Back to Journals » Nature and Science of Sleep » Volume 17

Psychological Resilience and Sleep Quality Among the Elderly: The Mediating Role of Social Support
Authors Li J ![]() , Zhang J, Hou Y, Cui Y
, Zhang J, Hou Y, Cui Y ![]() , Wang Q, Ouyang A, Cai M, Hua Y
, Wang Q, Ouyang A, Cai M, Hua Y
Received 2 May 2025
Accepted for publication 13 August 2025
Published 3 October 2025 Volume 2025:17 Pages 2469—2483
DOI https://doi.org/10.2147/NSS.S536878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sarah L Appleton
Jiayao Li,1,* Jingyu Zhang,2,* Yingying Hou,3,* Yi Cui,1 Qianqian Wang,1 Anping Ouyang,4 Min Cai,5 Yan Hua1
1Department of Nursing, Air Force Medical University, Xi’an, Shaanxi, People’s Republic of China; 2Department of Cardiology, First Affiliated Hospital of Naval Medical University, Shanghai, People’s Republic of China; 3Department of Hepatobiliary Surgery, Xijing Hospital, Air Force Medical University, Xi’an, Shaanxi, People’s Republic of China; 4Department of Military Medical Psychology, Air Force Medical University, Xi’an, Shaanxi, People’s Republic of China; 5Department of Psychiatry, Xijing Hospital, Air Force Medical University, Xi’an, Shaanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Cai, Department of Psychiatry, Xijing Hospital, Air Force Medical University, Xi’an, Shaanxi, People’s Republic of China, Email [email protected] Yan Hua, Department of Nursing, Air Force Medical University, Xi’an, Shaanxi, People’s Republic of China, Email [email protected]
Objective: This study aims to explore the mediating role of social support among the elderly in the relationship between psychological resilience and sleep quality.
Methods: From December 2024 to March 2025, researchers conducted a questionnaire survey among elderly individuals aged ≥ 65 years in Shaanxi Province and Shanghai Municipality. The Connor-Davidson Resilience Scale, Perceived Social Support Scale, and Pittsburgh Sleep Quality Index (PSQI) were used to assess the psychological resilience, social support, and sleep quality of the elderly. Structural equation modeling was employed to explore the relationships among the variables.
Results: This study included a total of 359 elderly participants, with an average sleep quality score of 12.69 (standard deviation = 4.15), indicating poor sleep quality. Psychological resilience was significantly associated with sleep quality in the elderly (r = − 0.781, p < 0.001). In the model constructed in this study, social support was considered a partial mediating factor in the relationship between psychological resilience and sleep quality among the elderly, with the mediating effect accounting for 33.7% of the total effect (indirect effect β = − 0.070, 95% CI = − 0.108 to − 0.025, p = 0.006).
Conclusion: In the elderly population, psychological resilience and sleep quality are significantly associated, with social support acting as a mediator in this relationship. The above findings provide scientific basis for the formulation of intervention strategies.
Keywords: elderly, psychological resilience, social support, sleep quality, cross-sectional study
Introduction
The World Health Organization (WHO) defines individuals aged 65 and older as elderly, with a significant portion of the elderly population residing in developing countries.1 According to United Nations data, 9.3% of individuals worldwide are 65 years of age or older.2 In China, the population aged 65 and above has reached 190 million, and is projected to reach 400 million by 2050, making it one of the nations with the fastest aging populations.3 With the advancement of technology, increased life expectancy, and declining birth rates leading to a global increase in the elderly population, aging has become a primary challenge in public health.4,5
Sleep participates in regulating the body’s immune system and metabolic processes. It is a crucial behavioral component that influences both mental and physical health and is a significant predictor of a person’s current state of health.6,7 However, sleep problems become increasingly prominent with age. According to surveys, Sleep issues, such as inadequate or excessive sleep duration, affect about 40% of the elderly.8 As they get older, elderly folks eventually get less sleep than young adults and middle-aged adults.9 Additionally, studies reveal that while the time it takes to fall asleep and wake up gradually increases with age, rapid eye movement and slow-wave sleep decrease. This could result in excessive naps, which could cause sleep problems and poor sleep quality in older persons.10,11 Numerous epidemiological and laboratory studies have confirmed that poor sleep quality is not only associated with mortality, mental illness, and cardiovascular disease in older adults, but also leads to fatigue, weakness, and cognitive decline, ultimately affecting their quality of life.12,13 It is clear that improving sleep quality in older adults has become an urgent issue that needs to be addressed.
Psychological resilience is broadly defined as the ability to adapt to stressors, recover from adversity and life crises, and return to normal psychological and social functioning shortly after adverse events.14 The traditional Chinese model of multi-generational households provides emotional support and life care for the elderly, helping to buffer the psychological stress they face when confronted with adversity. However, with the development of the urbanization process, young and middle-aged people are migrating on a large scale to urban areas, and some elderly people may leave their hometowns with their children, creating stressors such as environmental maladjustment and cultural barriers.15 In addition, because they are separated from their loved ones, left-behind elderly are prone to feelings of loneliness and other negative emotions, which often affects their psychological resilience level. Consequently, we discovered that the elderly may experience interpersonal stressors (such as separation from family members) and social/structural stressors (such as financial difficulties and lack of information), which have a certain impact on their psychological resilience. Lazarus and Folkman’s stress and coping theory suggests that in stressful situations, individuals typically conduct cognitive assessments of stress and adopt coping strategies.16 Based on this theory, individuals with high psychological resilience are frequently more proactive in establishing and maintaining support networks, prefer to adopt positive coping strategies such as social support in response to stress, and are more likely to enter a resource gain spiral. As an important part of positive psychology and a personal protective resource. It has been demonstrated that psychological resilience mediates individuals’ sleep quality. For example, one of the common factors affecting sleep quality in different populations such as HIV patients, pregnant women, and the elderly is low psychological resilience.17–19 Previous studies have shown that compared to individuals with high psychological resilience, those with low resilience typically assess stressful tasks as more threatening and exhibit stronger physiological responses to social stress. As a result, corticotropin-releasing hormone (CRH) secretion increases during stressful processes, excessive or prolonged activation of the hypothalamic-pituitary-adrenal (HPA) axis, elevated cortisol secretion levels, suppression of rapid eye movement (REM) sleep, and sleep fragmentation, thereby impairing sleep quality.20 Additionally, low psychological resilience often leads to impaired emotional regulation mechanisms that rely on prefrontal cortex activity, causing individuals to experience insomnia symptoms.21 Apart from psychological factors, the elderly’s health status (such as myopia, pain, etc) may also affect their sleep quality.22 Furthermore, pharmacological interventions (such as orexin receptor antagonists) and non-pharmacological interventions (such as physical exercise and dietary guidance) also have varying degrees of effect on sleep quality in the elderly.23–26 Since sleep quality is a modifiable factor, exploring factors associated with sleep quality to guide behavioral interventions aimed at enhancing the quality of life of older adults is of great significance. Some recent research have examined the factors influencing older persons’ sleep quality and found a substantial association between psychological resilience and sleep quality, but the underlying mechanisms are still unknown. Therefore, this study used CD-RISC and PSQI to measure psychological resilience and sleep quality in the elderly, respectively, and incorporated them into a structural equation model to explore the pathways among the variables.
