Back to Journals » Journal of Inflammation Research » Volume 18
Neutrophil-to-Albumin Ratio Predicts Stroke-Associated Pneumonia in Patients with Intracerebral Hemorrhage
Authors Wan J, Liu Y, Yuan X, Fan S, Xiao Y, Fang F, Zhang Y
Received 27 January 2025
Accepted for publication 1 July 2025
Published 11 August 2025 Volume 2025:18 Pages 10835—10843
DOI https://doi.org/10.2147/JIR.S519664
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Adam Bachstetter
Jun Wan,1,* Yuyang Liu,1,* Xiang Yuan,2 Shijie Fan,1 Yangchun Xiao,3 Fang Fang,2 Yu Zhang3
1Center for Evidence-Based Medicine, Clinical Medical College and Affiliated Hospital of Chengdu University, Chengdu, Sichuan, People’s Republic of China; 2Department of Neurosurgery, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 3Department of Neurosurgery, Clinical Medical College and Affiliated Hospital of Chengdu University, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Zhang, Department of Neurosurgery, Clinical Medical College and Affiliated Hospital of Chengdu University, Chengdu, Sichuan, People’s Republic of China, Tel +8618113034616, Email [email protected]
Background and Aim: Pneumonia is a significant complication that negatively impacts outcomes in patients with intracerebral hemorrhage (ICH). Identifying reliable biomarkers for predicting such infections is crucial for timely intervention and improving patient management. This study aims to evaluate the predictive value of neutrophil-to-albumin Ratio (NAR)for pneumonia in patients undergoing surgical intervention for ICH.
Methods: This was a retrospective multicenter cohort study conducted at four tertiary hospitals. A total of 8016 patients diagnosed with spontaneous intracerebral hemorrhage (ICH) between were included. The neutrophil-to-albumin ratio (NAR) was calculated within 24 hours of admission. Logistic regression models, receiver operating characteristic (ROC) curves, and reclassification metrics (C-index, IDI, cNRI) were used to evaluate the association between NAR and the risk of pneumonia. The primary outcome was pneumonia.
Results: A total of 8016 ICH patients were included in this study. Among them, 3921 patients (48.9%) had pneumonia. There was an association between NAR levels and pneumonia (OR = 1.81, 95% CI: 1.69– 1.94, p < 0.001). After adjustment, the results remained significant (adjusted OR = 1.62, 95% CI: 1.51– 1.75, p < 0.001). Compared to patients in the Low Group (NAR ≤ 0.21), those in the High Group (NAR > 0.21) had a higher long-term mortality risk (OR = 2.95, 95% CI: 2.68– 3.24, p < 0.001; adjusted OR = 1.99, 95% CI: 1.79– 2.21, p < 0.001). Additionally, the predictive performance of NAR for pneumonia was also significant (area under the ROC curve [95% CI] 0.663 [0.651– 0.675]; p < 0.001).
Conclusion: Higher NAR is independently associated with pneumonia in patients with ICH. The early prediction of pneumonia using the simple biomarker NAR is feasible.
Keywords: intracerebral hemorrhage, neutrophil-to-albumin ratio, inflammation, pneumonia
Introduction
Intracerebral hemorrhage (ICH) remains one of the most devastating types of strokes, characterized by high morbidity and mortality rates.1–3 Pneumonia are a common complication in patients with ICH, contributing significantly to poor outcomes, prolonged hospital stays, and increased healthcare costs.4–6 Stroke-associated pneumonia (SAP) is a common and serious complication following intracerebral hemorrhage, arising due to a combination of stroke-induced immunosuppression, impaired consciousness, dysphagia, and reduced airway protective reflexes.7 Several clinical trials have assessed the use of antibiotics to prevent pneumonia following a stroke; however, the results from these trials demonstrate that antibiotic prophylaxis is ineffective in preventing pneumonia.8–11 Identifying reliable biomarkers to predict the risk of infection is therefore crucial to enhance clinical decision-making and improve patient management.
The development of SAP significantly worsens patient outcomes, leading to increased morbidity, prolonged hospitalization, higher healthcare costs, and elevated mortality rates. Early identification of patients at risk for SAP is crucial for timely preventive interventions. Biomarkers reflecting systemic inflammation and nutritional status, such as the Neutrophil-to-Albumin Ratio (NAR), offer promising tools for improving early risk stratification and guiding clinical decision-making.
Systemic inflammatory responses following a hemorrhagic event are associated with an increased risk of various complications, including infections.12–14 Numerous studies have suggested that inflammation-based biomarkers, such as the neutrophil-to-lymphocyte ratio (NLR),15 platelet-to-lymphocyte ratio (PLR),16 platelet to albumin ratio (PAR),11 and neutrophil percentage to albumin ratio (NPAR),17 can serve as effective predictors of outcomes in ICH patients.
The Neutrophil-to-Albumin Ratio (NAR) is an emerging inflammatory marker that combines changes in neutrophil and albumin levels, reflecting the body’s immune-inflammatory status and nutritional condition.18 NAR was initially discovered to be closely related to the level of inflammation and disease prognosis in cardiovascular diseases. Currently, its application has expanded to other fields such as cancer, critical illness, and more.19–22 However, it remains unclear whether the NAR can serve as an inflammatory biomarker to predict pneumonia in ICH patients. Our study aims to determine whether the NAR is associated with pneumonia in patients with ICH and compare it with other inflammatory biomarkers.
