Back to Journals » Drug Design, Development and Therapy » Volume 20
Association Between Perioperative Dexmedetomidine Exposure and Post-Transplant Renal Outcomes: A Retrospective Analysis
Authors Hung KC ![]() , Yu TS, Ho CN, Yu CH, Lai YC, Chang YJ, Chen IW
, Yu TS, Ho CN, Yu CH, Lai YC, Chang YJ, Chen IW ![]()
Received 16 November 2025
Accepted for publication 16 February 2026
Published 25 February 2026 Volume 2026:20 581944
DOI https://doi.org/10.2147/DDDT.S581944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Tamer Ibrahim
Kuo-Chuan Hung,1,2 Ting-Sian Yu,3 Chun-Ning Ho,1,2 Chia-Hung Yu,1 Yi-Chen Lai,1,2 Ying-Jen Chang,1 I-Wen Chen4
1Department of Anesthesiology, Chi Mei Medical Center, Tainan City, Taiwan; 2School of Medicine, College of Medicine, National Sun Yat-sen University, Kaohsiung, Taiwan; 3Department of Anesthesiology, E-Da Hospital, I-Shou University, Kaohsiung City, Taiwan; 4Department of Anesthesiology, Chi Mei Medical Center, Liouying, Tainan City, Taiwan
Correspondence: I-Wen Chen, Department of Anesthesiology, Chi Mei Medical Center, Liouying, Tainan City, Taiwan, Tel +886 6 281 2811, Fax +886 6 283 3806, Email [email protected]
Purpose: Delayed graft function remains a significant complication of kidney transplantation and affects outcomes and healthcare costs. This investigation examined the associations between perioperative dexmedetomidine exposure and postoperative outcomes in kidney transplant recipients.
Methods: This retrospective cohort study analyzed data from the TriNetX Research Network of patients who underwent kidney transplantation between January 2014 and December 2024. Adult recipients were stratified according to intraoperative dexmedetomidine exposure. The primary outcome was delayed graft function within seven days post-transplantation. Secondary outcomes included acute rejection, graft failure, infection, mortality, and an estimated glomerular filtration rate (eGFR)< 45 mL/min/1.73 m2 across multiple time intervals.
Results: Following propensity score matching, 3,366 patients were included in each cohort. Dexmedetomidine exposure was associated with a lower incidence of delayed graft function at seven days (22.0% versus 24.7%; odds ratio [OR] 0.86, 95% confidence interval [CI] 0.77– 0.96, p=0.009). More pronounced associations emerged for acute rejection (1.2% vs 3.5%; OR 0.34, 95% CI 0.24– 0.48, p< 0.001) and graft failure (1.6% vs 3.8%; OR 0.42, 95% CI 0.30– 0.57, p< 0.001). These associations persisted through 30 days postoperatively but attenuated progressively thereafter. No significant differences were observed in transplant infection, mortality, or eGFR < 45 mL/min/1.73 m2 across any time interval.
Conclusion: Intraoperative dexmedetomidine exposure was associated with reduced early complications following kidney transplantation. The observational design necessitates cautious interpretation, and randomized controlled trials are required to establish causality.
Keywords: dexmedetomidine, kidney transplantation, delayed graft function, acute rejection, graft failure, renoprotection
Introduction
Kidney transplantation represents the optimal therapeutic intervention for patients with end-stage renal disease, offering superior survival rates and enhanced quality of life compared to chronic dialysis therapy.1–4 However, delayed graft function remains a substantial perioperative complication, affecting 2.6–3.25% of living-donor transplant recipients and 15–67% of deceased-donor transplant recipients.5–12 Delayed graft function, operationally defined as dialysis requirement within the first postoperative week,13 is associated with increased acute rejection episodes, prolonged hospitalization, compromised long-term graft survival, and elevated healthcare costs.14–17 Despite extensive investigation, effective preventive strategies remain elusive, as interventions including hypothermic machine perfusion, dopamine, erythropoietin, and complement inhibitors have yielded minimal or inconsistent benefits.18–20
Dexmedetomidine, a highly selective alpha-2 adrenergic receptor agonist with sedative and analgesic properties, has emerged as a potential renoprotective agent.21–23 Preclinical studies have demonstrated that dexmedetomidine attenuates renal ischemia-reperfusion injury through anti-inflammatory effects, preservation of microvascular perfusion, and enhancement of endothelial function.22,24 A retrospective cohort study by Chen et al reported associations between perioperative dexmedetomidine use and reduced delayed graft function, infection, and acute rejection in 780 kidney transplant recipients.25 Subsequently, Shan et al conducted a randomized controlled trial (RCT) in 111 donation-after-cardiac-death transplant recipients, demonstrating that 24-hour perioperative dexmedetomidine infusion reduced the incidence of delayed graft function from 34.5% to 17.9%.26 A recent meta-analysis by Guo et al27 synthesized 11 studies encompassing 1,417 patients and demonstrated a significantly lower incidence of delayed graft function, along with improvements in serum creatinine, blood urea nitrogen, urine output, and hospital stay. Notably, acute rejection was not assessed in the analysis by Guo et al. Despite these promising findings, clinical evidence remains inconsistent. Park et al reported no beneficial effects of intraoperative dexmedetomidine on renal function or delayed graft function incidence in 104 living-donor kidney transplant recipients,28 in sharp contrast to Shan et al’s findings in donation-after-cardiac-death transplants.26
Previous studies have been constrained by several important limitations. Most existing studies have been conducted within single institutions, which may restrict the generalizability of their findings across diverse healthcare systems and transplant practices. Moreover, relatively small sample sizes, often involving fewer than 800 participants, have limited the statistical power to detect associations with infrequent yet clinically meaningful outcomes, such as acute rejection or graft failure. In addition, follow-up durations in previous studies have also tended to be short, leaving the longer-term implications of dexmedetomidine exposure uncertain. Given the promising preliminary evidence and absence of large-scale confirmatory studies, this investigation examined the association between intraoperative dexmedetomidine exposure and postoperative outcomes following kidney transplantation using a comprehensive multicenter database. We hypothesized that dexmedetomidine exposure would be associated with reduced delayed graft function and improved early graft outcomes.
