Back to Journals » Journal of Inflammation Research » Volume 18
Therapeutic Potential of Acupuncture in Knee Osteoarthritis: Clinical Efficacy and Mechanistic Insights
Authors Yao K ![]() , Shamim MF
, Shamim MF ![]() , Xia J, Liu TT, Guo Y, Lin X
, Xia J, Liu TT, Guo Y, Lin X ![]()
Received 8 March 2025
Accepted for publication 21 August 2025
Published 5 September 2025 Volume 2025:18 Pages 12169—12190
DOI https://doi.org/10.2147/JIR.S526890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Yan Chen
Kaifang Yao,1,* Md Forhad Shamim,1,* Jiaqi Xia,1 Tingting Tingting Liu,1 Yi Guo,1– 3 Xiaowei Lin1– 3
1Research Center of Experimental Acupuncture Science, School of Acupuncture & Moxibustion and Tuina, Tianjin University of Traditional Chinese Medicine, Tianjin, 301617, People’s Republic of China; 2Tianjin Key Laboratory of Modern Chinese Medicine Theory of Innovation and Application, School of Traditional Chinese Medicine, Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 3National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, Tianjin, 301617, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yi Guo, School of Traditional Chinese Medicine, Tianjin University of Traditional Chinese Medicine, No. 10 Poyang Lake Road, Tuanbo New Town, Jinghai District, Tianjin, 301617, People’s Republic of China, Tel +86-22-2748-5189, Email [email protected] Xiaowei Lin, School of Traditional Chinese Medicine, Tianjin University of Traditional Chinese Medicine, No. 10 Poyang Lake Road, Tuanbo New Town, Jinghai District, Tianjin, 301617, People’s Republic of China, Tel +86-22-2748-5189, Email [email protected]
Abstract: Knee osteoarthritis (KOA) is a prevalent degenerative joint disorder that significantly compromises joint function due to the progressive degradation of cartilage and persistent inflammation. Acupuncture is an effective technique that has been employed in Traditional Chinese Medicine to treat KOA. This review aims to summarize 21 randomized controlled trials (RCTs) and mechanistic research to investigate acupuncture’s clinical efficacy and biological mechanisms in KOA. The literature was sourced from various databases, including PubMed, CNKI, and Google Scholar. Clinical data revealed that acupuncture monotherapy significantly reduces pain intensity (Visual Analogue Scale reductions: 32– 54%) and enhances functional capacity (WOMAC score improvements: 25– 40%). Furthermore, the combination of acupuncture with moxibustion or electroacupuncture induced synergistic improvements. Mechanistically, acupuncture modulates KOA pathophysiology by suppressing NF-κB-mediated pro-inflammatory cytokines, inhibiting chondrocyte apoptosis (caspase-3 downregulation) while activating autophagy (LC3-II/Beclin-1 upregulation), rebalancing cartilage metabolism by increasing aggrecan/COL2A1 synthesis and MMP-13 inhibition, as well as by attenuating pain transmission through μ-opioid receptor activation and central descending inhibition. These multimodal interventions position acupuncture as a dual-target treatment, mitigating symptoms while inhibiting structural degradation. However, despite promising evidence, further research is warranted for protocol standardization and long-term outcome validation. This review highlights acupuncture’s scientific legitimacy as a non-pharmacological approach for the integrated management of KOA, combining traditional methods with modern mechanistic insights.
Keywords: acupuncture, electroacupuncture, knee osteoarthritis, knee osteoarthritis mechanism, Traditional Chinese Medicine
Introduction
KOA is a chronic joint disorder and the predominant form of osteoarthritis (OA), characterized by the progressive deterioration of articular components, including cartilage, synovium, subchondral bone, menisci, ligaments, and infrapatellar fat pad (IFP).1–5 Epidemiological studies have indicated that KOA affects about 654 million people worldwide, specifically affecting the elderly population over 45 years old (30%).6 Its clinical manifestations include pain, swelling, morning stiffness, and limited functional activities.7 The incidence of KOA has increased annually because of an aging population and rising obesity rates.8 KOA incidence has been related to certain known risk factors, such as gender (more common in females), age (> 50), physical constitution, genetic factors, etc.7,9,10 Moreover, certain medical diseases, such as hypertension and type 2 diabetes, are significant risk factors for KOA.11 Its prevalence rate in women is 1.8 times that in men.12 KOA pathogenesis includes complex interactions between mechanical stress, low-grade inflammation, and metabolic dysregulation.13–17 The breakdown of articular cartilage, due to an imbalance in extracellular matrix (ECM) remodeling and inflammation, is the predominant cause of joint discomfort in patients. Compared to rheumatoid arthritis (RA), the inflammation in KOA is persistent and low-grade, primarily associated with the innate immune system and inflammatory mediators.18 Pain is one of the main manifestations and disabling symptoms of KOA-associated inflammation. Pain and limited mobility can substantially promote depression and anxiety in patients.10,19 Research suggests that the use of antidepressants can help reduce pain sensitization in KOA patients.20 The clinical guidelines for KOA treatment include medication, non-drug interventions, and surgical intervention.21 Knee replacement is the predominant intervention for KOA; however, it is associated with significant adverse effects, including elevated costs, substantial risks, infection susceptibility, and postoperative prosthesis displacement. Therefore, it is recommended only for the advanced stage.6
In recent years, there has been an increasing interest in complementary and integrative therapies, such as acupuncture, a traditional Chinese medicine (TCM), which has garnered significant interest for its efficacy and cost-effectiveness in the treatment of KOA.22,23 Acupuncture can reduce inflammation, relieve pain, and improve joint function by stimulating specific acupoints, addressing the limitations of conventional analgesics.24 Compared with traditional analgesics and nonsteroidal anti-inflammatory drugs such as acetaminophen and chondroitin sulfate, different acupuncture techniques, like manual acupuncture (MA), electroacupuncture (EA), etc., have fewer side effects, are easy to operate, and are highly safe.25 This review summarizes the latest reports on KOA-associated chemical and pathological changes, as well as clinical research reports on the efficacy of acupuncture in treating KOA. Furthermore, the mechanisms of acupuncture in treating KOA were also reviewed from multiple perspectives.
Materials And Methods
Literature Search
A systematic search was carried out across PubMed and Google Scholar from 1994 to 2024 using the following keywords: “Acupuncture”, “Electroacupuncture”, “Moxibustion”, “Traditional Chinese Medicine”, “Knee Osteoarthritis”, and related terms in English. Furthermore, Boolean operators “AND”, “OR”, and “NOT” were used to refine the search (Table 1).
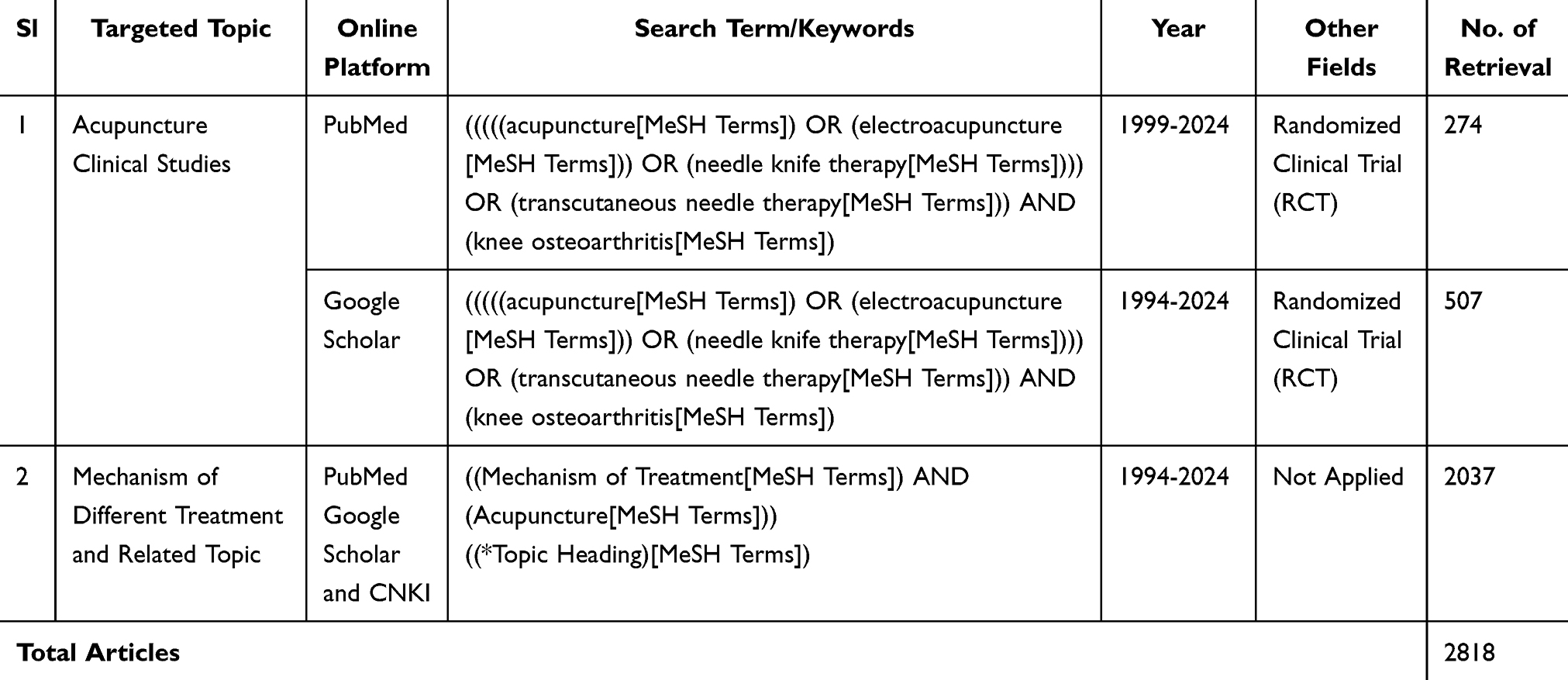 |
Table 1 Article Search Strategy |
Study Selection and Data Extraction
The literature was screened for population, intervention, study design, outcome, etc. Then, based on screening results, the articles (a) on KOA, (b) explaining treatment efficacy randomized controlled trials (RCTs) on Human Subjects], (c) related to mechanism and other terminologies-scientific articles, etc., (d) those published between 1994 and 2024, (e) in English language, and (f) with complete available texts were included in this study. Furthermore, articles that did not meet the above inclusion criteria, which lacked results, were duplicates or retracted, had broken links, missing information, or lacked organization in writing, and were excluded.
Study Selection and Description
A total of 2818 articles were read, including 781 RCTs, of which 21 were selected after screening, removing duplicates, and reviewing titles and abstracts to explain treatment efficacy. An additional 1918 articles were acquired to evaluate the mechanisms and related topics (Figure 1). These selected studies, published over the last 30 years (1994–2024), analyzed 3176 KOA patients aged 30 to 91. The selected data ensured the inclusion of the most recent findings.
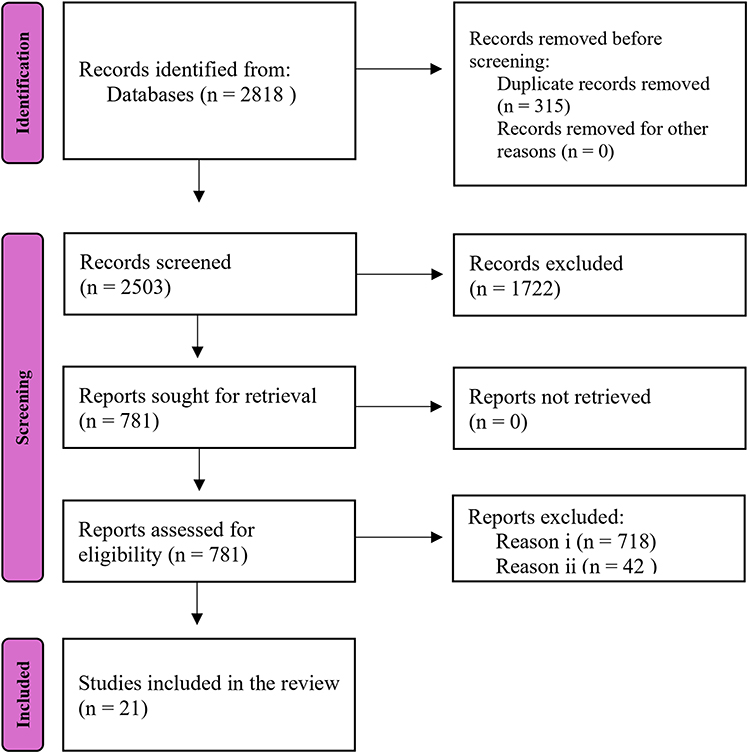 |
Figure 1 Article Selection Process-Flow Diagram. |
Risk of Bias Assessment Results
The selected articles’ bias risk was assessed using Cochrane’s “Risk of Bias 2” Version-9 Excel tool for RCTs (Figure 2). The overall report is shown in Figure 2A, risk indicators are presented in Figure 2B, and the percentage of the overall Risk of Bias is depicted in Figure 2C.
