Back to Journals » Research and Reports in Urology » Volume 18
Assessing the Knowledge and Awareness of Urinary Incontinence Among Urogynecology Clinic Patients in Jordan: A Cross-Sectional Study
Authors Abufaraj M ![]() , Mohammed D
, Mohammed D ![]() , Al-Amoosh H
, Al-Amoosh H ![]() , Shwyiat RM, Alkhoury TS, Alamoush A, Sulaiman S, Kilani A
, Shwyiat RM, Alkhoury TS, Alamoush A, Sulaiman S, Kilani A ![]() , Alqatawneh DA
, Alqatawneh DA ![]() , Abu AlHaija DT, Haddadin O
, Abu AlHaija DT, Haddadin O
Received 7 March 2026
Accepted for publication 4 June 2026
Published 12 June 2026 Volume 2026:18 607618
DOI https://doi.org/10.2147/RRU.S607618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Guglielmo Mantica
Mohammad Abufaraj,1,2 Dina Mohammed,3 Hamza Al-Amoosh,4 Rami Mohammed Shwyiat,5 Tina Sami Alkhoury,3 Aysheh Alamoush,6 Samia Sulaiman,3 Akram Kilani,3 Dana Ayman Alqatawneh,3 Diala Tareq Abu AlHaija,3 Omar Haddadin4
1Division of Urology, Department of Special Surgery, Jordan University Hospital, The University of Jordan, Amman, 11942, Jordan; 2Department of Urology, Medical University of Vienna, Vienna, Austria; 3School of Medicine, The University of Jordan, Amman, Jordan; 4Faculty of Medicine, Hashemite University, Prince Hamza Hospital, Amman, Jordan; 5Obstetrics and Gynecology Department, King Hussein Medical Center, Amman, Jordan; 6Faculty of Nursing, Applied Science University, Amman, Jordan
Correspondence: Mohammad Abufaraj, Division of Urology, Department of Special Surgery, Jordan University Hospital, The University of Jordan, Amman, 11942, Jordan, Email [email protected]
Objective: To assess knowledge and awareness of urinary incontinence (UI) among Jordanian women attending a urogynecology clinic and identify sociodemographic and clinical factors associated with knowledge levels.
Methods: A cross-sectional study was conducted involving 294 women aged 18 to 80 years who attended the urogynecology clinic at King Hussein Medical Center (KHMC) in Amman, Jordan, from February 2022 to April 2023. Knowledge was measured using the validated Prolapse and Incontinence Knowledge Questionnaire (PIKQ) through structured interviews. Each correct answer was awarded one point, while incorrect or “do not know” responses were scored as zero. Total scores, ranging from 0 to 12, were converted to percentages. Data normality was assessed using the Shapiro–Wilk and Kolmogorov–Smirnov tests. Associations between knowledge scores and sociodemographic or clinical variables were examined using Spearman’s rank correlation coefficient. Statistical analyses were performed with IBM SPSS version 28.0, and statistical significance was set at p < 0.05.
Results: The mean knowledge score was 8.77 ± 1.39 out of 12 (73.06%). Higher knowledge scores were significantly associated with greater educational level, higher income, employment in healthcare, and previous treatment for UI (p< 0.05). In contrast, increasing age, higher number of children, and postmenopausal status were significantly associated with lower knowledge scores (p< 0.05). No significant associations were found between knowledge scores and marital status, prior consultation with a urologist or urogynecologist, or personal history of UI.
Conclusion: Women attending a urogynecology clinic in Jordan demonstrated moderate overall knowledge of UI. However, substantial knowledge gaps remain, particularly concerning treatment options and disease management. These results underscore the need for targeted educational interventions, particularly for older, multiparous, and postmenopausal women, to improve understanding, address misconceptions, and enhance clinical outcomes and quality of life.
Keywords: urinary incontinence, awareness, knowledge, urogynecology
Introduction
Urinary incontinence (UI), the involuntary loss of urine, is a highly prevalent condition affecting around 423 million individuals worldwide.1 Women are disproportionately affected, with prevalence rates approximately twice those observed in men.2 The prevalence of UI in women increases with age, ranging from approximately 25% in young women to 44–57% in middle-aged and postmenopausal women, and up to 75% in older women.3 Clinically, UI includes several distinct subtypes: stress, urge, and mixed urinary incontinence. Each subtype is associated with unique pathophysiological mechanisms and management strategies.4 Accurate identification of the UI subtype is critical for selecting appropriate treatment and achieving optimal outcomes.5
The impact of UI extends beyond physical symptoms. Women with UI often experience diminished quality of life, social isolation, decreased work productivity, and sexual dysfunction. Furthermore, there are higher rates of anxiety, depression, falls, and urinary tract infections among this population.4,6 The economic burden is considerable, with direct costs in the United States estimated at $19.5 billion annually and total direct and indirect costs reaching $51.4 billion.2 Despite the availability of effective treatments, such as pelvic floor muscle training, behavioral interventions, pharmacologic therapies, and surgical procedures, only 25% of affected women seek care, and fewer than half of these receive treatment.4 A study in Jordan reported that less than half (37.9%) of participant with UI receive medical care.7
Several interrelated barriers contribute to the treatment gap for UI. Frequently cited factors include embarrassment, social stigma, misconceptions that UI is a normal aspect of aging, and limited awareness of available treatment options.4 Approximately 55% of women with UI do not disclose symptoms to healthcare providers.2 In Jordan, one study suggested only 43.8% of women with UI sought medical consultation. Embarrassment (52.2%), normalization of symptoms with aging (41.5%), and limited expectations of improvement from treatment (42.0%) were identified as primary barriers.8 These obstacles may be exacerbated in conservative Middle Eastern societies, where cultural norms discourage discussion of urinary symptoms, especially when care is provided by male physicians.9
Knowledge deficits are a significant, modifiable factor contributing to the underdiagnosis and undertreatment of UI. A landmark study reported that 71.2% of community-dwelling women in the United States lacked adequate knowledge of UI.10 Data from Middle Eastern countries remains limited, which is concerning given the high prevalence of UI reported in developing regions. For instance, Jordan reports one of the highest rates at 64.1%.11 The current literature is further limited by methodological issues, including a predominant focus on community-dwelling populations rather than on women actively seeking urogynecologic care and inconsistent use of validated assessment instruments.10,12
Given these gaps, systematic assessment of UI knowledge using validated instruments in regional clinical populations is necessary. The present study aimed to evaluate knowledge and awareness of UI among women attending a urogynecology clinic in Jordan, utilizing the validated Prolapse and Incontinence Knowledge Questionnaire (PIKQ). Furthermore, the study sought to identify sociodemographic and clinical factors associated with variations in knowledge levels.13,14
Materials and Methods
Study Design and Setting
This cross-sectional study was conducted between February 2022 and April 2023 at the urogynecology clinic of King Hussein Medical Center (KHMC) in Amman, Jordan. The study was designed and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies.15
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Review Board of the Hashemite University, Amman, Jordan (approval number: 2300604). Participation was voluntary, and prior to enrollment, all participants provided verbally informed consent before inclusion in the study, following an explanation of the study’s objectives, methodology, and confidentiality measures.
