Back to Journals » Journal of Inflammation Research » Volume 19
Association Between Admission Prognostic Nutritional Index and Pulmonary Infection Status in Hospitalized Lung Cancer Patients: A Retrospective Cohort Study
Authors Wang X, Fang X, Li T, Gao Y, Gao Y, Zhu Y
Received 19 January 2026
Accepted for publication 20 March 2026
Published 12 April 2026 Volume 2026:19 594032
DOI https://doi.org/10.2147/JIR.S594032
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Junhao Wang
Xiaowu Wang,1,2 Xiaoyu Fang,3 Tuantuan Li,1,2 Yong Gao,1,2 Yuxin Gao,4 Yilang Zhu1,2
1Department of Clinical Laboratory, The Second People’s Hospital of Fuyang City, Fuyang, People’s Republic of China; 2Department of Clinical Laboratory, Fuyang Infectious Disease Clinical College of Anhui Medical University, Fuyang, People’s Republic of China; 3Department of Pharmacy, Jieshou City People’s Hospital, Fuyang, People’s Republic of China; 4Department of Biostatistics-Data Science of Health, UCLA Fielding School of Public Health, Los Angeles, CA, 90024, USA
Correspondence: Yilang Zhu, The Second People’s Hospital of Fuyang City, No. 1088, West Yinghe Road, Fuyang, Anhui, People’s Republic of China, Email [email protected] Yuxin Gao, Departments of Biostatistics-Data Science of Health, UCLA Fielding School of Public Health, Los Angeles, CA, 90024, USA, Email [email protected]
Objective: To evaluate the association of the admission Prognostic Nutritional Index (PNI) with concomitant pulmonary infection and in-hospital mortality in hospitalized lung cancer patients.
Methods: In this retrospective cohort study, 417 lung cancer patients admitted between December 2022 and November 2023 were categorized into those with (n=218) and without (n=199) concomitant pulmonary infection based on clinical, radiological, and microbiological evidence within 48 hours of admission. The PNI and other inflammatory indices, including the systemic immune-inflammation index (SII), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR), were calculated from admission laboratory data. Multivariable logistic regression [adjusted for age, sex, cancer stage, chronic obstructive pulmonary disease (COPD), etc.] and receiver operating characteristic (ROC) analyses were used.
Results: Patients with concomitant pulmonary infection had significantly lower PNI (median: 45.03 vs. 47.25, P < 0.001) and higher SII (median: 724.00 vs. 448.00, P < 0.001) compared to those without infection. Lower PNI (aOR: 0.964, 95% CI: 0.942– 0.986) and higher SII (aOR: 1.001, 95% CI: 1.000– 1.001) were independently associated with concomitant infection. Among infected patients, non-survivors had significantly lower PNI (mean: 39.85 vs. 46.67, P < 0.001) and higher MLR (median: 0.50 vs. 0.32, P < 0.001) compared to survivors. Lower PNI (aOR: 0.854, 95% CI: 0.796– 0.916) and higher MLR (aOR: 1.377, 95% CI: 1.026– 1.849) were independently associated with in-hospital mortality. The combination of PNI and MLR achieved an AUC of 0.806 (95% CI: 0.747– 0.857) for mortality discrimination.
Conclusion: Admission PNI is significantly associated with concomitant pulmonary infection and independently associated with in-hospital mortality in infected lung cancer patients. Combining PNI with SII or MLR may enhance risk stratification and nutritional-immunological assessment in this vulnerable population.
Keywords: lung cancer, pulmonary infection, prognostic nutritional index, nutritional status, inflammation, in-hospital mortality
A Letter to the Editor has been published for this article.
Introduction
Lung cancer represents one of the most prevalent malignancies globally and constitutes a leading cause of cancer-related mortality, with an estimated 2 million new cases and 1.76 million deaths annually.1 Approximately 50–70% of lung cancer patients develop pulmonary infections during their disease course, often presenting at the time of hospitalization. However, early identification of infection status is frequently challenging, potentially attributable to impaired immune competence and an attenuated inflammatory response, which may obscure typical clinical signs of infection.2 Pathogens implicated in pulmonary microbial infections among lung cancer patients encompass fungi, bacteria, viruses, mycoplasma, and others. Nevertheless, current etiological detection methods exhibit limitations in timely confirmation, and definitive pathogen identification remains technically constrained.3 Studies indicate that cancer patients with concurrent pulmonary bacterial infection exhibit significantly higher mortality rates than those without.4 Moreover, non-surgical cancer patients frequently receive radiotherapy, which may contribute to immunosuppression and increase susceptibility to invasive fungal infections, further elevating cancer-associated mortality.5
The Prognostic Nutritional Index (PNI), a composite of serum albumin and lymphocyte count, integrates nutritional and immunological status and has been widely studied as a prognostic factor in various malignancies, including lung cancer.6,7 However, the specific association of PNI with pulmonary infection status at hospital admission, and with outcomes in infected lung cancer patients, remains underexplored.
Currently, several biomarkers are used to predict infection or prognosis in lung cancer patients, such as procalcitonin (PCT), C-reactive protein (CRP), and various interleukins.8–10 While these markers reflect systemic inflammation, they have notable limitations. PCT and CRP are acute-phase reactants that may be elevated in non-infectious inflammatory conditions (eg, post-surgery, post-chemotherapy), limiting their specificity.11 More importantly, these markers do not capture the patient’s nutritional status, which is a critical determinant of immune competence and infection susceptibility. Hypoalbuminemia, a key component of PNI, is a well-established predictor of poor outcomes in cancer patients,12 reflecting both malnutrition and chronic inflammation. Similarly, lymphopenia indicates impaired adaptive immunity.13,14 Thus, existing biomarkers may not fully integrate the dual dimensions of nutrition and immunity that are essential for risk stratification in this vulnerable population.
Given the well-established links between malnutrition, immune dysfunction, and infection susceptibility,15 we hypothesized that a lower admission PNI would be associated with a higher likelihood of concomitant pulmonary infection. Furthermore, among infected patients, we hypothesized that lower PNI would predict increased in-hospital mortality. Therefore, this study aimed to investigate whether this simple immunonutritional index could aid in risk stratification for pulmonary infection and mortality in hospitalized lung cancer patients.