As older adults age, their cognitive functions decline, their sleep duration shortens, and they are more vulnerable to negative emotions and sleep disorders.27 Good social support is crucial for the elderly. A multidimensional concept, social support is typically categorized into four types: emotional support, instrumental support, informational support, and appraisal support.28,29 Previous studies have shown that older adults who receive good emotional support tend to feel less lonely, have higher subjective well-being, and exhibit shorter sleep latency and higher sleep efficiency.30 Instrumental support refers to providing specific material assistance or practical help, including financial, material, or services. According to the survey, older adults who receive adequate financial support are better able to meet their daily needs, which helps alleviate their psychological distress and insomnia symptoms.31 Good life care services, such as a quiet, temperature- and humidity-controlled sleeping environment, and comfortable bedding and furnishings, can help increase the deep sleep duration in the elderly.32,33 Providing information support, such as popularizing scientific knowledge about sleep or guiding the elderly on their daily routines and dietary structure, can help shorten their sleep latency.34 Additionally, positive evaluations or affirmative feedback from relatives and healthcare workers often have a positive effect on older adults’ sense of control over their health behaviors. Currently, traditional multi-generational families provide comprehensive support for the elderly through financial support and life care provided by their children. However, with changes in family structure, declining birth rates, and accelerated urbanization, the living distance between elderly parents and their adult children has widened, which has had a certain impact on the connections between multigenerational social networks.29,35 For example, ordinary Chinese families are less efficient in caring for their growing number of elderly relatives, the percentage of the elderly living in nursing homes or empty nests has increased, and family emotional support has declined, but community elderly care services and peer support levels have improved.36 In addition, urban-rural disparities also have a certain impact on the level of tool and information support available to older adults in different regions. It is evident that social support is closely related to psychological resilience, sleep quality, and health outcomes in older adults. However, the effect of social support on sleep quality and whether social support plays a mediating role between psychological resilience and sleep quality in Chinese older adults remains to be determined, suggesting whether healthcare professionals should consider incorporating psychological interventions, such as social support, into their daily sleep quality management practices.
In summary, we found that the biological, psychological, and social aspects of elderly people are affected by traditional Chinese families, the accelerated urbanization process, and urban-rural disparities, and may generate certain pressures. The stress response model proposed by Lazarus and Folkman describes the continuity of cognitive assessment, coping resources, coping strategies, and adaptive outcomes in the process of perceived stress.16 The model proposes that the process of stress and coping is referred to as cognitive assessment (including primary assessment and secondary assessment). Secondary assessment is mainly an evaluation of an individual’s coping resources and is closely related to coping strategies. Among these, social support (eg, emotional support, instrumental support, informational support, and appraisal support) serves as a positive coping resource, not only buffering stress evaluations but also playing a crucial role in decision-making and survival/coping strategies. Additionally, seeking social support is also considered an adaptive coping strategy, and good coping resources/strategies (social support) can have a certain impact on adaptive outcomes (sleep quality).37 In addition, individuals with high psychological resilience often view stress assessment as a challenge rather than a threat and tend to adopt problem-focused coping strategies, such as proactively seeking support, which has a positive impact on social well-being and quality of life in stressful situations. Despite conceptual frameworks exist linking psychological resilience, social support, and sleep quality, there remain considerable gaps in the literature, and the paths via which psychological resilience affects sleep quality in older persons have not been completely studied. In addition to these observations, few studies have examined the mediating role of social support on the relationship between psychological resilience and sleep quality in older adults. To fill this gap, this study intends to unravel the complex relationships between psychological resilience, social support, and sleep quality. Research of social support to be a mediating factor not only fills an important gap in existing research, but also opens up avenues for targeted interventions.
In summary, we propose the following hypotheses:
1. Psychological resilience is significantly related to sleep quality in older adults.
2. Social support mediates the relationship between psychological resilience and sleep quality in older adults.
Methods
Participants
This study adopted a multicenter cross-sectional design. Researchers conducted a study from December 2024 to March 2025 using convenience sampling to select elderly individuals in Shaanxi Province and Shanghai Municipality. The following were the requirements for inclusion: 1) ≥ 65 years of age; 2) moderate communication ability, capable of understanding the questionnaire; 3) voluntary involvement and informed consent. Criteria for exclusion: 1) diagnosed with other severe medical conditions, such as malignant tumors with an expected survival period of ≤ 6 months, multi-organ failure, malignant organic lesions, or concomitant severe illnesses; 2) presence of significant cognitive impairments, mental confusion, or abnormal thinking, or a history of psychiatric disorders. The minimum sample size for this study was determined using the formula for the sample size of an unknown population (n = t² · p · q / d²), with a 95% confidence interval (CI) and an error range (d) of 0.05, t = 1.96, P = 0.5, and q = 0.5, resulting in a minimum sample size of 384. Considering a 10% non-response rate, a total of 425 questionnaires were distributed, with 359 valid responses collected, yielding an effective response rate of 84.5%. Based on the results of the 359 study participants in this study, post-hoc power analysis was conducted using G*Power software version 3.1.9.4 to assess the statistical power of the study. The test family was set as the χ2 test. The results indicated that the statistical power of this study was 99% at the 95% confidence interval level with a moderate effect size.
Ethics
This study was approved by the Ethics Committee of the First Affiliated Hospital of Air Force Medical University (Approval No: XJS20242323-C-1). The research was conducted in strict accordance with the Declaration of Helsinki, ensuring the rights and safety of participants. In particular, participants were made fully aware by researchers that the study was anonymous, voluntary, and that they could leave at any moment. Before the study began, all subjects provided written informed consent.
Measurement
General Information Questionnaire
We created a general information questionnaire by looking over earlier research. It includes age, gender, ethnicity, residential area, per capita family income (monthly), medical payment methods, and number of chronic diseases.
Connor-Davidson Resilience Scale (CD-RISC)
CD-RISC was developed by Connor et al38 in 2003. The scale was adapted to Chinese and revised by Yu X in 2007 and is now widely used in China.39 Three dimensions are included in the 25 items in the questionnaire: optimism, tenacity, and strength. A 5-point Likert scale is used for each item, and values range from 0 (completely incorrect) to 4 (almost entirely correct). Higher psychological resilience is indicated by higher scores. The Cronbach’s α coefficient for the total scale is 0.983, indicating that the Chinese version of the Psychological Resilience Scale has strong internal consistency. We have obtained the license to use an adapted version of the CD-RISC for this study from the developer.
Perceived Social Support Scale (PSSS)
The Perceived Social Support Scale was developed by Zimet in 1990 and adapted for a Chinese cultural context by Jiang et al in 2001.40 The scale consists of three dimensions—other support, family support, and friend support—and includes 12 items. The Likert scale has seven points for each item, with 1 denoting “strongly disagree” and 7 denoting “strongly agree.” Perceived social support is positively correlated with better scores. The whole scale’s Cronbach’s α coefficient in this study was 0.94. This scale is currently in widespread usage in China.
Pittsburgh Sleep Quality Index (PSQI)
Pittsburgh Sleep Quality Index is a widely used self-report measurement tool created to evaluate sleep quality in individuals over the past month.41 It has been validated in the Chinese population and is extensively used in sleep quality research in China. The questionnaire consists of 19 items, including seven dimensions. Poorer sleep quality is indicated by higher scores. The PSQI’s Cronbach’s α in this study was 0.960.
Data Collection
The research team discussed and created a standardized questionnaire guide before to the study’s start, which mostly comprised instructions and safety measures for completing the questionnaire. They also gave the questionnaire investigators consistent training. Before administering the questionnaire, the survey staff had to inform the participants of the study’s goal, its scope, and the confidentiality of the survey’s findings. The elderly voluntarily signed informed consent forms before the questionnaire survey was conducted. Elderly participants completed paper-based questionnaires or online questionnaires within 30–40 minutes. During the survey, for participants with visual impairments, difficulty writing, or low educational attainment, researchers asked them questions based on the questionnaire items and filled out the questionnaire on their behalf in strict accordance with their wishes. Participants who had questions about the questionnaire were provided with answers by the researchers in person. The completed questionnaire was deemed invalid if respondents were unable to finish it for private reasons. After completing the questionnaire, the researchers verified the participants’ responses to ensure that there were no errors, omissions, or invalid answers, thereby ensuring the authenticity and validity of the research data. Two investigators entered the data and cross-checked it to ensure accuracy.
Pilot Study
Prior to the commencement of the main study, we conducted a pilot study on 30 elderly individuals in the target area. They were not part of the main study. To determine its viability, they were required to finish an evaluation. They confirmed that the questions were understandable and straightforward by offering feedback on the assessment’s layout and substance after it was completed. The participants did not exhibit any signs of weariness after finishing the assessment, which took about thirty minutes.
Covariates
Based on the literature review, this study controlled for sociodemographic characteristics of participants as covariates, including age, gender, ethnicity, residential area, education, per capita family income(monthly), medical payment methods, and number of chronic diseases.
