase, aspartate aminotransferase, AST/ALT ratio, total bilirubin, globulin, albumin, total protein, albumin/globulin ratio); renal function-related (urea, uric acid, creatinine, pH, urine specific gravity); and metabolites (homocysteine, vitamin B12, folic acid, total cholesterol, fasting blood glucose, low/high-density lipoprotein cholesterol, triglycerides).
Confounders
Confounders included demographic factors (sex, age, education, dwelling status, spouse, monthly income); lifestyle factors (smoking, drinking, physical activities, intellectual activities, BMI); and comorbidities (history of hypertension, diabetes, hyperlipidemia, coronary heart disease, cerebrovascular disease).
Statistical Analysis
Multiple Imputation by Chained Equations (MICE) addressed covariates with <10% missingness via 100 imputations (5 iterations); further details are provided in Table S2. Imputation diagnostics confirmed model convergence (stable trace plots for all variables) and no significant differences between imputed and observed data distributions. Normally distributed continuous data are presented as  ; categorical data as n (%). Group differences were compared via chi-square and t-tests. Multivariate logistic regression and trend tests analyzed c-PF-cognitive impairment associations across four models: model 1 (c-PF only); model 2 (plus sociodemographics); model 3 (plus lifestyle); model 4 (plus comorbidities). Restricted cubic splines (knots at 10th, 50th, 90th percentiles of c-PF) visualized relationships. General linear regression analyzed associations of PF indices (PEF, FEV1 and FVC) and RMS indices (MIP and MEP) with global cognition and cognitive subdomains (standardized scores), with sex-stratified analyses for RMS indices.
; categorical data as n (%). Group differences were compared via chi-square and t-tests. Multivariate logistic regression and trend tests analyzed c-PF-cognitive impairment associations across four models: model 1 (c-PF only); model 2 (plus sociodemographics); model 3 (plus lifestyle); model 4 (plus comorbidities). Restricted cubic splines (knots at 10th, 50th, 90th percentiles of c-PF) visualized relationships. General linear regression analyzed associations of PF indices (PEF, FEV1 and FVC) and RMS indices (MIP and MEP) with global cognition and cognitive subdomains (standardized scores), with sex-stratified analyses for RMS indices.
Participants were grouped by PF (normal/abnormal) and APOE Ɛ4 status (negative/positive); ANOVA compared global cognition between groups, with LSD post-hoc tests. Laboratory blood biomarkers (inflammation-, red blood cell-, liver/renal function-, and metabolite-related) were correlated with c-PF and cognitive function via Pearson’s r to identify potential mediators for mediation analysis.
Sensitivity analyses included subgroup analyses (by sex, age, smoking) with interaction tests, and association exploration after excluding participants with PF test quality < Grade D, extremely severe mixed ventilatory dysfunction, or dementia.
Analyses used IBM SPSS 26.0 and R 4.1.3. A two-tailed P < 0.05 was statistically significant.
