Back to Journals » Advances in Medical Education and Practice » Volume 12
Association Between Learning Approaches and Medical Student Academic Progression During Preclinical Training
Authors Bansal S, Bansal M, White S
Received 13 July 2021
Accepted for publication 28 October 2021
Published 18 November 2021 Volume 2021:12 Pages 1343—1351
DOI https://doi.org/10.2147/AMEP.S329204
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Sandeep Bansal,1 Minakshi Bansal,2 Stanley White3
1Department of Medical Education, TCU and UNTHSC School of Medicine, Fort Worth, TX, USA; 2Harris College of Nursing and Health Sciences, Texas Christian University, Fort Worth, TX, USA; 3All Saints University School of Medicine, Roseau, Commonwealth of Dominica
Correspondence: Sandeep Bansal
Department of Medical Education, TCU & UNTHSC School of Medicine, Fort Worth, TX, USA
Email [email protected]
Purpose: Students have diverse learning preferences that can impact the achievement of learning outcomes. However, there is a lack of unequivocal evidence for an association between the learning preferences and academic success. The purpose of the study was to examine the association between learning approaches and academic success of medical students during the basic science curriculum.
Methods: In this cross-sectional comparative study, low-achieving (n=80) and high-achieving students (n=50) from semesters 1 through 3 of the Ross University School of Medicine’s basic science curriculum completed the Approaches and Study Skills Inventory for Students (ASSIST) short-form to provide data on their learning approaches. Student’s-t test was applied to find statistical differences in learning approaches of low and high achievers, and point-biserial was used to analyze the correlation between academic performance and learning approaches. Mean sum scores with standard deviation on ASSIST short-form scales (deep, surface, and strategic approaches) as well as subscales are reported.
Results: High-achieving students reported a preference for using deep and strategic learning approaches compared to low-achieving students (p < 0.05). Low achievers indicated that they predominantly used the surface approach to learning (p< 0.05). Yet, “fear of failure,” a subscale of the surface approach, was greater among high achievers. Additionally, significant gender differences were found on subscales of “lack of purpose,” “syllabus bound,” “unrelated memorization” (surface approach), and “time management” and “organized studying” (strategic approach).
Conclusion: Our results suggest that low-achieving medical students’ predominant reliance on the surface approach to learning may affect their academic success and that it may be worthwhile to help medical students become aware of the effectiveness of their individual preferred learning approaches early on in their training. Identification and adoption of optimal learning approaches should increase the achievement of successful learning outcomes.
Keywords: learning approaches, learning outcomes, remediation, medical curriculum, ASSIST short-form
Introduction
Preclinical training of medical students is demanding because of the vast volume of content students need to learn in a limited period of time. Moreover, content needs to be efficiently attained, assimilated, integrated, and applied to solve problems, to score well on assessments. Medical students bring with them diverse learning experiences at the time of matriculating into a medical school. These experiences lead to the development of diverse learning preferences that the students use to engage with learning material.1 Diverse learning preferences, however, present a challenge to educators to meet their individual educational needs. Student motivation and performance is reported to improve when instruction is adapted to their learning preferences.2
Learning preferences are understood and characterized in several different ways based on a variety of theoretical models.3 Two of these are “learning styles” and “learning approaches.”4 One of the most widely used learning style models, the VARK model, is based on the preferred sensory modality used for learning, and differentiates learning styles into visual (V), auditory (A), read/write (R), and kinesthetic (K) modalities.4,5 Learning approaches, on the other hand, are based on the work of Marton and Säljö,6 which defines learning preferences in terms of “deep,” “surface,” and “strategic” learning approaches.7 Students using the deep approach to learning interact with the study material with a deep desire to understand and make meaning of what is being learned as well as to connect dots across concepts to synthesize knowledge. Students using the surface approach to learning are driven by a desire to avoid failure. They primarily employ rote-learning and memorization to become able to recollect and regurgitate material in examinations. The strategic approach entails student efficiency in studying to achieve the highest possible grades. Students using the strategic approach tend to organize their time well and be informed by the structure and content of previous examinations to guide what to learn and to what depth so as to perform well in examinations.
