Back to Journals » Clinical Interventions in Aging » Volume 17
Coexisting Frailty and Cognitive Impairment as a Predictor of Adverse Outcomes in Older Inpatients After Discharge: Results from a One-Year Follow-Up Study
Authors Zeng XK ![]() , Shen SS, Guan HL, Chen LY, Chen XJ
, Shen SS, Guan HL, Chen LY, Chen XJ
Received 5 July 2022
Accepted for publication 17 November 2022
Published 29 November 2022 Volume 2022:17 Pages 1697—1706
DOI https://doi.org/10.2147/CIA.S376691
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Xing-Kun Zeng,* Shan-Shan Shen,* Hui-Lan Guan, Ling-Yan Chen, Xu-Jiao Chen
Department of Geriatrics, Zhejiang Hospital, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xu-Jiao Chen, Department of Geriatrics, Zhejiang Hospital, Lingyin Road #12, Hangzhou, 310013, People’s Republic of China, Tel +86 180 6989 7567, Fax +86 571 8798 5100, Email [email protected]
Purpose: This study aimed to investigate the combined effects of frailty and cognitive impairment on adverse outcomes, including new falls and new activities of daily living (ADL) dependency over a 1-year follow-up.
Patients and Methods: A total of 311 older hospitalized patients participated in this retrospective observational study and completed a 1-year follow-up. Frailty was assessed by the Clinical Frailty Scale (CFS). Cognitive function was evaluated by the Mini-Mental State Examination (MMSE). All participants were classified into four groups: 1) the healthy group (n=180); 2) the cognitive impairment group only (n=38); 3) the frailty group only (n=44); and 4) coexisting frailty and cognitive impairment group (n=49). The follow-up data of adverse outcomes include the incidences of new falls and new ADL dependence. Binary logistic regression analysis was used to explore the associations of frailty and/or cognitive impairment with adverse outcomes.
Results: The prevalence rates of frailty, cognitive impairment, and co-occurring frailty with cognitive impairment were 29.9%, 28%, and 15.8%, respectively. Among these four groups, there was a statistical difference in the incidence of new ADL dependence during the follow-up period (9.5% vs 11.4% vs 35.9% vs 61.9%, P < 0.001). After adjusting the confounding variables, older hospitalized patients with frailty and cognitive impairment had a higher risk of new ADL dependence when compared with the healthy group (OR: 4.786, 95% CI: 1.492– 15.355), but frailty only or cognitive impairment only was not associated with new ADL dependency.
Conclusion: Elderly inpatients with comorbid frailty and cognitive impairment on admission were significantly associated with an increased risk of new ADL dependency 1 year after discharge. Therefore, it is necessary for the early identification of frailty and cognitive impairment, and effective interventions should be implemented.
Keywords: cognitive impairment, frailty, older adults, ADL dependency, fall
Introduction
With the accelerated aging of the population, older adults are accompanied by multi-symptoms, such as frailty and cognitive impairment, which predict adverse outcomes. Research shows that the prevalence of inpatients with frailty and cognitive impairment has increased rapidly.1–3 The reported prevalence of frailty and cognitive impairment in hospitalized elderly patients were 43.9% and 36.6%, respectively,4,5 which were higher than the prevalence in the community.6,7 Disability during hospitalization ranges from 5% to 50%,8–10 and it continues to appear and even worsens after discharge.8,11,12 Except for disability, hospitalization itself also contributes to frailty and cognitive impairment.13–15
Frailty and cognitive impairment often coexist among older patients, and the cumulative effect on health is more pronounced when both occur.16–19 A recent study pointed out that co-existing frailty and cognitive impairment were associated with poorer health-related quality of life than either symptom existing alone.20 Allan et al found that this multiplicative effect reduced parts of IADL functions (primarily shopping and telephone use) and increased the risk of hospitalization.21 Similarly, a prospective cohort study showed that frailty and cognitive impairment were independent predictors of ADL dependency. Yet, both conditions had a higher risk of ADL dependency compared with either alone.17 In addition, another study indicated that cognitive impairment or physical frailty was associated with the risk of falls.22,23 ADL dependency and the high risk of falls are associated with increased morbidity and mortality in elderly patients; it has a significant societal impact in terms of deteriorating quality of life and increased medical costs. Therefore, it is essential to investigate risk factors related to ADL dependence and the high risk of falls to formulate interventions. Most of the evidence came from community-based older populations; little evidence was found from older adults in hospitals.17,24,25
Frailty and cognitive function screening in hospital settings require simpler and more effective tools to improve the accessibility of clinical risk stratification. The Fried frailty phenotype (FP) and Rockwood’s frailty index (FI) were widely used in current clinical studies.26,27 However, in the practical methodological evaluation of the FP, data on walking speed and self-reported activity levels are difficult to be collected due to acute events or multiple comorbidities in older patients. The FI includes multidimensional accumulation deficits, such as biological aspects, mood, cognition, nutrition, and social support, but it cannot be used to distinguish frailty from disability and comorbidity. Furthermore, the cumbersome and time-consuming process of evaluation itself also limited the clinical application. The Clinical Frailty Scale (CFS) is a feasible frailty assessment tool for older hospitalized patients, based on the clinician’s judgment in terms of mobility and independent ability in daily living.28–30 CFS is reported to be strongly associated with the frailty index and predicts adverse outcomes for elderly inpatients.28,30 A prospective cohort study from China has used the FP, the CFS, and the Frail Scale (FS) to assess the frailty status of elderly hospitalized patients. This study found that the CFS was more valuable in predicting mortality risk than those two other assessment tools.31 The Mini-Mental State Examination (MMSE) instrument was broadly used to assess cognitive function. Previous studies demonstrated that it could be reliably administered in the clinical setting and highlighted the test’s value in identifying cognitive impairment in older adults.32–34
In this study, CFS and MMSE were used to screen elderly inpatients for frailty and cognitive impairment on admission. We hypothesized that older hospitalized patients with both frailty and cognitive impairment were at higher risk of adverse outcomes, which included new falls and new ADL dependency, than those with frailty alone or cognitive impairment alone in 1-year follow-up after discharge.
