Back to Journals » Patient Related Outcome Measures » Volume 14
Association Between Hematologic Response and Change in Health-Related Quality of Life Among Patients with Light-Chain (AL) Amyloidosis
Authors Rizio AA ![]() , McCausland KL, Carty MK, Conrad A, Quock TP
, McCausland KL, Carty MK, Conrad A, Quock TP ![]()
Received 15 June 2023
Accepted for publication 13 September 2023
Published 10 October 2023 Volume 2023:14 Pages 297—304
DOI https://doi.org/10.2147/PROM.S421211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Avery A Rizio,1 Kristen L McCausland,1 Michelle K Carty,1 Ansgar Conrad,2 Tiffany P Quock2
1QualityMetric Incorporated, LLC, Johnston, RI, USA; 2Prothena Biosciences Inc, South San Francisco, CA, USA
Correspondence: Avery A Rizio, QualityMetric Incorporated, LLC, 1301 Atwood Avenue, Suite 216E, Johnston, RI, 02919, USA, Tel +1 401-903-4631, Email [email protected]
Purpose: The purpose of this secondary data analysis was to examine the association between hematologic response and health-related quality of life (HRQoL) among patients with light-chain (AL) amyloidosis.
Patients and Methods: Data for this secondary analysis were collected through a non-interventional, longitudinal, online self-report survey of patients with AL amyloidosis. Patients completed an initial online survey, with follow-up surveys administered 1, 6, 12, 18, and 24 months after completion of the initial survey. The online survey included an assessment of patients’ most recent self-reported hematologic response status. Eight domains and 2 summary components of HRQoL were evaluated with the SF-36v2® Health Survey. A series of logistic regression models were used to examine the association between self-reported hematologic response at 24 months (dichotomized as new or maintained complete hematologic response; less than a complete response) and change in HRQoL from baseline to 24 months (dichotomized as meaningful worsening; improvement or preservation).
Results: For all measured domains of HRQoL except physical functioning, there was no statistically significant relationship between meaningful worsening in HRQoL and hematologic response status at 24 months. Patients without a complete hematologic response had an odds of experiencing meaningful worsening of HRQoL that was similar to that of patients with a complete hematologic response.
Conclusion: Among patients with AL amyloidosis, change in HRQoL was generally not associated with hematologic response. Achieving a complete hematologic response does not necessarily mean that a patient will experience increased or stable HRQoL. When defining treatment success, it is important to recognize that clinical markers such as hematologic response may not fully encapsulate the patient experience.
Keywords: patient-reported outcomes, SF-36v2, treatment response, primary amyloidosis
Introduction
Light-chain (AL) amyloidosis is a rare disease caused by misfolded protein deposits composed of monoclonal immunoglobulin light-chain fibrils, which are secreted by plasma cells. These amyloid deposits, as well as circulating toxic free light-chains, cause long-term tissue and organ damage, ultimately resulting in death.
Current therapies for AL amyloidosis include stem cell transplant and plasma cell-targeted therapy such as daratumumab and cyclophosphamide, bortezomib, and dexamethasone (CyBorD), or other chemotherapy and steroid combination regimens.1,2 The goal of plasma-cell targeted therapy is the achievement of a complete hematologic response, followed by organ response.3,4 A complete hematologic response is defined as no evidence of monoclonal protein (from serum and urine immunofixation) and a normal free light-chain ratio.5 Little is known about what achieving a complete hematologic response, or not achieving a response, means from the perspective of the patient. The goal of the analysis described here was to examine the association between hematologic response and health-related quality of life (HRQoL), to examine the degree to which this commonly used clinical marker captures the patient experience.
Materials and Methods
Data for this secondary analysis were collected through a non-interventional, longitudinal, online self-report survey of patients with AL amyloidosis. Detailed descriptions of the study methods have been published elsewhere.6,7 All study materials were approved by the New England Independent Review Board (IRB #15–355). Participants were recruited to the study through collaboration with the Amyloidosis Support Groups and the Amyloidosis Foundation. Eligible participants — those who were ≥18 years old and reported having been diagnosed with AL amyloidosis by a physician – completed an initial online survey, with follow-up surveys administered 1, 6, 12, 18, and 24 months after completion of the initial survey. Data collection for the initial survey began in 2015; data collection for the 24-month follow-up survey completed in 2017.