Methods
Study Design
This study was a retrospective, multicenter cohort analysis investigating the association between the Neutrophil-to-Albumin Ratio (NAR) and pneumonia in patients with ICH. A total of 8016 patients diagnosed with spontaneous ICH were included from four hospitals: West China Hospital of Sichuan University (January 2011–July 2019), The First People’s Hospital of Longquanyi District Chengdu (January 2017–October 2020), the Affiliated Hospital of Chengdu University (August 2012–November 2020) and Shanxi Provincial People’s Hospital (July 2014–November 2021). This study adhered to the STROBE guidelines and complied with the principles of the Declaration of Helsinki. Ethical approvals were obtained from the respective institutional review boards of all four hospitals, and informed consent was waived due to the study’s retrospective nature.
Patient Selection
Patients were included if they were aged 18 years or older and diagnosed with spontaneous ICH confirmed by computed tomography (CT), magnetic resonance imaging (MRI), or neurosurgical diagnosis during hospitalization. Exclusion criteria included: (1) ischemic stroke with hemorrhagic transformation, trauma, cerebral aneurysm, arteriovenous malformations, or coagulation-related hemorrhagic disorders; (2) evidence of infection or hospital-acquired infection before admission; (3) missing NAR data or albumin/neutrophil counts not measured within 24 hours of admission.
Exposure
The primary exposure of this study was NAR, which was calculated as the ratio of the neutrophil count to serum albumin levels. Peripheral blood samples were taken, and serum neutrophil and albumin levels were evaluated at the time of admission. Serum albumin concentrations were measured using the Beckman Coulter AU5800 automated biochemical analyzer based on the bromocresol green method. Complete blood counts, including neutrophil counts, were obtained using the Sysmex XN-9000 automated hematology analyzer. We used NAR to compare with other inflammatory markers, including NPAR, NLR, PLR, and PAR, to assess their predictive power. The NAR values were categorized into two groups based on the Youden index: Low group (≤0.21) and High group (>0.21).
Clinical Assessment
The following data were collected from the patients: demographic characteristics, anthropometric characteristics, medical history data, clinical features, and imaging information, including the Glasgow Coma Scale (GCS, with a lower score indicating a worse level of consciousness) score, infratentorial hematoma, hematoma size, intraventricular hematoma, hypertension, diabetes, smoking status, and alcohol consumption. Laboratory tests were performed within 24 hours of admission, including routine blood tests. We calculated the NAR, NPAR, NLR, PLR and NAR according to the following equations: NAR= neutrophil count/albumin, NPAR = neutrophil percentage/albumin, NLR = neutrophil count/lymphocyte count; PLR = platelet count/lymphocyte count; and PAR = platelet/albumin.
Outcome
The primary outcome was pneumonia. Pneumonia was defined as lower respiratory tract infections that satisfied the Modified Centers for Disease Control and Prevention criteria, which also incorporated diagnostic alterations observed on at least one chest x-ray or chest computed tomography.23
Statistical Analysis
All statistical analyses were performed using R software version 4.4.1 and R Studio.
Continuous variables, including age, hematoma volume, Glasgow Coma Scale (GCS), and laboratory data, were summarized as means with standard deviations or medians with interquartile ranges and compared using Student’s t-test or Mann–Whitney U-test, as appropriate. Categorical variables were presented as frequencies or percentages and compared using the chi-square test or Fisher’s exact test.
We used restricted cubic spline (RCS) models to evaluate the potential nonlinear relationship between NAR and pneumonia risk. Significant variables (p < 0.10) in univariate analyses were included in the multivariable logistic regression models. NAR trends over time were displayed using trajectory plots.
As suggested by the TRIPOD statement, Harrell’s C-statistics (C-index) and integrated discrimination improvement (IDI) were used to compare the ability of NAR and other inflammatory biomarkers to predict pneumonia.24,25 The IDI is computed by adding the proportion of patients whose probability is forecasted to increase to the proportion of non-patients whose probability is predicted to decrease. The cNRI is an index for comparing the classification ability of old and novel models using the gold standard diagnosis. IDI and cNRI were used to assess whether the addition of NAR improved the discrimination and classification of pneumonia risk compared to existing models. A higher IDI or cNRI value indicates better model performance. According to the previous study,26 we defined risk ratio < 0.1 as low, 0.1–0.6 as moderate, and > 0.6 as high risk of pneumonia. We used the Receiver Operating Characteristic (ROC) curve and the Area Under the ROC Curve (AUROC) to calculate the predictive value of NAR, NPAR, NLR, PLR, and PAR for hospital-acquired infection.
Subgroup analyses explored heterogeneity in associations based on age, sex, smoking, alcohol use, hypertension, diabetes, hematoma location, volume, intraventricular hemorrhage, GCS scores, and intracranial hematoma clearance. Based on the best cutoff value of NAR (0.21), patients were divided into low and high groups. All factors were selected based on clinical recommendations, previous studies, and the review of risk scores. All statistical analyses were performed using R software (version 4.4.1), with P-values < 0.05 considered statistically significant. All p-values were two-sided. Missing and infinite data were estimated using the median.