Statistical Analysis
This study examined the connection between older individuals’ psychological resilience, social support, and sleep quality using statistical analysis. Mplus 8.3 and IBM SPSS 27 were used for data analysis. Using descriptive statistical methods, the mean (M) and standard deviation (SD) of older adults’ demographic data were determined. To examine and assess the variations among the variables under study, we employed analysis of variance (ANOVA) and independent t-tests. To investigate the correlation between the research variables, Pearson’s correlation coefficients were computed. To further analyze the aforesaid link, such as the mediating role of social support between psychological resilience and sleep quality in older adults. We used Mplus 8.3 software to calculate the direct, indirect, and overall effects in the structural equation model. Indirect effects were examined using bootstrap methods to establish 95% confidence interval (CI). If the bootstrap 95% CI did not include 0, the indirect effect was significant. When examining the goodness-of-fit indices, the following criteria were judged acceptable: Root mean square error of approximation (RMSEA) < 0.80, IFI, TLI, and CFI values ≥ 0.90 or higher, and chi-square to degrees of freedom ratio (χ2/df) ≤ 3. In the model, sociodemographic characteristics such as age, gender, and so on are controlled as covariates. A two-tailed p-value of less than 0.05 was considered statistically significant.
Results
Sociodemographic Characteristics and Univariate Analysis
Sociodemographic characteristics and chronic disease status are presented in Table 1. 359 senior citizens in all took part in the study, including 209 women (58.2%) and 150 men (41.8%). Most older adults resided in rural areas, with only 3.9% having a bachelor’s degree or higher. Most elderly individuals (61.9%) had three or more chronic diseases. Univariate analysis results indicated that, except for medical payment methods, all other variables are statistically significant. Based on the effect size, we can see that among the statistically significant variables, except for residential area, which has a moderate effect, all other variables have large effects.
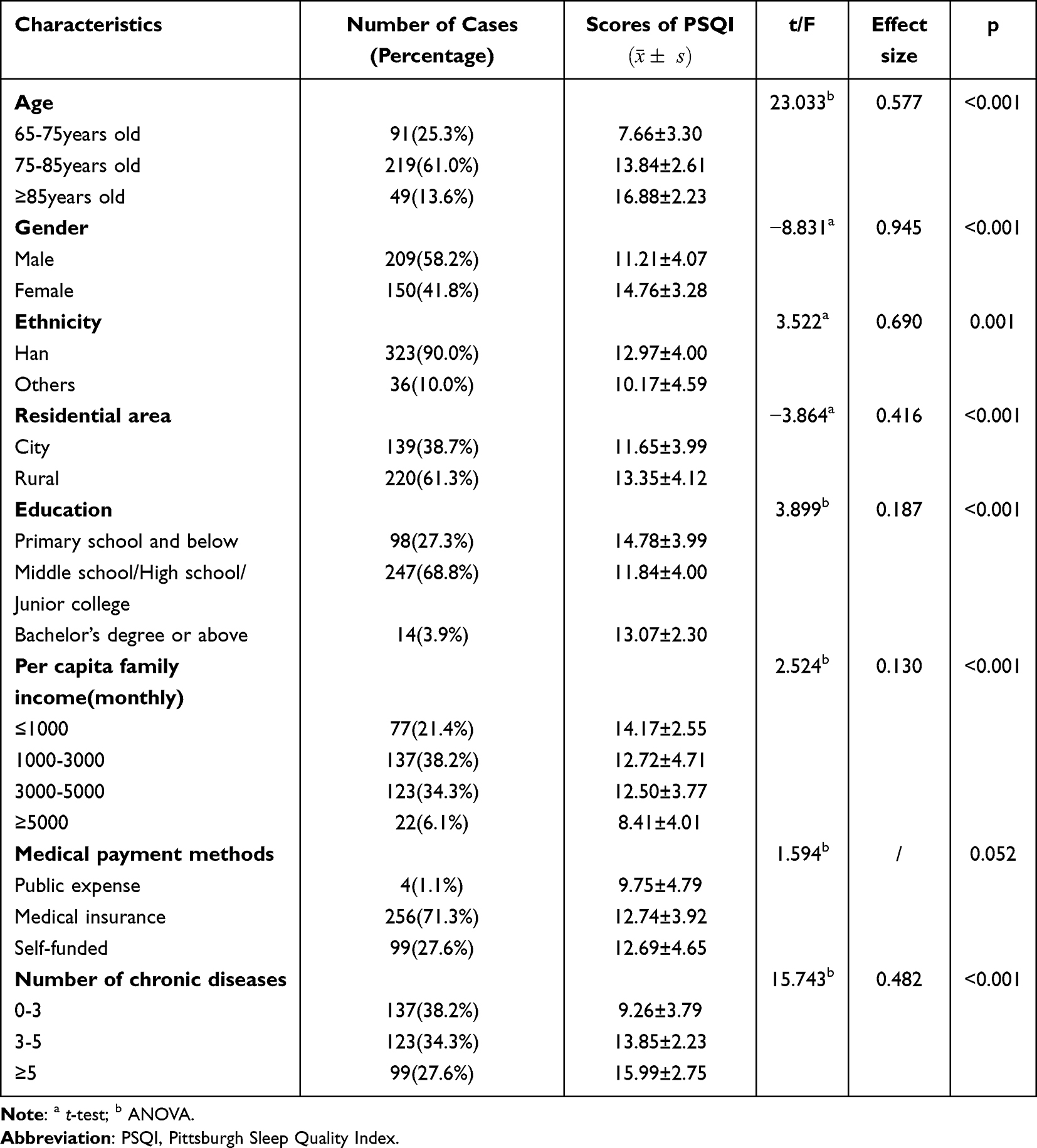 |
Table 1 Characteristics of the Participants and Univariate Analysis of PSQI Scores (N = 359) |
Correlation Analysis
The correlation matrix for the primary study variables is shown in Table 2. The CD-RISC’s overall score had a substantial negative correlation with the PSQI score (r = −0.781, p < 0.001) and a strong positive correlation with the PSSS’s overall score (r = 0.927, p < 0.001). There was a substantial negative correlation between the PSSS and PSQI total scores (r = −0.764, p < 0.001).
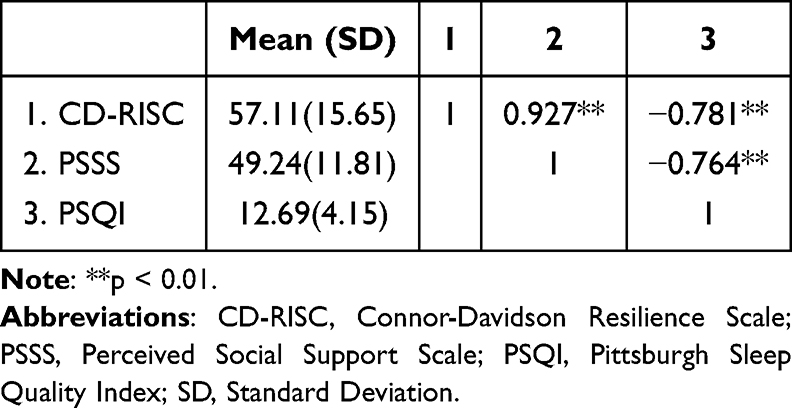 |
Table 2 Correlations of the Study Variables (N= 359) |
Multifactorial Analysis
When sociodemographic characteristics variables with significant statistical differences were included in a linear regression model with PSQI as the dependent variable, psychological resilience, social support, age, education, per capita family income, and number of chronic diseases were independent predictors of sleep quality, while gender, ethnicity, and residential area were not independent predictors of sleep quality. Additionally, we found that older adults aged 75–85 years old, with an income ≥5000, and ≥5 chronic diseases had poorer sleep quality. Older adults with high psychological resilience, high social support, and a middle school/high school/junior college education reported better sleep quality. In addition, we found that VIF < 5 in the results, indicating that there was no serious multicollinearity between variables, as shown in Table 3.