Study Population
The study population comprised women aged 18–80 years attending the urogynecology clinic at KHMC during the study period. Participants were recruited through convenience sampling, in which all eligible patients presenting to the clinic were invited to participate. Inclusion criteria were: (1) female sex; (2) age 18–80 years; (3) attendance at the urogynecology clinic during the study period; (4) willingness to participate; and (5) ability to provide informed consent.
Exclusion criteria were: (1) age outside the specified range; (2) inability or unwillingness to provide informed consent; and (3) incomplete questionnaire responses.
Data Collection Instrument
Data were collected using the PIKQ tool, a validated instrument designed to assess knowledge related to pelvic floor disorders. The questionnaire comprised three sections. The first section included 13 items capturing sociodemographic and clinical characteristics: age, marital status, educational attainment, occupation, monthly household income, number of children, menopausal status, and history of condition. The second section comprised 12 true/false statements assessing knowledge of UI, including items related to risk factors, symptoms, diagnosis, and management strategies. Similarly, the third section included 12 true/false statements evaluating knowledge of Pelvic organ prolapse (POP). However, to minimize respondent burden and maintain focus on the study’s primary objective assessing knowledge and awareness of UI specifically, only the UI domain was applied. Response options for knowledge items included “agree”, “disagree”, or “do not know”. (Table 1).
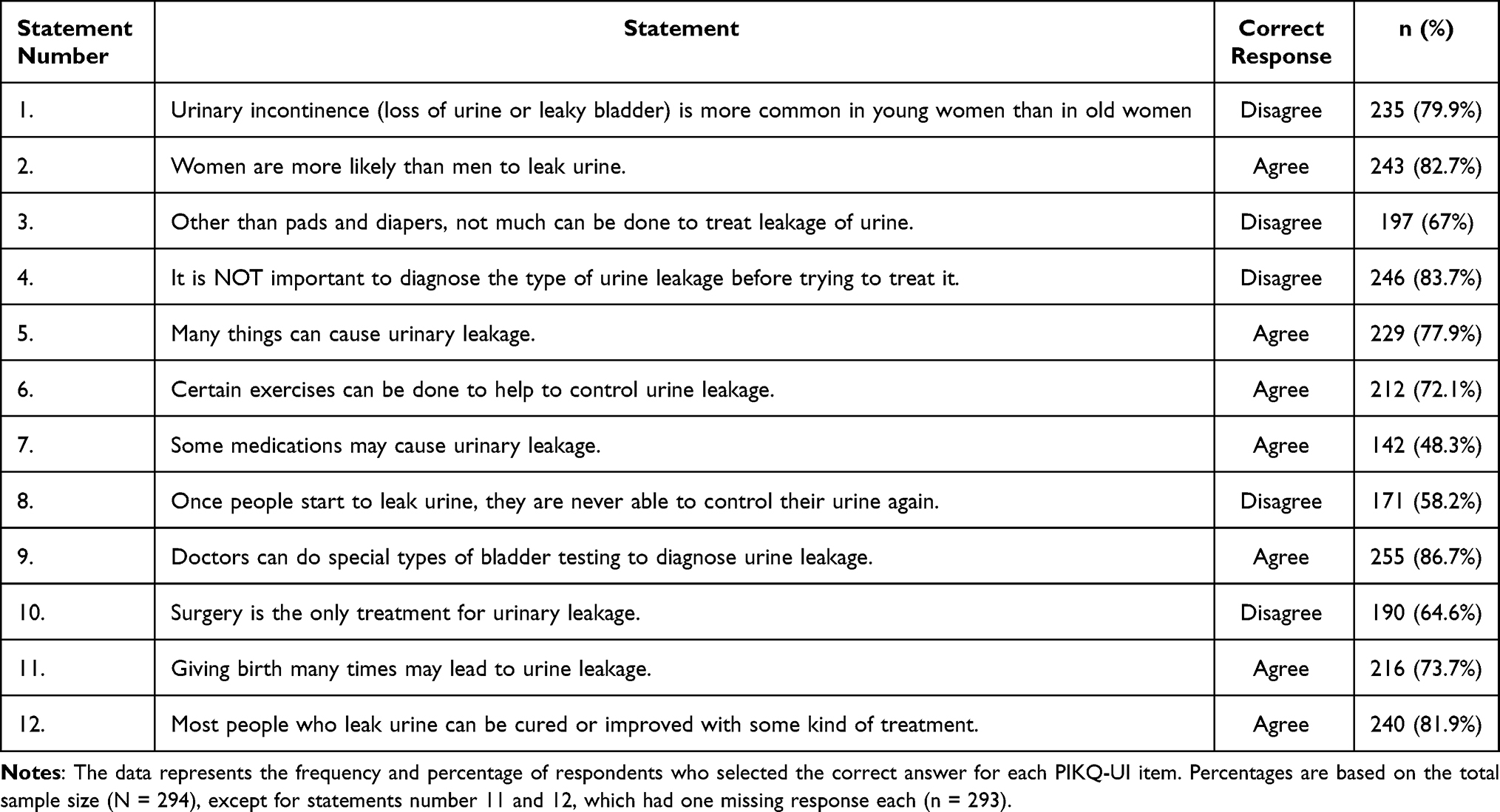 |
Table 1 Prolapse and Incontinence Knowledge Quiz–Urinary Incontinence (PIKQ-UI): Correct Responses by Item |
Questionnaire Translation and Adaptation
The survey was translated from English into Arabic by bilingual experts to ensure participant comprehension. An independent translator blinded to the original version performed a back-translation to verify semantic equivalence. The questionnaire was subsequently pilot tested among 20 participants representative of the target population, and feedback was incorporated to finalize the Arabic version.