Result
Baseline Characteristics of the Cohort
A total of 8016 ICH patients were enrolled in this study (Figure 1). Table 1 presents the baseline characteristics of the included patients. The mean age of the cohort was 58.22 ± 14.48 years, with 3297 (41.1%) being female. Patients in the high NAR group (> 0.21) were more likely to have a history of smoking (p = 0.002) and diabetes (p = 0.004). Additionally, patients in the high NAR group tended to have larger hematoma volumes and lower Glasgow Coma Scores (p < 0.001, both). Platelet counts, blood glucose levels, and neutrophil counts were also significantly higher in the high NAR group compared to the low NAR group (p < 0.001). These differences in baseline characteristics suggest a potential association between NAR and the severity of ICH in patients.
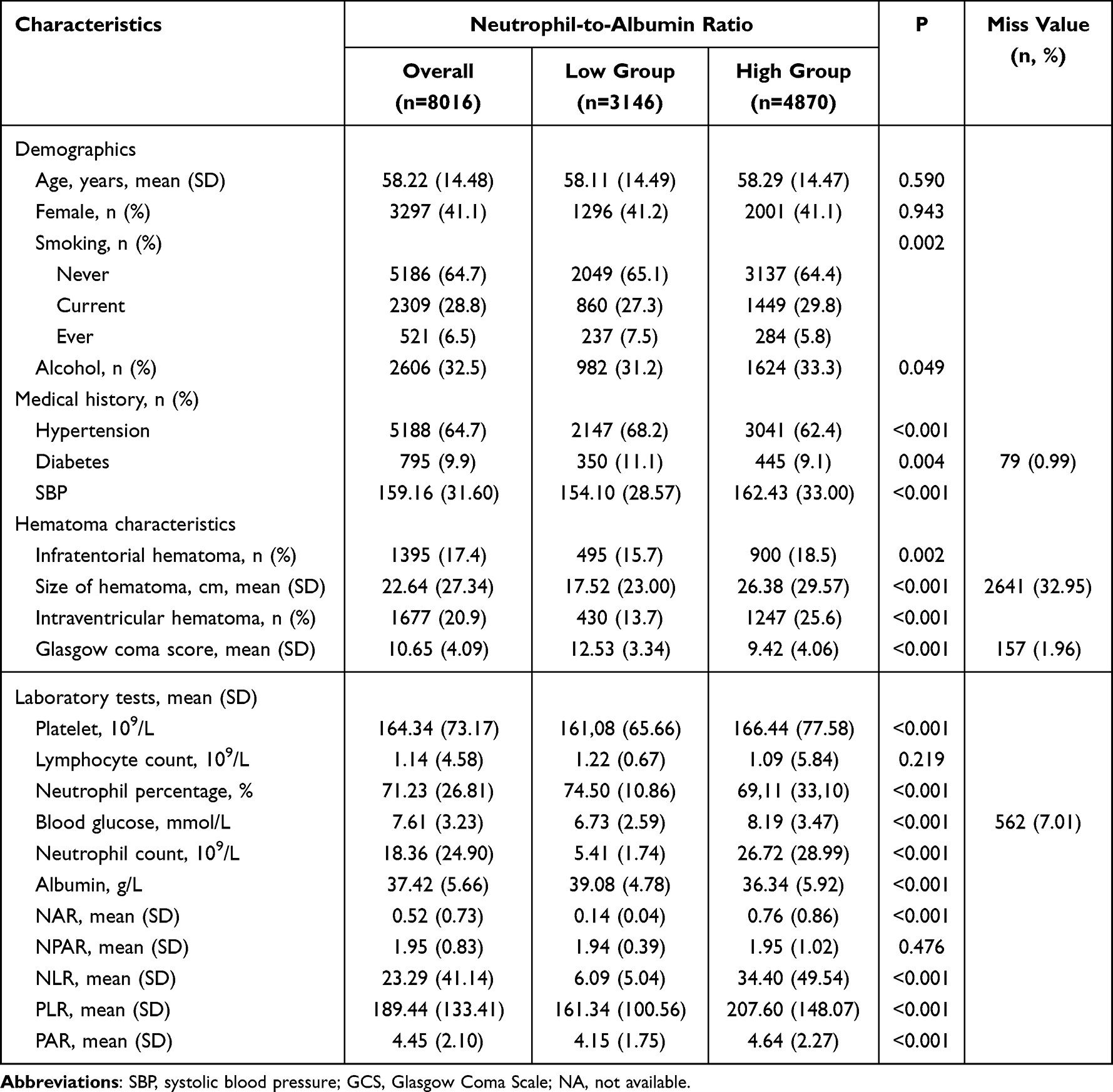 |
Table 1 Baseline Characteristics of the Patients |
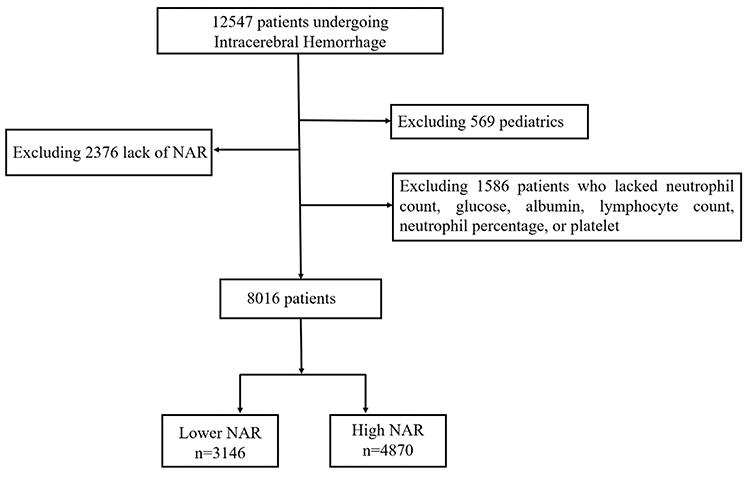 |
Figure 1 Flow diagram for the selection of participants included in the present analysis. |
Association Between NAR and Pneumonia
As shown in Figure 2, there was a significant and linear association between NAR levels and the risk of pneumonia (P for nonlinearity <0.001). The adjusted odds ratio (OR) increased markedly with higher NAR values, indicating that elevated NAR is associated with an increased risk of pneumonia in patients with ICH.
