Back to Journals » Psychology Research and Behavior Management » Volume 15
Left-Behind Experience and Behavior Problems Among Adolescents: Multiple Mediating Effects of Social Support and Sleep Quality
Authors Ge M ![]() , Yang M, Sheng X, Zhang L, Zhang K, Zhou R, Ye M, Cao P, Sun Y, Zhou X
, Yang M, Sheng X, Zhang L, Zhang K, Zhou R, Ye M, Cao P, Sun Y, Zhou X ![]()
Received 5 August 2022
Accepted for publication 23 November 2022
Published 7 December 2022 Volume 2022:15 Pages 3599—3608
DOI https://doi.org/10.2147/PRBM.S385031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Menglin Ge,1– 3,* Meng Yang,1– 3,* Xuanlian Sheng,1– 3,* Ling Zhang,2,3 Kai Zhang,1– 3 Ruochen Zhou,1– 3 Mengting Ye,1– 3 Panpan Cao,1– 3 Yehuan Sun,2,4,5 Xiaoqin Zhou1– 3
1School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei City, People’s Republic of China; 2Chaohu Hospital of Anhui Medical University, Hefei City, People’s Republic of China; 3Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei City, People’s Republic of China; 4Department of Epidemiology and Health Statistics, School of Public Health, Anhui Medical University, Hefei City, People’s Republic of China; 5Center for Evidence-Based Practice, Anhui Medical University, Hefei City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoqin Zhou, Chaohu Hospital of Anhui Medical University, Hefei City, People’s Republic of China, Tel +8613865913378, Email [email protected] Yehuan Sun, Department of Epidemiology and Health Statistics, School of Public Health, Anhui Medical University, Hefei City, People’s Republic of China, Email [email protected]
Purpose: Adolescence has always been a period prone to behavior problems. Some studies have shown that left-behind experience, social support, and sleep quality are all crucial factors influencing behavior problems, but the mechanisms of how they are influenced are unclear. This cross-sectional study investigated the prevalence of behavior problems among school-aged adolescents and explored the mediating role of social support and sleep quality in the association between left-behind experience and behavior problems.
Patients and Methods: A total of 738 school adolescent students completed this questionnaire. We collected basic information about the participants using a general demographic scale and assessed their sleep quality, social support, and behavioral problems using the Pittsburgh Sleep Quality Index scale, Social Support Rating Scale, and Strengths and Difficulties Questionnaire. The multiple mediating effects of sleep quality and social support were examined by path analysis.
Results: Among 738 school-aged adolescent students who completed the survey, a total of 198 students had behavior problems, with an overall prevalence of 26.8%. In the multiple mediation model, the mediation effect of social support and sleep quality on left-behind experience to behavior problems was 56.7% (direct effect: standardized estimate=0.946, indirect effect: standardized estimate=1.239). The model was a saturated model, and fit was no longer considered.
Conclusion: We found that social support and sleep quality had a series of multiple mediating effects in the pathway from left-behind experience to behavior problems, and both significantly moderated behavior problems. Therefore, we suggest that we should pay more attention to students’ psychological status and improve their use of social support for left-behind adolescents, in addition to giving more external social support. And paying attention to their sleep problems to reduce the occurrence of behavior problems, considering that their psychological development is not mature.
Keywords: adolescents, left-behind experience, behavior problems, social support, sleep quality
Introduction
Adolescence has always been a time of high risk for behavior problems. The World Health Organization (WHO) estimates that screening at any given point in time will result in approximately 10–20% of adolescents worldwide having behavior problems,1 with approximately 30% or more having experienced behavior problems <16 years old.2 In 2018, Austria interviewed 3446 students aged 10 to 18 with behavioral problems, of which 16.5% identified behavioral problems.3 According to a cross-sectional survey conducted in China, 10.7% of school-aged adolescents had behavioral and emotional issues.4 In recent years, emotional and behavior problems in adolescents have increased in China and abroad. Furthermore, research suggests that emotional and behavioral problems in childhood affect mental health in later life, and an 11-year longitudinal study found that students with behavioral problems in first grade showed more significant and long-term negative outcomes later in life.5,6
Lack of parental companionship is an essential factor affecting behavior problems in children and adolescents.7 Due to China’s rapid economic growth, accompanied by high modernization and urbanization rates, many rural young adult laborers have migrated to cities. However, because of the high cost of living in cities, most adults do not choose to bring their children to the cities, so a large number of children are left behind in rural areas, unable to live with their parents, and are instead cared for by one parent or grandparents or relatives.8,9 These children are called left-behind children(LBC) because one or both parents have moved to other areas for more than six months and, therefore, cannot live with both parents in the household registration area.10 For this group of adolescents, the childhood experience of missing parental companionship makes them more prone to behavior and emotional problems.11 Additionally, research has revealed that LBC and students who have experienced being left behind have lower levels of social support, particularly emotional support than children who were not left behind, and they also have poorer sleep quality.12,13 The level of social support is closely related to behavior problems, and Sun Shihong et al found that social support has a protective effect on adolescent behavior problems.14 Sleep quality also affects behavior problems. A 2018 survey showed that sleep difficulties in adolescents promote behavior problems, and a review also suggested that sleep disorders are associated with emotional and behavior difficulties in children and adolescents.15,16 Although the mechanism by which left-behind leads to behavior problems has been discussed, its specific mechanism remains unclear, and sleep quality and social support might play a crucial mediating role between left-behind and behavior problems.
Social support is known to impact sleep quality, and a meta-analysis of 61 research found a high correlation between social support and positive sleep outcomes.17 Supportive social ties were independently linked to higher sleep quality at 15 years of follow-up, according to a UK birth cohort study.18 As a result, social support can mediate the relationship between left-behind and sleep, implying that social support and sleep quality are sequential mediators of the impacts of left-behind on behavior problems. Due to the strong correlation and predictive effect between left-behind, sleep quality, social support and behavior problems, we speculate that students who remain and experience being left behind may have worse sleep quality due to lower levels of social support, and then have a higher risk of behavior problems.