Data Collection Procedure
Data were collected through structured face-to-face interviews conducted in a private setting within the clinic. Trained members of the research team administered the questionnaire verbally to each participant to ensure standardization and to accommodate participants with limited literacy. Responses were recorded contemporaneously in a standardized Excel spreadsheet.
Scoring System
Knowledge scores were calculated by assigning one point for each correct response and zero points for incorrect or “do not know” responses. Total scores ranged from 0 to 12, with higher scores indicating greater knowledge of UI. Total scores were converted to percentages to facilitate interpretation and comparison across subgroups. The mean knowledge score was calculated by summing the number of correct responses for each participant, yielding a total score ranging from 0 to 12. Scores were subsequently converted to percentages by dividing the total score by 12 and multiplying by 100.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 28.0 (IBM Corporation, Armonk, NY). Descriptive statistics were used to summarize sociodemographic characteristics and questionnaire responses. Continuous variables were reported as means with standard deviations or as medians with interquartile ranges, depending on data distribution. Categorical variables were summarized as frequencies and percentages. Prior to inferential analysis, the distribution of continuous variables was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests. All assessed variables demonstrated significant deviation from normality (p<0.001); therefore, non-parametric statistical methods were used. (Supplementary Table S1) Associations between UI knowledge scores and sociodemographic or clinical variables were evaluated using Spearman’s rank correlation coefficient. Pairwise deletion addressed missing data, excluding cases only from analyses involving the affected variables. Variables demonstrating significance in Spearman correlation analysis were subsequently analyzed using multivariate regression model to evaluate their independent impact on UI knowledge. Statistical significance was set at a two-tailed p-value less than 0.05.
Results
Demographic Characteristics
The study included 294 participants (Table 2), where those aged 46–60 years comprised 42.9% of the study group (n=126). The most frequently reported number of children was four (n=55, 18.8%). The mean knowledge score was 8.77 ± 1.39 out of 12 (73.06%).
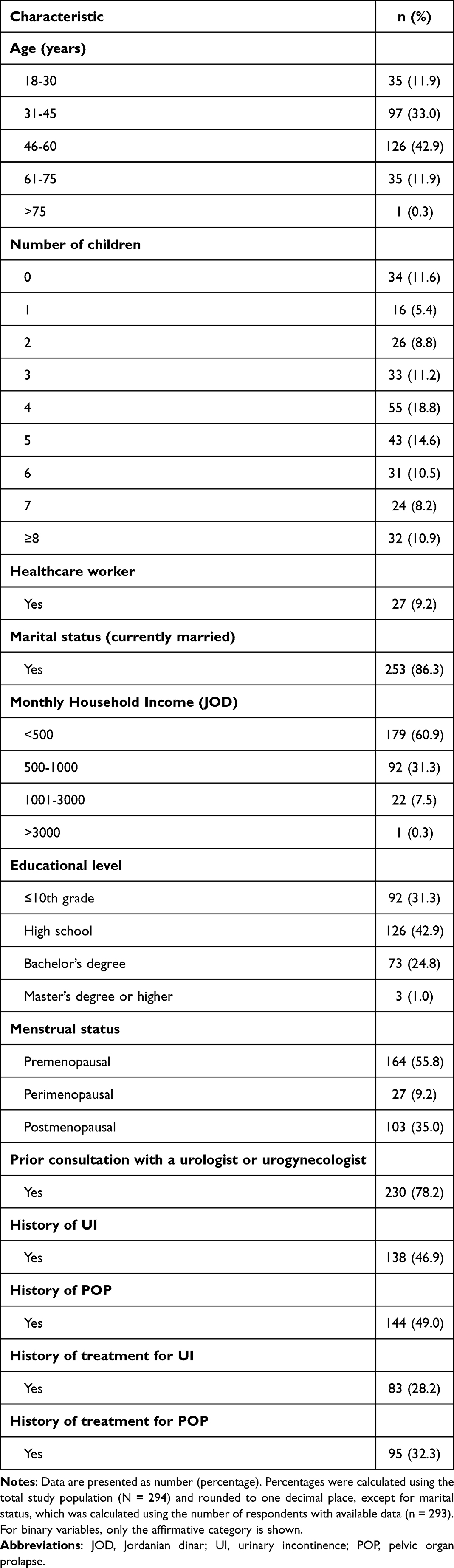 |
Table 2 Demographic Characteristics of Patients |
A total of 86.3% of participants (n=253) were currently married, while the remaining 13.7% were not currently married. The educational backgrounds of participants were diverse, with 31.3% having completed grade 10 or lower (n=92), 42.9% having completed high school (n=126), 24.8% holding a bachelor’s degree (n=73), and 1% holding a master’s degree or higher (n=3).