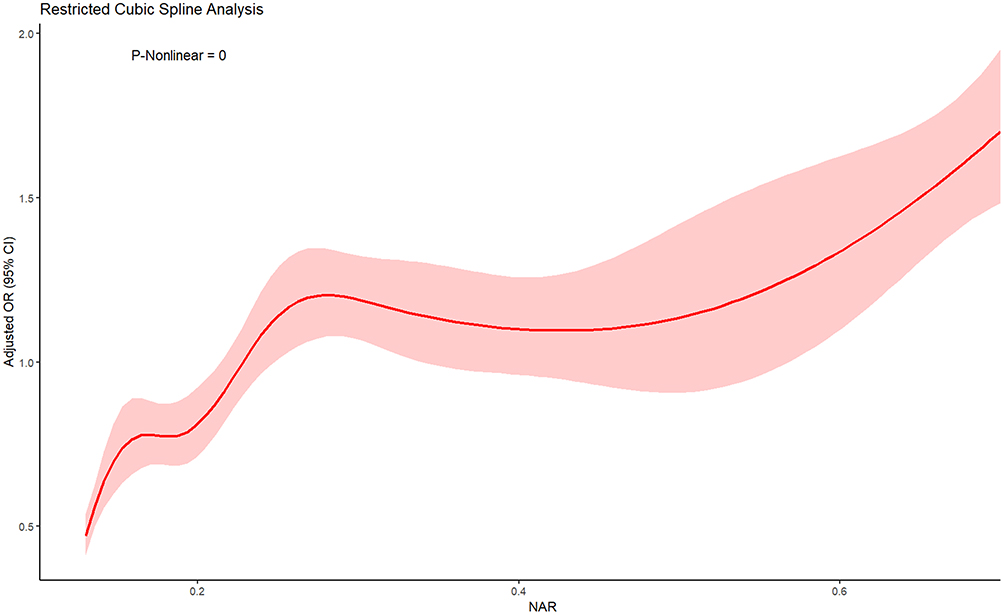 |
Figure 2 The Restricted Cubic Spline Depicting the Odds Ratio of Neutrophil-to-Albumin Ratio and hospital infection among Patients with Intracerebral Hemorrhage. |
The results of the logistic regression analysis are shown in eTable 1. In the univariable analysis, factors including age, diabetes, SBP, infratentorial hematoma, size of hematoma, intraventricular hematoma, GCS score, lymphocyte count, neutrophil percentage, blood glucose, and albumin level were all significantly associated with NAR (p < 0.1). In the multivariable logistic regression model, adjusted for age, smoking, diabetes, infratentorial hematoma, size of hematoma, intraventricular hematoma, and GCS score.
As shown in Table 2, higher NAR levels were significantly associated with an increased risk of pneumonia (adjusted OR=1.62, 95% CI: 1.51–1.75, p < 0.001), indicating that elevated NAR is an independent risk factor for pneumonia among ICH patients. A total of 8016 patients were included in the final cohort. 3921 patients (48.9%) developed pneumonia, while 4095 patients (51.1%) did not. Using the best cutoff value of NAR at 0.21, patients were categorized into low (NAR ≤ 0.21) and high (NAR > 0.21) groups. Compared to the low NAR group, patients in the high NAR group had a significantly increased risk of pneumonia (adjusted OR=1.99, 95% CI: 1.79–2.21, p < 0.001). In the quartile analysis, a positive dose-response relationship was observed between NAR levels and the risk of pneumonia (p for trend < 0.001). Compared to the lowest quartile (Q1: NAR < 0.17), patients in the highest quartile (Q4: NAR ≥ 0.39) had a markedly increased risk of pneumonia (adjusted OR=3.09, 95% CI: 2.55–3.74, p < 0.001). In this study, the OR for the derivation cohort was 1.80 (95% CI: 1.65–1.96), adjusted to 1.62 (95% CI: 1.49–1.77), and for the validation cohort, it was 1.83 (95% CI: 1.62–2.09), adjusted to 1.64 (95% CI: 1.43–1.89), indicating a consistent significant association after adjusting for confounders. In Figure 3, we conducted subgroup analyses based on age, sex, smoking, alcohol use, hypertension, diabetes, hematoma characteristics (intraventricular hematoma, hematoma size, infratentorial hematoma), and GCS score. OR and 95% CI are shown for each subgroup. The interaction P-values assess whether the effect of high NAR differs significantly across subgroups.