The analytic sample included all patients who completed both initial and 24-month follow-up assessments and were able to self-report their hematologic response at the 24-month follow-up. At each survey administration, participants were asked to select from 4 options that best described their most recent hematologic response status, as described by the specialist treating their AL amyloidosis. Response options included: no response to treatment; partial hematologic response or partial remission; complete hematologic response or complete remission; and I do not know. HRQoL was assessed by the SF-36v2® Health Survey (SF-36v2), which is a 36-item, self-report measure of HRQoL in the past 4 weeks.8 The SF-36v2 produces 8 scale scores (Physical Functioning, Role Limitations due to Physical Health, Bodily Pain, General Health, Vitality, Social Functioning, Role Limitations due to Emotional Health, Mental Health) and 2 component scores that describe overall physical and mental well-being (Physical Component Summary and Mental Component Summary, respectively).8 Published evidence supports the content validity9 and other measurement properties10 of the SF-36v2 in patients with AL amyloidosis, indicating that it is relevant and understandable to this patient population and meets standards for psychometric properties such as reliability, convergent validity, known-groups validity, and responsiveness.
A series of logistic regression models were used to examine the association between hematologic response and HRQoL. The dichotomous independent variable represented hematologic response at the 24-month assessment (new or maintained complete hematologic response; less than a complete response), and the dichotomous dependent variable represented whether the patient had experienced meaningful worsening in HRQoL, as defined by scale-specific responder definition thresholds (meaningful worsening; improvement or preservation).8 One model was built for each of the 8 scales and 2 summary component scores of the SF-36v2. Each model included 4 covariates: patient age, cardiac involvement, history of stem cell transplant, and time since diagnosis. The odds ratios estimating the association between hematologic response and meaningful worsening of HRQoL are interpreted as the odds of experiencing a meaningful worsening of HRQoL between the initial and 24-month assessment among patients without a complete hematologic response (no treatment response or less than a complete response) versus those with a complete response (either newly reported or maintained since the initial assessment).
