Back to Journals » Infection and Drug Resistance » Volume 15
Antimicrobial Resistance Trends of the Most Common Causative Pathogens Associated with Community-acquired Respiratory Infections in China: 2009–2018
Authors Zhao C, Yang S, Zhang F, Wang Z, Zhang Y, Wang X, Li H ![]() , Chen H
, Chen H ![]() , Wang H
, Wang H
Received 21 May 2022
Accepted for publication 5 August 2022
Published 31 August 2022 Volume 2022:15 Pages 5069—5083
DOI https://doi.org/10.2147/IDR.S374805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Chunjiang Zhao, Shuo Yang, Feifei Zhang, Zhanwei Wang, Yawei Zhang, Xiaojuan Wang, Henan Li, Hongbin Chen, Hui Wang
Department of Clinical Laboratory, Peking University People’s Hospital, Beijing, People’s Republic of China
Correspondence: Hui Wang, Department of Clinical Laboratory, Peking University People’s Hospital, No. 11, Xizhimen South Street, Xicheng District, Beijing, 100044, People’s Republic of China, Email [email protected]
Background: Emergence of antimicrobial resistance poses new challenges in the management of community acquired respiratory tract infections (CARTIs). Therefore, surveillance on the antimicrobial susceptibilities of common respiratory pathogens is valuable and guides empirical therapeutic choices in management of CARTIs.
Objective: The objective of the current study is to summarize the antimicrobial resistance trends in common respiratory tract pathogens isolated from patients with CARTIs in China, over a 10-year period (2009– 2018).
Methods: Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis strains were collected from multicenter, and antimicrobial susceptibility testing was performed in the research central laboratory of each study period from 2009– 2018. The pathogens that accounted for CARTIs in the adult population was considered and summarized.
Results: From 2009– 2018 a total of 3750 isolates were collected from 22 cities located across different regions of China. Among these the most common bacterial isolates include S. pneumoniae (53.7%) followed by H. influenza (32.4%), M. catarrhalis (13.9%). S. pneumoniae exhibited reduction in susceptibility and increase in resistance to penicillin, cephalosporins (cefaclor, cefuroxime, ceftriaxone) during the surveillance period. Invasive and noninvasive S. pneumoniae showed similar resistance. In the case of H. influenzae susceptibility to β-lactam and β-lactamase inhibitors (ampicillin, amoxicillin and AMC), SXT, clarithromycin and cephalosporins (cefuroxime, cefaclor, ceftazidime) was reduced over the past 10 years with an exception of ceftriaxone. Overall, moxifloxacin and levofloxacin have the highest susceptibility rates against S. pneumoniae (> 95%) and H. influenza (> 90%). M. catarrhalis exhibited susceptibility to almost all the tested antimicrobials.
Conclusion: In China the 10-year trends showed a substantial increase in resistance to β-lactam drugs and reduction in sensitivity. However, certain antimicrobial agents namely fluoroquinolones including moxifloxacin and levofloxacin maintained low resistance rates with better susceptibility. Further, with few exceptions decline in susceptibility rates to macrolides and cephalosporins was observed among the tested pathogens.
Keywords: Community-acquired respiratory tract infections, antimicrobial resistance, susceptibility, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis
Introduction
Globally, community-acquired respiratory tract infections (CARTIs) are a serious public health problem representing a leading cause of hospitalization and accounts for a significant proportion of antimicrobial prescriptions.1,2 Typically, there are three major bacterial pathogens namely Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis that account for CARTIs.3,4 Treatment for CARTI is often empirical as isolation, identification, and local drug susceptibility test to guide treatment is not feasible for each individual patient.5 Furthermore, β-lactam and other substitute antibiotics are the common principal therapeutic agents used in the empiric management of CARTIs.6,7 Community-acquired respiratory infection is a common type of community-acquired infection in China. There are usually no conditions for etiological testing in community hospitals, so it mainly relies on empirical treatment. The guidelines in China also recommend empirical treatment as the first choice for community-acquired respiratory infections.8 At this juncture, several studies reported high resistance rates of these pathogens to the more commonly used antimicrobial agents thereby complicating the empirical therapy in CARTIs management.9,10 However, the distribution of these major bacterial pathogens and development of antimicrobial resistance varies across different regions.11
Surveillance is the cornerstone in understanding and controlling antimicrobial resistance. Although there were many drug resistance surveillance programs in mainland China, Taiwan, and other Asian regions, there were few drug resistance surveillance programs dedicated to monitoring the main pathogens of community-acquired respiratory infections. Furthermore, knowledge of local resistance patterns and predominant mechanisms underlying the resistance development plays a pivotal role in success of empiric therapy.12 In this context, the main objective of the current community-acquired respiratory tract infection pathogen surveillance (CARTIPS) study is to summarizes the susceptibility and resistance trends of various primary CARTI pathogens (S. pneumoniae, H. influenzae and M. catarrhalis) against conventional antimicrobials in the adult Chinese population. The CARTIPS study published two articles, in 201110 and 2016.9 Combined with previous studies, changes in antimicrobial resistance over long timescales (2009–2018) can be clearly demonstrated, providing solid evidence for future empirical treatment and prevention of the emergence of drug-resistant strains.