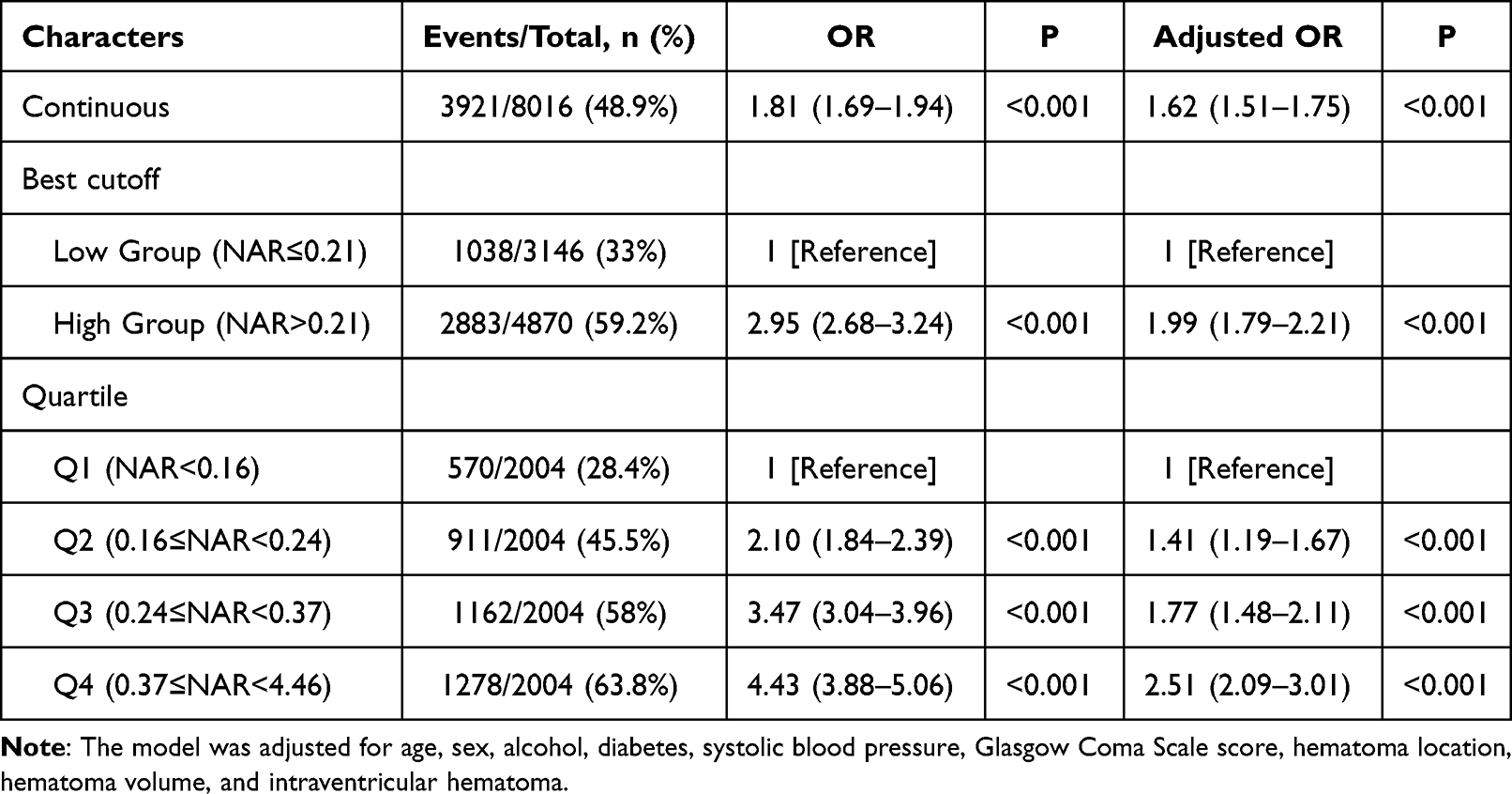 |
Table 2 The Association Between Neutrophil-to-Albumin Ratio and Pneumonia Using Logistic Regression |
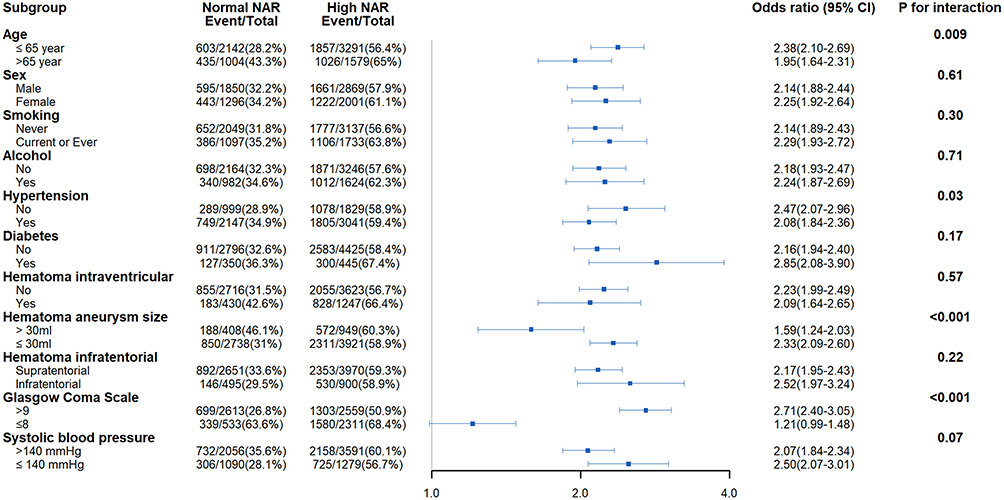 |
Figure 3 Subgroup Analysis of Association between N Neutrophil-to-Albumin Ratio and hospital infection. |
Promising Biomarker of ICH Pneumonia
The ROC curves for predicting pneumonia show that NAR and NLR have the highest AUC 0.663, 95% CI: 0.590–0.615), indicating better predictive accuracy compared to NPAR, NLR, PLR, and PAR (eFigure 1A). C-index, cNRI, and integrated IDI were calculated to compare the predictive efficacy of NAR with that of other inflammatory biomarkers, including NPAR, NLR, PLR, and PAR (eFigure 1B). NAR demonstrated a higher C-index (0.663, 95% CI: 0.590–0.615) compared to NPAR, NLR, and PAR, and was comparable to NLR, but NAR showed higher cNRI and IDI than NLR.
Discussion
In this retrospective observational study, we demonstrated that NAR is associated with an increased risk of pneumonia in patients with ICH, and that NAR has good predictive ability for pneumonia. Our findings are consistent with previous studies demonstrating the prognostic value of NAR in neurological diseases. For instance, Xin Zhang et al reported that elevated NAR levels predicted unfavorable outcomes in patients with aneurysmal subarachnoid hemorrhage (aSAH).27 Similarly, Zhibo Chen et al found that higher NAR was associated with increased all-cause mortality in stroke patients.28 These studies support the broader applicability of NAR as a valuable biomarker for risk stratification across various types of cerebrovascular events.
In our study, patients in the high NAR group were more likely to have a history of smoking and diabetes, both of which are established risk factors for systemic inflammation and impaired nutritional status. These comorbidities may partly explain the elevated inflammatory burden and lower serum albumin levels observed in these patients, leading to higher NAR values. Interestingly, although patients in the low NAR group exhibited slightly higher neutrophil percentages, the absolute neutrophil counts were actually lower compared to the high NAR group. Since NAR is calculated based on the absolute