Materials and Methods
Study Subjects
A retrospective observational study with 1-year follow-up for older hospitalized patients was conducted by Zhejiang Hospital of China. We enrolled 572 patients aged 60 years or older from October 2014 to July 2018, and the 1-year follow-up data collection ended in July 2019. The inclusion criteria for the study were age ≥60 years, ability to communicate in Chinese and write informed consent, self-reported vision and hearing status sufficient for compliance with cognitive and frailty assessments. Participants with psychiatric diseases (eg, delirium, dementia), acute medical events (eg, acute infection, acute cerebrovascular and cardiovascular diseases), severe acoustical and visual decline, long-term hospitalization, active malignancy, or terminal illness were excluded from this study. Patients and their family members were informed of the survey’s aim and detailed process when they visited the Department of Geriatrics. After obtaining their informed consent, they were interviewed by a trained researcher, and another researcher analyzed the data. This study was approved by the medical ethics committees of Zhejiang Hospital, and all the participants offered written informed consent to use their clinical records. The design of the study and conducted procedures conformed to the ethical principles of the Helsinki Declaration.
Baseline Assessment
Trained and experienced investigators performed data collection. The investigator at follow-up was blinded to the baseline data and conducted telephone calls or face-to-face interviews using the standard protocol.
Socio-demographic characteristics and clinical information were collected, including gender, age, marital status, body mass index (BMI), education, lifestyle factors (eg, alcohol intake, smoking), prescription drug use, and medical history. BMI was calculated using body weight divided by height squared (kg/m2). Patients with five or more kinds of chronic diseases were considered as comorbidities. Polypharmacy was defined as patients who took no less than five oral prescription drugs.36,37 We conducted a baseline assessment of frailty status, cognitive function, and activities of daily living (ADL) at admission.
Classification of the Groups
Frailty criteria: The CFS was used to assess frailty and conducted by an experienced assessor.
The CFS is mainly graded by clinicians based on the comprehensive assessment of the functional status and disease degree of the elderly, and it was divided into nine grades (1, very fit; 2, well; 3, managing well; 4, vulnerable; 5, mildly frail; 6, moderately frail; 7, severely frail; 8, very severely frail; 9, terminally ill). The patient who scored ≥5 was defined as frailty.28,38
Cognitive impairment: Cognitive function was assessed by the MMSE. The score ranges from 0 to 30. Patients with a score ≤ 24 were considered as having cognitive impairment.39
According to the frailty and cognitive impairment criteria, all participants were classified into four groups: 1) the healthy group; 2) the cognitive impairment group only; 3) the frailty group only; and 4) coexisting frailty and cognitive impairment group.
ADL Assessment
We assessed ADL by using questionnaires of the Barthel Index.40 The patient was asked to answer 10 questions, including feeding, personal toilet, controlling bowels and bladder, moving from chair to bed and return bathing, dressing, walking, using the toilet, ascending and descending stairs for which they needed assistance, each ADL item was scored based on the extent to which older adults completed each task independently. The higher score indicated the better ADL independence.
Adverse Outcomes Assessment
The follow-up data of adverse outcomes, including new falls and new ADL dependency, were recorded. Fall was defined as an unexplained non-accidental change of physical position resulting in rest on the lower plane.41 The patient was asked to answer the question, “Did you ever fall during the last year? The number of falls, reasons, and consequences were recorded. New falls were defined as falls that occurred during 1-year follow-up, and new ADL dependency was defined as an at least five-point drop in ADL score in hospitalized elderly patients 1 year after discharge.
Statistical Analysis
All statistical analyses were conducted using the SPSS version (Statistical Package for the Social Sciences, Chicago, IL, USA) 22.0 software. Continuous variables with a normal distribution were compared by using the unpaired t-test (for a report as mean ± standard deviation (mean ± SD)), the Mann–Whitney U-Test for the data without a normal distribution (for a report as the median and interquartile range (IQR)). Categorical variables were reported as a percentage or constituent ratio by using the chi-square test or Fisher’s exact test. Binary logistic regression analysis was performed to explore the associations of frailty and/or cognitive impairment with adverse outcomes; odds ratios (ORs) and 95% confidence intervals (CIs) were reported for a significant relationship. All statistical analyses were two-tailed, and P-values <0.05 was assumed statistically significant.
Results
A total of 572 older hospitalized patients agreed to participate in this study. Twenty-two patients were excluded due to dementia, 39 patients were excluded as a result of long-term hospitalization, and 10 patients were not included for some serious medical conditions, 182 patients were excluded due to loss to follow-up, and 8 patients were excluded due to incomplete data on MMSE. All the remaining 311 cases were recruited for the study. Figure 1 shows the procedure for selecting patients.