Materials and Methods
Study Design and Participants
This retrospective cohort study adhered to the Declaration of Helsinki and was approved by the Medical Ethics Committee of The Second People’s Hospital of Fuyang City (Approval No: 20251204132). The requirement for informed consent was waived because of the retrospective nature of the study. All patient information and data used in this study were handled with strict confidence and de-identified to protect patient privacy in compliance with the relevant ethical and legal standards. We screened 455 consecutive adult patients with a discharge diagnosis of lung cancer admitted to the Department of Respiratory Infection between December 2022 and November 2023. After excluding 38 patients due to readmission (n=25), incomplete clinical data (n=7), or other exclusion criteria (n=6), a total of 417 patients were included in the final analysis. Patients were classified according to the presence or absence of concomitant pulmonary infection at admission, as defined below. Data on pathogen identification were extracted from electronic medical records, where they had been documented as part of routine clinical care. For bacterial and fungal identification, respiratory specimens were processed by the hospital’s clinical microbiology laboratory using culture and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). For mycoplasma and respiratory viruses, polymerase chain reaction (PCR) assays were performed. A flow diagram of patient selection and grouping is presented in Figure 1.
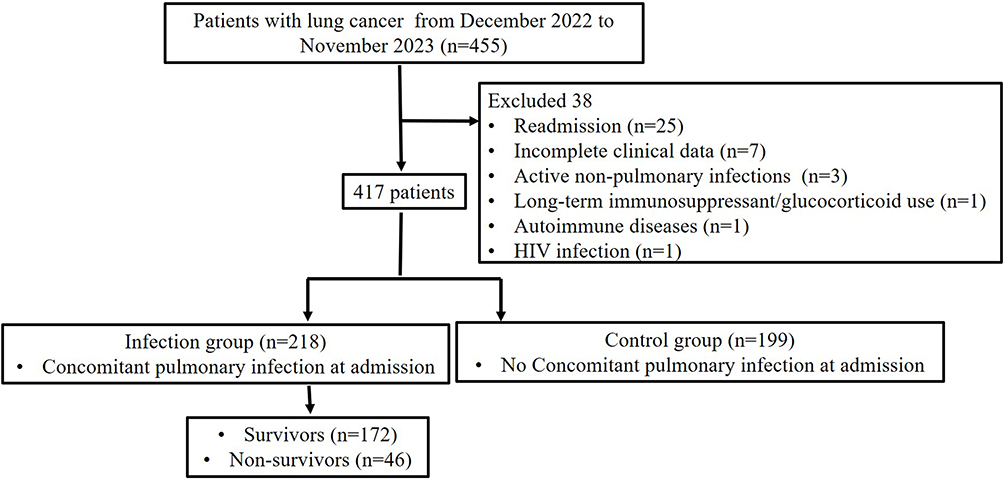 |
Figure 1 Flow diagram of patient selection and grouping. |
Definition of Exposure and Outcomes
Concomitant Pulmonary Infection (Primary Exposure): Patients were classified as having a concomitant pulmonary infection if they met predefined clinical, radiological (new or progressive infiltrates on chest imaging), and microbiological criteria within the first 48 hours of admission. Accordingly, 218 patients were assigned to the infection group and 199 to the control group.
In-Hospital Mortality (Primary Outcome): Among patients with concomitant infection, the primary outcome was all-cause in-hospital mortality. Within the infected group, patients were further stratified by discharge outcome into non-survivors (n=46) and survivors (n=172).
Inclusion and Exclusion Criteria
Inclusion criteria: pathologically confirmed lung cancer [International Association for the Study of Lung Cancer (IASLC) criteria] and pulmonary infection meeting established diagnostic criteria.
Exclusion criteria: missing/incomplete data, unclear etiology, or active non-pulmonary infections.
Data Collection
Clinical and laboratory data were extracted from Hospital Information System (HIS) and Laboratory Information System (LIS). Laboratory parameters (serum albumin, lymphocyte, neutrophil, monocyte, and platelet counts) were collected within 48 hours of admission to reflect baseline status. The following indices were calculated:
- PNI = albumin (g/L) + 5 × lymphocyte count (×109/L)
- NLR = neutrophil count / lymphocyte count
- MLR = monocyte count / lymphocyte count
- PLR = platelet count / lymphocyte count
- SII = neutrophil count × platelet count / lymphocyte count
Statistical Analysis
Analyses were performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA) and MedCalc (MedCalc Software Ltd., Ostend, Belgium). SPSS was used for descriptive statistics, Mann–Whitney U-tests, chi-square tests, and multivariable logistic regression analyses (both enter method and forward likelihood ratio selection). MedCalc was employed for receiver operating characteristic (ROC) curve analysis, including calculation of area under the curve (AUC), optimal cut-off values, sensitivity, specificity, and comparison of ROC curves. Multivariable logistic regression models were constructed to assess independent associations. Covariates were selected based on clinical relevance and established associations with infection risk or mortality in lung cancer patients, as identified in prior literature.16–18 For the model analyzing infection status, covariates included age, sex, smoking history, pathological type, chronic obstructive pulmonary disease (COPD), lymph node metastasis, and treatment modalities (chemotherapy, radiotherapy, targeted therapy, immunotherapy, and nutritional support). For the model analyzing in-hospital mortality among infected patients, covariates included age, sex, smoking history, pathological type, and treatment modalities (chemotherapy, radiotherapy, targeted therapy, immunotherapy, and nutritional support). PNI, SII, NLR, PLR, and MLR were entered into the models as continuous variables. All covariates were entered simultaneously into the full multivariable models (Supplementary Tables S1 and S2). Variable selection for the final parsimonious models was performed using the forward likelihood ratio (LR) method. Results are presented as adjusted odds ratios (aOR) with 95% confidence intervals (CI). ROC curve analysis was performed to evaluate the discriminative ability of the indices and their combinations for concomitant infection and in-hospital mortality. Since the primary outcome was in-hospital mortality, a binary event occurring during hospitalization and the follow-up period was limited to the hospital stay, traditional ROC analysis was deemed appropriate for assessing the discriminative ability of baseline markers for this binary outcome. Time-dependent ROC analysis and Cox proportional hazards models, which are designed for time-to-event data, were not applicable to our study design. Although no formal sample size calculation was performed a priori, the sample size (N=417) satisfied the events-per-variable (EPV) criterion (>10) for both logistic regression models,18 ensuring model stability.
Results
Baseline Characteristics
Baseline characteristics of the study population are summarized in Table 1. The median age was 69 years in both groups (IQR: 60–75 in infection group vs. 60–74 in control group, P=0.664), and the proportion of female patients was similar between groups (28.44% vs. 28.14%, P=0.946). The prevalence of comorbidities including hypertension (26.61% vs. 26.63%, P=0.995), diabetes (10.55% vs. 13.57%, P=0.368), cardiovascular disease (24.77% vs. 27.64%, P=0.506), and COPD (24.31% vs. 28.64%, P=0.320) did not differ significantly between the infection and control groups. However, patients with concomitant pulmonary infection had a significantly longer median hospital stay (9 vs. 5 days, P<0.001). Regarding tumor characteristics, the infection group had a lower proportion of lymph node metastasis (39.91% vs. 51.26%, P=0.024) and a different distribution of pathological types (P=0.03). Smoking status was comparable between groups (P=0.121). Notably, patients in the control group were more likely to have received chemotherapy (59.30% vs. 26.15%, P<0.001), while no significant differences were observed for radiotherapy, targeted therapy, immunotherapy, or nutritional support.
