Back to Journals » Clinical Interventions in Aging » Volume 19
Influence of Knee Osteoarthritis Severity, Knee Pain, and Depression on Physical Function: A Cross-Sectional Study
Authors Sonobe T ![]() , Otani K
, Otani K ![]() , Sekiguchi M, Otoshi K, Nikaido T
, Sekiguchi M, Otoshi K, Nikaido T ![]() , Konno S, Matsumoto Y
, Konno S, Matsumoto Y
Received 9 June 2024
Accepted for publication 25 September 2024
Published 5 October 2024 Volume 2024:19 Pages 1653—1662
DOI https://doi.org/10.2147/CIA.S470473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Tatsuru Sonobe,1 Koji Otani,1 Miho Sekiguchi,1 Kenichi Otoshi,2 Takuya Nikaido,1 Shinichi Konno,1 Yoshihiro Matsumoto1
1Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine, Fukushima, 960-1295, Japan; 2Department of Sports Medicine, Fukushima Medical University School of Medicine, Fukushima, 960-1295, Japan
Correspondence: Koji Otani, Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine, 1 hikarigaoka, Fukushima-shi, Fukushima, 960-1295, Japan, Tel +81-24-547-1276, Fax +81-24-548-5505, Email [email protected]
Purpose: Decreased physical function with increasing life expectancy is a public health concern worldwide. Knee osteoarthritis (KOA) is considered one of the primary illnesses causing decreased physical function. Depression affects decreased physical function and is closely related to knee pain in KOA. However, the effect of these interacting factors on physical function is not clear.
Patients and Methods: We conducted a cross-sectional analysis of the baseline data of 1106 subjects of the 2009 Locomotive Syndrome and Health Outcome in Aizu Cohort Study (LOHAS). We determined the association between their Timed Up and Go test (TUG) scores and radiographic KOA, knee pain, and depression in a multivariate analysis.
Results: Severe knee pain was significantly associated with decreased physical function (the odds ratio [OR] was 2.13, 95% confidence interval [CI]: 1.32– 4.89), as was depression (OR 2.64, 95% CI 1.61– 4.33). Only Kellgren-Lawrence (KL) grade 4 was significantly associated with decreased physical function in the radiographic KOA severity (OR 6.58, 95% CI 1.75– 24.68).
Conclusion: Severe knee pain and depression were significantly associated with decreased physical function, but not radiographic KOA severity except for KL grade 4. The limitations of using radiographic KOA severity alone as the indicator of assessment for physical function were suggested. When assessing decreased physical function, the clinical focus tends to be on radiographic KOA severity, but it is important to consider the patient’s knee pain and psychological factors.
Keywords: knee osteoarthritis, knee pain, physical function, depression, aging, TUG test
Introduction
Disability is conceptualized by the World Health Organization (WHO) International Classification of Functioning, Disability and Health (ICF). A health condition (eg, arthritis) can impair body functions and structures (eg, joints), limit activities (eg, reduced mobility) and restrict participation (eg, reduced social engagement).1 Disability contributes to increased healthcare costs2 and mortality3 and a decline in quality of life (QOL),4 especially among the elderly. One of the frequently reported functional limitations among older people is decreased physical function.5 Poor physical functioning is associated with total mortality,6 increased healthcare costs,7 and adverse health outcomes.8 Decreased physical function in combination with increasing life expectancy is a worldwide public health problem that needs to be solved.9
Knee osteoarthritis (KOA) is a common musculoskeletal disorder in the elderly. It causes significant loss of joint function,10 with pain, inflammation, and dysfunction due to progressive articular cartilage degeneration11 and synovitis.12 The global prevalence of KOA is predicted to reach 40% by 2025.13 KOA-related functional decline leads to decreased mobility, limited activities of daily living (ADLs),14 and an increased frequency of limited participation in social and community activities.15 Difficulties in social participation can lead to social isolation and heightened economic burdens.16
KOA is often diagnosed basis of subjective symptoms such as pain, stiffness, limited joint range of motion and crepitus, and plain radiographs such as osteophyte formation and narrowing of joint space.17 Based on the European League Against Rheumatism (EULAR) evidence-based recommendations,18 the most typical symptom of KOA is pain. In patients with symptomatic KOA, knee symptoms such as knee pain and physical function assessed by TUG score are negatively correlated.19 However, musculoskeletal pain and depression interact with each other, with knee pain also being closely related to depression.20–22 Furthermore, depression itself also reduces physical function in adults,23 but there are few quantitative evaluation reports.24 As regards imaging findings, the association between radiographic KOA itself and physical function assessed by TUG score has been described in two cross-sectional studies, one of which found that radiographic KOA severity is not associated with physical function25 and the other of which reported a positive correlation.26 Thus, this association remains controversial. However, these studies did not evaluate interacting factors that may affect physical function, such as pain or depression. The purpose of this study was to clarify how knee pain, a common symptom of KOA, radiographic KOA severity, and depression affect decreased physical function.
