Back to Journals » Journal of Asthma and Allergy » Volume 16
Medication Adherence in People with Asthma: A Qualitative Systematic Review of Patient and Health Professional Perspectives
Authors Zhang X ![]() , Ding R, Zhang Z, Chen M, Yin Y, Quint JK
, Ding R, Zhang Z, Chen M, Yin Y, Quint JK ![]()
Received 7 February 2023
Accepted for publication 3 May 2023
Published 9 May 2023 Volume 2023:16 Pages 515—527
DOI https://doi.org/10.2147/JAA.S407552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Xiubin Zhang,1 Rong Ding,2 Zhaoxin Zhang,3 Mengyun Chen,4 Yueheng Yin,5 Jennifer K Quint1
1National Heart and Lung Institute, Imperial College London, London, W12 0BZ, UK; 2School of Health in Social Science, The University of Edinburgh, Edinburgh, Scotland, EH8 9AG, UK; 3Medical college, Xijing University, Xi’an, 710123, People’s Republic of China; 4School of Nursing, Lanzhou University, Lanzhou, 730000, People’s Republic of China; 5School of Nursing, Nanjing Medical University, Nanjing, 210000, People’s Republic of China
Correspondence: Jennifer K Quint, National Heart and Lung Institute, Imperial College London, White City Campus, London, W12 0BZ, UK, Email [email protected]
Background: Increased medication adherence leads to better asthma control and health outcomes. However, many studies have found that patient adherence to maintenance medication is poor.
Aim: We undertook a meta-synthesis of qualitative studies, to investigate asthma patient and healthcare professionals’ perspectives of medication adherence.
Methods: This systematic review was reported by following the PRISMA guidelines. The Joanna Briggs Institute (JBI) meta-aggregative approach was used for the qualitative synthesis. The protocol was registered in PROSPERO (CRD42022346831).
Results: In total, 12 articles were included in the review. These articles reported findings from 433 participants in total, which included 315 patients and 118 healthcare professionals. Four synthesised findings with sub-themes were identified from the reviewed studies. These synthesised findings were described as: 1) The role of relationship and communication with/between Healthcare Professionals in medication adherence; 2) Insufficient information from Healthcare Professionals acting as a barrier for adherence; 3) How patient’s attitude/beliefs effect their adherence to medication; and 4) Patients’ personal behaviour and other relevant barriers.
Conclusion: The synthesized findings provide a strong evidence-base of patient and health professionals’ perspectives and behaviours toward medication adherence, which helps to identify and address non-adherence. Healthcare providers can use these findings to support patients’ adherence to asthma medications. The findings suggest that empowering people to make informed decisions around medication adherence rather than “adherence controlling” by health professionals is very important. Effective dialogue and appropriate education are critical approaches to increase medication adherence.
Keywords: asthma patients, healthcare professional, medication adherence, perspectives, systematic review
Introduction
Asthma presents with coughing, breathlessness, wheezing, and tightness in the chest, is associated with airway inflammation and occasionally airflow obstruction.1 The use of bronchodilators or short-acting beta-agonists (SABA) for symptom relief, and inhaled corticosteroids (ICS) sometimes combined with long-acting beta-agonist (LABA) for management of persistent asthma are recommended by 2022 Global Initiative for Asthma (GINA) Report.2 The indicators of good asthma control are improved health outcomes, reduced exacerbations and reduced hospitalization.3 Prolonged excessive use of SABA and inadequate use of ICS are recognized as the main risk factors that exacerbate asthma, increase hospitalization and even risk of death.2–4 However, many studies have found that patient adherence to the use of maintenance medication is poor, the reasons behind barriers to adherence in controlling asthma vary widely.5–9
Some patients only adhere to medication during symptomatic episodes, but not when they are symptom free.10 Studies also show that adherence to treatment is associated with patients’ health perceptions, or misjudgement of their condition.11,12 One study found that underuse of asthma controller medications among ethnic minorities was due to culture and underlying beliefs.7 Furthermore, another study found that higher SABA use may be attributed to an over prescription by primary care practitioners.13 Prescribing behaviours have been associated with several factors including inadequate training on asthma management amongst medical staff, the increased cost of maintenance therapy, the generalised definition of the disease and the doctor-patient relationship.14,15 One study has indicated that effective communication between patients and healthcare practitioners has a significant role in engaging and motivating people with asthma to adhere to their medication.14
Increased medication adherence leads to better asthma control and health outcomes, decreases the risk of future asthma exacerbations and healthcare costs.16 Therefore, understanding patient perceptions and behaviours and the possible barriers to assess this adherence issue is very important. Moreover, there is also a need to understand the role healthcare professionals play in enabling these behaviours, their attitudes and approaches to prescribing treatments. Conducting a qualitative systematic review has the potential to provide a strong evidence-base of patient and health professionals’ perspectives and behaviours toward medication adherence.