Materials and Method
Participating Centers and Profile of Strains
Between 2009 and 2018 around 34 hospitals from 22 cities of China (Beijing, Changchun, Changsha, Chengdu, Chongqing, Guangzhou, Hangzhou, Harbin, Hefei, Hohhot, Jinan, Kunming, Nanchang, Nanning, Shanghai, Shenyang, Tianjin, Urumchi, Wuhan, Xian, Yinchuan, Zhengzhou) took part in this study (Figure 1).
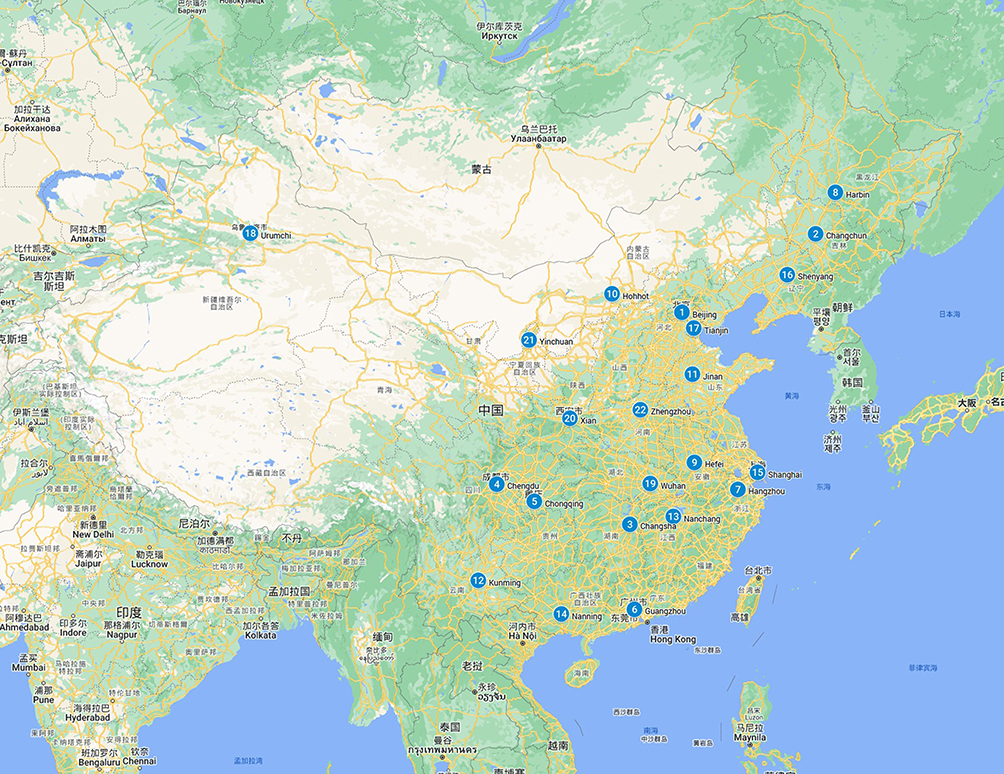 |
Figure 1 Geographical location of different cities participating in this study. |
Patients aged >18 years with clinically diagnosed CARTIs, such as community-acquired pneumonia, acute attack of chronic bronchitis, acute attack of chronic obstructive pulmonary disease, acute and/or chronic tonsillitis, pharyngitis and sinusitis occurring in the community or within 48 hour after hospital admission were included. Patients aged <18 years, nonpathogenic strains, duplicate isolates, colonization by bacteria without any clinical evidence of infection and noncommunity-acquired pathogenic strains isolated from patients who had been hospitalized for >48 h were excluded from the study.
Strains isolated form specimens obtained by invasive procedures were considered as pathogenic strains. The most majority of noninvasive strains were cultured from sputum, and the quality of sputum specimens were assessed to determine whether the isolates were pathogenic. For some cases imaging evidence (such as X-ray) was also used to determine pathogenicity of cultured strains. During the study period major bacterial pathogens namely S. pneumoniae (2015 isolates), H. influenzae (1215 isolates), M. catarrhalis (520 isolates) that are deemed pathogenic for CARTIs were collected from the Chinese adult patients. Further, based on combined results of culture test and immunopathology the isolates were judged to be pathogenic bacteria or colonized bacteria and the pathogenic bacteria were included in the study. Specimens from nasal and pharyngeal swab, sputum with white blood cells (WBC) >25 and squamous epithelial cells <10 under low power microscopy were considered as qualified. Other specimens such as blood, pleural effusion and cerebrospinal fluid (CSF) were considered as sources for invasive bacterial infections. The number of strains from every center collected in each monitoring year was presented in Supplementary Table 1.
The Ethics Statement
All the adult patients participating in this study signed informed consent. The study protocols of different years were approved by the Ethics Committee of the Peking University People’s Hospital (No. 2010PHB065, No. 2013PHB188, No. 2014PHB104, No. 2016PHB135, No. 2018PHB129), and all procedures were conducted according to the Declaration of Helsinki revised in 2008.