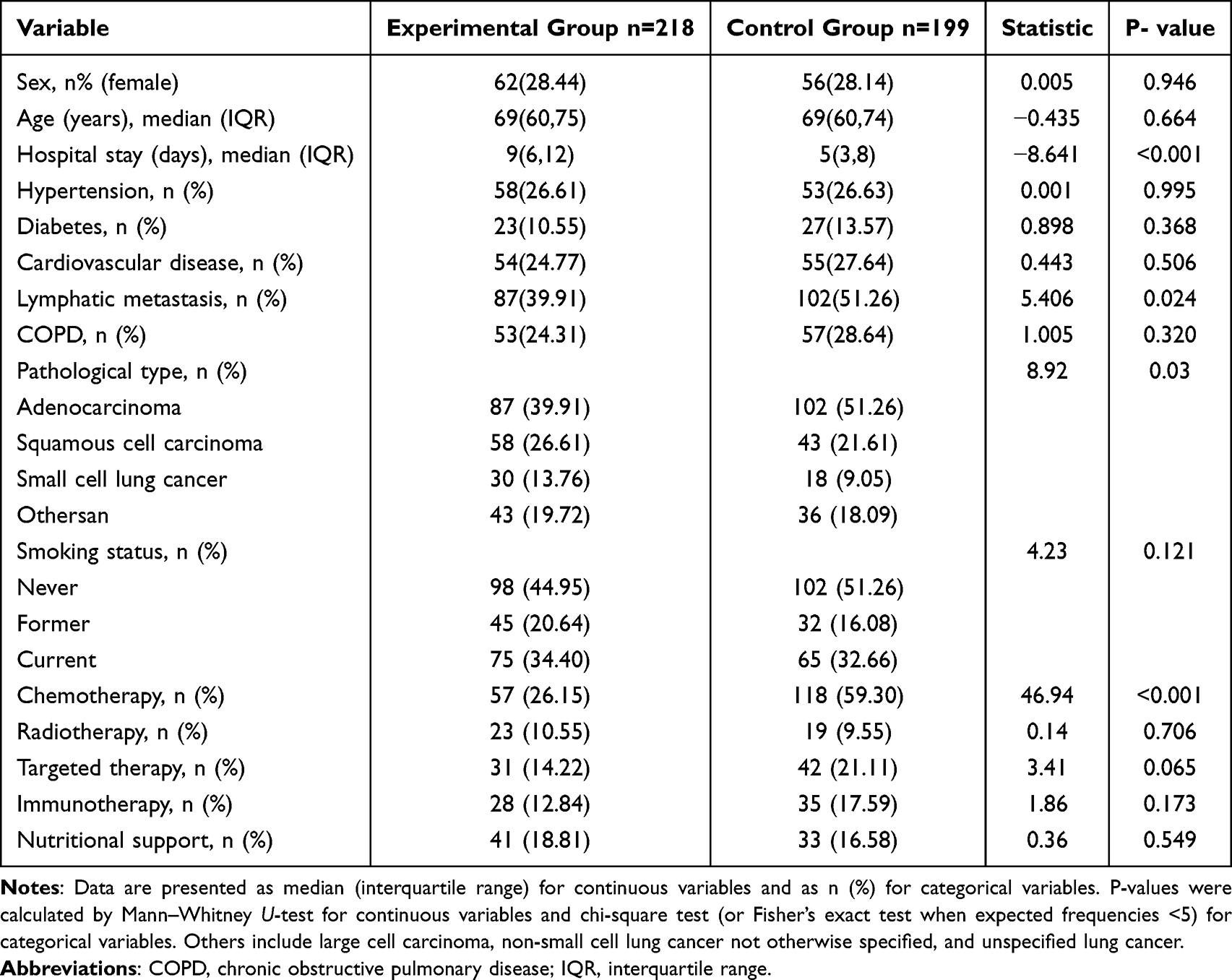 |
Table 1 Baseline Characteristics of Lung Cancer Patients Stratified by Concomitant Pulmonary Infection Status |
Microbiological and Radiological Characteristics of Infected Patients
Among the 218 patients with concomitant pulmonary infection, radiological evidence (new or progressive infiltrates on chest imaging) was present in 218 patients (100.00%). Microbiological confirmation was obtained in 153 patients (70.18%), including bacterial infections (110, 50.46%), fungal infections (10, 4.59%), viral infections (20, 9.17%), and mixed infections (13, 5.96%). The remaining patients were diagnosed based on clinical and radiological criteria in the absence of pathogen identification.
Association Between Admission Indices and Concomitant Infection
Compared to the control group, the infection group had significantly lower PNI and higher NLR, PLR, MLR, and SII levels (all P<0.05; Table 2). In the fully adjusted multivariable model (Supplementary Table S1), lower PNI aOR: 0.964, 95% CI: 0.942–0.986, P=0.002 and higher SII aOR: 1.001, 95% CI: 1.000−1.001, P<0.001 remained independently associated with concomitant infection. The final parsimonious model containing only these two significant variables is shown in Table 3.
 |
Table 2 Comparison of Laboratory Indicators Between Experimental and Control Groups |
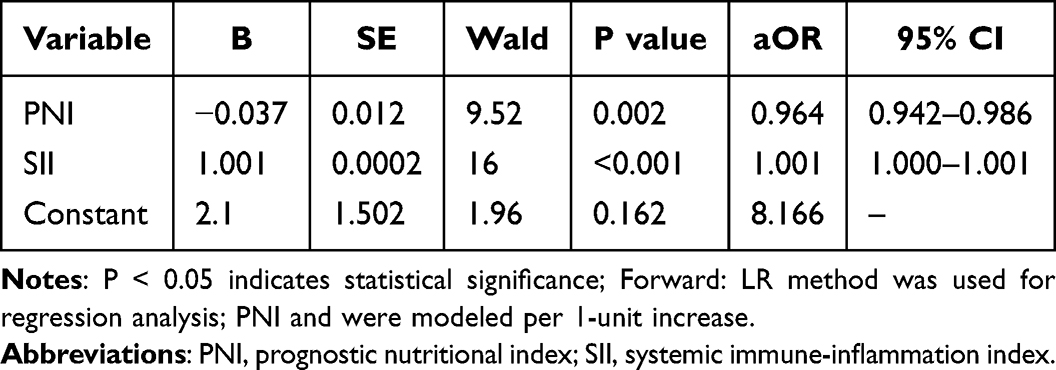 |
Table 3 Parsimonious Multivariable Model for Concomitant Pulmonary Infection |
Association Between Admission Indices and In-Hospital Mortality in Infected Patients
Among the 218 patients with concomitant infection, 46 (21.1%) died during hospitalization. Compared to survivors, non-survivors had significantly lower PNI and higher NLR, PLR, MLR, and SII (all P<0.01) (Table 4). In the fully adjusted multivariable model for mortality (Supplementary Table S2), lower PNI (aOR: 0.854, 95% CI: 0.796–0.916, P<0.001) and higher MLR (MLR (aOR: 1.377, 95% CI: 1.026–1.849) were independently associated with in-hospital mortality. The final parsimonious model is shown in Table 5.
