Back to Journals » Clinical Interventions in Aging » Volume 20
Association Between Nephrolithiasis and the Prevalence of Sarcopenia in Chinese Older Adults: A Cross-Sectional Study Using Propensity Score Matching
Authors Wu C ![]() , Li XQ, Lu SS, Shen ZK, Lu X
, Li XQ, Lu SS, Shen ZK, Lu X
Received 18 June 2025
Accepted for publication 25 November 2025
Published 2 December 2025 Volume 2025:20 Pages 2353—2362
DOI https://doi.org/10.2147/CIA.S547830
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Cheng Wu,1,* Xiao-Qing Li,1,* Shan-Shan Lu,1,* Zheng-Kai Shen,2 Xiang Lu1
1Department of Geriatrics, Sir Run Run Hospital, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 2Jiangsu Province Center for Disease Control and Prevention, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiang Lu, Department of Geriatrics, Sir Run Run Hospital, Nanjing Medical University, Nanjing, 211166, People’s Republic of China, Email [email protected] Zheng-Kai Shen, MPH, Jiangsu Province Center for Disease Control and Prevention, Nanjing, 210009, People’s Republic of China, Email [email protected]
Background: Sarcopenia is an age-related condition characterized by loss of muscle mass and function. Nephrolithiasis represents a prevalent urological disorder that imposes a substantial burden on healthcare resources. However, the association between sarcopenia and nephrolithiasis remains poorly characterized.
Methods: A total of 2586 older adults were included in this cross-sectional study. We used the univariate and multivariate logistic regression models to assess the relationship between nephrolithiasis and sarcopenia. Additionally, stratified analyses and propensity score matching (PSM) were performed to account for potential confounding factors.
Results: The prevalence of sarcopenia in the present study was 7.2%. In Model 4, which integrated for all relevant covariates, nephrolithiasis was associated with approximately a 190% increased prevalence of sarcopenia compared to non-nephrolithiasis patients (OR: 2.912, 95% CI: 1.708– 4.968, P < 0.001). Following PSM, the results also confirmed the association between nephrolithiasis and sarcopenia (OR: 4.426, 95% CI: 1.547– 12.661, P = 0.006). Notably, this association was more pronounced in subgroups including males (OR: 3.296, 95% CI: 1.436– 7.564, P = 0.005), lower education level (OR: 8.127, 95% CI: 3.057– 21.609, P < 0.001), and diabetes (OR: 6.686, 95% CI: 2.626– 17.027, P < 0.001).
Conclusion: Our findings demonstrate that nephrolithiasis is positively related to the potential risk of sarcopenia in Chinese older adults. This finding indicates that nephrolithiasis may contribute to sarcopenia development, thereby emphasizing that prevention and intervention strategies for sarcopenia should account for the adverse effects of nephrolithiasis.
Keywords: cross-sectional study, nephrolithiasis, older adults, propensity score matching, sarcopenia
Introduction
Sarcopenia is defined as an age-associated, progressive syndrome characterized by the loss of skeletal muscle mass, and function.1 Accumulating evidence establishes sarcopenia as an independent risk factor for falls, frailty, disability, and death.2 The development of sarcopenia has been established to be associated with multiple factors, including age, gender, body mass index (BMI), nutritional status, and diabetes, among others.3 The overall prevalence of sarcopenia among older adults ranges from 10% to 16%, with a higher prevalence rate in patient populations.3 In China, The prevalence of sarcopenia among middle-aged and older adults has been reported to range from 7.7% to 19.3%.4–6 Consequently, sarcopenia has emerged as a prevalent medical burden in older adult populations.
Urolithiasis remains one of the most prevalent urological disorders globally, imposing a significant burden across diverse patient populations. Over the past few decades, the global prevalence and incidence of urolithiasis have demonstrated a consistent upward trend.7,8 As a prevalent form of urolithiasis, nephrolithiasis imposes both chronic pain and substantial economic burdens on patients.9–11 In the United States, nephrolithiasis affects approximately 10.6% of men and 7.1% of women, with prevalence rates comparable to those of diabetes (9.7%).12–14 Concurrently, the medical costs for nephrolithiasis exceeded $5 billion in 2005.10 Age, sex, BMI, diabetes, and other risk factors have been established to be associated with the pathogenesis of kidney stones.11,15 This finding is partially congruent with the established risk factors for sarcopenia. Interestingly, a recent study leveraging data from the National Health and Nutrition Examination Survey (NHANES) has revealed a positive association between sarcopenia and the potential risk of kidney stones in the adult population of the United States.16 Unfortunately, in this study, sarcopenia was assessed using the sarcopenia index, with insufficient data provided on muscle strength and physical performance. However, the association between nephrolithiasis and the prevalence of sarcopenia remains underexplored in the current study, particularly among elderly populations across diverse geographic regions. Additionally, recent pathophysiological evidence indicates that chronic inflammation is one of the common potential mechanisms underpinning sarcopenia pathogenesis.17,18 Inflammatory responses have also been demonstrated to exert a critical regulatory role in kidney stone formation.19 Based on the aforementioned associations, it can be hypothesized that the relationship between sarcopenia and nephrolithiasis may be mediated by inflammation.
The objective of this study was to examine the association between nephrolithiasis and the prevalence of sarcopenia in a population of older adults in China.
Materials and Methods
Study Population
The cross-sectional study was based on the National Basic Public Health Project, which provides physical examinations for older adults in China annually as previously described.20 Data were extracted from participants aged ≥60 years in the 2020 project conducted at Maigaoqiao Community Medical Center in Nanjing, Jiangsu Province. The exclusion criteria were: (1) non-ambulatory or bedridden; (2) unable to complete sarcopenia-specific assessment maneuvers; (3) cardiac dysfunction (New York Heart Association class III/IV); (4) Severe hepatic impairment (aminotransferase elevation exceeding twice the upper limit of normal) or renal impairment (creatinine clearance rate <60 mL/min); (5) malignant tumor; (6) psychiatric disorders or dementia. This study was conducted in accordance with the Declaration of Helsinki21 and received ethical approval from the Ethics Committee of Sir Run Run Hospital, Nanjing Medical University (approval No. 2019-SR-S041). Written informed consent was obtained from all participants.