Results
Details regarding the creation of the analytic sample (N = 175) are provided in Figure 1A; demographic and clinical characteristics of the sample are provided in Table 1. At the initial assessment, patients were, on average, 60.5 years old, and had been diagnosed with AL amyloidosis 4.6 years ago. Approximately half of the sample had cardiac involvement (49.1%); 44% had 3 or more organs affected by the disease. At month 24, 107 patients had a newly achieved or maintained complete hematologic response, while the remaining 68 patients had less than a complete response. As shown in Figure 1B, most of the patients who were categorized as having a complete response at month 24 also had a complete response at the initial survey (ie maintained complete response; N = 78), though some patients moved from having a partial response at baseline to a complete response by month 24 (ie newly reported complete response; N = 23). Six patients did not know their hematologic response at the initial survey but reported a complete response at month 24. Characteristics such as patient age, time since diagnosis, cardiac involvement, and number of treatment series received (at initial assessment) were similar across groups defined by hematologic response.
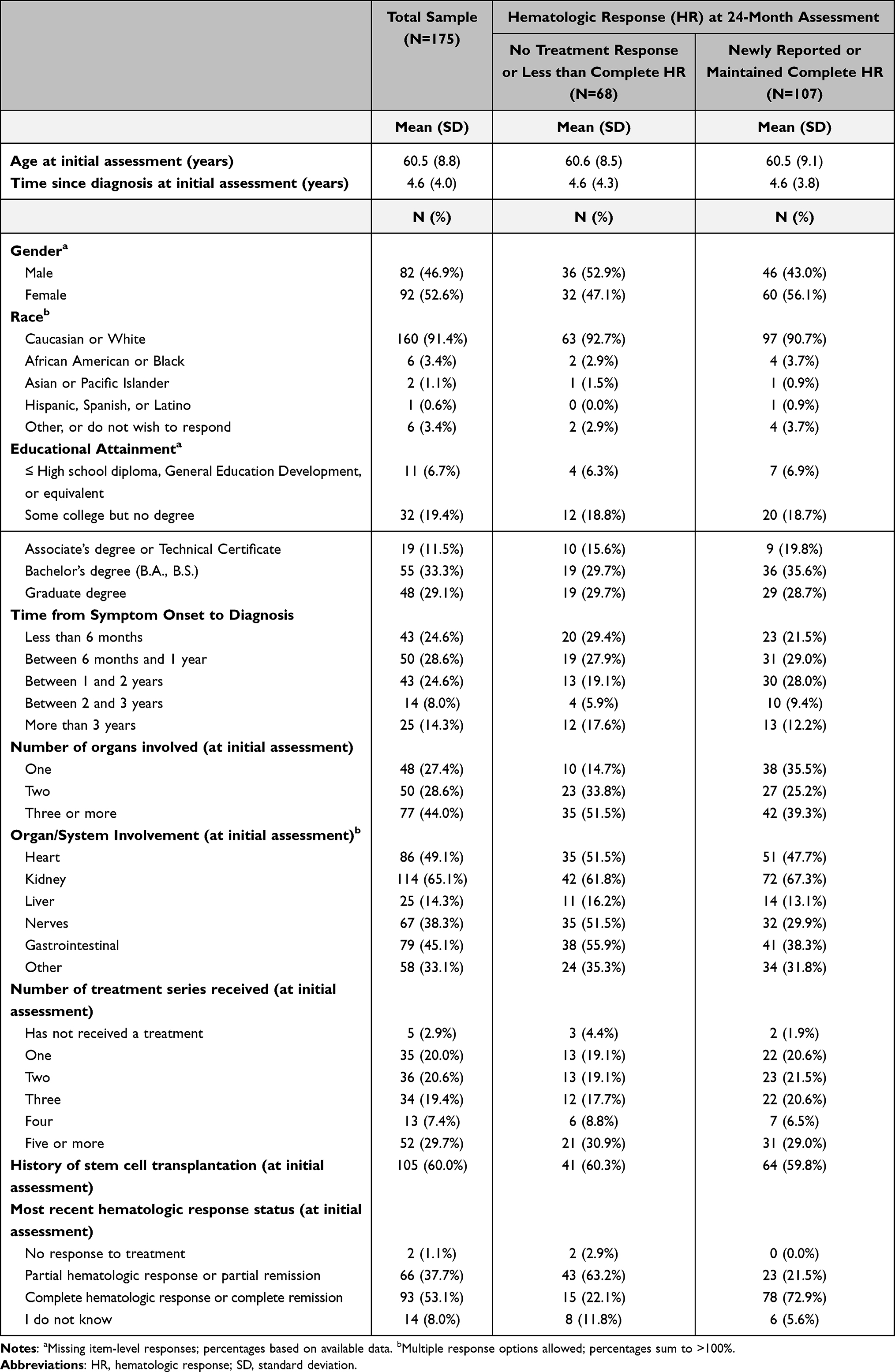 |
Table 1 Demographic and Clinical Characteristics of Analytic Sample by Patient-Reported Hematologic Response at 24-Month Assessment |
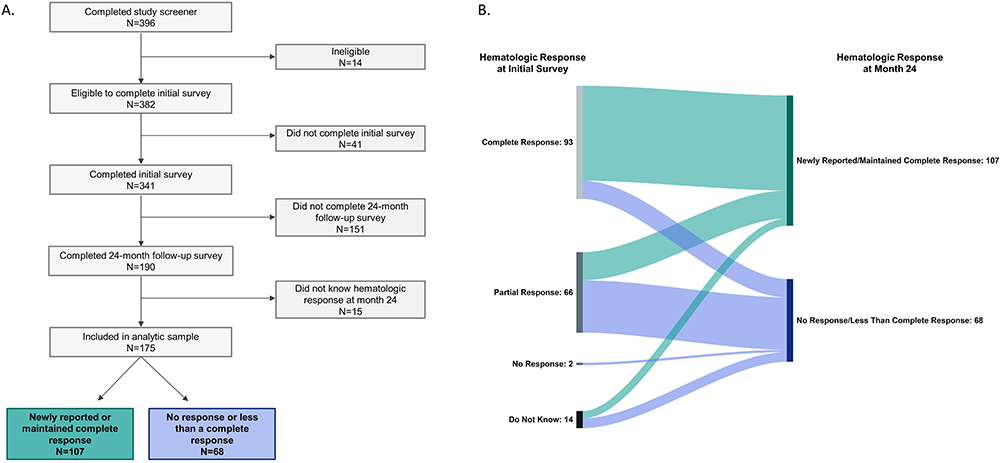 |
Figure 1 Flowchart of Participant Disposition. (A) Derivation of the analytic sample based on completion of initial and 24-month follow-up surveys. (B) Hematologic response to treatment at month 24, stratified according to self-reported hematologic response to treatment at the initial survey. |
Odds ratios estimating the association between hematologic response and meaningful worsening of HRQoL are depicted in Figure 2 along with 95% confidence intervals (CIs) and p-values. Patients without a complete hematologic response had a 2.24 greater odds of experiencing meaningful worsening on the Physical Functioning scale than patients with a complete hematologic response (p = 0.047, 95% CI: 1.01–4.94). Patients without a complete hematologic response had a 2.25 greater odds of experiencing meaningful worsening on the General Health scale than patients with a complete hematologic response, though this effect estimate did not reach statistical