neutrophil count rather than the proportion of neutrophils, these findings are biologically plausible and support the validity of using NAR as an integrated biomarker reflecting both inflammation and nutritional deficits. Additionally, we observed that platelet counts and blood glucose levels were somewhat higher in the low NAR group. These variations likely reflect baseline metabolic differences among patients rather than inconsistencies in the predictive capacity of NAR. Overall, the strong association between high NAR and increased risk of pneumonia in ICH patients highlights the potential utility of NAR for early risk stratification and targeted intervention.
A previous study29 demonstrated a significant association between elevated levels of NPAR and pneumonia, as well as adverse functional outcomes in ICH patients. That study emphasized the importance of incorporating albumin into inflammatory markers to enhance predictive performance. Our study has several advantages over the previous research. First, we have a larger sample size, providing higher statistical power and robustness to our findings. Second, we found that NAR had a higher AUC compared to NPAR, indicating that NAR may serve as a more accurate predictor of pneumonia. Third, our study was conducted as a multicenter study, enhancing the generalizability of our results to a broader patient population.
Our study highlights the advantages of NAR over other commonly used inflammatory biomarkers such as NPAR, NLR, PLR, and PAR. While NLR primarily reflects the degree of inflammation, NAR offers a more comprehensive evaluation of the inflammatory burden by incorporating serum albumin levels, which also reflect nutritional status. We also compared the predictive performance of NAR with other biomarkers, demonstrating that NAR exhibited superior ability in risk stratification and accuracy. NAR achieved the highest C-index (0.663, 95% CI: 0.651–0.675), and demonstrated incremental improvement in reclassification performance, as evidenced by favorable IDI and cNRI values. Therefore, although the AUC of NAR is similar to that of NLR, in practical clinical applications, NAR has demonstrated better predictive ability and patient classification accuracy.