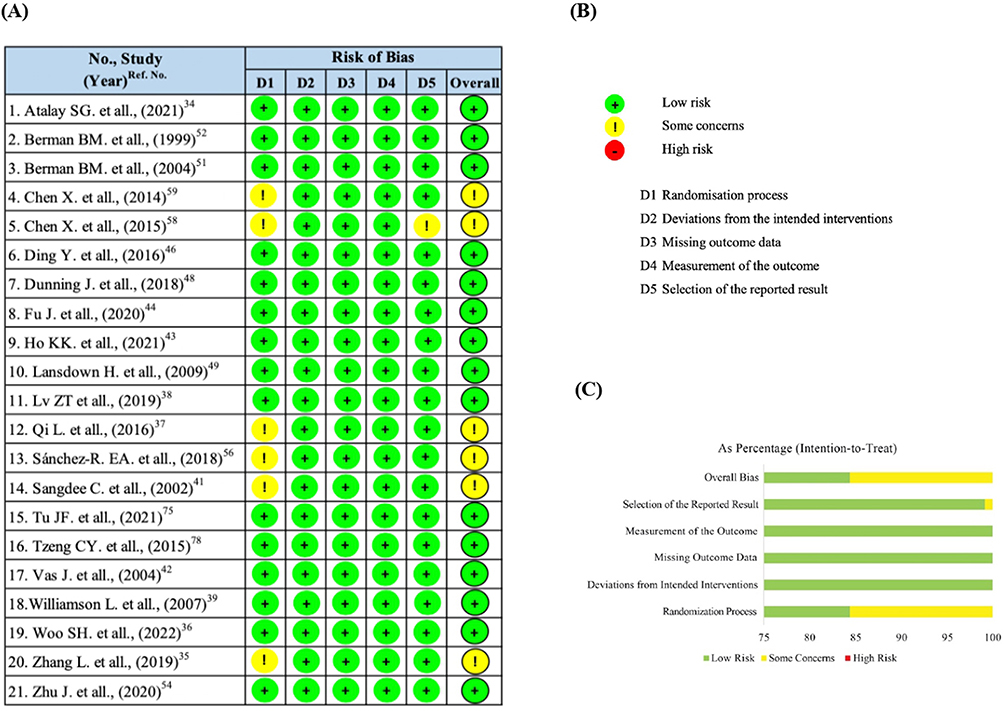 |
Figure 2 (A) Overall Risk of Bias (Assessed by Cochrane’s RoB-2 Excel Tool, Version 9). (B) Risk of Bias Indicators. (C) Percentage of Overall Risk of Bias. |
Pathological Changes and Pathogenesis of KOA
Cartilage Degradation
The main starting feature of KOA is the breakdown of articular cartilage.26 The knee joint cartilage is a smooth, avascular substance that facilitates low-friction movement.27 In KOA, mechanical stress and biochemical imbalances destroy chondrocytes, the cells responsible for maintaining cartilage integrity.27,28
Subchondral Bone Remodeling
As cartilage degrades, the underlying subchondral bone becomes progressively exposed to mechanical stress. This results in alterations to the bone structure, including sclerosis (hardening), the development of osteophytes (bone spurs), and modifications in bone marrow lesions.29 These changes promote joint stiffness and pain, further aggravating the degenerative process.
Synovial Inflammation
In response to cartilage damage, the synovial membrane, which lines the joint, becomes inflamed, and this inflammation is called synovitis.30 This chronic inflammation intensifies cartilage degradation by releasing pro-inflammatory mediators and degrading enzymes into the joint space.30 Synovitis is also associated with joint swelling, effusion, and increased pain sensitivity.31
Loss of Joint Homeostasis
In healthy joints, there is a specific homeostasis between cartilage degradation and regeneration. In KOA, this balance is disturbed, resulting in an increased rate of degeneration.10 Factors such as aging, genetic predisposition, mechanical overload (eg, obesity, malalignment, repetitive joint use), and metabolic disorders promote this imbalance, inhibiting the joint’s ability to repair itself.10,32
Pain and Functional Decline
With the progression of joint structural changes, KOA patients experience chronic pain, primarily due to mechanical stress on the bone, synovial inflammation, and nerve sensitization.10,17 The pain, together with joint stiffness and reduced range of motion, promotes functional deterioration and limited mobility, which significantly affect the quality of life.10,23 The literature suggests that the IFP and synovium are functionally interconnected structures in OA pathogenesis, where their inflammatory crosstalk may facilitate peripheral and central sensitization mechanisms that contribute to the progression of pain.33
Clinical Research Progress on Acupuncture Treatment of KOA
Evaluation Indicators
In clinical research on KOA treatment, several key indicators are commonly used to assess the efficacy and safety of acupuncture, including the Visual Analog Scale (VAS),34–47 Western Ontario and McMaster University Osteoarthritis Index Scale (WOMAC),34–44,48–53 Oxford Knee Scores Scale (OKS),39,49,54,55 Numeric Rating Scale (NRS),56,57 Knee Injury and Osteoarthritis Outcome Score (KOOS),58–60 Short Form Health Survey of 36 Questions (SF-36),34,35,40,44,51,61 and Arthritis Life Quality Measurement Scale-Simplified Scale (AIMS2-SF).43,62,63 Furthermore, some parameters such as the Beck Anxiety Inventory (BAI) for anxiety measurement62,64,65 are used with the Beck Depression Inventory (BDI) for depression,62,64,66 the Mankin score for cartilage damage assessment,67,68 and Conditioned Pain Modulation (CPM)38 for assessing the recovery and adaptive changes of joints under continuous passive movement, a crucial indicator of chronic pain.57,69,70 Since KOA involves inflammatory processes, biochemical markers of inflammation are often monitored to assess the impact of acupuncture, such as C-reactive protein (CRP) and Erythrocyte Sedimentation Rate (ESR).38 Pro-inflammatory cytokines, such as Interleukin (IL)-1β, Tumor Necrosis Factor (TNF)-α, and Interleukin-6 (IL-6), are commonly elevated in KOA and can be modulated by acupuncture and EA.67 Imaging techniques, including X-rays or Magnetic Resonance Imaging (MRI) scans,14 can also be employed to assess structural changes in the knee joint over time, such as cartilage thickness, osteophyte formation, and joint space narrowing.
Acupoint Selection for KOA
Similar to other disorders treated by TCM, KOA is alleviated by classifying the type of syndrome, which is based on the disease’s underlying etiologies and the patient’s distinct symptoms.71 The commonly used acupoints and acupuncture methods are depicted in Figure 3.
 |
Figure 3 Local Acupoints & Acupuncture Treatment Parameters for KOA. Abbreviations: NM, Name of Method; DS, Duration Per Session; RS, Required Session; RD, Required Duration; SA, Special Attention. |
Commonly Used Local Acupoints
Dubi (ST35) is located just below the patella and is commonly used for knee pain, and helps to expel cold and dampness from the joint. Xuehai (SP10) is targeted to cool the blood and dispel heat to help alleviate inflammation and redness in the knee. Yanglingquan (GB34) is an essential point for musculoskeletal disorders; it helps to clear dampness and benefits the tendons and ligaments. Yinlingquan (SP9), Liangqiu (ST34), and Zusanli (ST36) tonify Qi and blood, strengthen the body’s defenses, and dispel cold and dampness. Weizhong (BL40) clears heat from the lower body and benefits the knee joint.72–75
Commonly Used Local Extra Points
Xiyan (EX-LE5), Heding (EX-LE2), and Neixiyan (EX-LE4): Located on either side of the patellar ligament. These points directly target the knee joint and help to unblock Qi and blood stagnation.72–74,76
Ashi Points
Ashi points refer to tender spots near the knee joint corresponding to local pain and swelling. They are frequently selected alongside conventional acupoints and activated to deliver immediate treatment to the impacted region.74
Distal Supporting Acupoints
Hegu (LI4) and Taichong (LV3); these two points combined are known as the “Four Gates” and regulate the flow of Qi and blood throughout the body, relieving pain and stagnation. Fengshi (GB 31), Waiqiu (GB 36), Xuanzhong (GB 39), Zulinqi (GB 41), Sanyinjiao (SP6): Strengthens the spleen, liver, and kidneys. Taixi (KI3): Tonifies the kidney, helps expel cold, and benefits the knees.72,73
Acupuncture Intervention Methods & Parameters
Manual Acupuncture
In MA, fine needles are inserted with the hands, often used for their analgesic and anti-inflammatory effects in treating joint pain. The duration of MA typically spans 20 to 30 minutes per session, with treatments administered 2 to 3 times weekly for 4 to 6 weeks. The frequency and length fluctuate based on the intensity of symptoms. The depth and angle of insertion are contingent upon the individual acupoint and the patient’s reaction. General acupuncture effectively reduces mild to moderate KOA-related pain and inflammation, with a shorter recovery time and fewer side effects compared to invasive treatments.39,42,49,51,52,54,59,61
Electroacupuncture
The EA involves inserting needles at specific acupoints and attaching them to an electrical device that generates continuous low-frequency electrical pulses. This approach exerts a more powerful stimulation on the neurological system than MA. Sessions generally last 20–40 minutes and are conducted 2–3 times per week for 4–8 weeks. The electrical frequency and intensity are adjustable, with 2–4 Hz being employed for chronic pain alleviation and 80–120 Hz for acute pain. Low-frequency, high-intensity stimulation is effective for chronic pain, while high-frequency, low-intensity stimulation is better suited for acute pain relief.37,38,41,46,77,78
Warm Needle Acupuncture (WNA)
This type of acupuncture involves heating mugwort (moxa) to enhance its therapeutic effects. A standard session takes 30–40 minutes, with treatment administered 2–3 times weekly for 6–8 weeks. The heat intensity is calibrated according to the patient’s comfort level. Furthermore, WNA particularly benefits patients with cold-related joint pain or stiffness.40,79
Small Needle Knife (SNK)
The SNK is often employed in cases where scar tissue or fibrous bands restrict movement. This technique is performed in short sessions (10–20 minutes) and may require only 1–2 sessions for significant improvements. However, follow-up treatments are often necessary to maintain results. Moreover, it is significantly effective for breaking down fibrotic tissue and restoring mobility in severe KOA cases, especially in patients who do not respond well to conservative treatments.54
Combination Therapy
The integration of acupuncture procedures, such as EA or WNA, with complementary therapies like cupping, bloodletting, and moxibustion can provide more comprehensive pain relief, reduce stiffness, and improve joint function. Furthermore, combining these with conventional therapies, such as physical or pharmacological interventions, could considerably improve outcomes, particularly for patients with advanced KOA or those unresponsive to monotherapies.42 Zhang et al, Lansdown et al, and Sangdee et al compared usual pharmacological non-steroidal anti-inflammatory (NSAID) drugs as Usual care with MA and EA. They revealed that the efficacy of MA and EA co-treatment on VAS and WOMAC, overall pain and quality of life scores, was higher than the usual care, where the combination with EA showed the highest efficacy.35,41,49 Zhang et al40 further combined WNM and Usual care, and indicated a similar higher efficacy in the combined treatment group. Moreover, the manual therapy with electric dry needles also significantly reduced the WOMAC analysis.48 The co-treatment with acupuncture and Moxibustion reduces articular cartilage thickness observed in CT imaging of patients.80 This co-treatment down-regulated serum cyclophosphamide (CTX-I), Matrix Metalloproteinase-9 (MMP-9), Tissue Inhibitor of Metalloproteinase-1 (TIMP-1) levels, and MMP-9/TIMP-1 ratio. Whereas it upregulated the levels of serum Insulin-like Growth Factor-1 (IGF) and Bone Gamma-Carboxyglutamic Acid-Containing Protein (BGP) to regulate bone metabolism and improve the KOA damage in patients.80–83 Acupuncture combined with cupping and bloodletting also indicated better efficacy in multiple clinical studies.74,84–87 Zhuang et al88 combined acupuncture with Sodium hyaluronate intra-articular injection in 150 patients and found substantially reduced pain levels compared to the medicated group (p < 0.05). Certain clinical research indicates that the combination of acupuncture and physiotherapy could accelerate the reduction of KOA pain and alleviate other symptoms.30,34,81,84,89–92
Summary of Clinical Efficacy of Acupuncture Clinical Research in Treating KOA
The review of the selected studies revealed that patients receiving acupuncture experienced significant pain relief compared to those receiving sham acupuncture or standard care.34–46 The most frequently utilized clinical outcome measure, VAS with NRS, which assesses pain on a 0–10 range, has demonstrated a significant reduction of 2–4 points on the pain scale after combining traditional treatment with acupuncture.34–46 Furthermore, WOMAC, comprising multiple subscales to measure related clinical outcomes such as assessing pain, stiffness, and physical function, also indicated similar findings.34–44,48–52 In WOMAC, acupuncture has been linked with improvements in joint mobility and function, particularly in chronic KOA patients.93 Figure 3 illustrates the application parameters of different acupuncture methods. This review summarizes the characteristics of all selected clinical studies and the clinical efficacies by integrating the changes in parameters employed to assess clinical outcomes of acupuncture treatment for KOA (Table 2).