Material and Methods
Participants
In this study, we analyzed data from the Aizu Cohort Study on Locomotive Syndrome and Health Outcomes (LOHAS). LOHAS is a cohort study to assess the risk of cardiovascular disease, QOL, healthcare costs and mortality attributable to locomotor dysfunction.27 Cohort participants were recruited from residents between 40 and 80 years old who received regular health check-ups conducted by local government each year between 2008 and 2010 in Minami-Aizu Town and Tadami Town in Fukushima Prefecture, Japan. Musculoskeletal examination included physical examination of the cervical spine, lumbar spine, upper and lower limbs and assessment of physical functions such as grip strength, and Timed Up and Go (TUG) test. A self-administered questionnaire survey was also conducted. This cross-sectional analysis used data from the 2009 LOHAS baseline survey, which included 3790 subjects. Previously, we have reported using the same database.28 The 1,484 subjects who requested to be examined underwent plane radiography of both knee joints in the standing position and a TUG test. Twenty-six subjects with a history of knee surgery, trauma, rheumatoid arthritis, or joint disease other than KOA were excluded from this study. Another 352 subjects with missing data were also excluded from the study. Ultimately, 1,106 subjects were included in the present analyses (Figure 1).
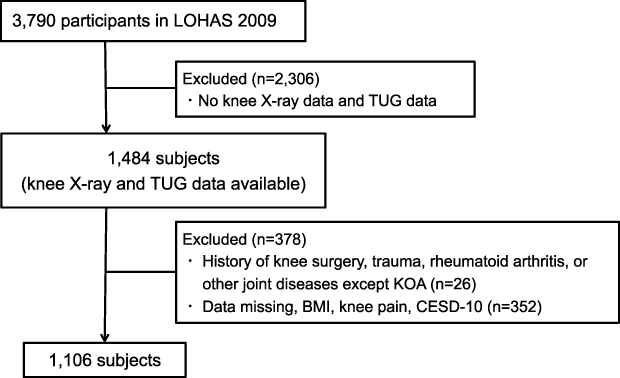 |
Figure 1 Flowchart for the study. A total of 1,106 subjects were included in the analysis. LOHAS: the Locomotive Syndrome and Health Outcome in Aizu Cohort Study; KOA: knee osteoarthritis; BMI: body mass index; CESD-10: Center of Epidemiologic Studies Depression Scale-10. |
Ethical Consideration
We complied with the Declaration of Helsinki and provided written informed consent for the use of the collected data to all subjects. The present study was approved by the Research Ethics Committee of Fukushima Medical University (No. 673).
Data Collection
Knee Symptoms
Knee pain is based on subjects’ self-administered questionnaire reports, the degree of knee pain was described on a six-point Likert scale (0 points: complete absence of pain; 1 point: very slight pain; 2 points: slight pain; 3 points: moderate pain; 4 points: very painful; 5 points: severe pain). For the purposes of the present analyses, knee pain was classified 0 points as no pain, 1 or 2 points as mild pain, 3 points as moderate pain, and 4 or 5 points as severe pain.
Radiological Assessment
As in our previous reports,28 the radiographic KOA severity was assessed by two well-trained knee surgeons with more than 20 years’ experience and more than 200 cases per year based on the Kellgren-Lawrence classification (ie KL grade).29 In the present study, the KL grades on the subject’s more severe side were used.
Psychological Factors
The CESD-10 score was used as the psychological factors questionnaire in LOHAS. The CESD-10 is a short form of the Center of Epidemiologic Studies Depression Scale30 as a 10-item questionnaire that provides a simple assessment of depression which has been translated and validated into Japanese;31 scores of ≥10 points indicate the presence of clinical depression.32
Physical Function
We assessed the subjects’ physical function by the TUG test. The TUG score is calculated from the time taken to rise from a chair without armrests, walk 3 meters, return to the chair, and sit down. The TUG test is a performance-based measure recommended by the Osteoarthritis Research Society International (OARSI) to assess physical function in individuals diagnosed with KOA.33 Although there are various reports on cut-off values for TUG time,34–36 we defined normal physical function as <10 and decreased physical function as ≥10 sec, which is considered a general indication of physical function.36
Statistical Analysis
The data from 1,106 subjects with complete data were included in the primary analysis.
Descriptive statistics were calculated for the baseline characteristics of subjects, with continuous data presented as means and standard deviations. Binomial or categorical data were presented as proportions. The χ2-test was used to compare categorical variables. Univariate and multivariate logistic analyses were conducted to examine the association between mobility and each factor, with the categorical variable TUG score as the dependent variable. Categorical variables of age, gender, BMI, knee pain, CESD-10 and radiographic KOA severity were included in the analysis as independent variables, regardless of the results of the univariate analysis, as they were considered clinically important. The variance inflation factor (VIF) indicates multicollinearity in multivariate analysis and expresses the correlation between independent variables. VIF ≥10 was considered to be multicollinearity.37 The odds ratios (ORs) and 95% confidence intervals (CIs) were obtained from logistic analysis. All tests were two-sided, and probability (p)-values <0.05 were considered statistically significant. The sample size required for logistic regression analysis is proposed to be n= 10k/p (K: number of terms in the independent variables, p: proportion of the smaller of the two groups of dependent variables).38 The sample size required for this study was n=10*6/0.127=472.4. The data we used in this study of 1106 individuals was sufficient for the required sample size. All statistical analyses were conducted using JMP PRO 16 (SAS, Cary, NC, USA).
Results
The Subjects’ Characteristics
We summarized the characteristics of the 1,106 subjects and 352 excluded from the analysis due to missing data in Table 1. The subjects included in present analysis tended to be older and more male compared to the missing data subjects.