Thus, the purpose of our research is to (1) investigate the behavior problems of adolescent students in central Anhui Province; (2) examine the relationship between left-behind, social support, sleep quality, and behavior problems; (3) explore the series of multiple mediating roles of social support and sleep quality between left-behind and behavior problems.
Materials and Methods
Participants and Procedure
The survey was conducted from October 2020 to April 2021 in Anhui Province, China. According to the World Health Organization’s definition of adolescence (10–19 years old),19 participants in this study were required to meet the following criteria (1) they were between 10 and 19 years old (meeting the definition of adolescence); (2) they agreed to participate in this survey voluntarily; and (3) they were able to complete this questionnaire independently. Adolescents with the following criteria were not considered for inclusion: (1) meeting the diagnostic criteria for psychiatric disorders (including depressive disorder, schizophrenia, bipolar disorder, intellectual developmental disorder, etc.) and their related disorders in ICD-10; (2) unable to complete the investigation due to a severe physical disease.
Before the start of the survey, accompanied by the school teacher, we explained to the participants the purpose of the survey and the method of filling out the questionnaire. We informed the participants that the data collected in this survey will be used for research purposes only and will be kept s Before the survey, this school survey was conducted with informed consent from the school, participating students, and their guardians (parents or other caregivers). This survey was approved by the Ethics Committee of Chaohu Hospital, Anhui Medical University (2019-kyxm-012). All study procedures were in strict compliance with the principles of the Declaration of Helsinki.
Measures
Demographic Characteristics
The following demographic characteristics were analyzed: age, gender, grade level, siblings, residence in the dormitory, left-behind experience, parent’s marital status, household economic level, and mother’s and father’s education level. These demographic characteristics were selected by reference.
Regarding previous definitions of left-behind experience, this study defines the left-behind experience as the experience of adolescents who have lived or are currently living with only one parent or other relative or alone because their parent or one of them has been out of work for more than six months.20 Therefore participants were asked: Are the parents or one of the parents currently or ever working away from home for more than six months? If participants answered “yes”, they were considered to have left-behind experience.
Behavior problems
The Strengths and Difficulties Questionnaire (SDQ) was used to assess adolescents’ behavioral problems. Psychiatrist Goodman, R. developed the SDQ in 1997, and the scale has been introduced in 40 countries and regions since 2001.21–23 The scale was introduced to China by Du Yasong et al in 2005, and the results reported that the SDQ remains a reliable and valid screening method for behavior problems in Chinese children and adolescents.24 The SDQ (Student Version) consists of 25 items, each rated on a three-level scale of 0–2 (0: “does not meet”, 1: “somewhat meets”, 2: “fully meets”). Items 7, 14, 21, and 25 are reversed scores. The SDQ consists of five subscales, including conduct problems, hyperactivity-inattention, peer problems, emotional symptoms, and prosocial behavior, with the prosocial behavior subscale reflecting positive social behavior in children and adolescents. The total difficulty score is obtained by summing the remaining subscales except for prosocial behavior; the higher the total score, the more severe the child’s behavior problems, defining a total difficulty score >17 as having abnormal behavior problems.24
Sleep Quality
The Pittsburgh Sleep Quality Index (PSQI) assesses participants’ sleep quality and disturbance in the most recent month.25 It consists of 19 self-assessment items and five other-rated items, with the 19th self-assessment item and five other-rated items not involved in the scoring. The 18 self-assessment items involved in scoring consisted of 7 parts: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, hypnotic use, and daytime dysfunction; each part was scored on a scale of 0 to 3. The cumulative score of each part was the total PSQI score, with a total score range of 0 to 2L. The higher the score, the worse the sleep quality, and a PSQI score ≥7 suggests that sleep quality is poor, with a sensitivity of 98.3% and specificity of 90.2%.26 It has been determined that the Chinese version of the PSQI shows good validity and reliability.27
Social Support
The Social support rating scale (SSRS) has ten entries and consists of three subscales: objective support (entries 2, 6, and 7), subjective support (entries 1, 3, 4, and 5), and social support utilization (entries 8, 9, and 10).28 The actual objective support, subjective experience, and individual utilization of social support were calculated by calculating the sum of the entry scores for each subscale.
Statistical Analysis
We used IBM SPSS Statistics 23.0 for descriptive and correlation analyses. Firstly, this study conducted a descriptive analysis of the background characteristics and sleep quality of adolescents’ behavior problems, using Mean±Standard deviations (SD) for continuous variables and frequencies (percentages) for categorical variables, followed by the Wilcoxon Mann–Whitney test or Chi-square test for differences between the two groups with and without behavior problems. Secondly, the psychological scales were described using the Mean±SD. Then Wilcoxon Mann–Whitney test was used to compare the differences in scale scores with and without behavioral problems and to conduct a simple correlation analysis between the left-behind experience and the psychological scales. The relationship between the social support subscale, sleep quality and behavior problem factors were further examined using Spearman correlation analysis because not all data were normally distributed.
Preacher and Hayes’ technique evaluated the sequential multiple mediation hypotheses for left-behind experience, sleep quality, social support, and behavioral issues.29 1000 resamples were used in a bootstrapping approach to testing mediating effects’ significance.30 The data were normalized before analysis. When evaluating the goodness of fit of the model, because the model in this study is a saturated model, that is, all the parameters to be estimated are exactly equal to the elements in the covariance matrix, and the degree of freedom is 0, the fitting index is no longer estimated, only the path coefficient is concerned.31 Mplus version 8.3 was used for path analysis. P-values <0.05 (two-tailed) were considered statistically significant.
