Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Artificial Intelligence–Enabled Multi-Omics for Predicting Immune Checkpoint Inhibitor Response and Resistance
Authors Wang X ![]() , He J, Ding G, Tang Y, Wang Q
, He J, Ding G, Tang Y, Wang Q
Received 4 October 2025
Accepted for publication 27 January 2026
Published 26 February 2026 Volume 2026:19 572089
DOI https://doi.org/10.2147/JMDH.S572089
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Brian Nyatanga
Xiaodong Wang, Jing He, Gouping Ding, Yixuan Tang, Qianqian Wang
Department of Oncology, Zhuzhou Hospital Affiliated to Xiangya School of Medicine, Central South University, Zhuzhou, People’s Republic of China
Correspondence: Qianqian Wang, Email [email protected]
Abstract: Immune checkpoint inhibitors (ICIs) have reshaped oncology, yet overall response rates remain modest and resistance is common, driven by tumor heterogeneity and evolving tumor–immune crosstalk. Established biomarkers (PD-L1, tumor mutational burden, microsatellite instability) provide incomplete prediction. Multi-omics profiling across genomic, transcriptomic, proteomic, epigenomic, metabolomic and microbiomic layers offers a systems-level view of malignant and immune states, uncovering determinants of ICI efficacy such as lineage plasticity, stromal remodeling, immunometabolic reprogramming and microbiome-associated immune modulation. Artificial intelligence (AI) is uniquely positioned to fuse these heterogeneous data, learn non-linear cross-layer signatures, and enable interpretable predictions using approaches such as SHAP and Grad-CAM. Representative models link routine histology or imaging to molecular phenotypes, stratify patients beyond single biomarkers, and may nominate rational combinations that target oncogenic pathways, lactate-driven immune suppression, or the gut microbiome. In this narrative review, we synthesize recent AI–multi-omics advances for response modeling, immune-relevant tumor subtyping, and clinical translation, including radiomics/pathomics integration and liquid-biopsy–based monitoring, as well as emerging applications in toxicity risk prediction. We also discuss barriers to implementation—platform heterogeneity, limited prospective validation, bias, interpretability and cost—and outline future directions, including single-cell and spatial multi-omics integration, federated learning and generative modeling to improve robustness and equity of precision immunotherapy.
Keywords: artificial intelligence, multi-omics, immunotherapy, cancer, biomarkers
Introduction
Immune checkpoint inhibitors (ICIs) targeting PD-1, PD-L1, and CTLA-4 have reshaped oncology by restoring anti-tumor immunity, enabling durable remissions in subsets of patients with melanoma, non-small cell lung cancer (NSCLC), renal cell carcinoma (RCC), and other malignancies.1–3 However, overall response rates remain modest (~20–40%), and both primary and acquired resistance are common.1,4 These failures reflect profound tumor heterogeneity, diverse immune-evasion programs, and dynamic tumor–immune crosstalk within the tumor microenvironment (TME).5,6 Conventional biomarkers—including tumor PD-L1 expression, tumor mutational burden (TMB), and microsatellite instability (MSI)—provide only limited predictive accuracy and often miss the multifactorial determinants of response, motivating integrative, high-dimensional strategies for precision immunotherapy.7,8
Multi-omics profiling, spanning genomics, transcriptomics, proteomics, epigenomics, metabolomics, and microbiomics, offers a layered systems view of malignant cells and immune contexture and has uncovered mechanisms that shape ICI efficacy across cancer types.8–10 In diffuse large B-cell lymphoma, genomic alterations such as TP53 and CREBBP mutations correlate with non-response, whereas responders often exhibit transcriptomic programs consistent with immune activation and cytotoxic T-cell engagement.11,12 In NSCLC, single-cell transcriptomics has traced some tumors to alveolar type II origins and revealed lineage plasticity driven by pathways such as SOX2/WNT/YAP, fostering immunosuppressive TMEs and ICI resistance.13,14 Epigenomic dysregulation can further promote immune escape; for example, enhancer activation in nasopharyngeal carcinoma upregulates oncogenic programs (eg, CACNA2D1) linked to immune evasion.15 Metabolomic reprogramming also contributes, including lactate-associated lactylation that reinforces suppressive states.16 The microbiome adds an additional regulatory layer: gut microbial communities can modulate systemic immunity and ICI responsiveness, with responder–non-responder differences in taxa composition (including enrichment patterns involving Bacteroides species) and consistent evidence that antibiotic-mediated microbiome disruption impairs outcomes.17,18
Artificial intelligence (AI), spanning machine learning (ML) and deep learning (DL), is well suited to integrating heterogeneous multi-omic data and extracting non-linear, cross-layer signatures that conventional statistics often miss.19,20 AI-driven “pathomics” can predict MSI status in colorectal cancer with AUCs around 0.85 by linking morphologic patterns to underlying molecular programs.21 In melanoma, a LASSO-regression model combining exome sequencing and RNA-seq outperformed TMB alone, with AUCs near 0.7 in training and ~0.64 on independent testing.22 Importantly, interpretability tools such as SHAP and Grad-CAM can connect predictions to specific features (eg, mutations, expression programs, or informative histologic regions), improving mechanistic insight and clinical trust.
Early translational studies underscore the promise of AI-enabled multi-omics for patient stratification and therapeutic design. In NSCLC, integrative models incorporating genomic, transcriptomic, and radiomic inputs improve response prediction relative to unimodal approaches.23,24 In hepatocellular carcinoma and bladder cancer, extreme heterogeneity and sampling constraints limit single-biopsy biomarkers, accelerating interest in multi-omic liquid biopsies for real-time monitoring of evolving disease.25,26 Integrative AI–multi-omics frameworks aim to refine tumor subtypes and nominate tailored combinations, including pairing ICIs with targeted agents addressing FGFR/EGFR pathway alterations; research trends also highlight growing interest in multi-target strategies and microbiome modulation to overcome resistance.
This narrative review synthesizes mechanistic foundations and clinical applications of AI–multi-omics approaches for predicting ICI responses. We qualitatively integrate findings across platforms and tumor types, highlight state-of-the-art predictive models, discuss translational challenges, and outline future directions including single-cell integration paradigms, federated learning, and cross-disciplinary innovation, with explicit attention to gaps in validation and equity.
Biological Foundations of ICI Response and Multi-Omics Insights
Molecular Mechanisms of ICI Efficacy and Resistance
By blocking inhibitory signaling (PD-1/PD-L1 and CTLA-4 axes), ICIs restore cytotoxic T-cell function.27 Efficacy nevertheless varies because tumors can induce T-cell dysfunction (exhaustion) and/or physically exclude immune cells from tumor nests, and because TMEs differ in stromal and immune composition.28,29 In NSCLC, single-cell transcriptomics traces subsets of tumors to alveolar progenitor origins and implicates lineage plasticity driven by developmental programs such as SOX2/WNT/YAP.30 This plasticity fosters immunosuppressive niches enriched for cancer-associated fibroblasts and macrophages whose reciprocal interactions impede T-cell infiltration and effector function, promoting immune evasion across immune-editing phases.31 These datasets also highlight potential vulnerabilities: specific immune and stromal subsets, including CXCL13⁺ CD8⁺ T cells and antigen-presenting fibroblasts, are enriched in “hot,” inflamed tumors and may be leveraged to strengthen anti-tumor immunity.32
The gut microbiome provides an additional systemic control point. In some settings, fecal microbiota transplantation from immunotherapy responders enhances anti-tumor T-cell activity in recipients, supporting a functional role for commensals and microbe-derived metabolites, while also underscoring that non-optimized transplantation could introduce or amplify immunosuppressive elements.33,34 In NSCLC, metagenomic profiling links response to greater abundance of taxa such as Bacteroides (eg, Bacteroides caccae) and Prevotella, whereas antibiotic exposure can reduce microbial diversity and impair ICI efficacy by depleting beneficial taxa or enriching pathways that suppress immunity.35,36
In RCC, large transcriptomic cohorts (including datasets from >1000 patients) integrated with single-cell and spatial profiling reveal outcome-linked immune–tumor crosstalk.37 Responders are characterized by pro-inflammatory macrophages engaging exhausted CD8⁺ T cells and by patient-specific HLA allele variants that preferentially present particular neoantigens.37 Non-responding tumors more often activate alternative immunosuppressive programs.38 Notably, machine-learning analyses of HLA profiles identify allele “signatures” that favor high-quality neoantigen presentation and predict improved outcomes, underscoring the importance of HLA genotype and neoantigen landscape in shaping ICI success.39
Tumor genetics can further constrain benefit. In gastrointestinal cancers, loss-of-function alterations in CREBBP and TP53 are enriched in non-responders to PD-1 blockade, likely through effects on antigenicity and immune-related signaling, with context dependence that may vary by PD-L1 expression in the TME.40,41 Beyond DNA sequence, epigenomic and metabolic reprogramming contributes to resistance: lactate accumulation can drive histone lactylation, inhibit T-cell function, and associate with resistance to both ICIs and radiotherapy, consistent with metabolite-to-chromatin feedback loops that reinforce immune suppression.42,43 In bladder cancer, multi-omics assays also enable immune-relevant subclassification; for example, DNA methylation profiling from liquid biopsy samples can distinguish luminal versus basal subtypes with distinct immune landscapes and differential ICI sensitivity, informing treatment selection.44
Taken together, these mechanisms define a continuum from “hot” tumors—high neoantigen load, inflamed TME, and robust T-cell infiltration—to “cold” tumors that exhibit immune exclusion or suppression due to dense stroma, high cancer cell stemness, particular microbiome configurations, or immunosuppressive metabolites. Hot tumors are generally more responsive to ICIs, whereas cold tumors often require combination strategies to convert the TME into an immune-permissive state (Figure 1 and Table 1).