Aims of the Study
The aim of this review was to undertake a meta-synthesis of qualitative studies on medication adherence among people with asthma and healthcare professionals. The review question was “what are asthma patients” experience of medication adherence’ and “what are the healthcare professionals” perspectives of asthma patients’ medication adherence’. The specific objectives were to:
Methods
This systematic review was reported by following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. The Joanna Briggs Institute (JBI) meta-aggregative approach was used for the qualitative synthesis.17 The protocol was registered in PROSPERO (CRD42022346831).
Search Strategy
We applied the population, phenomenon of interest and context (PICo) framework suggested by Stern et al to form keywords: population for “patient” or “healthcare professional”; phenomenon of interest for “asthma”, “medication adherence”, “perspective”; and context for “qualitative research, all healthcare settings”.18 All synonymous words used have been illustrated in a search term table (Appendix 1). Databases of CINAHL, Embase, PubMed, Scopus, and Web of Science were used to search for related studies. Only studies published in English were included, with no publishing date limitation. Grey literature, conference proceedings, these were excluded as they lacked peer review. PRISMA flow diagram was used to display the literature searching and screening process (Figure 1). The search process of each database is shown in Appendix 2.
 |
Figure 1 PRISMA chart: Searching and screening process. |
Inclusion Criteria
The inclusion criteria included: asthma patients who were 18 years and older, and healthcare professionals who cared for adults with asthma; qualitative studies exploring the experiences of adherence or nonadherence to asthma medication were included.
Study Selection and Search Outcome
Two reviewers screened the titles and abstracts independently. One reviewer checked the duplicate literature via EndNote 11. Two reviewers independently read and screened the full articles to identify studies that fit into the inclusion criteria. Any disagreements were solved through discussion within the review team to come to a consensus.
In total, 1325 articles were identified from the database searching. After removing 312 duplicate studies, 1013 articles were screened by title and abstract. 982 studies were excluded. A total of 31 full text articles were read and screened based on the inclusion criteria. A total of 12 full articles were included in the review.
Quality Assessment/Risk of Bias in Individual Studies
The JBI Critical Appraisal Checklist was used to assess the quality of the included studies.19 The JBI qualitative research appraisal tool includes nine questions with four rating choices (ie, yes, no, unclear, not applicable) for each question. Two reviewers critically reviewed each article independently, any disagreements were discussed and solved through the review team meeting. The detailed quality appraisal information is listed in Table 1.
 |
Table 1 Critical Appraisal of Included Studies |
Data Extraction and Management
All selected studies were extracted using the standardized data extraction tool for qualitative research from JBI reviewers’ manual.20 The extracted data included details about the phenomena of interest, populations, study methods and outcomes which were clearly related to the review question and study objectives. The findings of the selected studies were pooled using three levels credibility: unequivocal, credible and unsupported by two independent reviewers.20 These levels were used to ensure the extracted findings and interpretations were consistent with the authors’ intended meaning of the selected studies (Appendix 3).
Data Synthesis
Data synthesis was conducted by following the JBI meta-aggregative, three-stepped approach to categorize the findings across all the included studies. Two reviewers were involved in the aggregation/synthesis process. All the findings were categorized to form a set of findings. These categories were then developed to a single comprehensive set of synthesized findings (Appendix 4). Review group meetings were conducted regularly to solve issues and disagreements during data synthesis.
Results
Characteristics of the Included Studies
Of the 12 included studies, 3 were conducted in Canada, 3 in Sweden, 2 in Australia, 2 in the UK and 2 in the USA. These articles reported findings from 433 participants in total. Of those, 315 patients and healthcare professionals (118) included caregivers, physicians, pharmacists, respiratory therapists, general doctors and allied healthcare professionals. Only one study included a minority ethnic group.18 The characteristics of the included 12 studies are summarised in Table 2.