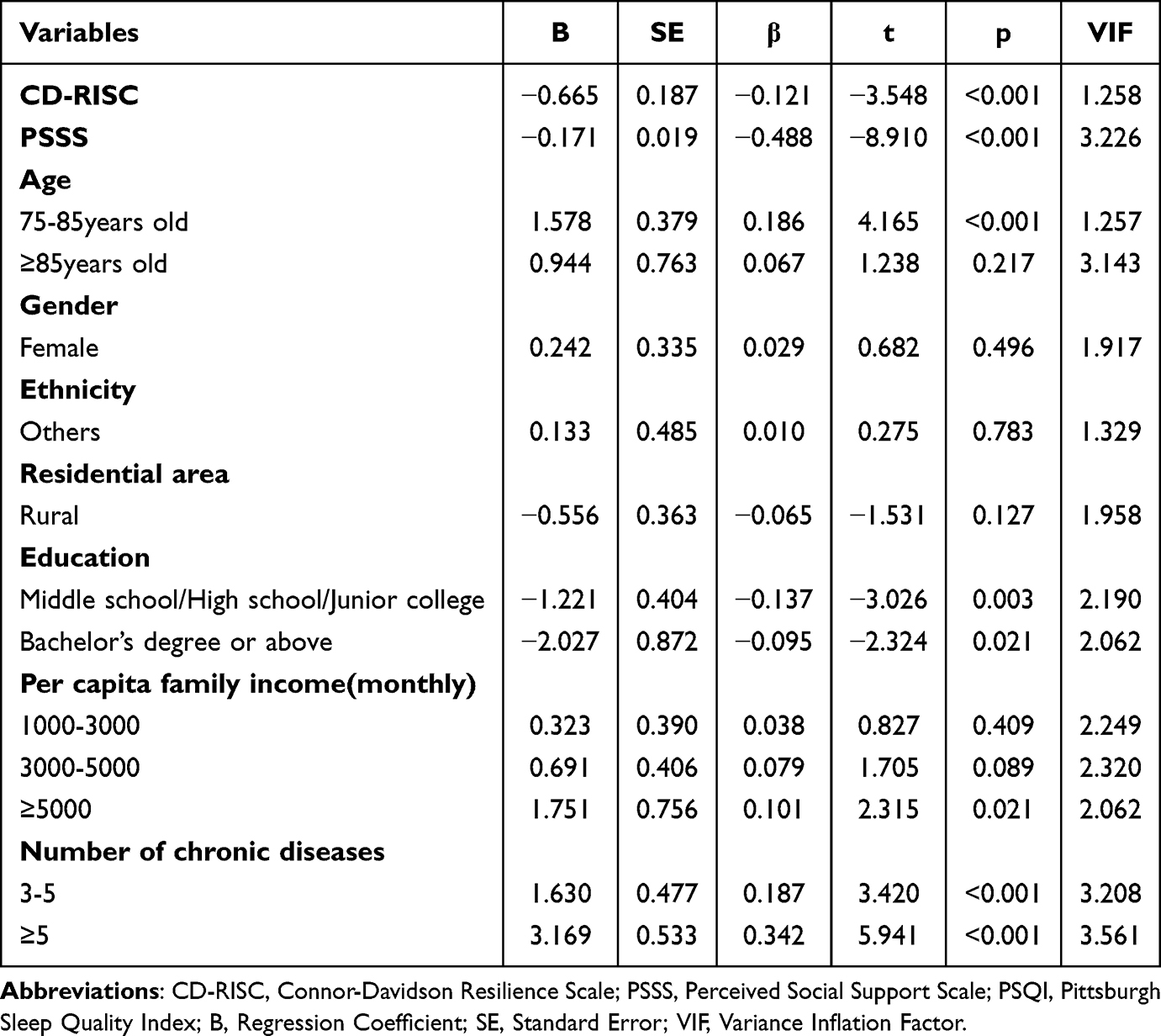 |
Table 3 Multivariate Linear Regression Analysis of Factors Influencing PSQI Scores in the Elderly (N= 359) |
Mediator Model
Table 4 and Figure 1 provide a comprehensive analysis of the pathways in our mediator model. Following Preacher and Hayes, this study uses structural equation modeling in Mplus software to test the proposed hypotheses. The results showed that there is an important correlation between psychological resilience, social support, and sleep quality. First, after controlling for the effects of age, gender, ethnicity, and other factors, we found a significant correlation between psychological resilience and sleep quality in the elderly, as indicated by a high beta coefficient (β = −0.137), with p < 0.05. The 95% CI for this effect, which falls between −0.182 and −0.098, emphasizing the robustness of this relationship. This result supports the rejection of the null hypothesis in Hypothesis 1: Psychological resilience is significantly associated with sleep quality in older adults.
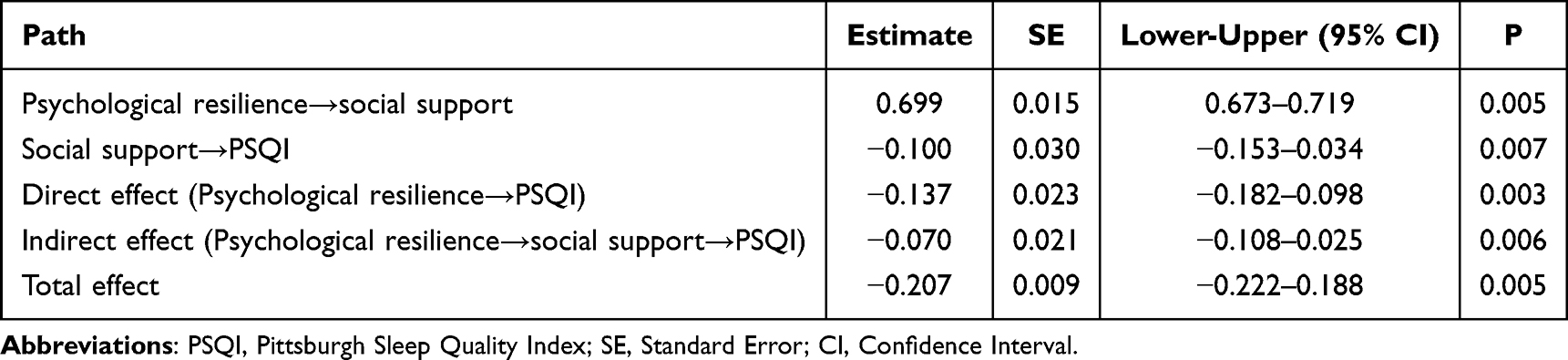 |
Table 4 Direct, Indirect and Total Effects Analysis of the Mediation Model (N= 359) |
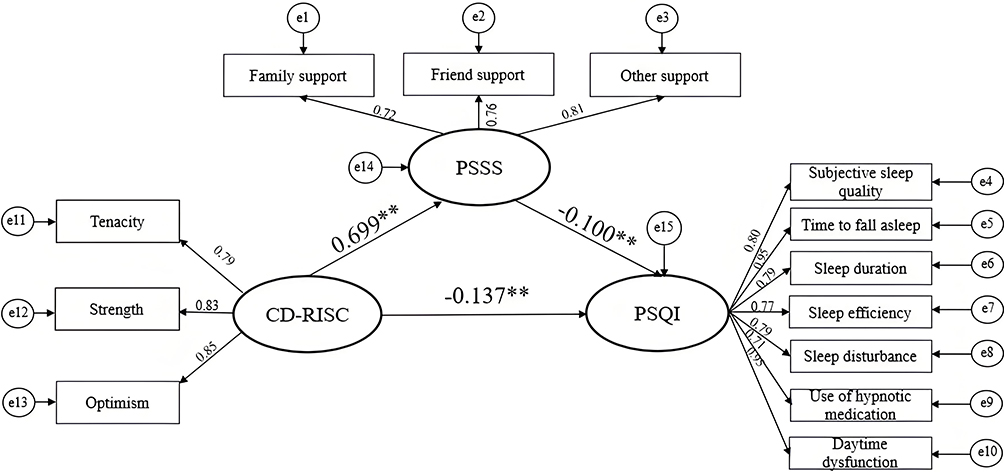 |
Figure 1 Mediating effect of social support in the relationship between psychological resilience and sleep quality. Abbreviations: CD-RISC, Connor-Davidson Resilience Scale; PSSS, Perceived Social Support Scale; PSQI, Pittsburgh Sleep Quality Index. Note: The model was controlled for the following covariates: age, gender, ethnicity, residential area, education, per capita family income(monthly), medical payment methods, and number of chronic diseases. **p < 0.01. |
The mediation effect model fits well. After introducing social support as a mediating variable and controlling for covariates, it was found that the relationship between psychological resilience and sleep quality among the elderly is partially mediated by social support. Additionally, the mediating factor (social support) accounts for 33.7% of the total effect (indirect effect β = −0.070, 95% CI = −0.108 to −0.025, p = 0.006). This finding supports the null hypothesis of rejecting hypothesis 2: Social support mediates the relationship between psychological resilience and sleep quality in older adults.