Data Collection
Body mass index (BMI) was calculated by dividing weight by height squared. The waist-to-hip ratio (WHR) was calculated as waist circumference divided by hip circumference. Fasting venous blood samples were collected in the morning for analysis of hematological and biochemical parameters. Alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum creatinine (SCr), blood urea nitrogen (BUN), total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL), and high-density lipoprotein cholesterol (HDL) were measured. Education level, marital status, smoking status, alcohol consumption, exercise situation, and chronic disease status were collected via self-administered questionnaires. Nephrolithiasis are defined as solid masses forming in the kidneys, resulting from supersaturation of urinary mineral components (eg, calcium oxalate, urate) that undergo crystallization and aggregation. They may be associated with urinary tract obstruction, infection, or chronic kidney injury. The presence of kidney stones was ascertained by abdominal ultrasonography.
Assessment of Sarcopenia
Sarcopenia was diagnosed according to the latest Asian Working Group for Sarcopenia criteria, defined as low appendicular skeletal muscle mass (ASM) plus low muscle strength and/or low physical performance.1 ASM was assessed via bioelectrical impedance analysis (BIA) using the Inbody S10 (Inbody, Korea). The height-adjusted ASM index (ASMI) was further calculated as ASM divided by height squared in meters (ASM/height2). Low ASM was defined as an ASMI <7.0 kg/m2 in men and <5.7 kg/m2 in women. Muscle strength was assessed by grip strength and measured using a dynamometer (CAMRY EH101, China). In the standing position, the grip strength of each hand was measured 3 times, and the maximum value was taken. Low muscle strength was defined as handgrip strength <28 kg in men and <18 kg in women. The walking speed was assessed by a 4-m course for 3 times and the average value was used. Low physical performance was defined as walking speed <1 m/s.
Statistical Analysis