Results
Univariate Analysis of Factors Influencing Behavior Problems in Adolescents
The behavior problems of adolescents with different characteristics are shown in Table 1. According to the classification standard of SDQ, among the 738 respondents, a total of 198 students had behavior problems, the prevalence rate was 26.8%, and the mean age was 13.12±1.63 years old, which was slightly higher than that of students without behavior problems (χ2= –2.552, P=0.011). The proportion of students with behavior problems in high school students is 45.0%, which is larger than that of elementary and junior high school students, 23.2% and 24.8% (χ2=19.661, P<0.001). 31.7% of left-behind adolescents have behavior problems, while only 21.9% of non-left-behind students have behavior problems (χ2=9.141, P=0.002). 39.3% of resident students had behavior problems, compared to 23.0% of non-residential students (χ2=17.920, P<0.001). Regarding parents’ marital status, the proportion of parents with divorced or widowed parents with behavior problems is significantly higher than that of students with intact families (χ2=13.943, P<0.001). In the case of sleep quality, 55.9% of students with poor sleep quality have behavior problems, while only 17.0% of students with good sleep quality have behavior problems (χ2=107.155, P<0.001). There were no significant differences in gender, siblings, family economic situation, and parents’ education level.
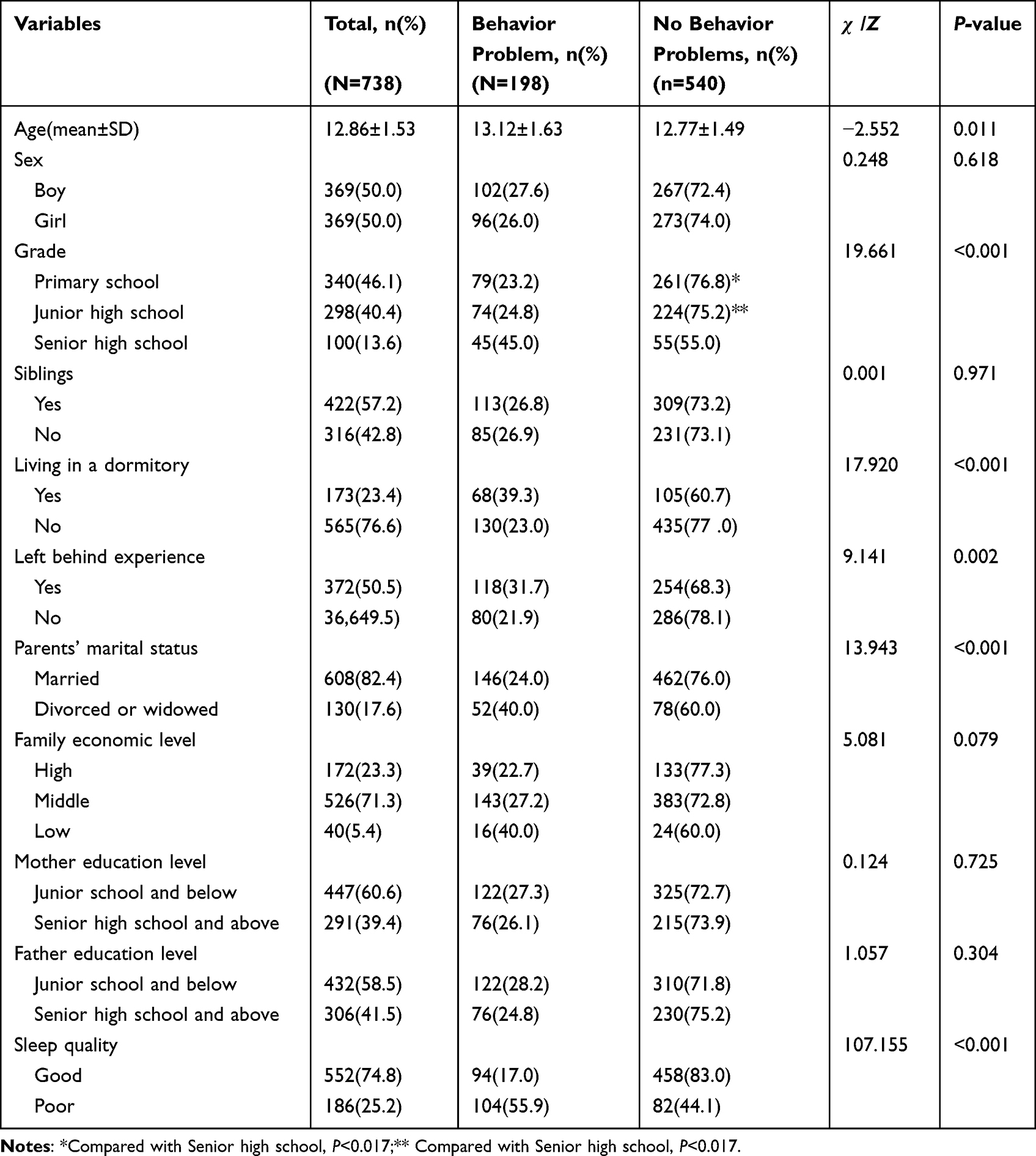 |
Table 1 Background Characteristics and Sleep Quality of Adolescents’ Behavior Problems |
Comparison of Psychological measures Between Adolescents with and without Left-Behind and Behavior Problems
The scores of the adolescents on each scale are shown in Table 2. Concerning behavior problems, students with behavior problems had lower sleep quality scores and social support scale scores than those without behavior problems (p < 0.01). In terms of left-behind experience, adolescents with left-behind experience had lower scores on sleep scales than non-left-behind students except for sleep efficiency and hypnotic use, and in the SSRS the two groups differed only in total score and social utilization. On the SDQ scale, the left-behind group scored higher on emotional symptoms, conduct problems, hyperactivity-inattention issues, and peer problems than the group with no left-behind experience, suggesting that adolescents in the left-behind group were more likely to have emotional problems, conduct problems, hyperactivity situations, and interpersonal difficulties. The prosocial behaviors factor scores were lower in the left-behind group, indicating that the left-behind group had more difficulties in prosocial aspects. In addition, the total scale score of the left-behind group was higher than that of the non-left-behind group, which indicated that the left-behind group was more likely to have emotional and behavioral problems. There was a correlation between left-behind experience, sleep quality, social support utilization, and behavior problems.