Regarding occupation, 90.8% of participants were not healthcare workers (n = 267), with 9.2% identifying as healthcare professionals (n=27). Concerning income distribution, the majority of participants (60.9%) reported incomes below 500 JODs (n=179), while 31.3% of participants reported an income within the range of 500 to 1000 JODs (n=92). A smaller percentage, 7.5% of participants, earn between 1001 and 3000 JOD (n=22), and only one participant had an income exceeding 3000 JODs.
Gynecologic History
A total of 55.8% of participants (n=164) were categorized as premenopausal, while 35.0% and 9.2% were identified as postmenopausal and perimenopausal, respectively. Of the participants, 78.2% have previously visited a urologist or urogynecologist (n=230). Concerning UI, 46.9% reported having a history of UI (n=138), of which 28.2% received treatment (n=83).
Normality Test Results
The normality of sociodemographic variables was assessed using Kolmogorov–Smirnov and Shapiro–Wilk tests. All variables displayed significant deviations from normal distribution, indicated by p-values less than 0.001. The normality assessment for the UI scale data indicates a significant non-normal distribution of observations (p < 0.001).
Urinary Incontinence Awareness
As for overall awareness regarding the population usually affected by UI, 79.9% of respondents correctly recognized that UI is more prevalent in older women than in younger women. Moreover, 82.7% recognized that women are more susceptible to urine leakage than men. Additionally, 77.9% and 73.7% of participants recognized that several factors and multiple births may be linked to urinary incontinence, respectively. Furthermore, 48.3%also recognized that certain medications could contribute to urinary leakage (Table 1).
Regarding the participants’ awareness of diagnosis and management, 86.7% of participants knew specialized bladder testing for diagnosing urine leakage and 83.7% believed that determining the type of urine leakage was important before beginning treatment. Moreover, 58.2% of participants believe that control is not permanently lost once it starts. However, only 67% of participants recognized that treatments beyond pads and diapers are available for managing urine leakage, and only 64.6% correctly identified that surgery is not the only treatment option, despite 72.1% being aware of specific exercises that can aid in controlling it. Regarding childbirth, 73.7% of the participants acknowledged multiparity as a contributing factor to UI and 81.9% recognized that proper treatment could improve or cure urinary leakage (Table 1).
The Relationship Between Urinary Incontinence and Sociodemographic Data
Normality tests revealed non-normal distribution; nonparametric tests assessed correlations between UI awareness and sociodemographic characteristics using Spearman’s rank correlation test. The research findings indicate significant links between sociodemographic factors and knowledge and awareness of UI (Table 3). Notably, participants working in the medical field exhibited a statistically significant positive correlation with UI awareness level (r (291) = [0.155], p = [0.004]), suggesting that UI awareness levels are higher among healthcare workers. Additionally, income demonstrated a statistically significant positive correlation with UI awareness level (r (291) = [0.144], p = [0.007]), indicating that higher income is associated with increased levels of UI awareness. Similarly, a statistically significant positive correlation was observed between the level of education and UI awareness level (r (291) = [0.356], p = [0.001]), implying that individuals with higher levels of education tend to have better knowledge and awareness regarding UI. Furthermore, receiving prior treatment for UI showed a statistically significant positive correlation with UI awareness level (r (291) = [0.111], p = [0.029]), indicating that individuals who received treatment for UI in the past tend to have higher levels of UI awareness. On the other hand, the study found a negative correlation between age and UI awareness level (r (291) = [−0.181], p = [0.001]), suggesting that older patients pertain less UI awareness than the younger patients in the study. A similar statistically significant negative correlation was found between the number of children and UI awareness level (r (291) = [−0.235], p = [0.001]), suggesting that women with more children demonstrate a lesser degree of awareness regarding UI in contrast to those with less children. A negative correlation was also observed between awareness of UI and menopausal status (r (291) = [−0.105], p = [0.036]), indicating that postmenopausal women exhibit a reduced level of awareness regarding UI compared to premenopausal women. No statistically significant correlation was found between marital status and UI awareness level (r (291) = [0.027], p = [0.32]). No statistically significant correlations were found between UI awareness level and visiting a urologist or urogynecologist (r (291) = [−0.077], p = [0.095]) or having a previous history of UI (r(291) = [0.011], p = [0.423]).