Continuous variables were tested for normality using the Kolmogorov–Smirnov test and were presented as mean ± standard deviation. The Mann–Whitney U-test or independent samples t-test was used to determine differences between two groups. Categorical variables were compared between groups using the χ2-test (Chi-square test). Univariate and multivariate logistic regression analyses were conducted to assess the relationship between sarcopenia and the prevalence of nephrolithiasis. The variables included in propensity score matching comprise age, gender, BMI, WHR, education level, marital status, smoke, drink, exercise, AST/ALT ratio, SCr, BUN, TC, TG, LDL, HDL, hypertension, diabetes, and nephrolithiasis. Propensity score matching was performed using a 1:1 nearest-neighbor algorithm, with a caliper width of 0.05 standard deviations of the logit-transformed propensity score, balancing covariate distribution while minimizing matched pair loss. For the matched cohort derived from propensity score matching, we confirmed a statistical power of 0.85, which was estimated using the expected between-group difference in nephrolithiasis prevalence and an α of 0.05. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. A p value <0.05 was considered to be statistically significant. All statistical analyses were conducted using SPSS 30.0 and R 4.5.0.
Results
Characteristics of Participants
In the present study, the overall prevalence of sarcopenia was 7.2% (186/2586). Table 1 presents the baseline characteristics of the older adults categorized by sarcopenia. In the sarcopenia group, levels of age, AST/ALT ratio, and BUN were higher, while the levels of BMI, grip strength, walking speed, and ASMI were lower. Additionally, sarcopenia patients had lower education level compared to those without sarcopenia. However, there was no significant difference in gender, WHR, SCr, TC, TG, LDL, HDL, marital status, smoke, drink, exercise, hypertension, and diabetes between the two groups. Specifically, the prevalence of nephrolithiasis was significantly higher in participants with sarcopenia.
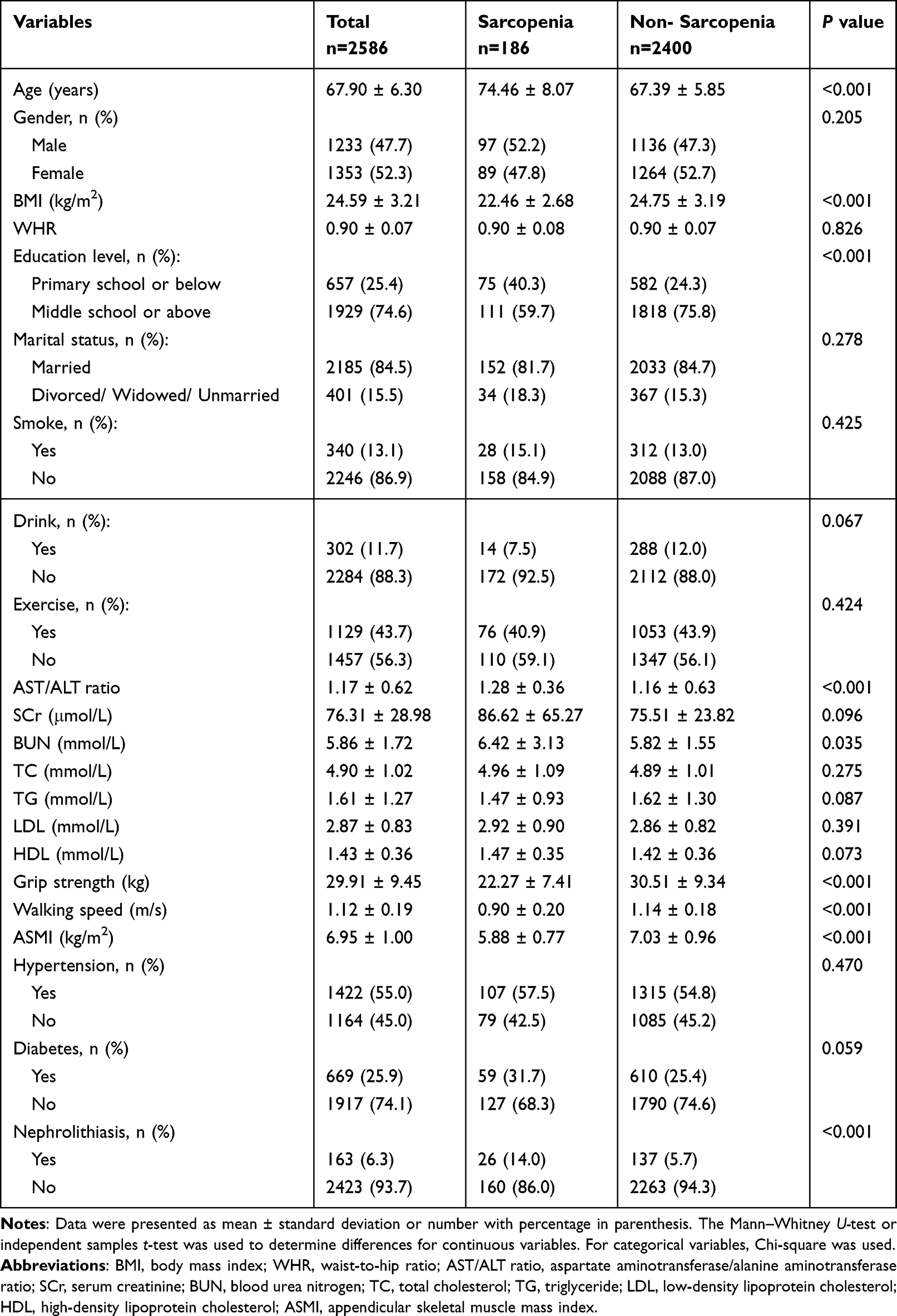 |
Table 1 Baseline Characteristics of Participants |
Relationship Between Sarcopenia and Covariates