significance (p = 0.056, 95% CI: 0.98–5.16). For the remainder of the SF-36v2 scales and component scores, there was no statistically significant relationship between meaningful worsening in HRQoL and hematologic response status. Patients without a complete hematologic response had an odds of experiencing meaningful worsening of HRQoL that was equal to that of patients with a complete hematologic response. For example, patients without a complete hematologic response only had a 1.59 greater odds of experiencing meaningful worsening on role limitations due to physical health (Role Physical scale); this estimate was not statistically significant (p = 0.210, 95% CI: 0.77–3.27). Likewise, patients without a complete hematologic response only had a 1.38 greater odds of experiencing meaningful worsening on the Vitality scale than patients with a complete hematologic response; this estimate was not statistically significant (p = 0.468, 95% CI: 0.58–3.29).
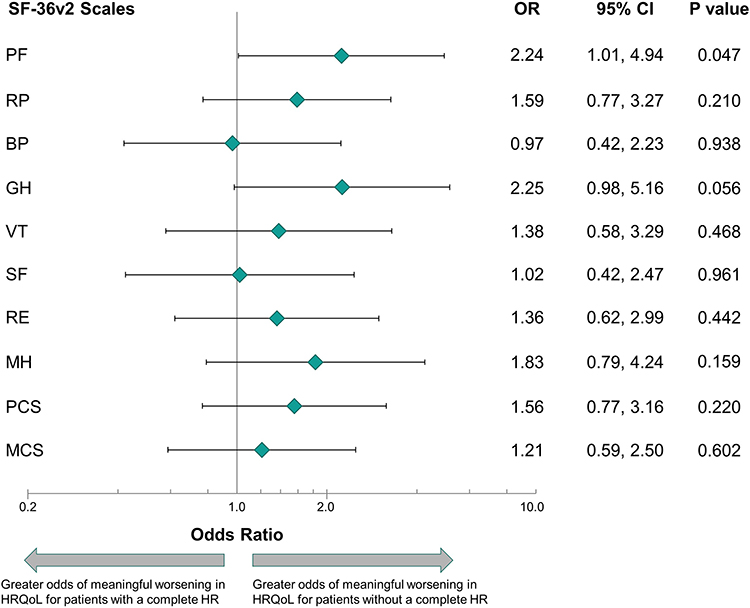 |
Figure 2 Association Between Clinically Meaningful Worsening of Health-Related Quality of Life During 24 Months of Observation and Patient-Reported Hematologic Response Status. Logistic models controlled for age, cardiac involvement, history of stem cell transplant, and duration of disease (ie, time since diagnosis). Odds ratios are interpreted as the odds of clinically meaningful worsening between the initial and 24-month assessment among patients without complete hematologic response (no treatment response or less than a complete response) versus those with newly reported or maintained complete response. Abbreviations: CI, confidence interval; HR, hematologic response; HRQoL, health-related quality of life; OR, odds ratio; SF-36v2, SF-36v2® Health Survey SF-36v2 scales, in order of appearance; PF, Physical Functioning; RP, Role-Physical; BP, Bodily Pain; GH, General Health; VT, Vitality; SF, Social Functioning; RE, Role-Emotional; MH, Mental Health; PCS, Physical Component Summary; MCS, Mental Component Summary. |
Discussion
The results of this analysis indicate that the odds of decline in HRQoL are not well-associated with hematologic response; achieving a complete hematologic response does not confer greater protection from the possibility of experiencing declines in HRQoL. These results help contextualize the potential limitations to defining treatment success based only on hematologic markers, as they may not adequately reflect the entirety of the patient’s health and well-being.