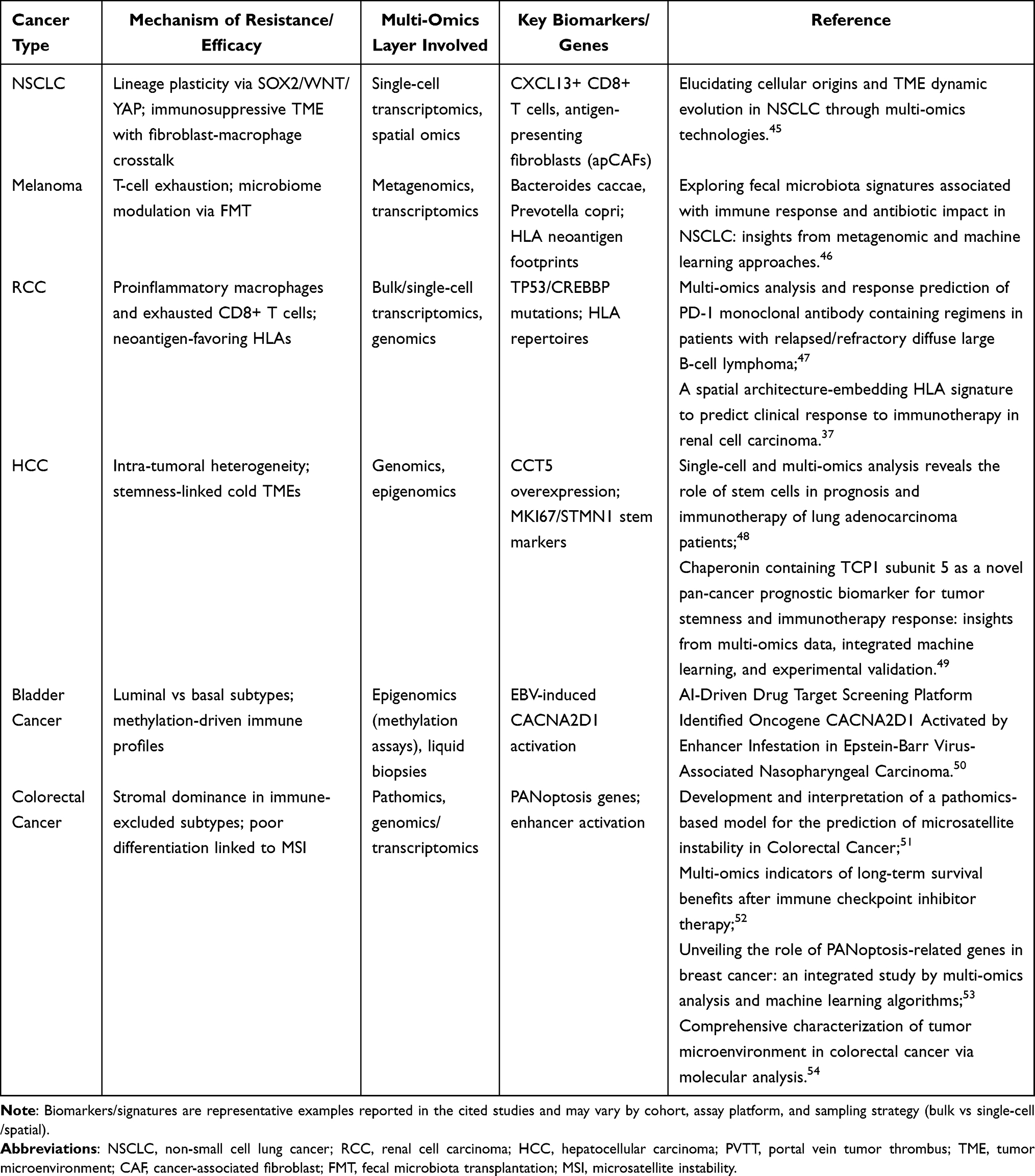 |
Table 1 Key Biological Mechanisms and Multi-Omics Insights Across Cancers |
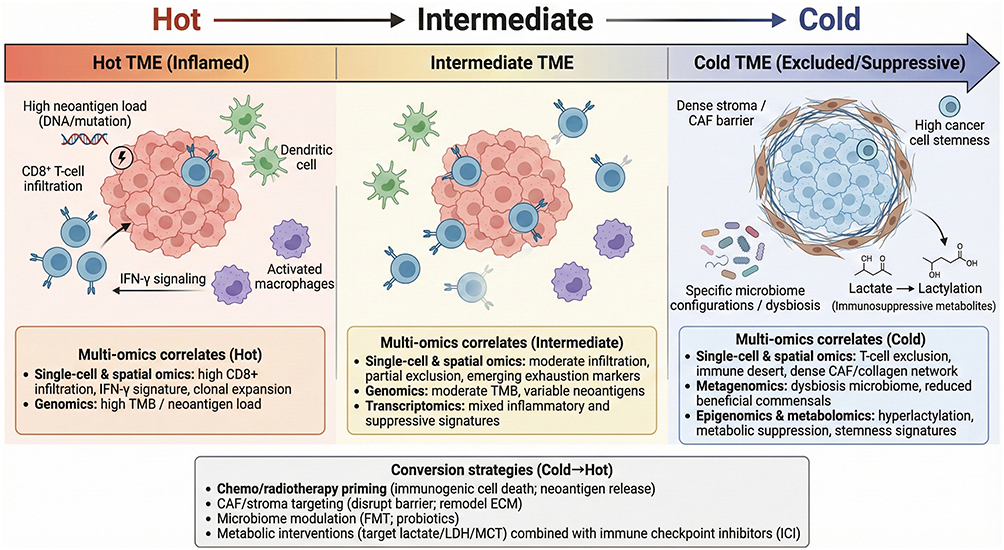 |
Figure 1 Hot–Intermediate–Cold tumor immune microenvironment continuum. Schematic overview of the spectrum of tumor immune microenvironments (TMEs) from hot (inflamed) to cold (excluded/suppressive). Hot TMEs feature high neoantigen load, prominent CD8β+ T-cell infiltration, and IFN-γ–associated immune activation, whereas intermediate TMEs show moderate infiltration with partial exclusion and emerging exhaustion features. Cold TMEs are characterized by T-cell exclusion and immune desert phenotypes driven by dense stroma/cancer-associated fibroblast (CAF) barriers, increased tumor cell stemness, dysbiotic microbiome configurations, and immunosuppressive metabolites (eg, lactate-linked lactylation). Representative multi-omics correlates across states and candidate cold→hot conversion strategies (eg, chemo/radiotherapy priming, stromal targeting, microbiome modulation, and metabolic interventions combined with immune checkpoint inhibitors) are summarized. |
Tumor Heterogeneity and Cancer Stemness in Immune Evasion
Intratumoral heterogeneity enables cancers to adapt under immune pressure, as distinct subclones deploy different genetic and phenotypic escape routes, undermining uniform responses to ICIs.55,56 Cancer stemness further amplifies resistance: stem-like tumor cells with self-renewal, quiescence, and multilineage potential can persist despite immune attack and regenerate disease.57 Quantitative stemness metrics, including an mRNA expression–based stemness index (mRNAsi) and algorithms such as CytoTRACE, link elevated stemness to immunosuppressive microenvironments and attenuated ICI responses in pan-cancer analyses.58
Across tumor types, specific mediators of stemness correlate with immune exclusion. The chaperonin CCT5 is frequently overexpressed in proliferative, stem-like cancer cells and associates with “cold” TMEs marked by sparse tumor-infiltrating lymphocytes and reduced CD8⁺ T-cell presence.59,60 Single-cell and spatial multi-omics suggest that CCT5 supports DNA repair and stress-response programs, and its overexpression correlates with inferior ICI outcomes across cohorts.59 In lung adenocarcinoma, stem-like subpopulations enriched for proliferation markers such as MKI67 and STMN1 contribute to intratumoral heterogeneity and are associated with cold immune profiles (minimal CD8⁺ infiltration) and poor ICI response; cohort analyses further link high stemness to reduced T-cell infiltration on immunofluorescence and worse outcomes after checkpoint blockade.48,61
Other malignancies show parallel biology. In nasopharyngeal carcinoma, Epstein–Barr virus–associated enhancer activation upregulates stemness-linked oncogenes such as CACNA2D1; experimental inhibition of CACNA2D1 reduces stem-like properties and increases immune vulnerability.50,62 In breast cancer, emerging PANoptosis-based subtypes differ in immune infiltration, and high stemness in aggressive subtypes aligns with pathways that exclude or suppress immune cells.63 In colorectal cancer, an immune-excluded subtype features a dominant stromal compartment that physically and biochemically blocks T-cell entry into the tumor core, yielding T-cell absence despite antigen presence and associating with poor differentiation, high heterogeneity, and MSI-related genomic instability patterns.64,65
Single-cell multi-omics further clarifies the niche logic of resistance. In urothelial carcinoma, combined bulk and single-cell RNA sequencing implicates myeloid-rich microenvironments in PD-1/PD-L1 resistance, consistent with niches that nurture stem-like, immune-evasive tumor states.66,67 Moreover, rare tumor subsets undergoing epithelial–mesenchymal transition can enter persister states expressing stem-cell markers (eg, Snail1), appear intrinsically resistant to PD-1 blockade, survive treatment, and drive relapse.68 Figure 1 and Table 1 summarize these pathways and representative multi-omic correlates of ICI efficacy and resistance.
AI-Driven Multi-Omics Integration for Biomarker Discovery
AI Algorithms in Multi-Omics Data Processing
Machine learning and deep learning are well suited to the dimensionality and heterogeneity of multi-omics datasets. Techniques such as LASSO regression, random forests, support vector machines, and deep neural networks (including convolutional neural networks) can integrate diverse feature types into robust predictors.23,24 In colorectal cancer, an ensemble multiple instance learning approach combined whole-slide histopathology with genomic and transcriptomic data to predict MSI status with an AUC of ~0.85, connecting subtle histologic patterns to mutation burden and immune pathway activation signatures.21,69 Such models can be adapted across cohorts via transfer learning, improving generalizability while retaining biologically interpretable signals.21,69
Deep learning is particularly useful for imaging–molecular integration. In NSCLC, a DenseNet-based network extracted radiomic features from routine CT scans and combined them with blood inflammatory markers to predict ICI outcomes, achieving AUCs >0.80 in training and ~0.86 in independent validation cohorts.24,70 Interpretability methods such as Grad-CAM have been applied to localize tumor regions driving predictions, providing imaging correlates of immune-active versus immune-suppressive biology.71 For microbiome data, random forest classifiers trained on fecal metagenomic profiles identified gut microbial patterns associated with ICI responsiveness; in that analysis, enrichment of certain Bacteroides species aligned with response, whereas antibiotic-associated loss of microbial diversity aligned with non-response.17,18
Beyond response prediction, AI enables cross-domain data fusion for safety and target discovery.72 In cardio-oncology, AI has integrated genomic, proteomic, and clinical data to identify multi-omics biomarkers that may predict ICI-related cardiotoxicity.73 In nasopharyngeal carcinoma, an AI platform integrating genomic, epigenomic, and transcriptomic profiles prioritized driver candidates and highlighted CACNA2D1 as activated by EBV-related enhancers; laboratory validation supported a role in immune evasion, and inhibition reduced tumor growth, nominating CACNA2D1 as a therapeutic target.15,50 Bibliometric analyses of recent literature further indicate accelerating growth of AI–multi-omics applications in immunotherapy biomarker research, consistent with a broader shift toward data-driven precision medicine.74
Predictive Models for ICI Response
Capitalizing on patterns extracted by AI, multiple predictive models have been constructed to forecast ICI benefit, frequently outperforming single biomarkers such as TMB or PD-L1 expression alone.75 Artificial neural networks and ensemble methods (eg, gradient-boosted decision trees) commonly integrate mutations, immune transcripts, immune-cell abundance, imaging-derived features, and clinical variables into composite predictors of response probability.76
In melanoma, a LASSO model fusing exome sequencing features with RNA-seq immune transcripts achieved an AUC of ~0.70 in training and ~0.64 in an independent test set, outperforming conventional mutational metrics such as non-synonymous TMB.19,77 In relapsed DLBCL, an ANN incorporating tumor PD-L1 score, patient age, and recurrent mutations (including TP53 and CREBBP) achieved AUCs of 0.97 (training) and 0.94 (testing) for anti–PD-1 response prediction.78 Analyses of model weights indicated that features reflecting spatial immune cell organization (eg, immune-cell proximity and localization patterns derived from pathology) were strongly linked to predicted outcomes, suggesting that the ANN learned clinically meaningful connections between tissue architecture and immunotherapy efficacy.12,78
In advanced gastroesophageal cancers, AI-derived genomic mutation signatures have been reported to predict overall survival after immunotherapy with high sensitivity and stable performance across cohorts, outperforming TMB and PD-L1 status as prognostic indicators.40,79 Such models can also propose combination strategies; one framework nominated the MEK inhibitor trametinib for “high-risk” patients based on an inverse correlation between signature score and trametinib IC50 in model systems.79 Stemness-associated modeling provides additional biologic resolution. In LUAD, a prognostic model combining CoxBoost and elastic net evaluated stem cell–associated genes (eg, MKI67 and STMN1) with immune markers and stratified ICI response with modest accuracy (AUC ~0.65); high stemness scores aligned with reduced CD8+ T-cell infiltration and worse outcomes, consistent with a cold tumor microenvironment.48,58
In HCC, an AI model integrating SNP variants, gene expression, and clinical factors has been used to predict ICI response and guide conversion strategies (eg, adding locoregional therapies) for patients unlikely to respond to ICIs alone.80,81 In NSCLC, multi-omics predictors have been extended to the neoadjuvant setting: integrating radiomic features with genomic and transcriptomic data can forecast pathologic response (eg, major pathological response) to neoadjuvant immunochemotherapy and inform perioperative decision-making.24 Reported performance across cancer types is summarized in Table 2, with several models externally validated.