Methods
Study Design and Data Source
This retrospective cohort study analyzed data from the TriNetX Research Network, a large-scale federated health research platform aggregating de-identified electronic health records from healthcare organizations, predominantly across the United States and other participating countries. The database encompasses comprehensive clinical information, including diagnostic codes according to the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), and procedural codes using Current Procedural Terminology (CPT) and ICD-10 Procedure Coding System (ICD-10-PCS). This platform maintains rigorous data quality standards and has been extensively used for epidemiological, surgical, and perioperative outcome investigations. The Institutional Review Board of Chi Mei Medical Center reviewed and approved the study protocol (approval no. 11406-E02). Given the exclusive use of de-identified secondary data without direct participant interaction, informed consent requirements were waived in accordance with the institutional guidelines governing observational research. This study was conducted in accordance with the principles of the Declaration of Helsinki. We have previously reported a database-based study of perioperative dexmedetomidine in a different surgical setting;29 the present study examined a distinct population and transplant-specific outcomes.
Study Population and Exposure Definition
Adult patients (≥18 years) with stage 5 chronic kidney disease or end-stage renal disease who underwent kidney transplantation between January 1, 2014, and December 31, 2024, were identified. Kidney transplant procedures were recorded using the validated CPT and ICD-10-PCS codes, and the date of surgery was defined as the index date. The patients were divided into two cohorts according to intraoperative dexmedetomidine exposure. The dexmedetomidine group included individuals who were exposed to the drug on the day of surgery, whereas the control group comprised those with no dexmedetomidine exposure within one month after the index procedure. To ensure that exposure only reflected intraoperative use, patients who received dexmedetomidine between postoperative days 2 and 30 were excluded from the dexmedetomidine cohort to avoid confounding from postoperative sedation. Patients who received intraoperative dexmedetomidine and were subsequently monitored in the intensive care unit without further dexmedetomidine administration were included in the analysis. The TriNetX database does not provide sufficient granularity to distinguish between a single intraoperative bolus and a continuous infusion of dexmedetomidine; therefore, exposure was defined based on documented administration on the day of surgery, regardless of the dosing pattern.
Exclusion Criteria
Several exclusion criteria were implemented to minimize confounding factors and enhance between-group comparability. Patients undergoing simultaneous kidney transplantation with other solid organ transplantation procedures, specifically cardiac or hepatic transplantation, were excluded because of substantially different perioperative management strategies and risk profiles. Patients with hemodynamic instability or severe acute illness within one month before surgery were excluded, including sepsis (ICD-10: A41), hepatic failure (ICD-10: K72.X), and shock (ICD-10: R57.X). These conditions represent critical illnesses that could substantially confound perioperative outcomes, independent of anesthetic management. Patients with hemodynamic instability within one month before transplantation were excluded to limit confounding from acute preoperative illness. Although such patients may be considered suitable transplant candidates, recent hemodynamic instability can independently influence early outcomes and anesthetic drug selection. This exclusion criterion was prespecified to minimize bias from pre-existing instability rather than to reflect surgical eligibility.
Propensity Score Matching
Propensity score matching was employed to minimize the confounding inherent in observational data and the approximate covariate balance achieved in randomized trials. Baseline characteristics encompassing demographic information, comorbidities, and laboratory parameters were extracted from the 2-year period preceding the index surgery. Propensity scores representing the conditional probability of receiving dexmedetomidine were estimated using multivariable logistic regression incorporating clinically relevant covariates, including age, sex, race, body mass index, preexisting comorbidities, and preoperative laboratory values. One-to-one matching was subsequently performed using a greedy nearest-neighbor algorithm without replacement, employing a caliper width of 0.1 standard deviations of the logit-transformed propensity score. Matching quality was assessed through standardized mean differences, with thresholds below 0.1 indicating acceptable balance, supplemented by graphical evaluation of propensity score distributions to verify adequate comparability between cohorts.
Outcome Assessment
The primary outcome was delayed graft function (DGF) incidence, operationally defined as dialysis requirement within seven days post-transplantation.25 Secondary outcomes included transplant rejection (ICD-10 T86.11), transplant failure (ICD-10 T86.12), transplant infection (ICD-10 T86.13), all-cause mortality, and impaired renal function defined as an estimated glomerular filtration rate (eGFR) below 45 mL/min/1.73m2. Although outcome ascertainment based on ICD-10 codes is standard in large database studies, this approach is more likely to capture clinically significant rejection episodes requiring documentation or intervention and may underestimate subclinical rejection events.
To comprehensively evaluate the temporal outcome patterns, analyses were conducted across multiple intervals: 7, 30, 30–90, and 90–365 days postoperatively. Analyses extending beyond the early postoperative period were prespecified as exploratory and performed to characterize the time-dependent attenuation of perioperative associations. Because dexmedetomidine exposure was limited to the intraoperative period, these analyses were intended to support the interpretation of early postoperative findings rather than to infer sustained drug effects or causality.
Sensitivity Analyses
Three sensitivity analyses were conducted to evaluate the robustness and internal validity of the findings. Model I excluded patients who received perioperative blood transfusions within 14 days of surgery, minimizing confounding from transfusion-related immunomodulation and hemodynamic alterations. Model II restricted the analysis to patients with documented intraoperative vasopressor exposure, including norepinephrine, dopamine, metaraminol, vasopressin, or phenylephrine, representing a hemodynamically complex subgroup wherein dexmedetomidine effects might differ substantially. Model III limited the inclusion to patients undergoing surgery between 2018 and 2024, addressing the potential temporal confounding from evolving surgical techniques, immunosuppression protocols, and perioperative management practices.
Statistical Analysis
Baseline characteristics were summarized using descriptive statistics, with continuous variables expressed as means with standard deviations and categorical variables as frequencies with percentages. For outcomes assessed within 90 days postoperatively, effect estimates were quantified using odds ratios (OR) with 95% confidence intervals (CI) derived from propensity-matched cohorts. For outcomes evaluated between 90 and 365 days, hazard ratios (HR) with 95% CI were calculated using Cox proportional hazards regression models. For Cox proportional hazards models applied to outcomes between 90 and 365 days, the proportional hazards assumption was assessed using Schoenfeld residuals and was found to be satisfied for all models. Statistical significance was determined using a two-sided alpha level of 0.05. All analyses were performed using integrated analytical tools on the TriNetX platform.
Results
Patient Selection and Baseline Characteristics
Following the application of inclusion and exclusion criteria, the initial dataset comprised 3,369 patients who received intraoperative dexmedetomidine and 43,478 patients who did not receive dexmedetomidine during kidney transplantation (Figure 1). Before propensity score matching, notable differences existed between the groups across several baseline characteristics (Table 1). The dexmedetomidine group demonstrated a lower mean age (47.9 years versus 51.8 years). Comorbidity prevalence varied between cohorts, with the dexmedetomidine group showing higher rates of essential hypertension (74.4% vs 65.7%), anemia (31.4% vs 24.2%), and overweight/obesity (26.7% vs 18.7%).