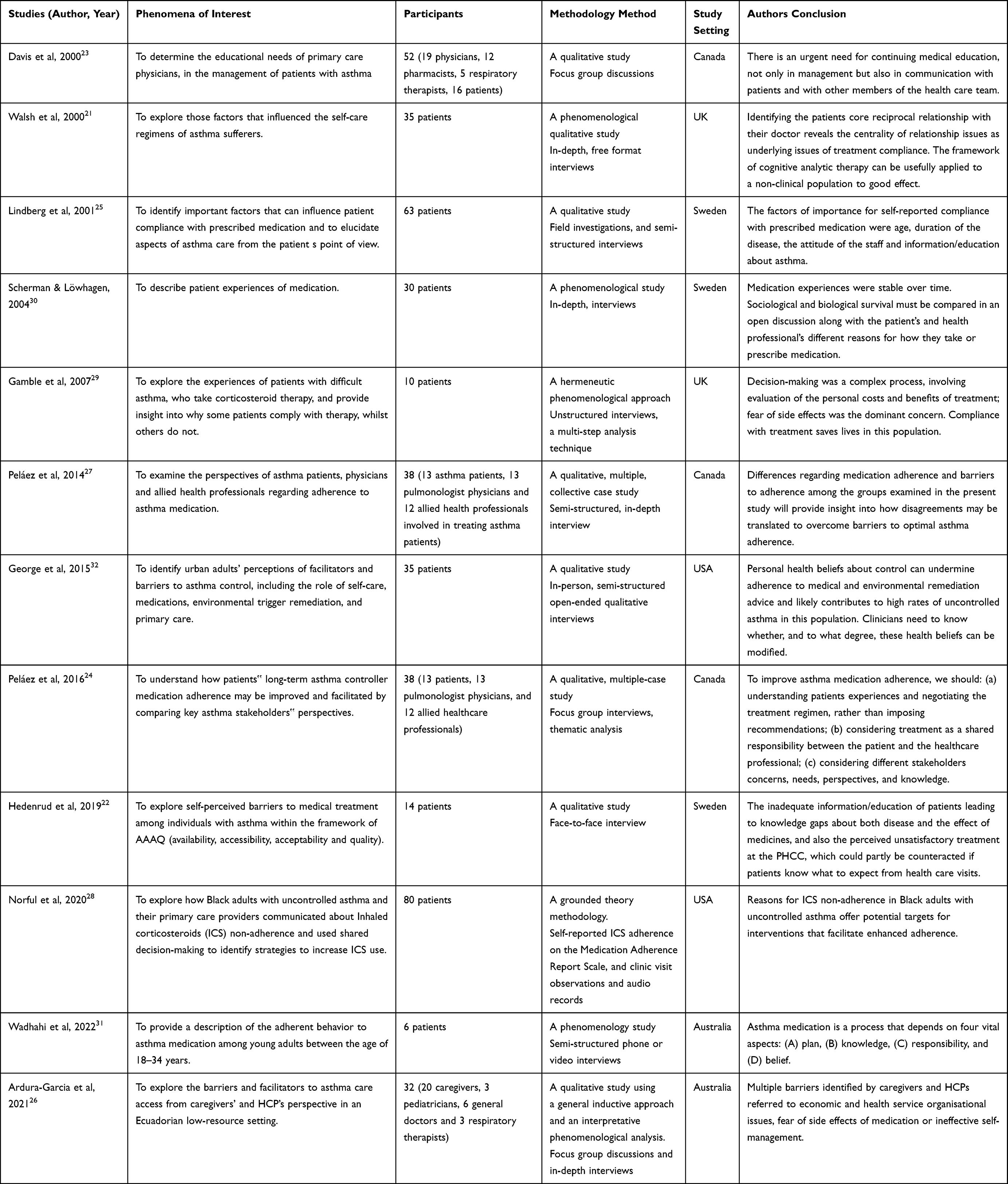 |
Table 2 Characteristic of Included Studies |
Synthesised Findings
In total, 59 findings were extracted from the 12 included studies (Appendix). 54 were identified as unequivocal, one was identified as credible and 4 were identified as unclear. Based on similarities that were found, 13 categories were stratified. These categories were further categorified and conceptualised into 4 synthesised findings based on the aims of this review (Appendix 4). These synthesised findings are described as: (1) The role of the relationship and communication with/ between healthcare professionals in medication adherence; (2) Insufficient information from healthcare professionals acting as barrier for adherence; (3) How patients’ attitude/beliefs affect their adherence to medication; (4) Patients’ personal behaviour and other relevant barriers.
The ConQual summary of findings is presented in Appendix 5. The synthesised findings and categories are presented in the following sections.
Synthesised Finding 1: The Role of Relationship and Communication with/Between Healthcare Professionals in Medication Adherence
Relationship with Healthcare Professionals
One important factor in medication adherence identified in this review was the relationship between patients and healthcare professionals. The synthesised findings show that a positive clinical experience and relationship increased patients’ trust in their treatment and improved medication adherence. One of the included studies reported that when a good rapport is built between patients and healthcare professionals, patients are more likely to listen and adhere to their physicians’ clinical advice and guidance.21 Just as the patient said:
An I ve got to be in there (the hospital) cos I am scared. Everything’s done for you. He (the doctor) makes it safe
Therefore, relationship between the patient and healthcare professional(s) played an important role in medication adherence. Another participant in the same paper also said:
I m on me knees, gasping, they take you in. And there you feel safe but on the other hand you get taken over—into pyjamas, told what to do, what to swallow. Nobody tells you anything. You have to obey’ em…(patient)’21
The patient perceived a negative experience of loss of autonomy and respect from the physician. This decreased the patients’ adherence to disease management. Attitude and compassion of healthcare professionals also play a role in building a good relationship, one patient from another included study stated:
… I have been contacting a doctor a number of times because it is an incredible amount of cough and phlegm. But it has not been taken seriously22
These cases revealed that patients and physicians’ relationship play an important role in disease management and medication adherence.