As shown in Table 2, univariate and multivariate logistic regression models were employed to investigate the relationship between sarcopenia and nephrolithiasis. Model 1, adjusted for no factors, indicated that the presence of nephrolithiasis was associated with a higher prevalence of sarcopenia (OR: 2.684, 95% CI: 1.713–4.205, P <0.001). In Model 2, which adjusted for age, gender, BMI, and WHR, nephrolithiasis was associated with a 202% increased prevalence of sarcopenia compared to non-nephrolithiasis patients (OR: 3.021, 95% CI: 1.799–5.073, P <0.001). Model 3, further adjusted for education level, marital status, smoke, drink, and exercise, revealed a statistically significant positive association between nephrolithiasis and sarcopenia (OR: 3.050, 95% CI: 1.807–5.149, P <0.001). Model 4, adjusted for all covariates, maintained a significant positive association between nephrolithiasis and sarcopenia (OR: 2.912, 95% CI: 1.708–4.968, P <0.001). Then, multivariable logistic regression analyses were performed to assess independent associations between sarcopenia and variables, detailed in Figure 1. Besides nephrolithiasis, age (OR: 1.516, 95% CI: 1.127–1.185, P <0.001), BMI (OR: 0.723, 95% CI: 0.675–0.774, P <0.001), and education level (OR: 0.547, 95% CI: 0.376–0.796, P = 0.002) also were shown to be significantly and independently associated with sarcopenia in adjusted models.
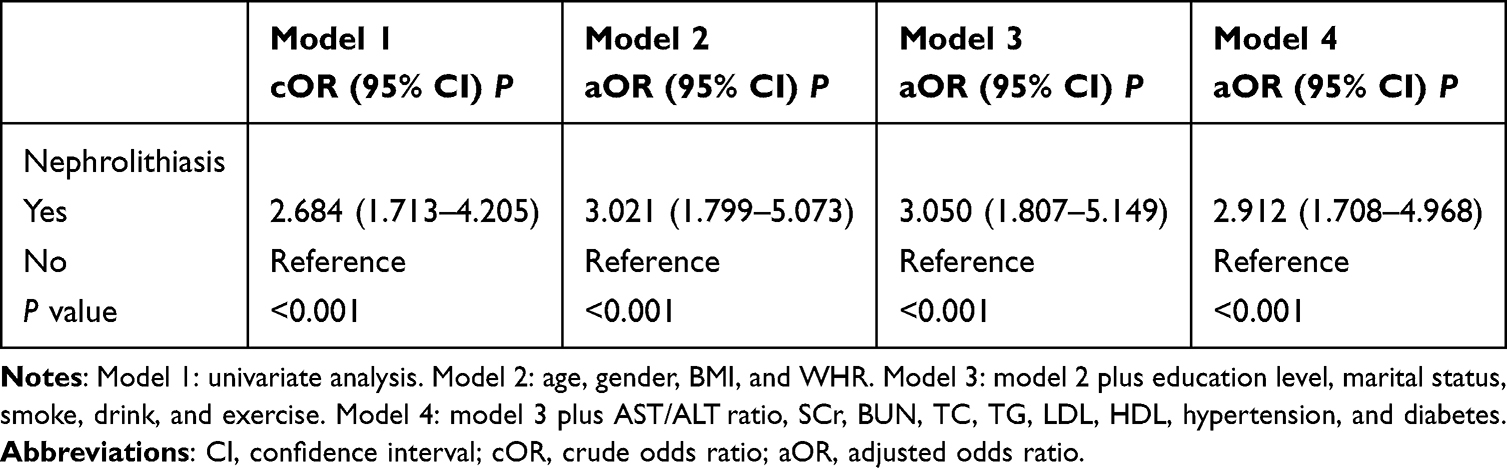 |
Table 2 Logistic Regression Analyzed the Relationship Between the Presence of Nephrolithiasis and Sarcopenia |
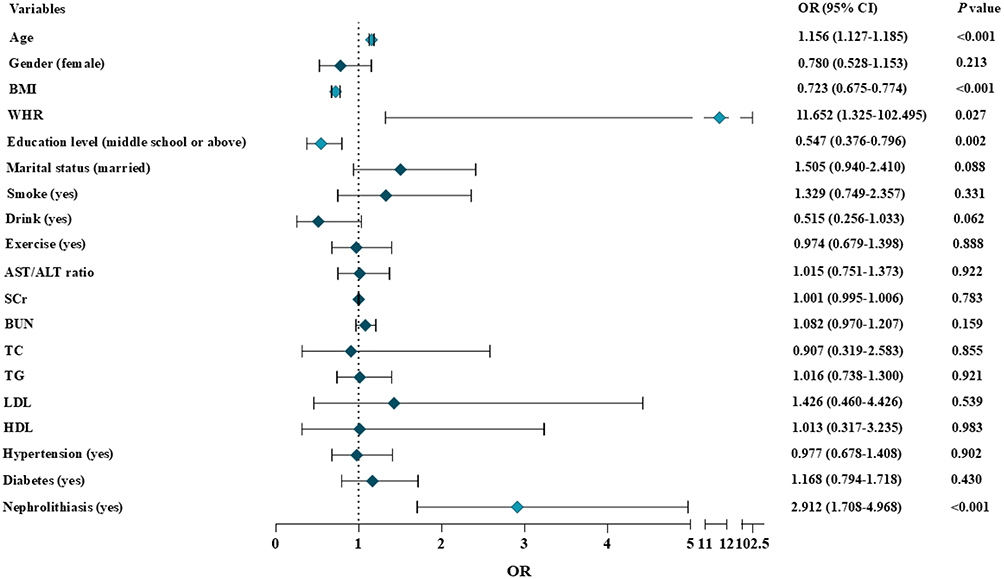 |
Figure 1 Association between selected variables and the prevalence of sarcopenia. Logistic regression model adjusted for age, gender, BMI, WHR, education level, marital status, smoke, drink, exercise, AST/ALT ratio, SCr, BUN, TC, TG, LDL, HDL, hypertension, diabetes, and nephrolithiasis. |
Stratified Analysis
Stratified analyses were used to assess the relationship between nephrolithiasis and sarcopenia across different populations (Table 3). The presence of nephrolithiasis was associated with higher risk of sarcopenia after adjustment for potential confounders only in males (OR: 3.296, 95% CI: 1.436–7.564, P = 0.005) but not in females. In addition, crude and adjusted models revealed a significant association between nephrolithiasis and sarcopenia in the lower education level (OR: 8.127, 95% CI: 3.057–21.609, P <0.001). Similarly, the association of nephrolithiasis and sarcopenia was only observed in the older adults with diabetes (OR: 6.686, 95% CI: 2.626–17.027, P <0.001). However, subgroup analyses stratified by age, BMI, hypertension, and exercise consistently demonstrated significant associations between nephrolithiasis and elevated sarcopenia risk in both crude and adjusted models.