In vitro Antimicrobial Susceptibility Testing
The agar dilution method was used to determine the minimum inhibitory concentrations (MICs) of all S. pneumoniae isolates against antibiotics commonly used in community. For H. influenza and M. catarrhalis, broth microdilution method was used for the determination of MICs of different antibiotics. All the tests were strictly in accordance with the guidelines established by the Clinical and Laboratory Standards Institute (CLSI).13
In China, combined with the distribution characteristics of pathogenic bacteria and the antibacterial spectrum of antibacterial drugs, β-lactams, macrolides and fluoroquinolones were usually used for empirical treatment of community-acquired respiratory infections in adults.14 There were 16 antibiotics tested in this study includes penicillin (only for S. pneumoniae), amoxicillin-clavulanic acid, ampicillin (only for H. influenzae), cefaclor, cefuroxime, ceftriaxone, vancomycin (only for S. pneumoniae), erythromycin (only for S. pneumoniae), azithromycin, clarithromycin, tetracycline, levofloxacin, moxifloxacin (for S. pneumoniae and H. influenzae), sulfamethoxazole-trimethoprim, chloramphenicol, and clindamycin. All drug standards used in the current study were purchased from the National Institute for the Control of Pharmaceutical and Biological Products, China. For S. pneumoniae and H. influenzae, the CLSI 2017 criteria were applied to classify isolates as susceptible (S), intermediate (I), or resistant (R).
For S. pneumoniae, the oral penicillin breakpoint was used to classify isolates as penicillin-susceptible (MIC ≤0.06 μg/mL), penicillin-intermediate (MIC between 0.12 and 1 μg/mL), and penicillin-resistant (MIC ≥2 μg/mL). Penicillin non-meningitis breakpoints (susceptible, MIC ≤2 μg/mL; resistant, MIC ≥8 μg/mL) and penicillin meningitis breakpoints (susceptible, MIC ≤0.06 μg/mL; resistant, MIC ≥0.12 μg/mL) were also applied to evaluation the susceptibilities. For ceftriaxone, the non-meningitis breakpoints (susceptible, MIC ≤1 μg/mL; resistant, MIC ≥4 μg/mL) and meningitis breakpoints (susceptible, MIC ≤0.5 μg/mL; resistant, MIC ≥2 μg/mL) were used to classify isolates as susceptible and resistant.15 For M. catarrhalis, resistance was interpreted according to the breakpoints in CLSI M45-A2.16
S. pneumoniae ATCC 49619 was used as the quality control strain and was included in each batch of tests to ensure accurate results. MIC50 and MIC90 (MICs that inhibit 50% and 90% of the isolates, respectively) were calculated by R. Multidrug-resistance was defined as tested strains which were resistant to at least three different antibiotic classes simultaneously. Nitrocefin disk (Oxoid, UK) was used for the detection of β-lactamase production17 by H. influenzae and M. catarrhalis. For S. pneumoniae strains that tested erythromycin-resistant and clindamycin-susceptible or -intermediate, the D-zone test was performed to detect inducible clindamycin resistance in accordance with CLSI guidelines.13 Moreover, differences in the antibiotic susceptibility patterns between the earlier and later study years for a given antimicrobial agent were compared to the resistance profiles of respiratory isolates of the period 2009–10, 2012, 2013–14, 2016 and 2018.
Statistical Analysis
Data from the antibiotic susceptibility tests were analyzed using WHONET 5.6 software, a Windows-based database software developed by the World Health Organization for managing and analyzing microbiological laboratory data with a special focus on the analysis of antimicrobial susceptibility test results. The chi-squared and Fisher’s exact probability tests were performed using R version 4.0.2 to compare proportions. Data visualization was done with ggplot2 package version 3.3.2.18 A p-value less than 0.05 was considered statistically significant.
Results
Profile of Pneumococcal Isolates
During the surveillance period 2009–2018, a total of 3750 nonduplicated isolates were collected from 34 representative hospitals located across 22 different regions of mainland China. All the strains were divided into East (788), Middle (357), North (1392), Northeast (320), Northwest (282), South (292) and Southwest (319) by their geological locations. Among these the most common bacterial isolates include S. pneumoniae (2015, 53.7%) followed by H. influenza (1215, 32.4%), M. catarrhalis (520, 13.9%). The strains were mainly isolated from elderly patients, 48% (1800/3750) of the strains were isolated from patients over 60 years old; only 20.4% (764/3750) of the strains were isolated from patients under 40 years old. Sputum was the most important specimen type (3071 strains, 81.9%), followed by bronchoalveolar lavage fluid (269 strains, 7.2%), throat swab (165 strains, 4.4%) and blood (152 strains, 4.1%). The specific number of strains collected by various centers in different regions in different years were summarized in Supplementary Table 1.