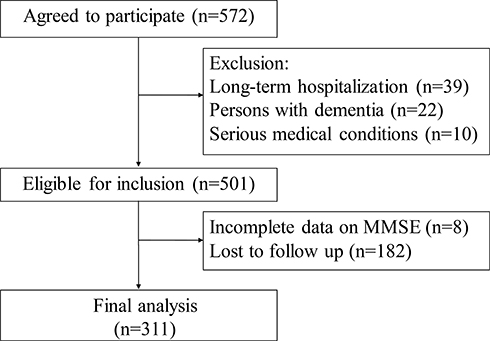 |
Figure 1 The procedure of patient selection. Abbreviation: MMSE, Mini-Mental State Examination. |
Clinical characteristics and demographic of all these older hospitalized patients by the presence of frailty and/or cognitive impairment are summarized in Table 1. Among all the participants, the prevalence of frailty, cognitive impairment, and co-occurring frailty with cognitive impairment was 29.9%, 28%, and 15.8%, respectively, while the prevalence of them increased with age advancing (Figure 2). Significant differences were observed among the four groups concerning comorbidities such as diabetes mellitus, cardiovascular disease, cerebrovascular disease, and osteoporosis, and baseline ADL score at admission (all P <0.05). Among these four groups, there was a statistical difference in the incidence of new ADL dependency during the follow-up period (9.5% vs 11.4% vs 35.9% vs 61.9%, P <0.001, Figure 3). The presence of frailty or/and cognitive impairment was not correlated with new falls in hospitalized older patients after the 1-year follow-up (10.1% vs 5.7% vs 12.8% vs 23.8%, P>0.05, Figure 3).
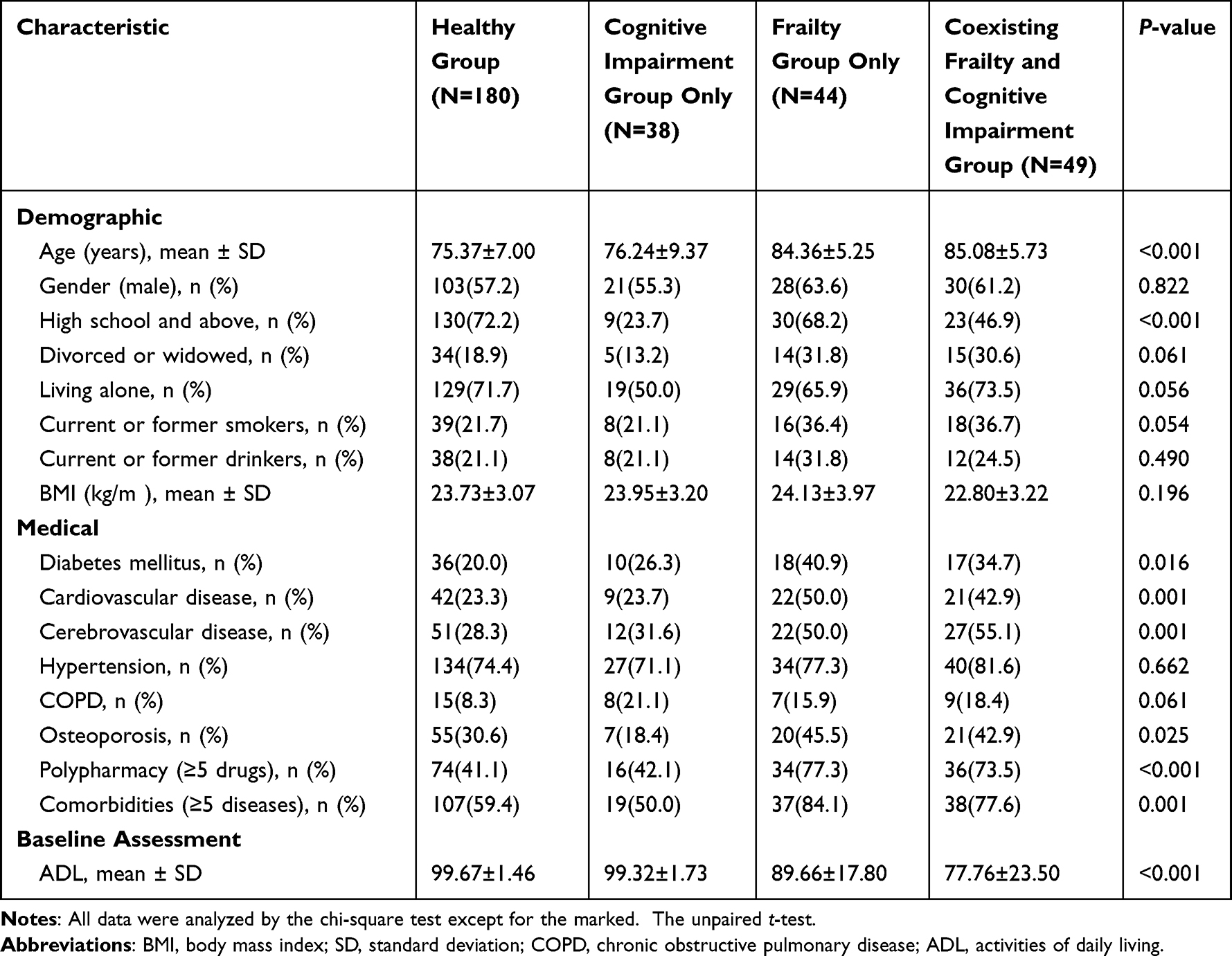 |
Table 1 Baseline Characteristics of Patients by the Presence of Cognitive Impairment and/or Frailty |
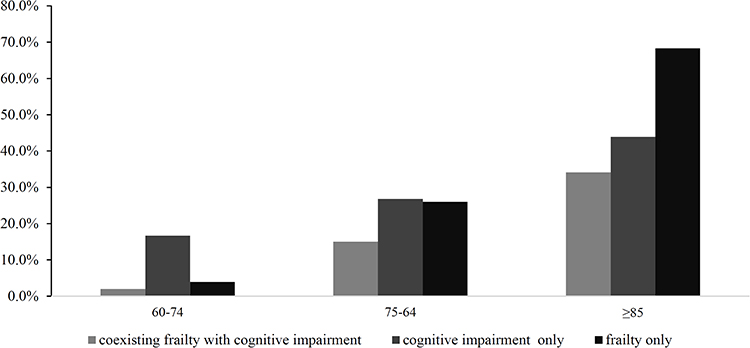 |
Figure 2 Prevalence and trend of coexisting frailty with cognitive impairment, cognitive impairment only, and frailty only by age. |
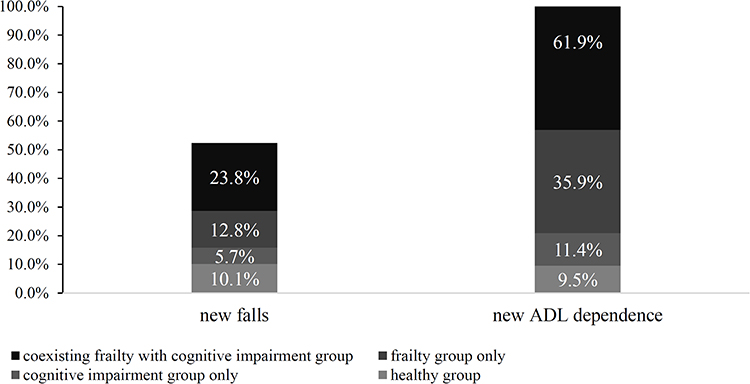 |
Figure 3 Adverse outcomes of inpatients by the presence of cognitive impairment and/or frailty. Abbreviation: ADL, activities of daily living. Note: All data were analyzed by the chi-square test except for the marked. |