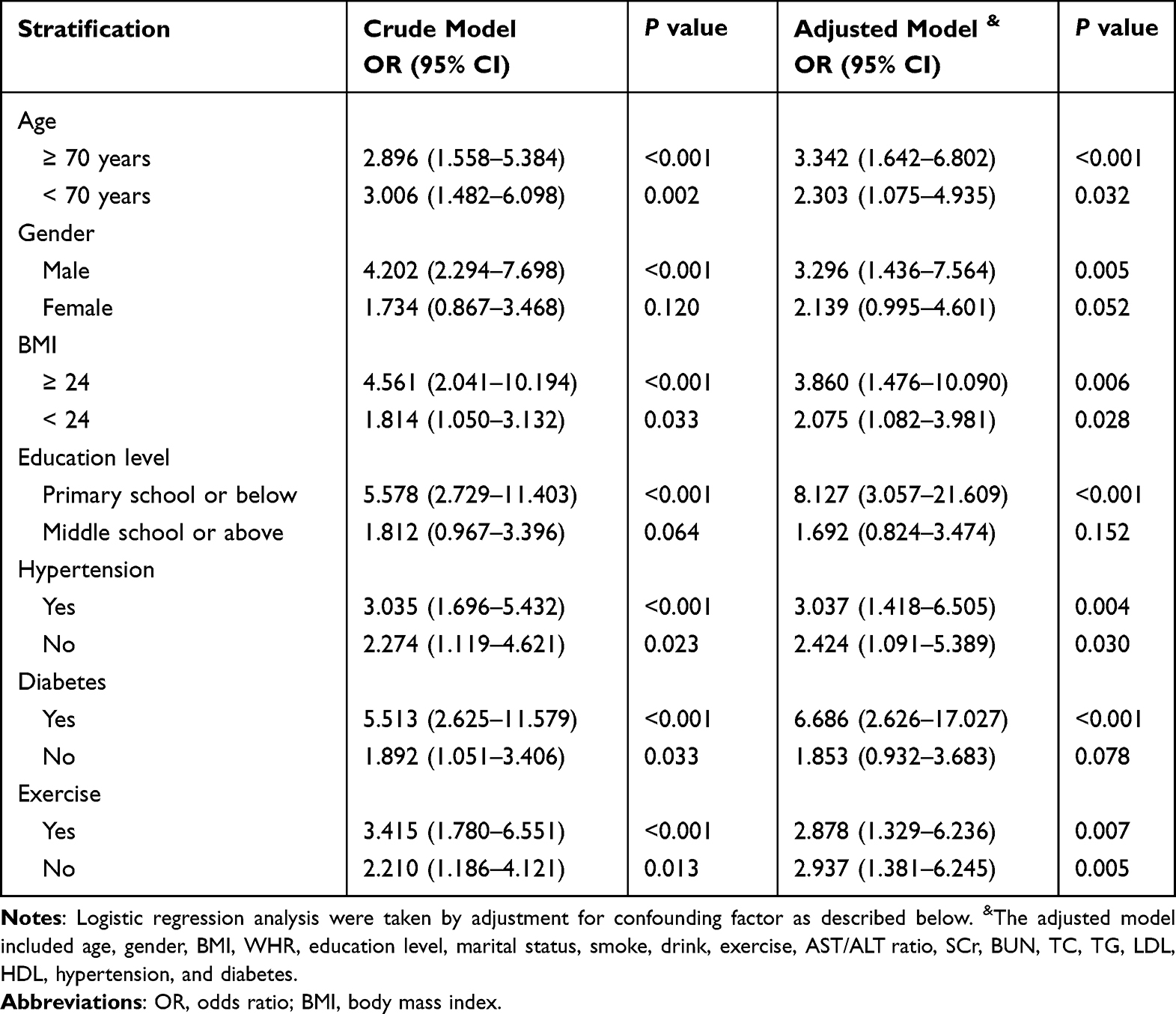 |
Table 3 Stratification Analyses for the Relationship Between the Presence of Nephrolithiasis and Sarcopenia |
Propensity Score Matching Analysis
To address potential confounding baseline characteristics between the sarcopenic and non-sarcopenic groups, propensity score matching (PSM) was performed. Baseline characteristics after PSM are presented in Supplementary Table 1, with PSM results shown in Figure 2. Univariate and multivariate logistic regression analyses were performed on post-PSM data, with results presented in Table 4. We found that the results from all four models consistently indicated a positive association between nephrolithiasis and sarcopenia (Table 4, P <0.05). There were adjusted covariates in four models. Model 1 was not adjusted. Model 2 was adjusted for age, gender, BMI, and WHR. Model 3 was adjusted for model 2 plus education level, marital status, smoke, drink, and exercise. Model 4 was adjusted for model 3 plus AST/ALT ratio, SCr, BUN, TC, TG, LDL, HDL, hypertension, and diabetes.
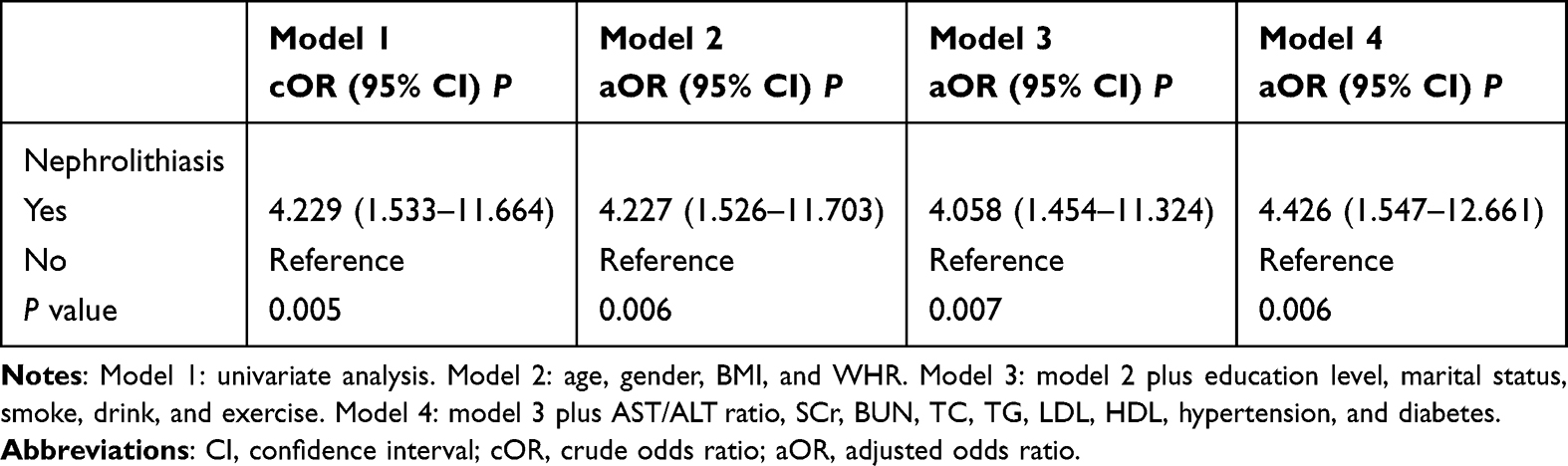 |
Table 4 Logistic Regression Analyzed the Relationship Between the Presence of Nephrolithiasis and Sarcopenia After Propensity Score Matching |
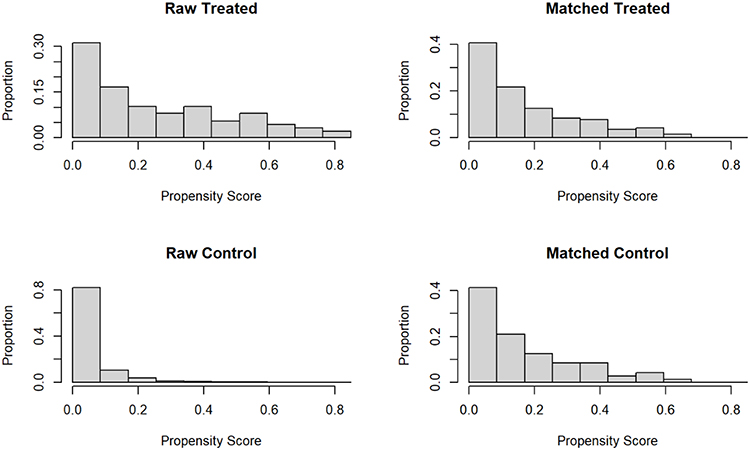 |
Figure 2 Distribution of propensity score before and after matching. |
Discussion
In this study, we conducted a cross-sectional analysis using data from older adults in China to explore the relationship between sarcopenia and nephrolithiasis. We found that the prevalence of sarcopenia increased significantly with the presence of nephrolithiasis, suggesting that nephrolithiasis may serve as a risk factor for sarcopenia. To minimize the impact of confounding variables, propensity score matching was performed. The findings from the propensity score-matched analysis further validated the positive association between sarcopenia and nephrolithiasis. Notably, this association was more evident in male participants, individuals with lower educational attainment, and subgroups with diabetes.