Communication Issue with/Between Healthcare Professionals
In the synthesised findings, both patients and physicians indicated that good communication could increase patients’ trust in their physicians, consequently, increasing their adherence to disease management. It showed that patients would not take the physician’s advice seriously if they felt that physicians did not take their concerns seriously. For example, one patient said:
Nobody wants to know yer poorly. Nobody tends to listen (Patient)22
In this previous study, the patients felt that physicians tended not to listen intently to their concerns, as a result the patient’s negative clinical experience would subsequently decrease his/or her adherence to disease management and medical treatment.
Communication between physicians was also indicated as a barrier to patients’ adherence to medication, which is reflected in the lack of continuity of care and follow up. As one physician said:
There is often a lack of continuity of therapy due to patients seeking advice from different physicians and health care providers (Physician)23
In another included study, one physician also said this:
Some need a closer follow-up, a weekly phone call. If they get to adhere at that point, then it’s done because they notice the benefits of medication adherence, but if we offer a 3-to-4 month follow-up, we lose them’ (Physician)24
In Lindberg et al study, patients also expressed their desire to follow up with physicians:
I d like to have continual follow-up visits for my asthma to keep my illness under control, and I’d like to be seen by the same staff person who has training in asthma (Patient)25
So good communication with/between healthcare professionals and patients played a role in continuity of care and subsequently, disease management and medical adherence.
Healthcare Accessibility
Timely appointments with a physician to renew prescriptions is another key component for treatment adherence. Otherwise, diseases management continuity will not be kept, one patient said:
So then you get stuck in a queue, maybe wait one to two weeks, or that all doctors should come home from their holidays, to get to one s doctor, to get the prescription… (Patient)22
One healthcare professional also said:
There aren t even enough human resources. It has happened to me sometimes that just one doctor oversees all the emergency area (HCP)26
Other factors such as the cost of treatment and medication are also a barrier to medication adherence when the review studies were conducted in a paid for healthcare system. This has been identified from both patients and physicians’ perspectives. For example, one patient said:
My physician told me to take my medication in the mornings and in the evenings, but I take it every two days because that’s a lot of money!27
One allied health professional also claimed:
You have rent to pay, you have your debts, your car; you have to dress your kids, feed them, feed yourself. So when your medication comes into your paying line, probably it annoys you to go and get it. (Allied health professionals)27
When this happens in a paid for healthcare service, the cost becomes a barrier to medicine adherence.
Synthesised Finding 2: Insufficient Information from Healthcare Professionals Acting as Barrier for Adherence
Patients Lack Information and Knowledge
Patients who lack knowledge and information about their diseases and medicines are less likely to adhere to medication, as one patient said:
I didn t know that it is prescribed for twice a day. I just use it when I am short of breath. Other times I go through an inhaler a day28
In an included review paper, one patient expressed his/her feeling by saying:
I d like to know exactly what they do to you - and they do not tell you that! It took me a few years to realise you should always request information, you are never told these things, you have to find out for yourself29
From these quotes, it can be seen that participants’ lack of knowledge was a barrier to treatment concordance. When healthcare professionals were not providing enough information, the patients were less likely to take their health condition and treatment seriously. However, there were some contradictions in the reviewed papers; while participants stated that they had not received sufficient information on their treatment, they also expressed their worries about the side effects of the medication. This will be explored further in the following findings. However, most patients wanted more accurate information and more education from healthcare professionals.
Education is Needed for Patients
The patients agreed that educational intervention from their physician would facilitate medication adherence. Patients also expressed that such an intervention should be delivered at the last stage of the asthma continuum, ie, after having an exacerbation, because that was when they were ready to engage in appropriation of asthma and self-management, as one patient explained:
When the physician tells you take the medication, unless you know what may happen to you, you don’t really pay attention. You start considering seriously … when you accept that you will have to take it for the rest of your life24
Another participant also expressed his/her desire for education:
I think that in general everybody, relatives, people you work with, need more information, because asthma is increasing in the community25
The need for educating patients was also desired from healthcare professionals as one participant said:
Education programs and health programs that teach what asthma is and that can remove all the taboos that we have about asthma (HCP)26
One Allied Healthcare Professional (AHP) also said:
I would say that the intervention has to have an impact on the patient… it has to improve the patient’s health… it has to have an overall positive impact that the patient can notice. The patient will be pleased with such an intervention… (APH)24
In this review paper, an AHP described patient’s knowledge as a core component for medicine adherence and it was key to supporting the patient in achieving asthma self-management. AHPs also agreed that healthcare professionals are the key contributors to this process by offering patients educational support.