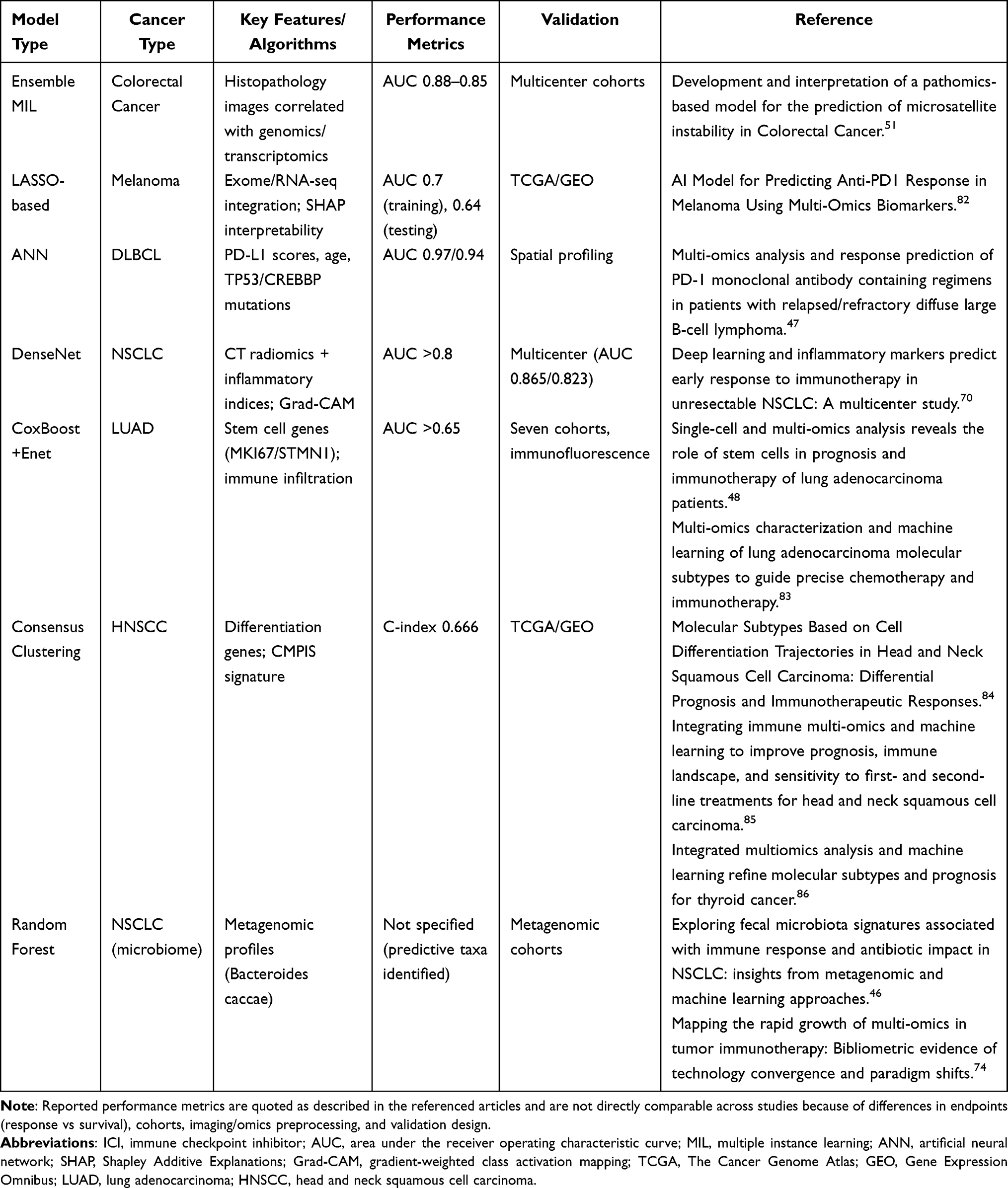 |
Table 2 Performance of AI Predictive Models for ICI Response |
Subtype Classification and Patient Stratification
Beyond predicting binary response, AI and multi-omics have been used to classify tumors into subtypes with distinct immunotherapy sensitivities, guiding selection of ICIs alone versus combination regimens.87 In HNSCC, unsupervised clustering of differentiation-related gene expression revealed three robust subtypes characterized by stromal/mesenchymal features, metabolic programs, or immune activation.88 Low-differentiation (dedifferentiated, mesenchymal-like) tumors tended to be immune-inflamed and respond better to anti–PD-1/PD-L1, whereas more differentiated tumors were often immune-cold.89
Machine learning has extended these stratifications into prognostic signatures. A composite immunotherapy sensitivity signature (CMPIS) for HNSCC achieved a concordance index of ~0.66 and suggested treatment tailoring: hot tumors (low differentiation score, high immune infiltration) benefit more from ICIs or chemotherapy, whereas cold tumors (high differentiation score, low infiltration) may respond better to radiotherapy or EGFR-targeted agents.19,85 In melanoma, integrative analyses of TCGA and GEO datasets identified subtypes with different immunotherapy outcomes; one subtype with low signature scores corresponded to highly immunogenic hot tumors enriched for interferon-γ programs and active T-cell infiltration, associated with improved outcomes on ICIs.90
In NSCLC, multi-omics stratification has refined LUAD taxonomy; one subgroup driven by lineage plasticity and oncogenic pathways showed an immune-excluded microenvironment and resistance to both immune checkpoint blockade and tyrosine kinase inhibitors, implying a need for alternative or dual strategies.13,30 In bladder cancer, emerging work integrates genomic and transcriptomic profiles with liquid-biopsy features (circulating tumor DNA and circulating tumor cells) to infer luminal versus basal phenotypes noninvasively and predict ICI benefit.91 Metabolic–epigenomic integration is also expanding: models incorporating lactylation patterns suggest a lactate-driven immune-evasion state that may benefit from rational combinations such as immunotherapy plus radiotherapy.42
Figure 2 schematizes the integrated AI–multi-omics workflow: genomics, transcriptomics, epigenomics, metabolomics, microbiomics, pathomics, and radiomics feed into an AI core using feature selection and representation learning (LASSO, random forests, DenseNet-class networks, multiple instance learning). Outputs include biomarker/target prioritization (eg, TP53, CREBBP, CACNA2D1), predictive response models summarized by ROC curves and interpreted with SHAP-like attribution, and immune-relevant subtype calls distinguishing immune-inactive tumors, hot inflamed tumors, and strongly immunosuppressive subtypes to support patient stratification and treatment tailoring.
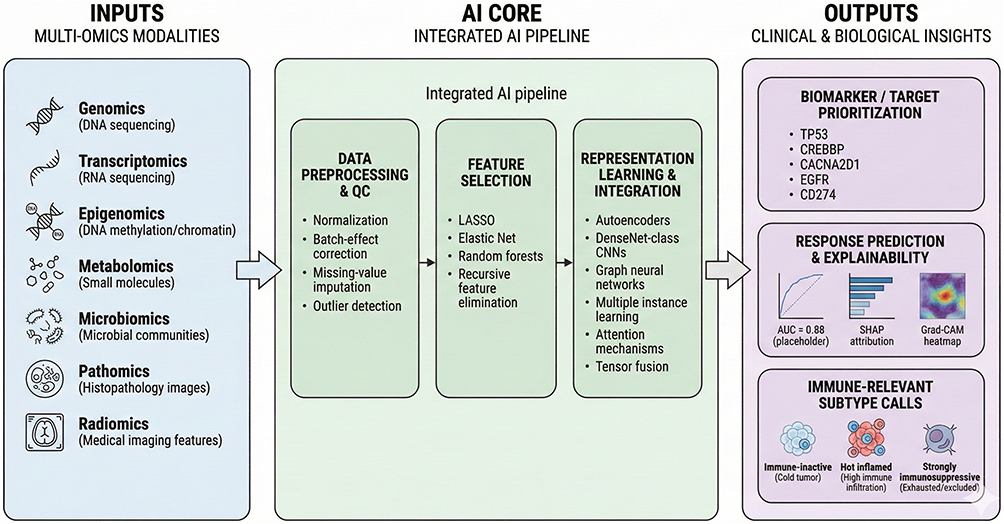 |
Figure 2 Integrated AI pipeline for multi-omics integration and clinical outputs. End-to-end workflow linking multi-omics inputs (genomics, transcriptomics, epigenomics, metabolomics, microbiomics, pathomics, and radiomics) to an AI core composed of data preprocessing/quality control (normalization, batch-effect correction, missing-value imputation, and outlier detection), feature selection (eg, LASSO, elastic net, random forests, recursive feature elimination), and representation learning/integration (eg, autoencoders, CNNs, graph neural networks, multiple-instance learning, attention mechanisms, and tensor fusion). The pipeline outputs clinically actionable results, including biomarker/target prioritization, treatment response prediction with explainability (eg, AUC/ROC, attribution scores, and heatmap-based localization), and immune-relevant subtype calls (immune-inactive/cold, hot inflamed, and strongly immunosuppressive exhausted/excluded) to support patient stratification. |
Clinical Applications and Translational Challenges
Predicting Therapeutic Outcomes and Guiding Combination Therapies
AI–multi-omics frameworks are increasingly used to anticipate ICI outcomes before, or early during, treatment and to guide selection of monotherapy versus combination regimens.23,77 In melanoma, an integrative model combining tumor exome and transcriptome features predicts anti–PD-1 efficacy with an AUC of about 0.7 and stratifies patients by expected benefit from combination approaches.77 Low predicted response scores often correspond to immune-cold tumors with limited T-cell infiltration; such patients can be triaged to ICI plus cytotoxic chemotherapy to induce tumor inflammation, whereas high-score patients may proceed with ICI monotherapy.13,19 Early trials guided by this logic suggest improved outcomes when chemotherapy is added for low-score patients, illustrating how model-based stratification can individualize intensity of care.3,92
In advanced gastroesophageal cancers, AI-driven genomic signatures have been used to forecast overall survival benefit from ICIs and to identify patients unlikely to benefit from immunotherapy alone.40,79 Tumors classified as high risk displayed profiles consistent with sensitivity to targeted agents, leading to the MEK inhibitor trametinib as a candidate partner for ICIs in this subgroup and motivating follow-up studies.40,79 In another setting, immunogenomic modeling of treatment-resistant cancers has suggested HSP90 inhibitors as ICI partners, weakening resistance and improving antigen presentation.93 These analyses generate mechanistically plausible, trial-testable hypotheses for overcoming immune escape.
Rational combination strategies extend beyond drug–drug pairing to include modulation of the microbiome and tumor metabolism. In non-small-cell lung cancer (NSCLC), fecal microbiota transplantation (FMT) is being explored to shift the gut microbiome toward states associated with improved ICI responsiveness.18,36 AI analyses of microbiome profiles have identified taxa associated with better outcomes, including Prevotella copri, suggesting that enriching such commensals through FMT or probiotics may be beneficial.17 Early clinical studies indicate that transferring stool from an ICI responder to a non-responder can sometimes induce responses in the recipient, but safety, donor selection, and microbiome profiling remain crucial and could be strengthened by AI-guided matching.34,94
On the metabolic front, multi-omics integration has implicated lactylation-linked programs in resistance.95 Models combining epigenomic and transcriptional features can identify tumors most driven by lactylation-associated regulatory patterns, motivating strategies that reduce lactate production or block lactate transport and signaling (for example, LDH inhibition or lactate-transporter blockade) alongside ICIs.16,43 These approaches are being evaluated to sensitize resistant tumors and to synergize immunotherapy with radiotherapy.
AI-based stratification can also inform modality choice and sequencing. In head and neck squamous cell carcinoma (HNSCC), the CMPIS immunotherapy sensitivity signature helps distinguish patients likely to do well with immunotherapy or conventional chemotherapy (immune-hot tumors with low risk scores) from those more likely to benefit from alternative options such as radiotherapy or EGFR-targeted inhibitors (immune-cold tumors with high risk scores).19,75 In hepatocellular carcinoma (HCC), models integrating tumor genomics with liquid-biopsy features are being explored to guide conversion strategies, in which patients predicted not to respond to ICIs alone may receive locoregional therapies (such as transarterial chemoembolization or radiofrequency ablation) alongside immunotherapy to reduce tumor burden and promote immune recognition.80,96
In NSCLC, multi-omics AI systems are being implemented in neoadjuvant immunotherapy-plus-chemotherapy trials to predict major pathologic response or pathologic complete response before surgery.24,70 Patients with low predicted probability of deep response can be triaged to alternative or intensified regimens, whereas those predicted to respond well can proceed without unnecessary additions that increase toxicity.24,97 Overall, these examples illustrate how AI–multi-omics can enable adaptive, response-guided immunotherapy, but prospective validation remains the decisive requirement for clinical uptake.