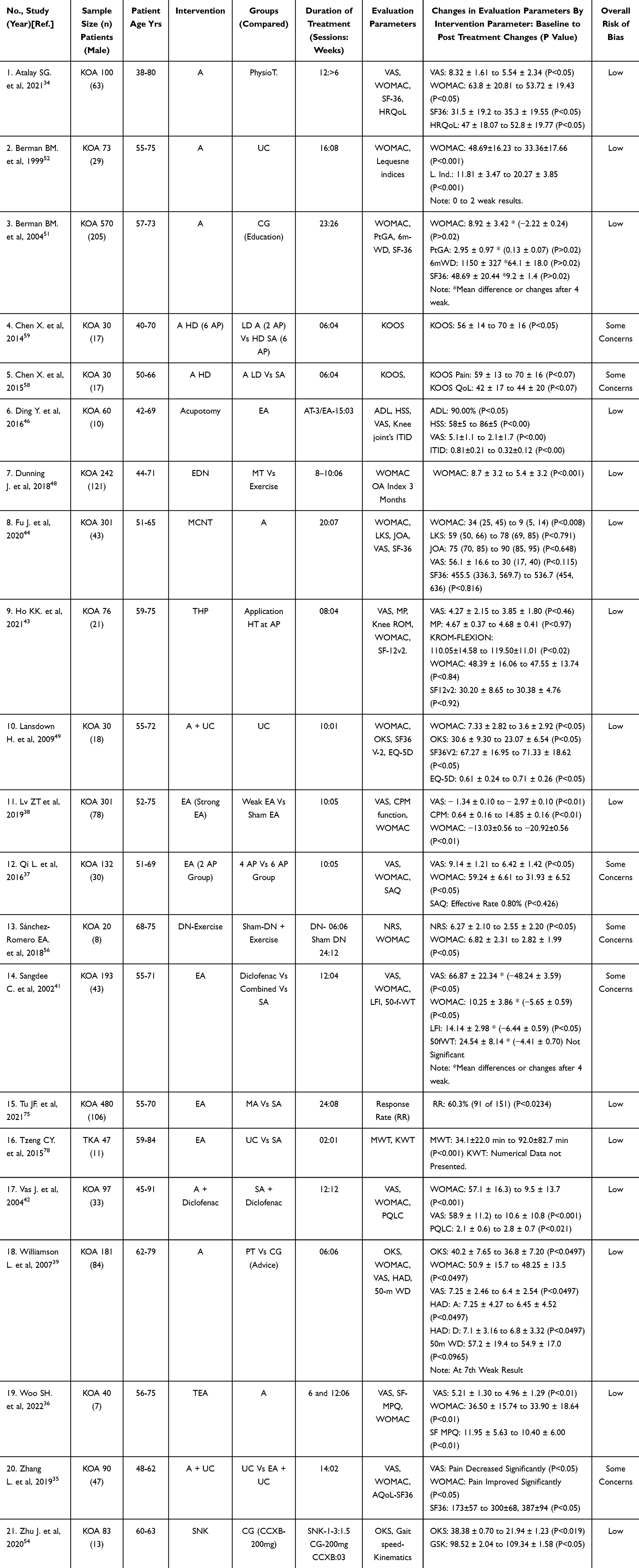 |
Table 2 Characteristics and Summery Results of Selected Clinical Studies |
Basic Research Progress in The Mechanism of Acupuncture Treatment of KOA
Immune Perspective
Reduction of Inflammatory Response
Acupuncture can regulate the activity of immune cells, such as regulatory T cells, inhibit overactive immune responses, and reduce inflammatory damage to joints.94 Immune repertoire sequencing technology has been employed to analyze the diversity of peripheral blood T cell receptors in KOA patients and the gene expression of peripheral blood neutrophils in mild to moderate KOA patients before and after 8 weeks of EA treatment. The results revealed that EA treatment reduced the serum proinflammatory factors IL-8 and IL-18, along with MMP-3 and MMP-13. Furthermore, Transcriptomics analysis indicated that after EA treatment, the expression of Chemokine (C-X-C motif) Ligand 2 (CXCL2), Interferon Regulatory Factor 8 (IRF8), and Platelet Endothelial Aggregation Receptor 1 (PEAR1) was downregulated, suggesting that it improves the inflammatory response of KOA by regulating T-cell homeostasis.94 The aggregation of M1 macrophages in joints and synovium accelerates KOA, and inducing M2 macrophages to secrete IL-4 and IL-10 can improve symptoms.95 Fire needle therapy alleviates symptoms in individuals with mild to moderate KOA and reduces the serum concentrations of IL-1α and MMP-3.96,97 Moreover, this treatment down-regulated the expression of F4/80 and M1 macrophage marker Cluster of Differentiation 86 (CD86), whereas it up-regulated the M2 macrophage marker CD206. It alleviated synovial injury and pain in KOA mice induced by monosodium iodoacetate (MIA), indicating that fire needle treatment can modify the transformation of macrophages from M1 to M2 in KOA patients.98 M2-type polarization increases the expression of Arginase 1 (ARG1), CD206, and IL-4. A study revealed that a 2 week Tug-of-war acupuncture (BHZF)99 treatment alleviated KOA rabbits’ joint pain and swelling, reduced CD86-positive cells, decreased ARG1 levels in cartilage, increased synovium, inhibited IL-1β and TNF-α in serum and synovium, and elevated the anti-inflammatory factors IL-4 and IL-10, suggesting that acupuncture improves cartilage tissue damage by regulating the imbalance of macrophage polarization.26 Xu et al100 treated KOA mice with nanomedicine lidocaine to acupuncture (nd-Acu) for 28 consecutive days. Their histological analysis revealed reduced cartilage damage, synovial inflammation, and pro-inflammatory factor IL-1β in the joint cavity. It was inferred that the underlying mechanism involved reducing pain and inflammation by inhibiting the macrophage High Mobility Group Box 1/ Toll-like Receptor 4 (HMGB1/TLR4) signaling pathway.
Acupuncture can regulate inflammatory signaling pathways and cytokine levels, reduce the expression of pro-inflammatory factors, increase anti-inflammatory factors, and promote the balance of the local microenvironment.101 Acupuncture modulates inflammatory signaling pathways to reduce pro-inflammatory factor release. For example, EA inhibits the TLR4/MyD88/NF-κB pathway in synovium, suppressing downstream inflammatory cascades.102 Under physiological conditions, MMPs play a wound healing role, while when joints are damaged and mechanically stressed, they enhance matrix decomposition via proinflammatory factors. MMPs impact chondrocytes, synovial cells, joints, surrounding tissues, and immune cells. They are involved in KOA initiation and progression; therefore, their targeted inhibition can treat KOA.103 EA inhibits the activation of mitogen-activated protein kinase (MAPK) in articular cartilage in KOA by reducing MMP13, therefore preventing articular cartilage degeneration.104 The NF-κB signaling pathway plays a dual role in KOA. It maintains and modulates the homeostasis of chondrocytes and tissues, and may also be activated by inflammatory mediators in KOA to exacerbate destruction.105 Needle knife delays pain and joint mobility in moderate KOA rabbits, inhibits integrin ITG-β1 and MMP13 through the Focal Adhesion Kinase- p38 Mitogen-Activated Protein Kinase (FAK-p38MAPK) pathway, and retains Type II Collagen (Col-II) expression.106 Ras-Raf-mitogen-activated protein kinase (MEK) 1/2-extracellular signal-regulated kinase (ERK) 1/2 promotes MMP release and accelerates cartilage degradation.107 In a study, the serum of EA-treated OA rats was used to inhibit TNF-α-treated chondrocytes. It was found that the protein expression levels of Ras-Raf-MEK1/2 were reduced in the EA-treated group, and the phosphorylation of RK1/2 and the expression of downstream regulatory factors MMP-3 and MMP-13 were reduced.108
Inflammatory mediators generated by the synovial inflammatory response are essentially involved in KOA pathogenesis.103,109 TNF-α is a key inflammatory mediator in KOA pathogenesis, which can directly prevent the synthesis of cartilage matrix collagen and proteoglycans, increasing matrix degradation, and initiating the early inflammatory cascade of KOA. Shi et al110 found that after 8 weeks of EA and MA treatment, knee pain and swelling symptoms were alleviated, serum inflammatory factors TNF-α, IL-1β, IL-13, and cartilage degradation biomarkers MMP-3 and MMP-13 were reduced, and anti-inflammatory cytokine IL-13 was upregulated in patients with mild to moderate KOA. Compared with MA, the reduction of TNF-α in the EA group was more significant. Inflammatory mediators, including IL-1 and IL-6, can directly enhance the expression of MMPs and accelerate ECM degradation. In-vivo studies have demonstrated that EA treatment to the nose and inner knee eye points of New Zealand white rabbit calves decreases IL-1β, TNF-α, and MMP-3 via the NF-κB signaling pathway, considerably enhances the structural organization of cartilage, and mitigates cartilage degeneration.111 Fire needle treatment significantly improves symptoms in patients with mild and moderate KOA and reduces serum IL-1α and MMP-3 levels.96,97 Moreover, EA at ST36 and GB34 mitigates lipid metabolism disorders in diet-induced obesity-mediated OA rats, suppresses MMP-1 and MMP-13 levels in rat cartilage, preserves cartilage integrity, decreases inflammatory cytokines in serum and synovium, and enhances the relative abundance of advantageous intestinal microorganisms such as lactic acid bacteria.112
Overall, these data showed that acupuncture regulates inflammatory cells and factors through multiple pathways. It can inhibit the activation and aggregation of inflammatory cells, diminish their infiltration and destruction of joint tissues, lower the expression levels of inflammatory factors, and mitigate inflammatory reactions.
Oxidative Stress Management
Oxidative stress arises from an imbalance between the generation of Reactive Oxygen Species (ROS) and the antioxidant defense system, which becomes compromised due to exposure to harmful stimuli, resulting in cellular damage, tissue deterioration, and chronic inflammation.113 ROS can directly damage articular chondrocytes, leading to chondrocyte apoptosis and cartilage matrix degradation. Oxidative stress includes certain factors such as Nuclear factor erythroid 2-related factor 2 (NRF2), Peroxiredoxin 1 (PRDX1), superoxide dismutase (SOD) enzyme, and glutathione peroxidase (GSH-Px), and the absence of NRF2 can aggravate KOA.32 Angiogenesis and inflammation are involved in KOA initiation and development. The literature suggests that EA significantly increases the antioxidant gene transcript SOD2 in KOA guinea pigs.114 Following 21 days of WNA of MIA-induced KOA mice, knee joint swelling and cartilage degradation were reduced, SOD2-positive cells were increased, while NOX2 and IL-1β-positive cells were decreased. The therapeutic impact was improved compared to that of standard acupuncture or moxibustion, indicating that WNA enhances KOA function by mitigating oxidative stress and inflammation.115 Ding et al116 used optical resolution photoacoustic microscopy (OR-PAM) to dynamically observe the structural changes of microcirculation at ST36 and Yanglingquan (GB34) acupoints and non-acupoints of MIA-induced KOA mice on days 0, 7, and 21. The findings indicated no substantial difference in microvascular density and vascular distribution, implying that structural alterations in microcirculation transpire after functional changes.
Vascular Endothelial Growth Factor (VEGF) is an angiogenic factor that can increase vascular permeability and promote angiogenesis.117 Increased Hypoxia-Inducible Factor-1α (HIF-1α) in the synovium leads to chronic synovitis.118 Deoxyhemoglobin (DHb) is inversely proportional to local blood oxygen partial pressure. Acupotomy decreases intra-articular pressure, enhances the hypoxic conditions of the synovium, downregulates HIF-1α activity and VEGF production, and mitigates inflammation and angiogenesis in KOA rabbits.119 EA restored the synovial microcirculation and oxygen partial pressure of hypoxia-induced KOA rabbits, slowed the degradation rate of glycolytic enzymes glucose transporter 1 (GLUT1), pyruvate kinase M2 (PKM2), and lactate dehydrogenase A (LDHA), as well as reduced lactate levels.120 Acupuncture attains its therapeutic effect by stimulating the antioxidant enzyme system, enhancing the synovial vascular milieu, and suppressing the expression of inflammatory factors.
Cellular Apoptosis
Chondrocyte apoptosis is the programmed death of cartilage cells, which is a crucial process in KOA pathogenesis, encompassing apoptosis, pyroptosis, ferroptosis, and other modalities, with the release of inflammatory agents associated with these processes. MAPK participates in apoptosis, with the p38MAPK signaling pathway being a subtype that influences MMP activity and induces matrix degradation.121 Another pathway involved in apoptosis is B-cell lymphoma-2 (Bcl-2) and Bcl-2 Associated X Protein (Bax), Cysteine Aspartic Acid Protease-3 (Caspase-3) in the mitochondria-related signaling pathway. Effective inhibition of chondrocyte apoptosis is the key to treating KOA.122,123 NOD-like receptor protein 3 (NLRP3) is present in the synovium of KOA. It triggers the NF-κB signaling pathway by identifying damage-associated molecular patterns (DAMPs), initiates innate immunity, and results in synovitis.124 EA treatment alleviates mechanical pain in OA guinea pigs, inhibits NLRP3 activation in cartilage tissue, and reduces the protein expression levels of caspase-1 and IL-1.125
GTPase (cdc42) can promote apoptosis in chondrocytes, while nd-Acu demonstrates anti-inflammatory properties by blocking GTPase-associated pathways.100 MiR-214 can inhibit KOA-induced inflammation by disrupting NF-κB signal transduction.126 Transient Receptor Potential Vanilloid 4 (TRPV4) participates in the mechanical hyperalgesia of chondrocytes and is a target gene of miR-214.127 Bax is an apoptosis factor that accelerates cell apoptosis by increasing mitochondrial membrane permeability and promoting the release of cytochrome C (Cyt-C).128 EA treatment alleviated mechanical pain in KOA rats, enhanced the expression of microRNA-214 (miR-214) in rat chondrocytes, and decreased the levels of BAX, thus facilitating chondrocyte apoptosis, and TRPV4, which enhances nociception, indicating that EA protects the joints by inhibiting chondrocyte apoptosis.129 Lin et al130 showed that EA could inhibit chondrocyte apoptosis in OA rats induced by sodium nitroprusside (SNP). Compared with the SNP group, the EA group inhibited the decrease of chondrocyte mitochondrial membrane potential, increased Bcl-2 expression, and reduced Bax, Cytochrome C (Cyt-C), Caspase-9, and Caspase-3 expression, suggesting that EA inhibited chondrocyte apoptosis via the mitochondrial pathway. MMP-13, a crucial downstream component of the Wnt/β-catenin signaling pathway, is the most potent type II collagen-degrading enzyme among the known MMPs. Its overexpression can lead to cartilage degradation, whereas the stimulation of the Wnt/β-catenin signaling pathway can influence chondrocyte apoptosis. EA improves the cartilage morphology and structure of KOA rats, reduces MMP-13 and IL-1β levels through the Wnt/β-catenin signaling pathway, and inhibits chondrocyte apoptosis.131
Pyroptosis is an inflammatory cell death mediated by Caspase-1 activity, and Gasdermin D (GSDMD) is the effector of pyroptosis.132 The literature has indicated that EA papain-induced treatment of the inner knee and Ashi points of KOA rats significantly improved knee joint dysfunction and downregulated NLRP3, apoptosis-associated speck-like protein (ASC), Caspase-1, GSDMD, and IL-1 in synovial tissue, suggesting that EA inhibits inflammatory response by reducing cell pyroptosis in synovial tissue.67
Ferroptosis is a novel mechanism of chondrocyte death induced by iron accumulation, lipid peroxidation, and plasma membrane impairment. Chondrocyte ferroptosis is associated with matrix deterioration. Heat Shock Protein A5/Glutathione Peroxidase 4 (HSPA5/GPX4) is linked to the ferroptosis pathway.133 COL-II is an essential protein that constitutes articular cartilage. Iron overload inhibits COL-II levels and increases MMP expression through ROS production and mitochondrial dysfunction.134 Acupuncture knife therapy treats KOA by loosening soft tissues such as muscles and fascia. In comparison to KOA model rabbits, the acupuncture knife group exhibited elevated expression levels of HSPA5, GPX4, and COL-II mRNA and proteins, whereas the mRNA and protein expression of MMP3 and MMP13 was decreased, suggesting that the acupuncture knife enhances chondrocyte survival by inhibiting ferroptosis.135 Studies have shown that promoting chondrocyte proliferation can prevent and treat KOA. Inhibition of the PI3K/Akt pathway dysregulates proliferation and apoptosis.136 Akt is an upstream regulator of GSK3β. Acupuncture combined with adipose-derived stem cells (ASCs) enhances the GSK3β-cyclin D1-CDK4/CDK6 pathway to mitigate cartilage degeneration.90
Overall, the aforementioned results indicate that acupuncture can suppress aberrant cell apoptosis, mitigate the loss of articular chondrocytes and ferroptosis, and preserve the normal structure and function of joint tissue.