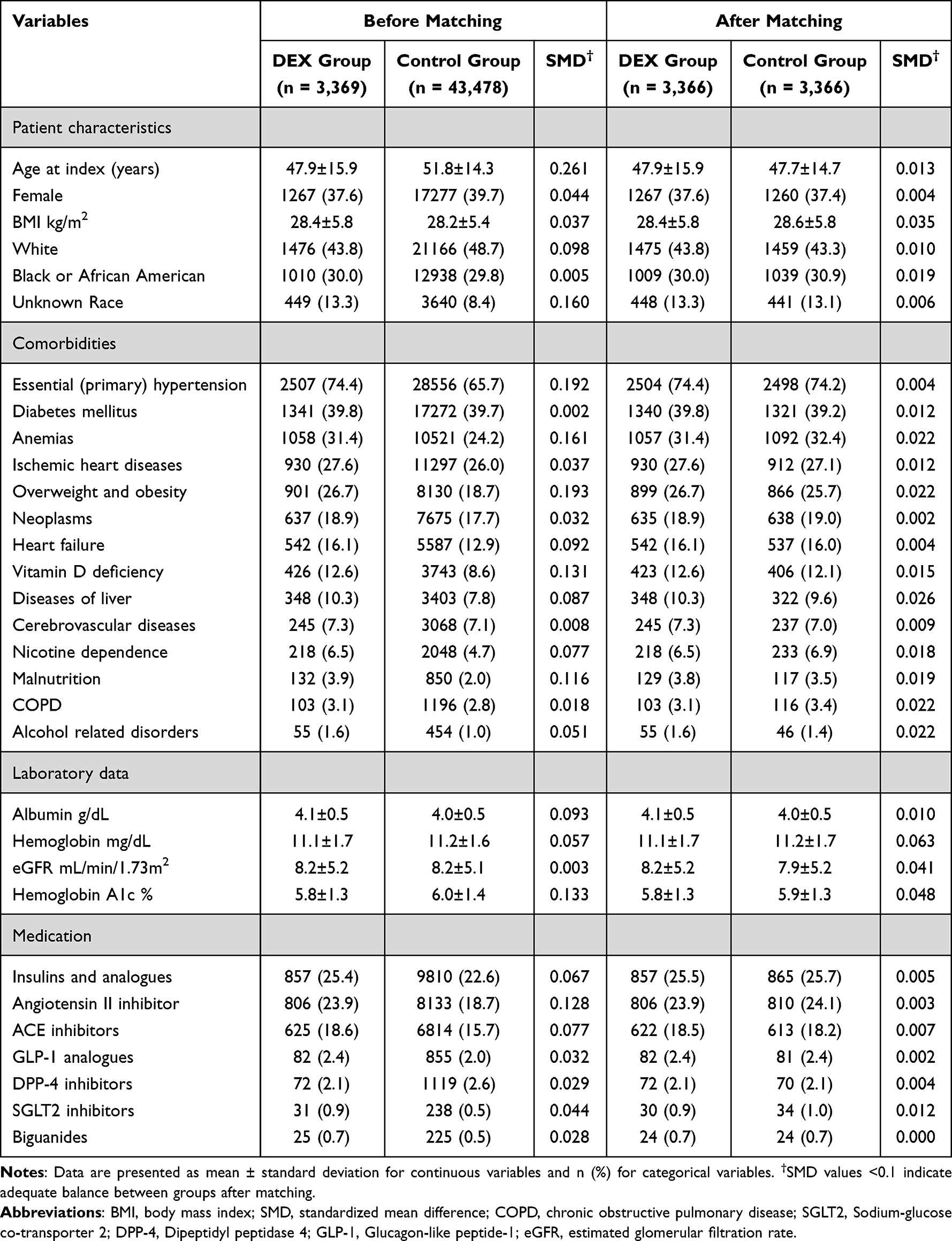 |
Table 1 Baseline Characteristics of Kidney Transplant Recipients Before and After Propensity Score Matching |
 |
Figure 1 Patient selection flowchart from the TriNetX database. DEX: dexmedetomidine. Abbreviation: DEX, dexmedetomidine. |
Following one-to-one propensity score matching, 3,366 patients remained in each cohort, with substantially improved covariate balance (Table 1). All post-matching SMD values fell below 0.1, indicating adequate equilibration between the groups. The matched dexmedetomidine and control cohorts demonstrated comparable distributions across age (47.9 versus 47.7 years), sex, body mass index (28.4 versus 28.6 kg/m2), and racial composition. Baseline comorbidities (eg, hypertension, diabetes, and ischemic heart disease) and laboratory values were comparably distributed across cohorts. Medication usage patterns, including insulin analogs, angiotensin II inhibitors, and ACE inhibitors, were similarly distributed between groups after matching. Figure 2 illustrates the propensity score distributions before and after matching, demonstrating an improved overlap between cohorts following the matching procedure.
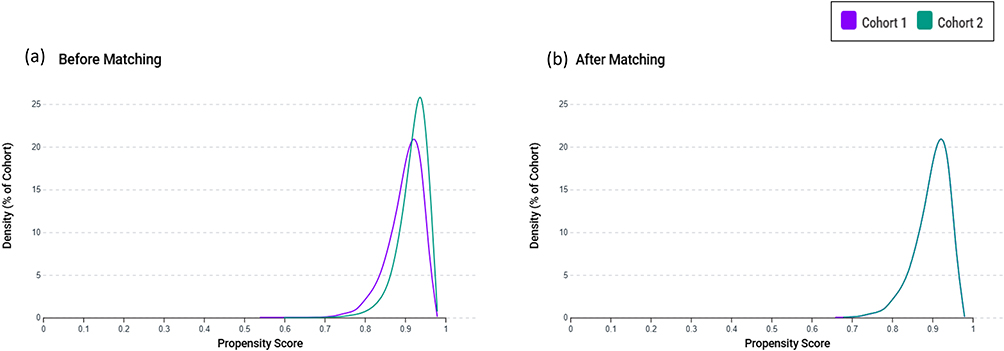 |
Figure 2 Propensity score distributions before and after matching. (a) shows the propensity score distributions between the dexmedetomidine group (Cohort 1, purple) and the control group (Cohort 2, green) before matching, demonstrating baseline imbalance. (b) displays distributions after one-to-one matching based on age, sex, race, laboratory values, and comorbidities, with improved overlap confirming successful covariate balance between groups. |
Association Between Dexmedetomidine Use and Postoperative Outcomes at 7-Day Follow-Up
Analysis of early postoperative outcomes revealed several associations between dexmedetomidine exposure and kidney transplant outcomes within the first seven days following surgery (Table 2). The incidence of delayed graft function, defined as hemodialysis requirement within seven days post-transplantation, was lower in the dexmedetomidine group than in the controls (22.0% versus 24.7%; OR 0.86, 95% CI 0.77–0.96, p=0.009).