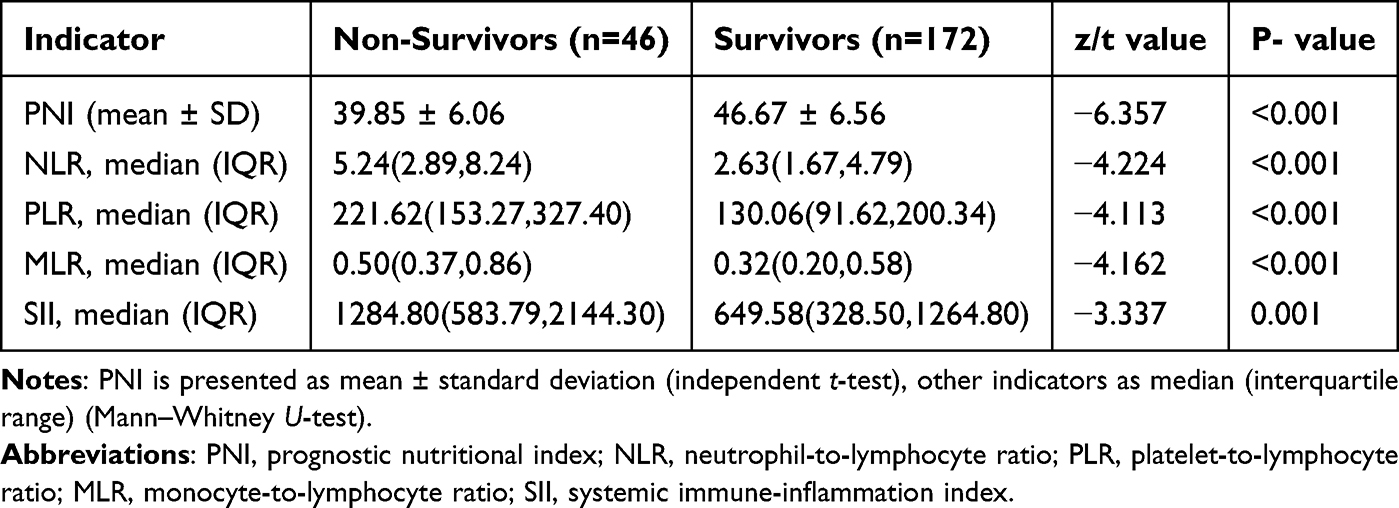 |
Table 4 Laboratory Indices in Infected Patients Stratified by In-Hospital Mortality |
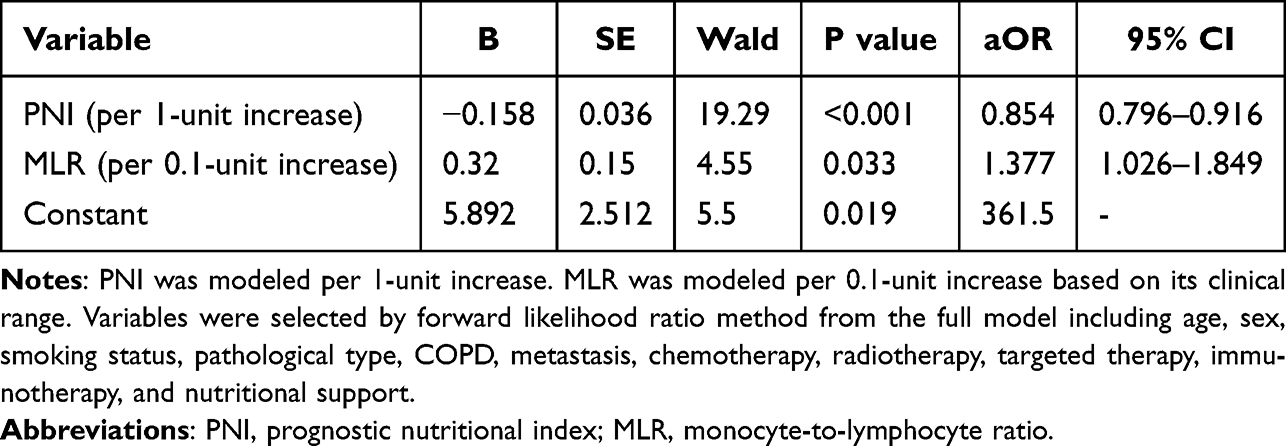 |
Table 5 Parsimonious Multivariable Model for In-Hospital Mortality in Infected Patients |
Discriminative Performance
For discriminating concomitant infection, the combined PNI+SII model had an AUC of 0.645 (Table 6). The optimal cut-off value for PNI was ≤ 43.80, yielding a sensitivity of 42.59% and a specificity of 77.61%. For SII, the optimal cut-off was ≥ 223.81, with a sensitivity of 27.31% and a specificity of 88.56%. For predicting in-hospital mortality among infected patients, PNI alone had an AUC of 0.784, MLR alone 0.700, and their combination achieved an AUC of 0.806 (Table 7). The optimal cut-off for PNI was ≤ 46.20, with a sensitivity of 93.48% and a specificity of 54.07%. For MLR, the optimal cut-off was ≥ 0.35, with a sensitivity of 80.43% and a specificity of 53.49%.