Dual-Directional Regulation of Autophagy in Cells
Autophagy plays a protective role by removing damaged proteins and organelles in chondrocytes, thus maintaining cellular function and integrity.137 It has been shown that moderate autophagy can restore the function of damaged cells.138 Putative kinase protein 1 (PINK1) is a serine kinase that specifically targets mitochondria. Pink1-Parkin interacts with the autophagy protein LC3 to initiate mitochondrial autophagy, mitigate mitochondrial damage, decrease oxidative stress in chondrocytes, and enhance chondrocyte survival.139 Under chronic oxidative stress, inflammation, or mechanical injury, autophagy may become dysregulated. Insufficient autophagy promotes the accumulation of damaged cellular components, leading to chondrocyte apoptosis, ECM degradation, and KOA progression. However, excessive autophagy can induce autophagic cell death, exacerbating the loss of chondrocytes and further cartilage breakdown.140–142 Acupuncture intervention in KOA rabbits also promotes mitochondrial autophagy by regulating the PINK1/Parkin pathway and improves cartilage damage in KOA rabbits.143 Acupuncture delays cell autophagy by promoting AMPK (AMP-activated protein kinase) activation, which stimulates autophagy by inhibiting mTOR (mechanistic target of rapamycin), a primary negative regulator of autophagy.142 Furthermore, Acupuncture attenuates autophagic activity in conditions where increased autophagy is harmful by regulating inflammatory pathways such as the PI3K/Akt/mTOR pathway, inhibiting autophagic cell death, preventing chondrocyte death, and maintaining cartilage health.142,144
Acupuncture Delays Cell Senescence
Cell senescence is a process wherein cells undergo a series of physiological and biochemical alterations, leading to functional deterioration and reduced proliferative capacity. Epigenetics primarily includes DNA methylation, non-coding RNA, and histone tail modifications. Recent research indicates that epigenetics is linked with KOA development.145 miR-146a and miR-140-5p are two microRNAs that play a protective role in OA and delay chondrocyte aging.146 It has been observed that EA alleviates cartilage damage in OA rats and upregulates miR-146a and miR-140-5p levels in rat cartilage and synovial tissue. Furthermore, EA reduces the expression of methylation-related proteins DNA methyltransferase 1 (DNMT1), DNMT3a and DNMT3b, as well as NF-κB and cartilage tissue transcription activator 3 (SMAD3) in synovial tissue.147 The ratio of osteoprotegerin (OPG) to receptor activator of nuclear factor-κB ligand (RANKL) reflects osteoclast activity.148 Acupuncture enhances cartilage remodeling in KOA rabbits by suppressing the production of OPG mRNA, protein, and/or RANKL. In comparison to the EA group, acupuncture exerts a more pronounced inhibitory effect on cartilage thickening, which is associated with the distinct mechanical stimulation of EA.149 Bone morphogenetic protein 2-Smad1 (BMP2) participates in bone metabolism and promotes the formation of chondrocytes. In rabbits, acupuncture treated early cartilage degeneration by upregulating factors related to the BMP2-Smad1 pathway in subchondral bone, indicating that acupuncture can restore the mechanical properties of cartilage.29 Moreover, acupotomy mitigates chondrocyte premature senescence in KOA through mechanotransduction-mediated YAP/FOXD1 axis regulation. Mechanistic studies have revealed that acupotomy-generated mechanical stimulation stimulates Yes-associated protein (YAP), a core effector of the Hippo pathway. Nuclear translocation of YAP transcriptionally upregulates Forkhead box D1 (FOXD1), which subsequently represses key senescence markers (p16 (INK4a) and p21 (Cip1/Waf1)) in chondrocytes. This cascade prevents cell cycle arrest and reduces the senescence-associated secretory phenotype (SASP). Simultaneously, FOXD1 might promote ECM anabolism while inhibiting catabolic processes, thus maintaining cartilage homeostasis.150 The aforementioned research shows that acupuncture restores cartilage tissue by influencing the physiological condition of chondrocytes, thus maintaining their activity (Figure 4).
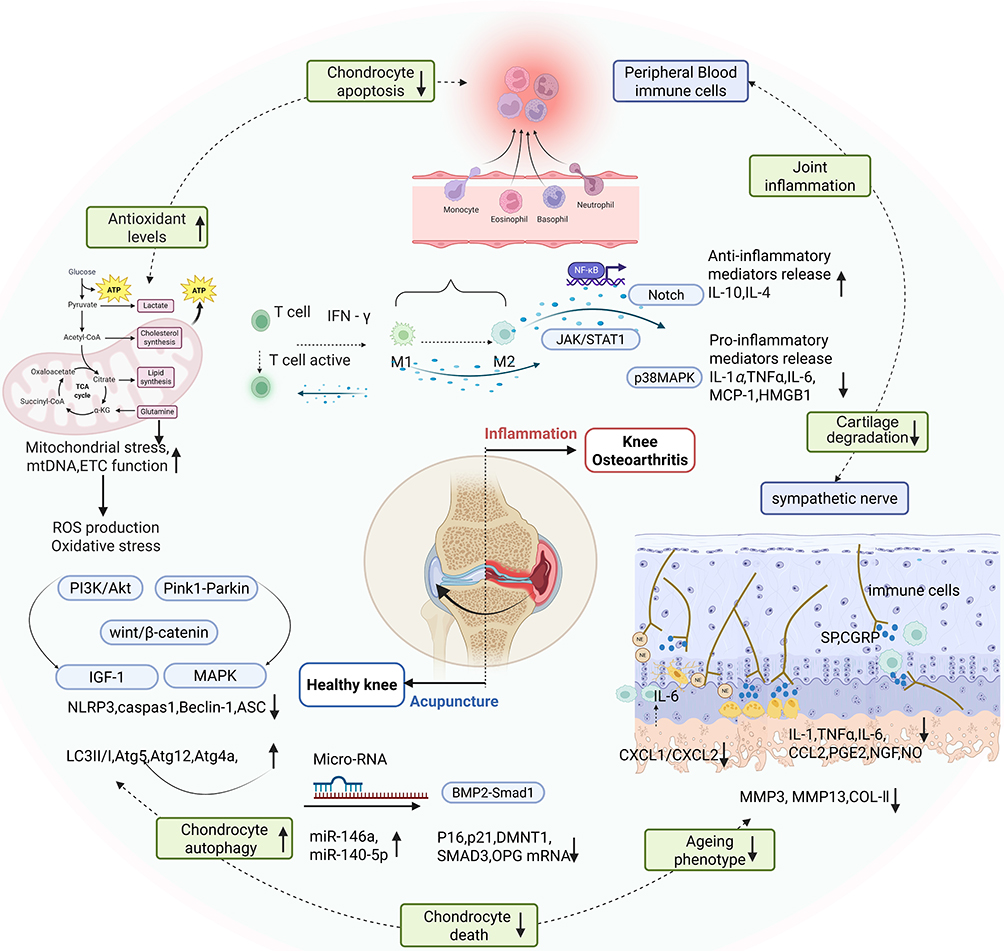 |
Figure 4 Mechanism of Acupuncture to Reduce Inflammation in KOA. Notes: Acupuncture promotes the polarization of macrophages from pro-inflammatory M1 type to anti-inflammatory M2 type, which inhibits inflammatory pathways such as NF-κB, Notch, and p38MAPK, reduces the pro-inflammatory cytokines secretion (such as IL-1β, IL-6, and TNF-α), and increases anti-inflammatory factors (such as IL-10). This reduces the expression of MMP3 and MMP13, delaying the degradation and destruction of cartilage tissue. Acupuncture increases the activity of the antioxidant enzyme system, such as SOD2, which can effectively remove free radicals, reduce oxidative stress damage, restore the oxidation-antioxidant balance in joints, and alleviate the destruction of joint tissue caused by inflammation. Further, Acupuncture maintains mitochondrial function, elevates ATP and mtDNA levels, obstructs the caspase-mediated apoptotic cascade by blocking Wnt/β-catenin and other pathways, and inhibits the apoptosis and mortality of articular chondrocytes. Acupuncture also induces moderate autophagy by activating the Pink1-Parkin signaling pathway, maintaining mitochondrial morphology, and enhancing the inflammatory stress response. Moreover, it increases microRNA expression, inhibits chondrocyte senescence-related signaling pathways, such as p53-p21 and p16-Rb pathways, and reduces the production of aging-related secretory phenotypes. Created in BioRender. Dwad, D (2025) https://BioRender.com/y94k592. |
Nervous System Perspective
Acupuncture Regulates Peripheral Sensitization and Reduces Pain
Signs of effusion/synovitis may correlate positively with signs of neuropathic-like pain and pain sensitivity.151 The analgesic effect of acupuncture results from the interaction between β-endorphins and endogenous opioid receptors.152 Ahsin S et al153 compared the symptoms in 40 chronic pain KOA patients after 10 days of EA treatment. They observed significant improvements in the patients’ WOMAC index and VAS scores, as well as a significant increase in plasma beta-endorphin levels and a decrease in plasma cortisol levels. Acupuncture modulates pain by regulating the hypothalamic-pituitary-adrenal axis (HPA). The activation of the HPA system releases the hormone plasma cortisol. Javier et al used the Goldberg Anxiety and Depression Scale to assess depression and anxiety caused by KOA pain.154 Collagenase-induced OA thermal pain and mechanical hyperalgesia in rats can be alleviated by EA, with a higher effect observed at 2Hz compared to 100Hz. The analgesic effect of 2Hz EA is inhibited by serotonin receptors HT1A and 5, with partial reversal by HT3 receptor antagonists.155 The Nerve Growth Factor (NGF) and the Monocyte Chemotactic Protein-1/ C-C Chemokine Receptor 2 (MCP1/CCR2) axis play a role in the transduction of peripheral pain in KOA. The MCP1/CCR2 axis activation recruits macrophages to the site of damage. The release of IL-6, IL-1β, and TNF-α by macrophages induces synovial inflammation and the synthesis of NGF in tissues.156 Acupuncture can alleviate OA rats’ pain and cartilage damage induced by right knee anterior cruciate ligament amputation by inhibiting the MCP1/CCR2 axis and reducing NGF in synovial tissue.2 Subcutaneous acupuncture (FSN) stimulates the subcutaneous region to alleviate soft tissue injury. Furthermore, it can alleviate peripheral soft tissue pain in KOA individuals.157 Muscle pain resulting from KOA is attributed to stiffness or tightness induced by localized muscular ischemia or hypoxia. FSN can alleviate muscle stiffness, diminish discomfort, and improve knee joint function.158 Yang et al159 employed shear wave elastography and near-infrared spectroscopy (NIRS) to measure blood flow and oxygenation in KOA patients and found that FSN significantly relieved pain and increased oxyhemoglobin (O2Hb), deoxygenated hemoglobin (HHb), total hemoglobin (THb), and tissue saturation index (TSI). This suggests that FSN relieves pain by relaxing skeletal muscles and alleviating the compression of peripheral blood flow. Sensory nerves and sympathetic nerves innervate the knee joint, and neurotransmitters modulate cartilage metabolism.160 EA inhibits the release of noradrenergic neurotransmitters from sympathetic nerves and inhibits the growth of monocytes and macrophages in the gliding joints.161 Complement component 3 (C3) is a constituent of the complement system that has a role in innate immunity. Prostaglandin E2 (PGE2) serves as a mediator in the inflammatory pain response. After 2 weeks of EA treatment, KOA guinea pigs indicated significant improvement in the activity and gait, as well as reduced serum inflammation marker C3. However, there was no significant difference in PGE2 levels, indicating that EA reduces PGE2 levels for a short time.114 Acupuncture can regulate multiple aspects of peripheral sensitization. Furthermore, it can inhibit the over-excitation of nociceptors and reduce the generation and transmission of pain signals. Moreover, it can modulate the release of neurotransmitters by reducing nociceptive neurotransmitter levels and enhancing the secretion of endogenous analgesic chemicals, thus alleviating pain resulting from peripheral sensitization.