Table 2 presents the results of the binary logistic regression analysis on adverse outcomes by the presence of frailty and/or cognitive impairment. After adjusting for age, sex, and education, model 1 showed that older hospitalized patients with frailty and cognitive impairment had a higher risk of new ADL dependency than healthy patients (OR: 7.403, 95% CI: 3.022–18.132). In model 2, after the adjustment of confounders in model 1, polypharmacy and comorbidities, a significant association was found between new ADL dependency and co-occurring frailty with cognitive impairment (OR: 9.138, 95% CI: 3.391–24.623). The fully adjusted Model 3, the result remained unchanged (OR: 4.786, 95% CI: 1.492–15.355). However, no significant associations were observed in new ADL dependency between the healthy individuals and those with cognitive impairment only or frailty only. Meanwhile, no significant differences were found between new falls and the presence of frailty and/or cognitive impairment in older hospitalized patients.
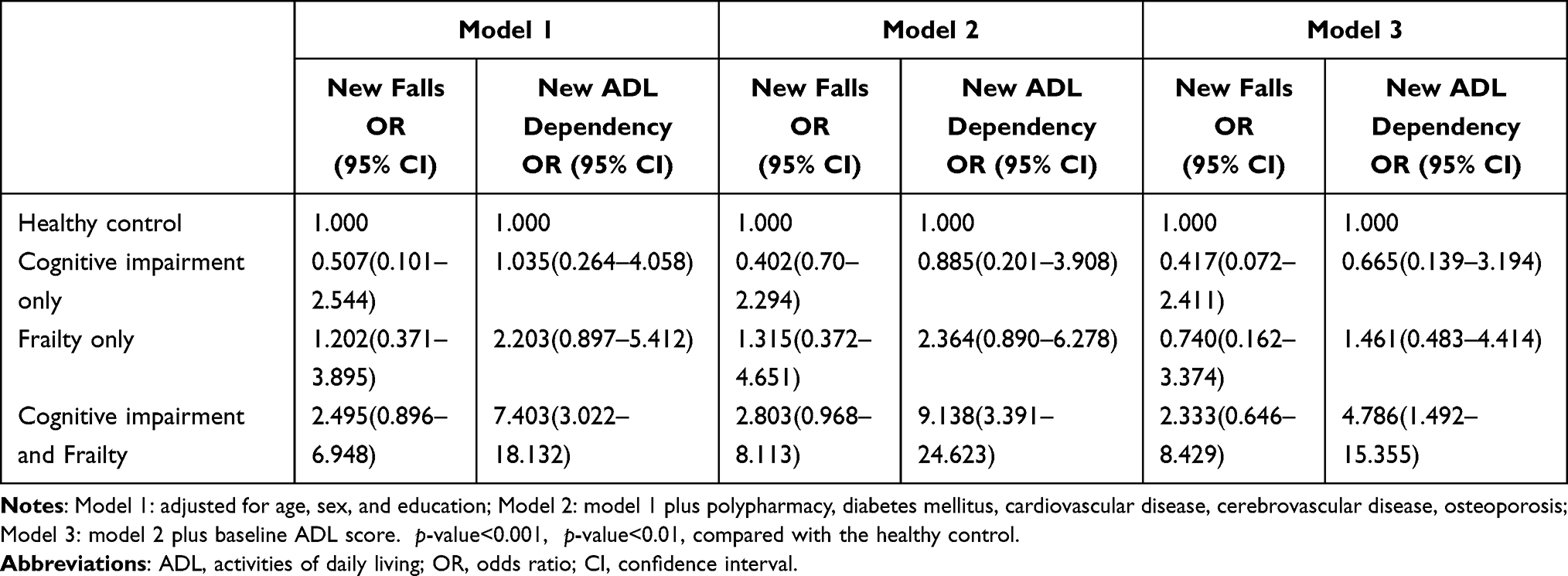 |
Table 2 Associations of Cognitive Impairment and/or Frailty and Adverse Outcomes Over 1-Year Follow-Up Using Binary Logistic Regression Model |
Discussion
In this study, we identified that older inpatients with comorbid frailty and cognitive impairment on admission were significantly associated with an increased risk of new ADL dependency 1 year after discharge, and the result remained unchanged after adjusting for covariates. Our research showed that the study of comorbid frailty and cognitive impairment of elderly hospitalized patients might help us get great predictive value for the new ADL dependency after discharge.