Research on students’ learning approaches is relevant because the way students choose to approach the learning material has an impact on achievement of learning outcomes as measured by performance on assessments.8 Unless the educator learns how individual students approach learning, efforts to make changes in teaching-learning methods in a curriculum may not be successful in yielding desired learning outcomes.9 Prior studies have examined learning approaches of medical students and have reported varying results.7,10,11 Samarakoon et al showed that advancement from undergraduate to postgraduate medical training is associated with increasing preference for deep and strategic learning approaches over time.7 Salamonson et al studied learning approaches across disciplines and found no significant difference in the use of surface approach, but wide variations in the use of deep approach.12 While Reid et al showed higher preference for deep approach to learning among undergraduate medical students and attributed them to changes made to curriculum,10 Shah et al found that preference for deep approaches decreased after the first year of undergraduate medical training.11 These studies did not examine the difference in learning approaches of students with varying academic abilities. The studies in other health science fields that have attempted to explore the association between learning approaches and academic performance have done so prospectively using performance on a single examination or student grades at the time of data collection.13,14 Naqvi et al found no significant relationship between learning approaches and academic performance of undergraduate medical students,15 whereas, Bonsaksen et al reported that approaches to studying predict academic performance.16 Lack of unequivocal findings on the association between learning approaches and student academic performance requires further exploration to inform refinements in educational strategies.
We engaged in an academic enhancement program to facilitate the academic success of low-achieving medical students who failed to progress to the next semester. The motivation to undertake this project was to explore the learning approaches of low-achieving and high-achieving medical students, with the goal of using the findings to promote academic success of low-achieving students. The study was designed to answer the research question
What is the difference in learning approaches of medical students who failed a semester (low-achieving students) and their classmates who passed the semester with high grades (high-achieving students) in the basic science curriculum of the Ross University School of Medicine (RUSM)?
We hypothesized that high-achieving medical students use primarily the deep learning approach to excel in medical training and the low-achieving medical students rely primarily on the surface learning approach.
Materials and Methods
Study Design and Setting
We conducted this cross-sectional, comparative, and a quasi-experimental study at the Center for Teaching and Learning (CTL; now The Academy for Teaching and Learning) of the RUSM, Commonwealth of Dominica, in the Summer of 2013. The Institutional Review Board of RUSM granted permission for the study.
The RUSM students complete their basic sciences preclinical training in an organ systems-based integrated curriculum at the school’s Caribbean campus (at the time of study in Dominica; the campus is now located in Barbados) and the clinical training in the United States at certified clinical sites. RUSM offers students two curriculum tracks, a four-semester accelerated track and a five-semester track, to complete basic science training in 60 weeks and 75 weeks, respectively. The first-semester program is common for all students. At the completion of the first semester, students have the option to remain in the standard four-semester accelerated track to complete the basic sciences course in the next three semesters or “decelerate” into the five-semester track to complete basic sciences course in the next four semesters. An appropriate track is selected based on the student’s academic progress in semester one. The remaining six semesters (clinical sciences) of the medical school training are the same in duration for all students and are completed at various clinical sites in the United States.
Students who fail to pass a semester are required to repeat that semester. The repeating students, defined as low-achieving students in the study, of each semester are enrolled in a mandatory Essential Lifelong Learning Skills (ELLS) program of 13-weeks duration, which is taken concurrently with the regular basic science classes through the semester. The ELLS program focuses on enhancing students’ cognitive, language, and reasoning skills. The program’s design involves a facilitator devoted to a small group of students (usually 4–5). The facilitator provides a safe environment for students to discuss their weaknesses and strengths with regard to their study habits and subject matter, with the purpose of enabling students to identify their own learning needs and learn to develop strategies to manage their time efficiently.
Participants and Recruitment
Students who failed to progress to the next semester were defined as low achievers. These students would repeat the failed semester. Students who passed and progressed to next semester by scoring >80% marks were defined as high achievers. In this manner, first-semester students who failed were defined as first-semester low achievers and their classmates who progressed to second semester by scoring >80% marks were defined as first-semester high achievers. Similarly, students who failed second and third semesters were defined as second- and third-semester low achievers, respectively, and their classmates who progressed to next semesters by scoring >80 marks were defined as second- and third-semester high achievers, respectively. Lists of low achievers and high achievers of first, second, and third semesters were obtained from the RUSM exam center.