Results
Study Flow and Clinical Characteristics
A total of 1,081 eligible HMACS participants were included (mean age 70.52 ± 5.55, mean education 12.04 ± 3.29 years), with 449 (41.5%) males. Among them, 799 (73.9%) had normal cognition and 282 (26.1%) had cognitive impairment. The latter showed lower global cognition and PF scores, with a higher proportion in Q1 for c-PF, MIP, and MEP (Table 1). APOE genotyping was completed in 330 participants, of whom 78 (23.6%) were ε4 carriers and 252 (76.4%) were non-carriers.
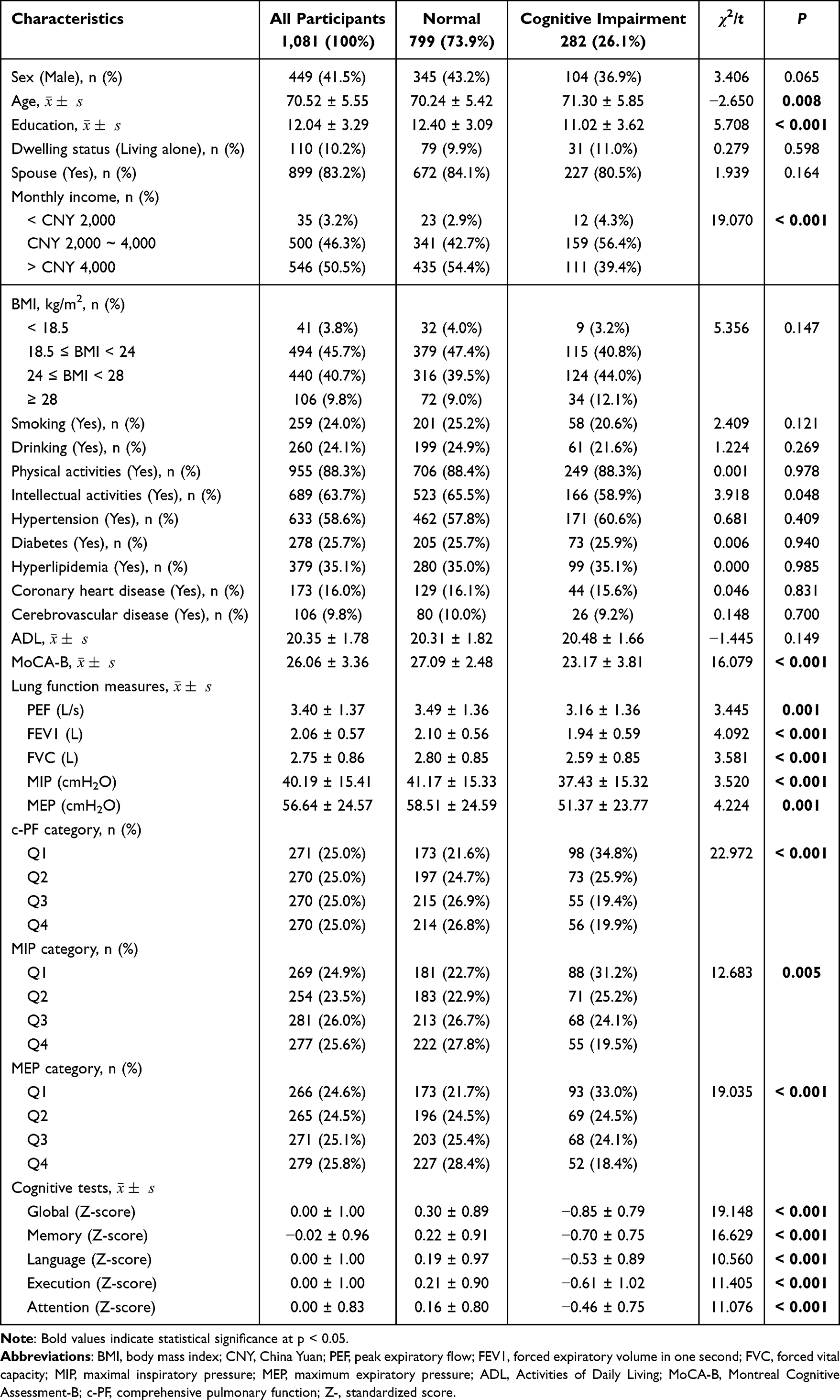 |
Table 1 Characteristics of Study Participants by Cognitive Status |
Correlation Between PF and RMS Indices
PF indices (PEF, FEV1 and FVC) and RMS indices (MIP and MEP) correlated positively (r = 0.442–0.932, all P < 0.01), with strongest correlations between PEF-MEP (r = 0.932) and FEV1-FVC (r = 0.805) (Table S3).
In regression Model 1 (cognitive function) including PEF, FEV1, FVC, MIP and MEP, strong multicollinearity (eg, VIF = 8.057 for PEF, 7.986 for MEP) masked associations for PEF and FEV1 (Table S4). After constructing c-PF (combining PEF, FEV1 and FVC) for Model 2, c-PF, MIP and MEP (all VIF < 2.8) showed significant associations with cognitive function.
Correlation Between c-PF and Cognitive Impairment
In the fully adjusted multiple logistic regression model (Figure 1), higher c-PF scores were significantly associated with a reduced risk of cognitive impairment. Across c-PF quartiles, this risk reduction was statistically significant for Q2 (OR = 0.609, P = 0.025), Q3 (OR = 0.482, P = 0.003) and Q4 (OR = 0.525, P = 0.017) relative to Q1, with a clear downward trend (P for trend = 0.016). For RMS indices, MIP showed significant risk reductions in Q3 (OR = 0.612, P = 0.027) and Q4 (OR = 0.485, P = 0.004) (vs Q1), while MEP only reached significance in Q4 (OR = 0.464, P = 0.002) (vs Q1); both indices exhibited significant downward trends in cognitive impairment risk with increasing quartiles (P for trend = 0.001 and 0.003, respectively).
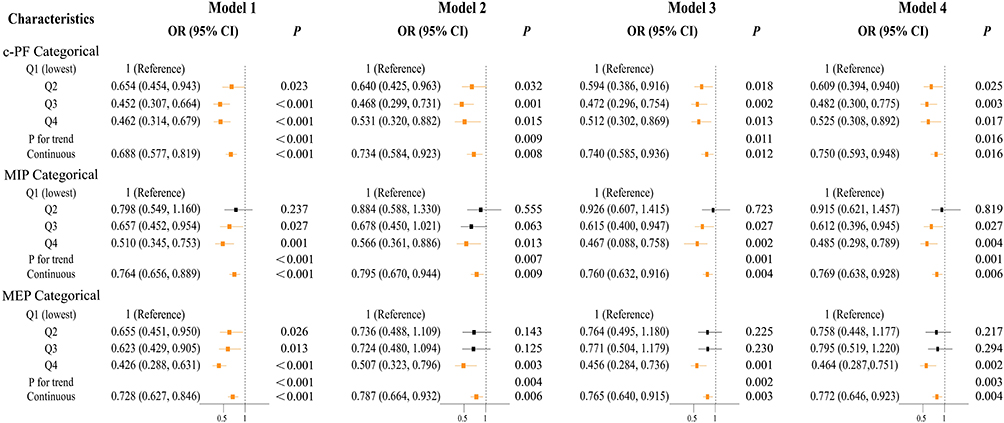 |
Figure 1 Association of c-PF, RMS indices (MIP and MEP) and cognitive impairment by logistic regression. Abbreviations: CI, confidence interval; OR, odd ratio; c-PF, comprehensive pulmonary function; c-RMS, comprehensive respiratory muscle strength; Q, quartile; MIP, maximal inspiratory pressure; MEP, maximum expiratory pressure. Notes: Model 1: Crude Model. Model 2: Adjusted for baseline age, sex, education, monthly income, spouse and dwelling status. Model 3: Further adjust for lifestyle variables such as smoking, drinking, BMI, physical activities and intellectual activities. Model 4: Further adjust for comorbidities such as hypertension, diabetes, hyperlipidemia, coronary heart disease and cerebrovascular diseases. All continuous variables (c-PF, MIP and MEP) were included in the analysis after being standardized by z-score. |
Treated as continuous, each 1-unit increase in c-PF was linked to 25.0% lower risk (OR = 0.750, P = 0.016), with a non-linear association (P non-linear = 0.017; Figure 2A).