Despite the promising results, several limitations of our study should be acknowledged. First, the retrospective nature of the study design may introduce biases, including selection bias and confounding factors that could affect the results. Although we attempted to adjust for potential confounders, residual confounding cannot be entirely ruled out. Second, our reliance on electronic health records may have led to incomplete or inaccurate data, which could impact the reliability of our findings. Third, while our study was multicenter, it was still limited to specific healthcare settings, which may limit the generalizability of our results to other regions or healthcare systems. Fourth, the study did not account for all potential factors that might influence postoperative infection, such as detailed information on perioperative care protocols and antibiotic use. Finally, our findings are based on associations and cannot establish causality, highlighting the need for future prospective studies to validate our results.
Conclusion
NAR may serve as a promising and practical biomarker for early identification of pneumonia risk in ICH patients, showing relatively better predictive performance than other inflammatory markers based on AUROC, C-index, and cNRI analyses. This suggests that NAR can enhance risk stratification and help clinicians better identify high-risk patients for targeted interventions.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
All methods were carried out in accordance with relevant guidelines and regulations. All experimental protocols were approved by the ethics committee of West China Hospital (No. 20211701). The study was approved by the West China Hospital Institutional Review Board, with a waiver of informed consent from all subjects due to the retrospective nature of the study. Patient data were anonymized and de-identified prior to analysis to ensure confidentiality.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interests.
References
1. Cordonnier C, Demchuk A, Ziai W, Anderson CS. Intracerebral haemorrhage: current approaches to acute management. Lancet. 2018;392(10154):1257–1268. doi:10.1016/S0140-6736(18)31878-6
2. van Asch CJJ, Luitse MJA, Rinkel GJE, van der Tweel I, Algra A, Klijn CJM. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9(2):167–176. doi:10.1016/S1474-4422(09)70340-0
3. Tu WJ, Wang LD. China stroke surveillance report 2021. Mil Med Res. 2023;10(1):33. doi:10.1186/s40779-023-00463-x
4. Manesh MN, DiBartolomeo AD, Potter HA, et al. Association of anemia and transfusion with major adverse cardiac events and major adverse limb events in patients undergoing open infrainguinal bypass. Ann Vasc Surg. 2024;111:25–38. doi:10.1016/j.avsg.2024.10.007
5. Stein M, Hamann GF, Misselwitz B, Uhl E, Kolodziej M, Reinges MHT. In-hospital mortality and complication rates in surgically and conservatively treated patients with spontaneous intracerebral hemorrhage in central Europe: a population-based study. World Neurosurg. 2016;88:306–310. doi:10.1016/j.wneu.2015.11.075
6. Lindner A, Kofler M, Rass V, et al. Early predictors for infectious complications in patients with spontaneous intracerebral hemorrhage and their impact on outcome. Front Neurol. 2019;10:817. doi:10.3389/fneur.2019.00817
7. Grossmann I, Rodriguez K, Soni M, et al. Stroke and pneumonia: mechanisms, risk factors, management, and prevention. Cureus. 2021;13(11):e19912. doi:10.7759/cureus.19912
8. Westendorp WF, Vermeij JD, Zock E, et al. The Preventive Antibiotics in Stroke Study (PASS): a pragmatic randomised open-label masked endpoint clinical trial. Lancet. 2015;385(9977):1519–1526. doi:10.1016/s0140-6736(14)62456-9
9. Vermeij JD, Westendorp WF, Dippel DW, van de Beek D, Nederkoorn PJ. Antibiotic therapy for preventing infections in people with acute stroke. Cochrane Database Syst Rev. 2018;1(1):Cd008530. doi:10.1002/14651858.CD008530.pub3
10. Meisel A. Preventive antibiotic therapy in stroke: PASSed away? Lancet. 2015;385(9977):1486–1487. doi:10.1016/s0140-6736(15)60076-9
11. Rae N, Chalmers JD. Antibiotic prophylaxis is ineffective in preventing pneumonia post-stroke. J R Coll Physicians Edinb. 2015;45(4):276–277. doi:10.4997/jrcpe.2015.405
12. Binkowska AM, Michalak G, Słotwiński R. Current views on the mechanisms of immune responses to trauma and infection. Cent Eur J Immunol. 2015;40(2):206–216. doi:10.5114/ceji.2015.52835
13. Zhao G, Chen Y, Gu Y, Xia X. The clinical value of nutritional and inflammatory indicators in predicting pneumonia among patients with intracerebral hemorrhage. Sci Rep. 2024;14(1):16171. doi:10.1038/s41598-024-67227-y
14. Hagen M, Sembill JA, Sprügel MI, et al. Systemic inflammatory response syndrome and long-term outcome after intracerebral hemorrhage. Neurol Neuroimmunol Neuroinflamm. 2019;6(5):e588. doi:10.1212/nxi.0000000000000588