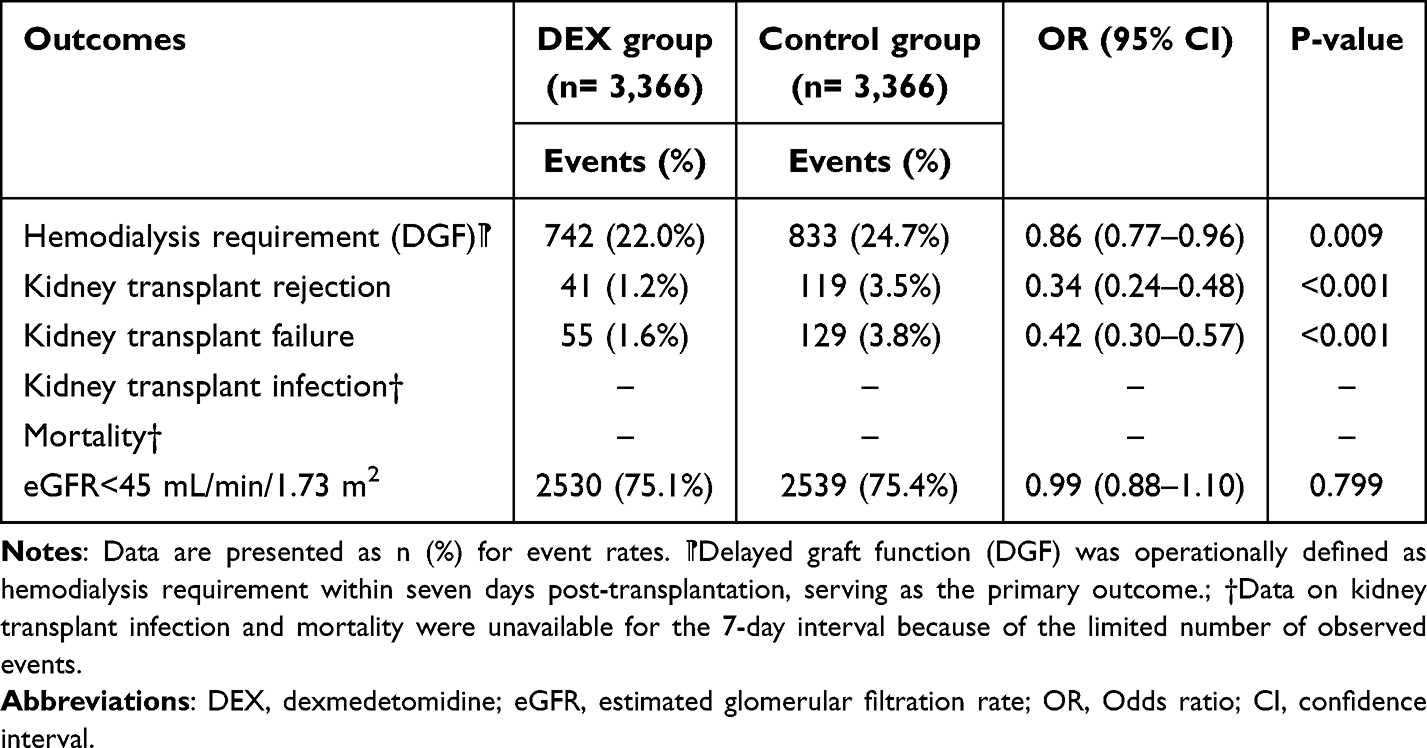 |
Table 2 Association Between Dexmedetomidine and Kidney Transplant Outcomes at 7-Day Follow-Up |
More pronounced associations emerged between acute rejection and graft failure outcomes. Kidney transplant rejection occurred in 1.2% of dexmedetomidine-exposed patients compared to 3.5% of controls (OR 0.34, 95% CI 0.24–0.48, p<0.001). Similarly, kidney transplant failure showed a lower incidence in the dexmedetomidine cohort (1.6% versus 3.8%; OR 0.42, 95% CI 0.30–0.57, p<0.001). The rate of impaired renal function, defined as an eGFR< 45 mL/min/1.73m2, showed comparable distributions between groups (75.1% versus 75.4%; OR 0.99, 95% CI 0.88–1.10, p=0.799). Data on kidney transplant infection and mortality were unavailable for the 7-day interval because of the limited number of observed events.
Association Between Dexmedetomidine Use and Postoperative Outcomes at 365-Day Follow-Up
Temporal analysis across extended follow-up intervals demonstrated evolving associations between dexmedetomidine exposure and transplant outcome (Table 3). During the 1–30 day postoperative period, hemodialysis requirement remained associated with dexmedetomidine use (OR 0.85, p=0.002). Kidney transplant rejection (OR 0.68, p<0.001) and failure (OR 0.62, p<0.001) showed persistent associations during this interval.
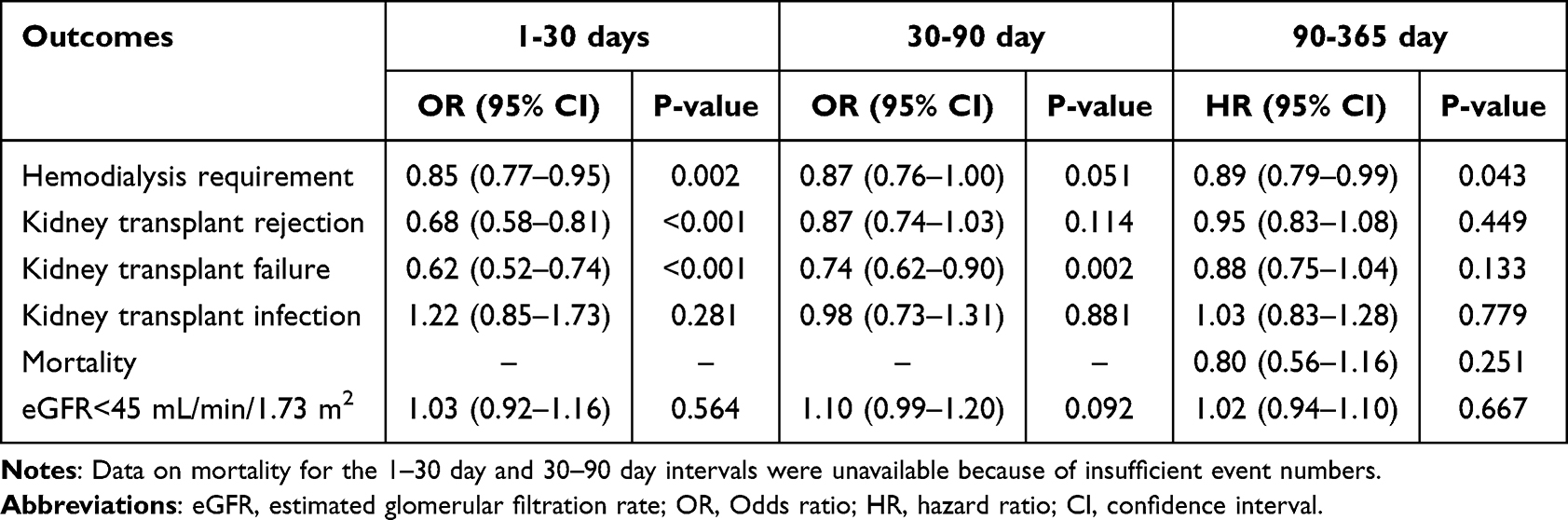 |
Table 3 Association Between Dexmedetomidine and Kidney Transplant Outcomes at Extended Follow-Up Intervals |
In the 30–90 day period, the association with hemodialysis requirement approached but did not reach statistical significance (OR 0.87, p=0.051). Kidney transplant failure maintained a statistically significant association (OR 0.74, p=0.002), whereas the association with rejection was attenuated (OR 0.87, p=0.114).