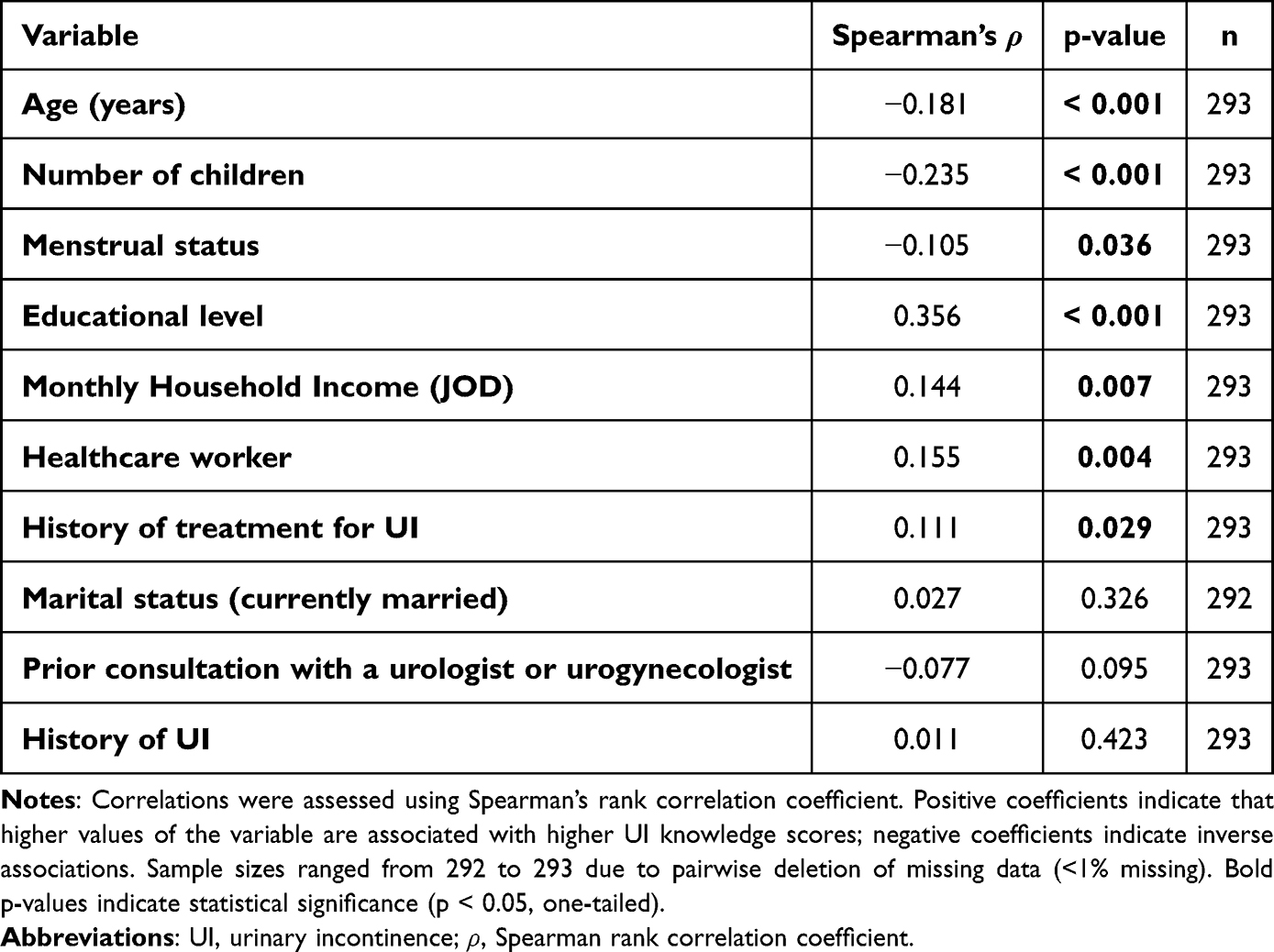 |
Table 3 Correlations Between Urinary Incontinence Knowledge Scores and Sociodemographic and Clinical Characteristics |
The Independent Association Between Urinary Incontinence Knowledge and Sociodemographic Data
Overall, the multivariate analysis model (Tables 4 and 5) demonstrated significant outcome, with an F of 12, 279 at 5.483, and p less than 0.001. It explained about 19.1% of the variance, so R squared was 0.191. Only two variables remained independently and significantly associated with UI knowledge proficiency in the multivariable analysis: higher educational level (B = 0.967, β = 0.332, p < 0.001) and prior treatment for UI (B = 1.063, β = 0.211, p = 0.015).
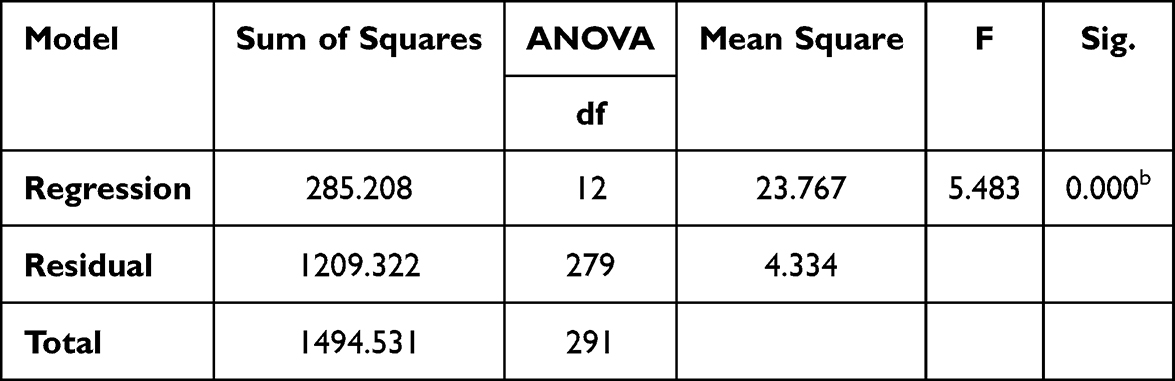 |
Table 4 Overall Model Fit for Multiple Linear Regression Analysis |
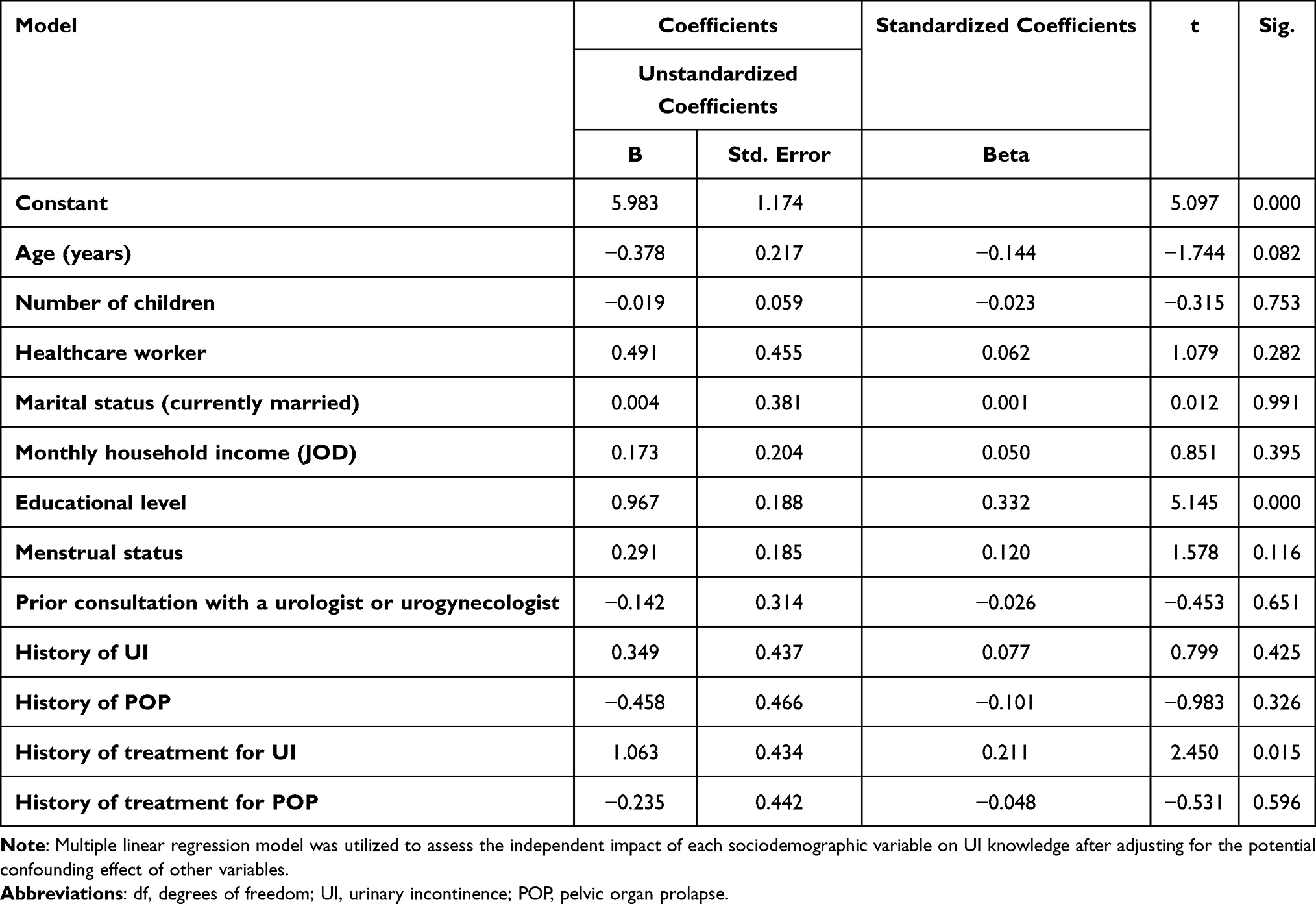 |
Table 5 Multiple Linear Regression Coefficients for Predictors of UI Knowledge |
Discussion
Overall, participants demonstrated a moderate general understanding of UI, likely influenced by recruitment from a gynecology clinic where awareness is expected to be higher.
Several studies reported comparable levels of UI knowledge levels.16–18 A Polish study revealed that 46% of participants had high knowledge in comparison to only 38% and 16% demonstrating average and low levels of awareness, respectively.16 Similarly, over half of the patients were aware of UI causes, diagnosis, management, and the course of the condition. Consistently, according to Hobdy’s study findings, 54% of the study sample were UI knowledge proficient.18 However, other studies highlighted substantial knowledge deficits, with over 70% of respondents in Indonesia19 and US10 demonstrating inadequate UI awareness. Lower proficiency as evident in two other studies carried out in the UK20 and at KK Women’s and Children’s hospital21 only 41% and 46.2% of the respondents were UI knowledge proficient correspondingly.
Age was inversely associated with UI knowledge in multiple studies.10,22 One study found that the odds of having limited UI knowledge are 2.88 times greater in women of 79 years and above relevant to those of 19–29 years.10 Another study in the US has shown an association between the younger generation and the number of correct answers in 8 out of the 14 items22 possibly due to social stigma, reluctance to discuss symptoms, and misinterpretation of UI as a normal aging process. Moreover, premenopausal women demonstrated higher knowledge level, while postmenopausal often likely misattributed UI symptoms to physiological processes. A study in Indonesia19 showed that 71% of postmenopausal women showed insufficient UI awareness. However, other studies show no significant association was established, likely related to differences in the communities between studies and available counseling.16,20