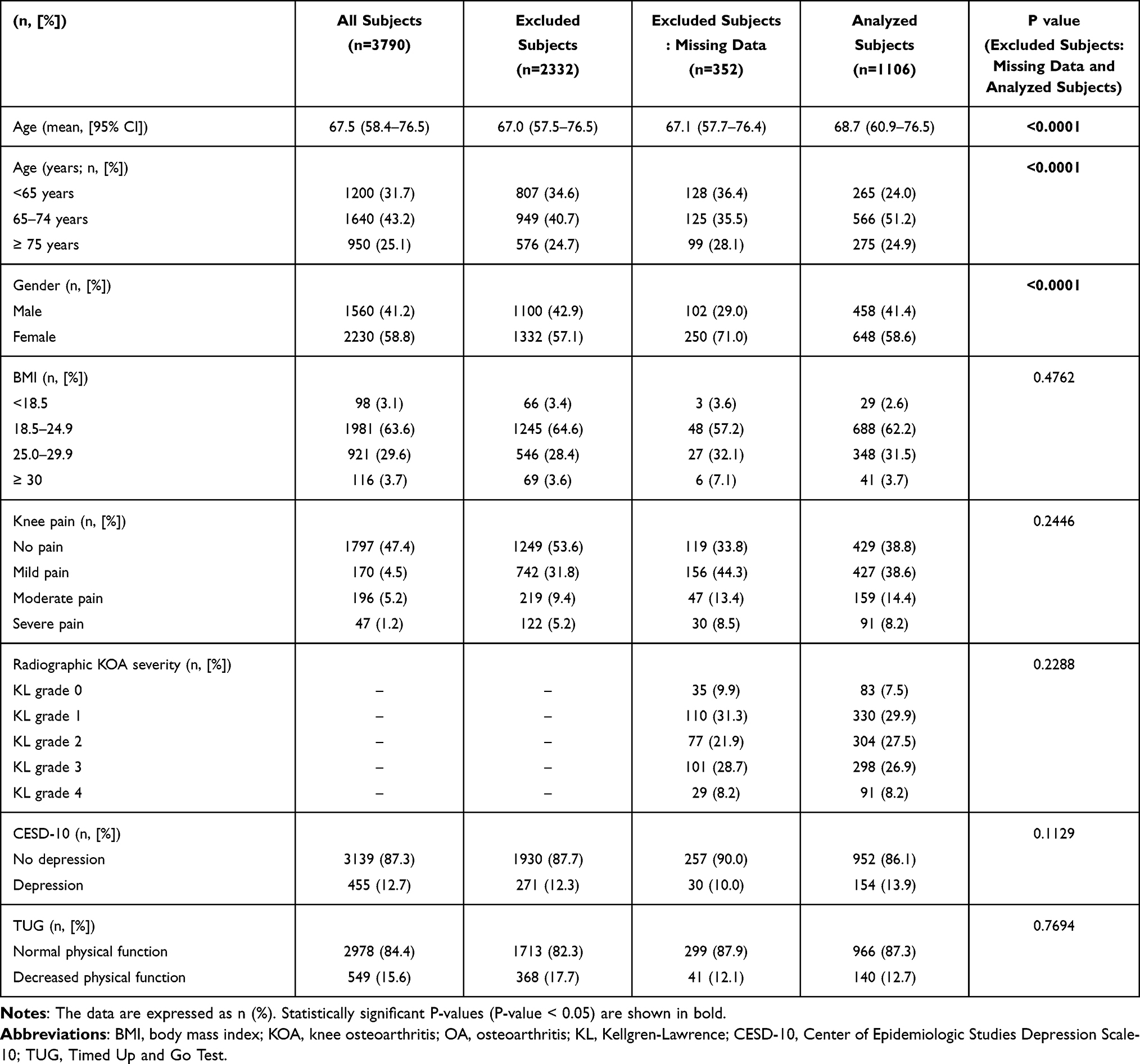 |
Table 1 Subject Characteristics |
Relationship Between Subjects’ Depression and Knee Pain
Table 2 shows the present data concerning the relationship between depression and knee pain. Depression was significantly associated with the severity of the subjects’ knee pain.
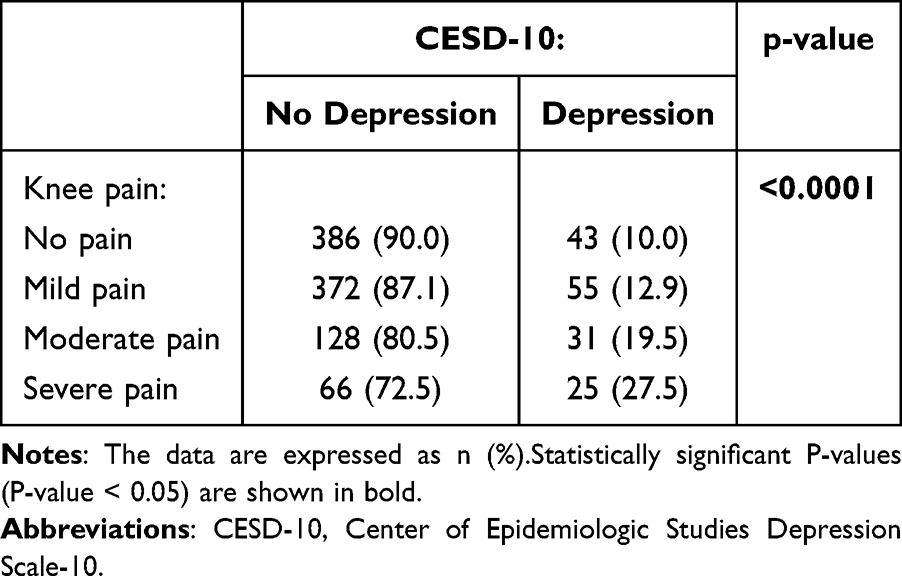 |
Table 2 Association Between CESD-10 and Knee Pain |
Univariate Analysis: Association Between TUG Score and Confounders
We found significant associations with TUG score in subjects’ age 65–74 years (OR, 2.76; 95% CI, 1.33–5.69), age ≥75 years (OR, 11.88; 95% CI, 8.82–24.24), moderate knee pain (OR, 2.81; 95% CI, 1.66–4.76), severe knee pain (OR, 4.90; 95% CI, 2.77–8.67), KL grade 3 (OR, 4.38; 95% CI, 1.32–14.50), KL grade 4 (OR, 17.45; 95% CI, 5.12–59.53), and depression (OR, 2.73; 95% CI, 1.79–4.15) in univariate analysis (Table 3).