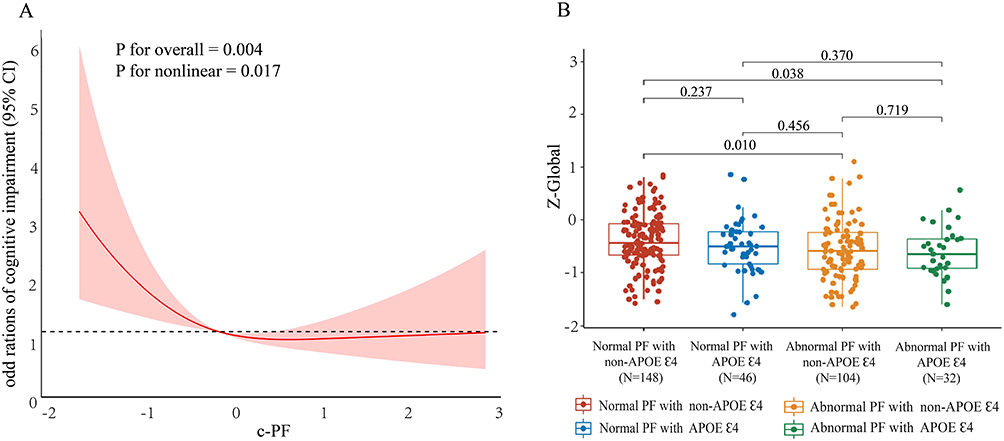 |
Figure 2 Comprehensive PF and cognition. Abbreviations: PF, pulmonary function; c-PF, comprehensive pulmonary function; Z-, standardized score. Notes: (A) The nonlinear relationship between c-PF and the risk of cognitive dysfunction. (B) PF combined with APOE status is associated with overall cognitive function. All models are covariant baseline age, sex, education, income, spouse, dwelling status, smoking, drinking, BMI, physical activities, intellectual activities, hypertension, diabetes, hyperlipidemia, coronary heart disease and cerebrovascular diseases. |
Subgroup analyses (stratified by sex, age, and smoking status) showed better c-PF was linked to lower cognitive impairment risk in females (OR = 0.671, P = 0.027), individuals 70–80 years (OR = 0.560, P = 0.004), and smokers (OR = 0.599, P = 0.039). A significant c-PF × age interaction emerged (P for interaction = 0.020, Figure S2), with the protective effect of c-PF on cognitive impairment being more pronounced in those 70–80 years, this interaction is visualized in a plot (Figure S3).
Correlation Between PF Indices, RMS Indices and Cognitive Function
Correlation Between PF Indices and Cognitive Function
Multivariate fully adjusted models demonstrated consistent positive associations between PF indices (PEF, FEV1, FVC) and cognitive function (Table S5 and Figure 3). All three PF indices correlated positively with global cognition, language function, and executive function. Among these, PEF showed the broadest associations—it additionally correlated with memory and attention—while FEV1 also linked to memory, and FVC’s associations were limited to global cognition, language function, and executive function.
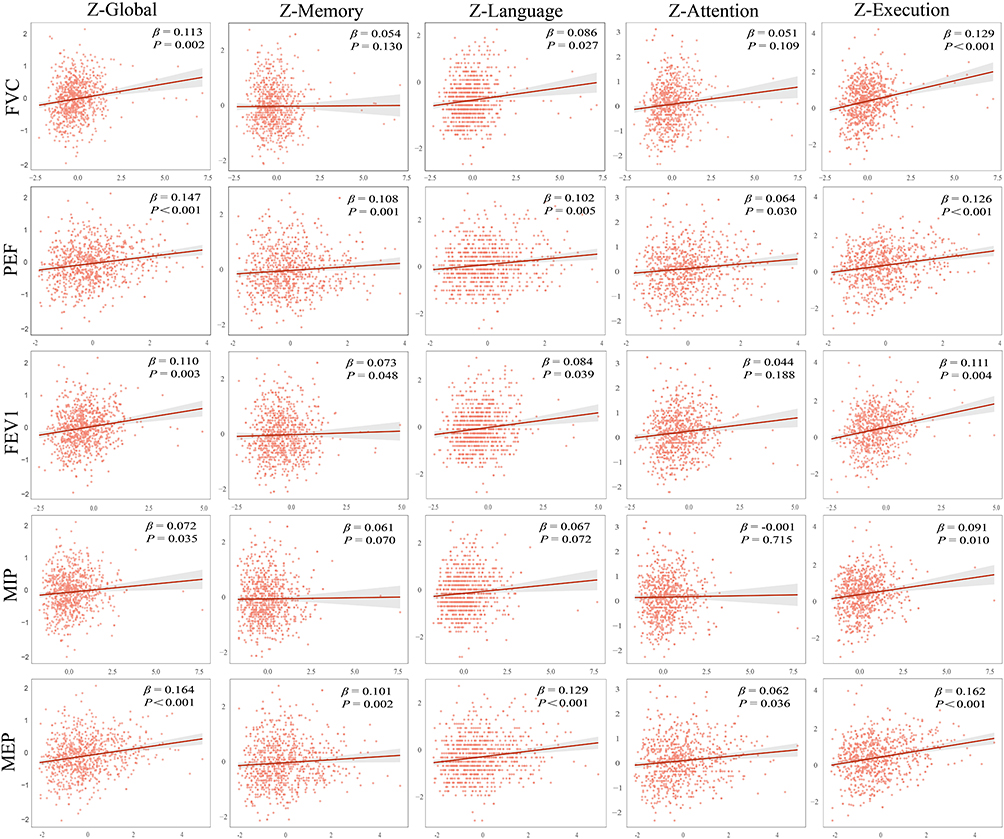 |
Figure 3 Linear association between PF indices, RMS indices and various cognitive domains. Abbreviations: FEV1, forced expiratory volume in one second; FVC, forced vital capacity; PEF, peak expiratory flow; MIP, maximal inspiratory pressure; MEP, maximum expiratory pressure; Z-, standardized score. Notes: All continuous variables (PEF, FEV1, FVC, MIP and MEP) were included in the analysis after being standardized by Z-score. The coordinate axes have been uniformly scaled for visualization. The true standardized β is marked in the upper right corner. All β are standardized regression coefficients, and the corresponding models have controlled for baseline age, sex, education, monthly income, spouse, dwelling status, smoking, drinking, BMI, physical activities, intellectual activities, hypertension, diabetes, hyperlipidemia, coronary heart disease and cerebrovascular diseases. The straight lines in the figure are the fitting lines at the original scale and are only for visualization. Statistical tests use the standardized model. |
PF (normal/abnormal) combined with APOE ε4 status (positive/negative) (n = 330) was analyzed for associations with cognition. Results showed significant differences in global cognitive scores across the four groups (one-way ANOVA: F = 0.294, P = 0.032). LSD post-hoc tests revealed that regardless of APOE ε4 status, abnormal PF was associated with lower cognitive scores than normal PF (Figure 2B and Table S6).