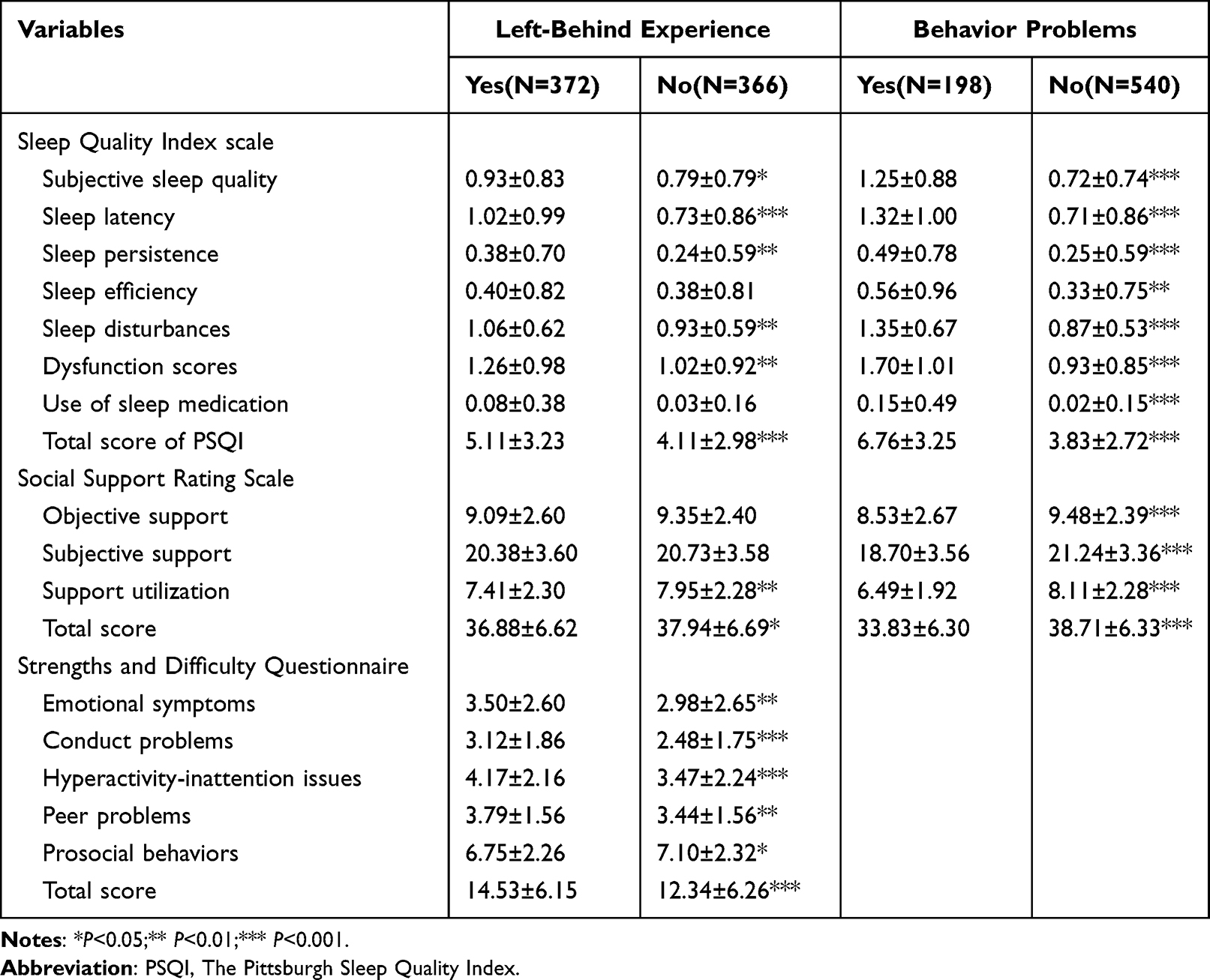 |
Table 2 Comparison of Psychological Measures Between Adolescents with and without Left-Behind and Behavior Problems |
Pairwise Correlation Analysis
Table 3 shows the results of the Spearman correlation analysis. There was a significant positive correlation between sleep quality, subjective support, objective support, utilization, and behavior problem (P<0.001).
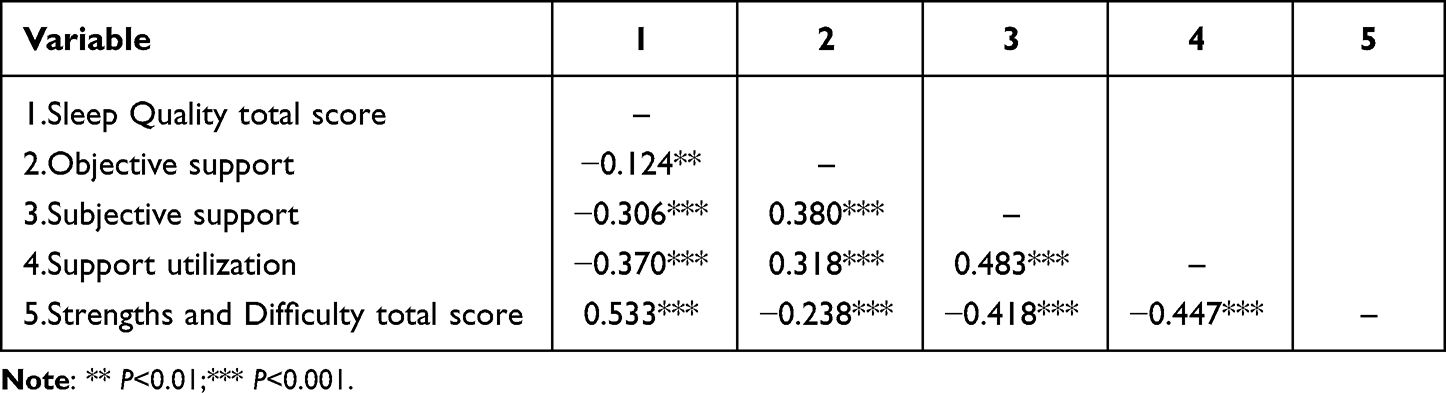 |
Table 3 Questionnaire Scores and Correlation Analysis(N=738) |
Path Analysis
Table 2 shows no correlation between left-behind experience and subjective support and objective support, indicating that subjective and objective support cannot be used as mediating variables. Therefore, in the serial multiple mediation path analysis, we no longer discuss the mediation of subjective and objective support but only discuss the significance of utilization in the path.