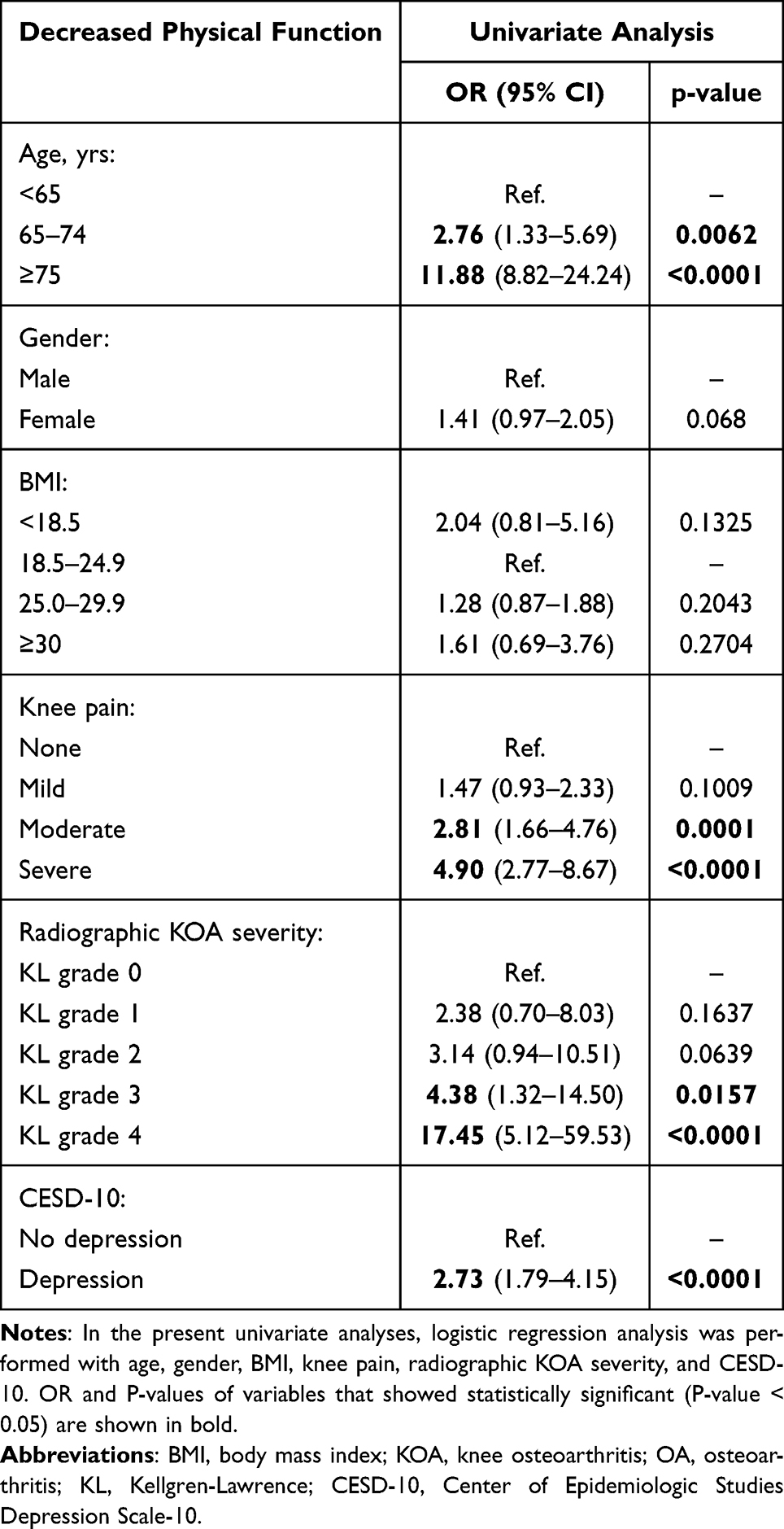 |
Table 3 Univariate Analysis of TUG |
Multivariate Analysis: Association Between TUG Score and Confounders
We summarized the relationships between TUG score and confounders (age, gender, BMI, knee pain, KOA category, and CESD-10) in Table 4. Compared to subjects aged <65 years, the OR was 2.13 times higher in those aged 65–74 years (95% CI, 1.00–4.52) and 8.93 times higher in subjects ≥75 years old (95% CI, 4.18–19.05). Significant associations with decreased physical function were found in severe pain (OR, 2.13; 95% CI, 1.08–4.21). Depression was also significantly associated with decreased physical function (OR, 2.64; 95% CI, 1.61–4.33). Only KL grade 4 was significantly associated with decreased physical function in the radiographic KOA severity (OR 6.58, 95% CI 1.75–24.68). Physical function was independently associated with age, knee pain and depression, but not with the radiographic KOA severity except for KL grade 4. We determined that there was no multicollinearity between confounders in this study because the VIF of each confounder was quite low.