Correlation Between RMS and Cognitive Function
For RMS indices, MIP and MEP exhibited differential positive associations with cognitive domains, with results visualized in Figure 3 and detailed in Table S7. MIP correlated only with global cognition and executive function, whereas MEP showed more extensive positive links, spanning global cognition, memory, language, attention, and executive function.
When stratified by sex (Tables S8, S9): In males, both MIP and MEP correlated positively with global cognition, memory, and language, with MEP further linked to executive function; in females, MIP associated only with executive function, whereas MEP maintained the same broad positive associations—with global cognition, memory, language, attention, and executive function—observed in the overall population.
Sensitivity analyses (excluding participants with PF test quality < Grade D (n = 36), extremely severe mixed ventilatory dysfunction (n = 81), and dementia (n = 12)) confirmed all PF (PEF, FEV1 and FVC) and RMS (MIP and MEP) indices remained positively correlated with total cognitive function, with stronger associations for PEF and MEP (Tables S10–S12).
Mediation Effect Analysis of Laboratory Indicators
Correlation analyses of blood biomarkers (inflammation-, red blood cell-, liver/renal function-, and metabolism-related) with c-PF and cognitive function showed multiple indicators (eg, monocytes, lymphocyte count, red blood cell count, total bilirubin, mean hemoglobin content/concentration) correlated significantly with c-PF, while only total bilirubin, urea, and urine pH correlated with cognitive function (Table S13).
Total bilirubin—correlating significantly with both—was included in mediation analysis. Stepwise regression showed significance, but unstable confidence intervals for indirect effects yielded no valid results (Table S14 and Table 2).
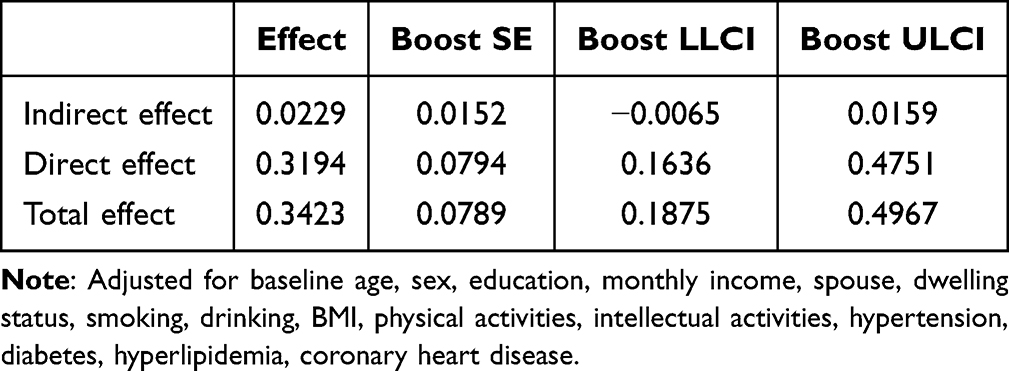 |
Table 2 Summary of Total Bilirubin Mediating Effects |
Discussion
In Chinese community-dwelling older adults, PF (PEF, FEV1 and FVC) and RMS (MIP and MEP) synergistically relate to cognitive function. They negatively correlate with cognitive impairment risk (dose-effect relationship) and positively associate with global cognition—especially executive and language functions—with PEF and MEP showing stronger links. APOE ε4 does not moderate the PF-cognition relationship. Though total bilirubin correlates with both c-PF and cognition, its mediating effect was not validly confirmed.
European cohort studies link declining baseline PF to higher dementia and cognitive impairment risk, likely via chronic hypoxia and inflammation.11,27,28 Our study aligns: higher c-PF quartiles associate with lower cognitive impairment risk (significant trend), validating cross-ethnic shared regulatory mechanisms between PF and cognition in Chinese older adults, supporting PF as a universal cognitive health marker.
We identified a non-linear c-PF-cognition relationship (P non-linear = 0.017), with a “threshold range”: risk reduction was strongest from Q1 to Q3 (51.8% lower in Q3 vs Q1), slowing thereafter. Clinically, c-PF levels in the upper-middle range (eg, Q3) are associated with relatively lower cognitive impairment risk—this observation may provide practical reference for interventions targeting older adults with irreversible PF decline, though no causal relationship between maintaining PF and cognitive protection can be established.