While some studies reported higher UI knowledge among married women,18 this association was not significant in our study and other studies as well.16 This suggests that with the wider availability of health-related information, there is no significant difference in the knowledge of both groups. Furthermore, having a higher number of children demonstrates lower awareness in our study. Other studies support this, where multiparous women demonstrated a lower mean knowledge score of 36% relative to nulliparous women with a score of 45%.21 Similarly, results from another study suggested that a higher number of children was associated with greater odds of lacking UI knowledge.10 This may reflect increased household responsibilities and reduced prioritization of health education. However, a survey conducted in the US showed significantly higher odds of lacking UI knowledge upon primiparity but not multiparity.23 Another study in Malaysia shows no statistically significant association was established between parity and UI awareness, highlighting population-based differences.24
In line with previous studies,10,17,23 working in the medical field was significantly associated with higher UI knowledge. Educational level also showed a positive correlation with UI knowledge. Similar findings were reported in Poland, where 60% of respondents who received higher education had “high” UI knowledge level in comparison to only 44% and 30% of those receiving secondary and vocational education, respectively.16 Likewise, a UK study suggested an 18% lower knowledge score of participants with mid-secondary education relative to those with tertiary education.20 This association may be explained by increased access to academic resources and specialized public health education in higher institutions.21
The relationship between income and UI knowledge demonstrated diverse outcomes. Consistent with our findings, Mandimika et al study found that the odds of lacking proficient UI knowledge was 158 times higher in participants with an income of (10,000–49,000$) relative to those with >100,000$,10 while higher awareness of UI was evident in respondents receiving among higher-income groups (>50,000$) in another study.18 These findings may reflect better access to quality education among economically stable individuals. However, a study conducted in the US demonstrated a non-significant correlation between income and UI awareness upon multivariate analysis23 possibly due to differences in the demographic composition of the study population and presence of confounding factors that could collectively contribute to these discrepancies across various studies.