In a cross-section study based on the National Health and Nutrition Examination Survey (NHANES), researchers enrolled 759 kidney stones and 8713 unexposed individuals to investigate the relationship between sarcopenia and nephrolithiasis in United States adult population during 2011–2018.16 However, this study solely relied on sarcopenia index (total appendicular skeletal muscle mass/body mass index) for diagnosis and did not assess muscle strength and physical function. In 2019, the Asian Working Group on Sarcopenia in Older Adults and the European Working Group on Sarcopenia in Older People jointly recommended that sarcopenia should be diagnosed in individuals with low muscle strength, low muscle mass, and poor physical function.1,22 Therefore, relying solely on the sarcopenia index can not completely replace the diagnosis of sarcopenia. Additionally, diagnosing nephrolithiasis via questionnaires rather than imaging examinations represents another limitation. Nonetheless, this study has offered some valuable insights.
In our study, advanced age, lower BMI, and lower educational level were identified as independent risk factors for sarcopenia, which is consistent with findings from prior studies.3,23 Several studies have demonstrated significant associations between sarcopenia and factors such as gender, smoking status, alcohol consumption, physical activity, or diabetes.23,24 Unfortunately, these correlations were not observed in the present study. Potential explanations may include the absence of large-scale population data and the influence of confounding factors. Historically, nephrolithiasis are more common in male patients than in female patients, which is consistent with our findings. However, epidemiological trends in nephrolithiasis suggest that this sex disparity is narrowing.25 The stronger association observed in individuals with lower educational attainment may be attributable to their suboptimal economic conditions and nutritional status. Concurrently, we observed a positive association between sarcopenia and nephrolithiasis across diabetes subgroups. Previous studies have established that diabetes is closely associated with not only sarcopenia but also nephrolithiasis.3,11 Subgroup analysis and propensity score matching (PSM) confirmed that nephrolithiasis remained positively associated with sarcopenia after adjustment for confounding factors.
Although the exact mechanism underlying the association between nephrolithiasis and sarcopenia remains unclear, several possible hypotheses have been proposed. First, nephrolithiasis has been reported to be associated with several unhealthy behaviors, such as poor nutrition, a sedentary lifestyle, and physical inactivity,15,25,26 which may reduce muscle protein synthesis, accelerate muscle catabolism, and ultimately contribute to muscle atrophy.27 Second, the pathogenesis of sarcopenia involves multiple pathophysiological processes, including inflammation, mitochondrial dysfunction, and apoptosis.17,18 The primary constituent of kidney stones is calcium oxalate (CaOx) crystals, which comprise up to 80% of all nephrolithiasis cases.28 CaOx induces renal damage primarily through mechanisms such as apoptosis, autophagy, inflammation, and fibrosis.19,29–31 Upon infiltrating muscle cells, pro-inflammatory cytokines trigger NF-κB pathway activation, driving inflammatory cell recruitment and mitochondrial dysfunction. This cascading reaction disrupts muscle protein homeostasis, impairs muscle regenerative capacity, and contributes to the pathogenesis of sarcopenia.32–34 Third, metabolic disorders including obesity and diabetes have been established as risk factors for nephrolithiasis development.11,35,36 The presence of these chronic diseases activates the insulin signaling pathway, inducing glucose metabolism disorders and muscle energy dysregulation, thereby accelerating muscle loss.37–39 However, current research on this association remains limited, and further studies are warranted to elucidate the underlying mechanisms.
This study identifies nephrolithiasis as a previously underestimated risk factor in elderly individuals with sarcopenia, thereby providing a novel insight into the long-term management of this patient population. Accordingly, to translate this finding into primary care practice, nephrolithiasis screening should be integrated into the routine assessment of elderly patients with sarcopenia, aiming to facilitate the early detection of high-risk groups. Additionally, multidisciplinary consultations with nephrologists, geriatricians, nurses, and nutritionists are advised to design personalized interventions for elderly patients with both sarcopenia and nephrolithiasis. These strategies, including dietary adjustments and targeted resistance training, may help reduce nephrolithiasis and improve muscle function and quality.
Our study has several strengths. Firstly, to the best of our knowledge, we are the first to assess the association between nephrolithiasis and sarcopenia in Chinese older adults. Secondly, our study enrolled a relatively large sample from the elderly population, thereby minimizing the influence of certain primary diseases on muscle mass and function. However, there are still limitations in our study. First, as a cross-sectional analysis, this study cannot establish a causal relationship between nephrolithiasis and sarcopenia. Second, the exclusion of participants due to missing data may have introduced selection bias into the final results. Third, this study was limited to older adults in eastern China. Fourth, despite multivariable adjustment for established confounding factors, residual confounding may persist—particularly regarding unmeasured variables such as stone composition and burden, genetic factors, and dietary patterns. Fifth, BIA measurements may be affected by individual hydration status—despite standardized testing conditions (eg, overnight fasting, post-voiding)—leading to potential inaccuracies. Therefore, future studies should incorporate larger sample sizes, more comprehensive variable assessments, and more reliable diagnostic tools to explore potential mechanisms and establish causal relationships.