Acupuncture Regulates Central Sensitization and Reduces Pain
Acupuncture regulates central sensitization through multiple pathways. It can influence neuronal activity, suppress hyperactive neurons, and decrease the transmission and processing of pain signals inside the central nervous system (CNS). Moreover, acupuncture may modulate the release of neurotransmitters and neuromodulators, which inhibits the secretion of pro-nociceptive neurotransmitters and enhances the creation of endogenous analgesics to alleviate pain resulting from central sensitization. Functional brain imaging shows that plastic changes in brain structure and function play a role in pain and emotion in KOA.162 KOA induces alterations in joint structures and neuronal plasticity within brain regions associated with pain perception. In a study, rs-fMRI was employed to assess the cerebral structures of KOA and healthy individuals, which showed that the gray matter reduced volume of the insula, parietal lobe, cingulate cortex, hippocampus, visual cortex, temporal lobe, prefrontal cortex, and basal ganglia in KOA patients.163 EA inhibits peripheral inflammatory responses through peripheral opioid peptide mechanisms and activation of the HPA axis. In animal pain models, low-frequency EA stimulates the release of endorphins and enkephalins, whereas its high-frequency stimulates the release of dynorphins.164 It has been observed that chronic pain KOA patients have abnormal dorsolateral PFC (dlPFC) activity, FC dysregulation, or even destruction.165,166 Acupuncture can induce alterations in cerebral activity and modulate pain processing-related regions, including the rFPN, rACC, insula, and the descending pain modulation system (DPMS), whereas neural markers in the brain can indicate pain perception.167 After acupuncture, the cortical thickness of the left medial prefrontal cortex (pMPFC) of KOA patients increased. Furthermore, the resting-state functional connectivity (rsFC) between the pMPFC and the anterior cingulate cortex (rACC), medial frontal (mFP), and periaqueductal gray (PAG) was significantly enhanced.59 Chen discovered that acupuncture alleviates KOA pain by stimulating the insula, activating the right frontoparietal network (rFPN), the executive control network (ECN), and the descending pain modulation network via the rACC/MPFC.58 Zhou et al14 compared the central therapeutic mechanisms of acupuncture, sham acupuncture, celecoxib (SC), and placebo (PB) in treating KOA pain. They found that pain in the four groups improved, but their analgesic mechanisms were different. Compared with the SC and PB groups, acupuncture stimulated the right dorsolateral prefrontal cortex (DLPFC) and the right ventrolateral periaqueductal gray (vlPAG) in patients, whereas the SC group did not affect the vlPAGrs-FC. The activation of the NGF/TrkA axis contributes to pain in KOA. The MA obstructs the activation of the NGF/TrkA pathway in the DRG of KOA mice. Subsequent research has validated that peripheral pain can exacerbate central sensitization. The activation of the NGF/TrkA axis is induced by the MCP1/CCR2 axis stimulation in peripheral joint tissues.2 CPM reflects the synthesis of endogenous neurotransmitters and the function of the descending pain inhibition system. Strong EA (> 2 mA), weak EA (< 0.5 mA), and sham EA (non-acupoint) were used to treat KOA patients for 1 week. The EA group showed improved VAS, WOMAC, NPRS, and ES; however, CPM did not improve. After one week of therapy, it was determined that the CPM function in the strong EA group surpassed that of the low EA group, indicating that strong EA is more effective than weak EA in alleviating KOA pain and that acupuncture exhibits a cumulative effect.38
Microglia are the source of proinflammatory factors in the CNS and initiate neuroimmune responses. In chronic KOA pain, microglia can release inflammatory factors and be activated to maintain pain. Brain-derived neurotrophic factor (BDNF) enhances neuronal plasticity in the hippocampus. The bilateral hippocampus blood flow in KOA patients is significantly associated with pain intensity.168 Electroacupuncture enhanced the weight-bearing capacity of the left hind limb in KOA rats, significantly elevated the expression of BDNF in the CA1 region of the hippocampus, and reduced the levels of Iba-1, IL-1β, and TNF-α in both the dorsal horn of the spinal cord and the CA1 region of the hippocampus, thus protecting hippocampal neurons. This indicates that EA alleviates KOA pain by suppressing CNS inflammation.169 Peripheral sensitization of primary sensory neurons in the Dorsal Root Ganglion (DRG) and central sensitization of the dorsal horn of the spinal cord are the primary mechanisms for pain in KOA. Neurotransmitters SP and CGRP transmit pain signals to the CNS, and PGE2 causes pain by stimulating nerve endings. EA alleviated MIA-induced KOA in rats by decreasing the synthesis of pain mediators SP, CGRP, and PGE2, mitigating spinal cord central sensitization, and decelerating the course of KOA.170 Similarly, acupuncture can modulate pain-associated brain regions’ functional connectivity and activity patterns, altering the pain perception and control network. The aforementioned research indicates that acupuncture analgesia constitutes a complex process (Figure 5).
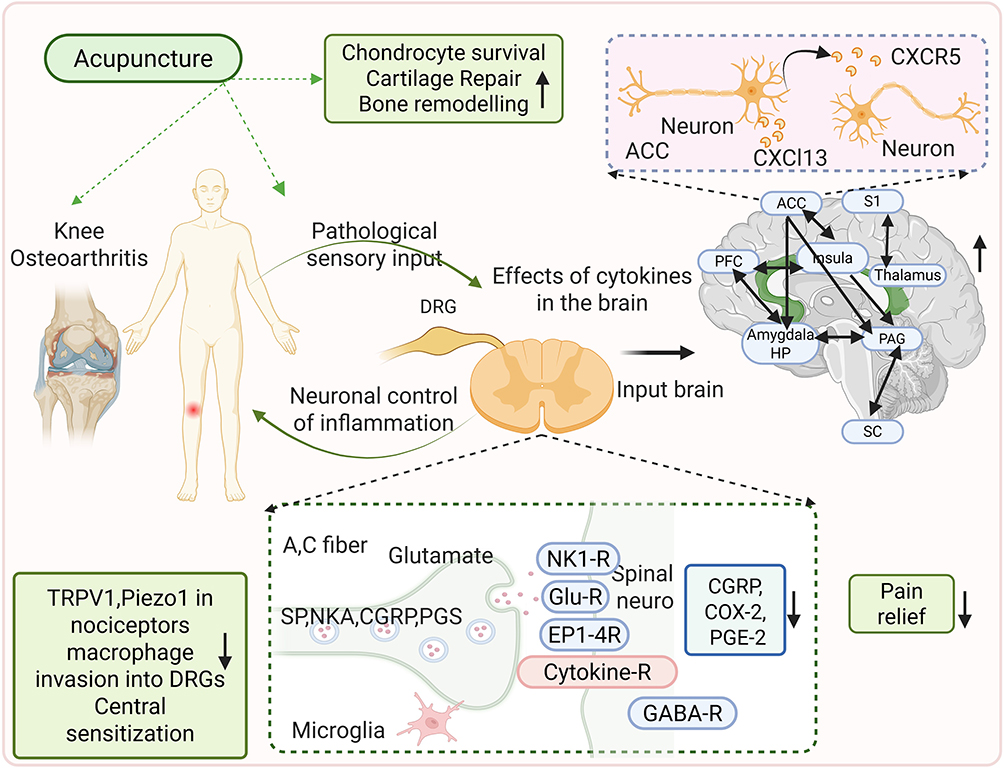 |
Figure 5 Mechanism of Acupuncture in Alleviating Pain in KOA Patients. Notes: From the peripheral mechanism, acupuncture first activates the Aδ and C-type nerve fibers, triggering the afferent nerve impulse. It regulates the level of local inflammatory cytokines, reduces the production of pain-causing substances (CGRP, SP, PGE2, IL-1β, and COX2), and decreases the sensitivity of nociceptive receptors (such as TRPV1). In the dorsal horn of the spinal cord, it can inhibit the release of excitatory neurotransmitters such as Glu, NK1, GABA, neuropeptides, etc., suppress microglia cell activity, and reduce the transmission of pain signals. In the central mechanism, acupuncture enhances the functional connectivity of pain-related brain areas such as ACC, PFC, and PAG, changes the neuronal excitability of the ACC region, and reduces pain. Created in BioRender. Dwad, D (2025) https://BioRender.com/58xi9pn. |
Conclusion
This review summarizes the latest clinical research reports on KOA’s pathogenesis and acupuncture treatment. KOA is a multifaceted degenerative disorder caused by chronic inflammation, cartilage degradation, and subchondral bone remodeling. Conventional therapies (eg, NSAIDs, surgery) have several limitations because of their adverse effects and invasiveness, underscoring the need for complementary strategies. Acupuncture is administered via MA, EA, TEA, or other techniques at clinically relevant acupoints. Furthermore, acupuncture as monotherapy or in multimodal regimens can significantly alleviate pain as observed by VAS/NRS, improve joint function (WOMAC), and enhance quality of life (SF-36) in KOA patients.
Mechanistically, acupuncture modulates inflammation by promoting M2 macrophage polarization, inhibiting pro-inflammatory mediators (TNF-α/MMP3), and enhancing antioxidant pathways (SOD2/NRF2). Moreover, it preserves chondrocyte integrity by preventing apoptosis and ferroptosis via MAPK/Wnt/β-catenin signaling, autophagy (Pink1-Parkin, PI3K/AKT), and senescence inhibition through microRNA regulation. It also regulates pain perception by attenuating peripheral neuropeptides (PGE2, SP, CGRP) and alleviating central sensitization in specific brain regions (pMPFC, ACC).
Despite substantial clinical data, there are limitations; for instance, the evaluation of pain relief mainly depends on subjective outcomes (VAS/WOMAC) rather than objective biomarkers or structural imaging (eg, MRI), and the mechanistic association between symptom alleviation and disease progression is lacking. Furthermore, the heterogeneity in acupuncture protocols across the literature, such as variations in acupoint selection, needle manipulation techniques, and treatment frequency, complicates the comparison and synthesis of research findings. The lack of sham controls in some trials and the paucity of long-term outcome data limit the complete validation of the sustained efficacy and specificity of acupuncture for KOA. Future studies should validate key findings in human primary cells or clinical cohorts to strengthen clinical relevance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the National Science Foundation of China (NSFC)(Nos. 82105024, 82030125).