A quasi-experimental design was used for enrolment of subjects in the study. A total of 80 low achievers and 95 high achievers were identified. The ideal sample sizes of 67 and 77 subjects were estimated for the low achiever and the high achiever groups, respectively, at a confidence interval of 95% with margin of error of 5%.17
An informed consent was obtained from each subject before the commencement of the study. All 80 low achievers participated in the study. These students were required to respond to the study survey at the time of enrollment into the ELLS program. Out of 95 high achievers, 50 participated in the study.
Those students who had failed a semester more than once or failed more than one semester were excluded from the study. Students in the final basic science semester (fourth semester of the four-semester accelerated curriculum track and fifth semester of the five-semester track) were also excluded.
Assessment Tool
The Approaches and Study Skills Inventory for Students (ASSIST) short-form was used to assess learning approaches of medical students during their preclinical training.18 ASSIST is a validated tool based on the conception of learning described by Marton and Säljö.6,19 The ASSIST short-form (Appendix 1) presents three scales of learning approaches, deep, surface, and strategic, with six items under each, for a total of 18 items. Six items of each scale are further grouped under four subscales.18 The subscales define the themes covered by items under them.
The tool consists of statements that students indicate the ways in which they are going about their studying by describing their typical actions. The items of the tool are scored using a 5-point Likert scale in which score 1 indicates strongly disagree, 2 disagree, 3 undecided, 4 agree, and 5 strongly agree. Studies have reported internal consistency of ASSIST short-form. In one study, Cronbach α for the deep, the surface, and the strategic approaches were 0.65, 0.70, and 0.75, respectively.18 Furthermore, the strength of associations of ASSIST short-form with the scales on the full-form was r = 0.86 (the deep scale), 0.87 (the surface scale), and 0.85 (the strategic scale). The strong association of the short-form with the full-form renders it relatively equal in terms of its ability to predict outcomes.20
Data Collection
Low-achieving students from each semester (first, second, and third semester) were enrolled in the study from their respective ELLS groups at the CTL. High-achieving students who had progressed to the next semester were sent emails informing them about the purpose of the study and inviting them to participate. The ASSIST short-form questionnaire, in printed form, was administered to low-achieving students at the beginning of their ELLS sessions. The identified high-achieving students who volunteered to participate in the study received emails with an attached pdf copy of the questionnaire. These students were asked to either print the questionnaire, enter their responses to items, and leave the questionnaire in author SB’s departmental mail box, or send their responses by email by attaching the filled-in questionnaire. Students who chose to visit the authors’ (SB, MB) department to respond to the questionnaire were provided private sitting space. Demographic data on age and gender were collected along with the responses to the ASSIST questionnaire. The data were immediately codified to anonymize the respondents, and confidentiality of the data was maintained throughout the study.
Data Analysis
We used IBM SPSS Statistics for Windows, version 25 (IBM Corp., Armonk, NY, USA) for data compilation and running statistical tests. As learning approaches of low- and high-achieving students of a class were analyzed to answer the study’s research question, Student’s t-test with post-hoc Bonferroni correction was applied to determine statistical significance of differences in learning approaches of the two student groups of each semester.21 Point-biserial was applied to find correlations between academic performance (two student groups: low achievers and high achievers) and their learning approaches. Mean sum scores on ASSIST scales and subscales with standard deviations are reported. A p-value ≤0.05 was used for statistical significance.
Results
One hundred thirty basic science medical students participated in the study. There were 61.5% (n=80) low-achieving students and 38.5% (n=50) high-achieving students. Out of 130 students, 38.5% (n=50; 32/18, low/high achievers) were first semester, 31.5% (n=41; 26/15, low/high achievers) second semester, and 30% (n=39; 22/17, low/high achievers) third semester students. The study cohort was balanced in terms of gender distribution, with 50.7% male (n=67; 44/23, low/high achievers) and 49.3% female (n=63; 36/27, low/high achievers) students. The mean age of students was 25.8 years. The response rate of low-achieving and high-achieving students to the ASSIST short-form questionnaire was 100% and 53% (50/95), respectively.