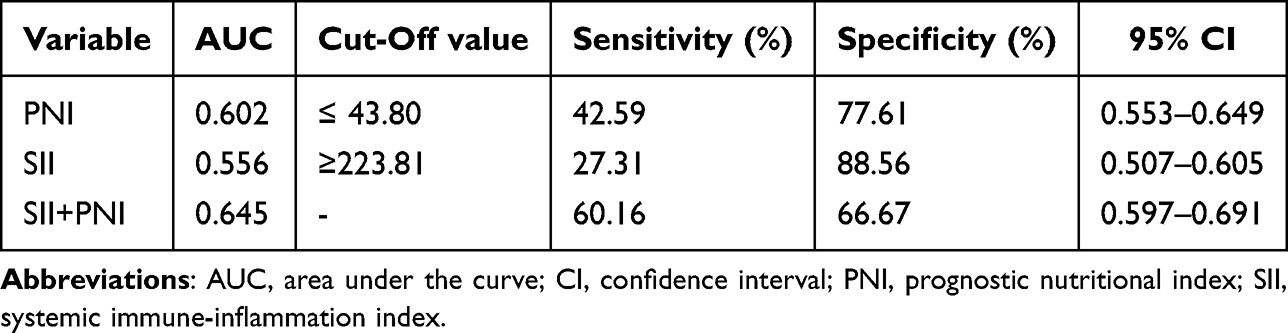 |
Table 6 Discriminative Performance of Indices for Concomitant Pulmonary Infection |
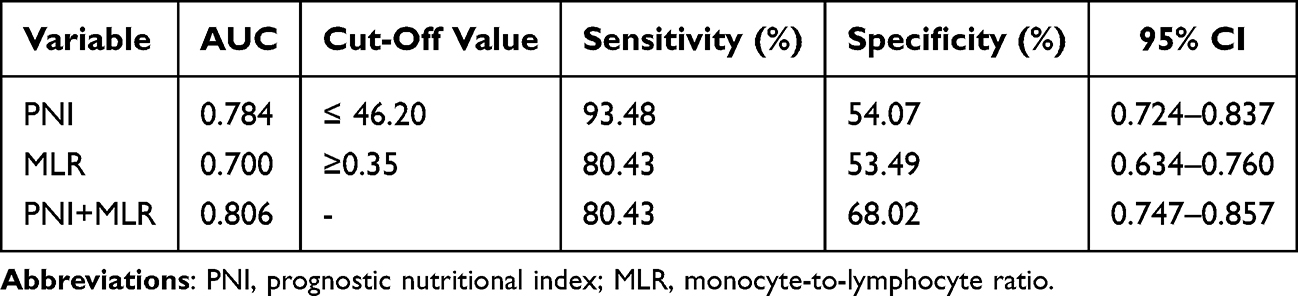 |
Table 7 Discriminative Performance of Indices for In-Hospital Mortality in Infected Patients |
Discussion
This retrospective cohort study demonstrates that a lower admission PNI is independently associated with both the presence of concomitant pulmonary infection and, among infected patients, in-hospital mortality. These associations remained robust after adjustment for key confounders including cancer stage, chemotherapy status, and other inflammatory indices. Although PNI has been studied as a prognostic tool in several cancers, including oral cancer and stage III non-small cell lung cancer,6,7 its specific role in lung cancer patients with concomitant pulmonary infection has been less explored.
Pulmonary infection represents a critical complication that adversely impacts the prognosis of lung cancer patients. Structural alterations such as bronchial obstruction and atelectasis frequently lead to impaired mucociliary clearance and sputum retention, thereby enhancing susceptibility to microbial colonization and invasion.19 Compromised systemic immunity, often present in this population, further amplifies the risk of infection. In our cohort, among 218 lung cancer patients with pulmonary infection, 46 (21.1%) experienced in-hospital mortality, underscoring the substantial burden of this comorbidity and the need for early prognostic stratification. The microbiological profile of our infected cohort (bacterial predominance, 50.46%; mixed infections, 5.96%) is consistent with previous reports in lung cancer patients.2,19
The search for reliable, readily available biomarkers to predict infection risk and outcomes in lung cancer patients remains active. Previous studies have highlighted the potential of various serum markers such as CEA, VEGF, MMP-9, presepsin, PGRN, and interleukins IL-6, IL-8, IL-10 in the context of lung cancer complicated by pulmonary infection.10,16,20 However, many of these assays are not routinely accessible in primary or secondary care settings. In contrast, PNI is derived from two common laboratory parameters: serum albumin and lymphocyte count, both widely available and inexpensive. Albumin serves as a well-established marker of nutritional status and visceral protein reserve, with hypoalbuminemia being a recognized predictor of poor outcomes in various malignancies.21 Lymphocytes are central to adaptive immunity, and lymphopenia reflects impaired immune competence. Thus, PNI integrates both nutritional and immunological dimensions into a single composite index.13,14 The biological plausibility of low PNI as a risk marker for infection and mortality in lung cancer patients is supported by the distinct roles of its two components. Hypoalbuminemia, a key feature of low PNI, reflects not only protein-energy malnutrition but also systemic inflammation and oxidative stress.22 Albumin exerts direct immunomodulatory effects by binding bacterial lipopolysaccharides (LPS), thereby neutralizing endotoxin and modulating endothelial barrier function;23 consequently, low albumin levels may impair host defense against gram-negative bacterial infections. Concurrently, lymphopenia indicates compromised adaptive immunity, with reduced CD4+ and CD8+ T-cell counts impairing pathogen clearance and increasing susceptibility to opportunistic infections.13,14 In the context of lung cancer, tumor-derived immunosuppressive factors such as transforming growth factor-beta (TGF-β) and interleukin-10 (IL-10) further exacerbate lymphopenia and promote regulatory T-cell (Treg) expansion, creating a permissive microenvironment for microbial colonization and invasion.24 Thus, the combination of nutritional depletion and immune dysfunction encapsulated by low PNI represents a high-risk phenotype for both infection acquisition and progression to mortality.