Consistent with previous literature,18 no significant association was established between UI awareness and prior urogynecology consultation, potentially due to limited consultation time, high clinic workload, or variable patient engagement. In addition, previous UI history was not significantly associated with UI knowledge in our study, aligning with findings from multiple States, Massachusetts, Johnson City, and Connecticut, where social stigma and symptom misattribution to aging were suggested as contributing factors.10,18,22 Nevertheless, Chen et al25 found that absent prior UI history remained independently associated with non-proficient UI knowledge.
In contrast, prior UI treatment was positively associated with higher knowledge levels, primarily as treatment planning involves a multifactorial approach that focuses on discussing symptoms, avoiding modifiable risk factors, and treating the underlying cause. However, UI knowledge proficiency remained non-significantly associated with prior treatment according to Mandimika et al cross-sectional survey.10 The discrepancies in outcomes pertaining to the association between prior UI treatment and awareness across various studies could be attributed to the study population characteristics.
Although multiple variables demonstrated a significant correlation to UI knowledge in Spearman’s correlation analysis, only higher levels of knowledge and receiving prior treatment to UI remained statistically significant in the multivariate analysis model after adjustment to potential confounding factors. While some studies reported findings consistent with our results, demonstrating significant independent correlations between prior treatment to UI and UI knowledge levels,7 as well as, between higher educational levels and UI awareness,7,20 they additionally identified other independently associated variables that were not demonstrated in our findings. For instance, in a study conducted in the same region increasing parity emerged as a significant independent predictor to UI knowledge.7 Additionally, in contrast to our findings, another study conducted in Singapore involving third-trimester pregnant women showed significant independent correlation between age and UI knowledge proficiency.21 Discrepancy in finding across different studies may be attributed to variation in the characteristics of the study population and differences in methodological approach.
Despite providing valuable insights into the knowledge and awareness of UI among patients at the urogynecology clinic in KHMC, certain limitations must be acknowledged. First, the use of convenience sampling solely within the KHMC clinic may restrict the generalizability of our findings to the broader population of Jordanian women and to the broader MENA and global population. Secondly, the small population size of this study remains limited in accurately reflecting UI knowledge in Jordan. Moreover, the involvement of multiple interviewers may introduce interviewer bias and variability. Lastly, the cross-sectional design of the study limits our ability to establish causality or infer temporal relationships. These limitations underscore the need for cautious result interpretation and highlight potential areas for future research to address these constraints.
Conclusions
The study demonstrates positive correlations between education, involvement in the medical field, higher income and education levels, and receiving previous treatment for urinary incontinence with higher knowledge and awareness. Future studies must aim to establish a comprehensive understanding of the knowledge deficits regarding UI that demand specific attention and focused interventions to enhance existing knowledge and awareness levels, tackle misinformation, and improve the overall health status of women.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available but may be made available from the corresponding author upon reasonable request.
Ethical Approval and Informed Consent
This study adhered to ethical standards set by the World Medical Association’s Declaration of Helsinki principles. Verbal informed consent was obtained from the study participants prior to study commencement which was approved by The Hashemite University Institutional Review Board (approval number: 2300604).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Irwin DE, Kopp ZS, Agatep B, Milsom I, Abrams P. Worldwide prevalence estimates of lower urinary tract symptoms, overactive bladder, urinary incontinence and bladder outlet obstruction. BJU Int. 2011;108(7):1132–11. doi:10.1111/J.1464-410X.2010.09993.X
2. O’Reilly N, Nelson HD, Conry JM, et al. Screening for urinary incontinence in women: a recommendation from the women’s preventive services initiative. Ann Intern Med. 2018;169(5):320–328. doi:10.7326/M18-0595
3. Kenton KS, Smilen SW. ACOG practice bulletin no. 155: urinary incontinence in women. Obstetrics Gynecol. 2015;126(5):E66–E81. doi:10.1097/AOG.0000000000001148
4. Lukacz ES, Santiago-Lastra Y, Albo ME, Brubaker L. Urinary incontinence in women: a review. JAMA. 2017;318(16):1592–1604. doi:10.1001/JAMA.2017.12137
5. Wu JM. Stress incontinence in women. N Engl J Med. 2021;384(25):2428–2436. doi:10.1056/NEJMCP1914037
6. Soysal P, Veronese N, Ippoliti S, et al. The impact of urinary incontinence on multiple health outcomes: an umbrella review of meta-analysis of observational studies. Aging Clin Exp Res. 2023;35(3):479–495. doi:10.1007/S40520-022-02336-0
7. Al-Kharabsheh AM, Abufraijeh SM, Al-Nawaiseh N. Validation of the Arabic linguistic version of the prolapse and incontinence knowledge questionnaire. Int Urogynecol J. 2024;35(7):1435–1446. doi:10.1007/s00192-024-05823-2
8. Mahfouz IA, Blanker MH, Asali F, et al. Seeking consultation for urinary incontinence: behaviours and barriers among Jordanian women. Neurourol Urodyn. 2023;42(6):1299–1310. doi:10.1002/NAU.25189
9. Hammad FT. Prevalence, social impact and help-seeking behaviour among women with urinary incontinence in the Gulf countries: a systematic review. Eur J Obstetrics Gynecol Reprod Biol. 2021;266:150–156. doi:10.1016/j.ejogrb.2021.10.005
10. Mandimika CL, Murk W, Mühlhäuser McPencow A. Knowledge of pelvic floor disorders in a population of community-dwelling women. Am J Obstet Gynecol. 2014;210(2):165.e1–165.e9. doi:10.1016/j.ajog.2013.10.011
11. Rostami P, Mostafaei H, Salehi-Pourmehr H, Hajebrahimi S. An updated systematic review and meta-analysis on the prevalence of female urinary incontinence in developing countries-a collaborative report by the international continence society (developing world committee) and the Iranian research center for eviden…. Neurourol Urodyn. 2025;44(8):1639–1668. doi:10.1002/NAU.70127
12. LaCoursiere DY, D. Cunningham S, P. Vaughan C, et al. A scoping review of quantitative assessments of women’s bladder health knowledge, attitudes, and beliefs. J Womens Health. 2025;34(9):1099–1124. doi:10.1089/JWH.2024.0997
13. Komon W, Manonai J, Kijmanawat A, et al. Validation of the Thai version of the prolapse and incontinence knowledge questionnaire (PIKQ). Int Urogynecol J. 2022;33(11):3045–3052. doi:10.1007/S00192-021-05020-5
14. Aydemir D, Çıtak Karakaya İ, Günay Avcı S, Gürhan Karakaya M. Psychometric properties and feasibility of three scales assessing the level of knowledge and awareness about pelvic floor health. Eur J Obstet Gynecol Reprod Biol. 2024;301:135–141. doi:10.1016/J.EJOGRB.2024.07.035
15. Equator network. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies | the EQUATOR network. 2023. Available from: https://www.equator-network.org/reporting-guidelines/strobe/.