Discussion
In the complex process of caring for the elderly, understanding the connection between psychological factors and sleep quality is crucial. This study investigated the subtle relationship between psychological resilience (emotional regulation framework) and sleep quality in older adults.42 What makes this study unique is that it explores the mediating role of social support (one of the most widely studied social psychological concepts).43 By investigating the mediating role of social support in the association between older persons’ psychological resilience and sleep quality, this study aims to reveal key insights.
The results of this study indicate that 60.7% of older adults have poor sleep quality, and most participants slept less than 7 hours, failing to meet the National Sleep Foundation’s recommendation of 7–8 hours of sleep per day for older adults.44 This may be due to the high proportion of participants in this study who had three or more chronic diseases (61.9%). A longitudinal study from China has shown that chronic disease comorbidity is significantly negatively associated with sleep duration in older adults.45 Additionally, the results of a prospective cohort study indicate that less than five hours of sleep at night is linked to a higher risk of developing asthma and chronic renal disease.46 This shows that the two can easily form a vicious cycle. In the study results, we found that the elderly with per capita family income(monthly) >5000 had better sleep quality in the single-factor analysis, while in the multiple linear regression analysis, the elderly with per capita family income(monthly) >5000 had poorer sleep quality compared with those with per capita family income(monthly) <1000. This may be due to the fact that multiple linear regression analysis typically considers the combined effects of other independent variables on the dependent variable. Additionally, only 22 elderly individuals (6.1%) with per capita family income(monthly) >5000, which is a small sample size that may generate some errors and be influenced by low risk multicollinearity, leading to certain contradictions and differences between the two results. We also found that while the elderly aged ≥85 years had higher PSQI scores, the multiple linear regression analysis results showed that there was no statistically significant difference in sleep quality between older adults aged ≥85 years and those aged 65–75 years. Previous studies have shown that compared with older adults aged <85 years, those aged 85 years and older are more likely to experience difficulty falling asleep within 30 minutes, waking up in the middle of the night or early morning, and urinating at night, and have poorer sleep quality.47 However, in this study, there was no statistically significant difference in sleep quality between the two groups. This may be due to the small sample size of only 49 elderly individuals aged ≥85 years in this study, which lacks representativeness. Additionally, during the multiple linear regression analysis, age may have been influenced by other sociodemographic independent variables, resulting in non-statistically significant outcomes. This is common in statistics. In summary, in the future, we should expand the sample size and include more variables to explore the impact of sociodemographic characteristics on sleep quality in the elderly.
Psychological Resilience in Older Adults Is Closely Related to Sleep Quality
The results of this study revealed that psychological resilience in older adults is closely related to sleep quality (r = −0.781, p < 0.001). The results of this study are consistent with previous studies. According to psychology studies, more resilient people are likely to possess psychological resource.48 Within this framework, resilient older individuals are more likely to have improved social adaptation and stronger coping skills, which allow them to react to life’s challenges or diversity in a good and productive way.49 These traits can mitigate the impact of negative stressful events on physical and mental health. However, when older adults have low psychological resilience, they frequently suffer from greater emotional and physical health issues, like persistent discomfort and trouble breathing.50 Insomnia, frequent nightly awakenings, and other conditions that impair sleep quality can result from the physical and mental health problems mentioned above.51 In summary, our study emphasizes that psychological resilience in the elderly is closely related to sleep quality. This relationship highlights the importance of good psychological resilience.
Social Support Mediates the Relationship Between Psychological Resilience and Sleep Quality in Older Adults
The association between psychological resilience and sleep quality in older adults is partially mediated by social support (indirect effect = −0.070, mediating effect accounts for 33.7% of the total effect). This finding is of great significance. Consistent with the findings of Yang52 and Zhou et al53 the mediating influence of social support among the elderly suggests nuanced interconnections between positive psychological resources, emotional and material resources, and sleep quality. When people feel stressed, they often experience physical tension and mental pressure, become more sensitive to their sleep environment, or focus too much on sleep, which can affect their sleep quality and shorten their sleep duration. According to the social support buffer model, social support can buffer the impact of negative life events on individuals, thereby enhancing the tolerance of older adults and others to disease and their confidence in recovery.54 Specifically, a positive family environment can provide patients with more family resources. In addition, older adults can also gain a sense of security from interacting with others and participating in group activities. Higher levels of trust and social relationships help alleviate stress, facilitate the dissemination of information (related to health), which is of great significance for the physical and mental health of individuals.
Clinical Significance
This study confirmed that there is a close relationship between psychological resilience, social support, and sleep quality in the elderly. It can provide evidence and appropriate strategies for clinical healthcare professionals and community workers to enhance the psychological resilience and social support levels of the elderly and improve their sleep quality. Additionally, this study’s exploration of sociodemographic factors influencing sleep quality lays the foundation for clinicians to identify high-risk populations for sleep disorders and develop personalized intervention measures. Specific enlightenments and strategies are as follows:
Enhancing Psychological Resilience in Older Adults
With the rise of positive psychology, psychological resilience, as an important component and protective resource for individuals, has been proven to have a positive effect on individuals’ stress, emotional perception, and sleep quality. Previous studies have shown that cognitive behavioral therapy (CBT) can significantly improve an individual’s psychological resilience by using structured methods to identify negative thoughts, adjust cognitive biases, and increase self-efficacy.55 In addition to CBT, mindfulness-based stress reduction (MBSR) has also been shown to reduce emotional responses to specific negative self-beliefs, increase activity in attention-related brain regions, and have a positive role in improving individual psychological resilience level.56 In summary, clinical healthcare professionals may consider selecting appropriate interventions, such as implementing CBT/MBSR, to enhance older adults’ psychological resilience level.
Improving the Level of Social Support for the Elderly
A good level of social support is important for older adults. It can buffer the effects of rumination and psychological distress, and has a close correlation with sleep quality.57,58 Firstly, medical staff should positively evaluate the level of social support among the elderly. Since the current evaluation method is still mainly based on multidimensional scales, it prompts that we can select appropriate tools according to specific needs. Examples include tools that assess specific supportive behaviors (Inventory of Socially Supportive Behaviors, ISSB) and tools that measure subjective perceptions of social support levels (Perceived Social Support Scale, PSSS).40,59 In addition to scales, we can also conduct observation methods or semi-structured interviews for comprehensive assessment. Second, at the family level, children should give the elderly more care, including material and emotional support in multiple dimensions. For example, (1) family members should meet the elderly’s daily needs, provide them with living security, and help them plan their retirement funds/savings reasonably. (2) Family members can regularly accompany elderly people to medical appointments/check-ups to enable the timely detection and treatment of potential health problems or ensure that their condition is well-controlled. (3) Family members should communicate and interact with the elderly regularly, listen to their thoughts and feelings, and provide good emotional support. Third, at the community level, (1) improve community facilities for elderly care services and strengthen service guarantees for community seniors. Do a good job of family doctor contracts and supportive services. Increase the frequency of visits to the elderly with special difficulties, encourage community managers to actively build community smart platforms, and integrate functions such as housekeeping reservation and health consultations. (2) Focus on the quality of community health services, strengthen close ties with Class A tertiary hospitals, and actively conduct community-led, hospital-supported health education to help the elderly better understand and manage their health. In addition to offline medical support, community personnel can also actively utilize big data platforms to carry out remote medical services. (3) Establish volunteer service stations based on community comprehensive service facilities, focus on the elderly to carry out volunteer services extensively, and vigorously carry out neighborly mutual assistance services and interactive exchange activities. (4) Community workers can also regularly organize sports, cultural, and recreational activities to meet the elderly’s cultural demands and emotional communication desires and strengthen their social networks. Fourth, environmental aspects. It is necessary to ensure that older adults have a quiet living environment with appropriate temperature and humidity. Age-friendly modifications can be made, such as removing obstacles in the home, installing handrails, and anti-slip facilities in bathrooms to ensure the safety of older adults’ daily activities. In addition, communities also need to create an elderly-friendly living environment and improve the friendliness of the spatial environment. For example, ensuring that roads are smooth and equipped with fitness facilities and rest seats suitable for the elderly; promoting the aging-friendly renovation of transportation vehicles and the optimization of station layouts.