Real-World Evidence and Multicenter Validation
As AI–multi-omics models move toward clinical use, validation in real-world patient populations and across multiple centers is essential to avoid overfitting to a single cohort, platform, or workflow. In NSCLC, a model combining CT imaging features with peripheral inflammatory markers achieved AUCs of 0.865 and 0.823 in two external hospital-based validation sets, supporting reproducibility.24,70 In diffuse large B-cell lymphoma, an artificial neural network model predicting anti–PD-1 response achieved about 94% AUC in an independent cohort, closely mirroring training performance; concordant spatial immune-profiling results provided biological support for its predictions.78,98
Cross-cohort consistency has also been reported for genomic models in gastrointestinal cancers, where mutation-signature predictors maintained prognostic accuracy across multiple cohorts and outperformed tumor mutational burden in predicting overall survival after immunotherapy.40,79 Large consortia and public resources further enable validation: melanoma immune subtypes and machine-learning signatures initially derived from TCGA were reproduced in independent datasets and clinical-trial cohorts, confirming that immune-hot programs (including interferon signaling and T-cell–inflamed expression) associate with better outcomes under ICIs.19 In lung adenocarcinoma, stemness-based stratification applied to multiple independent cohorts consistently separated patients into risk groups, with predicted immune-cold cases showing low CD8 T-cell infiltration on immunofluorescence, consistent with the model’s biological premise.48,58
Another translational advantage is the potential to reduce invasive procedures through noninvasive monitoring. In bladder cancer, multicenter studies are evaluating AI-enhanced liquid-biopsy approaches that measure tumor DNA or methylation markers in urine and blood.44,99 Early results suggest that machine learning can detect recurrence or evolving resistance patterns without repeated cystoscopy or serial tissue biopsies, enabling earlier treatment adjustment while reducing patient burden.61,100
Validation efforts also reveal biases that must be addressed. Models trained in cohorts from specific geographic regions, care settings, or ancestral backgrounds may not generalize elsewhere without recalibration, underscoring the need for diverse training data and systematic external testing. Overall, multicenter evidence supports feasibility and sets the stage for embedding these tools into prospective trials and routine practice.
Challenges in Implementation
Despite promise, several barriers impede routine clinical use. Data heterogeneity is a dominant issue: multi-omics inputs arise from different platforms and protocols (sequencing chemistries, imaging devices, sample-processing methods, and analytic pipelines), and even modest variation can alter readouts and degrade model performance.23,101 Pre-analytical variability is particularly problematic for liquid biopsies, motivating efforts to harmonize specimen handling, establish quality-control standards, and implement shared normalization procedures so that models remain portable across laboratories.102
Tumor heterogeneity and evolving resistance further complicate prediction. In HCC, high mutational complexity and multiple resistance pathways, including angiogenesis programs and WNT/β-catenin signaling, limit the utility of static biomarkers.103,104 Maintaining accuracy may require longitudinal sampling, incorporation of on-treatment dynamics, and periodic model updating to reflect tumor evolution. Moreover, some AI-derived biomarkers are not easily actionable: a high-risk classification may reflect complex multi-gene patterns without a clear therapeutic lever, emphasizing the need for interpretable modeling and experimentally validated mechanisms.105
The black-box nature of many algorithms remains a hurdle for clinicians and regulators. Interpretability techniques, including SHAP-based feature attribution, attention visualization, and multi-omics correlation analysis, are essential to connect predictions to established biology and to support trust.71,106 For example, in colorectal cancer, deep-learning pathomics models predicting microsatellite instability gain credibility when attention maps are presented and linked to mismatch-repair alterations and immune infiltration, offering a plausible biological rationale for the output.21
Prospective evidence is still limited. Most results remain retrospective, and few trials are designed to test AI-guided treatment strategies as the intervention.107 Prospective studies are beginning—for example, neoadjuvant NSCLC programs such as CAMEL that incorporate multi-omics and AI for subgroup analyses of response determinants—but definitive evidence may require randomized designs comparing AI-guided selection with standard decision-making, measuring outcomes, toxicity, and resource use.70 Such trials also demand prespecified decision rules, timely data turnaround, and clear accountability for how recommendations are applied.
Equity and global representativeness are additional concerns. AI–omics research is concentrated in a limited number of countries and centers, raising risks of population bias and limited applicability.108 Expanding datasets to under-represented groups and tumor types, strengthening international collaboration, and using privacy-preserving approaches such as federated learning are critical to avoid widening disparities.109,110
Finally, cost and workflow integration must be addressed. Comprehensive multi-omics profiling can be expensive and slow;111 the field must demonstrate that added predictive value justifies cost or develop streamlined assays (for example, focused panels) that preserve performance while improving feasibility.112 Outputs must be clinically usable and timely, delivered as clear risk scores with interpretation at decision points and integrated into clinical decision-support systems. Regulatory pathways are evolving, and harmonized validation protocols will be needed before guideline-level endorsement becomes routine.113
Many of these challenges are summarized in Figure 3, which depicts the path from AI–multi-omics discovery to clinical application, emphasizing the need for real-world validation and solutions to heterogeneity, interpretability, and governance. Addressing these barriers will determine whether AI–multi-omics becomes routine in oncology practice and sets the stage for forthcoming technologies that further enhance predictive utility.
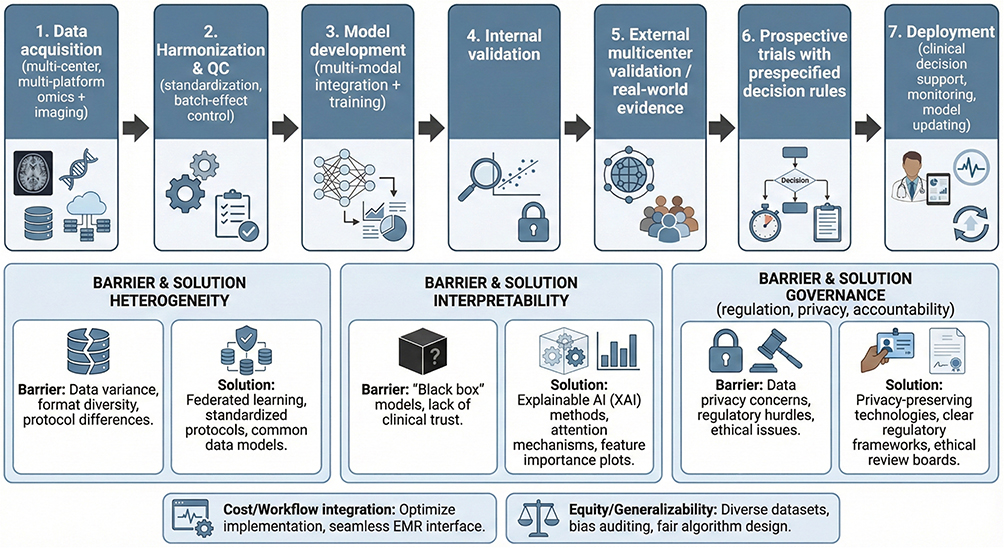 |
Figure 3 Translational roadmap for clinical deployment of AI–multi-omics models. Stepwise framework for moving AI–multi-omics models from development to real-world implementation: multicenter data acquisition (multi-platform omics and imaging), harmonization and QC (standardization and batch control), multimodal model development and training, internal validation, external multicenter validation/real-world evidence, prospective trials with prespecified decision rules, and deployment within clinical decision support with continuous monitoring and model updating. Key “barrier–solution” pairs are highlighted, including heterogeneity (federated learning, standardized protocols, common data models), interpretability and clinical trust (“black-box” concerns addressed by explainable AI), and governance (privacy-preserving technologies, regulatory frameworks, and ethical oversight), alongside practical considerations of cost/workflow integration and equity/generalizability. |
Future Directions and Emerging Technologies
Advanced AI–Multi-Omics Paradigms
A major frontier is the integration of single-cell and spatial omics with AI. Single-cell RNA sequencing and spatial transcriptomics can resolve the tumor microenvironment (TME) at cellular and micro-architectural scales, capturing heterogeneity and dynamic tumor–immune interactions that bulk profiling obscures.30,114 AI models that ingest spatiotemporal structure may better predict response trajectories that vary across tumor regions and evolve during therapy.115 In non-small-cell lung cancer (NSCLC), single-cell multi-omics has revealed spatial niches characterized by lineage plasticity and immune suppression linked to SOX2/WNT/YAP signaling.30,116 Incorporating such heterogeneity into AI frameworks could support spatially resolved predictions and suggest when and where adjunct interventions—such as adding an immune agonist or targeting specific sites with radiotherapy—might convert “cold” regions to “hot” and improve overall response.117,118
Federated learning is an increasingly relevant paradigm for multi-center immunotherapy modeling. In federated settings, data remain within the originating institutions while model updates are shared and aggregated, addressing privacy and governance barriers that limit pooled multi-omics studies.119,120 In pharmacogenomics, federated AI has already demonstrated the feasibility of discovering chemotherapy-response biomarkers across hospitals without centralizing raw patient data.121 Applying analogous infrastructure to immunotherapy could enable global consortia to jointly train ICI response predictors on diverse populations, thereby improving generalizability and reducing bias while maintaining confidentiality.122
Generative AI offers a complementary strategy to increase effective sample size, particularly for rare cancers, uncommon resistance phenotypes, and underpowered trials. Generative adversarial networks and diffusion models can synthesize multi-omics samples that preserve essential properties of real tumors.118,123 For single-cell data, synthetic immune-cell profiles can expand coverage of tumor-infiltrating states and improve robustness of downstream predictors.124 Early diffusion-based approaches have simulated realistic tumor gene-expression patterns and immune-cell distributions, providing a pragmatic route to strengthen model training when real examples are limited.125,126
Hardware and algorithmic innovation may further extend feasibility at the scale demanded by multi-omics. Quantum computing is being explored for its potential to address the combinatorial complexity of ultra-high-dimensional datasets.127 Although practical oncology applications remain nascent, quantum algorithms are hypothesized to accelerate pattern recognition and optimization, potentially enabling faster exploration of interactions among tens of thousands of features.127,128 If realized, these capabilities could speed simulation of TME interaction networks under different perturbations and help prioritize candidate resistance drivers for experimental follow-up.129
Parallel advances in pathomics and radiomics are moving the field toward more integrated and interpretable multimodal models. Pathomics is progressing through ensemble deep learning and transfer learning approaches that correlate whole-slide histology with genomic and transcriptomic programs, including prediction of microsatellite instability, with improving robustness across scanners and staining protocols.51,130 Radiomics is evolving through fused models that combine CT representations with multi-omic biomarkers; in NSCLC, architectures such as DenseNet-based encoders have been paired with interpretability methods (eg, Grad-CAM) to highlight radiographic regions driving predictions and to connect imaging features to underlying gene-expression patterns or immune-cell densities.131,132 Such alignment between model outputs and biological signals is likely to increase clinical acceptance.
Beyond efficacy prediction, AI–multi-omics is extending to survivorship and adverse-event management. In cardio-oncology, integrating genomic predisposition, blood biomarker trajectories, and clinical risk factors has revealed multi-omic patterns associated with increased risk of ICI-associated myocarditis and other cardiotoxicities.133,134 Predicting toxicity risk could enable proactive monitoring, earlier intervention, and risk-adapted treatment strategies, expanding the translational value of AI from selecting therapy to managing long-term safety.135
Personalized Medicine and Biomarker Validation
A central near-term objective is truly personalized immunotherapy paired with rigorous biomarker validation. As mechanistic understanding deepens, personalization is expected to extend beyond choosing therapy to optimizing dose, schedule, sequencing, and adaptive modification over time based on evolving tumor biology and immune state.