ASSIST Short-Form Scores
Mean sum scores on each scale (deep, surface, and strategic approach) as well as mean sum scores of subscales of each scale are reported (Table 1). Scores for each scale range from 6 to 30. A minimum score of 6 is possible when a student gives a score of 1 on each item of a scale, and a maximum score of 30 can be attained when a student gives a score of 5 to each item of a scale. For subscales, the range of mean scores is 1–5 when a subscale comprises only one item, and 2–10 when a subscale comprises 2 items. A higher mean score on a scale or subscale depicts higher agreement with the theme of the scale or subscale.
 |
Table 1 Comparison of Mean Scores on ASSIST Short-Form Scales and Subscales Between Low-Achieving and High-Achieving Medical Students (n=130) |
Table 1 shows that high-achieving students used the deep and the strategic learning approaches significantly more than low-achieving students (p<0.05). Mean sum scores with standard deviations (M(SD)) on the ASSIST short-form scales of deep approach and strategic approach of low-achieving medical students were 21.72 (3.26) and 22.11 (3.15), respectively, and of high-achieving students were 26.12 (1.64) and 26.61 (1.94), respectively. On the surface approach, low-achieving students scored significantly higher (M(SD), 24.63 (2.7)) than high-achieving students (M(SD), 19.32 (4.09)) (p<0.05)). The difference between ASSIST scores of low- and high-achieving students was significant (p<0.05) for all subscales except subscales of “seeking meaning,” “interest in ideas,” “fear of failure,” and “organized studying.”
Similarly, as shown in Table 2, the low-achieving students of each individual semester (first, second, and third semester) scored significantly lower on the scales of deep and strategic approaches (p<0.05); whereas on the scale of surface approach, they scored significantly greater compared to high-achieving students.
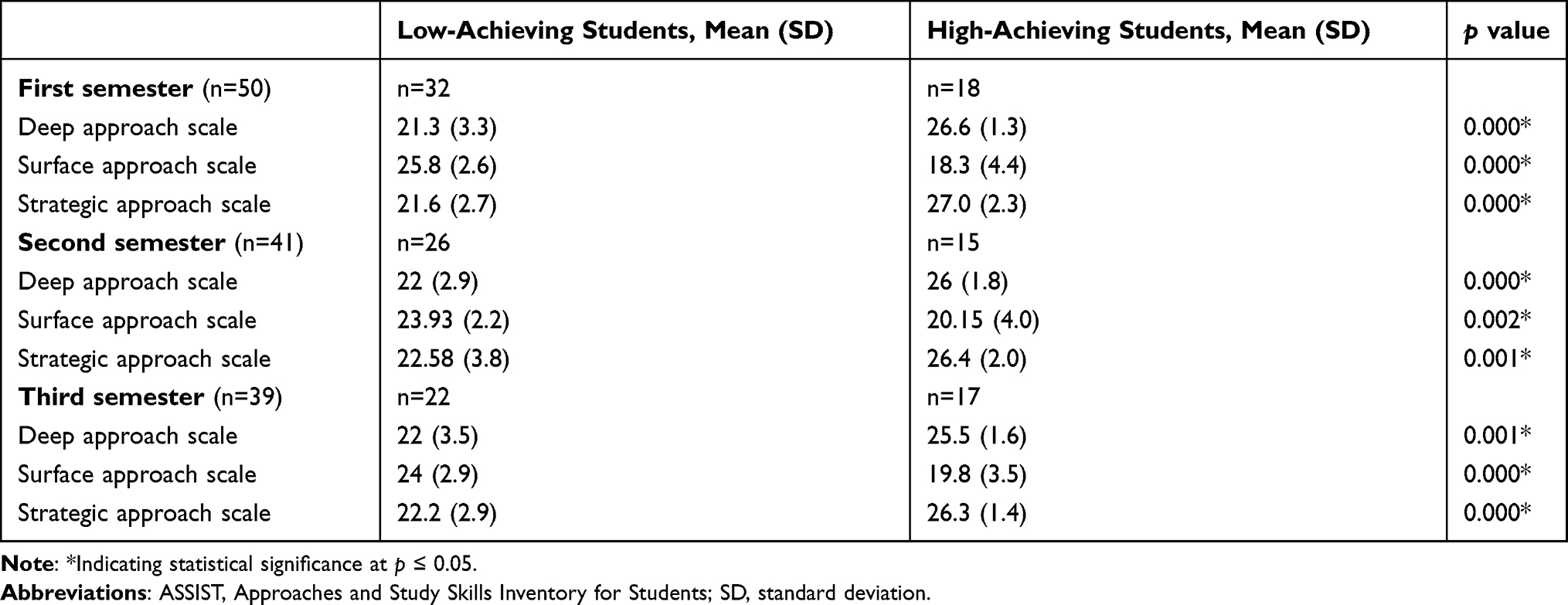 |
Table 2 Comparison of Mean Scores on ASSIST Short-Form Scales Between Low-Achieving and High-Achieving Students of Individual Semesters (First, Second, and Third Semester) (n=130) |
Point-biserial analysis revealed that progression from low to high achievers shows a positive correlation of academic performance with deep and strategic learning approaches, rpb = 0.614 and 0.623, respectively, and a negative correlation with surface approach, rpb= −0.582, with significance level of <0.001.