Our data demonstrated that the risk of new ADL dependency was the highest in older hospitalized patients suffering from both frailty and cognitive impairment. This was in line with the Brazilian study using different assessment methods to screen for frailty and cognitive impairment, which revealed that frailty and cognitive impairment in the elderly increased the risk of ADL dependency.25 Moreover, another prospective cohort study showed that the combined effects of frailty with cognitive impairment were associated with a higher risk of ADL dependency than either frailty alone or cognitive impairment alone.12 The mechanisms underlying the cumulative impact of frailty and cognitive impairment on adverse outcomes may come from similar pathophysiologies, such as age-related degeneration of frontal lobe structures, including gray matter loss, white matter lesions, reduced dopaminergic activity, and dendritic branching. Several studies have indicated that the pathogenesis mechanisms involved in frailty were also prone to promote cognitive impairment, including oxidative stress, chronic inflammation, and insulin resistance.43–46 Other clinical comorbidities, such as atherosclerosis, diabetes, heart failure, and hypertension, may increase the risk of frailty and cognitive impairment as well. In other researches, older age, depression, social participation, sedentary lifestyle, and sleep problems had been identified as critical contributors to the co-occurrence of physical frailty and cognitive impairment.48 Both conditions were multifactorial and interactional, boosting their negative cumulative effect.
Regarding the association between different frailty-cognitive impairment groups and the risk of new falls, we found that inpatients with coexisting frailty and cognitive impairment had a higher odds ratio for new falls than those with neither symptoms or either symptom. However, there were no significant associations in our samples. We all know that falls in the older population are closely related to functional decline, especially the balance function. Cognitive impairment increases the risk of falling in older adults with impaired balance function, slow walking speed, and muscle weakness. Different from our study, a study from the National Health and Aging Trends Study (NHATS), including 6000 older adults in community or non-nursing home residential care settings, had found that physical frailty, with or without cognitive impairment, was all associated with recurrent falls, which were independent of disease burden, obesity, and mobility limitation.23 This discrepancy may come from the different sizes and the different characteristics of the samples in diverse designs.
ADL dependency is prevalent among older hospitalized patients who are seriously impacted by physical frailty and cognitive impairment.49,50 Our research found that 61.9% of the inpatients with concomitant frailty and cognitive impairment experienced new ADL dependency after discharge. Old patients with new ADL dependency were associated with reduced quality of life, poorer physical performance, and higher risk of mortality.51–53 A longitudinal study from Italian showed that the earlier identification of frailty and cognitive impairment, the more likely it was to be reversed.54 Frailty, cognitive impairment, independence, and comorbidities all influence treatment decision-makings, especially in older (≥65 years) patients and very older (≥85 years) patients. Recently, frailty and cognitive impairment have been written into some age-related disease guidelines and expert consensus to guide risk stratification and clinical management.55,56 Early rehabilitation programs can reverse hospitalization-associated disabilities. A randomized clinical trial showed that inpatients who received exercise intervention had a mean increase of 2.2 points on the SPPB scale, 6.9 points on the Barthel Index, and 1.8 points on the cognitive level at discharge than those who were in the usual hospital care group.57 Another research conducted in a nursing home showed that residents who participated in a daily routine of inertial training got lower risks of falls and better independence through improvements in muscle strength, gait speed, and balance.58 As stated above, by targeting the reversible risk factors and comorbidities and improving the intrinsic capacity, we could effectively delay or even reverse frailty and cognitive impairment, which may lead to better life expectancies and life qualities of the elders.59–62 Further study is required to investigate the early identification of frailty and cognitive impairment in hospitalized older patients may help decrease adverse outcomes and formulate effective interventions.