Liquid biopsy is likely to be pivotal for personalization because it can capture tumor evolution through serial, minimally invasive sampling. Circulating tumor DNA, circulating tumor cells, and epigenetic signals such as methylation can indicate molecular response, minimal residual disease, and emerging resistance, sometimes earlier than conventional imaging.25,26 In bladder cancer, AI-enhanced liquid biopsy strategies are being evaluated to detect recurrence or resistance patterns and to reduce reliance on repeated cystoscopies or tissue biopsies.44 More broadly, integrating longitudinal liquid-biopsy signals with multi-omics and clinical features could support earlier therapy switching, escalation, or de-escalation, provided prospective trials confirm clinical benefit.25
Prospective validation remains decisive. Retrospective discrimination—however impressive—does not establish that model-guided decisions improve outcomes. In melanoma, multi-omics predictors integrating mutational profiles and immune signatures have outperformed tumor mutational burden in retrospective analyses, yet larger prospective studies are required to test whether biomarker-guided treatment selection improves survival, reduces toxicity, and is cost-effective.77,87 Accordingly, trial designs are evolving: umbrella and platform trials increasingly incorporate biomarker-defined arms in which AI-derived signatures determine stratification, and neoadjuvant studies provide early, quantifiable endpoints such as major pathological response and pathologic complete response.9,10
Biomarker pipelines are also being refined into integrated discovery–validation loops. AI can screen multi-omics for outlier signals and pathway connectivity, prioritize candidates with plausible actionability, and accelerate experimental confirmation.9 In nasopharyngeal carcinoma, AI-driven screening has highlighted targets such as CACNA2D1 by connecting multi-omic anomalies to known pathways before laboratory validation.50 In ovarian cancer, multi-omics analyses have identified stemness-related expression programs and genetic alterations associated with ICI response; machine-learning models have then been strengthened by experimental validation in cell lines and organoids.57,58 Increasing integration of epigenomic assays (eg, chromatin accessibility or enhancer mapping) is expected to expand discovery of regulatory elements that drive resistance and to support development of epigenetic or transcriptional combination strategies.15
Neoadjuvant personalization is advancing in parallel. In NSCLC, multi-omics AI systems are being evaluated to predict pathological response to neoadjuvant immunotherapy and to interpret resistance through features such as radiomic signatures and DNA repair mutations, informing escalation, de-escalation, alternative sequencing, or earlier surgery.24,70 In hepatocellular carcinoma, where one or two driver alterations may dominate, AI tools are being developed to standardize how single-gene status—such as TP53 mutation status—should be combined with broader omics context to guide decisions between immunotherapy and targeted agents, moving from prognostic associations toward actionable guidance.80,81
Personalization will also increasingly involve longitudinal physiologic data. Wearables and digital health platforms provide continuous measures (heart rate, activity, symptom reporting) that can be synchronized with laboratory trends and omics readouts.9,10 In principle, AI systems could detect subtle early patterns suggestive of cytokine release syndrome or autoimmune toxicity and trigger earlier evaluation, dosing adjustments, or supportive interventions, thereby enabling dynamic management rather than static dosing.9,73
The immunotherapy landscape is also broadening to engineered modalities such as CAR-T cells and bispecific T-cell engagers. AI is being applied to predict which construct designs or target combinations may maximize tumor control while limiting toxicity by integrating tumor multi-omics with patient T-cell state and host factors.9,72 Similar integration of host polymorphisms, baseline cytokines, and clinical features is being used to forecast severe adverse events, including neurotoxicity and cytokine storms, supporting risk-adapted monitoring and design of safer therapeutic strategies.73,81
Bibliometric analyses suggest continued momentum in AI-enabled biomarker discovery while emphasizing the need for prospective, well-designed studies and regulatory-grade validation.9,74 In the near term, AI–multi-omics may guide trial enrollment by enriching predicted responder or resistant populations to test mechanistic hypotheses efficiently.10 Over time, such models could function as companion diagnostics paired with newly approved immunotherapies, potentially as co-developed drug–test strategies, contingent on reproducibility, clinical utility, and regulatory evaluation.
Interdisciplinary Integration
The next phase of progress will be driven by deeper interdisciplinary integration across immunology, oncology, pathology, bioinformatics, data science, engineering, and related domains. A prominent axis is the microbiome–metabolism–immune interface. Gut microbes shape systemic metabolites (including short-chain fatty acids and tryptophan-derived products) that modulate immune-cell function and influence ICI response.17 In NSCLC, integrating fecal metagenomics with serum metabolomics and tumor transcriptomics, then analyzing the combined dataset with machine learning, has clarified how microbial taxa may modulate systemic immune pathways relevant to ICI efficacy.24,36 Such models could ultimately inform individualized microbial or metabolic interventions, ranging from donor selection in fecal microbiota transplantation to targeted probiotic or dietary strategies, if safety and efficacy are prospectively established.
Metabolism and epigenetics are converging in clinically relevant ways. Lactylation exemplifies a metabolic–epigenetic mark linked to immune evasion and resistance.16 AI can support patient selection for combinations in which metabolic agents (such as lactate dehydrogenase inhibitors or lactate-transport inhibitors) are paired with ICIs by integrating metabolic gene-expression programs, lactate-associated measures from serum or imaging surrogates, and immune signatures.23,43 This integration can generate rational hypotheses for overcoming resistance and help define subgroups most likely to benefit from metabolic add-ons.
Spatial biology further illustrates the value of cross-field collaboration. In diffuse large B-cell lymphoma, combining spatial proteomics platforms (eg, GeoMX or CODEX) with genomics and machine learning has revealed immune-escape architectures—such as tumor cells surrounded by macrophages and fibroblasts—that pure genomics would miss.9,12 Similar cross-modal integration has enabled compound biomarkers that combine genetic context with spatial immune organization; in renal cell carcinoma, “spatial HLA signatures” that integrate HLA genotype with spatial T-cell distribution exemplify how genetic and spatial information can jointly improve response prediction.10,37
Interdisciplinary interpretation is crucial for converting machine-learned subtypes into treatment strategies. In head and neck squamous cell carcinoma, integrating metabolic measures (hypoxia and glycolysis), stemness indices, and immune profiles has defined subtypes with therapeutic implications, requiring joint interpretation from oncologists, metabolic specialists, and data scientists.9,85 In melanoma, single-cell immune states gain clinical value when integrated with pathology and clinical covariates to guide whether to prioritize ICIs or alternative immune modalities.90 In lung adenocarcinoma, stemness-based stratification of “cold” tumors has motivated combination strategies that target cancer stemness pathways or epigenetic modulators alongside immunotherapy, illustrating how computational subtyping can yield mechanistically grounded treatment hypotheses when interpreted collaboratively.48,58
Looking ahead, proposed directions include broader global consortia enabled by federated learning to ensure equitable performance across ancestries and care settings, and deeper mechanistic simulations that couple AI with emerging computing paradigms, including speculative links to quantum biology. Synthesis frameworks commonly emphasize needs in data handling, validation, interpretability, therapeutic expansion, and interdisciplinary cooperation. Ultimately, the field’s trajectory will be defined by whether increasingly sophisticated AI–multi-omics models can be operationalized into timely, interpretable, and prospectively validated tools that measurably improve outcomes in precision immunotherapy (Table 3).
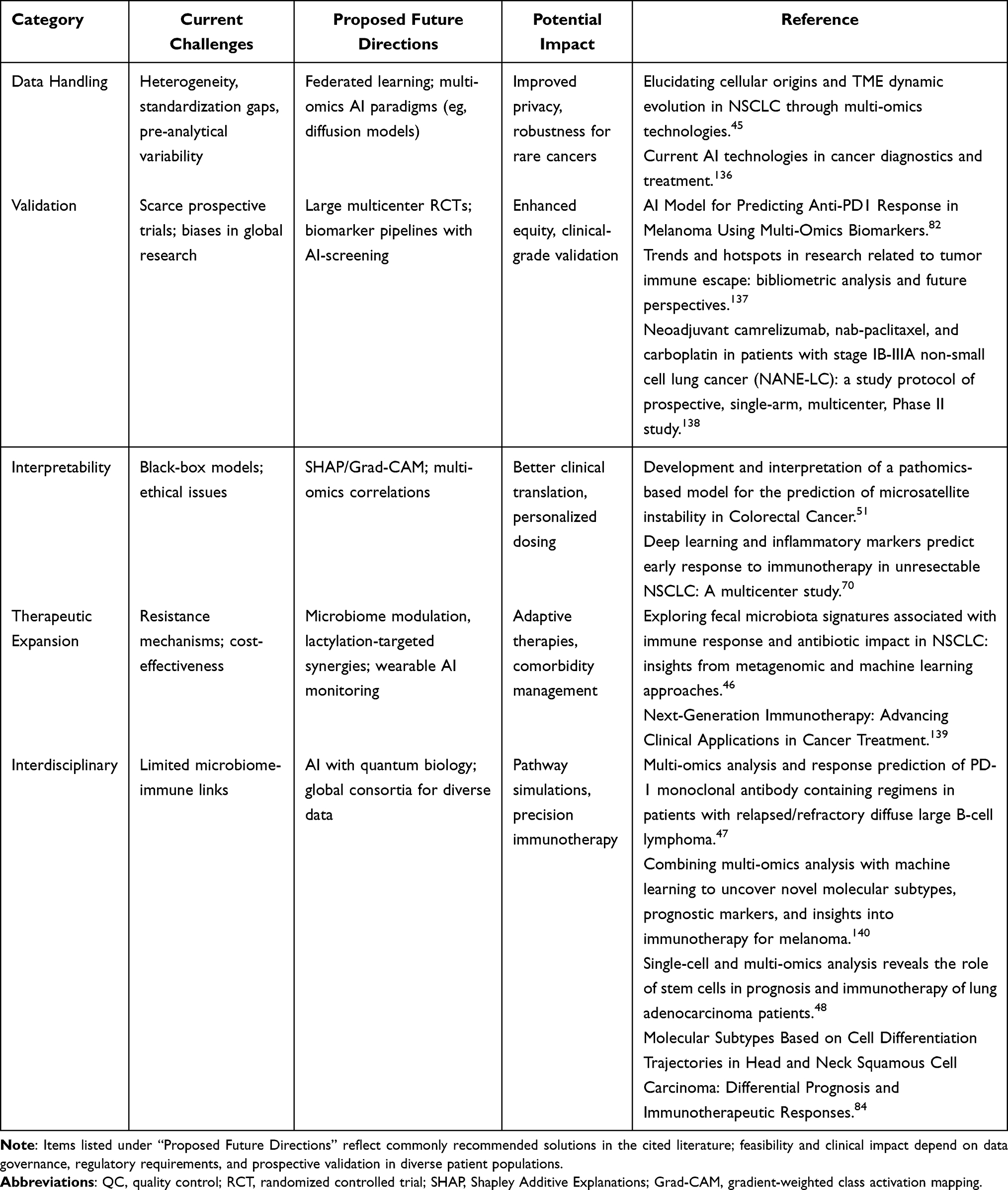 |
Table 3 Challenges and Future Directions in AI-Multi-Omics Integration |
Data Sharing Statement
This manuscript is a narrative review based on publicly available literature and data sources. No original datasets were generated or analyzed in this study. All data supporting the conclusions (such as performance metrics, model details, and outcome statistics) are derived from the cited studies and are accessible through those publications or public databases. Additional details or materials related to the review are available from the corresponding author upon reasonable request.
Author Information
Qianqian Wang, MD, is an Associate Chief Physician and Teaching Director of the Oncology Department at Zhuzhou Central Hospital (Hunan, China). With 16 years of clinical experience in medical and radiation oncology, she specializes in gynecological malignancies and neuroendocrine tumors. Dr. Wang initiated the hospital’s Neuroendocrine Tumor MDT program and leads oncology training programs. Her research focuses on breast cancer mechanisms and AI-driven oncology models, including participation in a Hunan Provincial Key R&D Project. She has authored publications in journals such as Cancer Management and Research and holds multiple committee positions in provincial oncology societies.