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Lespasio MJ, Piuzzi NS, Husni ME, Muschler GF, Guarino A, Mont MA. Knee osteoarthritis: a primer. Perm J. 2017;21:16–183. doi:10.7812/TPP/16-183
2. Li B, Jing L, Jia L, et al. Acupuncture reduces pain in rats with osteoarthritis by inhibiting MCP2/CCR2 signaling pathway. Exp Biol Med. 2020;245:1722–1731. doi:10.1177/1535370220952342
3. Siddiq MAB, Oo WM, Hunter DJ. New therapeutic strategies in osteoarthritis. Joint Bone Spine. 2024;91:105739. doi:10.1016/j.jbspin.2024.105739
4. Qu Y, Peng Y, Xiong Y, Dong X, Ma P, Cheng S. Acupuncture-related therapy for knee osteoarthritis: a narrative review of neuroimaging studies. J Pain Res. 2024;17:773–784. doi:10.2147/JPR.S450515
5. Vina ER, Kwoh CK. Epidemiology of osteoarthritis: literature update. Curr Opin Rheumatol. 2018;30:160–167. doi:10.1097/BOR.0000000000000479
6. Duong V, Oo WM, Ding C, Culvenor AG, Hunter DJ. Evaluation and treatment of knee pain: a review. JAMA. 2023;330:1568–1580. doi:10.1001/jama.2023.19675
7. Sparks JA. Rheumatoid Arthritis. Ann Intern Med. 2019;170:ITC1–ITC16. doi:10.7326/AITC201901010
8. Pope JE. Management of fatigue in rheumatoid arthritis. RMD Open. 2020;6:e001084. doi:10.1136/rmdopen-2019-001084
9. Moseng T, Vliet Vlieland TPM, Battista S, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis: 2023 update. Ann Rheum Dis. 2024;83:730–740. doi:10.1136/ard-2023-225041
10. Geng R, Li J, Yu C, et al. Knee osteoarthritis: current status and research progress in treatment (Review). Exp Ther Med. 2023;26:481. doi:10.3892/etm.2023.12180
11. Lee BJ, Yang S, Kwon S, Choi KH, Kim W. Association between metabolic syndrome and knee osteoarthritis: a cross-sectional nationwide survey study. J Rehabil Med. 2019;51:464–470. doi:10.2340/16501977-2561
12. Cui A, Li H, Wang D, Zhong J, Chen Y, Lu H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 2020;29–30:100587. doi:10.1016/j.eclinm.2020.100587
13. Whittaker JL, Losciale JM, Juhl CB, et al. Risk factors for knee osteoarthritis after traumatic knee injury: a systematic review and meta-analysis of randomised controlled trials and cohort studies for the OPTIKNEE consensus. Br J Sports Med. 2022;56:1406–1421. doi:10.1016/j.eclinm.2020.100587
14. Zhou J, Zeng F, Cheng S, et al. Modulation effects of different treatments on periaqueductal gray resting state functional connectivity in knee osteoarthritis knee pain patients. CNS Neurosci Ther. 2023;29:1965–1980. doi:10.1111/cns.14153
15. Shane Anderson A, Loeser RF. Why is osteoarthritis an age-related disease? Best Pract Res Clin Rheumatol. 2010;24:15–26. doi:10.1016/j.berh.2009.08.006
16. Du X, Liu ZY, Tao XX, et al. Research progress on the pathogenesis of knee osteoarthritis. Orthop Surg. 2023;15:2213–2224. doi:10.1111/os.13809
17. Maly MR, Costigan PA, Olney SJ. Mechanical factors relate to pain in knee osteoarthritis. Clin Biomech. 2008;23:796–805. doi:10.1016/j.clinbiomech.2008.01.014
18. Robinson WH, Lepus CM, Wang Q, et al. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat Rev Rheumatol. 2016;12:580–592. doi:10.1038/nrrheum.2016.136
19. Veronese N, Honvo G, Bruyère O, et al. Knee osteoarthritis and adverse health outcomes: an umbrella review of meta-analyses of observational studies. Aging Clin Exp Res. 2023;35:245–252. doi:10.1007/s40520-022-02289-4
20. Leaney AA, Lyttle JR, Segan J, et al. Antidepressants for hip and knee osteoarthritis. Cochrane Database Syst Rev. 2022;10:Cd012157. doi:10.1002/14651858.CD012157.pub2
21. Liow Y, Wang W, Loh VW. Outpatient management of knee osteoarthritis. Singapore Med J. 2017;58:580–584. doi:10.11622/smedj.2017097
22. Lin X, Huang K, Zhu G, Huang Z, Qin A, Fan S. The effects of acupuncture on chronic knee pain due to osteoarthritis: a meta-analysis. J Bone Joint Surg Am. 2016;98:1578–1585. doi:10.2106/JBJS.15.00620
23. Lee H, Lee JY, Kim YJ, et al. Acupuncture for symptom management of rheumatoid arthritis: a pilot study. Clin Rheumatol. 2008;27:641–645. doi:10.1007/s10067-007-0819-3
24. Mei F, Yao M, Wang Y, et al. Acupuncture for knee osteoarthritis: a systematic review and meta-analysis. J Evid Based Med. 2023;16:138–140. doi:10.1111/jebm.12532
25. Arden NK, Perry TA, Bannuru RR, et al. Non-surgical management of knee osteoarthritis: comparison of ESCEO and OARSI 2019 guidelines. Nat Rev Rheumatol. 2021;17:59–66. doi:10.1038/s41584-020-00523-9
26. Yan J, Jiang S, Ma J, et al. Use of the improved tug-of-war acupuncture for promoting cartilage repair by inducing macrophage polarization in knee osteoarthritis. Heliyon. 2024;10:e25495. doi:10.1016/j.heliyon.2024.e25495
27. Shi X, Yu W, Wang T, et al. Electroacupuncture alleviates cartilage degradation: improvement in cartilage biomechanics via pain relief and potentiation of muscle function in a rabbit model of knee osteoarthritis. Biomed Pharmacother. 2020;123:109724. doi:10.1016/j.biopha.2019.109724
28. Diamond LE, Grant T, Uhlrich SD. Osteoarthritis year in review 2023: biomechanics. Osteoarthritis Cartilage. 2024;32:138–147. doi:10.1016/j.joca.2023.11.015
29. Chen X, Guo Y, Lu J, et al. Acupotomy ameliorates subchondral bone absorption and mechanical properties in rabbits with knee osteoarthritis by regulating bone morphogenetic protein 2-Smad1 pathway. J Tradit Chin Med. 2023;43:734–743. doi:10.19852/j.cnki.jtcm.20230404.001
30. Mathiessen A, Conaghan PG. Synovitis in osteoarthritis: current understanding with therapeutic implications. Arthritis Res Ther. 2017;19:18. doi:10.1186/s13075-017-1229-9
31. McAlindon TE, LaValley MP, Harvey WF, et al. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis: a randomized clinical trial. JAMA. 2017;317:1967–1975. doi:10.1001/jama.2017.5283
32. Bolduc JA, Collins JA, Loeser RF. Reactive oxygen species, aging, and articular cartilage homeostasis. Free Radic Biol Med. 2019;132:73–82. doi:10.1016/j.freeradbiomed.2018.08.038
33. Belluzzi E, Stocco E, Pozzuoli A, et al. Contribution of infrapatellar fat pad and synovial membrane to knee osteoarthritis pain. Biomed Res Int. 2019;2019:6390182. doi:10.1155/2019/6390182
34. Atalay SG, Durmus A, Gezginaslan Ö. The effect of acupuncture and physiotherapy on patients with knee osteoarthritis: a randomized controlled study. Pain Physician. 2021;24:E269–E278. doi:10.36076/ppj.2021/24/E269
35. Zhang L, Yuan H, Zhang L, Li J, Li H. Effect of acupuncture therapies combined with usual medical care on knee osteoarthritis. J Tradit Chin Med. 2019;39:103–110.
36. Woo SH, Lee HJ, Park YK, et al. Efficacy and safety of thread embedding acupuncture for knee osteoarthritis: a randomized controlled pilot trial. Medicine. 2022;101:e29306. doi:10.1097/MD.0000000000029306
37. Qi L, Tang Y, You Y, et al. Comparing the effectiveness of electroacupuncture with different grades of knee osteoarthritis: a prospective study. Cell Physiol Biochem. 2016;39:2331–2340. doi:10.1159/000447925
38. Lv ZT, Shen LL, Zhu B, et al. Effects of intensity of electroacupuncture on chronic pain in patients with knee osteoarthritis: a randomized controlled trial. Arthritis Res Ther. 2019;21:120. doi:10.1186/s13075-019-1899-6
39. Williamson L, Wyatt MR, Yein K, Melton JT. Severe knee osteoarthritis: a randomized controlled trial of acupuncture, physiotherapy (supervised exercise) and standard management for patients awaiting knee replacement. Rheumatology. 2007;46:1445–1449. doi:10.1093/rheumatology/kem119
40. Zhang L, Yuan H. Effectiveness and clinical benefit of a therapy of combined non-pharmaceutical Traditional Chinese Medicine for knee osteoarthritis: a randomized controlled study. J Tradit Chin Med. 2020;40:447–454. doi:10.19852/j.cnki.jtcm.2020.03.013
41. Sangdee C, Teekachunhatean S, Sananpanich K, et al. Electroacupuncture versus diclofenac in symptomatic treatment of osteoarthritis of the knee: a randomized controlled trial. BMC Complement Altern Med. 2002;2:3. doi:10.1186/1472-6882-2-3
42. Vas J, Méndez C, Perea-Milla E, et al. Acupuncture as a complementary therapy to the pharmacological treatment of osteoarthritis of the knee: randomised controlled trial. BMJ. 2004;329:1216. doi:10.1136/bmj.38238.601447.3A
43. Ho KK, Kwok AW, Chau WW, Xia SM, Wang YL, Cheng JC. A randomized controlled trial on the effect of focal thermal therapy at acupressure points treating osteoarthritis of the knee. J Orthop Surg Res. 2021;16:282. doi:10.1186/s13018-021-02398-2
44. Fu J, Shang HC, Wang LY, et al. Clinical efficacy evaluation of a traditional Miao technique of crossbow needle therapy in the treatment of knee osteoarthritis: a multi-center randomized controlled trial. Trials. 2020;21:560. doi:10.1186/s13063-020-04508-7
45. Sun Z, Qu X, Wang T, Liu F, Li X. Effects of warm acupuncture combined with meloxicam and comprehensive nursing on pain improvement and joint function in patients with knee osteoarthritis. J Healthc Eng. 2022;2022:9167956. doi:10.1155/2022/9167956
46. Ding Y, Wang Y, Shi X, Luo Y, Gao Y, Pan J. Effect of ultrasound-guided acupotomy vs electro-acupuncture on knee osteoarthritis: a randomized controlled study. J Tradit Chin Med. 2016;36:450–455.
47. Revill SI, Robinson JO, Rosen M, Hogg MI. The reliability of a linear analogue for evaluating pain. Anaesthesia. 1976;31:1191–1198. doi:10.1111/j.1365-2044.1976.tb11971.x
48. Dunning J, Butts R, Young I, et al. Periosteal electrical dry needling as an adjunct to exercise and manual therapy for knee osteoarthritis: a multicenter randomized clinical trial. Clin J Pain. 2018;34:1149–1158. doi:10.1097/AJP.0000000000000634
49. Lansdown H, Howard K, Brealey S, MacPherson H. Acupuncture for pain and osteoarthritis of the knee: a pilot study for an open parallel-arm randomised controlled trial. BMC Musculoskelet Disord. 2009;10:130. doi:10.1186/1471-2474-10-130
50. Chen LX, Mao JJ, Fernandes S, et al. Integrating acupuncture with exercise-based physical therapy for knee osteoarthritis: a randomized controlled trial. J Clin Rheumatol. 2013;19:308–316. doi:10.1097/RHU.0b013e3182a21848
51. Berman BM, Lao L, Langenberg P, Lee WL, Gilpin AM, Hochberg MC. Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med. 2004;141:901–910. doi:10.7326/0003-4819-141-12-200412210-00006
52. Berman BM, Singh BB, Lao L, et al. A randomized trial of acupuncture as an adjunctive therapy in osteoarthritis of the knee. Rheumatology. 1999;38:346–354. doi:10.1093/rheumatology/38.4.346
53. Jinks C, Jordan K, Croft P. Measuring the population impact of knee pain and disability with the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Pain. 2002;100:55–64. doi:10.1016/s0304-3959(02)00239-7
54. Zhu J, Zheng Z, Liu Y, et al. The effects of small-needle-knife therapy on pain and mobility from knee osteoarthritis: a pilot randomized-controlled study. Clin Rehabil. 2020;34:1497–1505. doi:10.1177/0269215520938852
55. Lin K, Bao L, Wang J, Fujita K, Makimoto K, Liao X. Validation of the Chinese (Mandarin) version of the oxford knee score in patients with knee osteoarthritis. Clin Orthop Relat Res. 2017;475:2992–3004. doi:10.1007/s11999-017-5495-2
56. Sánchez-Romero EA, Pecos-Martín D, Calvo-Lobo C, Ochoa-Sáez V, Burgos-Caballero V, Fernández-Carnero J. Effects of dry needling in an exercise program for older adults with knee osteoarthritis: a pilot clinical trial. Medicine. 2018;97:e11255. doi:10.1097/MD.0000000000011255
57. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005;14:798–804. doi:10.1111/j.1365-2702.2005.01121.x
58. Chen X, Spaeth RB, Freeman SG, et al. The modulation effect of longitudinal acupuncture on resting state functional connectivity in knee osteoarthritis patients. Mol Pain. 2015;11:67. doi:10.1186/s12990-015-0071-9
59. Chen X, Spaeth RB, Retzepi K, Ott D, Kong J. Acupuncture modulates cortical thickness and functional connectivity in knee osteoarthritis patients. Sci Rep. 2014;4:6482. doi:10.1038/srep06482
60. Roos EM, Toksvig-Larsen S. Knee injury and Osteoarthritis Outcome Score (KOOS) - validation and comparison to the WOMAC in total knee replacement. Health Qual Life Outcomes. 2003;1:17. doi:10.1186/1477-7525-1-17
61. Huang W, Bliwise DL, Carnevale CV, Kutner NG. Acupuncture for pain and sleep in knee osteoarthritis. J Am Geriatr Soc. 2010;58:1218–1220. doi:10.1111/j.1532-5415.2010.02886.x
62. Yin S, Chang Y, Yan X, Feng X, Wu N. Effect of acupuncture for patients with knee osteoarthritis: study protocol for a double-dummy randomized controlled trial. J Orthop Surg Res. 2023;18:779. doi:10.1186/s13018-023-04198-2
63. Guillemin F, Coste J, Pouchot J, Ghézail M, Bregeon C, Sany J. The AIMS2-SF: a short form of the arthritis impact measurement scales 2. french quality of life in rheumatology group. Arthritis Rheum. 1997;40:1267–1274. doi:10.1002/1529-0131(199707)40:7<1267::AID-ART11>3.0.CO;2-L
64. Yuan J, Wang H, Chen J, et al. Effect of low frequency repetitive magnetic stimulation at Shenmen (HT7) on sleep quality in patients with chronic insomnia. Medicine. 2020;99:e21292. doi:10.1097/MD.0000000000021292
65. Geissner E, Huetteroth A. Beck anxiety inventory german version - a reliable, valid, patientfriendly instrument for measuring clinical anxiety. Psychother Psychosom Med Psychol. 2018;68:118–125. doi:10.1055/s-0043-122941
66. Garcia-Batista ZE, Guerra-Pena K, Cano-Vindel A, Herrera-Martinez SX, Medrano LA. Validity and reliability of the Beck Depression Inventory (BDI-II) in general and hospital population of Dominican Republic. PLoS One. 2018;13:e0199750. doi:10.1371/journal.pone.0199750
67. Huang Y, Huang H, Chen Q, et al. Efficacy and immune-inflammatory mechanism of acupuncture-related therapy in animal models of knee osteoarthritis: a preclinical systematic review and network meta-analysis. J Orthop Surg Res. 2024;19:177. doi:10.1186/s13018-024-04660-9
68. Van der Sluijs JA, Geesink RG, van der Linden AJ, Bulstra SK, Kuyer R, Drukker J. The reliability of the Mankin score for osteoarthritis. J Orthop Res. 1992;10:58–61. doi:10.1002/jor.1100100107
69. Scher C, Petti E, Meador L, Van Cleave JH, Liang E, Reid MC. Multidimensional pain assessment tools for ambulatory and inpatient nursing practice. Pain Manag Nurs. 2020;21:416–422. doi:10.1016/j.pmn.2020.03.007
70. Breivik H, Borchgrevink PC, Allen SM, et al. Assessment of pain. Br J Anaesth. 2008;101:17–24. doi:10.1093/bja/aen103
71. Qiang Q, Zhou M, Lv Y, et al. Exploring the correlation between knee osteoarthritis and musculoskeletal ultrasound manifestations based on changes in traditional Chinese medical syndrome types. Medicine. 2024;103:e40718. doi:10.1097/MD.0000000000040718
72. Mi BH, Wang XZ, Yang JW, et al. Thermographic evaluation of acupoints in lower limb region of individuals with osteoarthritis: a cross-sectional case-control study protocol. PLoS One. 2023;18:e0284381. doi:10.1371/journal.pone.0284381
73. Tillu A, Roberts C, Tillu S. Unilateral versus bilateral acupuncture on knee function in advanced osteoarthritis of the knee--a prospective randomised trial. Acupunct Med. 2001;19:15–18. doi:10.1136/aim.19.1.15
74. Wang B, Hu J, Zhang N, Wang J, Chen Z, Wu Z. Clinical study of fire acupuncture with centro-square needles for knee osteoarthritis. Zhongguo Zhen Jiu. 2017;37:463–466. doi:10.13703/j.0255-2930.2017.05.003
75. Tu JF, Yang JW, Shi GX, et al. Efficacy of intensive acupuncture versus sham acupuncture in knee osteoarthritis: a randomized controlled trial. Arthritis Rheumatol. 2021;73:448–458. doi:10.1002/art.41584
76. Wang XY, Nie ZY, Yu QQ, et al. Acupuncture enhances signals at sensitized acupoints to elevate pressure pain threshold in knee osteoarthritis patients. Chin J Integr Med. 2022;28:1105–1110. doi:10.1007/s11655-022-3588-6
77. Bao F, Zhang Y, Wu ZH, et al. Efficacy observation on knee osteoarthritis treated with electroacupuncture and its influence on articular cartilage with T2 mapping. Zhongguo Zhen Jiu. 2013;33:193–197.