PEF shows the strongest cognition association, consistent with literature, due to high sensitivity to small airway function and early brain structural changes. Unlike FEV1/FVC (marking chronic obstruction), PEF detects small airway dysfunction earlier; hypoxia/inflammation from such lesions drive cognitive impairment. Low PEF links to higher COPD, dementia risk, and brain changes (eg, ventricular enlargement),7,29 while FEV1/FVC lags 2–5 years.29,30 Quantitatively, PEF decline correlates more strongly with dementia risk (RR = 1.84) than FEV1 (1.25) or FVC (1.40).31 Domain-specifically, PEF strongly associates with executive function (β = 0.126) and memory (β = 0.108), reflecting small airway lesion-induced prefrontal/hippocampal damage.30,32 It should be noted that other factors, such as respiratory rhythm abnormalities caused by small airway dysfunction (which may disrupt cerebral blood flow stability), could also contribute to cognitive changes, though current evidence for hypoxia/inflammation mechanisms is more robust.33
PF and RMS indices act synergistically, not independently, on cognitive function, stemming from their close physiological links. As the “power source” of ventilation, RMS indices—especially MEP—correlate strongly with PF indices (eg, PEF, r = 0.932), forming a “respiratory muscle drive-ventilation efficiency” network.
Collinearity analysis supported this: including individual indices alone (Model 1) caused high correlation (eg, VIF > 7 for PEF and MEP), masking some associations. Constructing c-PF reduced collinearity (all VIF < 2.8; Model 2), and MEP’s β dropped from 0.224 (Model 1) to 0.128 (Model 2), indicating joint regulation via physiological synergies rather than independent pathways. This synergy arises because RMS provides ventilation’s motivational basis, while PF reflects efficiency; together, they support cerebral oxygenation and reduce inflammation—aligning with studies linking MEP to PEF,34 MIP to FVC/FEV1,35 and RMS-small airway synergy.36 Alternative explanations, such as shared genetic factors regulating both respiratory and cognitive function, cannot be fully excluded, though physiological synergy remains the most parsimonious interpretation based on current data.37
MEP, a core expiratory muscle strength index, shows the strongest cognitive association. Reduced MEP drives restrictive lung disease via expiratory muscle weakness, impairing alveolar gas evacuation and limiting lung expansion—pathology for restrictive dysfunction.38 Restrictive impairment (dominated by muscle weakness) links more strongly to cognitive decline than obstructive disease: cohort studies found higher dementia/MCI risk in restrictive (OR = 1.58) vs obstructive (OR = 1.33) patients,39 with restrictive injury tied to brain structural changes (eg, reduced frontoparietal gray matter).40 Additionally, RMS metrics better reflect PF in cognitive impairment,41 supporting MEP’s unique role in the “respiratory-brain axis,” strengthening its cognitive association.
Sex-stratified analyses showed that in males, MIP and MEP associated with memory, language, and executive function, while in females, MEP correlated with more cognitive subdomains and MIP’s influence was limited—differences stemming from sex-specific physiology. Specifically, testosterone enhances respiratory muscle metabolic efficiency and innervation via androgen receptors,42 making male MIP/MEP associations with language and executive function more dependent on muscle strength (eg, MIP stabilizes airflow for language fluency;43 MEP supports prefrontal function).44 In contrast, estrogen mediates female respiratory muscle-neurovascular coupling,45 improving vascular function and cerebrovascular reactivity46 to support multiple cognitive domains—explaining MEP’s broad associations—while MIP’s limited female influence may reflect lower inspiratory muscle strength,44 overshadowed by estrogen’s systemic regulation. Additionally, muscle structure/function reinforces this: males have higher absolute MIP/MEP,44 with stronger respiratory muscles directly regulating processes linked to language and executive function (eg, vocal fold stability),43 whereas in females with weaker muscles, MEP’s cognitive associations may rely more on breathing pattern stability.
Our results showed APOE Ɛ4 does not modify the PF-cognition association: regardless of APOE Ɛ4 status, abnormal PF linked to lower cognitive scores, stemming from distinct cognitive influence pathways. APOE Ɛ4 drives Alzheimer’s pathogenesis via β-amyloid deposition (eg, higher brain β-amyloid oligomer burden and synaptic binding in carriers),47 while abnormal PF impacts cognition mainly through vascular mechanisms (eg, hypoxemia, inflammation-induced cerebral hypoperfusion and microvascular damage).3 APOE Ɛ4 weakly modulates vascular factors,48 keeping their pathways independent. Clinically, improvements in PF are associated with slower cognitive decline in APOE Ɛ4-positive individuals (genetic high-risk groups), while maintaining good PF is associated with better cognitive outcomes in APOE Ɛ4-negative individuals—no causal effect of PF on cognitive decline can be inferred.
While our study found total bilirubin correlated with both c-PF and cognitive function, its mediating effect showed unstable confidence intervals, with no valid results. Two key factors may explain this: First, sample size limitation (n = 1081) likely reduced the precision of mediating effect estimates—previous studies have shown that small samples increase the variance of indirect effect calculations, leading to unstable confidence intervals.49 Second, bilirubin may not be a strong mediator in this Chinese community-dwelling older adult population: Bilirubin’s antioxidant role in the “pulmonary-brain axis” often synergizes with other antioxidants (eg, superoxide dismutase, glutathione),50 and measuring only total bilirubin (without fractionated bilirubin or other antioxidant markers) may incompletely capture its biological role. Additionally, in this population, vascular factors (eg, cerebral microangiopathy) may be more dominant mediators between PF and cognition, overriding bilirubin’s potential mediating effect. Though bilirubin counteracts oxidative stress via mechanisms like ROS scavenging and antioxidant enzyme induction, in complex in vivo environments, total bilirubin may incompletely reflect its role in the “lung-brain axis”.