Compared to previous literature, our study has the following advantages. First, our data were collected by a well-trained team that had been conducting a comprehensive geriatric assessment (CGA), a multidimensional diagnostic assessment including physical performance, cognition, sarcopenia, and frailty of elderly individuals. All the assessments were conducted through professional software systems. Therefore, the consistency and validity of the evaluation are well guaranteed. Information from CGA was entirely used to identify the high-risk inpatients of developing functional decline. Second, our research showed that comorbid frailty and cognitive impairment could generate greater detrimental effects on the risk of post-discharge ADL dependency among the elderly in China. Thirdly, our finding highlighted that it was much necessary to implant the multidisciplinary team intervention in hospitalized elderly patients into the medical model – especially for the inpatients with multiple geriatric syndromes, which may help prevent and reverse the deterioration of physical and mental function and mitigate the risk of adverse outcome. There are some limitations in this study as well. One shortage was that we failed to assess the inpatient’s cognitive functions and frailty within 1 year after discharge. Another was the follow-up time after release, which was not long enough. Thus, the effects of other factors on new falls and new ADL dependency may be covered up. To explore the causal relationship and formulate early interventions, which help decrease the adverse outcomes among older inpatients, we are supposed to enlarge samples in further multicenter studies.
Conclusion
Elderly inpatients with comorbid frailty and cognitive impairment on admission were significantly associated with an increased risk of new ADL dependency 1 year after discharge. The early identification of frailty and cognitive impairment in hospitalized older patients may be helpful in practice guidelines of risk stratification and timely preventive interventions.
Acknowledgments
We sincerely thank the staff from the geriatric department of Zhejiang Hospital for their positive involvement in this study.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funds from China National Key R&D Program (Grant number: 2020YFC2008606), the Zhejiang Medical Science and Techology Project (Grant number: 2019KY262), innovation disciplines of Zhejiang Province, the National Health and Family Planning Commission of Scientific Research Fund of People’s Republic of China (Grant number: WKJ2013-2-001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hanlon P, Nicholl BI, Jani BD, et al. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: a prospective analysis of 493 737 UK biobank participants. Lancet Public Health. 2018;3(7):e323–e332. doi:10.1016/S2468-2667(18)30091-4
2. Panza F, Seripa D, Solfrizzi V, et al. Targeting cognitive frailty: clinical and neurobiological roadmap for a single complex phenotype. J Alzheimers Dis. 2015;47(4):793–813. doi:10.3233/JAD-150358
3. Martin Prince MG, Ali G-C, Wimo A. World Alzheimer Report 2015. London: Alzheimer’s Disease International (ADI); 2015.
4. Buurman BM, Hoogerduijn JG, van Gemert EA, et al. Clinical characteristics and outcomes of hospitalized older patients with distinct risk profiles for functional decline: a prospective cohort study. PLoS One. 2012;7(1):e29621. doi:10.1371/journal.pone.0029621
5. Lu C, Zhang H, Fu X, et al. Clinical investigation and analysis of chronic diseases and geriatric syndromes in elderly inpatients. Chin J Geriatr. 2019;38(8):913–916. doi:10.3760/cma.j.issn.0254-9026.2019.08.021
6. Lin CC, Li CI, Chang CK, et al. Reduced health-related quality of life in elders with frailty: a cross-sectional study of community-dwelling elders in Taiwan. PLoS One. 2011;6(7):e21841. doi:10.1371/journal.pone.0021841
7. Wu MS, Lan TH, Chen CM, et al. Socio-demographic and health-related factors associated with cognitive impairment in the elderly in Taiwan. BMC Public Health. 2011;11:22. doi:10.1186/1471-2458-11-22
8. Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56(12):2171–2179. doi:10.1111/j.1532-5415.2008.02023.x
9. Buurman BM, Hoogerduijn JG, de Haan RJ, et al. Geriatric conditions in acutely hospitalized older patients: prevalence and one-year survival and functional decline. PLoS One. 2011;6(11):e26951. doi:10.1371/journal.pone.0026951
10. Hoogerduijn JG, Buurman BM, Korevaar JC, et al. The prediction of functional decline in older hospitalised patients. Age Ageing. 2012;41(3):381–387. doi:10.1093/ageing/afs015
11. Gill TM, Allore HG, Gahbauer EA, et al. Change in disability after hospitalization or restricted activity in older persons. JAMA. 2010;304(17):1919–1928. doi:10.1001/jama.2010.1568
12. Brown CJ, Redden DT, Flood KL, et al. The underrecognized epidemic of low mobility during hospitalization of older adults. J Am Geriatr Soc. 2009;57(9):1660–1665. doi:10.1111/j.1532-5415.2009.02393.x