Author Contributions
All authors contributed significantly to this work and meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. Xiaodong Wang: Conceptualization, Methodology, Writing – original draft (Introduction and Biological Foundations sections), Writing – review & editing. Jing He: Methodology, Investigation (literature search and data curation for multi-omics insights), Writing – original draft (AI Integration section), Writing – review & editing. Gouping Ding: Investigation (literature search for AI algorithms and predictive models), Writing – original draft (Clinical Applications and Challenges sections), Writing – review & editing. Yixuan Tang: Visualization (figure and table preparation), Writing – original draft (Abstract and Keywords), Writing – review & editing. Qianqian Wang: Conceptualization, Supervision, Project administration, Writing – original draft (integrating all sections and Future Directions), Writing – review & editing. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. Sharma P, Hu-Lieskovan S, Wargo JA, et al. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell. 2017;168(4):707–20. doi:10.1016/j.cell.2017.01.017
2. Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. New Engl J Med. 2012;366(26):2443–2454. doi:10.1056/NEJMoa1200690
3. Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2019;381(16):1535–1546. doi:10.1056/NEJMoa1910836
4. O’Neill RE, Cao X. Co-stimulatory and co-inhibitory pathways in cancer immunotherapy. Adv Cancer Res. 2019;143:145–194. doi:10.1016/bs.acr.2019.03.003
5. Binnewies M, Roberts EW, Kersten K, et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat Med. 2018;24(5):541–550. doi:10.1038/s41591-018-0014-x
6. Chen DS, Mellman I. Elements of cancer immunity and the cancer-immune set point. Nature. 2017;541(7637):321–330. doi:10.1038/nature21349
7. Samstein RM, Lee C-H, Shoushtari AN, et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nature Genet. 2019;51(2):202–206. doi:10.1038/s41588-018-0312-8
8. Havel JJ, Chowell D, Chan TA. The evolving landscape of biomarkers for checkpoint inhibitor immunotherapy. Nat Rev Cancer. 2019;19(3):133–150. doi:10.1038/s41568-019-0116-x
9. Prelaj A, Miskovic V, Zanitti M, et al. Artificial intelligence for predictive biomarker discovery in immuno-oncology: a systematic review. Ann Oncol. 2024;35(1):29–65. doi:10.1016/j.annonc.2023.10.125
10. Wang SL, Chan TA. Navigating established and emerging biomarkers for immune checkpoint inhibitor therapy. Cancer Cell. 2025;43(4):641–664. doi:10.1016/j.ccell.2025.03.006
11. Schmitz R, Wright GW, Huang DW, et al. Genetics and pathogenesis of diffuse large B-cell lymphoma. New Engl J Med. 2018;378(15):1396–1407. doi:10.1056/NEJMoa1801445
12. Li J, Chin CR, Ying H-Y, et al. Loss of CREBBP and KMT2D cooperate to accelerate lymphomagenesis and shape the lymphoma immune microenvironment. Nat Commun. 2024;15(1):2879. doi:10.1038/s41467-024-47012-1
13. Torres-Mejia E, Weng S, Whittaker CA, et al. Lung cancer–intrinsic SOX2 expression mediates resistance to checkpoint blockade therapy by inducing treg‐dependent CD8+ T-cell exclusion. Cancer Immunol Res. 2025;13(4):496–516. doi:10.1158/2326-6066.CIR-24-0184
14. Spranger S, Bao R, Gajewski TF. Melanoma-intrinsic β-catenin signalling prevents anti-tumour immunity. Nature. 2015;523(7559):231–235. doi:10.1038/nature14404
15. Mizokami H, Okabe A, Choudhary R, et al. Enhancer infestation drives tumorigenic activation of inactive B compartment in Epstein-Barr virus-positive nasopharyngeal carcinoma. eBioMedicine. 2024;102:105057. doi:10.1016/j.ebiom.2024.105057
16. Zhang D, Tang Z, Huang H, et al. Metabolic regulation of gene expression by histone lactylation. Nature. 2019;574(7779):575–580. doi:10.1038/s41586-019-1678-1
17. Gopalakrishnan V, Spencer CN, Nezi L, et al. Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients. Science. 2018;359(6371):97–103. doi:10.1126/science.aan4236
18. Routy B, Le Chatelier E, Derosa L, et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science. 2018;359(6371):91–97. doi:10.1126/science.aan3706
19. Jiang P, Gu S, Pan D, et al. Signatures of T cell dysfunction and exclusion predict cancer immunotherapy response. Nat Med. 2018;24(10):1550–1558. doi:10.1038/s41591-018-0136-1
20. Camps J, Jiménez-Franco A, García-Pablo R, et al. Artificial intelligence-driven integration of multi-omics and radiomics: a new hope for precision cancer diagnosis and prognosis. Biochim Biophys Acta Mol Basis Dis. 2025;1871(6):167841. doi:10.1016/j.bbadis.2025.167841
21. Kather JN, Pearson AT, Halama N, et al. Deep learning can predict microsatellite instability directly from histology in gastrointestinal cancer. Nat Med. 2019;25(7):1054–1056. doi:10.1038/s41591-019-0462-y
22. Peng F, Sinjab A, Dai Y, et al. Multimodal spatial-omics reveal co-evolution of alveolar progenitors and proinflammatory niches in progression of lung precursor lesions. Cancer Cell. 2025;44(2):321–339.e13. doi:10.1016/j.ccell.2025.10.004
23. Li Y, Wu X, Fang D, et al. Informing immunotherapy with multi-omics driven machine learning. NPJ Digit Med. 2024;7(1):67. doi:10.1038/s41746-024-01043-6
24. Mei T, Wang T, Zhou Q. Multi-omics and artificial intelligence predict clinical outcomes of immunotherapy in non-small cell lung cancer patients. Clin Exp Med. 2024;24(1):60. doi:10.1007/s10238-024-01324-0
25. Di Sario G, Rossella V, Famulari ES, et al. Enhancing clinical potential of liquid biopsy through a multi-omic approach: a systematic review. Front Genet. 2023;14:1152470. doi:10.3389/fgene.2023.1152470
26. Chen G, Zhang J, Fu Q, et al. Integrative analysis of multi-omics data for liquid biopsy. Br J Cancer. 2023;128(4):505–518. doi:10.1038/s41416-022-02048-2
27. Leach DR, Krummel MF, Allison JP. Enhancement of antitumor immunity by CTLA-4 blockade. Science. 1996;271(5256):1734–1736. doi:10.1126/science.271.5256.1734
28. Pauken KE, Sammons MA, Odorizzi PM, et al. Epigenetic stability of exhausted T cells limits durability of reinvigoration by PD-1 blockade. Science. 2016;354(6316):1160–1165. doi:10.1126/science.aaf2807
29. He F, Tay AHM, Calandigary A, et al. FPR2 shapes an immune-excluded pancreatic tumor microenvironment and drives t-cell exhaustion in a sex-dependent manner. Cancer Res. 2023;83(10):1628–1645. doi:10.1158/0008-5472.CAN-22-2932
30. Salcher S, Sturm G, Horvath L, et al. High-resolution single-cell atlas reveals diversity and plasticity of tissue-resident neutrophils in non-small cell lung cancer. Cancer Cell. 2022;40(12):1503–1520.e8. doi:10.1016/j.ccell.2022.10.008
31. Ford K, Hanley CJ, Mellone M, et al. NOX4 inhibition potentiates immunotherapy by overcoming cancer-associated fibroblast-mediated CD8 T-cell exclusion from tumors. Cancer Res. 2020;80(9):1846–1860. doi:10.1158/0008-5472.CAN-19-3158
32. O’Connor RA, Martinez BR, Koppensteiner L, et al. Cancer-associated fibroblasts drive CXCL13 production in activated T cells via TGF-beta. Front Immunol. 2023;14:1221532. doi:10.3389/fimmu.2023.1221532
33. Kim Y, Kim G, Kim S, et al. Fecal microbiota transplantation improves anti-PD-1 inhibitor efficacy in unresectable or metastatic solid cancers refractory to anti-PD-1 inhibitor. Cell Host Microbe. 2024;32(8):1380–1393.e9. doi:10.1016/j.chom.2024.06.010
34. Davar D, Dzutsev AK, McCulloch JA, et al. Fecal microbiota transplant overcomes resistance to anti-PD-1 therapy in melanoma patients. Science. 2021;371(6529):595–602. doi:10.1126/science.abf3363
35. Nyein AF, Bari S, Hogue S, et al. Effect of prior antibiotic or chemotherapy treatment on immunotherapy response in non-small cell lung cancer. BMC Cancer. 2022;22(1):101. doi:10.1186/s12885-022-09210-2
36. Hakozaki T, Richard C, Elkrief A, et al. The gut microbiome associates with immune checkpoint inhibition outcomes in patients with advanced non-small cell lung cancer. Cancer Immunol Res. 2020;8(10):1243–1250. doi:10.1158/2326-6066.CIR-20-0196
37. Kinget L, Naulaerts S, Govaerts J, et al. A spatial architecture-embedding HLA signature to predict clinical response to immunotherapy in renal cell carcinoma. Nat Med. 2024;30(6):1667–1679. doi:10.1038/s41591-024-02978-9
38. Alaluf E, Vokaer B, Detavernier A, et al. Heme oxygenase-1 orchestrates the immunosuppressive program of tumor-associated macrophages. JCI Insight. 2020;5(11). doi:10.1172/jci.insight.133929
39. Müller M, Huber F, Arnaud M, et al. Machine learning methods and harmonized datasets improve immunogenic neoantigen prediction. Immunity. 2023;56(11):2650–2663.e6. doi:10.1016/j.immuni.2023.09.002
40. Gusakova M, Sharko F, Mamchur A, et al. Mutations in CREBBP and EP300 HAT and bromo domains drive hypermutation and predict survival in GI cancers treated with immunotherapy. Biomedicines. 2025;13(11):2592. doi:10.3390/biomedicines13112592
41. Principe DR. Patients deriving long-term benefit from immune checkpoint inhibitors demonstrate conserved patterns of site-specific mutations. Sci Rep. 2022;12(1):11490. doi:10.1038/s41598-022-15714-5
42. Li W, Zhou C, Yu L, et al. Tumor-derived lactate promotes resistance to bevacizumab treatment by facilitating autophagy enhancer protein RUBCNL expression through histone H3 lysine 18 lactylation (H3K18la) in colorectal cancer. Autophagy. 2024;20(1):114–130. doi:10.1080/15548627.2023.2249762
43. Chen J, Zhao D, Wang Y, et al. Lactylated apolipoprotein C-II induces immunotherapy resistance by promoting extracellular lipolysis. Adv Sci. 2024;11(38):e2406333. doi:10.1002/advs.202406333
44. Silva-Ferreira M, Carvalho JA, Salta S, et al. Diagnostic test accuracy of urinary DNA methylation-based biomarkers for the detection of primary and recurrent bladder cancer: a systematic review and meta-analysis. Eur Urol Focus. 2024;10(6):922–934. doi:10.1016/j.euf.2024.05.024
45. Chao NN, Zhang L. Elucidating cellular origins and TME dynamic evolution in NSCLC through multi-omics technologies. Biochim Biophys Acta Rev Cancer. 2025;1880(5):189425. doi:10.1016/j.bbcan.2025.189425
46. Han W, Zhou Y, Wang Y, et al. Exploring fecal microbiota signatures associated with immune response and antibiotic impact in NSCLC: insights from metagenomic and machine learning approaches. Front Cell Infect Microbiol. 2025;15:1591076. doi:10.3389/fcimb.2025.1591076
47. Chen X, Qin Y, Xue X, et al. Multi-omics analysis and response prediction of PD-1 monoclonal antibody containing regimens in patients with relapsed/refractory diffuse large B-cell lymphoma. Cancer Immunol Immunother. 2024;73(12):250. doi:10.1007/s00262-024-03840-0
48. Zheng J, Lin H, Ye W, et al. Single-cell and multi-omics analysis reveals the role of stem cells in prognosis and immunotherapy of lung adenocarcinoma patients. Front Immunol. 2025;16:1634830. doi:10.3389/fimmu.2025.1634830