Our analysis revealed that patients with pulmonary infection had significantly lower PNI and higher systemic inflammatory indices (NLR, PLR, MLR, SII) at admission. In multivariable analysis, lower PNI and higher SII emerged as independent factors associated with concomitant infection. Malnutrition and immune dysfunction are highly prevalent and closely intertwined in cancer patients.25 A low PNI reflects a state of compromised nutrition and attenuated immune defense, which may predispose individuals to infectious complications.26 Meanwhile, SII incorporates neutrophil, platelet, and lymphocyte counts, collectively capturing the balance between pro-inflammatory and immune-regulatory pathways. Elevated neutrophils and platelets signify ongoing inflammation and a pro-thrombotic state, while lymphopenia indicates immunosuppression.27–30 Thus, the combination of low PNI and high SII may identify a subgroup of patients with both nutritional deficit and heightened inflammatory response, rendering them particularly vulnerable to pulmonary infection. The combined PNI+SII model achieved an AUC of 0.645 for discriminating infection status, suggesting modest but potentially useful discriminative ability in clinical practice. Based on our findings, we propose the following clinical application protocols for PNI in hospitalized lung cancer patients: Patients with PNI ≤ 43.80 (the optimal cut-off for concomitant infection) may be considered at increased risk of pulmonary infection at presentation. Given the high specificity (77.61%) of this threshold, it is particularly useful for “ruling in” high-risk patients who warrant closer monitoring, including early sputum cultures, chest imaging, and low-threshold initiation of diagnostic workup for infection. However, due to its modest sensitivity (42.59%), PNI alone should not replace clinical judgment or microbiological confirmation; rather, it serves as an adjunctive tool to heighten clinical suspicion. Among those with established pulmonary infection, a PNI ≤ 46.20 demonstrates excellent sensitivity (93.48%) for identifying patients at high risk of in-hospital mortality. This threshold could serve as an effective screening tool to trigger early intensive interventions, such as admission to intermediate care units, aggressive nutritional support, and enhanced infection management (eg, broader empirical antibiotic coverage or earlier infectious disease consultation). The addition of MLR (cut-off ≥ 0.35) to PNI improves specificity (from 54.07% to 68.02%), and the combined PNI+MLR model (AUC = 0.806) may be used for more refined risk stratification in clinical decision-making, particularly when resources for intensive monitoring are limited. These cut-off values should be validated in prospective studies before widespread clinical implementation. Furthermore, the dynamic monitoring of PNI during hospitalization may provide additional prognostic information for instance, whether an increase in PNI following nutritional support correlates with improved outcomes a hypothesis warranting future investigation.
Among patients with pulmonary infection, we further observed that lower PNI and higher MLR were independently associated with in-hospital mortality. Infections during cancer treatment can disrupt scheduled chemotherapy, reduce dose intensity, prolong hospitalization, and ultimately worsen oncological outcomes.31 In our study, a higher proportion of non-survivors had received chemotherapy, which may reflect treatment-related immunosuppression. Chemotherapy-induced myelosuppression, particularly neutropenia and lymphopenia, is a well-established risk factor for severe infections and poor outcomes in cancer patients.32 Cytotoxic agents not only reduce the absolute number of immune cells but also impair their function, including antigen presentation, pathogen clearance, and cytokine production.33 Furthermore, chemotherapy can disrupt mucosal barriers in the respiratory tract, facilitating microbial invasion and dissemination.34 These mechanisms collectively may render patients more vulnerable to infection progression and mortality, particularly in the context of pre-existing nutritional deficits reflected by low PNI. Monocytes play pivotal roles in antigen presentation, phagocytosis, and cytokine production, serving as precursors to macrophages and dendritic cells.35 An elevated MLR suggests a relative increase in monocyte-driven inflammation coupled with lymphopenia, indicating an imbalanced immune response that has been linked to poorer outcomes in other inflammatory lung conditions.36,37 The integration of PNI and MLR improved mortality prediction AUC=0.806, highlighting the additive value of combining nutritional and inflammatory markers for risk stratification in this high-risk population. Notably, the PNI cut-off of ≤46.20 for mortality demonstrated excellent sensitivity (93.48%), suggesting that it could serve as an effective screening tool to identify infected patients at high risk of death who may benefit from early aggressive intervention. The MLR cut-off of≥0.35, with moderate sensitivity and specificity, may complement PNI by capturing the inflammatory component of the risk profile. Future studies should incorporate additional clinical indicators such as Eastern Cooperative Oncology Group (ECOG) performance status, nutritional interventions, and inflammatory cytokines to further optimize predictive performance and validate these findings in prospective cohorts.
Our findings suggest that early identification of lung cancer patients with a low PNI at admission could facilitate targeted clinical actions. Specifically, integrating PNI into routine admission assessments may help flag individuals at higher risk for pulmonary infection or poor outcomes, prompting closer monitoring, timely microbiological investigation, or consideration of prophylactic strategies. Furthermore, these results underscore the potential importance of nutritional status in clinical outcomes. The association between low PNI and adverse events raises the possibility that systematic nutritional assessment and early intervention such as dietary counseling, oral nutritional supplements, or immunonutrition might help improve immune competence and potentially modify the risk trajectory in this vulnerable population. Our findings extend the existing literature on PNI in several important ways. Previous studies have established PNI as a prognostic factor for overall survival in various malignancies, including non-small cell lung cancer6,7 and oral cancer.6 Matsuura et al7 reported that pre-durvalumab PNI predicted overall survival in stage III NSCLC patients after chemoradiotherapy, consistent with our observation that low PNI is associated with poor outcomes. However, our study specifically focuses on the association between admission PNI and concomitant pulmonary infection a distinct endpoint that has been less explored in the oncologic literature. While Hazer et al26 demonstrated that low PNI predicted postoperative infections following lobectomy in NSCLC patients, our study uniquely examines infection present at admission and mortality among infected patients, providing insights applicable to both surgical and non-surgical candidates. Furthermore, while SII has been widely studied as an inflammatory marker in various diseases,27–30 its combination with PNI for infection risk stratification, and the addition of MLR for mortality prediction, represent novel integrated approaches that capture both nutritional and inflammatory dimensions. These findings complement prior work by Zhang et al13 and Peng et al,14 who demonstrated the utility of PNI in non-cancer populations (diabetic kidney disease and migraine, respectively), by extending its applicability to the specific context of lung cancer complicated by infection. Collectively, our results suggest that immunonutritional indices such as PNI, SII, and MLR may offer complementary value in risk stratification and should be further explored in prospective, multi-center cohorts. However, this hypothesis requires testing in prospective, interventional studies designed to evaluate whether nutritional support can effectively reduce infection incidence or mortality in lung cancer patients with low PNI.