This study has limitations: first and foremost, its cross-sectional design severely limits causal inference—prospective cohort studies are urgently needed to confirm whether a temporal relationship exists; while collinearity was managed via simplified models, potential complex inter-indicator interactions may remain unaccounted for; the sample, from an urban Hubei community cohort, restricts generalizability to other regions; lack of air pollutant data may omit key confounders; and the small sample size of APOE Ɛ4 carriers necessitates further validation of their interaction with PF.
Conclusion
This study confirms that abnormal PF and reduced RMS in Chinese community-dwelling older adults are significantly associated with cognitive impairment risk and cognitive decline. It underscores that better preserved RMS is linked to better performance in language, executive function, and attention, with total bilirubin identified as a potential biological mediator.
Notably, the cross-sectional design of this study precludes any conclusions about causality or directionality between PF/RMS and cognitive function—this limitation must be emphasized, as temporal relationships remain unaddressed. These findings shed new light on the “pulmonary-cognition axis” and suggest that respiratory muscle training to improve PF could be a hypothesis worth testing in future trials for preventing cognitive impairment in older adults. Future prospective cohort studies with long-term follow-up, diverse populations, and mechanistic research are needed to clarify causal relationships and regulatory pathways between PF and cognition.
Abbreviations
PF, pulmonary function; RMS, respiratory muscle strength; APOE Ɛ4, apolipoprotein Ɛ4; PEF, peak expiratory flow; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; MIP, maximal inspiratory pressure; MEP, maximum expiratory pressure; c-PF, comprehensive pulmonary function; c-RMS, comprehensive respiratory muscle strength; HMACS, Hubei Memory and Aging Cohort Study; OR, odd ratio; CI, confidence interval; SD, standard deviation; PET, Positron Emission Tomography; MRI, Magnetic Resonance Imaging; EVs, Extracellular Vesicles; ICC, Intraclass Correlation Coefficient; GLI-2012, Global Lung Initiative 2012; MoCA-B, Basic Montreal Cognitive Assessment; ADL, Activities of Daily Living; MCI, Mild Cognitive Impairment; PCR, Polymerase Chain Reaction; SAP, Alkaline Phosphatase; MICE, Multiple Imputation by Chained Equations; BMI, Body Mass Index; ANOVA, Analysis of Variance; LSD, Least Significant Difference; VIF, Variance Inflation Factor; Q1, Quartile 1; Q2, Quartile 2; Q3, Quartile 3; Q4, Quartile 4.
Data Sharing Statement
The datasets used in the current study are not publicly available because of privacy and ethical restrictions but are available from the corresponding author, Guirong Cheng, upon reasonable request.
Ethics Approval and Consent to Participate
The Hubei Memory and Aging Cohort Study (HMACS) (ChiCTR, https://www.chictr.org.cn; registration number: ChiCTR1800019164) was approved by the Ethics Committee of Wuhan University of Science and Technology (protocol code: 201845; approved on October 22, 2018), Wuhan, China. Written informed consent was obtained from all participants or, in the case of cognitively impaired individuals, from a proxy (usually a guardian or family member).
Acknowledgments
We thank all the participants for their willingness to participate in the study and for the time they devoted to it.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Innovation 2030 Major Projects (2022ZD0211600).
Disclosure
The authors declare that they have no competing interests.
References
1. Shrine N, Guyatt AL, Erzurumluoglu AM, et al. New genetic signals for lung function highlight pathways and chronic obstructive pulmonary disease associations across multiple ancestries. Nat Genet. 2019;51(3):481–13. doi:10.1038/s41588-018-0321-7
2. Brandenberger C, Mühlfeld C. Mechanisms of lung aging. Cell Tissue Res. 2017;367(3):469–480. doi:10.1007/s00441-016-2511-x
3. Wang J, Song R, Dove A, et al. Pulmonary function is associated with cognitive decline and structural brain differences. Alzheimer’s Dement. 2022;18(7):1335–1344. doi:10.1002/alz.12479
4. Batty GD, Shipley MJ, Kvaavik E, et al. Biomarker assessment of tobacco smoking exposure and risk of dementia death: pooling of individual participant data from 14 cohort studies. J Epidemiol Community Health. 2018;72(6):513–515. doi:10.1136/jech-2017-209922
5. Stigger FS, Zago Marcolino MA, Portela KM. Plentz RDM. effects of exercise on inflammatory, oxidative, and neurotrophic biomarkers on cognitively impaired individuals diagnosed with dementia or mild cognitive impairment: a systematic review and meta-analysis. J Gerontol a Biol Sci Med Sci. 2019;74(5):616–624. doi:10.1093/gerona/gly173