13. Gill TM, Gahbauer EA, Han L, et al. The role of intervening hospital admissions on trajectories of disability in the last year of life: prospective cohort study of older people. BMJ. 2015;350(may14 20):h2361. doi:10.1136/bmj.h2361
14. Ida S, Kaneko R, Imataka K, et al. Relationship between frailty and mortality, hospitalization, and cardiovascular diseases in diabetes: a systematic review and meta-analysis. Cardiovasc Diabetol. 2019;18(1):81. doi:10.1186/s12933-019-0885-2
15. Ehlenbach WJ, Hough CL, Crane PK, et al. Association between acute care and critical illness hospitalization and cognitive function in older adults. JAMA. 2010;303(8):763–770. doi:10.1001/jama.2010.167
16. Lee Y, Kim J, Chon D, et al. The effects of frailty and cognitive impairment on 3-year mortality in older adults. Maturitas. 2018;107:50–55. doi:10.1016/j.maturitas.2017.10.006
17. Aliberti MJR, Cenzer IS, Smith AK, et al. Assessing risk for adverse outcomes in older adults: the need to include both physical frailty and cognition. J Am Geriatr Soc. 2019;67(3):477–483. doi:10.1111/jgs.15683
18. St John PD, Tyas SL, Griffith LE, et al. The cumulative effect of frailty and cognition on mortality - results of a prospective cohort study. Int Psychogeriatr. 2017;29(4):535–543. doi:10.1017/S1041610216002088
19. Liu Z, Han L, Gahbauer EA, et al. Joint trajectories of cognition and frailty and associated burden of patient-reported outcomes. J Am Med Dir Assoc. 2018;19(4):304–309 e302. doi:10.1016/j.jamda.2017.10.010
20. Li CL, Chang HY, Stanaway FF. Combined effects of frailty status and cognitive impairment on health-related quality of life among community dwelling older adults. Arch Gerontol Geriatr. 2020;87:103999. doi:10.1016/j.archger.2019.103999
21. Brigola AG, Ottaviani AC, Alexandre TDS, et al. Cumulative effects of cognitive impairment and frailty on functional decline, falls and hospitalization: a four-year follow-up study with older adults. Arch Gerontol Geriatr. 2020;87:104005. doi:10.1016/j.archger.2019.104005
22. Naharci MI, Tasci I. Frailty status and increased risk for falls: the role of anticholinergic burden. Arch Gerontol Geriatr. 2020;90:104136. doi:10.1016/j.archger.2020.104136
23. Ge ML, Simonsick EM, Dong BR, et al. Frailty, with or without cognitive impairment, is a strong predictor of recurrent falls in a US population-representative sample of older adults. J Gerontol a Biol Sci Med Sci. 2021;76(11):e354–e360. doi:10.1093/gerona/glab083
24. Montero-Odasso MM, Barnes B, Speechley M, et al. Disentangling cognitive-frailty: results from the gait and brain study. J Gerontol a Biol Sci Med Sci. 2016;71(11):1476–1482. doi:10.1093/gerona/glw044
25. Aprahamian I, Suemoto CK, Aliberti MJR, et al. Frailty and cognitive status evaluation can better predict mortality in older adults? Arch Gerontol Geriatr. 2018;77:51–56. doi:10.1016/j.archger.2018.04.005
26. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.M146
27. Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. Sci World J. 2001;1:323–336. doi:10.1100/tsw.2001.58
28. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489–495. doi:10.1503/cmaj.050051
29. Church S, Rogers E, Rockwood K, et al. A scoping review of the clinical frailty scale. BMC Geriatr. 2020;20(1):393. doi:10.1186/s12877-020-01801-7
30. Wallis SJ, Wall J, Biram RW, et al. Association of the clinical frailty scale with hospital outcomes. QJM. 2015;108(12):943–949. doi:10.1093/qjmed/hcv066
31. Fu L, Wang Q, Lv W, et al. Comparison of predictability on adverse events among different assessment tools in elderly discharged inpatients. Chin J Geriatr. 2019;38(12):1329–1333. doi:10.3760/cma.j.issn.0254-9026.2019.12.003
32. Mystakidou K, Tsilika E, Parpa E, et al. Brief cognitive assessment of cancer patients: evaluation of the Mini-Mental State Examination (MMSE) psychometric properties. Psychooncology. 2007;16(4):352–357. doi:10.1002/pon.1090
33. Fountoulakis KN, Tsolaki M, Chantzi H, et al. Mini Mental State Examination (MMSE): a validation study in Greece. Am J Alzheimers Dis Other Demen. 2000;15(6):342–345. doi:10.1177/153331750001500604
34. Li H, Jia J, Yang Z, Moreau N. Mini-mental state examination in elderly Chinese: a population-based normative study. J Alzheimers Dis. 2016;53(2):487–496. doi:10.3233/JAD-160119
35. Salive ME. Multimorbidity in older adults. Epidemiol Rev. 2013;35(1):75–83. doi:10.1093/epirev/mxs009
36. Viktil KK, Blix HS, Moger TA, et al. Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br J Clin Pharmacol. 2007;63(2):187–195. doi:10.1111/j.1365-2125.2006.02744.x
37. Masnoon N, Shakib S, Kalisch-Ellett L, et al. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17(1):230. doi:10.1186/s12877-017-0621-2
38. Kahlon S, Pederson J, Majumdar SR, et al. Association between frailty and 30-day outcomes after discharge from hospital. CMAJ. 2015;187(11):799–804. doi:10.1503/cmaj.150100
39. Folstein MF, Folstein SE, McHugh PR. ”Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
40. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65.