Female students scored significantly greater (p<0.05) on subscales of “lack of purpose,” “syllabus bound,” “unrelated memorization” (the subscales of surface approach) as well as “time management” and “organized studying” (the subscales of strategic approach) (Table 3).
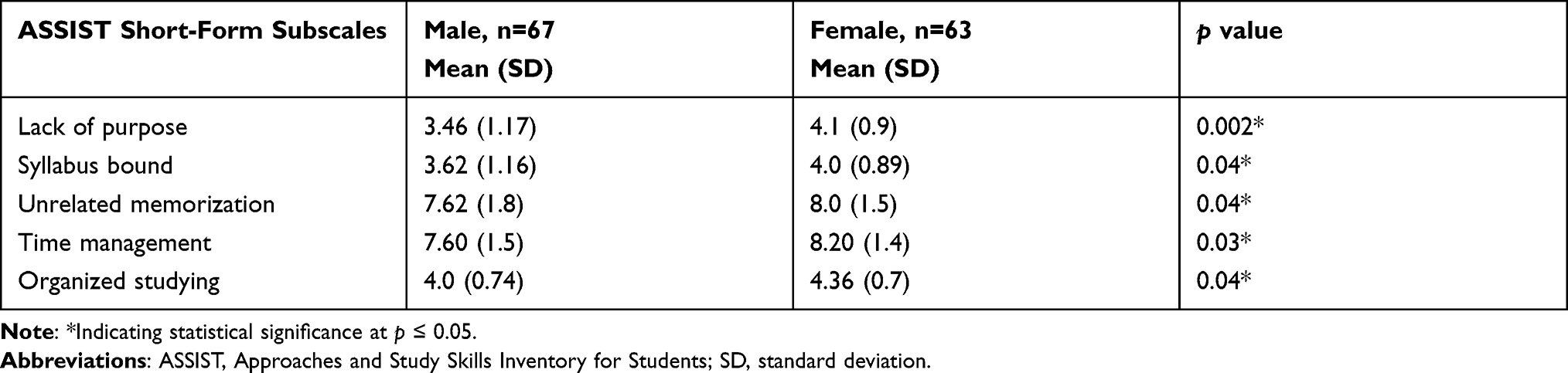 |
Table 3 ASSIST Short-Form Subscales with Significant Gender Differences (n=130) |
Discussion
The present study was conducted to explore learning approaches of low-achieving and high-achieving medical students during their preclinical training with the objective of planning effective interventions that could help low-achieving students to overcome previously utilized ineffective learning approaches.