15. Wang RH, Wen WX, Jiang ZP, et al. The clinical value of neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), platelet-to-lymphocyte ratio (PLR) and systemic inflammation response index (SIRI) for predicting the occurrence and severity of pneumonia in patients with intracerebral hemorrhage. Front Immunol. 2023;14:1115031. doi:10.3389/fimmu.2023.1115031
16. Luo S, Yang WS, Shen YQ, et al. The clinical value of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and D-dimer-to-fibrinogen ratio for predicting pneumonia and poor outcomes in patients with acute intracerebral hemorrhage. Front Immunol. 2022;13:1037255. doi:10.3389/fimmu.2022.1037255
17. Zhang H, Wu T, Tian X, Lyu P, Wang J, Cao Y. High neutrophil percentage-to-albumin ratio can predict occurrence of stroke-associated infection. Front Neurol. 2021;12:705790. doi:10.3389/fneur.2021.705790
18. Peng Y, Xue Y, Wang J, et al. Association between neutrophil-to-albumin ratio and mortality in patients with cardiogenic shock: a retrospective cohort study. BMJ Open. 2020;10(10):e039860. doi:10.1136/bmjopen-2020-039860
19. Xie H, Jia P, Wei L, et al. Evaluation and validation of neutrophil to albumin ratio as a promising prognostic marker for all-cause mortality in patients with cancer: a multicenter cohort study. Nutrition. 2024;121:112365. doi:10.1016/j.nut.2024.112365
20. Zhang X, Zhang S, Wang C, Liu R, Li A. High neutrophil-to-albumin ratio predicts postoperative pneumonia in aneurysmal subarachnoid hemorrhage. Front Neurol. 2022;13:840858. doi:10.3389/fneur.2022.840858
21. Bao B, Xu S, Sun P, Zheng L. Neutrophil to albumin ratio: a biomarker in non-alcoholic fatty liver disease and with liver fibrosis. Front Nutr. 2024;11:1368459. doi:10.3389/fnut.2024.1368459
22. Li R, Sun Z, Song S, et al. NARFIB: a novel prognostic score based on the neutrophil-to-albumin ratio and fibrinogen can predict the prognosis of gastrointestinal stromal tumors. Cancer Manag Res. 2020;12:11183–11190. doi:10.2147/cmar.S281375
23. Smith CJ, Kishore AK, Vail A, et al. Diagnosis of stroke-associated pneumonia: recommendations from the pneumonia in stroke consensus group. Stroke. 2015;46(8):2335–2340. doi:10.1161/strokeaha.115.009617
24. Heus P, Reitsma JB, Collins GS, et al. Transparent reporting of multivariable prediction models in journal and conference abstracts: TRIPOD for abstracts. Ann Intern Med. 2020;173(1):42–47. doi:10.7326/m20-0193
25. Patzer RE, Kaji AH, Fong Y. TRIPOD reporting guidelines for diagnostic and prognostic studies. JAMA Surg. 2021;156(7):675–676. doi:10.1001/jamasurg.2021.0537
26. Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. Lancet. 2017;389(10069):655–666. doi:10.1016/s0140-6736(16)30668-7
27. Zhang X, Zhang S, Wang C, Li A. Neutrophil-to-albumin ratio as a novel marker predicting unfavorable outcome in aneurysmal subarachnoid hemorrhage. J Clin Neurosci. 2022;99:282–288. doi:10.1016/j.jocn.2022.03.027
28. Chen Z, Xie D, Li Y, et al. Neutrophil albumin ratio is associated with all-cause mortality in stroke patients: a retrospective database study. Int J Gen Med. 2022;15:1–9. doi:10.2147/ijgm.S323114
29. Lv XN, Shen YQ, Li ZQ, et al. Neutrophil percentage to albumin ratio is associated with stroke-associated pneumonia and poor outcome in patients with spontaneous intracerebral hemorrhage. Front Immunol. 2023;14:1173718. doi:10.3389/fimmu.2023.1173718
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knockdown of LCN2 Attenuates Brain Injury After Intracerebral Hemorrhage via Suppressing Pyroptosis
Zhao Y, Xiao Q, Sun T, Yu H, Luo M
Neuropsychiatric Disease and Treatment 2024, 20:83-99
Published Date: 17 January 2024
A Novel Nomogram for Predicting the Risk of Pneumonia After Intracerebral Hemorrhage
Sun Y, Zhang L, Huang B, He Q, Hu B
Journal of Inflammation Research 2025, 18:1333-1351
Published Date: 30 January 2025
Coagulation and Inflammatory Indicators in Pneumonia Patients with Venous Thromboembolism: A Propensity-Score Matching Study
Liu Y, Guo B, Meng Z, Fan Y, Xie Y, Gao L, Ma R
Journal of Inflammation Research 2025, 18:5627-5635
Published Date: 25 April 2025
Impact of Beta-Blockers on Pneumonia, Mortality and Functional Outcomes of Patients with Intracerebral Hemorrhage-A Retrospective Multicenter Study
Gao B, Wang A, Zhang X, Zhang J, Ju Y, Zhao X, Wang W
Journal of Inflammation Research 2025, 18:9355-9364
Published Date: 17 July 2025
Neutrophil Percentage-to-Albumin Ratio is Associated with Functional Outcome, Hematoma Clearance, and Peak Perihematomal Edema in Supratentorial Intracerebral Hemorrhage
Dong W, Li Y, Guan Q, Ma F, Xing W, Chen H, Zhang R, Sui B, Zhao X, Ji R
Journal of Inflammation Research 2026, 19:581386
Published Date: 12 March 2026