Conclusions
To summarize, nephrolithiasis is positively associated with the risk of sarcopenia in elderly Chinese adults. Notably, this association was stronger in males, those with lower education, and individuals with diabetes. These results highlight that the adverse impact of nephrolithiasis should be considered in future strategies for preventing and managing sarcopenia. Further prospective studies are warranted to validate this association and explore its underlying mechanisms.
Data Sharing Statement
Data supporting this study’s findings are not publicly available due to sensitivity but are available from the corresponding author upon reasonable request.
Acknowledgments
We acknowledge the members and all participants of the National Basic Public Health Project. This study was approved by the Ethics Committee of Sir Run Run Hospital, Nanjing Medical University (approval number 2019-SR-S041). Written informed consent was obtained from each participant.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Key Research and Development Plan of China (No.2020YFC2008505 to Xiang Lu), the National Natural Science Foundation of China (81970218 to Xiang Lu), and the Jiangsu Commission of Health (No. LKM2023004 to Zheng-Kai Shen).
Disclosure
The authors declare no conflicts of interest.
References
1. Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307.e2. doi:10.1016/j.jamda.2019.12.012
2. Liguori I, Russo G, Aran L, et al. Sarcopenia: assessment of disease burden and strategies to improve outcomes. Clin Interv Aging. 2018;13:913–927. doi:10.2147/cia.S149232
3. Yuan S, Larsson SC. Epidemiology of sarcopenia: prevalence, risk factors, and consequences. Metabolism. 2023;144:155533. doi:10.1016/j.metabol.2023.155533
4. Gao K, Cao LF, Ma WZ, et al. Association between sarcopenia and cardiovascular disease among middle-aged and older adults: findings from the China health and retirement longitudinal study. EClinicalMedicine. 2022;44:101264. doi:10.1016/j.eclinm.2021.101264
5. Liu X, Hou L, Xia X, et al. Prevalence of sarcopenia in multi ethnics adults and the association with cognitive impairment: findings from West-China health and aging trend study. BMC Geriatr. 2020;20(1):63. doi:10.1186/s12877-020-1468-5
6. Wu X, Li X, Xu M, Zhang Z, He L, Li Y. Sarcopenia prevalence and associated factors among older Chinese population: findings from the China Health and Retirement Longitudinal Study. PLoS One. 2021;16(3):e0247617. doi:10.1371/journal.pone.0247617
7. Skolarikos A, Somani B, Neisius A, et al. Metabolic evaluation and recurrence prevention for urinary stone patients: an eau guidelines update. Eur Urol. 2024;86(4):343–363. doi:10.1016/j.eururo.2024.05.029
8. Chewcharat A, Curhan G. Trends in the prevalence of kidney stones in the United States from 2007 to 2016. Urolithiasis. 2021;49(1):27–39. doi:10.1007/s00240-020-01210-w
9. Eisner BH, Goldfarb DS. A nomogram for the prediction of kidney stone recurrence. J Am Soc Nephrol. 2014;25(12):2685–2687. doi:10.1681/asn.2014060631
10. Hyams ES, Matlaga BR. Economic impact of urinary stones. Transl Androl Urol. 2014;3(3):278–283. doi:10.3978/j.issn.2223-4683.2014.07.02
11. Ma Y, Cheng C, Jian Z, et al. Risk factors for nephrolithiasis formation: an umbrella review. Int J Surg. 2024;110(9):5733–5744. doi:10.1097/js9.0000000000001719
12. Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1):160–165. doi:10.1016/j.eururo.2012.03.052
13. Sorokin I, Mamoulakis C, Miyazawa K, Rodgers A, Talati J, Lotan Y. Epidemiology of stone disease across the world. World J Urol. 2017;35(9):1301–1320. doi:10.1007/s00345-017-2008-6
14. Xu G, Liu B, Sun Y, et al. Prevalence of diagnosed type 1 and type 2 diabetes among US adults in 2016 and 2017: population based study. BMJ. 2018;
15. Kittanamongkolchai W, Vaughan LE, Enders FT, et al. The changing incidence and presentation of urinary stones over 3 decades. Mayo Clin Proc. 2018;93(3):291–299. doi:10.1016/j.mayocp.2017.11.018
16. Zhang Y, Tian C, Wang Y, et al. Association between sarcopenia and kidney stones in United States adult population between 2011 and 2018. Front Nutr. 2023;10:1123588. doi:10.3389/fnut.2023.1123588
17. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646. doi:10.1016/s0140-6736(19)31138-9
18. Najm A, Niculescu AG, Grumezescu AM, Beuran M. emerging therapeutic strategies in sarcopenia: an updated review on pathogenesis and treatment advances. Int J Mol Sci. 2024;25(8). doi:10.3390/ijms25084300
19. Khan SR, Canales BK, Dominguez-Gutierrez PR. Randall’s plaque and calcium oxalate stone formation: role for immunity and inflammation. Nat Rev Nephrol. 2021;17(6):417–433. doi:10.1038/s41581-020-00392-1
20. Wu C, Wang Q, Zhou CY, et al. Association of AST/ALT (De Ritis) ratio with sarcopenia in a Chinese population of community-dwelling elderly. Heliyon. 2023;9(10):e20427. doi:10.1016/j.heliyon.2023.e20427
21. Code of ethics on human experimentation adapted from the helsinki declaration of the world medical association. Am J Orthopsychiatry. 1968;38(4):589–590. doi:10.1111/j.1939-0025.1968.tb02426.x
22. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