The total impact of left-behind experience on behavior problems was significant, as demonstrated in Table 4 and Figure 1 (standard estimate [Std. estimate] =2.18, P 0.001). It was also found that left-behind experience directly impacted behavior problems (Std. estimate =0.946, P=0.015). Additionally, there were substantial indirect impacts of left-behind experience on behavioral issues via sleep quality (Std. estimate = 0.623, p = 0.001) and via utilization then sleep quality (Std. estimate = 0.213, p=0.005). It was also significant that utilization had an indirect influence (Std. estimate = 0.404, p=0.004). In the pathway from left-behind experience to behavior problems, utilization and sleep quality had a mediating effect of 56.7% (Std. estimate of total indirect effect/Std. estimate of total effect=1.239/2.185).
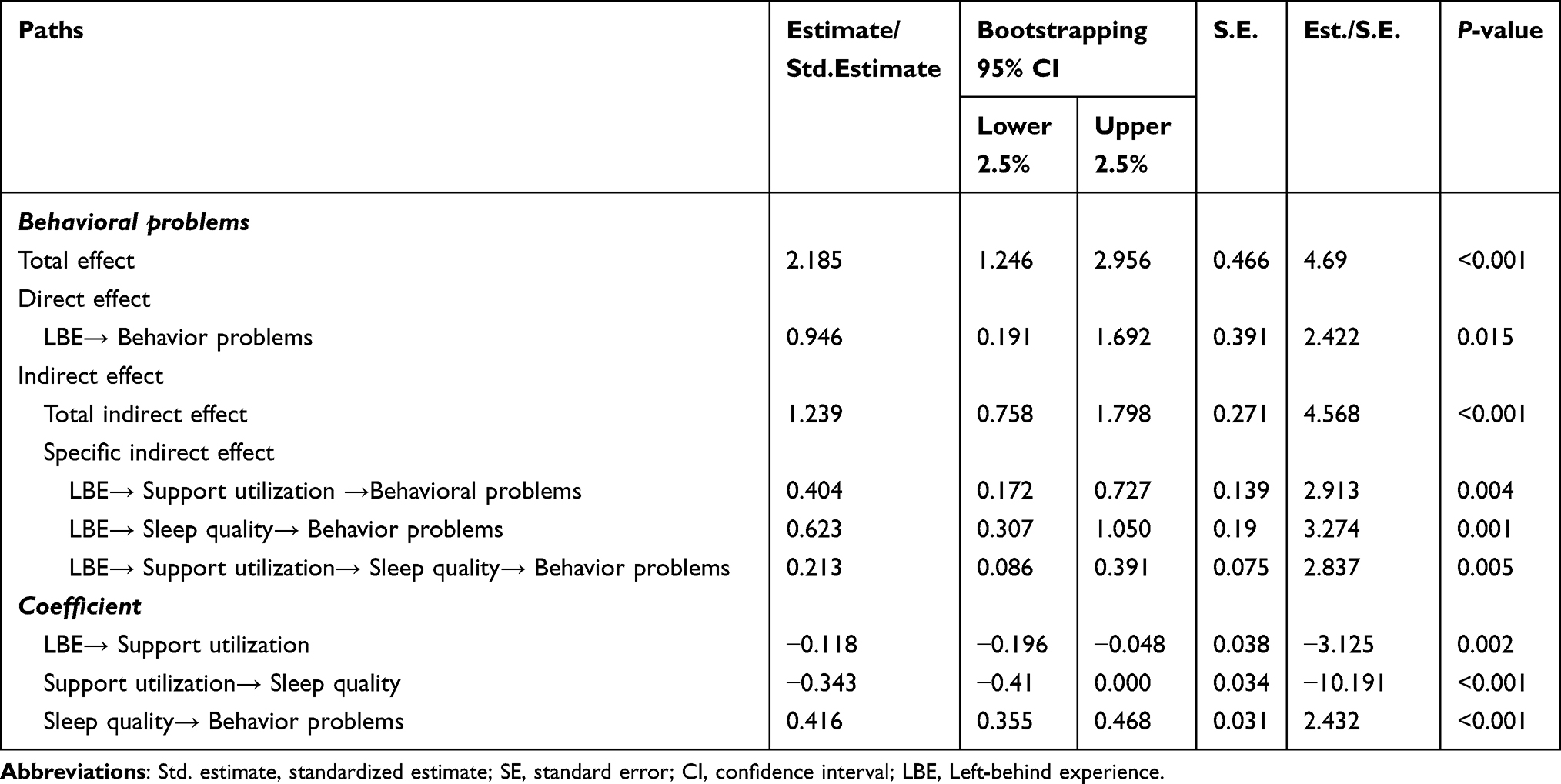 |
Table 4 Results of Path Analysis (N=738) |
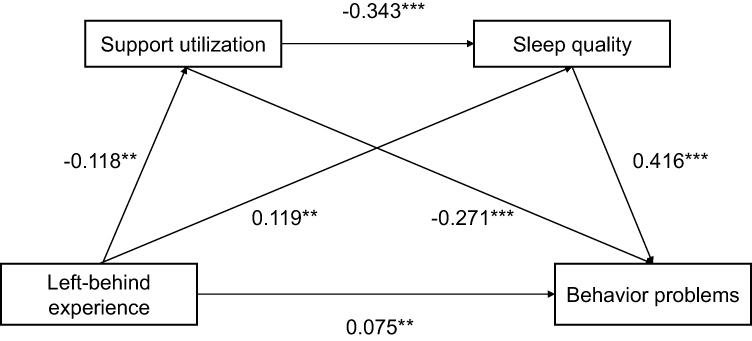 |
Figure 1 Path analysis of left-behind experience, behavior problems, social support utilization, and sleep quality among adolescents (N = 738). The numbers beside the arrows indicate standardized estimates of the direct effect on each pathway. **p < 0.01, ***p<0.001. |
Discussion
This study not only provided epidemiological data on behavior problems of school adolescents, but also used a series of multiple mediation models to elucidate the relationship between left-behind experience, behavior problems, social support utilization, and sleep quality and their underlying mechanisms. We found that the prevalence of behavior problems among adolescents was higher in this study compared to other surveys, that the left-behind experience was significantly associated with sleep quality, social support and behavior problems. And that social support and sleep quality did play a sequential mediating role between the left-behind experience and behavior problems.