78. Tzeng CY, Chang SL, Wu CC, et al. Single-blinded, randomised preliminary study evaluating the effects of 2 Hz electroacupuncture for postoperative pain in patients with total knee arthroplasty. Acupunct Med. 2015;33:284–288. doi:10.1136/acupmed-2014-010722
79. Zhang D, Song S, Bian Z, Huang Z. Clinical effect of catgut embedding plus warm needle moxibustion on improving inflammation and quality of life of knee osteoarthritis patients. Comput Math Methods Med. 2022;2022:5315619. doi:10.1155/2022/5315619
80. Jiang G, Ding J, Ge C. Deep learning-based CT imaging to evaluate the therapeutic effects of acupuncture and moxibustion therapy on knee osteoarthritis. Comput Math Methods Med. 2022;2022:1135196. doi:10.1155/2022/1135196
81. Li S, Dong A, Hu Z, Zhu X. JI Laixi’s experience of acupuncture and moxibustion for knee osteoarthritis. Zhongguo Zhen Jiu. 2018;38:71–74. doi:10.13703/j.0255-2930.2018.01.018
82. Liu SR, Qiu JQ, Zhang LY, Lin QL, Ye GP, Zhu DY. Warming acupuncture combined with moxibustion at Yongquan (KI 1) for knee osteoarthritis with kidney-marrow deficiency: a randomized controlled trial. Zhongguo Zhen Jiu. 2019;39:799–803. doi:10.13703/j.0255-2930.2019.08.001
83. Lü N, Cheng P, Xia JX, Yuan YP. Effect of acupuncture combined with moxibustion on serum matrix metalloproteinase-9 and matrix metalloproteinase inhibitor-1 in patients with knee osteoarthritis. Zhen Ci Yan Jiu. 2022;47:262–267. doi:10.10372/j.1000-0607.20210079
84. Gao YL, Yao JH, Guo JX. Clinical observation on fire needles at bones combined with cupping and Tuina for knee osteoarthritistis. Zhongguo Zhen Jiu. 2013;33:697–699.
85. Qin XY, Li XX, Berghea F, Suteanu S. Comparative study on Chinese medicine and western medicine for treatment of osteoarthritis of the knee in Caucasian patients. Zhongguo Zhen Jiu. 2008;28:459–462.
86. Qiu JQ, Liu SR, Lin QL, Li MJ, Zhuang JX, Wu GW. Acupuncture combined with cinesiotherapy cupping for knee osteoarthritis with qi stagnation and blood stasis syndrome: a randomized controlled trial. Zhongguo Zhen Jiu. 2019;39:462–466. doi:10.13703/j.0255-2930.2019.05.002
87. Wang B, Liu X, Hu Z, et al. YANG’s pricking-cupping therapy for knee osteoarthritis: a multi-center randomized controlled trial. Zhongguo Zhen Jiu. 2016;36:113–118.
88. Zhuang SQ, Zhuang KZ, Zhang LM, Zhang XL. Treatment of knee osteoarthritis with acupuncture plus intra-articular injection of sodium hyaluronate. Zhen Ci Yan Jiu. 2018;43:326–329. doi:10.13702/j.1000-0607.170371
89. Foster NE, Thomas E, Barlas P, et al. Acupuncture as an adjunct to exercise based physiotherapy for osteoarthritis of the knee: randomised controlled trial. BMJ. 2007;335:436. doi:10.1136/bmj.39280.509803.BE
90. An X, Wang T, Zhang W, et al. Chondroprotective effects of combination therapy of acupotomy and human adipose mesenchymal stem cells in knee osteoarthritis rabbits via the GSK3β-cyclin D1-CDK4/CDK6 signaling pathway. Aging Dis. 2020;11:1116–1132. doi:10.14336/AD.2019.1104
91. Yang F, Chen Y, Lu Z, et al. Treatment of knee osteoarthritis with acupuncture combined with Chinese herbal medicine: a systematic review and meta-analysis. Ann Palliat Med. 2021;10:11430–11444. doi:10.21037/apm-21-2565
92. Zheng J, Zhang H, Liu J. Different acupuncture and moxibustion methods at Heding (EX-LE 2) for knee osteoarthritis with yang-deficiency and cold-stagnation syndrome. Zhongguo Zhen Jiu. 2017;37:594–598. doi:10.13703/j.0255-2930.2017.06.006
93. Kim B, Lohman E, Yim J. Acupuncture-like transcutaneous electrical nerve stimulation for pain, function, and biochemical inflammation after total knee arthroplasty. Altern Ther Health Med. 2021;27:28–34.
94. Jia W, Zhang Y, Wang T, et al. Electroacupuncture ameliorates knee osteoarthritis by rebalancing t cell homeostasis as revealed by immune repertoire (IR) sequencing. Comb Chem High Throughput Screen. 2024. doi:10.2174/0113862073303471240805061026
95. Belluzzi E, Olivotto E, Toso G, et al. Conditioned media from human osteoarthritic synovium induces inflammation in a synoviocyte cell line. Connect Tissue Res. 2019;60:136–145. doi:10.1080/03008207.2018.1470167
96. Fu YB, Chen JW, Li B, Yuan F, Sun JQ. Effect of fire needling on mild to moderate knee osteoarthritis and related serum inflammatory cytokines. Zhongguo Zhen Jiu. 2021;41:493–497. doi:10.13703/j.0255-2930.20200708-k0003
97. Gao YJ, Sun JQ, Hou XS, et al. Point-pricking method with fire needle for knee osteoarthritis: a randomized controlled trial. Zhen Ci Yan Jiu. 2022;47:902–906. doi:10.13702/j.1000-0607.20210745
98. Wei J, Liu L, Li Z, et al. Fire needling acupuncture suppresses cartilage damage by mediating macrophage polarization in mice with knee osteoarthritis. J Pain Res. 2022;15:1071–1082. doi:10.2147/JPR.S360555
99. Au KY, Chen H, Lam WC, et al. Sinew acupuncture for knee osteoarthritis: study protocol for a randomized sham-controlled trial. BMC Complement Altern Med. 2018;18:133. doi:10.1186/s12906-018-2195-8
100. Xu W, Xiao Y, Zhao M, et al. Effective treatment of knee osteoarthritis using a nano-enabled drug acupuncture technology in mice. Adv Sci. 2023;10:e2302586. doi:10.1002/advs.202302586
101. Hirata Y, Nomura K, Kato D, et al. A Piezo1/KLF15/IL-6 axis mediates immobilization-induced muscle atrophy. J Clin Invest. 2022;132:1–13. doi:10.1172/JCI154611
102. Jin X, Yu Y, Lin Y, Yang J, Chen Z. Tendon-regulating and bone-setting manipulation promotes the recovery of synovial inflammation in rabbits with knee osteoarthritis via the TLR4-MyD88-NF-kappaB signaling pathway. Ann Transl Med. 2023;11:245. doi:10.21037/atm-22-3039
103. Mukherjee A, Das B. The role of inflammatory mediators and matrix metalloproteinases (MMPs) in the progression of osteoarthritis. Biomater Biosyst. 2024;13:100090. doi:10.1016/j.bbiosy.2024.100090
104. Liao Y, Li X, Li N, Zhou J. Electroacupuncture protects against articular cartilage erosion by inhibiting mitogen-activated protein kinases in a rat model of osteoarthritis. Acupunct Med. 2016;34:290–295. doi:10.1136/acupmed-2015-010949
105. Jimi E, Fei H, Nakatomi C. NF-κB signaling regulates physiological and pathological chondrogenesis. Int J Mol Sci. 2019;20:6275. doi:10.3390/ijms20246275
106. Li Y, Hou Y, Sun J, et al. Therapeutic effect of acupotomy at sanheyang for cartilage collagen damage in moderate knee osteoarthritis: a rabbit model. J Inflamm Res. 2023;16:2241–2254. doi:10.2147/JIR.S400956
107. Uehling DE, Harris PA. Recent progress on MAP kinase pathway inhibitors. Bioorg Med Chem Lett. 2015;25:4047–4056. doi:10.1016/j.bmcl.2015.07.093
108. Chen H, Shao X, Li L, et al. Electroacupuncture serum inhibits TNF‑α‑mediated chondrocyte inflammation via the Ras‑Raf‑MEK1/2‑ERK1/2 signaling pathway. Mol Med Rep. 2017;16:5807–5814. doi:10.3892/mmr.2017.7366
109. Berenbaum F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthritis Cartilage. 2013;21:16–21. doi:10.1016/j.joca.2012.11.012
110. Shi GX, Tu JF, Wang TQ, et al. effect of electro-acupuncture (ea) and manual acupuncture (ma) on markers of inflammation in knee osteoarthritis. j pain res. 2020;13:2171–2179. doi:10.2147/JPR.S256950
111. Wu GW, Chen J, Huang YM, et al. Electroacupuncture delays cartilage degeneration by modulating nuclear factor-κB signaling pathway. Chin J Integr Med. 2019;25:677–683. doi:10.1007/s11655-018-2916-8
112. Xie LL, Zhao YL, Yang J, et al. Electroacupuncture prevents osteoarthritis of high-fat diet-induced obese rats. Biomed Res Int. 2020;2020:9380965. doi:10.1155/2020/9380965
113. Liu L, Luo P, Yang M, Wang J, Hou W, Xu P. The role of oxidative stress in the development of knee osteoarthritis: a comprehensive research review. Front Mol Biosci. 2022;9:1001212. doi:10.3389/fmolb.2022.1001212
114. Spittler AP, Afzali MF, Martinez RB, et al. Evaluation of electroacupuncture for symptom modification in a rodent model of spontaneous osteoarthritis. Acupunct Med. 2021;39:700–707. doi:10.1177/09645284211020755
115. Tan Q, Li J, Li BC, Xiang HC, Cai GW. Warm needling reduces oxidative damage and inflammation of cartilage in knee osteoarthritis rats. Zhen Ci Yan Jiu. 2022;47:321–328. doi:10.13702/j.1000-0607.20210308
116. Ding N, Liu X, Chen N, et al. Lack of association between acupoint sensitization and microcirculatory structural changes in a mouse model of knee osteoarthritis: a pilot study. J Biophotonics. 2019;12:e201800458. doi:10.1002/jbio.201800458
117. Luo Q, Fan S, Li R, Ouyang Z, Liu Z, Lin Q. Effects of ultrasound on vascular endothelial growth factor in cartilage, synovial fluid, and synovium in rabbit knee osteoarthritis. Acta Biochim Pol. 2020;67:379–385. doi:10.18388/abp.2020_5238
118. Hu Y, Zhang T, Chen J, et al. Downregulation of hypoxia-inducible factor-1α by RNA interference alleviates the development of collagen-induced arthritis in rats. Mol Ther Nucleic Acids. 2020;19:1330–1342. doi:10.1016/j.omtn.2020.01.014
119. Guo Y, Xu Y, He M, et al. Acupotomy improves synovial hypoxia, synovitis and angiogenesis in KOA rabbits. J Pain Res. 2023;16:749–760. doi:10.2147/JPR.S396955
120. Ma W, Du W, Lu W, et al. Electroacupuncture improves articular microcirculation and attenuates cartilage hypoxia in a male rabbit model of knee osteoarthritis. J Tradit Complement Med. 2024;14:414–423. doi:10.1016/j.jtcme.2024.01.002
121. Zhou Y, Liu SQ, Yu L, et al. Berberine prevents nitric oxide-induced rat chondrocyte apoptosis and cartilage degeneration in a rat osteoarthritis model via AMPK and p38 MAPK signaling. Apoptosis. 2015;20:1187–1199. doi:10.1007/s10495-015-1152-y
122. Hwang HS, Kim HA. Chondrocyte apoptosis in the pathogenesis of osteoarthritis. Int J Mol Sci. 2015;16:26035–26054. doi:10.3390/ijms161125943
123. Ye JN, Su CG, Jiang YQ, et al. Effects of acupuncture on cartilage p38MAPK and mitochondrial pathways in animal model of knee osteoarthritis: a systematic evaluation and meta-analysis. Front Neurosci. 2022;16:1098311. doi:10.3389/fnins.2022.1098311
124. Han X, Lin D, Huang W, Li D, Li N, Xie X. Mechanism of NLRP3 inflammasome intervention for synovitis in knee osteoarthritis: a review of TCM intervention. Front Genet. 2023;14:1159167. doi:10.3389/fgene.2023.1159167
125. Wang Z, Chen M, Wang B, et al. Electroacupuncture alleviates osteoarthritis by suppressing NLRP3 inflammasome activation in guinea pigs. Evid Based Complement Alternat Med. 2020;2020:5476064. doi:10.1155/2020/5476064
126. Cao Y, Tang S, Nie X, et al. Decreased miR-214-3p activates NF-κB pathway and aggravates osteoarthritis progression. EBioMedicine. 2021;65:103283. doi:10.1016/j.ebiom.2021.103283
127. O’Conor CJ, Leddy HA, Benefield HC, Liedtke WB, Guilak F. TRPV4-mediated mechanotransduction regulates the metabolic response of chondrocytes to dynamic loading. Proc Natl Acad Sci U S A. 2014;111:1316–1321. doi:10.1073/pnas.1319569111