Antimicrobial Susceptibility of S. pneumoniae
The overall in vitro activities of the tested antimicrobial agents against S. pneumoniae strains during the study periods were shown in Table 1. Based on the MIC breakpoints of oral penicillin criteria, the overall rate of penicillin-resistant S. pneumoniae (PRSP), penicillin-intermediate S. pneumoniae (PISP), and penicillin-susceptible S. pneumoniae (PSSP) isolates was 40.8% (822/2015), 17.8% (359/2015), and 41.4% (834/2015), respectively. Macrolide and tetracycline exhibited limited antibacterial effects against S. pneumoniae during the study periods. The resistant rate of S. pneumoniae to erythromycin, azithromycin, clarithromycin, clindamycin, and tetracycline was 93.3%, 91.4%, 90.4%, 86.7%, and 91.5%, respectively. Furthermore, 1880 (93.3%) strains were resistant to erythromycin, and of these, 1588 were resistant to clindamycin simultaneously. For PSSP strains, all β-lactams except cefaclor showed excellent antibacterial activity, with susceptibility rates of >99%. Most PISP strains were susceptible to AMC, ceftriaxone, quinolones and chloramphenicol with susceptibility rates of >89%. However, compared with PSSP and PISP, the sensitivity of PRSP to ceftriaxone and AMC decreased to 47.9% and 34.8% respectively. In regard to PRSP isolates, cefuroxime, cefaclor, SXT, macrolides, tetracycline and clindamycin showed very low antibacterial activity (Table 2). Ceftriaxone had a good antibacterial activity against S. pneumoniae, but the average resistance rate of S. pneumoniae to cefaclor had