The study showed a 26.8% prevalence of behavior problems among the participating adolescents, but a national survey found a 17.6% prevalence of behavior problems among children and adolescents aged 6–16 years.32 We found a greater proportion of these students with left-behind experience experienced behavior problems, which is consistent with the results of a previous cross-sectional survey on emotional and behavior problems among left-behind children in rural China.33 Therefore, we speculate that the high proportion of left-behind children in Anhui Province may lead to the high incidence of behavior problems in our survey.34 Students in higher grades are more likely to have behavior problems than those in lower grades, and we consider academic stress an important factor.35
This study also found that the SSRS scores, PSQI scores, and SDQ scale scores were lower among the left-behind students compared to the adolescents with no left-behind experience, suggesting that the left-behind experience may affect adolescents’ social support, sleep quality, and behavior problems. Contrary to most prior research, we discovered no significant variations in the subjective and objective support measures between the two groups of teenagers with and without the experience of being left behind, except for scores on the social support utilization subscale. A survey on left-behind children in the Philippines also found that the social capital of left-behind children, including family social capital, school social capital, and community social capital, was not low. The study concluded that the popularity of modern communication tools made it easier for parents to communicate with their children, while the help from the school community also improved the social capital of left-behind children.36 This may also help to explain why the subjective and objective support scores of the left-behind adolescents in our study did not differ significantly from those of the non-left-behind experience adolescents, as there is also a great deal of concern for left-behind children in China, and many care activities are carried out by society and schools.37 On why the experience of staying behind is related to the degree of social support utilization, we speculate that this may be because the experience of missing parental companionship gives this group of adolescents a lower sense of security and, thus, a stronger sense of self-protection. Therefore, although society and schools are currently paying much attention to the left-behind children, adolescents with the left-behind experience may be less likely to express their demands in life and less willing to seek help from others, thus having a lower utilization of social support. Previous research supports our speculation that children who lack close parent-child relationships and communication due to parental migration or the influence of single-parent families are not trained in communication skills with others.38,39
Our model showed that social support utilization and sleep quality did play a sequential multiple mediator role between left-behind experiences and behavior problems, and both significantly moderated behavior problems. In the pathway of sequential mediation, the left-behind experience was negatively related to social support utilization, with left-behind experience leading to lower social utilization. And lower social support utilization leading to more severe sleep problems, which exacerbated behavior problems. Previous studies have shown that low social support utilization does reduce sleep quality.40 In a 2014 survey of sleep quality in the Chinese population, social support factors were found to be significantly negatively associated with sleep disturbance.41 Moreover, in a study on improving sleep quality through cognitive-behavioral and positive thinking interventions, behavioral problems were found to improve in adolescent subjects after sleep improvement.42 We were utilizing social support and getting enough sleep each to have their unique effects on behavioral problems, with the latter having a more apparent moderating influence. Therefore, to prevent and improve adolescents’ behavioral problems, we can start by increasing social support utilization and improving sleep quality, especially focusing on the sleep problems of left-behind adolescents.
It is the first series of multiple mediation models examining the relationship between the experience of being left-behind and social support, sleep quality, and behavior problems among adolescent students; previous studies have discussed only the mediating relationships among the three. The mediation models suggest that, in the first step, left-behind experience is associated with lower social support and further decreases sleep quality, thereby exacerbating the risk of behavior problems, with 56.7% of the overall mediators in this manner. As a result, in addition to providing children who experience left behind with greater outside support, it’s crucial to teach them how to use the resources available, encourage the use of social support systems, and emphasize bettering sleep hygiene as a critical strategy for reducing behavior problems.
The study also has some limitations. First, this study is only a cross-sectional study and does not clearly infer the directionality of the relationship between social support utilization, sleep quality, and behavior problems; a follow-up longitudinal investigation is necessary and meaningful to clarify better the causal connection. Second, because this study used a questionnaire survey as its primary research method, findings analysis may be impacted by subjective assessment and the possibility that students covered up sleep and behavior issues. Third, because this study mainly focused on the central part of China and used a small sample of high schools, the findings might not be generalizable to other regions. In the later stage, the sample size should continue to be expanded, and further investigations should be conducted on students at various learning stages, to more accurately identify students and intervene to reduce the risk of behavior problems.