We found that the use of the deep and the strategic learning approaches was significantly greater among high-achieving medical students. The high-achieving students relied significantly less on the surface approach while low-achieving students leaned predominantly towards the surface approach to learning. Similar differences were found between low-achieving and high-achieving students within each semester (first, second, and third semester). Correlation between academic performance and learning approaches showed increasing preference for deep and strategic learning approaches and decreasing preference for surface learning approach with increasing academic performance. These findings are in line with the results of Trigwell et al.8 In contrast, some studies have reported that students’ learning preferences do not influence their learning outcomes. Sadler-Smith et al reported that a majority of students among the mid-, high- and low-achiever category embraced the deep or the strategic learning approach and there was no significant difference among low- and high-achieving students.22 Similarly, Liew et al reported that learning approaches did not contribute significantly to learning outcomes.4 These findings might be influenced by the type of instructional methods and assessments used in delivering a curriculum.23 A curriculum that ensures a traditional didactic teaching style and assessments that measure only rote memorization skills without deep learning may not show any difference in learning approaches of students with varying academic abilities.24 Moreover, previous studies have shown that students do not use a single static learning approach to learn different subjects.25–27 Our findings suggest that even the high-achieving students use all learning approaches in studying a subject, but what appears to make them high achievers is their predominant preference for the deep and the strategic learning approaches. Using the deep and the strategic learning approaches simultaneously might have helped these students stay on track to complete their assignments efficiently.
Further analysis of subscales of the Approaches and Study Skills Inventory for Students (ASSIST) short-form revealed that high achievers scored greater on all the deep approach subscales, but the difference in scores on subscales of “seeking meaning” and “interest in ideas” between low-achieving and high-achieving students did not reach a statistical significance. While the results suggest that low-achieving students, too, had desire for seeking meaning and had interest in ideas, although less than high achievers, their lack of ability to use evidence and relate ideas in the presence of predominant use of the surface approach might have prevented them from succeeding in academics.
In stark contrast to findings of other studies,1,7,8,10,11,13 our study demonstrated that high-achieving students scored greater on the subscale of “fear of failure,” a subscale of the superficial approach to learning. Martin et al suggested that fear of failure can be divided into two themes, over-striving and self-protection.28 Students with anxiety, low resilience, and vulnerability to learned helplessness tend to be affected negatively by fear of failure. Students with self-belief, control, learning focus, and value of school tend to cope positively with fear of failure.28 We construe that fear of failure can be associated with nonproductive outcomes when standing alone, but when it is present along with traits that are constructive, it can lead to positive outcomes. Fear of failure might be driving high-achieving students in planning their studies meticulously so that they achieve better learning outcomes compared to low-achieving students who seem to be taking the escape pathway to avoid deeper engagement with the study material.
Our study revealed some gender differences in learning approaches. Female students reported significantly better “time management” and “organized studying,” the traits of the strategic approach to learning. Interestingly, female students also reported significantly more “syllabus-bound” study, “lack of purpose,” and “unrelated memorization,” all traits of the surface approach to learning. This shows female students used both the strategic and the surface learning approaches. Chonkar et al found gender differences in learning approaches of medical students attending a clinical posting.24 Their findings were similar to our study’s findings in terms of female students’ preference to utilize the strategic approach. Yet, some other studies have reported no gender difference in learning preferences.29
The Center for Teaching Learning (CTL) of the Ross University School of Medicine designed the Essential Lifelong Learning Skills (ELLS) program for the purpose of addressing learning issues of students and provide timely, appropriate, and mandatory intervention to facilitate students in modifying their learning approaches to achieve favorable learning outcomes. The program helped in providing needs-based interventions to individual students. Knowledge of learning approaches of low-achieving students helped in providing student-tailored support in enhancing their learning outcomes. Administration of the ASSIST short-form questionnaire complemented faculty efforts in making students aware of their existing as well as optimal learning approaches. We emphasize that the practice must not be to blame the struggling student even when other students are doing well.25,30 Learning outcomes, especially of struggling students, can be modified in response to changes made to the learning environment.2,31 Altering teaching practices can lead to increased student use of the deep approach to learning and, consequently, improved grades.32
Our study provides further insights into the field of research on learning approaches. The study’s findings can be helpful in curating medical school curricula and in taking preemptive steps in preventing student failure in academics. Students would benefit if they are made aware of their own learning approaches earliest at the time of matriculating into a medical school. This will help students to know “where they are” and “what they need to achieve” in terms of learning approaches to excel in medical training. In addition, knowing students’ learning approaches would benefit instructors in enhancing their classroom teaching-learning practices to motivate adoption of the deep and the strategic learning approaches by their students, with the goal of improving educational experiences and learning outcomes of all students. Such an approach of continuous quality improvement will be useful in tracking “actions taken” by faculty and students, and the “resulting learning outcomes,” which will further help in making informed and evidence-based interventions and instructional refinements.