During the 90–365 day interval, analyzed using Cox proportional hazards regression, hemodialysis requirement continued to show an association with dexmedetomidine exposure (HR 0.89, 95% CI 0.79–0.99, p=0.043). Associations with kidney transplant rejection (HR 0.95, p=0.449) and failure (HR 0.88, p=0.133) were no longer statistically significant. Kidney transplant infection and impaired renal function prevalence showed no significant association across any time interval.
Sensitivity Analysis
Three sensitivity analyses were conducted to evaluate the robustness of the observed associations under varying analytical conditions (Table 4). Model I excluded patients who received perioperative blood transfusions, analyzing 3,044 patients per group. This analysis demonstrated associations consistent with the primary findings.
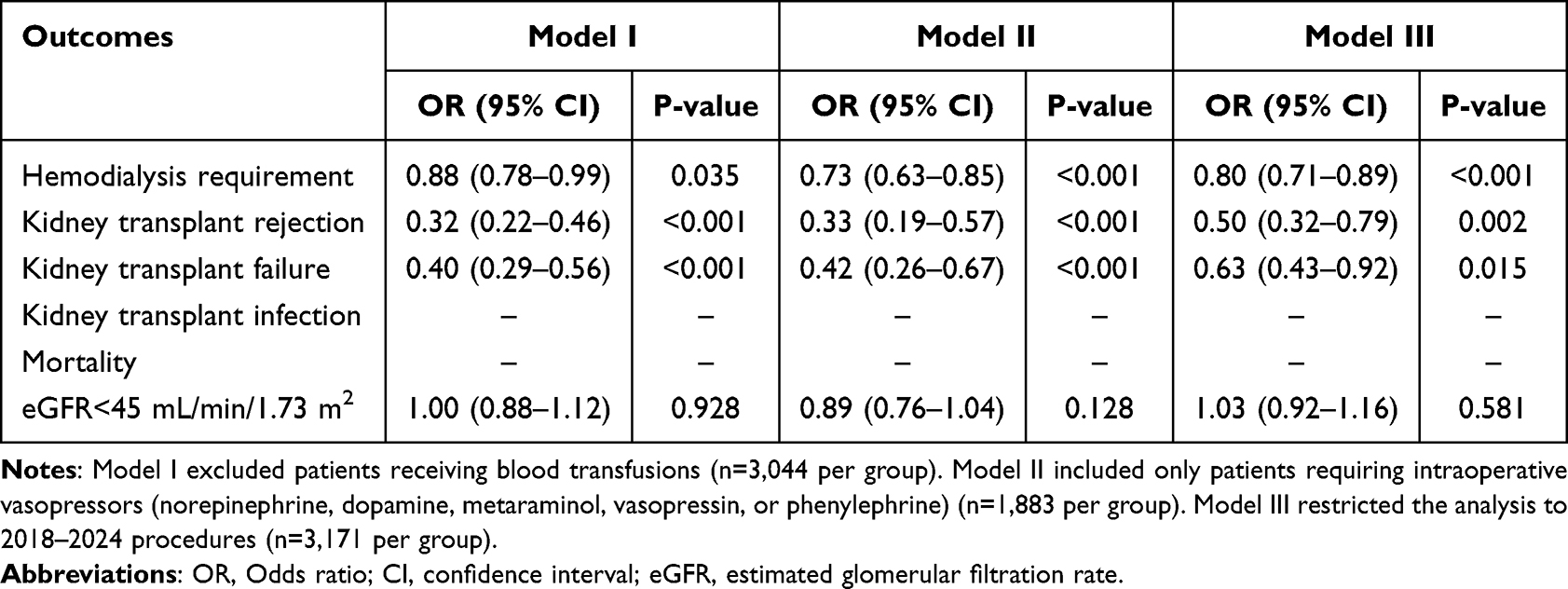 |
Table 4 Sensitivity Analyses of Associations Between Dexmedetomidine and Kidney Transplant Outcomes at 7-Day Follow-up |
Model II restricted the analysis to patients who received intraoperative vasopressors, representing a hemodynamically complex subpopulation. This subgroup analysis also revealed associations of a similar magnitude.
Model III limited the analysis to procedures performed between 2018 and 2024, encompassing 3,171 patients per group, to address potential temporal confounding from evolving clinical practices. The results remained directionally consistent with the primary analyses. Across all sensitivity models, impaired renal function showed no significant differences between the groups, corroborating the primary findings.
Discussion
This multicenter retrospective cohort study examined the associations between intraoperative dexmedetomidine exposure and kidney transplant outcomes in 6,732 propensity-matched patients. Dexmedetomidine exposure was associated with a lower incidence of delayed graft function, acute rejection, and graft failure within 7 days postoperatively. Temporal analysis revealed distinct trajectories: associations with delayed graft function and acute rejection were evident within the first 30 days but lost statistical significance thereafter, whereas the association with kidney transplant failure persisted up to 90 days before becoming non-significant. Sensitivity analyses corroborated the primary findings, with particularly strong associations among patients requiring intraoperative vasopressors. However, no differences emerged in eGFR across all intervals. These findings suggest potential perioperative benefits, although the observational design necessitates cautious interpretation.