6. Ma YH, Shen LX, Li YZ, et al. Lung function and risk of incident dementia: a prospective cohort study of 431, 834 individuals. Brain Behav Immun. 2023;109:321–330. doi:10.1016/j.bbi.2023.02.009
7. Grande G, Li Y, Trevisan C, et al. Lung function in relation to brain aging and cognitive transitions in older adults: a population-based cohort study. Alzheimers Dement. 2024;20(8):5662–5673. doi:10.1002/alz.14079
8. Vidal JS, Aspelund T, Jonsdottir MK, et al. Pulmonary function impairment may be an early risk factor for late-life cognitive impairment. J Am Geriatr Soc. 2013;61(1):79–83. doi:10.1111/jgs.12069
9. MacDonald SW, DeCarlo CA, Dixon RA. Linking biological and cognitive aging: toward improving characterizations of developmental time. J Gerontol B Psychol Sci Soc Sci. 2011;66(Suppl 1):i59–i70. doi:10.1093/geronb/gbr039
10. Grenville J, Granell R, Dodd J. Lung function and cognitive ability in children: a UK birth cohort study. BMJ Open Respir Res. 2023;10(1):e001528. doi:10.1136/bmjresp-2022-001528
11. Shang X, Scott D, Chan RK, Zhang L, He M. Association of pulmonary function with cognitive decline in older adults: a nationwide longitudinal study in China. J Gerontol a Biol Sci Med Sci. 2021;76(8):1423–1430. doi:10.1093/gerona/glab096
12. Dai C, Wang Z, Deng Z, et al. Association between serum total bilirubin level and lung function decline in patients with COPD: results from a pooled study. Int J Chron Obstruct Pulmon Dis. 2022;17:1031–1039. doi:10.2147/COPD.S360485
13. Brown KE, Sin DD, Voelker H, et al. Serum bilirubin and the risk of chronic obstructive pulmonary disease exacerbations. Respir Res. 2017;18(1):179. doi:10.1186/s12931-017-0664-0
14. Ficiarà E, Rabbito R, Roveta F, et al. Iron overload, microbleeding and the role of bilirubin in alzheimer’s disease brain: revisiting the vascular hypothesis. Int J Mol Sci. 2025;26(7):3060. doi:10.3390/ijms26073060
15. Jayanti S, Dalla Verde C, Tiribelli C, Gazzin S. Inflammation, dopaminergic brain and bilirubin. Int J Mol Sci. 2023;24(14):11478. doi:10.3390/ijms241411478
16. Choi Y, Lee SJ, Spiller W, et al. Causal associations between serum bilirubin levels and decreased stroke risk: a two-sample mendelian randomization study. Arterioscler Thromb Vasc Biol. 2020;40(2):437–445. doi:10.1161/ATVBAHA.119.313055
17. Creeden JF, Gordon DM, Stec DE, Hinds TD. Bilirubin as a metabolic hormone: the physiological relevance of low levels. Am J Physiol Endocrinol Metab. 2021;320(2):E191–E207. doi:10.1152/ajpendo.00405.2020
18. Qu Y, Ma YH, Huang YY, et al. Blood biomarkers for the diagnosis of amnestic mild cognitive impairment and Alzheimer’s disease: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2021;128:479–486. doi:10.1016/j.neubiorev.2021.07.007
19. Blennow K, Zetterberg H. Biomarkers for Alzheimer’s disease: current status and prospects for the future. J Intern Med. 2018;284(6):643–663. doi:10.1111/joim.12816
20. Chimthanawala NMA, Haria A, Sathaye S. Non-invasive biomarkers for early detection of alzheimer’s disease: a new-age perspective. Mol Neurobiol. 2024;61(1):212–223. doi:10.1007/s12035-023-03578-3
21. van Niel G, D’Angelo G, Raposo G. Shedding light on the cell biology of extracellular vesicles. Nat Rev Mol Cell Biol. 2018;19(4):213–228. doi:10.1038/nrm.2017.125
22. Li L, Cheng GR, Liu D, et al. The hubei memory and aging cohort study: study design, baseline characteristics, and prevalence of cognitive impairments. J Alzheimers Dis. 2022;85(2):561–571. doi:10.3233/JAD-215129
23. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. doi:10.1183/09031936.00080312
24. Wang F, Wang K, Bowerman C, et al. Evaluation of the global lung function initiative 2012 reference values for spirometry in China: a national cross-sectional study. Eur Respir J. 2022;60(6):2200490. doi:10.1183/13993003.00490-2022
25. China Consensus Expert Group on the Prevention and Treatment of cognitive dysfunction. Expert Consensus on Prevention and Treatment of Cognitive Dysfunction in China; 2006.
26. Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004;256(3):183–194. doi:10.1111/j.1365-2796.2004.01388.x
27. Warelow P, Holmes CA. Deconstructing the DSM-IV-TR: a critical perspective. Int J Ment Health Nurs. 2011;20(6):383–391. doi:10.1111/j.1447-0349.2011.00749.x
28. Xiao T, Wijnant SRA, Licher S, et al. Lung function impairment and the risk of incident dementia: the rotterdam study. J Alzheimers Dis. 2021;82(2):621–630. doi:10.3233/JAD-210162
29. Fan J, Fang L, Cong S, et al. Potential pre-COPD indicators in association with COPD development and COPD prediction models in Chinese: a prospective cohort study. Lancet Reg Health West Pac. 2023;44:100984. doi:10.1016/j.lanwpc.2023.100984
30. Wu XJ, Huang Y, Wang Y, et al. Association between peak expiratory flow and cognitive function in children with asthma. Nan Fang Yi Ke Da Xue Xue Bao. 2011;31(11):1900–1902.