One pharmacist also complained they used too much time to educate patients about medicine due to the lack of medication educational intervention from physicians:
More than 50% of time in dispensing a prescription is taken up by providing patient education which should have been provided by the physician23
All these above extracts highlight how educational intervention is needed for patients, as it is an important component of medication treatment adherence.
Synthesised Finding 3: How Patient’s Attitude/Beliefs Effect Their Adherence to Medication
Attitude Toward Disease
Patients not wanting to accept their diagnosis and the fact that asthma requires daily treatment can facilitate non-adherence to medication, as one participant said:
You’re not really yourself when you are on medication. (Patient)30
Participants hid their health condition due to stigmatisation of their illness:
We do not want others to know we are asthmatics and we have to take the inhalers. (Patient)27
In these two extracts, participants expressed feelings, such as loss of identity and embarrassment due to regular inhaler treatment, this appears to have played a role in how they perceived the changes in themselves. This has also affected their willingness to adhere to medicines.
Another participant was reluctant to take her asthma medicine to keep her health condition a secret from her children:
Even the children know now when I’m on them, they say Mummy’s back on her drugs
I am really bad tempered and wicked…I just go upstairs and sit in a room to get away from them all rather than say things that I’d regret… (Patient)29
Here, the participant perceived feelings of compromising her parental figure and that the illness had overall affected the daily life of her and her family.
Therefore, patient’s recognition and attitude toward the disease and knowledge of the severity and consequence of disease affects their diseases management and perception of medication. All of this is a very important for medication adherence.
Beliefs/Knowledge About Medicine
Perceptions or beliefs towards medication is another facilitator of adherence. Distrust and consideration of the side effects increases non-adherence to medication, as one patient said
I don’t really believe in the medication, and then I think about side effects. I am sceptical about all medications, and I have heard it can be dangerous to combine asthma medications with other drugs25
This had also happened in another review paper:
Steroids for me are all about your bones, that’s the thing for me, I sort of think it’s to do with your bone density and certainly your more prone to the likes of osteoporosis. (Patient)29
Another participant had similar issues:
the more you take something you get immune to it. That’s why they kept upping my asthma medication. (Patient)28
When participants hold negative images of the potential side effects of asthma controlling medicines, such as corticosteroids, it led them to fear taking the medicines and increases non-adherence thoughts and actions. This was also characterized by physicians, for example, one physician said:
[Patients] perceive the medication depending on their beliefs. For example, they think that if they take the medication when they have no symptoms, they will get used to it, so when they really need it, it won’t work. Like the narcotics, you know? (Physician)27
On the other hand, trusting the benefit of medications made patients adhere more to asthma treatment. This was presented in another study:
It [Seretide] definitely does prevent it [asthma] and you know like if I’m feeling little bit tightly and I take it [Ventolin], just treats it [asthma] for sure. (Patient)31
These extracts show that a correct perception and belief of medicine is another key component for medicine adherence.
Synthesised Finding 4: Patients’ Personal Behaviour and Other Relevant Barriers
Patients’ Personal Behaviour
This synthesised finding indicates that patients’ personal behaviour affects their adherence. For example, one participant stated:
Sometimes I wasn’t taking the inhaler (ICS), because like I am fine now…I do not take it when I am fine. I do not take it every day like I am supposed to…Like now, I do not have a cold. I am fine. So, I did not take it. (Patient)32
Similar findings were also identified in other review papers, such as one patient said:
I do not like so much taking them, so I avoid them sometimes, because I. It does not feel like you should take such substances. So then I’ve stopped taking them sometimes if I feel fine. (Patient)21
It is encouraging that some participants accepted that it was their responsibility as a patient to adhere to the medication.
For me, there are different levels of responsibility. That of the diagnosis and prescription, ok, it’s the physician’s. But once I have the prescription in my pocket or at the drug store, it’s my own responsibility. The adherence… that belongs to me! (Patient)27
For the participant, adherence to medication was achieved by being responsible and taking the medication as prescribed.
External Factor Influencing Asthma Control
External factors, such as a busy life can prevent medication adherence. As one patient said:
The nebuliser takes up quite a lot of time in the mornings when you are getting ready with the kids and things like that for school. (Patient)29
Other factors, such as, living environment was also asthma factor for some individuals.
Discussions and Recommendations
This systematic review synthesised evidence-based studies into patients and healthcare professionals’ perspectives of medication adherence from 12 previous studies. The synthesised findings identified the existing qualitative studies exploring medication adherence with respect to asthma control and explored the factors associated with medication adherence or nonadherence. It found that knowledge and belief are the main factors that affected medication adherence and that relationship and dialogue are also barriers to adherence.