Park et al, conducted a RCT involving 104 living-donor kidney transplant recipients and found no beneficial effects of intraoperative dexmedetomidine on renal function or the incidence of delayed graft function.28 In contrast, Shan et al exclusively enrolled donation-after-cardiac-death recipients, demonstrating a substantial reduction in delayed graft function with a 24-hour perioperative dexmedetomidine infusion.26 These divergent findings suggest that the potential benefits of dexmedetomidine may be most pronounced in high-risk donor scenarios characterized by prolonged ischemia and increased susceptibility to ischemia-reperfusion injury. In our study, delayed graft function occurred in 22.0% of patients in the dexmedetomidine group versus 24.7% of controls, compared with Shan et al’s findings of 17.9% versus 34.5% among donation-after-cardiac-death transplant recipients, respectively. This smaller relative risk reduction may reflect the heterogeneity of our cohort, which likely included a mix of living-donor, standard-criteria deceased-donor, and higher-risk donation-after-cardiac-death grafts. Consistent with the US transplant demographics, kidneys donated after circulatory death account for a substantial and increasing proportion of deceased kidney donors (37.3% in 2023), suggesting that a meaningful fraction of our cohort likely included higher-risk grafts.30 Unfortunately, the TriNetX database does not capture donor type or cold and warm ischemia times, precluding subgroup analyses based on these key determinants of ischemia-reperfusion injury severity. In addition, Shan et al’s 2019–2021 trial reflected modern transplant practices,26 whereas our 2014–2024 multicenter cohort spanned evolving protocols and expertise. Temporal and institutional variability likely contributed to the modest effect size observed in our real-world cohort compared to Shan et al’s single-center trial.
Sensitivity analysis limited to patients requiring intraoperative vasopressors showed a stronger association, with an OR of 0.73 for delayed graft function versus 0.86 overall. This result aligns with the growing evidence that the protective effects of dexmedetomidine are more evident in higher-risk patients, as reflected by the lack of benefit in Park et al’s low-risk living-donor cohort28 versus the pronounced reduction in delayed graft function observed in Shan et al’s high-risk cardiac-death cohort.26 Patients requiring vasopressor support likely experience periods of compromised renal perfusion, elevating the baseline risk for ischemia-reperfusion injury. In this hemodynamically unstable subgroup, the sympatholytic properties of dexmedetomidine and potential microvascular perfusion preservation through alpha-2 receptor-mediated mechanisms22,24 could confer disproportionate benefits, where even marginal perfusion improvements become critically important for graft outcomes. However, this pattern warrants cautious interpretation. Clinicians selecting dexmedetomidine in hemodynamically complex cases may concurrently employ other unmeasured protective strategies, including meticulous fluid management, earlier vasopressor initiation, or enhanced monitoring intensity, representing potential residual confounding.
The association between dexmedetomidine and reduced acute rejection represents an important finding that aligns with and extends the previous evidence. Our finding of a 7-day OR of 0.34 for acute rejection is consistent with Chen et al’s single-center retrospective analysis,25 which demonstrated an adjusted OR of 0.401 among 780 kidney transplant recipients treated with perioperative dexmedetomidine. This consistency across independent observational studies, despite different analytical approaches and patient populations, strengthens the confidence that a genuine association exists. The absence of statistically significant rejection-related benefits in a recent meta-analysis of 339 patients across four studies31 likely reflects insufficient statistical power, particularly for outcomes such as acute rejection that occur in relatively small proportions of patients. Our larger cohort of 6,732 propensity-matched patients, combined with Chen et al ‘s 780 patients, may provide cumulative evidence from nearly 7,500 observational subjects supporting this association. Our investigation extends beyond previous work through systematic temporal analysis, demonstrating that rejection associations persisted for 30 days postoperatively. Most notably, our study is the first to demonstrate that dexmedetomidine use was associated with a lower risk of kidney transplant failure that persisted for 90 days postoperatively.
However, graft rejection represents a heterogeneous clinical outcome with diverse underlying mechanisms, including vascular complications, drug-related toxicities, and immunological processes. The present study was not able to distinguish the specific causes of rejection events, such as renal vessel thrombosis or calcineurin inhibitor–associated thrombotic microangiopathy. Accordingly, the observed associations should not be interpreted as evidence that intraoperative dexmedetomidine influences all forms or etiologies of graft rejection. Rather, these findings reflect population-level associations identified within a real-world database and should be interpreted with appropriate caution.
If causal, the observed associations likely involve interconnected anti-inflammatory and vascular mechanisms. Preclinical studies have demonstrated that dexmedetomidine attenuates ischemia-reperfusion injury by reducing pro-inflammatory cytokines, including interleukin-6 and intercellular adhesion molecule-1, inhibiting high-mobility group box 1 release, and suppressing Toll-like receptor 4 signaling.32,33 These effects may reduce allograft immunogenicity by limiting the initial tissue damage that would otherwise trigger danger signals, upregulate major histocompatibility complex expression, and activate antigen-presenting cells. Dexmedetomidine also suppresses Janus kinase and signal transducer and activator of transcription signaling pathways, downregulating monocyte chemoattractant protein-1 and limiting inflammatory cell recruitment.34 Additionally, dexmedetomidine activates alpha-2 adrenergic receptors abundantly expressed in the renal tubular and peritubular vascular structures, modulating sympathetic tone and promoting nitric oxide-mediated vasodilation to preserve microvascular perfusion.35,36 Animal studies have shown that dexmedetomidine activates the Akt signaling pathway, promoting cellular survival and reducing apoptosis in ischemic renal tissues.33 Beyond its direct anti-inflammatory and vascular effects, dexmedetomidine may indirectly influence adaptive immune responses by attenuating early ischemia–reperfusion injury and the associated release of danger-associated molecular patterns, thereby potentially limiting dendritic cell activation and subsequent T-cell priming that contribute to acute rejection.33,37,38 The temporal concentration of associations within 90 days supports mechanisms involving acute perioperative injury rather than sustained immunomodulation. However, these mechanistic explanations remain speculative in the absence of direct investigations in human transplant recipients. Whether the observed associations reflect these proposed biological pathways or unmeasured confounding factors cannot be definitively determined from observational data.
The absence of differences in eGFR < 45 mL/min/1.73m2 aligns consistently with prior investigations,25,26 which reported no significant differences in renal function parameters at intermediate and long-term follow-up. This consistent pattern suggests that while dexmedetomidine may be associated with reduced acute complications, these reductions do not translate into measurably superior long-term functional outcomes among surviving grafts. Contemporary management of delayed graft function and acute rejection has substantially improved, and patients experiencing these complications may achieve functional recovery comparable to those without complications. Additionally, numerous factors beyond perioperative events influence long-term function, including chronic immunological processes, calcineurin inhibitor nephrotoxicity, and recipient comorbidities, which may overwhelm any perioperative advantage.