49. Li J, Xu N, Hu L, et al. Chaperonin containing TCP1 subunit 5 as a novel pan-cancer prognostic biomarker for tumor stemness and immunotherapy response: insights from multi-omics data, integrated machine learning, and experimental validation. Cancer Immunol Immunother. 2025;74(7):224. doi:10.1007/s00262-025-04071-7
50. Chung DL, Leung GHD, Liu S, et al. AI-driven drug target screening platform identified oncogene CACNA2D1 activated by enhancer infestation in epstein-barr virus-associated nasopharyngeal carcinoma. Int J Mol Sci. 2025;26(10):4697. doi:10.3390/ijms26104697
51. Cao R, Yang F, Ma S-C, et al. Development and interpretation of a pathomics-based model for the prediction of microsatellite instability in colorectal cancer. Theranostics. 2020;10(24):11080–11091. doi:10.7150/thno.49864
52. Zhao J, Dong Y, Bai H, et al. Multi-omics indicators of long-term survival benefits after immune checkpoint inhibitor therapy. Cell Rep Methods. 2023;3(10):100596. doi:10.1016/j.crmeth.2023.100596
53. Liu G, Pan L-Z, Chen J, et al. Unveiling the role of PANoptosis-related genes in breast cancer: an integrated study by multi-omics analysis and machine learning algorithms. Breast Cancer Res Treat. 2025;211(1):35–50. doi:10.1007/s10549-025-07620-x
54. Wu X, Yan H, Qiu M, et al. Comprehensive characterization of tumor microenvironment in colorectal cancer via molecular analysis. Elife. 2023;12. doi:10.7554/eLife.86032
55. Fustero-Torre C, Jiménez-Santos MJ, García-Martín S, et al. Beyondcell: targeting cancer therapeutic heterogeneity in single-cell RNA-seq data. Genome Med. 2021;13(1):187. doi:10.1186/s13073-021-01001-x
56. Kim JH, Seo M-K, Lee JA, et al. Genomic and transcriptomic characterization of heterogeneous immune subgroups of microsatellite instability-high colorectal cancers. J Immunother Cancer. 2021;9(12):e003414. doi:10.1136/jitc-2021-003414
57. Malta TM, Sokolov A, Gentles AJ, et al. Machine learning identifies stemness features associated with oncogenic dedifferentiation. Cell. 2018;173(2):338–354.e15. doi:10.1016/j.cell.2018.03.034
58. Zhang Z, Wang Z-X, Chen Y-X, et al. Integrated analysis of single-cell and bulk RNA sequencing data reveals a pan-cancer stemness signature predicting immunotherapy response. Genome Med. 2022;14(1):45. doi:10.1186/s13073-022-01050-w
59. Li Y, Liu C, Zhang X, et al. CCT5 induces epithelial-mesenchymal transition to promote gastric cancer lymph node metastasis by activating the Wnt/β-catenin signalling pathway. Br J Cancer. 2022;126(12):1684–1694. doi:10.1038/s41416-022-01747-0
60. Shi H, Yang Y. Identification of inhibitory immune checkpoints and relevant regulatory pathways in breast cancer stem cells. Cancer Med. 2021;10(11):3794–3807. doi:10.1002/cam4.3902
61. Giroux Leprieur E, Hélias-Rodzewicz Z, Takam Kamga P, et al. Sequential ctDNA whole-exome sequencing in advanced lung adenocarcinoma with initial durable tumor response on immune checkpoint inhibitor and late progression. J Immunother Cancer. 2020;8(1):e000527. doi:10.1136/jitc-2020-000527
62. Yang CF, Yang G-D, Huang T-J, et al. EB-virus latent membrane protein 1 potentiates the stemness of nasopharyngeal carcinoma via preferential activation of PI3K/AKT pathway by a positive feedback loop. Oncogene. 2016;35(26):3419–3431. doi:10.1038/onc.2015.402
63. He P, Ma Y, Wu Y, et al. Exploring PANoptosis in breast cancer based on scRNA-seq and bulk-seq. Front Endocrinol. 2023;14:1164930. doi:10.3389/fendo.2023.1164930
64. O’Malley G, Heijltjes M, Houston AM, et al. Mesenchymal stromal cells (MSCs) and colorectal cancer: a troublesome twosome for the anti-tumour immune response? Oncotarget. 2016;7(37):60752–60774. doi:10.18632/oncotarget.11354
65. Deschoolmeester V, Baay M, Lardon F, et al. Immune cells in colorectal cancer: prognostic relevance and role of MSI. Cancer Microenviron. 2011;4(3):377–392. doi:10.1007/s12307-011-0068-5
66. Wang L, Sfakianos JP, Beaumont KG, et al. Myeloid cell-associated resistance to PD-1/PD-L1 blockade in urothelial cancer revealed through bulk and single-cell RNA sequencing. Clin Cancer Res. 2021;27(15):4287–4300. doi:10.1158/1078-0432.CCR-20-4574
67. Drake CG. Myeloid resistance is not futile: biomarkers of immunotherapy in bladder cancer. Clin Cancer Res. 2021;27(15):4139–4141. doi:10.1158/1078-0432.CCR-21-1011
68. Sehgal K, Portell A, Ivanova EV, et al. Dynamic single-cell RNA sequencing identifies immunotherapy persister cells following PD-1 blockade. J Clin Invest. 2021;131(2). doi:10.1172/JCI135038
69. Yamashita R, Long J, Longacre T, et al. Deep learning model for the prediction of microsatellite instability in colorectal cancer: a diagnostic study. Lancet Oncol. 2021;22(1):132–141. doi:10.1016/S1470-2045(20)30535-0
70. Yuan L, Wang Q, Sun F, et al. Deep learning and inflammatory markers predict early response to immunotherapy in unresectable NSCLC: a multicenter study. Biomol Biomed. 2025;25(10):2252–2268. doi:10.17305/bb.2025.12324
71. Jiang J, Fan Z, Jiang S, et al. Interpretable multimodal deep learning model for predicting post-surgical international society of urological pathology grade in primary prostate cancer. Eur J Nucl Med Mol Imaging. 2025;52(10):3730–3743. doi:10.1007/s00259-025-07248-5
72. Nicolai CJ, Parker MH, Qin J, et al. In vivo CAR T-cell generation in nonhuman primates using lentiviral vectors displaying a multidomain fusion ligand. Blood. 2024;144(9):977–987. doi:10.1182/blood.2024024523
73. Li S, Tajiri K, Ishizuka Y, et al. Cytokine profiling of patients with immune checkpoint inhibitor-associated myocarditis: a pilot study. Mol Biol Rep. 2025;52(1):983. doi:10.1007/s11033-025-11095-w
74. Dong H, Wang X, Zheng Y, et al. Mapping the rapid growth of multi-omics in tumor immunotherapy: bibliometric evidence of technology convergence and paradigm shifts. Hum Vaccin Immunother. 2025;21(1):2493539. doi:10.1080/21645515.2025.2493539
75. Rakaee M, Adib E, Ricciuti B, et al. Association of machine learning-based assessment of tumor-infiltrating lymphocytes on standard histologic images with outcomes of immunotherapy in patients with NSCLC. JAMA Oncol. 2023;9(1):51–60. doi:10.1001/jamaoncol.2022.4933
76. Liu F, Huang R, Wang Q, et al. Leveraging readily available clinical data with machine learning to predict first-line immunotherapy outcomes in non-small cell lung cancer. Int Immunopharmacol. 2025;163:115259. doi:10.1016/j.intimp.2025.115259
77. Liu D, Schilling B, Liu D, et al. Integrative molecular and clinical modeling of clinical outcomes to PD1 blockade in patients with metastatic melanoma. Nat Med. 2019;25(12):1916–1927. doi:10.1038/s41591-019-0654-5
78. Ma J, Yan Z, Zhang J, et al. A genetic predictive model for precision treatment of diffuse large B-cell lymphoma with early progression. Biomark Res. 2020;8(1):33. doi:10.1186/s40364-020-00214-3
79. Jiao X, Wei X, Li S, et al. A genomic mutation signature predicts the clinical outcomes of immunotherapy and characterizes immunophenotypes in gastrointestinal cancer. Npj Precision Oncology. 2021;5(1):36. doi:10.1038/s41698-021-00172-5
80. Lin Z, Wang W, Yan Y, et al. A deep learning-based clinical-radiomics model predicting the treatment response of immune checkpoint inhibitors (ICIs)-based conversion therapy in potentially convertible hepatocelluar carcinoma patients: a tumor marker prognostic study. Int J Surg. 2025;111(5):3342–3355. doi:10.1097/JS9.0000000000002322
81. Sangro B, Melero I, Wadhawan S, et al. Association of inflammatory biomarkers with clinical outcomes in nivolumab-treated patients with advanced hepatocellular carcinoma. J Hepatol. 2020;73(6):1460–1469. doi:10.1016/j.jhep.2020.07.026
82. Gschwind A, Ossowski S. AI model for predicting anti-PD1 response in melanoma using multi-omics biomarkers. Cancers. 2025;17(5):714. doi:10.3390/cancers17050714
83. Zhang Y, Wang Y, Qian H. Multi-omics characterization and machine learning of lung adenocarcinoma molecular subtypes to guide precise chemotherapy and immunotherapy. Front Immunol. 2024;15:1497300. doi:10.3389/fimmu.2024.1497300
84. Huang ZD, Liu -Z-Z, Liu -Y-Y, et al. Molecular subtypes based on cell differentiation trajectories in head and neck squamous cell carcinoma: differential prognosis and immunotherapeutic responses. Front Immunol. 2021;12:791621. doi:10.3389/fimmu.2021.791621
85. Yin J, Xu L, Wang S, et al. Integrating immune multi-omics and machine learning to improve prognosis, immune landscape, and sensitivity to first- and second-line treatments for head and neck squamous cell carcinoma. Sci Rep. 2024;14(1):31454. doi:10.1038/s41598-024-83184-y
86. Zhang P, Qin M, Li F, et al. Integrated multiomics analysis and machine learning refine molecular subtypes and prognosis for thyroid cancer. Discov Oncol. 2025;16(1):1186. doi:10.1007/s12672-025-02918-0
87. Mariathasan S, Turley SJ, Nickles D, et al. TGFβ attenuates tumour response to PD-L1 blockade by contributing to exclusion of T cells. Nature. 2018;554(7693):544–548. doi:10.1038/nature25501
88. Cancer Genome Atlas Network. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature. 2015;517(7536):576–582. doi:10.1038/nature14129
89. Seiwert TY, Burtness B, Mehra R, et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): an open-label, multicentre, phase 1b trial. Lancet Oncol. 2016;17(7):956–965. doi:10.1016/S1470-2045(16)30066-3
90. Hugo W, Zaretsky JM, Sun L, et al. Genomic and transcriptomic features of response to anti-PD-1 therapy in metastatic melanoma. Cell. 2016;165(1):35–44. doi:10.1016/j.cell.2016.02.065
91. van Wilpe S, Croci D, Fonseca Costa SS, et al. Multimodal integration of blood RNA and ctDNA reflects response to immunotherapy in metastatic urothelial cancer. JCI Insight. 2025;10(5). doi:10.1172/jci.insight.186062
92. Ribas A, Puzanov I, Dummer R, et al. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): a randomised, controlled, Phase 2 trial. Lancet Oncol. 2015;16(8):908–918. doi:10.1016/S1470-2045(15)00083-2
93. Rahmy S, Mishra SJ, Murphy S, et al. Hsp90β inhibition upregulates interferon response and enhances immune checkpoint blockade therapy in murine tumors. Front Immunol. 2022;13:1005045. doi:10.3389/fimmu.2022.1005045
94. Baruch EN, Youngster I, Ben-Betzalel G, et al. Fecal microbiota transplant promotes response in immunotherapy-refractory melanoma patients. Science. 2021;371(6529):602–609. doi:10.1126/science.abb5920
95. Izzo LT, Wellen KE. Histone lactylation links metabolism and gene regulation. Nature. 2019;574(7779):492–493. doi:10.1038/d41586-019-03122-1
96. Sangro B, Gomez-Martin C, de la Mata M, et al. A clinical trial of CTLA-4 blockade with tremelimumab in patients with hepatocellular carcinoma and chronic hepatitis C. J Hepatol. 2013;59(1):81–88. doi:10.1016/j.jhep.2013.02.022