Our findings suggest that the relationship and communication with/between healthcare professionals and patients play an important role in medication adherence. This is consistent with previous studies that indicate communication between clinicians and patients was associated with medication adherence.33,34 Patients lack of trust in health professionals and self-motivation were also identified as barriers to treatment adherence.31 One study indicated that detecting patients’ non-adherence behaviours and appreciating their self-management may help to change their behaviour and increase adherence.35 On the other hand, patients think that their physicians did not have enough time or provide enough information to them, which contributed to patients lack of sufficient knowledge of the importance of treatment adherence to controlling their asthma.22,29 A systematic review reported that patient–provider interactions was significantly related to treatment adherence and patient health outcomes;36 so it is likely that adherence would increase if the rationale of the treatment plan was explained in a way that patients can understand and follow. Therefore, ensuring patients’ decisions are based on good information is very important. Effective communication between health professionals and patients will increase patients’ trust, motivation, and lead to improved adherence and health outcomes.
Adherence is also influenced by the patients’ knowledge and beliefs about their disease and medications, in particular, associated with how the patients judge their personal need for the treatment (severity of disease), and potential adverse effects of medications. Previous studies have indicated that a patient’s lower perception for the necessity of medication and lack of faith in the treatment was associated with non-adherence behaviour.37 These modifiable factors need to be addressed in order to increase medication adherence. In addition, studies found that limited health literacy, family and culture also contributed to underuse of asthma controller medications.7,38 So, it is important to consider the individual health literacy and cultural perspective of the patient when developing an education programme or self-management support strategies, so these interventions can be tailored at a personal level. One previous study found that patient’s attitude and behaviour of medication adherence were strongly associated with friends/family’s opinions.39 It is suggested that considering or involving family members with patients’ treatment plan may have the potential to increase medication adherence. In addition, in the studies reviewed, only one study included a minority ethnic group, therefore it is worth further exploring how cultural beliefs and perceptions of minority ethnic groups effect their personal behaviour and medication adherence.
Strategies for improving medication adherence are considered by many studies,14,38,40,41 which included shared treatment goals between healthcare professionals and patients, daily routine and bathroom strategies, health literacy techniques and patient-centred approaches or patient-targeted interventions. In recent two decades, there is a growing interest in using IT to support self-management and education.42 Building a dialogue platform between healthcare professionals and patients is critical to reach these aims. For example, via electronic devices or telecare to establish fluent communication in order to track adherence and remind patients to take their medication, gaining feedback on inhaler technique, avoiding triggers, or booking an appointment for check-up or reviews. Punctual following ups are also a very important element of controlling asthma. Patients’ healthcare annual review has been recommended across healthcare settings, however, due to various reasons, it is not done as well as it should be in some settings. Finally, educational interventions to improve patients’ knowledge of their disease and treatment adherence is needed based on individual understanding, to truly empower patients to make informed decisions on their treatment rather than decisions just being made by healthcare professionals.
Strengths and Limitations
This review applied the JBI meta-aggregated approach and tools which demonstrated a transparent process for the review. We did not set restriction on publishing date which, at maximum, included all previous related studies in the study field. However, the included studies were in the English language only, this may neglect the publications in non-English and potentially caused bias in data searched. Grey literature was also not included in this review.
Conclusion
Non-adherence remains a significant problem in asthma control. This review investigated the barriers and stimulators of medication adherence from 12 previous studies. The synthesized findings provide a strong evidence-base of patient and health professionals’ perspectives and behaviours toward medication adherence, which helps to identify and address non-adherence. Healthcare providers can use these findings to support patients’ adherence to asthma medications. The key element is to empower patients to make informed decisions rather than “adherence controlling” by health professionals. Effective dialogue and appropriate education are important approaches to increase medication adherence.
Disclosure
Professor Jennifer K Quint reports grants from MRC, grants from HDR UK, grants, personal fees from AZ, grants, personal fees from GSK, grants, personal fees from Insmed, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Menzies-Gow A, Corren J, Bourdin A, et al. Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N Eng J Med. 2021;384(19):1800–1809. doi:10.1056/NEJMoa2034975
2. Janson C, Menzies-Gow A, Nan C, et al. SABINA: an overview of short-acting β2-agonist use in asthma in European countries. Adv Ther. 2020;37(3):1124–1135. doi:10.1007/s12325-020-01233-0
3. Stanford RH, Shah MB, D’Souza AO, et al. Short-acting β-agonist use and its ability to predict future asthma-related outcomes. Ann Allergy Asthma Immunol. 2012;109(6):403–407. doi:10.1016/j.anai.2012.08.014
4. Makhinova T, Barner JC, Richards KM, et al. Asthma controller medication adherence, risk of exacerbation, and use of rescue agents among Texas Medicaid patients with persistent asthma. J Managed Care Specialty Pharmacy. 2015;21(12):1124–1132. doi:10.18553/jmcp.2015.21.12.1124
5. Amin S. Usage patterns of short-acting β2-Agonists and inhaled corticosteroids in asthma: a targeted literature review. J Allergy Clin Immunol. 2020;8(8):2556–2564. e8.