128. Westphal D, Kluck RM, Dewson G. Building blocks of the apoptotic pore: how Bax and Bak are activated and oligomerize during apoptosis. Cell Death Differ. 2014;21:196–205. doi:10.1038/cdd.2013.139
129. He J, Zuo J, Fan X, Li Z. Electro-acupuncture modulated miR-214 expression to prevent chondrocyte apoptosis and reduce pain by targeting BAX and TRPV4 in osteoarthritis rats. Braz J Med Biol Res. 2024;57:e13238. doi:10.1590/1414-431X2024e13238
130. Lin J, Wu G, Chen J, et al. Electroacupuncture inhibits sodium nitroprusside‑mediated chondrocyte apoptosis through the mitochondrial pathway. Mol Med Rep. 2018;18:4922–4930. doi:10.3892/mmr.2018.9498
131. Zhang YY, Li XH, Wu MX. Effect of electroacupuncture at Wnt/β-catenin signaling pathway on inhibiting cartilage degeneration in rats with knee osteoarthritis. Zhongguo Zhen Jiu. 2019;39:1081–1086. doi:10.13703/j.0255-2930.2019.10.013
132. Humphries F, Shmuel-Galia L, Ketelut-Carneiro N, et al. Succination inactivates gasdermin D and blocks pyroptosis. Science. 2020;369:1633–1637. doi:10.1126/science.abb9818
133. Sheng W, Liao S, Wang D, Liu P, Zeng H. The role of ferroptosis in osteoarthritis: progress and prospects. Biochem Biophys Res Commun. 2024;733:150683. doi:10.1016/j.bbrc.2024.150683
134. Xie Y, Kang R, Klionsky DJ, Tang D. GPX4 in cell death, autophagy, and disease. Autophagy. 2023;19:2621–2638. doi:10.1080/15548627.2023.2218764
135. Meng D, Lu M, Wu S, et al. Mechanism of acupotomy on chondrocyte ferroptosis in rabbits with knee osteoarthritis based on HSPA5/GPX4 signaling pathway. Zhongguo Zhen Jiu. 2024;44:555–564. doi:10.13703/j.0255-2930.20230901-k0001
136. Jie L, Zhang L, Fu H, et al. Xibining inhibition of the PI3K-AKT pathway reduces M1 macrophage polarization to ameliorate KOA synovial inflammation and nociceptive sensitization. Phytomedicine. 2025;136:156281. doi:10.1016/j.phymed.2024.156281
137. Mizushima N, Komatsu M. Autophagy: renovation of cells and tissues. Cell. 2011;147:728–741. doi:10.1016/j.cell.2011.10.026
138. Tang L, Ding J, Yang K, Zong Z, Wu R, Li H. New insights into the mechanisms and therapeutic strategies of chondrocyte autophagy in osteoarthritis. J Mol Med. 2024;102:1229–1244. doi:10.1007/s00109-024-02473-1
139. Ansari MY, Khan NM, Ahmad I, Haqqi TM. Parkin clearance of dysfunctional mitochondria regulates ROS levels and increases survival of human chondrocytes. Osteoarthritis Cartilage. 2018;26:1087–1097. doi:10.1016/j.joca.2017.07.020
140. Liu J, Zeng WQ, Lin QX, et al. Acupotomy relieves pain and improves motor function by regulating autophagy and apoptosis of cartilage in rabbits with knee osteoarthritis apoptosis. Zhen Ci Yan Jiu. 2022;47:1080–1087. doi:10.13702/j.1000-0607.20211184
141. Lu M, Meng DH, She ZY, et al. Promotion and mechanism of acupotomy on chondrocyte autophagy in knee osteoarthritis rabbits. Chin J Integr Med. 2024;30:809–817. doi:10.1007/s11655-024-3759-8
142. Tang L, Zeng Y, Li L, et al. Electroacupuncture upregulated ghrelin in rats with functional dyspepsia via AMPK/TSC2/Rheb-mediated mTOR inhibition. Dig Dis Sci. 2020;65:1689–1699. doi:10.1007/s10620-019-05960-5
143. Zhu T, Guo C, Du W, et al. Acupotomy alleviates knee osteoarthritis in rabbit by regulating chondrocyte mitophagy Pink1-Parkin pathway. J Tradit Chin Med. 2024;44:468–477. doi:10.19852/j.cnki.jtcm.20240402.001
144. Jiang B, Zhong X, Fang J, et al. Electroacupuncture attenuates morphine tolerance in rats with bone cancer pain by inhibiting PI3K/Akt/JNK1/2 signaling pathway in the spinal dorsal horn. Integr Cancer Ther. 2021;20:1534735421995237. doi:10.1177/1534735421995237
145. Simon TC, Jeffries MA. The Epigenomic Landscape in Osteoarthritis. Curr Rheumatol Rep. 2017;19:30. doi:10.1007/s11926-017-0661-9
146. Si HB, Yang TM, Li L, et al. miR-140 attenuates the progression of early-stage osteoarthritis by retarding chondrocyte senescence. Mol Ther Nucleic Acids. 2020;19:15–30. doi:10.1016/j.omtn.2019.10.032
147. Ding L, Wang H, Li Y, et al. Electroacupuncture stimulating Neixiyan (EX-LE5) and Dubi (ST35) alleviates osteoarthritis in rats induced by anterior cruciate ligament transaction affecting DNA methylation regulated transcription of miR-146a and miR-140-5p. J Tradit Chin Med. 2023;43:983–990. doi:10.19852/j.cnki.jtcm.2023.05.004
148. Zhou X, Cao H, Yuan Y, Wu W. Biochemical signals mediate the crosstalk between cartilage and bone in osteoarthritis. Biomed Res Int. 2020;2020:5720360. doi:10.1155/2020/5720360
149. Qin L, Guo C, Zhao R, et al. Acupotomy inhibits aberrant formation of subchondral bone through regulating osteoprotegerin/receptor activator of nuclear factor-κB ligand pathway in rabbits with knee osteoarthritis induced by modified Videman method. J Tradit Chin Med. 2022;42:389–399. doi:10.19852/j.cnki.jtcm.2022.03.006
150. Ma Y, Hu T, Liu N, et al. Acupotomy ameliorates KOA related chondrocyte premature senescence through YAP/FOXD1 pathway. J Pain Res. 2025;18:2011–2023. doi:10.2147/JPR.S475829
151. Mobasheri A, Rannou F, Ivanavicius S, Conaghan PG. Targeting the TRPV1 pain pathway in osteoarthritis of the knee. Expert Opin Ther Targets. 2024;28:843–856. doi:10.1080/14728222.2024.2416961
152. Harbach H, Moll B, Boedeker RH, et al. Minimal immunoreactive plasma beta-endorphin and decrease of cortisol at standard analgesia or different acupuncture techniques. Eur J Anaesthesiol. 2007;24:370–376. doi:10.1017/S0265021506001906
153. Ahsin S, Saleem S, Bhatti AM, Iles RK, Aslam M. Clinical and endocrinological changes after electro-acupuncture treatment in patients with osteoarthritis of the knee. Pain. 2009;147:60–66. doi:10.1016/j.pain.2009.08.004
154. Mata J, Cabrera S, Sanchís P, et al. Electro-acupuncture for treatment of knee pain from osteoarthritis and the possible endocrinology changes: a study protocol for a randomized controlled trial. Trials. 2015;16:248. doi:10.1186/s13063-015-0766-2
155. Seo BK, Sung WS, Park YC, Baek YH. The electroacupuncture-induced analgesic effect mediated by 5-HT1, 5-HT3 receptor and muscarinic cholinergic receptors in rat model of collagenase-induced osteoarthritis. BMC Complement Altern Med. 2016;16:212. doi:10.1186/s12906-016-1204-z
156. Takano S, Uchida K, Inoue G, et al. Nerve growth factor regulation and production by macrophages in osteoarthritic synovium. Clin Exp Immunol. 2017;190:235–243. doi:10.1111/cei.13007
157. Chiu PE, Fu Z, Sun J, Jian GW, Li TM, Chou LW. Fu’s Subcutaneous Needling for Knee Osteoarthritis Pain. J Vis Exp. 2023. doi:10.3791/65299
158. Chiu PE, Fu Z, Jian GW, Huang CH, Li TM, Chou LW. Evaluating effectiveness of fu’s subcutaneous needling for the pain nature and quality of life in patients with knee osteoarthritis: a study protocol of randomized clinical trial. J Pain Res. 2021;14:3163–3172. doi:10.2147/JPR.S333299
159. Yang X, Wang H, Sun J. Understanding tightened muscle in knee osteoarthritis and the impacts of Fu’s subcutaneous needling: a pilot trial with shear-wave elastography and near-infrared spectroscopy. Medicine. 2024;103:e38274. doi:10.1097/MD.0000000000038274
160. Grässel S, Muschter D. Peripheral nerve fibers and their neurotransmitters in osteoarthritis pathology. Int J Mol Sci. 2017;18:931. doi:10.3390/ijms18050931
161. Chen W, Zhang XN, Su YS, et al. Electroacupuncture activated local sympathetic noradrenergic signaling to relieve synovitis and referred pain behaviors in knee osteoarthritis rats. Front Mol Neurosci. 2023;16:1069965. doi:10.3389/fnmol.2023.1069965
162. Cheng S, Zeng F, Zhou J, et al. Altered static and dynamic functional brain network in knee osteoarthritis: a resting-state functional magnetic resonance imaging study: static and dynamic FNC in KOA. Neuroimage. 2024;292:120599. doi:10.1016/j.neuroimage.2024.120599
163. Salazar-Méndez J, Cuyul-Vásquez I, Viscay-Sanhueza N, et al. Structural and functional brain changes in people with knee osteoarthritis: a scoping review. PeerJ. 2023;11:e16003. doi:10.7717/peerj.16003
164. Seo BK, Park DS, Baek YH. The analgesic effect of electroacupuncture on inflammatory pain in the rat model of collagenase-induced arthritis: mediation by opioidergic receptors. Rheumatol Int. 2013;33:1177–1183. doi:10.1007/s00296-012-2502-5
165. Barroso J, Wakaizumi K, Reis AM, et al. Reorganization of functional brain network architecture in chronic osteoarthritis pain. Hum Brain Mapp. 2021;42:1206–1222. doi:10.1002/hbm.25287
166. Öztürk Ö, Algun ZC, Bombacı H, Erdoğan SB. Changes in prefrontal cortex activation with exercise in knee osteoarthritis patients with chronic pain: an fNIRS study. J Clin Neurosci. 2021;90:144–151. doi:10.1016/j.jocn.2021.05.055
167. Leung A, Zhao Y, Shukla S. The effect of acupuncture needle combination on central pain processing--an fMRI study. Mol Pain. 2014;10:23. doi:10.1186/1744-8069-10-23
168. Cottam WJ, Condon L, Alshuft H, Reckziegel D, Auer DP. Associations of limbic-affective brain activity and severity of ongoing chronic arthritis pain are explained by trait anxiety. Neuroimage Clin. 2016;12:269–276. doi:10.1016/j.nicl.2016.06.022
169. Zheng J, Yang F, Yuan PW, et al. Effect of electroacupuncture on the expression of Iba-1 in spinal dorsal horn and hippocampus of chronic pain rats with knee osteoarthritis. Zhen Ci Yan Jiu. 2023;48:431–437. doi:10.13702/j.1000-0607.20211398
170. Yang KW, Yuan PW, Dong B, et al. Effects of electroacupuncture on pain behavior and pain-related factors in spinal cord dorsal horn and dorsal root ganglia of rats with knee osteoarthritis. Zhen Ci Yan Jiu. 2020;45:818–822. doi:10.13702/j.1000-0607.200540
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
The Role of Acupuncture and Its Related Mechanism in Treating Chronic Prostatitis/Chronic Pelvic Pain Syndrome
Wang H, Zhang J, Ma D, Zhao Z
International Journal of General Medicine 2023, 16:4039-4050
Published Date: 6 September 2023
Effect of Traditional Chinese Non-Pharmacological Therapies on Knee Osteoarthritis: A Narrative Review of Clinical Application and Mechanism
Liu ZF, Zhang Y, Liu J, Wang YY, Chen M, Liu EY, Guo JM, Wang YH, Weng ZW, Liu CX, Yu CH, Wang XY
Orthopedic Research and Reviews 2024, 16:21-33
Published Date: 26 January 2024
Treatment of Depression with Acupuncture Based on Pathophysiological Mechanism
Sun B, Cao X, Xin M, Guan R
International Journal of General Medicine 2024, 17:347-357
Published Date: 31 January 2024
Mechanism of Traditional Chinese Medicine in Treating Migraine: A Comprehensive Review
Chen Q, Wang M, Fu F, Nie L, Miao Q, Zhao L, Liu L, Li B
Journal of Pain Research 2024, 17:3031-3046
Published Date: 17 September 2024