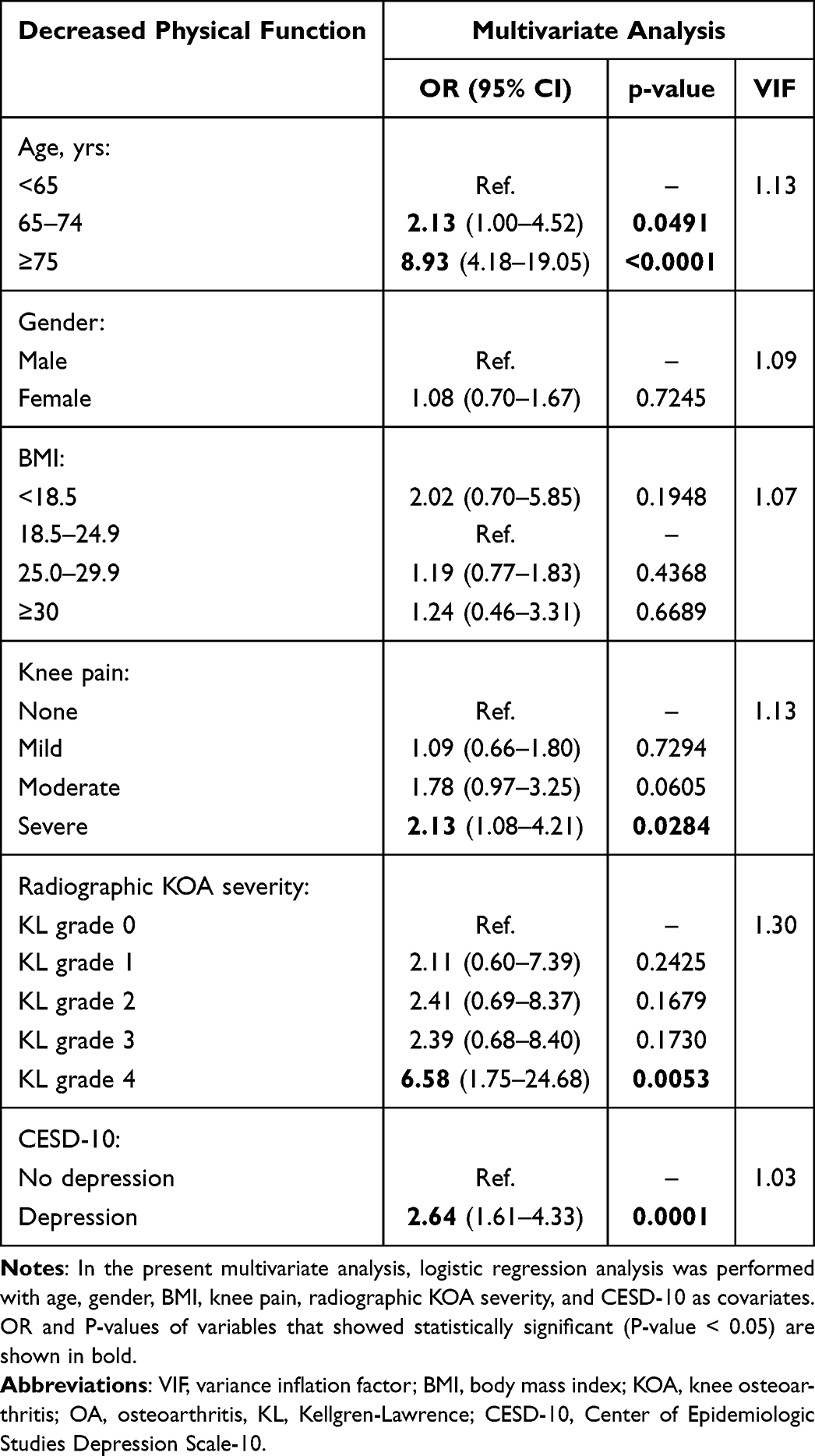 |
Table 4 Multivariate Analysis of TUG |
Discussion
The results of our multivariate analyses demonstrated that age, severe knee pain, and depression were significantly associated with decreased physical function, while radiographic KOA severity was not significantly associated with decreased physical function except for KL grade 4.
Symptomatic KOA has been thought to cause decreased physical function and a decline in ADLs.14 Depression affects decreased physical function,23 but there are a few quantitative evaluation reports.24 In addition, depression is closely related to knee pain in KOA.20–22 We analyzed the association of knee pain, a common symptom of KOA, radiographic KOA severity, and depression with decreased physical function. To the best of our knowledge, this investigation is the first to analyze the impact of KOA severity based on imaging findings and degree of knee pain on decreased physical function, taking psychological factors into account. Our results corroborate and extend the findings of previous studies.
Our analyses indicated that age ≥65 years was significantly associated with decreased mobility. Prior research found that increasing age is associated with decreased physical function,39 which is consistent with our results. Lower extremity muscle strength and one’s usual and maximum walking speeds are age-dependent mobility abilities.40 A decrease in physical function with age is plausible, and prevention and countermeasures are necessary. Identifying factors other than age that are associated with decreased physical function is important.
Our analyses revealed that decreased physical function was significantly associated with severe knee pain. Among the elderly, knee pain is considered a major cause of physical disability, including physical function and ADL impairment,41 and the present results are consistent with this understanding. Pain associated with OA causes reduced use of the affected limb or joint, muscle weakness, and gradual develop joint mobility disorders,42 resulting in decreased physical function.43 Accurate knee pain assessment is necessary as an indicator of physical function in KOA.