exceeded 50%, as well as cefuroxime. vancomycin, fluoroquinolones and chloramphenicol have high antibacterial activity against S. pneumoniae. No S. pneumoniae strains resistant to vancomycin have been found. The resistance rate of S. pneumoniae to fluoroquinolones was less than 3%, and the resistance rate to moxifloxacin was less than 1%. Compared to levofloxacin, moxifloxacin usually have lower MIC50 and MIC90 values against S. pneumoniae (1 μg/mL vs 0.125 μg/mL and 1 μg/mL vs 0.25 μg/mL). The resistance rate of S. pneumoniae to fluoroquinolones remained constant in the whole time span. Of all S. pneumoniae strains 60.9% (1227/2015) showed multi-drug resistance (MDR, Supplementary Table 2). Invasive and non-invasive strains demonstrated parallel resistance rate in all antibiotics tested in this study and the differences were not statistically significant (Table 3). The most common drug-resistant phenotype was simultaneously resistant to β-lactams, macrolides, tetracycline and sulfonamides, accounting for 53.1% (651/1227) of all multidrug resistant strains. S. pneumoniae strains showed a higher rate of resistance to β-lactams in age groups younger than 40 years than in age groups older than 60 years, most notably in penicillin, cefuroxime and ceftriaxone (Figure 2).
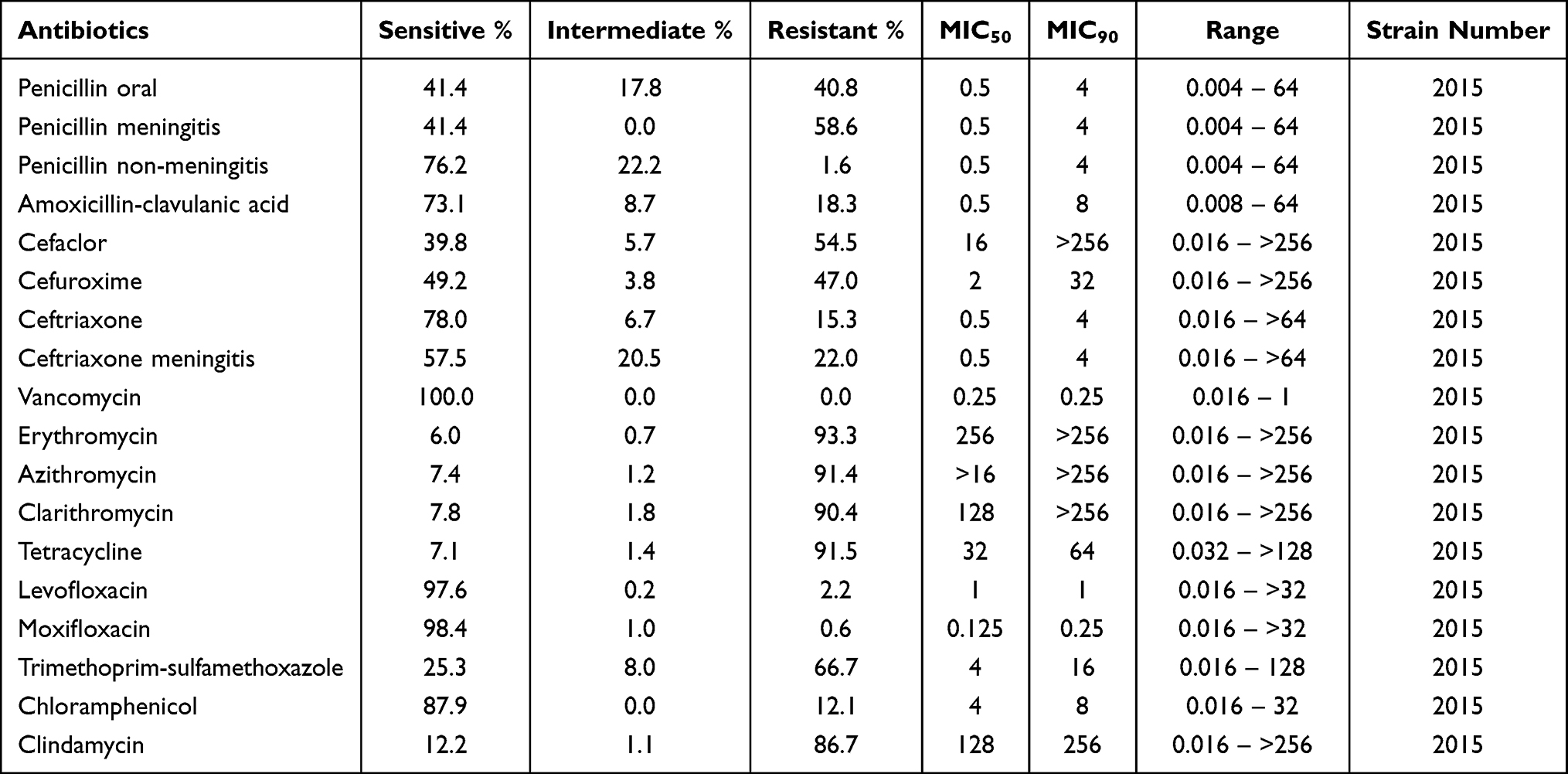 |
Table 1 The Overall Resistance Rate of S. pneumoniae to Different Antibacterial Agents, from 2010 to 2018 |
 |
Table 2 The Overall Resistance Rate of PSSP, PISP and PRSP to Different Antibacterial Agents, from 2010 to 2018 |