97. He B, Dong D, She Y, et al. Predicting response to immunotherapy in advanced non-small-cell lung cancer using tumor mutational burden radiomic biomarker. J Immunother Cancer. 2020;8(2):e000550. doi:10.1136/jitc-2020-000550
98. Carreras J, Hiraiwa S, Kikuti YY, et al. Artificial neural networks predicted the overall survival and molecular subtypes of diffuse large B-cell lymphoma using a pancancer immune-oncology panel. Cancers. 2021;13(24):6384. doi:10.3390/cancers13246384
99. Lee S, Lim B, Suh J, et al. Diagnostic accuracy of urinary PENK methylation test for urothelial and other cancers: a prospective study. Sci Rep. 2025;15(1):22149. doi:10.1038/s41598-025-07173-5
100. Levy JJ, Chan N, Marotti JD, et al. Examining longitudinal markers of bladder cancer recurrence through a semiautonomous machine learning system for quantifying specimen atypia from urine cytology. Cancer Cytopathology. 2023;131(9):561–573. doi:10.1002/cncy.22725
101. Argelaguet R, Velten B, Arnol D, et al. Multi-omics factor analysis-a framework for unsupervised integration of multi-omics data sets. Mol Syst Biol. 2018;14(6):e8124. doi:10.15252/msb.20178124
102. Batool SM, Hsia T, Beecroft A, et al. Extrinsic and intrinsic preanalytical variables affecting liquid biopsy in cancer. Cell Rep Med. 2023;4(10):101196. doi:10.1016/j.xcrm.2023.101196
103. Hoshida Y, Nijman SMB, Kobayashi M, et al. Integrative transcriptome analysis reveals common molecular subclasses of human hepatocellular carcinoma. Cancer Res. 2009;69(18):7385–7392. doi:10.1158/0008-5472.CAN-09-1089
104. Zhao Z, Cui T, Wei F, et al. Wnt/β-Catenin signaling pathway in hepatocellular carcinoma: pathogenic role and therapeutic target. Front Oncol. 2024;14:1367364. doi:10.3389/fonc.2024.1367364
105. Arango-Argoty G, Bikiel DE, Sun GJ, et al. AI-driven predictive biomarker discovery with contrastive learning to improve clinical trial outcomes. Cancer Cell. 2025;43(5):875–890.e8. doi:10.1016/j.ccell.2025.03.029
106. Auzine MM, Heenaye-Mamode Khan M, Baichoo S, et al. Development of an ensemble CNN model with explainable AI for the classification of gastrointestinal cancer. PLoS One. 2024;19(6):e0305628. doi:10.1371/journal.pone.0305628
107. Duwe G, Mercier D, Kauth V, et al. Development of an artificial intelligence-generated, explainable treatment recommendation system for urothelial carcinoma and renal cell carcinoma to support multidisciplinary cancer conferences. Eur J Cancer. 2025;220:115367. doi:10.1016/j.ejca.2025.115367
108. Tasci E, Zhuge Y, Camphausen K, Krauze AV. Bias and class imbalance in oncologic data-towards inclusive and transferrable ai in large scale oncology data sets. Cancers. 2022;14(12):2897. doi:10.3390/cancers14122897
109. Truhn D, Tayebi Arasteh S, Saldanha OL, et al. Encrypted federated learning for secure decentralized collaboration in cancer image analysis. Med Image Anal. 2024;92:103059. doi:10.1016/j.media.2023.103059
110. Warnat-Herresthal S, Schultze H, Shastry KL, et al. Swarm learning for decentralized and confidential clinical machine learning. Nature. 2021;594(7862):265–270. doi:10.1038/s41586-021-03583-3
111. Mehra T, Menges D, Gosztonyi B, et al. Comparative cost analysis of a diagnostic multi-omics platform for decision support in advanced cancer - results from the tumor profiler melanoma project. NPJ Precis Oncol. 2025;10(1). doi:10.1038/s41698-025-01229-5
112. Valeri N. Streamlining detection of fusion genes in colorectal cancer: having “faith” in precision oncology in the (Tissue) “agnostic. Era Cancer Res. 2019;79(6):1041–1043. doi:10.1158/0008-5472.CAN-19-0305
113. Derraz B, Breda G, Kaempf C, et al. New regulatory thinking is needed for AI-based personalised drug and cell therapies in precision oncology. NPJ Precis Oncol. 2024;8(1):23. doi:10.1038/s41698-024-00517-w
114. Wu Y, Wei B, Wei Z, et al. Single-cell and spatial transcriptomic profiling reveals distinct tumor microenvironment dynamics in cervical adenocarcinoma and squamous cell carcinoma. Commun Biol. 2025;9(1). doi:10.1038/s42003-025-09310-2
115. Laury AR, Zheng S, Aho N, et al. Opening the black box: spatial transcriptomics and the relevance of artificial intelligence–detected prognostic regions in high-grade serous carcinoma. Mod Pathol. 2024;37(7):100508. doi:10.1016/j.modpat.2024.100508
116. Ding Y, Wang D, Yan D, et al. Harnessing single-cell and multi-omics insights: STING pathway-based predictive signature for immunotherapy response in lung adenocarcinoma. Front Immunol. 2025;16:1575084. doi:10.3389/fimmu.2025.1575084
117. Park S, Ock C-Y, Kim H, et al. Artificial intelligence-powered spatial analysis of tumor-infiltrating lymphocytes as complementary biomarker for immune checkpoint inhibition in non-small-cell lung cancer. J Clin Oncol. 2022;40(17):1916–1928. doi:10.1200/JCO.21.02010
118. Noorbakhsh J, Foroughi Pour A, Chuang J. Emerging AI approaches for cancer spatial omics. GigaScience. 2025;14:giaf128.
119. Pati S, Baid U, Edwards B, et al. Federated learning enables big data for rare cancer boundary detection. Nat Commun. 2022;13(1):7346. doi:10.1038/s41467-022-33407-5
120. Sarma KV, Harmon S, Sanford T, et al. Federated learning improves site performance in multicenter deep learning without data sharing. J Am Med Inform Assoc. 2021;28(6):1259–1264. doi:10.1093/jamia/ocaa341
121. Casella B, Riviera W, Aldinucci M, et al. MERGE: a model for multi-input biomedical federated learning. Patterns. 2023;4(11):100856. doi:10.1016/j.patter.2023.100856
122. Li Y, Feng B, Chen Y, et al. FedCMC: a federated learning model with contribution fairness based on multi-center core data extraction for assessing the myometrial invasion status of endometrial cancer. Front Oncol. 2025;15:1648502.
123. Fatima I, Rehman A, Ding Y, et al. Breakthroughs in AI and multi-omics for cancer drug discovery: a review. Eur J Med Chem. 2024;280:116925. doi:10.1016/j.ejmech.2024.116925
124. Andreatta M, Garnica J, Carmona SJ. Identification of malignant cells in single-cell transcriptomics data. Commun Biol. 2025;8(1):1264. doi:10.1038/s42003-025-08695-4
125. Ai X, Smith MC, Feltus FA. GEMDiff: a diffusion workflow bridges between normal and tumor gene expression states: a breast cancer case study. Brief Bioinform. 2025;26(2). doi:10.1093/bib/bbaf093
126. Cui Y, Cui Y, Wang R, et al. DiffusionST: a deep generative diffusion model-based framework for enhancing spatial transcriptomics data quality and identifying spatial domains. Brief Bioinform. 2025;26(4):bbaf390.
127. Nassir N, Hashmi MA, Raji KG, et al. Quantum computing and the implementation of precision medicine. NPJ Genom Med. 2025;10(1):80. doi:10.1038/s41525-025-00537-w
128. Ghobadi MZ, Afsaneh E. Potential of quantum machine learning for solving the real-world problem of cancer classification. Discover Applied Sciences. 2024;6(10):513. doi:10.1007/s42452-024-06220-6
129. Weidner FM, Schwab JD, Wölk S, et al. Leveraging quantum computing for dynamic analyses of logical networks in systems biology. Patterns. 2023;4(3):100705. doi:10.1016/j.patter.2023.100705
130. You J, Zhang S, Zhang J, et al. Ensemble learning for predicting microsatellite instability in colorectal cancer using pretreatment colonoscopy images and clinical data. Front Oncol. 2026;15. doi:10.3389/fonc.2025.1734076
131. Zhang X, Zhang G, Qiu X, et al. Exploring non-invasive precision treatment in non-small cell lung cancer patients through deep learning radiomics across imaging features and molecular phenotypes. Biomark Res. 2024;12(1):12. doi:10.1186/s40364-024-00561-5
132. Sun Q, Yu L, Song Z, et al. Deep learning and radiomics fusion for predicting the invasiveness of lung adenocarcinoma within ground glass nodules. Sci Rep. 2025;15(1):29285. doi:10.1038/s41598-025-13447-9
133. Ayoub C, Appari L, Pereyra M, et al. Multimodal fusion artificial intelligence model to predict risk for MACE and myocarditis in cancer patients receiving immune checkpoint inhibitor therapy. JACC Adv. 2025;4(1):101435. doi:10.1016/j.jacadv.2024.101435
134. Khera R, Asnani AH, Krive J, et al. Artificial intelligence to enhance precision medicine in cardio-oncology: a scientific statement from the American Heart Association. Circ Genom Precis Med. 2025;18(2):e000097. doi:10.1161/HCG.0000000000000097
135. Wen Q, Qiu L, Qiu C, et al. Artificial intelligence in predicting efficacy and toxicity of immunotherapy: applications, challenges, and future directions. Cancer Lett. 2025;630:217881. doi:10.1016/j.canlet.2025.217881
136. Tiwari A, Mishra S, Kuo TR. Current AI technologies in cancer diagnostics and treatment. Mol Cancer. 2025;24(1):159. doi:10.1186/s12943-025-02369-9
137. Zhu H, Huang Y, Wang X, et al. Trends and hotspots in research related to tumor immune escape: bibliometric analysis and future perspectives. Front Immunol. 2025;16:1604216. doi:10.3389/fimmu.2025.1604216
138. Zhou H, Lin L, Qin T, et al. Neoadjuvant camrelizumab, nab-paclitaxel, and carboplatin in patients with stage IB-IIIA non-small cell lung cancer (NANE-LC): a study protocol of prospective, single-arm, multicenter, phase II study. J Thorac Dis. 2021;13(11):6468–6475. doi:10.21037/jtd-21-1022
139. Garg P, Pareek S, Kulkarni P, et al. Next-generation immunotherapy: advancing clinical applications in cancer treatment. J Clin Med. 2024;13(21):6537. doi:10.3390/jcm13216537
140. Zhao S, Li Z, Liu K, et al. Combining multi-omics analysis with machine learning to uncover novel molecular subtypes, prognostic markers, and insights into immunotherapy for melanoma. BMC Cancer. 2025;25(1):630. doi:10.1186/s12885-025-14012-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Application of Artificial Intelligence in the Analysis of Biomarkers for Diagnosis and Management of Uveitis and Uveal Melanoma: A Systematic Review
Bassi A, Krance SH, Pucchio A, Pur DR, Miranda RN, Felfeli T
Clinical Ophthalmology 2022, 16:2895-2908
Published Date: 30 August 2022
From COPD to Lung Cancer: Mechanisms Linking, Diagnosis, Treatment, and Prognosis

Qi C, Sun SW, Xiong XZ
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2603-2621
Published Date: 17 October 2022
Combined Photodynamic and Photothermal Therapy and Immunotherapy for Cancer Treatment: A Review
Kong C, Chen X
International Journal of Nanomedicine 2022, 17:6427-6446
Published Date: 16 December 2022
Ability of Blood Cell Parameters to Predict Clinical Outcomes of Nivolumab Monotherapy in Advanced Esophageal Squamous Cell Carcinoma
Hamai Y, Emi M, Ibuki Y, Kurokawa T, Yoshikawa T, Ohsawa M, Hirohata R, Kitasaki N, Okada M
OncoTargets and Therapy 2023, 16:263-273
Published Date: 10 April 2023
Cancer Immunotherapy and Medical Imaging Research Trends from 2003 to 2023: A Bibliometric Analysis

Tang S, Fan T, Wang X, Yu C, Zhang C, Zhou Y
Journal of Multidisciplinary Healthcare 2024, 17:2105-2120
Published Date: 6 May 2024