In summary, we can consider improving the level of social support for the elderly in multiple ways. It is important to consider both the amount and quality of social support when offering it to senior citizens. In other words, more focus needs to be placed on their own sentiments and on enhancing their capacity to perceive social support.
Identify Patients at High Risk of Sleep Disorders and Actively Provide Personalized Psychological Care
Sleep disorders predispose individuals to cognitive impairment, reduced quality of life, and economic burden.60,61 To achieve healthy aging in older adults, improving sleep quality is considered an important health promotion strategy. First, healthcare providers can assess the sleep quality of older adults and screen for sleep disorders using tools such as the Pittsburgh Sleep Quality Index (PSQI) or Insomnia Severity Index (ISI).41,62 Secondly, this study’s results indicate that age, education, per capita family income (monthly), and number of chronic diseases are factors influencing the sleep quality of the elderly. Therefore, healthcare professionals can identify the elderly who are prone to sleep disorders based on assessment results and sociodemographic characteristics and develop personalized care plans.
The European Guidelines for the Diagnosis and Treatment of Insomnia indicate that exercise can effectively treat insomnia. According to the survey, exercise can increase energy expenditure, endorphin secretion, and body temperature, while lowering plasma levels of pro-inflammatory cytokines at rest and promoting the secretion of melatonin and 5-hydroxytryptophan. These substances, in turn, can reduce the risk of insomnia, thereby improving sleep quality and helping the body recover from fatigue.63–65 Therefore, clinical healthcare professionals can recommend types of exercise based on the elderly’s different age groups and physical conditions. For example, advanced age elderly can engage in moderate activities such as walking with a walker, wiping tables, and folding towels, provided that safety is ensured. Younger older adults can engage in moderate- to vigorous-intensity exercise appropriately, such as aerobic training (brisk walking, dancing), resistance training (bodyweight training), or flexibility and balance training (Tai Chi). Since economic status has a certain impact on the sleep quality of the elderly, it is recommended that clinical healthcare providers develop diversified treatment plans for elderly patients without fixed income and low per capita family income (monthly) that not only meet their disease treatment needs but also take into consideration their family’s economic capacity. In addition, we can help them maximize their understanding of medical insurance policies, prioritize the use of drugs on the drug list, assist in registering for outpatient special diseases/applying for medical insurance green channels, and formulate precise examination strategies.
In addition, previous studies have shown that sleep is strongly linked to chronic illnesses and has crucial balancing roles. Elderly women who have trouble falling asleep had higher levels of low-density lipoprotein cholesterol, which raises the risk of coronary heart disease, according to physiological research.66 In addition, most studies indicate that patients with chronic diseases often have lower sleep quality. For example, within 4–6 weeks after coronary heart disease or acute cardiac events, patients have poor sleep quality, and the incidence of moderate to severe insomnia in myocardial infarction patients is as high as 36%-37%.67,68 High incidence rate of sleep quality abnormalities has also been found in elderly patients with lupus erythematosus and osteoarthritis, with the most common abnormalities being sleep fragmentation and increased sleep disorder scores.69 It can be seen that a vicious cycle can easily form between the two, and the relationship between sleep and chronic diseases may be bidirectional. For the elderly with multiple comorbidities, clinicians may consider forming a team consisting of geriatricians (co-morbidity medication integration/sleep disorder diagnosis), clinical specialty nurses (medication guidance, health education, and follow-up), clinical pharmacists (drug interaction screening), clinical psychologists (cognitive behavioral therapy for insomnia), and physical therapists (pain position guidance) and establish a multidisciplinary collaboration model based on groups to carry out comprehensive treatment and care for the elderly with multiple comorbidities, with the aim of improving their sleep quality. In addition, clinical healthcare professionals can further explore the mechanisms underlying sleep and chronic comorbidities in the future, thereby implementing precise interventions to reduce the risk of comorbidities.
Limitations and Future Directions
There are still several limitations, despite the fact that this study is important for comprehending the connection between older persons’ psychological resilience and sleep quality. A causal association between the variables cannot be confirmed by this study because it is a cross-sectional survey. In the future, we should actively conduct in-depth research based on experiments, qualitative analysis, or interventions. Due to the convenience sampling method used in this study, which only surveyed areas in Shaanxi Province and Shanghai Municipality and the prevalence of chronic diseases among the study subjects was relatively high. Therefore, this study has certain sampling biases. The non-random sampling method reduces the generalizability of research results. Since the sample was only from the elderly in China, there are cultural specificities, which also hinder the generalizability of the findings of this study to the elderly in other regions, countries, or cultural contexts. This study relies on self-reporting methods such as questionnaires, which may have certain method bias. In future research, we should employ random sampling methods, increase objective measurement indicators, conduct multi-center studies in different regions, and attempt to validate our findings in groups from other cultural backgrounds or regions. In addition, we also found an unusually high correlation between psychological resilience and social support in this study (r = 0.927), which may in the Chinese cultural context, social support levels and individual emotional coping are often closely intertwined. This indicates that there may be some measurement overlap in this study, which we will consider as an important factor in statistical analysis and scale improvement in future studies. Finally, this study only controlled for sociodemographic variables and did not consider potential confounding variables such as activity level, medication, mental health status, or bruxism. In future studies, we will include more variables to validate our findings. We will continue this research in the future to overcome existing shortcomings.
Conclusion
This study reveals the intricate connection between older persons’ psychological resilience, social support, and sleep quality. Since the subjects of this study are elderly Chinese people, there may be certain cultural specificities. Research findings indicate that psychological resilience in older adults is significantly associated with sleep quality. Furthermore, social support plays a crucial mediating role in psychological resilience and sleep quality. Healthcare professionals should pay attention to the close relationship between psychological resilience, social support, and sleep quality in older adults and adopt appropriate intervention measures such as mindfulness-based stress reduction (MBSR), cognitive behavioral therapy (CBT), organizing group activities for older adults, and assessing their physical condition to develop personalized exercise and lifestyle plans to improve their quality of life from a bio-psycho-social perspective.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Statement
This study was approved by the Ethics Committee of the First Affiliated Hospital of Air Force Medical University (Approval No. XJS20242323-C-1). All participants voluntarily participated in the study and signed an informed consent form. The research was conducted in accordance with the principles of the Declaration of Helsinki.
Author Contributions
Jiayao Li: Writing - original draft, Writing - review & editing, Visualization, Formal analysis, Conceptualization. Jingyu Zhang: Writing - review & editing, Investigation, Data curation. Yingying Hou: Writing - original draft, Investigation, Data curation. Yi Cui: Writing - review & editing, Investigation. Qianqian Wang: Writing - review & editing, Investigation. Anping Ouyang: Writing - review & editing, Investigation. Min Cai: Writing - review & editing, Methodology, Supervision. Yan Hua: Writing - review & editing, Methodology, Supervision, Project administration. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by “Clinical Medicine + X” Research Center Research Topics (No: LHJJ24HL05).