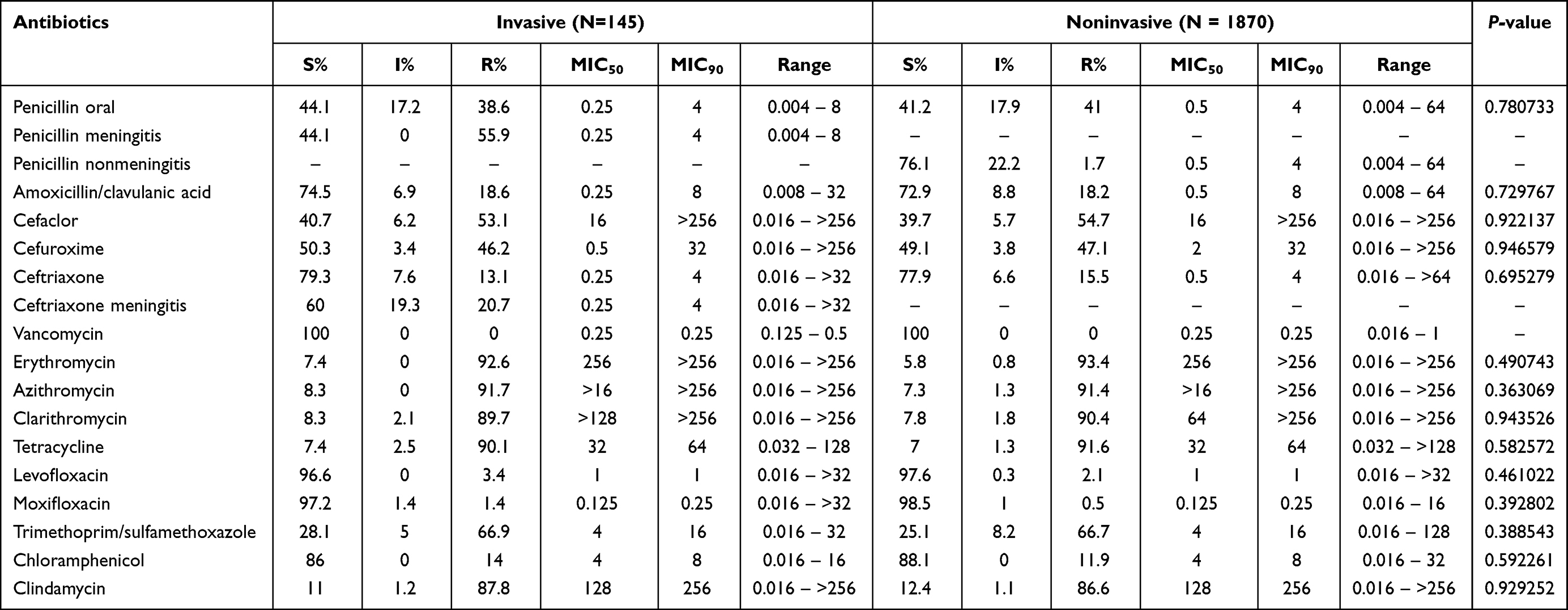 |
Table 3 The Differences in Drug Resistance Rates Between Invasive and Noninvasive S. pneumoniae |
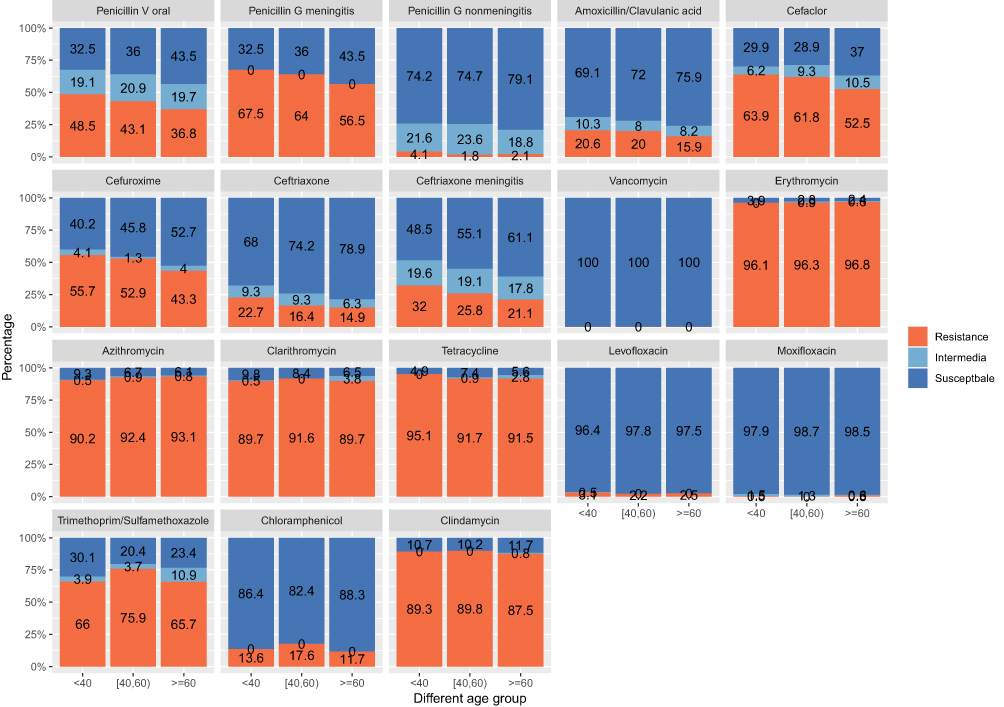 |
Figure 2 Changes in resistance rates of S. pneumoniae to various drugs in different age groups. |
During the study period, a striking uptrend of resistance was observed, especially for β-lactams. The resistance to penicillin (oral) raised from 24.4% in 2010 to 61.6% in 2018, and other β-lactams shared the similar trend. Although the resistance rate was relatively low in cephalosporins, a clear and definitive upward trend of the resistance rate was observed. For macrolides, the resistance rate remains at high level during the entire study period. (Figure 3).
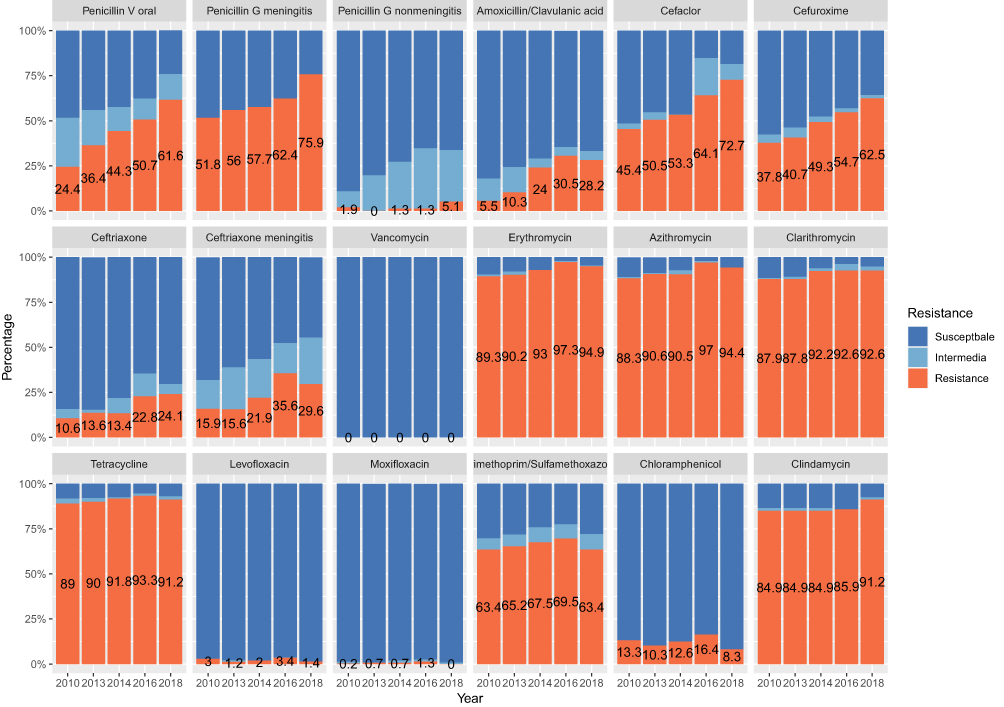 |
Figure 3 Resistance of S. pneumoniae to routine antibiotics in different years. |
Antimicrobial Susceptibility of H. influenzae
For H. influenzae, most of the tested antimicrobial agents showed excellent activity against isolates from different years from China (Table 4). SXT and ampicillin showed relatively lower activity against H. influenzae, with resistance rates of 36.6% and 60.5%, respectively. Ceftriaxone, levofloxacin, moxifloxacin, azithromycin and chloramphenicol demonstrated high activity (>90%) against all H. influenzae strains. During all research periods, there were 319 (26.3%) β-lactamase positive strains, among all 1215 H. influenzae strains. The rates of β-lactamase producing strains have shown a clear upward trend, from 14.5% in 2010 to 35.1% in 2018.