Conclusion
In summary, this is the first examination of a series of multiple mediating models between the left-behind experience and social support, sleep quality, and behavior problems among school-aged adolescents. Most previous studies have only discussed the prevalence of behavior problems among left-behind children and the factors that influence them, with little discussion of the specific mechanisms of why left-behind children are more likely to have behavior problems. In this study, we found that social support and sleep quality were indeed influential factors for behavior problems, which is the same as previous results in the literature, but we found that the left-behind experience was only related to social support utilization, which is a new finding. We also explored how social support utilization and sleep quality play a role in the pathway of left-behind experiences leading to behavior problems, and constructed a model of serial mediation to elucidate a possible mechanism of influence, which provides new ideas to help adolescents with left-behind experiences better. The findings suggest that compared to students without the left-behind experience, left-behind students have poorer social utilization, and the poorer the social utilization, the poorer the sleep quality, and ultimately the more severe the degree of behavior problems. Considering school adolescents’ immature psychological development, we suggest that we should pay more attention to the students’ psychological state and improve the utilization of social support in addition to giving more external social support. And also pay attention to their sleep problems to reduce the occurrence of behavioral problems.
Abbreviations
WHO, World Health Organization; LBE, Left-behind experience; SDQ, Strengths and Difficulties Questionnaire; PSQI, Pittsburgh Sleep Quality Index scale; SSRS, Social support rating scale; SD, Standard deviations; CI, confidence interval; Std. estimate, standardized estimate; SE, standard error; Est, estimate.
Data Sharing Statement
As this study is still ongoing, the raw datasets for the current study will not be available until the end of this research project. Please contact the first author (Menglin Ge, [email protected]) for raw data requests.
Ethics Approval and Informed Consent
This survey was approved by the Ethics Committee of Chaohu Hospital, Anhui Medical University (2019-kyxm-012). All study procedures were in strict compliance with the principles of the Declaration of Helsinki. We informed the participants that the data collected in this survey will be used for research purposes only and will be kept strictly confidential to ensure that they fully understand the content and safety of the study. This school survey was conducted with informed consent from the school, participating students and their guardians (parents or other caregivers) prior to the survey.
Acknowledgments
We thank all the participants who volunteered to participate in this study.
Funding
This study was supported by the National Natural Science Foundation of China (81801341), China International Medical Exchange Foundation (Z-2018-35-2002), the Anhui Provincial Key R&D Programme (202004j07020030), and Interdisciplinary project of clinical and basic disciplines of Anhui Medical University (No. 2101025103).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kashala E, Elgen I, Sommerfelt K, Tylleskar T. Teacher ratings of mental health among school children in Kinshasa, Democratic Republic of Congo. Eur Child Adolesc Psychiatry. 2005;14(4):208–215. doi:10.1007/s00787-005-0446-y
2. Weitzman C, Wegner L, Blum NJ. Promoting optimal development, screening for behavioral and emotional problems. Pediatrics. 2015;135(2):384–395. doi:10.1542/peds.2014-3716
3. Philipp J, Zeiler M, Waldherr K, et al. Prevalence of emotional and behavioral problems and subthreshold psychiatric disorders in Austrian adolescents and the need for prevention. Soc Psychiatry Psychiatr Epidemiol. 2018;53(12):1325–1337. doi:10.1007/s00127-018-1586-y
4. Wang JN, Liu L, Wang L. Prevalence and associated factors of emotional and behavioural problems in Chinese school adolescents, a cross-sectional survey. Child Care Health Dev. 2014;40(3):319–326. doi:10.1111/cch.12101
5. Darney D, Reinke WM, Herman KC, Stormont M, Ialongo NS. Children with co-occurring academic and behavior problems in first grade, distal outcomes in twelfth grade. J Sch Psychol. 2013;51(1):117–128. doi:10.1016/j.jsp.2012.09.005
6. Jones P, Rodgers B, Murray R, Marmot M. Child development risk factors for adult schizophrenia in the British 1946 birth cohort. Lancet. 1994;344(8934):1398–1402. doi:10.1016/S0140-6736(94)90569-X
7. Astrup A, Pedersen CB, Mok PLH, Carr MJ, Webb RT. Self-harm risk between adolescence and midlife in people who experienced separation from one or both parents during childhood. J Affect Disord. 2017;208:582–589. doi:10.1016/j.jad.2016.10.023
8. Jingzhong Y, Lu P. Differentiated childhoods, impacts of rural labor migration on left-behind children in China. J Peasant Stud. 2011;38(2):355–377. doi:10.1080/03066150.2011.559012
9. Duan CR, Yang K, Wang Y. Investigation and research on rural left-behind children. J Xuehai. 2005;6:25–29.
10. Duan CR, Zhou FL. Studies on left behind children in China. Popul Res. 2005;26(01):29–36.
11. Zhou YM, Zhao CX, Qi YJ, et al. Emotional and behavioral problems of left-behind children in impoverished Rural China, A comparative cross-sectional study of fourth-grade children. J Adolesc Health. 2020;67(5s):S48–s54. doi:10.1016/j.jadohealth.2020.06.016
12. Li Y. A Study on the Relationship Among Loneliness, Sleep Quality and Learning Burnout Among Left-Behind Children [Dissertation]. Hebei Normal University; 2018.
13. Luo J, Wang W, Gao W-B. Review of the studies on rural left-behind children in China. Adv Psychol Sci. 2009;17(05):990.
14. Sun SX, Guan YH, Qin YY, Zhang L, Fan F. Social support and emotional-behavioral problems: resilience as a mediator and moderator. J Clin Psychol. 2013;21(1):114–118.
15. Kosticova M, Husarova D, Dankulincova Z. Difficulties in getting to sleep and their association with emotional and behavioural problems in adolescents, does the sleeping duration influence this association? Int J Environ Res Public Health. 2020;17:5. doi:10.3390/ijerph17051691
16. Gregory AM, Sadeh A. Sleep, emotional and behavioral difficulties in children and adolescents. Sleep Med Rev. 2012;16(2):129–136. doi:10.1016/j.smrv.2011.03.007
17. Kent de Grey RG, Uchino BN, Trettevik R, Cronan S, Hogan JN. Social support and sleep, A meta-analysis. J Health Psychology. 2018;37(8):787. doi:10.1037/hea0000628
18. Stafford M, Bendayan R, Tymoszuk U, Kuh D. Social support from the closest person and sleep quality in later life, evidence from a British birth cohort study. J Psychosom Res. 2017;98:1–9. doi:10.1016/j.jpsychores.2017.04.014
19. World Health Organization. Health topics: adolescent health Overview. Available from: https://www.who.int/health-topics/adolescent-health#tab=tab_1.