Several limitations of this study should be acknowledged. First, its retrospective, single-center design precludes causal inference and may limit the generalizability of our findings. While our study included a diverse cohort of lung cancer patients, the inherent heterogeneity of this population was not fully explored. Future studies should incorporate stratified analyses based on specific pathological types (eg, adenocarcinoma, squamous cell carcinoma) and various treatment modalities (eg, chemotherapy, targeted therapy, immunotherapy) to better delineate the prognostic value of PNI in different clinical contexts and improve sample representativeness. Second, infection status was assessed at admission rather than tracked as incident infections during hospitalization; accordingly, our results reflect the baseline burden of concomitant infection rather than the ability to predict new-onset infections. Third, despite adjustment for multiple confounders, residual confounding from unmeasured variables cannot be excluded. Key factors such as ECOG performance status, smoking index, and prior antibiotic exposure, which may influence both nutritional status and clinical outcomes, were not available in this retrospective dataset. Furthermore, data on specific nutritional interventions (eg, protein supplementation, immunonutrition formulas) administered during hospitalization were not collected, precluding analysis of their potential impact on reversing the risk associated with a low PNI. The potential benefit of such interventions remains to be prospectively tested. Fourth, while we identified an association between low PNI and poor outcomes, this study was not designed to evaluate the impact of these nutritional interventions. Fifth, no formal sample size calculation was performed prior to this retrospective study, as is common in studies based on consecutive admissions. However, post-hoc assessment confirmed that the sample size satisfied the events-per-variable criterion for logistic regression (EPV > 10),18 supporting the reliability of our findings. Future prospective studies with larger, multicenter cohorts are warranted to validate these results and to enable the stratified analyses mentioned above. Sixth, the association between chemotherapy and higher mortality should be interpreted cautiously, as it may be confounded by indication. Patients with more aggressive disease may be more likely to receive chemotherapy, and these same factors could increase infection risk. Although we adjusted for pathological type and treatment modalities, residual confounding from chemotherapy intensity, timing, or specific regimens cannot be excluded. Future studies with detailed chemotherapy data are needed to clarify these effects. Finally, while we used traditional ROC analysis to evaluate the discriminative ability of markers for in-hospital mortality, this approach does not account for the time-to-event nature of survival outcomes. However, because our primary outcome was in-hospital mortality within a relatively short and fixed hospitalization period, the use of time-dependent ROC and Cox regression was not applicable. Future studies with longer follow-up and time-to-event data should employ these methods to assess long-term prognostic value.
In conclusion, this observational study demonstrates that admission PNI is independently associated with both the presence of pulmonary infection and in-hospital mortality in lung cancer patients. When combined with SII or MLR, it provides moderate discriminative ability for infection and mortality risk, respectively. These findings suggest that integrating simple, routinely available immunonutritional indices into the initial assessment of hospitalized lung cancer patients may aid in risk stratification. However, given the observational design, causal inferences cannot be drawn, and the potential clinical utility of PNI-based profiling such as guiding enhanced infection surveillance or nutritional support requires validation in prospective, interventional studies.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request. The data include de-identified patient laboratory results and clinical characteristics. Access will be granted for academic non-commercial purposes after approval by the institutional ethics committee. The data are not publicly available due to privacy restrictions.
Author Contributions
Xiaowu Wang and Xiaoyu Fang contributed equally to this work and share first authorship.
Xiaowu Wang: Conceptualization, Methodology, Writing - original draft, Supervision. Xiaoyu Fang: Data Curation, Formal Analysis, Writing - review & editing. Tuantuan Li: Investigation, Resources, Visualization, Writing - review & editing. Yong Gao: Software, Validation, Project Administration, Writing - review & editing. Yuxin Gao: Formal Analysis, Data curation, Writing - review & editing. Yilang Zhu: Conceptualization, Methodology, Writing - original draft, Writing - review and editing, Funding acquisition, Supervision. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Fuyang City Key Research and Development Program (Grant No. FYZDYF2023CYX042) and The Qilu Special Project of Fuyang Municipal Health Commission (Grant No. FY2024-012), and the Fuyang City Science and Technology Bureau Project (Grant No. FK20254620).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021;398(10299):535–11. doi:10.1016/S0140-6736(21)00312-3
2. Lai Q, Liao K, Kuang G, Liao W, Zhang S. Construction of a nomogram prediction model for individualized prediction of the risk of pulmonary fungal infection in lung cancer. Infect Drug Resist. 2025;18:3137–3147. doi:10.2147/IDR.S526221
3. Chen CA, Ho CH, Wu YC, Chen YC, Wang JJ, Liao KM. Epidemiology of Aspergillosis in cancer patients in Taiwan. Infect Drug Resist. 2022;15:3757–3766. doi:10.2147/IDR.S370967
4. Terrones-Campos C, Ledergerber B, Specht L, Vogelius IR, Helleberg M, Lundgren J. Risk of bacterial, viral, and fungal infections in patients with solid malignant tumors treated with curative intent radiation therapy. Adv Radiat Oncol. 2022;7(6):100950. doi:10.1016/j.adro.2022.100950
5. Woodard GA, Jones KD, Jablons DM. Lung cancer staging and prognosis. Cancer Treat Res. 2016;170:47–75. doi:10.1007/978-3-319-40389-2_3
6. Momokita M, Abe A, Shibata K, et al. Prognostic nutritional index in patients with end-stage oral cancer. Am J Hosp Palliat Care. 2023;40(4):396–400. doi:10.1177/10499091221102581
7. Matsuura S, Serizawa S, Yamashita R, et al. The Prognostic Nutritional Index before durvalumab after chemoradiation predict the overall survival in patients with stage III non-small cell lung cancer. Ann Med. 2023;55(1):2196089. doi:10.1080/07853890.2023.2196089
8. Wang B, Wei Y. Diagnostic value of CRP, PCT, NC, and NLR in peripheral blood for bacterial infections in non-small cell lung cancer patients after chemotherapy. J Med Biochem. 2025;44(7):1421–1428. doi:10.5937/jomb0-57772