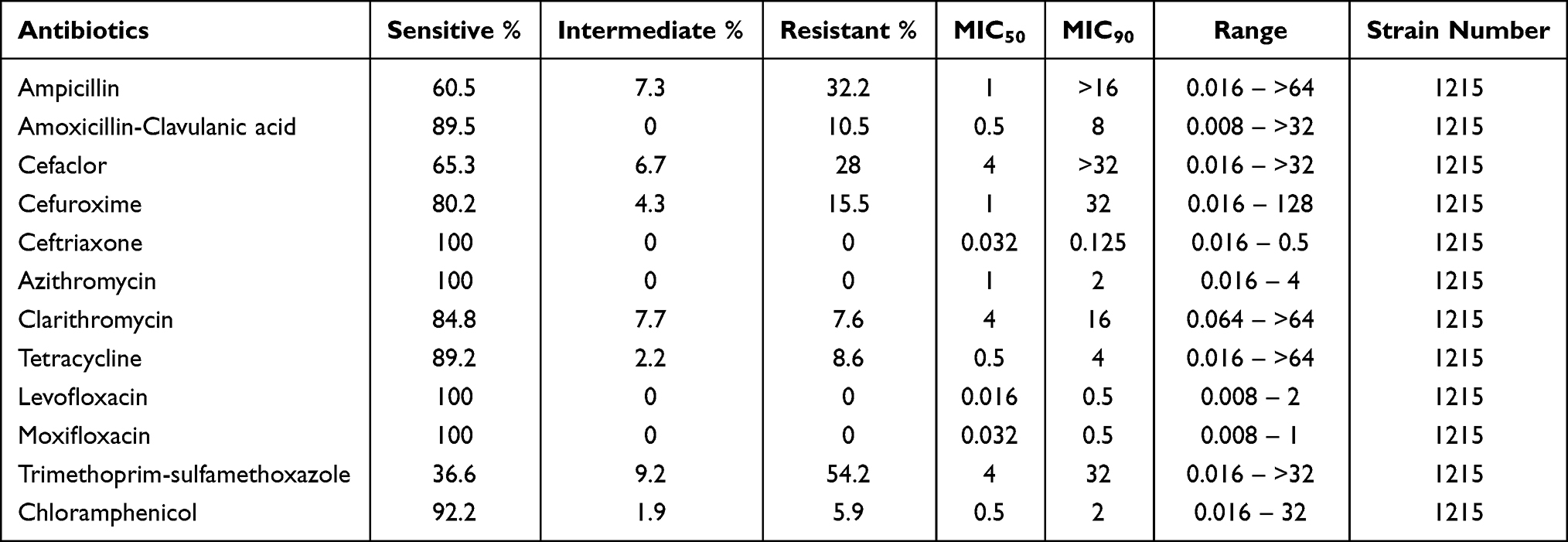 |
Table 4 The Overall Resistance Rate of H. influenzae to Different Antibacterial Agents, from 2010 to 2018 |
Rates of β-lactamase producing H. influenzae varied with geographical regions, with the highest rate of 42.2% (46/109) in Southwest, followed by 29.9% (23/77) in Northeast, 27.5% (25/91) in Northwest, 27.1% (92/340) in East, 23.6% (93/394) in North, 20.6% (21/102) in Middle and 18.6% (19/102) in South. In addition, for β-lactamase negative strains, there were 79 strains demonstrated resistance to ampicillin, regarding as β-lactamase-negative ampicillin-resistant (BLNAR) strains. Resistance rates of BLNAR strains to ampicillin, AMC, cefaclor and cefuroxime were 100%, 67.5%, 77.5% and 55.0%, respectively. Compared with β-lactamase negative strains, β-lactamase positive H. influenzae usually exhibited higher resistance rates to β-lactams agents (Table 5). Although H. influenzae strains were sensitive to a variety of antibacterial agents tested, a remarkable upward trend of resistance rate was still observed during the entire study periods, especially in ampicillin, AMC, cefaclor and cefuroxime (Figure 4). The incidence of multidrug resistance (MDR) in H. influenzae was 10.0% (122/1215), and the most important multidrug resistance pattern was simultaneously resistant to β-lactams, macrolides and co-sulfonamides, accounting for 41.0% (50/122) of all MDR strains (Supplementary Table 3).