23. Petermann-Rocha F, Chen M, Gray SR, Ho FK, Pell JP, Celis-Morales C. Factors associated with sarcopenia: a cross-sectional analysis using UK Biobank. Maturitas. 2020;133:60–67. doi:10.1016/j.maturitas.2020.01.004
24. Anagnostis P, Gkekas NK, Achilla C, et al. Type 2 diabetes mellitus is associated with increased risk of sarcopenia: a systematic review and meta-analysis. Calcif Tissue Int. 2020;107(5):453–463. doi:10.1007/s00223-020-00742-y
25. Abufaraj M, Xu T, Cao C, et al. Prevalence and trends in kidney stone among adults in the USA: analyses of national health and nutrition examination survey 2007-2018 data. Eur Urol Focus. 2021;7(6):1468–1475. doi:10.1016/j.euf.2020.08.011
26. Li Y, Di X, Liu M, Wei J, Li T, Liao B. Association between daily sitting time and kidney stones based on the National Health and Nutrition Examination Survey (NHANES) 2007-2016: a cross-sectional study. Int J Surg. 2024;110(8):4624–4632. doi:10.1097/js9.0000000000001560
27. Nunes EA, Stokes T, McKendry J, Currier BS, Phillips SM. Disuse-induced skeletal muscle atrophy in disease and nondisease states in humans: mechanisms, prevention, and recovery strategies. Am J Physiol Cell Physiol. 2022;322(6):C1068–c1084. doi:10.1152/ajpcell.00425.2021
28. Sun XY, Ouyang JM, Gan QZ, Liu AJ. Renal epithelial cell injury induced by calcium oxalate monohydrate depends on their structural features: size, surface, and crystalline structure. J Biomed Nanotechnol. 2016;12(11):2001–2014. doi:10.1166/jbn.2016.2289
29. Xie H, Li J, Gao H, et al. Total flavone of Desmodium styracifolium relieved apoptosis and autophagy of COM-induced HK-2 cells by regulating KIM-1 via p38/MAPK pathway. Mol Cell Biochem. 2018;442(1–2):169–175. doi:10.1007/s11010-017-3201-z
30. Sun Y, Kang J, Tao Z, et al. Effect of endoplasmic reticulum stress-mediated excessive autophagy on apoptosis and formation of kidney stones. Life Sci. 2020;244:117232. doi:10.1016/j.lfs.2019.117232
31. Ye Z, Xia Y, Li L, et al. p53 deacetylation alleviates calcium oxalate deposition-induced renal fibrosis by inhibiting ferroptosis. Biomed Pharmacother. 2023;164:114925. doi:10.1016/j.biopha.2023.114925
32. Jimenez-Gutierrez GE, Martínez-Gómez LE, Martínez-Armenta C, Pineda C, Martínez-Nava GA, Lopez-Reyes A. Molecular mechanisms of inflammation in sarcopenia: diagnosis and therapeutic update. Cells. 2022;11(15). doi:10.3390/cells11152359
33. Zhang HJ, Wang BH, Wang X, et al. Handelin alleviates cachexia- and aging-induced skeletal muscle atrophy by improving protein homeostasis and inhibiting inflammation. J Cachexia, Sarcopenia Muscle. 2024;15(1):173–188. doi:10.1002/jcsm.13381
34. Wang K, Liu Q, Tang M, et al. Chronic kidney disease-induced muscle atrophy: molecular mechanisms and promising therapies. Biochem Pharmacol. 2023;208:115407. doi:10.1016/j.bcp.2022.115407
35. Lovegrove CE, Bešević J, Wiberg A, et al. Central adiposity increases risk of kidney stone disease through effects on serum calcium concentrations. J Am Soc Nephrol. 2023;34(12):1991–2011. doi:10.1681/asn.0000000000000238
36. Liu M, Wu J, Gao M, et al. Lifestyle factors, serum parameters, metabolic comorbidities, and the risk of kidney stones: a Mendelian randomization study. Front Endocrinol. 2023;14:1240171. doi:10.3389/fendo.2023.1240171
37. Lisco G, Disoteo OE, De Tullio A, et al. Sarcopenia and Diabetes: a Detrimental Liaison of Advancing Age. Nutrients. 2023;16(1). doi:10.3390/nu16010063
38. Lopez-Pedrosa JM, Camprubi-Robles M, Guzman-Rolo G, et al. The vicious cycle of type 2 diabetes mellitus and skeletal muscle atrophy: clinical, biochemical, and nutritional bases. Nutrients. 2024;16(1). doi:10.3390/nu16010172
39. Jun L, Robinson M, Geetha T, Broderick TL, Babu JR. Prevalence and mechanisms of skeletal muscle atrophy in metabolic conditions. Int J Mol Sci. 2023;24(3). doi:10.3390/ijms24032973
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Physical Activity Mediates the Relationship Between Sarcopenia and Cognitive Function Among Older Adults in Nursing Homes
Yao X, Liu B, Hua N, Huang J, Zhao X
Clinical Interventions in Aging 2023, 18:1863-1871
Published Date: 13 November 2023
Imaging of Sarcopenia in Type 2 Diabetes Mellitus
Wang D, Zhang G, Yu Y, Zhang Z
Clinical Interventions in Aging 2024, 19:141-151
Published Date: 26 January 2024
Four-Step Co-Designing of the Reablement Strategies Targeting Sarcopenia (ReStart-S): An Exercise-Based Multicomponent Program for Older Adults Residing in Long-Term Care Settings
Kumar P, Umakanth S, Marzetti E, Kalra S, N G
Journal of Multidisciplinary Healthcare 2024, 17:1415-1433
Published Date: 28 March 2024
Interprofessional Management of (Risk of) Malnutrition and Sarcopenia: A Grounded Theory Study from the Perspective of Professionals
Boxum SD, van Exter SH, Reinders JJ, Koenders N, Drenth H, van den Berg MGA, Tieland M, Spoorenberg SLW, Finnema EJ, van der Wees PJ, Jager-Wittenaar H
Journal of Multidisciplinary Healthcare 2024, 17:4677-4692
Published Date: 9 October 2024
Semaglutide Therapy and Accelerated Sarcopenia in Older Adults with Type 2 Diabetes: A 24-Month Retrospective Cohort Study
Ren Q, Zhi L, Liu H
Drug Design, Development and Therapy 2025, 19:5645-5652
Published Date: 3 July 2025