41. Lamb SE, Jorstad-Stein EC, Hauer K, et al. Development of a common outcome data set for fall injury prevention trials: the prevention of falls network Europe consensus. J Am Geriatr Soc. 2005;53(9):1618–1622. doi:10.1111/j.1532-5415.2005.53455.x
42. Yogev-Seligmann G, Hausdorff JM, Giladi N. The role of executive function and attention in gait. Mov Disord. 2008;23(3):329–342; quiz 472. doi:10.1002/mds.21720
43. Panza F, Solfrizzi V, Frisardi V, et al. Different models of frailty in predementia and dementia syndromes. J Nutr Health Aging. 2011;15(8):711–719. doi:10.1007/s12603-011-0126-1
44. Buchman AS, Bennett DA. Cognitive frailty. J Nutr Health Aging. 2013;17(9):738–739. doi:10.1007/s12603-013-0397-9
45. Halil M, Cemal Kizilarslanoglu M, Emin Kuyumcu M, et al. Cognitive aspects of frailty: mechanisms behind the link between frailty and cognitive impairment. J Nutr Health Aging. 2015;19(3):276–283. doi:10.1007/s12603-014-0535-z
46. Mulero J, Zafrilla P, Martinez-Cacha A. Oxidative stress, frailty and cognitive decline. J Nutr Health Aging. 2011;15(9):756–760. doi:10.1007/s12603-011-0130-5
47. Afilalo J, Karunananthan S, Eisenberg MJ, et al. Role of frailty in patients with cardiovascular disease. Am J Cardiol. 2009;103(11):1616–1621. doi:10.1016/j.amjcard.2009.01.375
48. Xie B, Ma C, Chen Y, et al. Prevalence and risk factors of the co-occurrence of physical frailty and cognitive impairment in Chinese community-dwelling older adults. Health Soc Care Community. 2021;29(1):294–303. doi:10.1111/hsc.13092
49. Peel NM, Alapatt LJ, Jones LV, et al. The association between gait speed and cognitive status in community-dwelling older people: a systematic review and meta-analysis. J Gerontol a Biol Sci Med Sci. 2019;74(6):943–948. doi:10.1093/gerona/gly140
50. Derry HM, Johnston CD, Burchett CO, et al. Gait speed is associated with cognitive function among older adults with HIV. J Aging Health. 2020;32(10):1510–1515. doi:10.1177/0898264320943330
51. Millan-Calenti JC, Tubio J, Pita-Fernandez S, et al. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch Gerontol Geriatr. 2010;50(3):306–310. doi:10.1016/j.archger.2009.04.017
52. DALYs GBD, Collaborators H, Murray CJ, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. Lancet. 2015;386(10009):2145–2191. doi:10.1016/S0140-6736(15)61340-X
53. Bossola M, Marino C, Di Napoli A, et al. Functional impairment and risk of mortality in patients on chronic hemodialysis: results of the Lazio dialysis registry. J Nephrol. 2018;31(4):593–602. doi:10.1007/s40620-018-0484-4
54. Solfrizzi V, Scafato E, Lozupone M, et al. Additive role of a potentially reversible cognitive frailty model and inflammatory state on the risk of disability: the Italian longitudinal study on aging. Am J Geriatr Psychiatry. 2017;25(11):1236–1248. doi:10.1016/j.jagp.2017.05.018
55. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
56. Williams B, Mancia G, Spiering W, et al. 2018 practice guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC task force for the management of arterial hypertension. J Hypertens. 2018;36(12):2284–2309. doi:10.1097/HJH.0000000000001961
57. Martinez-Velilla N, Casas-Herrero A, Zambom-Ferraresi F, et al. Effect of exercise intervention on functional decline in very elderly patients during acute hospitalization: a randomized clinical trial. JAMA Intern Med. 2019;179(1):28–36. doi:10.1001/jamainternmed.2018.4869
58. Naczk M, Marszalek S, Naczk A. Inertial training improves strength, balance, and gait speed in elderly nursing home residents. Clin Interv Aging. 2020;15:177–184. doi:10.2147/CIA.S234299
59. Negm AM, Kennedy CC, Thabane L, et al. Management of frailty: a systematic review and network meta-analysis of randomized controlled trials. J Am Med Dir Assoc. 2019;20(10):1190–1198. doi:10.1016/j.jamda.2019.08.009
60. Veronese N, Stubbs B, Noale M, et al. Adherence to a Mediterranean diet is associated with lower incidence of frailty: a longitudinal cohort study. Clin Nutr. 2018;37(5):1492–1497. doi:10.1016/j.clnu.2017.08.028
61. Ng TP, Ling LHA, Feng L, et al. Cognitive effects of multi-domain interventions among pre-frail and frail community-living older persons: randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2018;73(6):806–812. doi:10.1093/gerona/glx207
62. Romera-Liebana L, Orfila F, Segura JM, et al. Effects of a primary care-based multifactorial intervention on physical and cognitive function in frail, elderly individuals: a randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2018;73(12):1688. doi:10.1093/gerona/glx259
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combined Vision and Hearing Impairment is Associated with Frailty in Older Adults: Results from the West China Health and Aging Trend Study
Zhao Y, Ding Q, Lin T, Shu X, Xie D, Gao L, Yue J
Clinical Interventions in Aging 2022, 17:675-683
Published Date: 2 May 2022
Intrinsic Capacity Declines with Elevated Homocysteine in Community-Dwelling Chinese Older Adults
Lin S, Wang F, Zheng J, Yuan Y, Huang F, Zhu P
Clinical Interventions in Aging 2022, 17:1057-1068
Published Date: 7 July 2022
An Easy-to-Implement Clinical-Trial Frailty Index Based on Accumulation of Deficits: Validation in Zoster Vaccine Clinical Trials

Andrew MK, Matthews S, Kim JH, Riley ME, Curran D
Clinical Interventions in Aging 2022, 17:1261-1274
Published Date: 19 August 2022
Relationship Between Physical Exercise and Cognitive Impairment Among Older Adults with Type 2 Diabetes: Chain Mediating Roles of Sleep Quality and Depression
Zhang H, Zhang Y, Sheng S, Xing Y, Mou Z, Zhang Y, Shi Z, Yu Z, Gao Q, Cai W, Jing Q
Psychology Research and Behavior Management 2023, 16:817-828
Published Date: 17 March 2023
Recognition and Management of Hospital-Acquired Sepsis Among Older General Medical Inpatients: A Multi-Site Retrospective Study
Barker N, Scott IA, Seaton R, Mehta N, Kalke VR, Redpath L
International Journal of General Medicine 2023, 16:1039-1046
Published Date: 21 March 2023