In developing new treatments for AL amyloidosis, selection of outcomes to best evaluate treatment success is critical. Outcomes measured in prior clinical trials to evaluate efficacy of treatments for AL amyloidosis have included survival, organ response, hematologic response, and HRQoL.11 Results of the analyses presented here indicate that while those who do not achieve a complete hematologic response are at greatest risk of experiencing meaningful declines in physical functioning, they are not at a greater risk of experiencing meaningful declines in other aspects of HRQoL, as compared to those who do achieve a complete response. Because HRQoL is a multifaceted outcome that incorporates several different concepts, a full understanding of the patient experience should not focus on a single domain. Thus, the finding related to an association between hematological response and declines in physical functioning must be considered in conjunction with findings for the other 7 domains of HRQoL measured by the SF-36v2. Specifically, those who do achieve a complete response are at equal risk of experiencing declines in other areas of HRQoL as compared to those who do not achieve a complete response. These domains include Role Limitations (due to both physical and emotional problems), Bodily Pain, Vitality, Social Functioning, and Mental Health, and have been identified previously as being important to patients and impacted by AL amyloidosis.9,12 Declines in HRQoL despite achieving a complete hematologic response could be caused by a variety of factors, including treatment-related toxicity, persisting effects of organ damage/delayed organ response to treatment, or concerns about an uncertain or changing future. The influence of such factors suggests that the timescales over which different outcomes show improvement are likely not the same, with HRQoL outcomes slower to show improvement than clinical outcomes. This may account for differences in published patterns of change among patients receiving specific treatments,13–15 and suggests the need for more research on the time course of treatment-related changes in HRQoL among patients with AL amyloidosis. For example, in a recent analysis of newly diagnosed patients with AL amyloidosis, all patients, regardless of hematologic response status, reported an initial decline in most HRQoL outcomes (as measured by the SF-36v2) within 3 months of treatment initiation; however, by month 12, patients with a complete response reported improvements in the Physical Functioning, Role Limitations due to Physical Health, and Social Functioning domains, and these improvements exceeded the established responder definition thresholds for clinically meaningful change by month 24.15 It is possible that HRQoL outcomes are sensitive to the timing of treatment and to the overall composition of the sample (eg, time since diagnosis). Thus, findings that at first may appear incongruous instead signal important factors that may contribute to different outcomes among patients, further highlighting the importance of continued research in this area.
Our study is limited by the use of self-reported hematologic response. However, requiring clinician confirmation or input would likely have reduced the study’s initial sample size and contributed to attrition at follow-up. Participants were able to indicate that they did not know their hematologic response rather than being forced to provide an answer; those who did not know their status at month 24 were excluded from the analysis. In the analysis, a dichotomous variable was created, collapsing across those who had not responded at all to treatment and those who had a very good, but not complete, response. Though this created a heterogeneous group, it was determined to be the best strategy given the available sample size. Our study cohort likely represents healthier long-term survivors and may underrepresent the extent of decline in HRQoL experienced by patients who do not respond to treatment.
In the future, additional research might seek to examine the association between change in HRQoL and organ-specific response, which was outside the scope of the current analysis. Such analyses might clarify whether delays in achieving organ response contributed to the risk of decline observed among patients who had achieved a complete response. Given that most patients with a complete hematologic response had maintained this response for 24 months, however, other possibilities should also be explored. While this study presents findings related to a relatively heterogeneous sample of patients who were at different stages in their treatment journey, future work may also examine patterns among specific subgroups of patients defined by treatment history.
These findings are of importance as they indicate that while treatment may have been deemed successful from a hematologic perspective, even patients who have achieved a complete response may still be at risk for declines in HRQoL and require additional therapeutic intervention and support. In seeking to identify treatment-related change, it is important to consider whether the typical duration of a clinical trial is too short to assess meaningful change in certain domains of HRQoL that are more distal to the treatment’s direct effects. These findings can also inform selection of endpoints for clinical trials and serve as a reminder that a single clinical outcome is unlikely to fully capture the complexities or nuances of the patient-reported experience. As such, the definition of “treatment success” should incorporate measures of HRQoL to evaluate aspects of the disease experience that are important to patients that may not be reflected in clinical disease markers such as hematologic status.
Conclusion
The findings from this analysis call attention to the importance of measuring HRQoL among patients with AL amyloidosis, even among patients who have achieved complete hematologic response. The findings also illustrate the importance of evaluating outcomes from a variety of perspectives, including that of the patient.
Abbreviations
AL, amyloidosis, light-chain amyloidosis; CI, confidence interval; HRQoL, health-related quality of life; SF-36v2, SF-36v2® Health Survey.