9. Nardone V, Giannicola R, Bianco G, et al. Inflammatory markers and procalcitonin predict the outcome of metastatic non-small-cell-lung-cancer patients receiving PD-1/PD-L1 immune-checkpoint blockade. Front Oncol. 2021;11:684110. doi:10.3389/fonc.2021.684110
10. Reniers T, Noordzij PG, Veen EJ, et al. Does postoperative plasma IL-6 improve early prediction of infection after pulmonary cancer surgery? A two-centre prospective study. PLoS One. 2025;20(6):e0326537. doi:10.1371/journal.pone.0326537
11. Liang S, Yin X, Fu Y, Li X, Zhu J, Xu R. Comparison of inflammatory cytokine levels between single-port and three-port thoracoscopic lobectomy in the treatment of non-small-cell lung cancer. Biomed Res Int. 2022;2022:3240252. doi:10.1155/2022/3240252
12. Zhang L, Ma W, Qiu Z, et al. Prognostic nutritional index as a prognostic biomarker for gastrointestinal cancer patients treated with immune checkpoint inhibitors. Front Immunol. 2023;14:1219929. doi:10.3389/fimmu.2023.1219929
13. Zhang J, Chen Y, Zou L, Gong R. Prognostic nutritional index as a risk factor for diabetic kidney disease and mortality in patients with type 2 diabetes mellitus. Acta Diabetol. 2023;60(2):235–245. doi:10.1007/s00592-022-01985-x
14. Peng C, Gao L, Wu K, et al. Association between the prognostic nutritional index and severe headache or migraine: a population-based study. Nutr Neurosci. 2023;26(12):1202–1211. doi:10.1080/1028415X.2022.2143958
15. Torres A, Niederman MS, Chastre J, et al. Summary of the international clinical guidelines for the management of hospital-acquired and ventilator-acquired pneumonia. ERJ Open Res. 2018;4(2):00028–2018. doi:10.1183/23120541.00028-2018
16. Chen J, Liu Y, Cai H, Zheng W. Risk factors for pulmonary infection in patients with non-small cell lung cancer: a meta-analysis. BMC Pulm Med. 2024;24(1):353. doi:10.1186/s12890-024-03171-x
17. Sheervalilou M, Ghanei M, Arabfard M. Global trends, risk factors, and therapeutic associations of fungal pulmonary infections in lung cancer: a systematic review and meta-analysis. J Bras Pneumol. 2025;51(5):e20250076. doi:10.36416/1806-3756/e20250076
18. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/s0895-4356(96)00236-3
19. Shan H, Wang J, Zhang Q, et al. Pathogen surveillance and risk factors for pulmonary infection in patients with lung cancer: a retrospective single-center study. Open Med. 2025;20(1):20251180. doi:10.1515/med-2025-1180
20. Yanxing Zhu, Zhiren Lin, Chengde Wu. Retracted: apatinib plus radiotherapy on the expression of CEA and VEGF in advanced oligometastatic non-small-cell lung cancer. Evid Based Complement Alternat Med. 2023;2023:4242346. doi:10.1155/2023/4242346
21. Zhang J, Zhao T, Long S, Liu X, Yu H. Risk factors for postoperative infection in Chinese lung cancer patients: a meta-analysis. J Evid Based Med. 2017;10(4):255–262. doi:10.1111/jebm.12276
22. McLean TW, Stewart RM, Curley TP, et al. Hypoalbuminemia in children with cancer treated with chemotherapy. Pediatr Blood Cancer. 2020;67(2):e28065. doi:10.1002/pbc.28065
23. Wiedermann CJ. Albumin and its role in the prevention of infection: a narrative review. Eur J Intern Med. 2021;89:8–14. doi:10.1016/j.ejim.2021.04.021
24. Mao Y, Zhao Q, Yin S, et al. The role of regulatory T cells in the pathogenesis of lung cancer: a double-edged sword. Front Immunol. 2022;13:864084. doi:10.3389/fimmu.2022.864084
25. Arends J, Bachmann P, Baracos V, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36(1):11–48. doi:10.1016/j.clnu.2016.07.015
26. Hazer S, Gülhan SŞE, Solak N, et al. The effect of prognostic nutritional index in postoperative infection following lobectomy in non-small cell lung cancer patients. Cureus. 2023;15(4):e37611. doi:10.7759/cureus.37611
27. Adiguzel A, Arsava EM, Topcuoglu MA. Temporal course of peripheral inflammation markers and indexes following acute ischemic stroke: prediction of mortality, functional outcome, and stroke-associated pneumonia. Neurol Res. 2022;44(3):224–231. doi:10.1080/01616412.2021.1975222
28. Wu J, ZhangX, Liu H, et al. RDW, NLR and RLR in predicting liver failure and prognosis in patients with hepatitis E virus infection. Clin Biochem. 2019;63:24–31. doi:10.1016/j.clinbiochem.2018.11.012
29. Liu J, Niu H, Yue L, et al. Abnormal platelet phenotypes in patients with myelodysplastic syndromes. Int J Lab Hematol. 2020;42(4):371–379. doi:10.1111/ijlh.13191
30. Cognasse F, Laradi S, Berthelot P, et al. Platelet inflammatory response to stress. Front Immunol. 2019;10:1478. doi:10.3389/fimmu.2019.01478
31. Schabath MB, ML C. Cancer progress and priorities: Lung cancer. Cancer Epidemiol Biomarkers Prev. 2019;28(10):1563–1579. doi:10.1158/1055-9965.EPI-19-0221
32. Kuter DJ. Chemotherapy-induced neutropenia: mechanisms, risk factors, and clinical implications. Cancer Treat Rev. 2024;123:102718. doi:10.1016/j.ctrv.2024.102718
33. Das A, Roy S, Bairagi A, et al. Neoadjuvant chemotherapy alters exhaustion of CD4+ and CD8+ T cells in HER2-overexpressing metastatic breast cancer. J Curr Oncol Trends. 2025;2(2):127–139. doi:10.4103/JCOT.JCOT_15_25
34. Obeagu EI. Novel microbiome-driven approaches to counteract chemotherapy-induced mucositis in breast cancer patients. Breast Cancer. 2026;18:1–11. doi:10.2147/BCTT.S590718
35. Ji Y, Xie Q, Wei W, et al. Association between blood inflammatory status and the survival of tuberculosis: a five-year cohort study. Front Immunol. 2025;16:1556857. doi:10.3389/fimmu.2025.1556857
36. Fan F, Lv J, Yang Q, Jiang F. Clinical characteristics and serum inflammatory markers of community-acquired mycoplasma pneumonia in children. Clin Respir J. 2023;17(7):607–617. doi:10.1111/crj.13620
37. Cao H, Huang J, Chang J, et al. Predictors of progression in idiopathic inflammatory myopathies with interstitial lung disease. J Transl Int Med. 2022;11(1):46–56. doi:10.2478/jtim-2022-0029
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Lactate Dehydrogenase/Albumin Ratio and in-Hospital Mortality in Patients with Acute Aortic Dissection
Mutailifu S, Zhu Q, Wang M, Zhang D, Song S, Li N
Journal of Inflammation Research 2025, 18:6281-6292
Published Date: 14 May 2025
Wnt3a Inhibits Inflammatory Responses and Improves Survival in Immortalised Schwann Cells
Zheng J, Zhang Y, Nan G
Journal of Inflammation Research 2025, 18:17715-17730
Published Date: 18 December 2025
The Inflammatory Roles of n-3 and n-6 Polyunsaturated Fatty Acids in COPD: Clinical Implications and Underlying Mechanisms
Wang Y, Bao Y, Liu B, Li H, Duan H, Wang Y, Zhang J, Wu W, Li P, Liu X
Journal of Inflammation Research 2026, 19:556221
Published Date: 15 January 2026
Prognostic Factors in Upper Gastrointestinal Neuroendocrine Carcinoma: A Retrospective Cohort Study of Clinicopathological Features and Survival Outcomes
Şeyran E, Gökmen A
Cancer Management and Research 2026, 18:618644
Published Date: 17 July 2026