Limitations
All low-achieving students succeeded to progress to their next semester. This cross-sectional study did not track how these students performed in higher semesters. It would be beneficial to explore student learning preferences longitudinally to observe the impact of ELLS course and learn how the habit of employing deep approach to learning impacted their academic performance in senior semesters. The sample size of the high achiever group poses another limitation that restricts the generalizability of our findings.
Future Research
As noted, findings of a number of studies on learning approaches from diverse subject areas have not shown unequivocal associations between learning approaches and performance on assessments. It can be useful to design studies in collaboration with educators at different medical schools, nationally and internationally, in generating evidence for clearer directions about the associations between learning approaches and learning outcomes of medical students. It would also be meaningful to extend a similar study to the clinical training and residency period for learning these associations, when students are not so predominantly concerned about securing high grades on assessments.
Conclusions
The results of our study show significant differences in learning approaches of low-achieving and high-achieving medical students in single-institution context. Low achievers are found to use predominantly the surface approach to learning. In contrast, high achievers use mostly the deep and the strategic learning approaches that align with favorable academic outcomes. Our findings suggest that it is worthwhile to examine learning approaches of medical students so that students become aware of their own individual preferred learning approaches early in their medical training rather than to wait until receiving unfavorable academic results. The information may enable students to shed their existing non-effective learning preferences and adopt ones that are more likely to yield successful academic results in medical training. The findings support the need for early detection of inefficient learning approaches and providing education-supporting learning environment to improve academic success of medical students.
Ethical Approval
The Institutional Review Board of Ross University School of Medicine approved the study.
Informed Consent
Informed consent was obtained from each participant before data collection.
Acknowledgments
The authors would like to thank Cynthia Shearer (William L. Adams Center for Writing, Texas Christian University), and Michael Bernas and Lauren Mitchell (TCU and UNTHSC School of Medicine) for their editorial assistance.
Funding
There is no funding to report.
Disclosure
The authors report no financial or other conflicts of interest.
References
1. Hernández-Torrano D, Ali S, Chan CK. First year medical students’ learning style preferences and their correlation with performance in different subjects within the medical course. BMC Med Educ. 2017;17:131. doi:10.1186/s12909-017-0965-5
2. Miller P. Learning styles: the multimedia of the mind. Research Report; 2001 [
3. Cassidy S. Learning styles: an overview of theories, models, and measures. Educ Psychol. 2004;24:419–444. doi:10.1080/0144341042000228834
4. Liew SC, Sidhu J, Barua A. The relationship between learning preferences (styles and approaches) and learning outcomes among pre-clinical undergraduate medical students Approaches to teaching and learning. BMC Med Educ. 2015;15:44. doi:10.1186/s12909-015-0327-0
5. Lujan HL, Dicarlo SE. First-year medical students prefer multiple learning styles. Adv Physiol Educ. 2006;30:13–16. doi:10.1152/advan.00045.2005
6. Marton F, Säljö R. On qualitative differences in learning: outcome and process. Br J Educ Psychol. 1976;46:4–11. doi:10.1111/j.2044-8279.1976.tb02980.x
7. Samarakoon L, Fernando T, Rodrigo C. Learning styles and learning approaches among medical undergraduates and postgraduates. BMC Med Educ. 2013;13:42. doi:10.1186/1472-6920-13-42
8. Trigwell K, Ellis RA, Han F. Relations between students’ learning approaches, experienced emotions and outcomes of learning. Stud High Educ. 2012;37:811–824. doi:10.1080/03075079.2010.549220
9. Sharma DS. Accounting students’ learning conceptions, learning approaches, and the influence of the learning-teaching context on learning approaches. J Acc Educ. 1997;6:125–146. doi:10.1080/096392897331532
10. Reid WA, Evans P, Duvall E. Medical students’ approach to learning over a full degree program. Med Educ Online. 2012;17:1. doi:10.3402/meo.v17i0.17205
11. Shah DK, Yadav RL, Sharma D, et al. Learning approach among health science students in a medical college in Nepal: a cross-sectional study. Adv Med Educ Pract. 2016;7:137–143. doi:10.2147/AMEP.S100968
12. Salamonson Y, Weaver R, Chang S, et al. Learning approaches as predictors of academic performance in first year health and science studies. Nurse Educ Today. 2013;33(7):729–733. doi:10.1016/j.nedt.2013.01.013
13. Diseth Å. Learning approaches, course experience and examination grade among undergraduate psychology students: testing of mediator effects and construct validity. Stud High Educ. 2007;3:373–388. doi:10.1080/03075070701346949
14. Bonsaksen T, Brown T, Lim HB, Fong K, Småstuen MC. Associations between occupational therapy students’ approaches to studying and their academic grade results: a cross-sectional and cross-cultural study. J Occup Ther Educ. 2020;4:5. doi:10.26681/jote.2020.040105
15. Naqvi Z, Ahmed R. Learning approaches and academic performance of undergraduate medical students in Pakistan. J Pak Med Assoc. 2000;50(1):20–25.