Our analyses also demonstrated an interesting significant association between depression and decreased mobility. Depression has been shown to affect motor limitations and accelerate physical disability,23 which is consistent with our results. This may be explained by the effects of depression itself, since psychological distress leads to the avoidance of daily activities, resulting in muscle weakness;44 hence, the association between knee pain and depression. Depression has been reported to be a modifier of knee pain and is strongly related to knee pain.45 The present χ2 analysis also identified a significant association between depression and knee pain. We speculate that knee pain may be an intermediate factor between depression and decreased mobility. Rather than depression directly decreasing mobility, it may exacerbate knee pain, resulting in the avoidance of daily activities and decreased physical function. The assessment of depression in KOA in clinical practice has received little attention, but the results of this study indicate that it is an important indicator of physical function.
Our present finding that radiographic KOA severity except for KL grade 4 was not significantly associated with decreased physical function directly. A positive correlation between TUG scores and radiographic KOA severity had previously been reported.26 On the other hand, another investigation found no significant differences in TUG scores among subgroups of patients classified based on their radiographic KOA severity, although the patients with the most severe KOA (KL-4) tended to exhibit the worst performance.25 Both studies performed univariate analyses of KL grade and TUG score and did not consider the influence of knee pain or psychological factors. In other words, the association between severe OA on imaging findings and decreased physical function may be confounded by other factors. Patients with KOA included in KL grade 4 have been shown to have poorer physical function due to restricted limited joint range of motion, altered lower extremity alignment, and more severe synovitis, compared to patients with less severe KOA.46,47 In KL grade 4, the morphological changes have an impact on decreased physical function, as suggested by the present study. However, the radiographic KOA severity below KL-3 was not significantly associated with decreased physical function in this study, which limits the ability to assess decreased physical function based on the radiographic severity alone. National Institute for Health and Care Excellence (NICE) guidelines recommended that imaging should not be routinely used to diagnose osteoarthritis unless some atypical features or features suggest an alternative or additional diagnosis.48 The severity of imaging findings is only one indicator, and it is important to assess clinical symptoms and physical findings correctly.
One of the diagnostic criteria for KOA in clinical practice is its severity on imaging findings, but knee pain and psychological factors related to decreased physical function must also be assessed. Our present findings demonstrate the limitations of assessing physical function solely on the radiographic KOA severity, which tends to be the focus of clinical attention. When assessing the decreased physical function, it is necessary to take into account the patient’s knee pain and psychological factors, rather than being restricted to radiographic KOA severity. In addition, future intervention studies on knee pain and psychological factors are needed to validate these findings.
We must address several study limitations. (i) As this study was a cross-sectional analysis, a causal relationship cannot be definitively determined. (ii) There may have been a measurement error in measuring TUG times. Previous studies have reported a measurement error of 0.22 seconds.49 The measurement error in a TUG assessment is greater in frail older adults, and the longer it takes to perform the TUG test, the greater the variability.50 (iii) In our analyses, we were unable to include low socioeconomic status, comorbidities, or physiological factors (ie, inflammation or vitamin D deficiency), each of which is commonly considered a risk factor for decreased mobility.51 (iv) Plain radiographs of the knee were optional, which may have resulted in a high number of symptomatic subjects participating, possibly biasing in the study.
Conclusions
In conclusion, our findings demonstrate that age ≥65 years, severe knee pain, and depression were significantly associated with decreased mobility, but not radiographic KOA severity except for KL grade 4. The limitations of using radiographic KOA severity alone as the indicator of assessment for physical function were suggested. When assessing decreased physical function, the clinical focus tends to be on radiographic KOA severity, but it is important to consider the patient’s knee pain and psychological factors.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank the Japanese Orthopaedic Association (JOA-Subsidized Science Project Research 2022-1). We would like to thank the staff of the Tadami and Minamiaizu Town Office, and Institute for Health Outcomes and Process Evaluation Research for their help with participant recruitment and data acquisition. The authors also thank all of the subjects who agreed to participate in this study.
Funding
This research did not receive any specific grant.
Disclosure
The author reports no conflicts of interest in this work. This paper has a shared database with another paper published in BMC at: https://bmcmusculoskeletdisord.biomedcentral.com/articles/10.1186/s12891-024-07421-1. This paper has been uploaded to Research Square as a preprint: https://www.researchsquare.com/article/rs-4010731/v1.
References
1. World Health Organisation. World Bank. World Report on Disability. Geneva, Switzerland: World Health Organisation; 2011.
2. Fried LP, Ferrucci L, Darer J, et al. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol Biol Sci Med Sci. 2004;59:255–263. doi:10.1093/gerona/59.3.m255
3. Mehta KM, Pierluissi E, Boscardin WJ, et al. A clinical index to stratify hospitalized older adults according to risk for new-onset disability. J Am Geriatr Soc. 2011;59:1206–1216. doi:10.1111/j.1532-5415.2011.03409.x
4. Motl RW, McAuley E. Physical activity, disability, and quality of life in older adults. Phys Med Rehabil Clin N Am. 2010;21:299–308. doi:10.1016/j.pmr.2009.12.006
5. Prynn JE, Polack S, Mactaggart I, et al. Disability among older people: analysis of data from disability surveys in six low- and middle-income countries. Int J Environ Res Public Health. 2021;18(13):6962. doi:10.3390/ijerph18136962
6. Andrasfay T. Changes in Physical Functioning as Short-Term Predictors of Mortality. J Gerontol B Psychol Sci Soc Sci. 2020;75(3):630–639. doi:10.1093/geronb/gby133
7. Falck RS, Percival AG, Tai D, et al. International depiction of the cost of functional Independence limitations among older adults living in the community: a systematic review and cost-of-impairment study. BMC Geriatr. 2022;22(1):815. doi:10.1186/s12877-022-03466-w
8. Fried TR, Bradley EH, Williams CS, Tinetti ME. Functional disability and health care expenditures for older persons. Arch Intern Med. 2001;161(21):2602–2607. doi:10.1001/archinte.161.21.2602