Ethics Approval and Informed Consent
All procedures involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The informed consent forms, protocols, surveys, and interview guide were approved by the New England Independent Review Board (# 15-355). All participants provided consent.
Acknowledgments
We would like to thank the Amyloidosis Support Groups and the Amyloidosis Foundation for their help in patient outreach, and each of the patients who offered their time and insight for this project.
Disclosure
AC is an employee of and TPQ is a former employee of Prothena Bioscience Inc and both are stockholders of Prothena Corporation plc. AAR, KLM, and MKC are employees of QualityMetric Incorporated, LLC, and received funding from Prothena to conduct this research. QualityMetric owns the copyright to and receives licensing fees for the use of the SF-36v2® Health Survey. The authors report no other conflicts of interest in this work.
References
1. Gertz MA. Immunoglobulin light chain amyloidosis: 2020 update on diagnosis, prognosis, and treatment. Am J Hematol. 2020;95(7):848–860. doi:10.1002/ajh.25819
2. Mayo Clinic. Mayo consensus on AL amyloidosis: diagnosis, treatment, and prognosis; 2020. Available from: https://www.msmart.org/.
3. Palladini G, Milani P, Merlini G. Management of AL amyloidosis in 2020. Hematology Am Soc Hematol Educ Program. 2020;2020(1):363–371. doi:10.1182/hematology.2020006913
4. Sanchorawala V. Summary of the EHA-ISA Working Group guidelines for high-dose chemotherapy and stem cell transplantation for systemic AL amyloidosis. Hemasphere. 2022;6(2):e681. doi:10.1097/HS9.0000000000000681
5. Palladini G, Dispenzieri A, Gertz MA, et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes. J Clin Oncol. 2012;30(36):4541–4549. doi:10.1200/JCO.2011.37.7614
6. Bayliss M, McCausland KL, Guthrie SD, White MK. The burden of amyloid light chain amyloidosis on health-related quality of life. Orphanet J Rare Dis. 2017;12(1):15. doi:10.1186/s13023-016-0564-2
7. McCausland KL, Rizio AA, White MK, Bayliss MS, Quock TP. Associations between health-related quality of life and self-reported emergency room department visits and inpatient hospitalizations: insights from a secondary data analysis of patients with Light-Chain (AL) Amyloidosis. Pharmacoecon Open. 2019;3(3):367–375. doi:10.1007/s41669-019-0122-7
8. Maruish ME. User’s Manual for the SF-36v2 Health Survey.
9. White MK, Bayliss MS, Guthrie SD, Raymond KP, Rizio AA, McCausland KL. Content validation of the SF-36v2® health survey with AL amyloidosis patients. J Patient Rep Outcomes. 2017;1(1):13. doi:10.1186/s41687-017-0020-7
10. White MK, McCausland KL, Sanchorawala V, Guthrie SD, Bayliss MS. Psychometric validation of the SF-36 Health Survey in light chain amyloidosis: results from community-based and clinic-based samples. Patient Relat Outcome Meas. 2017;8:157–167. doi:10.2147/PROM.S146849
11. Popkova T, Hajek R, Jelinek T. Monoclonal antibodies in the treatment of AL amyloidosis: co-targetting the plasma cell clone and amyloid deposits. Br J Haematol. 2020;189(2):228–238. doi:10.1111/bjh.16436
12. Lin HM, Seldin D, Hui A-M, Berg D, Dietrich CN, Flood E. The patient’s perspective on the symptom and everyday life impact of AL amyloidosis. Amyloid. 2015;22(4):244–251. doi:10.3109/13506129.2015.1102131
13. Seldin DC, Anderson JJ, Sanchorawala V, et al. Improvement in quality of life of patients with AL amyloidosis treated with high-dose melphalan and autologous stem cell transplantation. Blood. 2004;104(6):1888–1893. doi:10.1182/blood-2004-01-0089
14. Carter J-P, Foard D, Rannigan L, et al. A good clonal response to chemotherapy in AL amyloidosis is associated with improved quality of life and function at 1 year. Amyloid. 2017;24(sup1):72–73. doi:10.1080/13506129.2017.1295944
15. Cohen O, Rendas-Baum R, McCausland K, et al. Linking changes in quality of life to haematologic response and survival in systemic immunoglobulin light-chain amyloidosis. Br J Haematol. 2023;201(3):422–431. doi:10.1111/bjh.18645
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.