31. Li QY, Li XM, Hu HY, et al. Associations of lung function decline with risks of cognitive impairment and dementia: a meta-analysis and systematic review. J Alzheimers Dis. 2023;92(3):853–873. doi:10.3233/JAD-221136
32. Xiao T, Wijnant SRA, van der Velpen I, et al. Lung function impairment in relation to cognition and vascular brain lesions: the rotterdam study. J Neurol. 2022;269(8):4141–4153. doi:10.1007/s00415-022-11027-9
33. Liu X, Ma Y, Ouyang R, et al. The relationship between inflammation and neurocognitive dysfunction in obstructive sleep apnea syndrome. J Neuroinflammation. 2020;17(1):229. doi:10.1186/s12974-020-01905-2
34. Mayer OH. Clinical pulmonary function testing in Duchenne muscular dystrophy. Paediatr Respir Rev. 2019;30:9–12. doi:10.1016/j.prrv.2018.08.004
35. Sriboonreung T, Leelarungrayub J, Yankai A, Puntumetakul R. Correlation and predicted equations of mip/mep from the pulmonary function, demographics and anthropometrics in healthy Thai participants aged 19 to 50 years. Clin Med Insights Circ Respir Pulm Med. 2021;15:11795484211004494. doi:10.1177/11795484211004494
36. van Bakel SIJ, Gosker HR, Langen RC, Schols AMWJ. Towards personalized management of sarcopenia in COPD. Int J Chron Obstruct Pulmon Dis. 2021;16:25–40. doi:10.2147/COPD.S280540
37. Higbee DH, Granell R, Hemani G, Smith GD, Dodd JW. Lung function, COPD and cognitive function: a multivariable and two sample Mendelian randomization study. BMC Pulm Med. 2021;21(1):246. doi:10.1186/s12890-021-01611-6
38. Verlato G, Olivieri M. Reduced lung function in midlife and cognitive impairment in the elderly. Am J Respir Crit Care Med. 2019;199(11):1304–1305. doi:10.1164/rccm.201811-2214ED
39. Lutsey PL, Chen N, Mirabelli MC, et al. Impaired lung function, lung disease, and risk of incident dementia. Am J Respir Crit Care Med. 2019;199(11):1385–1396. doi:10.1164/rccm.201807-1220OC
40. Zhou L, Yang H, Zhang Y, et al. Association of impaired lung function with dementia, and brain magnetic resonance imaging indices: a large population-based longitudinal study. Age Ageing. 2022;51(11):afac269. doi:10.1093/ageing/afac269
41. Carvalhaes-Neto N, Lorino H, Gallinari C, et al. Cognitive function and assessment of lung function in the elderly. Am J Respir Crit Care Med. 1995;152(5):1611–1615. doi:10.1164/ajrccm.152.5.7582303
42. Barok R, Grittner JML, Miller S, Dougherty BJ. Sex hormone supplementation improves breathing and restores respiratory neuroplasticity following C2 hemisection in rats. Front Physiol. 2024;15:1390777. doi:10.3389/fphys.2024.1390777
43. Cahana-Amitay D, Lee LO, Spiro A 3rd, Albert ML. Breathe Easy, speak easy: pulmonary function and language performance in aging. Exp Aging Res. 2018;44(5):351–368. doi:10.1080/0361073X.2018.1521374
44. Kawano-Dourado L, Glassberg MK, Assayag D, Borie R, Johannson KA. Sex and gender in interstitial lung diseases. Eur Respir Rev. 2021;30(162):210105. doi:10.1183/16000617.0105-2021
45. Torres A, Gómez-Gil E, Vidal A, Puig O, Boget T, Salamero M. Diferencias de género en las funciones cognitivas e influencia de las hormonas sexuales Gender differences in cognitive functions and influence of sex hormones. Actas Esp Psiquiatr. 2006;34(6):408–415.
46. Lager E, Sorjonen K, Melin M. Gender differences in operational and cognitive abilities. Front Psychol. 2024;15:1402645. doi:10.3389/fpsyg.2024.1402645
47. Mishra S, TM B, DM H, et al. Longitudinal brain imaging in preclinical Alzheimer disease: impact of APOE ε4 genotype. Brain. 2018;141(6):1828–1839. doi:10.1093/brain/awy103
48. Kivipelto M, Helkala EL, Laakso MP, et al. Midlife vascular risk factors and Alzheimer’s disease in later life: longitudinal, population based study. BMJ. 2001;322(7300):1447–1451. doi:10.1136/bmj.322.7300.1447
49. Koopman J, Howe M, Hollenbeck JR, Sin HP. Small sample mediation testing: misplaced confidence in bootstrapped confidence intervals. J Appl Psychol. 2015;100(1):194–202. doi:10.1037/a0036635
50. Ahn KM, Lee SY, Kim SS, Park HW, Park H-W. Lung function decline is associated with serum uric acid in Korean health screening individuals. Sci Rep. 2021;11(1):10183. doi:10.1038/s41598-021-89678-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Coexisting Frailty and Cognitive Impairment as a Predictor of Adverse Outcomes in Older Inpatients After Discharge: Results from a One-Year Follow-Up Study
Zeng XK, Shen SS, Guan HL, Chen LY, Chen XJ
Clinical Interventions in Aging 2022, 17:1697-1706
Published Date: 29 November 2022
Relationship Between Physical Exercise and Cognitive Impairment Among Older Adults with Type 2 Diabetes: Chain Mediating Roles of Sleep Quality and Depression
Zhang H, Zhang Y, Sheng S, Xing Y, Mou Z, Zhang Y, Shi Z, Yu Z, Gao Q, Cai W, Jing Q
Psychology Research and Behavior Management 2023, 16:817-828
Published Date: 17 March 2023
Physical Activity Mediates the Relationship Between Sarcopenia and Cognitive Function Among Older Adults in Nursing Homes
Yao X, Liu B, Hua N, Huang J, Zhao X
Clinical Interventions in Aging 2023, 18:1863-1871
Published Date: 13 November 2023
Association Between Nephrolithiasis and the Prevalence of Sarcopenia in Chinese Older Adults: A Cross-Sectional Study Using Propensity Score Matching
Wu C, Li XQ, Lu SS, Shen ZK, Lu X
Clinical Interventions in Aging 2025, 20:2353-2362
Published Date: 2 December 2025