Several clinically relevant details could not be evaluated because they were not available in the TriNetX database. These include specific anesthetic regimens used in patients who did not receive dexmedetomidine, reasons for discontinuation of dexmedetomidine owing to adverse effects, biopsy-confirmed findings and etiologies of graft rejection, immunosuppressive drug dosing and toxicity, and the use of circulatory or respiratory support during intensive care. Rejection events were identified using standardized diagnostic codes rather than adjudicated clinical or pathological criteria. Accordingly, the findings of this study should be interpreted as real-world associations rather than mechanistic or causal evidence.
This study had several important limitations. First, the observational design precludes causal inference despite propensity score matching. Unmeasured confounding factors may persist, particularly concerning clinicians’ dexmedetomidine selection based on factors not captured in administrative data. Second, the TriNetX database lacks granular details regarding dexmedetomidine dosing, exposure duration, and timing. Critical donor-specific variables, including ischemia times and donor quality indices, were unavailable. Third, outcome ascertainment relied on diagnostic coding and was potentially subject to misclassification. Rejection ascertainment depends on the clinical suspicion that prompts biopsy, potentially introducing differential ascertainment. Fourth, immunosuppression protocols varied across institutions and time periods, potentially confounding the results if dexmedetomidine use correlated with specific regimens. Fifth, the predominance of United States healthcare systems limits the generalizability to international populations with different transplant practices and healthcare structures. Finally, institutional-level factors, such as center volume, quality metrics, and care protocols, may correlate with both dexmedetomidine use and outcomes, representing confounding factors that propensity matching cannot address.
Conclusion
This large-scale multicenter investigation identified associations between intraoperative dexmedetomidine exposure and reduced early complications following kidney transplantation, including delayed graft function, acute rejection, and graft failure within 7 days postoperatively. These associations attenuated progressively over time and were not accompanied by improvements in short- and long-term estimated glomerular filtration rates, suggesting effects primarily on acute perioperative processes rather than ultimate functional outcomes. The observational design precludes causal inference, and the magnitude of associations, particularly for rejection, requires cautious interpretation, given potential residual confounding. These hypothesis-generating findings support the need for adequately powered multicenter RCTs to definitively establish causality and identify patient populations most likely to benefit from perioperative dexmedetomidine exposure.
Data Sharing Statement
The data used in this study were obtained from the TriNetX Research Network under collaborative agreement and are not publicly available. However, de-identified data may be accessed upon reasonable request from the author (Kuo-Chuan Hung) with permission from TriNetX and subject to a data-sharing agreement or network membership.
Ethics Approval Statement
The study protocol was approved by the Institutional Review Board of Chi Mei Medical Center, which waived the requirement for informed consent in accordance with the regulations for observational research (IRB No. 11406-E02).
Patient Consent Statement
Informed consent was not required for this retrospective study, as it involved secondary analysis of pre-existing data without any interventions or direct participant interaction.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflict of interest.
References
1. Ryu JH, Koo TY, Ro H, et al. Better health-related quality of life in kidney transplant patients compared to chronic kidney disease patients with similar renal function. PLoS One. 2021;16:e0257981. doi:10.1371/journal.pone.0257981
2. Tucker EL, Smith AR, Daskin MS, et al. Life and expectations post-kidney transplant: a qualitative analysis of patient responses. BMC Nephrol. 2019;20:175. doi:10.1186/s12882-019-1368-0
3. Gupta R, Woo K, Yi JA. Epidemiology of end-stage kidney disease. Semin Vasc Surg. 2021;34:71–12. doi:10.1053/j.semvascsurg.2021.02.010
4. Ngamvichchukorn T, Ruengorn C, Noppakun K, et al. Association between pretransplant dialysis modality and kidney transplant outcomes: a systematic review and meta-analysis. JAMA Network Open. 2022;5:e2237580. doi:10.1001/jamanetworkopen.2022.37580
5. Aceto P, Perilli V, Luca E, et al. Perioperative-, RECIPIENT-, AND DONOR-RELATED FACTORS AFFECTING DELAYED GRAFT FUNCTION IN KIDNEY TRANSPLANTation. Exp Clin Transplant. 2019;17:575–579. doi:10.6002/ect.2018.0225
6. Kaufmann KB, Baar W, Silbach K, et al. Modifiable risk factors for delayed graft function after deceased donor kidney transplantation. Prog Transplant. 2019;29:269–274. doi:10.1177/1526924819855357
7. Jahn L, Rüster C, Schlosser M, et al. Rate, factors, and outcome of delayed graft function after kidney transplantation of deceased donors. Transplant Proc. 2021;53:1454–1461. doi:10.1016/j.transproceed.2021.01.006
8. Mendez NV, Raveh Y, Livingstone JJ, et al. Perioperative risk factors associated with delayed graft function following deceased donor kidney transplantation: a retrospective, single center study. World J Transplant. 2021;11:114–128. doi:10.5500/wjt.v11.i4.114
9. Melih KV, Boynuegri B, Mustafa C, Nilgun A. Incidence, risk factors, and outcomes of delayed graft function in deceased donor kidney transplantation. Transplant Proc. 2019;51:1096–1100. doi:10.1016/j.transproceed.2019.02.013
10. Bronzatto EJ, da Silva Quadros KR, Santos RL, Alves-Filho G, Mazzali M. Delayed graft function in renal transplant recipients: risk factors and impact on 1-year graft function: a single center analysis. Transplant Proc. 2009;41:849–851. doi:10.1016/j.transproceed.2009.02.004
11. Damodaran S, Bullock B, Ekwenna O, et al. Risk factors for delayed graft function and their impact on graft outcomes in live donor kidney transplantation. Int Urol Nephrol. 2021;53:439–446. doi:10.1007/s11255-020-02687-5