9. Wan He DG, Kowal P. An Aging World: 2015. Washington DC: International Population Reports; 2016.
10. Benito MJ, Veale DJ, FitzGerald O, van den Berg WB, Bresnihan B. Synovial tissue inflammation in early and late osteoarthritis. Ann Rheum Dis. 2005;64:1263–1267. doi:10.1136/ard.2004.025270
11. Hinman RS, Bennell KL, Metcalf BR, et al. Balance impairments in individuals with symptomatic knee osteoarthritis: a comparison with matched controls using clinical tests. Rheumatology. 2002;41(12):1388–1394. doi:10.1093/rheumatology/41.12.1388
12. Cecchi F, Mannoni A, Molino-Lova R, et al. Epidemiology of hip and knee pain in a community-based sample of Italian persons aged 65 and older. Osteoarthritis Cartilage. 2008;16(9):1039–1046. doi:10.1016/j.joca.2008.01.008
13. Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):646–656. PMID: 14710506; PMCID: PMC2572542.
14. Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice. Lancet. 2011;377(9783):2115–2126. doi:10.1016/S0140-6736(11)60243-2
15. Clynes MA, Jameson KA, Edwards MH, et al. Impact of osteoarthritis on activities of daily living: does joint site matter? Aging Clin Exp Res. 2019;31(8):1049–1056. doi:10.1007/s40520-019-01163-0
16. Steultjens MP, Dekker J, Bijlsma JW. Avoidance of activity and disability in patients with osteoarthritis of the knee: the mediating role of muscle strength. Arthritis Rheum. 2002;46(7):1784–1788. doi:10.1002/art.10383
17. Michael JW, Schlüter-Brust KU, Eysel P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch Arztebl Int. 2010;107(9):152–162. doi:10.3238/arztebl.2010.0152
18. Zhang W, Doherty M, Peat G, et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann Rheum Dis. 2010;69(3):483–489. doi:10.1136/ard.2009.113100
19. Sabirli F, Paker N, Bugdayci D. The relationship between knee injury and osteoarthritis outcome score (KOOS) and timed up and go test in patients with symptomatic knee osteoarthritis. Rheumatol Int. 2013;33(10):2691–2694. doi:10.1007/s00296-012-2512-3
20. Zheng S, Tu L, Cicuttini F, et al. Depression in patients with knee osteoarthritis: risk factors and associations with joint symptoms. BMC Musculoskelet Disord. 2021;22(1):40. doi:10.1186/s12891-020-03875-1
21. Yao C, Zhang Y, Lu P, et al. Exploring the bidirectional relationship between pain and mental disorders: a comprehensive Mendelian randomization study. J Headache Pain. 2023;24(1):82. doi:10.1186/s10194-023-01612-2
22. Von Korff M, Simon G. The relationship between pain and depression. Br J Psychiatry. 1996;30:101–108. PMID: 8864155. doi:10.1192/S0007125000298474
23. Milaneschi Y, Penninx BW. Depression in older persons with mobility limitations. Curr Pharm Des. 2014;20(19):3114–3118. doi:10.2174/13816128113196660060
24. Burton C, McKinstry B, Szentagotai Tătar A, et al. Activity monitoring in patients with depression: a systematic review. J Affect Disord. 2013;145(1):21–28. doi:10.1016/j.jad.2012.07.001
25. Liikavainio T, Lyytinen T, Tyrväinen E, et al. Physical function and properties of quadriceps femoris muscle in men with knee osteoarthritis. Arch Phys Med Rehabil. 2008;89(11):2185–2194. doi:10.1016/j.apmr.2008.04.012
26. Özden F, Nadiye Karaman Ö, Tuğay N, et al. The relationship of radiographic findings with pain, function, and quality of life in patients with knee osteoarthritis. J Clin Orthop Trauma. 2020;11(Suppl 4):S512–S517. doi:10.1016/j.jcot.2020.04.006
27. Otani K, Takegami M, Fukumori N, et al. Locomotor dysfunction and risk of cardiovascular disease, quality of life, and medical costs: design of the locomotive syndrome and health outcome in aizu cohort study (LOHAS) and baseline characteristics of the study population. J Orthop Sci. 2012;17:261–271. doi:10.1007/s00776-012-0200-5
28. Sonobe T, Otani K, Sekiguchi M, et al. Radiographic knee osteoarthritis severity has no impact on fall risk: the locomotive syndrome and health outcomes in the aizu cohort study (LOHAS): a cross-sectional study. BMC Musculoskelet Disord. 2024;25(1):298. doi:10.1186/s12891-024-07421-1
29. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494–502. doi:10.1136/ard.16.4.494
30. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. doi:10.1177/014662167700100306