16. Bonsaksen T, Brown T, Lim HB, Fong K. Approaches to studying predict academic performance in undergraduate occupational therapy students: a cross-cultural study. BMC Med Educ. 2017;17:76. doi:10.1186/s12909-017-0914-3
17. Calculating sample size: a quick guide. [
18. Speth CA, Namuth DM, Lee DJ. Using the ASSIST short form for evaluating an information technology application: validity and reliability issues. Informing Sci. 2007;10:107–119. doi:10.28945/459
19. Tait H, Entwistle NJ, McCune V. ASSIST: a reconceptualisation of the approaches to studying inventory. In: Rust C, editor. Improving Students as Learners. Oxford: Oxford Brookes University; 1998.
20. Bonsaksen T. Psychometric Properties of the short ASSIST Scale. Uniped; 2018. [
21. Sullivan GM, Artino AR
22. Sadler-Smith E. Approaches to Studying: age, gender and academic performance. Educ Stud. 1996;22:367–379. doi:10.1080/0305569960220306
23. Husmann PR, Gibson DP, Davis EM. Changing study strategies with revised anatomy curriculum: a move for better or worse. Med Sci Educ. 2020;30:1231–1243. doi:10.1007/s40670-020-00998-x
24. Chonkar SP, Ha TC, Chu SSH, et al. The predominant learning approaches of medical students. BMC Med Educ. 2018;18:17. doi:10.1186/s12909-018-1122-5
25. Duff A, McKinstry S. Students’ approaches to Learning. Issues Acc Educ. 2007;22:183–214. doi:10.2308/iace.2007.22.2.183
26. Hodges LC. Teaching Undergraduate Science: A Guide to Overcoming Obstacles to Student Learning.
27. Mirghani HM, Ezimokhai M, Shaban S, van Berkel HJ. Superficial and deep learning approaches among medical students in an interdisciplinary integrated curriculum. Educ Health. 2014;27:10. doi:10.4103/1357-6283.134293
28. Martin AJ, Marsh HW. Fear of failure: friend or foe? Aust Psychol. 2003;38:31–38. doi:10.1080/00050060310001706997
29. Wilson KL, Smart RM, Walton RJ. Gender differences in approaches to learning in first year psychology students. Br J Educ Psychol. 1996;66(1):59–71. doi:10.1111/j.2044-8279.1996.tb01176.x
30. Ramsden P. Learning to Teach in Higher Education.
31. Bansal S, Bansal M, Ahmad K, Pandey J. Effects of a flipped classroom approach on learning outcomes of higher and lower performing medical students: a new insight. Adv Educ Res Eval. 2020;1:24–31. doi:10.25082/AERE.2020.01.005
32. Laird TFN, Seifert TA, Pascarella ET, Mayhew MJ, Blaich C. Deeply affecting first-year students’ thinking: deep learning approaches and three dimensions of cognitive development. J High Educ. 2014;85:402–432. doi:10.1353/jhe.2014.0017
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.