16. PuszczałowskaLizis E, Rychter P, Wilczyński M. Factors determining the knowledge of women aged 30-40 from the Rzeszów poviat about urinary incontinence. Polish J Physiother. 2022;22(1):198–206.
17. Saxer S, de Bie RA, Dassen T, Halfens RJ. Nurses’ knowledge and practice about urinary incontinence in nursing home care. Nurse Educ Today. 2008;28(8):926–934. doi:10.1016/j.nedt.2008.05.009
18. Hobdy D, Huffaker RK, Bailey B. Comprehension of pelvic organ prolapse and urinary incontinence in southern appalachian women. Southern Med J. 2018;111(1):18–22. doi:10.14423/SMJ.0000000000000746
19. Susiarno H, Prakasa R, Handono B. Knowledge and severity of female urinary incontinence and reasons for not seeking treatment. Majalah Kedokteran Bandung. 2021;53(3):138–142. doi:10.15395/mkb.v53n3.2310
20. O’Neill AT, Hockey J, O’Brien P, et al. Knowledge of pelvic floor problems: a study of third trimester, primiparous women. Int Urogynecol J. 2017;28(1):125–129. doi:10.1007/s00192-016-3087-4
21. Liu J, Tan SQ, Han HC. Knowledge of pelvic floor disorder in pregnancy. Int Urogynecol J. 2019;30(6):991–1001. doi:10.1007/s00192-019-03891-3
22. Branch LG, Walker LA, Wetle TT, DuBeau CE, Resnick NM. Urinary incontinence knowledge among community-dwelling people 65 years of age and older. J Am Geriatr Soc. 1994;42(12):1257–1262. doi:10.1111/j.1532-5415.1994.tb06507.x
23. Mckay ER, Lundsberg LS, Miller DT, et al. Knowledge of pelvic floor disorders in obstetrics. Female Pelvic Med Reconstructive Surg. 2019;25(6):419–425. doi:10.1097/SPV.0000000000000604
24. Nur farihan M, Ng BK, Phon SE, Nor Azlin MI, Nur Azurah AG, Lim PS. Prevalence, knowledge and awareness of pelvic floor disorder among pregnant women in a tertiary centre, Malaysia. Int J Environ Res Public Health. 2022;19(14):8314. doi:10.3390/ijerph19148314
25. Chen CCG, Cox JT, Yuan C, Thomaier L, Dutta S. Knowledge of pelvic floor disorders in women seeking primary care: a cross-sectional study. BMC Family Pract. 2019;20(1):70. doi:10.1186/s12875-019-0958-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Caregiver Perspectives on Physiotherapy Treatment for Paediatric Burns in the United Arab Emirates
Mohamed Muftah Alzaabi FS, Bairapareddy KC, Alaparthi GK, Hegazy F
Patient Preference and Adherence 2022, 16:1477-1486
Published Date: 17 June 2022
Knowledge and Awareness of Non-Technical Skills Over the Course of an Educational Program in Nursing - A Repeated Cross-Sectional Study
Wevling A, Olsen BF, Nygaard AM, Heiberg T
Advances in Medical Education and Practice 2023, 14:31-41
Published Date: 10 January 2023
Awareness and Knowledge of Adverse Effects of Topical Corticosteroids Among the General Population in Jeddah, Saudi Arabia
Roblah TM, Baabdullah AM
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3065-3075
Published Date: 26 October 2023
Ethical Awareness and Practices Among Emergency Department Personnel in Riyadh’s Tertiary Hospitals: A Cross-Sectional Analysis
Al-Wathinani AM, AlHokair AA, Almeshari AZ, Alsaqri FS, Aldaihan FM, Alrumeh AS, AlOtaibi AA, Alkanhal IA, Aljuaid M, Albusair MK, Alluhayb AA, Goniewicz K
Risk Management and Healthcare Policy 2024, 17:677-688
Published Date: 23 March 2024
Radiologic Technology Students’ Perceptions on Adoption of Artificial Intelligence Technology in Radiology
Arif WM
International Journal of General Medicine 2024, 17:3129-3136
Published Date: 16 July 2024