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Gildner T. Global aging: comparative perspectives on aging and the life course. Am J Hum Biol. 2016;28(3):445–446. doi:10.1002/ajhb.22860
2. Ataya J, Soqia J, Albani N, et al. The role of self-efficacy in managing type 2 diabetes and emotional well-being: a cross sectional study. BMC Public Health. 2024;24(1):3471. doi:10.1186/s12889-024-21050-2
3. Zeng Y. Towards deeper research and better policy for healthy aging --using the unique data of Chinese longitudinal healthy longevity survey. China Economic J. 2012;5(2–3):131–149. doi:10.1080/17538963.2013.764677
4. McMaughan DJ, Oloruntoba O, Smith ML. Socioeconomic status and access to healthcare: interrelated drivers for healthy aging. Front Public Health. 2020;8:231. doi:10.3389/fpubh.2020.00231
5. Hurjui I, Hurjui C. Population aging and the influence on healthcare spending. Rom J Leg Med. 2018;26(4):453–456. doi:10.4323/rjlm.2018.453
6. Yuan Y, Li J, Jing Z, et al. The role of mental health and physical activity in the association between sleep quality and quality of life among rural elderly in China: a moderated mediation model. J Affect Disord. 2020;273:462–467. doi:10.1016/j.jad.2020.05.093
7. Besedovsky L, Lange T, Haack M. The sleep-immune crosstalk in health and disease. Physiol Rev. 2019;99(3):1325–1380. doi:10.1152/physrev.00010.2018
8. Morin CM, Jarrin DC. Epidemiology of insomnia: prevalence, course, risk factors, and public health burden. Sleep Med Clin. 2022;17(2):173–191. doi:10.1016/j.jsmc.2022.03.003
9. Scullin MK, Bliwise DL. Sleep, cognition, and normal aging: integrating a half century of multidisciplinary research. Perspect Psychol Sci. 2015;10(1):97–137. doi:10.1177/1745691614556680
10. Hampton T. Sleep and the Elderly. JAMA. 2011;305(21):2162. doi:10.1001/jama.2011.723
11. Mander BA, Winer JR, Walker MP. Sleep and Human Aging. Neuron. 2017;94(1):19–36. doi:10.1016/j.neuron.2017.02.004
12. Sun XH, Ma T, Yao S, et al. Associations of sleep quality and sleep duration with frailty and pre-frailty in an elderly population Rugao longevity and ageing study. BMC Geriatr. 2020;20(1):9. doi:10.1186/s12877-019-1407-5
13. Cho J, Kwak N, Choi SM, et al. Sleep duration and health-related quality of life in Korean adults: 2007-2015 Korea National Health and Nutrition Examination Survey. Sleep Breath. 2020;24(2):725–733. doi:10.1007/s11325-019-01972-7
14. Bonanno GA, Westphal M, Mancini AD. Resilience to loss and potential trauma. Annu Rev Clin Psychol. 2011;7:511–535. doi:10.1146/annurev-clinpsy-032210-104526
15. Hou Y, Yan S, Zhang L, et al. Perceived stress and life satisfaction among elderly migrants in China: a moderated mediation model. Front Psychol. 2022;13:978499. doi:10.3389/fpsyg.2022.978499
16. Folkman S. Personal control and stress and coping processes: a theoretical analysis. J Pers Soc Psychol. 1984;46(4):839–852. doi:10.1037//0022-3514.46.4.839
17. Mj D, Houang ST, Scheinmann R, Yoon IS, Chiasson MA, Hirshfield S. Engagement in care, psychological distress, and resilience are associated with sleep quality among HIV-positive gay, bisexual, and other men who have sex with men. Sleep Health. 2016;2(4):322–329. doi:10.1016/j.sleh.2016.08.002
18. Hao X, Li M, Li J, Lv M, Qin Y, Li K. Sleep quality in relation to social support and resilience among rural empty-nest older adults in China. Sleep Med. 2021;82:193–199. doi:10.1016/j.sleep.2021.03.026
19. Li G, Kong L, Zhou H, Kang X, Fang Y, Li P. Relationship between prenatal maternal stress and sleep quality in Chinese pregnant women: the mediation effect of resilience. Sleep Med. 2016;25:8–12. doi:10.1016/j.sleep.2016.02.015
20. Kothgassner OD, Goreis A, Glenk LM, et al. Virtual and real-life ostracism and its impact on a subsequent acute stressor. Physiol Behav. 2021;228:113205. doi:10.1016/j.physbeh.2020.113205
21. Palagini L, Moretto U, Novi M, et al. Lack of resilience is related to stress-related sleep reactivity, hyperarousal, and emotion dysregulation in insomnia disorder. J Clin Sleep Med. 2018;14(5):759–766. doi:10.5664/jcsm.7100
22. Zieliński G, Matysik-Woźniak A, Baszczowski M, et al. Myopia & painful muscle form of temporomandibular disorders: connections between vision, masticatory and cervical muscles activity and sensitivity and sleep quality. Sci Rep. 2023;13(1):20231. doi:10.1038/s41598-023-47550-6
23. Boer J, Toncar T, Stange A, Rosenblum L, Fietze I. Effect of graduated drug therapy for moderate-to-severe chronic insomnia on the severity of disease: an observational study in Germany. J Clin Sleep Med. 2025;21(1):33–45. doi:10.5664/jcsm.11334
24. Gupta CC, Irwin C, Vincent GE, Khalesi S. The relationship between diet and sleep in older adults: a narrative review. Curr Nutr Rep. 2021;10(3):166–178. doi:10.1007/s13668-021-00362-4
25. Hasan F, Tu YK, Lin CM, et al. Comparative efficacy of exercise regimens on sleep quality in older adults: a systematic review and network meta-analysis. Sleep Med Rev. 2022;65:101673. doi:10.1016/j.smrv.2022.101673
26. Mullington JM, Cunningham TJ, Haack M, Yang H. Causes and consequences of chronic sleep deficiency and the role of orexin. Front Neurol Neurosci. 2021;45:128–138. doi:10.1159/000514956
27. Turrini S, Wong B, Eldaief M, et al. The multifactorial nature of healthy brain ageing: brain changes, functional decline and protective factors. Ageing Res Rev. 2023;88:101939. doi:10.1016/j.arr.2023.101939
28. Tomaka J, Thompson S, Palacios R. The relation of social isolation, loneliness, and social support to disease outcomes among the elderly. J Aging Health. 2006;18(3):359–384. doi:10.1177/0898264305280993
29. Zhao Z, Jing S, Yan Z, Yu L. Social change and birth cohort decrease in social support for older adults in China: a cross-temporal meta-analysis, 1994-2018. Health Soc Care Community. 2020;28(5):1438–1447. doi:10.1111/hsc.13004
30. Dickman KD, Thomas MC, Chin BN, Kamarck TW. Bidirectional associations between loneliness, emotional support, and sleep in daily life. Psychosom Med. 2024;86(4):252–260. doi:10.1097/PSY.0000000000001291
31. Zhu J, Xu L, Sun L, Qin D. Negative life events, sleep quality, and depression among older adults in Shandong Province, China: a conditional process analysis based on economic income. Geriatr Gerontol Int. 2024;24(8):751–757. doi:10.1111/ggi.14914
32. Billings ME, Hale L, Johnson DA. Physical and social environment relationship with sleep health and disorders. Chest. 2020;157(5):1304–1312. doi:10.1016/j.chest.2019.12.002
33. Yan Y, Zhang H, Kang M, Lan L, Wang Z, Lin Y. Experimental study of the negative effects of raised bedroom temperature and reduced ventilation on the sleep quality of elderly subjects. Indoor Air. 2022;32(11):e13159. doi:10.1111/ina.13159
34. Mo W, Yamakawa M, Takahashi S, et al. Effect of sleep report feedback using information and communication technology combined with health guidance on improving sleep indicators in community-dwelling older people: a pilot trial. Psychogeriatrics. 2023;23(5):763–772. doi:10.1111/psyg.12994
35. Cheng Y, Xi J, Rosenberg MW, Gao S. Intergenerational differences in social support for the community-living elderly in Beijing China. Health Sci Rep. 2018;1(11):e96. doi:10.1002/hsr2.96
36. Zhao X, Zhang D, Wu M, et al. Loneliness and depression symptoms among the elderly in nursing homes: a moderated mediation model of resilience and social support. Psychiatry Res. 2018;268:143–151. doi:10.1016/j.psychres.2018.07.011
37. Islam AKMN, Mäntymäki M, Laato S, Turel O. Adverse consequences of emotional support seeking through social network sites in coping with stress from a global pandemic. Int J Inf Manage. 2022;62:102431. doi:10.1016/j.ijinfomgt.2021.102431
38. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
39. Amichaud R, Donatini G, Barussaud ML, Charalambous C, Ingrand I, Faure JP. Health-related quality of life after laparoscopic sleeve gastrectomy. A multicentric experience. Minerva Chir. 2016;71(4):245–251.
40. Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the multidimensional scale of perceived social support. J Pers Assess. 1990;55(3–4):610–617. doi:10.1080/00223891.1990.9674095
41. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
42. Troy AS, Willroth EC, Shallcross AJ, Giuliani NR, Gross JJ, Mauss IB. Psychological Resilience: an Affect-Regulation Framework. Annu Rev Psychol. 2023;74:547–576. doi:10.1146/annurev-psych-020122-041854
43. Stevens M, Cruwys T, Murray K. Social support facilitates physical activity by reducing pain. Br J Health Psychol. 2020;25(3):576–595. doi:10.1111/bjhp.12424
44. Hirshkowitz M, Whiton K, Albert SM, et al. National sleep foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1(4):233–243. doi:10.1016/j.sleh.2015.10.004
45. He L, Biddle SJH, Lee JT, et al. The prevalence of multimorbidity and its association with physical activity and sleep duration in middle aged and elderly adults: a longitudinal analysis from China. Int J Behav Nutr Phys Act. 2021;18(1):77. doi:10.1186/s12966-021-01150-7
46. Wang Y, Jiang G, Hou N, et al. Effects and differences of sleep duration on the risk of new-onset chronic disease conditions in middle-aged and elderly populations. Eur J Intern Med. 2023;107:73–80. doi:10.1016/j.ejim.2022.11.005
47. Li J, Yao YS, Dong Q, et al. Characterization and factors associated with sleep quality among rural elderly in China. Arch Gerontol Geriatr. 2013;56(1):237–243. doi:10.1016/j.archger.2012.08.002
48. Mosheva M, Hertz-Palmor N, Dorman Ilan S, et al. Anxiety, pandemic-related stress and resilience among physicians during the COVID-19 pandemic. Depress Anxiety. 2020;37(10):965–971. doi:10.1002/da.23085
49. Liu Y, Zhang Q, Jiang F, et al. Association between sleep disturbance and mental health of healthcare workers: a systematic review and meta-analysis. Front Psychiatry. 2022;13:919176. doi:10.3389/fpsyt.2022.919176
50. Sihvola S, Kuosmanen L, Kvist T. Resilience and related factors in colorectal cancer patients: a systematic review. Eur J Oncol Nurs. 2022;56:102079. doi:10.1016/j.ejon.2021.102079
51. Szady P, Bączyk G, Kozłowska K. Fatigue and sleep quality in rheumatoid arthritis patients during hospital admission. Reumatologia. 2017;55(2):65–72. doi:10.5114/reum.2017.67600
52. Yang L, Wang H, Cheng J. Association between social capital and sleep duration among rural older adults in China. BMC Public Health. 2022;22(1):12. doi:10.1186/s12889-021-12441-w
53. Zhou K, Ning F, Wang X, Wang W, Han D, Li X. Perceived social support and coping style as mediators between resilience and health-related quality of life in women newly diagnosed with breast cancer: a cross-sectional study. BMC Womens Health. 2022;22(1):198. doi:10.1186/s12905-022-01783-1
54. Ditzen B, Heinrichs M. Psychobiology of social support: the social dimension of stress buffering. Restor Neurol Neurosci. 2014;32(1):149–162. doi:10.3233/RNN-139008
55. Henrich D, Glombiewski JA, Scholten S. Systematic review of training in cognitive-behavioral therapy: summarizing effects, costs and techniques. Clin Psychol Rev. 2023;101:102266. doi:10.1016/j.cpr.2023.102266
56. Goldin PR, Thurston M, Allende S, et al. Evaluation of cognitive behavioral therapy vs mindfulness meditation in brain changes during reappraisal and acceptance among patients with social anxiety disorder: a randomized clinical trial. JAMA Psychiatry. 2021;78(10):1134–1142. doi:10.1001/jamapsychiatry.2021.1862
57. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357. doi:10.1037/0033-2909.98.2.310
58. Zhang L, Cruz-Gonzalez M, Lin Z, Ouyang X, Zhao F, Alegría M. Association of everyday discrimination with health outcomes among Asian and non-Asian US older adults before and during the COVID-19 pandemic. Front Public Health. 2022;10:953155. doi:10.3389/fpubh.2022.953155
59. Stokes JP, Wilson DG. The inventory of socially supportive behaviors: dimensionality, prediction, and gender differences. Am J Community Psychol. 1984;12(1):53–69. doi:10.1007/BF00896928
60. Daley M, Morin CM, LeBlanc M, Grégoire JP, Savard J. The economic burden of insomnia: direct and indirect costs for individuals with insomnia syndrome, insomnia symptoms, and good sleepers. Sleep. 2009;32(1):55–64.
61. Liu Y, Chen L, Huang S, et al. subjective sleep quality in amnestic mild cognitive impairment elderly and its possible relationship with plasma amyloid-β. Front Neurosci. 2020;14:611432. doi:10.3389/fnins.2020.611432
62. Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/s1389-9457(00)00065-4
63. Uchida S, Shioda K, Morita Y, Kubota C, Ganeko M, Takeda N. Exercise effects on sleep physiology. Front Neurol. 2012;3:48. doi:10.3389/fneur.2012.00048
64. Kapsimalis F, Basta M, Varouchakis G, Gourgoulianis K, Vgontzas A, Kryger M. Cytokines and pathological sleep. Sleep Med. 2008;9(6):603–614. doi:10.1016/j.sleep.2007.08.019
65. Driver HS, Taylor SR. Exercise and sleep. Sleep Med Rev. 2000;4(4):387–402. doi:10.1053/smrv.2000.0110
66. Liu J, Son S, Giancaterino M, Narushima M. Difficulty of falling asleep and non-high-density lipoprotein cholesterol level among canadian older adults: a cross-sectional analysis of the canadian longitudinal study for aging baseline data. J Geriatr Cardiol. 2021;18(8):597–608. doi:10.11909/j.issn.1671-5411.2021.08.003
67. Da Costa D, Allman AA, Libman E, Desormeau P, Lowensteyn I, Grover S. Prevalence and determinants of insomnia after a myocardial infarction. Psychosomatic. 2017;58(2):132–140. doi:10.1016/j.psym.2016.11.002
68. Frøjd LA, Munkhaugen J, Moum T, et al. Insomnia in patients with coronary heart disease: prevalence and correlates. J Clin Sleep Med. 2021;17(5):931–938. doi:10.5664/jcsm.9082
69. Taylor-Gjevre RM, Gjevre JA, Nair B, Skomro R, Lim HJ. Components of sleep quality and sleep fragmentation in rheumatoid arthritis and osteoarthritis. Musculoskeletal Care. 2011;9(3):152–159. doi:10.1002/msc.208
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Left-Behind Experience and Behavior Problems Among Adolescents: Multiple Mediating Effects of Social Support and Sleep Quality
Ge M, Yang M, Sheng X, Zhang L, Zhang K, Zhou R, Ye M, Cao P, Sun Y, Zhou X
Psychology Research and Behavior Management 2022, 15:3599-3608
Published Date: 7 December 2022
The Influence of Social Support on the Mental Health of Elderly Individuals in Healthy Communities with the Framework of Mental Toughness
Zhang C, Dong C
Psychology Research and Behavior Management 2023, 16:2977-2988
Published Date: 4 August 2023
Factors Associated with the Delay in Seeing a Doctor: Evidence of Chinese Middle-Aged and Older Adults
Qin S, Ni X, Ding Y
Journal of Multidisciplinary Healthcare 2023, 16:4239-4253
Published Date: 28 December 2023
Social Support and Social Adjustment Among Chinese Secondary School Students: The Mediating Roles of Subjective Well-Being and Psychological Resilience

Yu L, Wu X, Zhang Q, Sun B
Psychology Research and Behavior Management 2024, 17:3455-3471
Published Date: 7 October 2024
Falls, Sleep Disorders and Cognitive Frailty in Hospitalized Older Adults with Hypertension:A Cross-Sectional Study
Li X, Li H, Gan S, Zhang Y, Yin D, Zhu B, Wang S, Liu Y
Clinical Interventions in Aging 2025, 20:859-872
Published Date: 17 June 2025