31. Shima S, Shikano T, Kitamura T, et al. New self-rating scale for depression. Clin Psychiatry. 1985;27:717–723.
32. Andresen EM, Malmgren JA, Cater WB, et al. Screening for depression in well older adults: evaluation of short form of the CES-D (center for epidemiologic studies depression scale). Am J Prev Med. 1994;10:77–84. PMID: 8037935. doi:10.1016/S0749-3797(18)30622-6
33. Dobson F, Hinman RS, Roos EM, et al. OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthritis Cartilage. 2013;21(8):1042–1052. doi:10.1016/j.joca.2013.05.002
34. Choo PL, Tou NX, Jun Pang BW, et al. Timed up and go (TUG) reference values and predictive cutoffs for fall risk and disability in Singaporean community-dwelling adults: Yishun cross-sectional study and Singapore longitudinal aging study. J Am Med Dir Assoc. 2021;22(8):1640–1645. doi:10.1016/j.jamda.2021.03.002
35. Beauchet O, Fantino B, Allali G, et al. Timed up and go test and risk of falls in older adults: a systematic review. J Nutr Health Aging. 2011;15(10):933–938. doi:10.1007/s12603-011-0062-0
36. Steffen TM, Hacker TA, Mollinger L. Age- and gender-related test performance in community-dwelling elderly people: six-minute walk test, berg balance scale, timed up & go test, and gait speeds. Phys Ther. 2002;82(2):128–137. doi:10.1093/ptj/82.2.128
37. Marquardt DW. Generalized inverses, ridge regression, biased linear estimation, and nonlinear estimation. Technometrics. 1970;12:591–612. doi:10.2307/1267205
38. Peduzzi P, Concato J, Kemper E, et al. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/s0895-4356(96)00236-3
39. Yamada K, Yamaguchi S, Ito YM, et al. Factors associated with mobility decrease leading to disability: a cross-sectional nationwide study in Japan, with results from 8681 adults aged 20-89 years. BMC Geriatr. 2021;21(1):651. doi:10.1186/s12877-021-02600-4
40. Bohannon RW. Comfortable and maximum walking speed of adults aged 20-79 years: reference values and determinants. Age Ageing. 1997;26(1):15–19. doi:10.1093/ageing/26.1.15
41. Felson DT. Clinical practice. Osteoarthritis of the knee. N Engl J Med. 2006;354(8):841–848. doi:10.1056/NEJMcp051726
42. Doré AL, Golightly YM, Mercer VS, et al. Lower-extremity osteoarthritis and the risk of falls in a community-based longitudinal study of adults with and without osteoarthritis. Arthritis Care Res. 2015;67:633–639. doi:10.1002/acr.22499
43. Focht BC. Effectiveness of exercise interventions in reducing pain symptoms among older adults with knee osteoarthritis: a review. J Aging Phys Act. 2006;14(2):212–235. doi:10.1123/japa.14.2.212
44. Rogers AH, Farris SG. A meta-analysis of the associations of elements of the fear-avoidance model of chronic pain with negative affect, depression, anxiety, pain-related disability and pain intensity. Eur J Pain. 2022;26(8):1611–1635. doi:10.1002/ejp.1994
45. Phyomaung PP, Dubowitz J, Cicuttini FM, et al. Are depression, anxiety and poor mental health risk factors for knee pain? A systematic review. BMC Musculoskelet Disord. 2014;15:10. doi:10.1186/1471-2474-15-10
46. Lee SY, Kim BR, Kim SR, et al. The combination of osteoporosis and low lean mass correlates with physical function in end-stage knee osteoarthritis: a retrospective observational study. Medicine. 2022;101(31):e29960. doi:10.1097/MD.0000000000029960
47. Guermazi A, Hayashi D, Roemer F, et al. Severe radiographic knee osteoarthritis--does Kellgren and Lawrence grade 4 represent end stage disease? The MOST study. Osteoarthritis Cartilage. 2015;23(9):1499–1505. doi:10.1016/j.joca.2015.04.018
48. NICE guideline [NG226]. UK: osteoarthritis in over 16s: diagnosis and management. Available from: https://www.nice.org.uk/guidance/ng226/.
49. Gautschi OP, Smoll NR, Corniola MV, et al. Validity and reliability of a measurement of objective functional impairment in lumbar degenerative disc disease: the timed up and go (TUG) test. Neurosurgery. 2016;79(2):270–278. doi:10.1227/NEU.0000000000001195
50. Nordin E, Rosendahl E, Lundin-Olsson L. Timed “up & go” test: reliability in older people dependent in activities of daily living – focus on cognitive state. Phys Ther. 2006;86(5):646–655. PMID: 16649889.
51. Yeom HA, Fleury J, Keller C. Risk factors for mobility limitation in community-dwelling older adults: a social ecological perspective. Geriatr Nurs. 2008;29(2):133–140. doi:10.1016/j.gerinurse.2007.07.002
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Spotlight on the Challenges of Depression following Retirement and Opportunities for Interventions
Dang L, Ananthasubramaniam A, Mezuk B
Clinical Interventions in Aging 2022, 17:1037-1056
Published Date: 7 July 2022
Anxiety and Depression Among US Nursing Home Residents with Chronic Obstructive Pulmonary Disease
Osundolire S, Goldberg RJ, Lapane KL
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1867-1882
Published Date: 28 August 2023
Efficacy and Temporal Dynamics of Genicular Nerve Block in Primary and Secondary Knee Osteoarthritis for Pain and Function: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Li Z, Bai Y, Liu C, Gu Y
Journal of Pain Research 2025, 18:3037-3048
Published Date: 17 June 2025
Random Forest Regression May Become the Optimal Regression Model for Osteoarthritis of the Knee in Elderly, in the Context of Embodied Cognition and Psychosomatic Medicine
Ma G, Chen J, Li J, Shi H, Chen Y
Journal of Multidisciplinary Healthcare 2025, 18:4219-4232
Published Date: 26 July 2025