6. Jeminiwa R, Hohmann L, Qian J, et al. Impact of eHealth on medication adherence among patients with asthma: a systematic review and meta-analysis. Respir Med. 2019;149:59–68. doi:10.1016/j.rmed.2019.02.011
7. McQuaid EL. Barriers to medication adherence in asthma: the importance of culture and context. Ann Allergy Asthma Immunol. 2018;121(1):37–42. doi:10.1016/j.anai.2018.03.024
8. Mes MA, Katzer CB, Chan AHY, et al. Pharmacists and medication adherence in asthma: a systematic review and meta-analysis. Eur Respir J. 2018;52(2):1800485. doi:10.1183/13993003.00485-2018
9. Murphy AC, Proeschal A, Brightling CE, et al. The relationship between clinical outcomes and medication adherence in difficult-to-control asthma. Thorax. 2012;67(8):751–753. doi:10.1136/thoraxjnl-2011-201096
10. O’Byrne PM, Jenkins C, Bateman ED. The paradoxes of asthma management: time for a new approach? Eur Respir J. 2017;50(3):20.
11. Brandstetter S, Finger T, Fischer W, et al. Differences in medication adherence are associated with beliefs about medicines in asthma and COPD. Clin Transl Allergy. 2017;7(1):1–7. doi:10.1186/s13601-017-0175-6
12. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol. 2013;110(2):75–79. e2. doi:10.1016/j.anai.2012.11.006
13. Kaplan A, Mitchell PD, Cave AJ, et al. Effective asthma management: is it time to let the AIR out of SABA? J Clin Med. 2020;9(4):921. doi:10.3390/jcm9040921
14. van Boven JF, Ryan D, Eakin MN, et al. Enhancing respiratory medication adherence: the role of health care professionals and cost-effectiveness considerations. J Allergy Clin Immunol Pract. 2016;4(5):835–846. doi:10.1016/j.jaip.2016.03.007
15. Canonica G, Baena-Cagnani CE, Blaiss MS, et al. Unmet needs in asthma: global Asthma Physician and Patient (GAPP) Survey: global adult findings. Allergy. 2007;62(6):668–674. doi:10.1111/j.1398-9995.2007.01352.x
16. Engelkes M, Janssens HM, de Jongste JC, et al. Medication adherence and the risk of severe asthma exacerbations: a systematic review. Eur Respir J. 2015;45(2):396–407. doi:10.1183/09031936.00075614
17. Lockwood C, Munn Z, Porritt K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta-aggregation. JBI Evidence Implementation. 2015;13(3):179–187.
18. Stern C, Jordan Z, McArthur A. Developing the review question and inclusion criteria. AJN Am J Nursing. 2014;114(4):53–56. doi:10.1097/01.NAJ.0000445689.67800.86
19. Munn Z, Barker TH, Moola S, et al. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evidence Synthesis. 2020;18(10):2127–2133. doi:10.11124/JBISRIR-D-19-00099
20. Peters MD, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
21. Walsh S, Hagan T, Gamsu D. Rescuer and rescued: applying a cognitive analytic perspective to explore the ‘mis‐management’of asthma. Br J Med Psychol. 2000;73(2):151–168. doi:10.1348/000711200160390
22. Hedenrud T, Jakobsson A, El Malla H, et al. “I did not know it was so important to take it the whole time”− self-reported barriers to medical treatment among individuals with asthma. BMC Pulm Med. 2019;19:1–10. doi:10.1186/s12890-019-0934-3
23. Davis P, Man P, Cave A, et al. Use of focus groups to assess the educational needs of the primary care physician for the management of asthma. Med Edu. 2000;34(12):987–993. doi:10.1046/j.1365-2923.2000.00685.x
24. Peláez S, Bacon SL, Lacoste G, et al. How can adherence to asthma medication be enhanced? Triangulation of key asthma stakeholders’ perspectives. J Asthma. 2016;53(10):1076–1084. doi:10.3109/02770903.2016.1165696
25. Lindberg M. Asthma care and factors affecting medication compliance: the patient’s point of view. Int J Quality Health Care. 2001;13(5):375–383. doi:10.1093/intqhc/13.5.375
26. Ardura-Garcia C, Blakey JD, Cooper PJ, et al. Caregivers’ and healthcare professionals’ perspective of barriers and facilitators to health service access for asthmatic children: a qualitative study. BMJ Open Respir Res. 2021;8(1):e001066. doi:10.1136/bmjresp-2021-001066
27. Peláez S, Bacon SL, Aulls MW, et al. Similarities and differences between asthma health care professional and patient views regarding medication adherence. Canadian Respir J. 2014;21(4):221–226. doi:10.1155/2014/738654