12. Tirtayasa PMW, Situmorang GR, Duarsa GWK, et al. Risk factors of delayed graft function following living donor kidney transplantation: a meta-analysis. Transpl Immunol. 2024;86:102094. doi:10.1016/j.trim.2024.102094
13. Mannon RB. Acute kidney injury in kidney transplants: new insights. Nephron. 2019;143:193–196. doi:10.1159/000500550
14. Kim DW, Tsapepas D, King KL, et al. Financial impact of delayed graft function in kidney transplantation. Clin Transplant. 2020;34:e14022. doi:10.1111/ctr.14022
15. Lim WH, Johnson DW, Teixeira-Pinto A, Wong G. Association between duration of delayed graft function, acute rejection, and allograft outcome after deceased donor kidney transplantation. Transplantation. 2019;103:412–419. doi:10.1097/TP.0000000000002275
16. Li MT, Ramakrishnan A, Yu M, et al. Effects of delayed graft function on transplant outcomes: a meta-analysis. Transplant Direct. 2023;9:e1433. doi:10.1097/TXD.0000000000001433
17. Budhiraja P, Reddy KS, Butterfield RJ, et al. Duration of delayed graft function and its impact on graft outcomes in deceased donor kidney transplantation. BMC Nephrol. 2022;23:154. doi:10.1186/s12882-022-02777-9
18. Ponticelli C, Reggiani F, Moroni G. Delayed graft function in kidney transplant: risk factors, consequences and prevention strategies. J Pers Med. 2022;12:1557. doi:10.3390/jpm12101557
19. Swanson KJ, Bhattarai M, Parajuli S. Delayed graft function: current status and future directions. Curr Opin Organ Transplant. 2023;28:1–7. doi:10.1097/MOT.0000000000001034
20. Franzin R, Stasi A, Fiorentino M, et al. Renal delivery of pharmacologic agents during machine perfusion to prevent ischaemia-reperfusion injury: from murine model to clinical trials. Front Immunol. 2021;12:673562. doi:10.3389/fimmu.2021.673562
21. Gao X, Wu Y. Perioperative acute kidney injury: the renoprotective effect and mechanism of dexmedetomidine. Biochem Biophys Res Commun. 2024;695:149402. doi:10.1016/j.bbrc.2023.149402
22. Bao N, Tang B, Wang J. Dexmedetomidine preconditioning protects rats from renal ischemia-reperfusion injury accompanied with biphasic changes of nuclear factor-Kappa B signaling. J Immunol Res. 2020;2020:3230490. doi:10.1155/2020/3230490
23. Liu X, Li Y, Kang L, Wang Q. Recent advances in the clinical value and potential of dexmedetomidine. J Inflamm Res. 2021;14:7507–7527. doi:10.2147/JIR.S346089
24. Yang SJ, Fan CN, Wang MJ, et al. Effects of dexmedetomidine on renal microcirculation in ischemia/reperfusion-induced acute kidney injury in rats. Sci Rep. 2021;11:2026. doi:10.1038/s41598-021-81288-3
25. Chen J, Perez R, de Mattos AM, et al. Perioperative dexmedetomidine improves outcomes of kidney transplant. Clin Transl Sci. 2020;13:1279–1287. doi:10.1111/cts.12826
26. Shan XS, Hu LK, Wang Y, et al. Effect of perioperative dexmedetomidine on delayed graft function following a donation-after-cardiac-death kidney transplant: a randomized clinical trial. JAMA Network Open. 2022;5:e2215217. doi:10.1001/jamanetworkopen.2022.15217
27. Guo Y, Lan G, Hu S. Perioperative effects of dexmedetomidine on renal function in allogeneic kidney transplant patients: a meta-analysis. Int Urol Nephrol. 2025;57:3821–3838. doi:10.1007/s11255-025-04576-1
28. Park JH, Koo BN, Kim MS, Shin D, Kwak YL. Effects of intraoperative dexmedetomidine infusion on renal function in elective living donor kidney transplantation: a randomized controlled trial. Can J Anaesth. 2022;69:448–459. doi:10.1007/s12630-021-02173-1
29. Hung KC, Chang LC, Lai YC, Wu JY, Chen IW. Perioperative dexmedetomidine exposure and one-year mortality risk after video-assisted thoracoscopic surgery: a multi-institutional study. Drug Des Devel Ther. 2025;19:10495–10506. doi:10.2147/DDDT.S560044
30. Lentine KL, Smith JM, Lyden GR, et al. OPTN/SRTR 2023 annual data report: kidney. Am J Transplant. 2025;25:S22–s137. doi:10.1016/j.ajt.2025.01.020
31. Abuelazm MT, Ghanem A, Johanis A, et al. Reno-protective effects of perioperative dexmedetomidine in kidney transplantation: a systematic review and meta-analysis of randomized controlled trials. Int Urol Nephrol. 2023;55:2545–2556. doi:10.1007/s11255-023-03568-3
32. Sugita S, Okabe T, Sakamoto A. Continuous infusion of dexmedetomidine improves renal ischemia-reperfusion injury in rat kidney. J Nippon Med Sch. 2013;80:131–139. doi:10.1272/jnms.80.131
33. Gu J, Sun P, Zhao H, et al. Dexmedetomidine provides renoprotection against ischemia-reperfusion injury in mice. Crit Care. 2011;15:R153. doi:10.1186/cc10283
34. Si Y, Bao H, Han L, et al. Dexmedetomidine protects against renal ischemia and reperfusion injury by inhibiting the JAK/STAT signaling activation. J Transl Med. 2013;11:141. doi:10.1186/1479-5876-11-141
35. Lempiäinen J, Finckenberg P, Mervaala EE, et al. Dexmedetomidine preconditioning ameliorates kidney ischemia-reperfusion injury. Pharmacol Res Perspect. 2014;2:e00045. doi:10.1002/prp2.45
36. Cai Y, Xu H, Yan J, Zhang L, Lu Y. Molecular targets and mechanism of action of dexmedetomidine in treatment of ischemia/reperfusion injury. Mol Med Rep. 2014;9:1542–1550. doi:10.3892/mmr.2014.2034
37. Braza F, Brouard S, Chadban S, Goldstein DR. Role of TLRs and DAMPs in allograft inflammation and transplant outcomes. Nat Rev Nephrol. 2016;12:281–290. doi:10.1038/nrneph.2016.41
38. Loverre A, Capobianco C, Stallone G, et al. Ischemia-reperfusion injury-induced abnormal dendritic cell traffic in the transplanted kidney with delayed graft function. Kidney Int. 2007;72:994–1003. doi:10.1038/sj.ki.5002468
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Flow Cytometric Analysis of Peripheral Blood Lymphocytes and Expression of HLA II Molecules in Lymphocyte During Acute Rejection After Renal Transplantation
Guo J, Qin C, Li X, Zhuang X
Journal of Inflammation Research 2023, 16:2607-2613
Published Date: 19 June 2023
Positive Metagenomic Next-Generation Sequencing of Renal Lavage Fluid Associates with Delayed Graft Function in Kidney Transplants from Donors After Circulatory Death: A Retrospective Study
Li D, Pan J, Yang M, Zhong J, Ding H, Chen W, Zhang J, Liao G
Infection and Drug Resistance 2025, 18:4579-4592
Published Date: 30 August 2025