20. Han L, Zhao SY, Pan XY, Liao CJ. The impact of students with left-behind experiences on childhood, The relationship between negative life events and depression among college students in China. Int J Soc Psychiatry. 2018;64(1):56–62. doi:10.1177/0020764017739332
21. Goodman R. The Strengths and Difficulties Questionnaire, a research note. J Child Psychol Psychiatry. 1997;38(5):581–586. doi:10.1111/j.1469-7610.1997.tb01545.x
22. Goodman R, Ford T, Simmons H, Gatward R, Meltzer H. Using the Strengths and Difficulties Questionnaire (SDQ) to screen for child psychiatric disorders in a community sample. Br J Psychiatry. 2000;177:534–539. doi:10.1192/bjp.177.6.534
23. Goodman R. Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry. 2001;40(11):1337–1345. doi:10.1097/00004583-200111000-00015
24. Du Y, Kou J, Coghill D. The validity, reliability and normative scores of the parent, teacher and self report versions of the Strengths and Difficulties Questionnaire in China. Child Adolesc Psychiatry Ment Health. 2008;2(1):8. doi:10.1186/1753-2000-2-8
25. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index, a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
26. Liu G, Tang M, Hu L. Reliability and validity of the Pittsburgh Sleep Quality Index. Asian J Psychiatr. 1996;29(2):103–107.
27. Zheng B, Li M, Wang KL, Lv J. Analysis of the reliability and validity of the Chinese version of Pittsburgh Sleep Quality Index among medical college students. Beijing da Xue Xue Bao Yi Xue Ban. 2016;48(3):424–428.
28. Xiao SY. The theoretical basis and research application of social support rating scale. J Clin Psychol Med. 1994;2:98–100.
29. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891. doi:10.3758/BRM.40.3.879
30. Wen Z, Ye B. Analyses of mediating effects, the development of methods and models. Adv Psychol Sci. 2014;22(5):731–745. doi:10.3724/SP.J.1042.2014.00731
31. Steeger CM, Gondoli DM. Mother-adolescent conflict as a mediator between adolescent problem behaviors and maternal psychological control. Dev Psychol. 2013;49(4):804–814. doi:10.1037/a0028599
32. Cui Y, Li F, Leckman JF, et al. The prevalence of behavioral and emotional problems among Chinese school children and adolescents aged 6-16, a national survey. Eur Child Adolesc Psychiatry. 2021;30(2):233–241. doi:10.1007/s00787-020-01507-6
33. Zhou SJ, Zhang LG, Wang LL, et al. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur Child Adolesc Psychiatry. 2020;29(6):749–758. doi:10.1007/s00787-020-01541-4
34. Ministry of Civil of the People’s Republic of China. Chart, Data of rural left-behind children in 2018; 2018. Available from: https://www.mca.gov.cn/article/gk/tjtb/201809/20180900010882.shtml.
35. Qin Y, Zhao Z. Much? Difficult? Tired?—A survey research on primary and middle school students workload in China. J Curric Teach Mater Method. 2014;34:42–49.
36. Tolentino MP, Arcinas MM. Social capital of left-behind children, Determinants and association with school performance. Asia-Pac Soc Sci Rev. 2018;18(2):16–33.
37. China Social News. Care for left-behind children in rural areas, from a family matter to a national matter; 2018. Available from: https://www.mca.gov.cn/article/xw/mtbd/201810/20181000012499.shtml.
38. Mmari K, Marshall B, Hsu T, Shon JW, Eguavoen A. A mixed methods study to examine the influence of the neighborhood social context on adolescent health service utilization. BMC Health Serv Res. 2016;16(1):433. doi:10.1186/s12913-016-1597-x
39. Ghimire S, Singh DR, Nath D, Jeffers EM, Kaphle M. Adult children’s migration and well-being of left behind Nepalese elderly parents. J Epidemiol Glob Health. 2018;8(3–4):154–161. doi:10.1016/j.jegh.2018.07.004
40. Grey I, Arora T, Thomas J, Saneh A, Tohme P, Abi-Habib R. The role of perceived social support on depression and sleep during the COVID-19 pandemic. Psychiatry Res. 2020;293:113452. doi:10.1016/j.psychres.2020.113452
41. Kong LM, Zhang LY, Zhang QJ. A study on relationship of Chinese peoples’ sleep quality and social support and its related factors. World J of Sleep Medicine. 2014;1(02):65–70.
42. Blake MJ, Snoep L, Raniti M, et al. A cognitive-behavioral and mindfulness-based group sleep intervention improves behavior problems in at-risk adolescents by improving perceived sleep quality. Behav Res Ther. 2017;99:147–156. doi:10.1016/j.brat.2017.10.006
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
HIV-Related Stigma Among Pregnant Adolescents: A Qualitative Study of Patient Perspectives in Southwestern Uganda
Kabunga A, Nabasirye CK, Kigingo E, Namata H, Shikanga EM, Udho S, Auma AG, Nabaziwa J, Tumwesigye R, Musinguzi M, Okalo P, Acup W
HIV/AIDS - Research and Palliative Care 2024, 16:217-227
Published Date: 16 May 2024
Glymphatic System in Adolescents with Major Depressive Disorder: No Dysfunction and No Association with Poor Sleep Quality
Zhang J, Zou X, Cai X, Zou M, Li H, Feng R
Nature and Science of Sleep 2025, 17:2155-2164
Published Date: 10 September 2025
Psychological Resilience and Sleep Quality Among the Elderly: The Mediating Role of Social Support
Li J, Zhang J, Hou Y, Cui Y, Wang Q, Ouyang A, Cai M, Hua Y
Nature and Science of Sleep 2025, 17:2469-2483
Published Date: 3 October 2025