28. Norful AA, Bilazarian A, Chung A, et al. Real-world drivers behind communication, medication adherence, and shared decision making in minority adults with asthma. J Prim Care Community Health. 2020;11:2150132720967806. doi:10.1177/2150132720967806
29. Gamble J, Fitzsimons D, Lynes D, et al. Difficult asthma: people’s perspectives on taking corticosteroid therapy. J Clin Nurs. 2007;16(3):59–67. doi:10.1111/j.1365-2702.2006.01750.x
30. Scherman MH, Löwhagen O. Drug compliance and identity: reasons for non-compliance: experiences of medication from persons with asthma/allergy. Patient Educ Couns. 2004;54(1):3–9. doi:10.1016/S0738-3991(03)00199-X
31. Wadhahi AA, Garvey, L, Edward, K-L, et al. The lived experience of adherence to asthma medication in young adults (18–34 years). J Asthma. 2022;59(12):2475–2490. doi:10.1080/02770903.2021.2018706
32. George M, Keddem S, Barg FK, et al. Urban adults’ perceptions of factors influencing asthma control. J Asthma. 2015;52(1):98–104. doi:10.3109/02770903.2014.947651
33. Sleath B, Carpenter DM, Slota C, et al. Communication during pediatric asthma visits and self-reported asthma medication adherence. Pediatrics. 2012;130(4):627–633. doi:10.1542/peds.2012-0913
34. Young HN, Len-Rios ME, Brown R, et al. How does patient-provider communication influence adherence to asthma medications? Patient Educ Couns. 2017;100(4):696–702. doi:10.1016/j.pec.2016.11.022
35. Dhruve H. Management of asthma: adherence, inhaler technique and self-management. Practice Nursing. 2018;29(10):465–468. doi:10.12968/pnur.2018.29.10.465
36. Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health. 2015;105(12):e60–e76. doi:10.2105/AJPH.2015.302903
37. Sofianou A, Martynenko M, Wolf MS, et al. Asthma beliefs are associated with medication adherence in older asthmatics. J Gen Intern Med. 2013;28(1):67–73. doi:10.1007/s11606-012-2160-z
38. Soones TN, Lin JL, Wolf MS, et al. Pathways linking health literacy, health beliefs, and cognition to medication adherence in older adults with asthma. J Allergy Clin Immunol. 2017;139(3):804–809. doi:10.1016/j.jaci.2016.05.043
39. Foster J, Smith L, Bosnic-Anticevich SZ, et al. Identifying patient‐specific beliefs and behaviours for conversations about adherence in asthma. Intern Med J. 2012;42(6):e136–e144. doi:10.1111/j.1445-5994.2011.02541.x
40. George M. Adherence in asthma and COPD: new strategies for an old problem. Respir Care. 2018;63(6):818–831. doi:10.4187/respcare.05905
41. Brooks TL, Leventhal H, Wolf MS, et al. Strategies used by older adults with asthma for adherence to inhaled corticosteroids. J Gen Intern Med. 2014;29(11):1506–1512. doi:10.1007/s11606-014-2940-8
42. Heaney LG, Busby J, Bradding P, et al. Remotely monitored therapy and nitric oxide suppression identifies nonadherence in severe asthma. Am J Respir Crit Care Med. 2019;199(4):454–464. doi:10.1164/rccm.201806-1182OC
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Medication Adherence and Risk of COPD in Adult Asthma Patients: A Retrospective Cohort Study in Canada
Asamoah-Boaheng M, Farrell J, Bonsu KO, Oyet A, Midodzi WK
Clinical Epidemiology 2022, 14:1241-1254
Published Date: 27 October 2022
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
Safety and Effectiveness of Magnesium Sulphate for Severe Acute Asthma Management Among Under-five Children: Systematic Review and Meta-analysis
Mega TA, Gugsa H, Dejenie H, Hussen H, Lulseged K
Journal of Asthma and Allergy 2023, 16:241-247
Published Date: 3 March 2023
Effect of Biologic Therapies on Airway Hyperresponsiveness and Allergic Response: A Systematic Literature Review
Spahn JD, Brightling CE, O’Byrne PM, Simpson LJ, Molfino NA, Ambrose CS, Martin N, Hallstrand TS
Journal of Asthma and Allergy 2023, 16:755-774
Published Date: 21 July 2023
Utilizing Social Determinants of Health Model to Understand Barriers to Medication Adherence in Patients with Ischemic Stroke: A Systematic Review
Ruksakulpiwat S, Benjasirisan C, Ding K, Phianhasin L, Thorngthip S, Ajibade AD, Thampakkul J, Zhang AY, Voss JG
Patient Preference and Adherence 2023, 17:2161-2174
Published Date: 30 August 2023