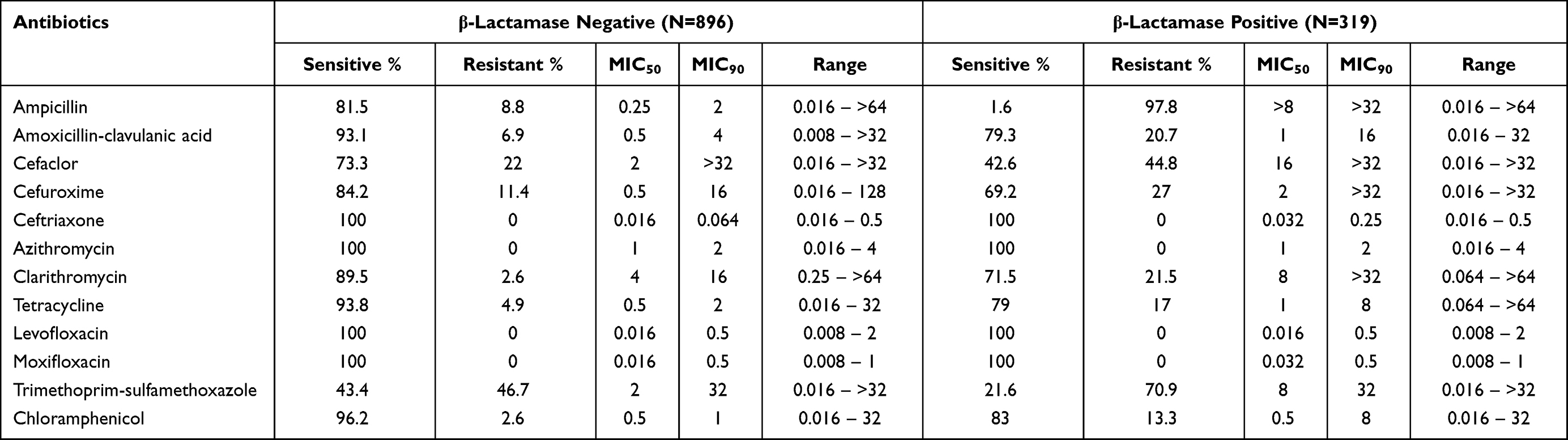 |
Table 5 The Sensitivities of β-Lactamase Negative and Positive H. influenzae to Different Antibacterial Agents, from 2010 to 2018 |
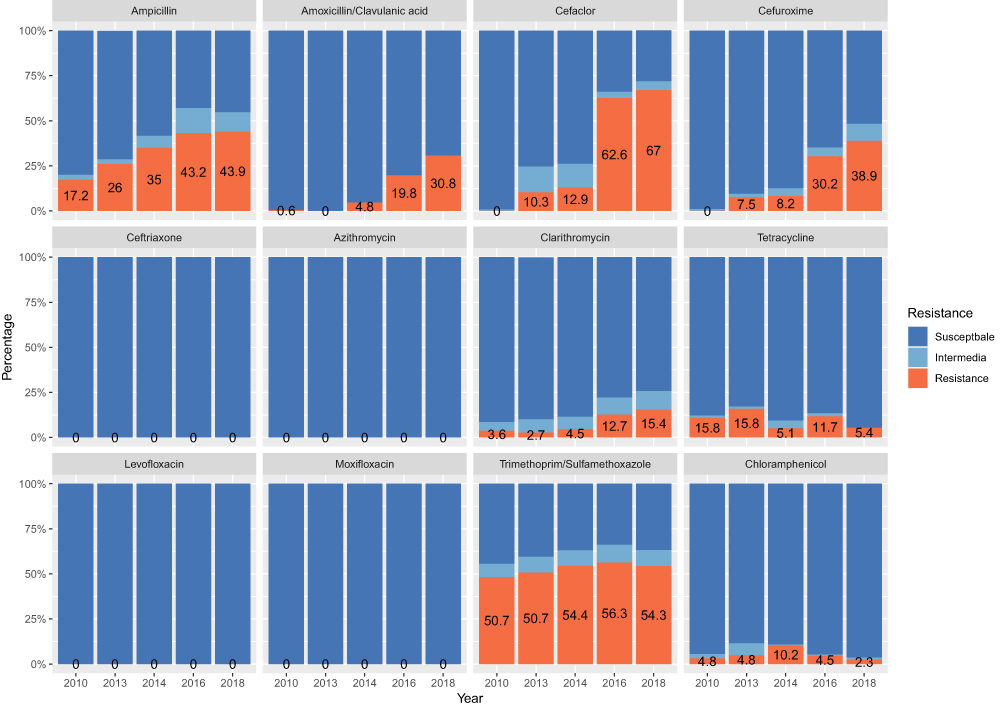 |
Figure 4 Resistance of H. influenzae to routine antibiotics in different years. |
Antimicrobial Susceptibility of M. catarrhalis
Most of the antimicrobial agents showed excellent activities against 520 isolates of M. catarrhalis, with susceptibility rates of >90%. M. catarrhalis strains from this study were 100% sensitive to amoxicillin-clavulanic acid, ceftriaxone, azithromycin, clarithromycin, and levofloxacin. However, clindamycin, trimethoprim-sulfamethoxazole and cefaclor showed relatively low activity against M. catarrhalis (Table 6). In addition, 90.8% of M. catarrhalis isolates produced a β-lactamase in this study. During the study period, the β-lactamase positive rate rose from 82.6% in 2010 to 94.4% in 2018 (Figure 5). The MDR in M. catarrhalis was much lower compared with S. pneumoniae and H. influenzae. The important patterns of MDR in M. catarrhalis isolates were summarized in Supplementary Table 4.
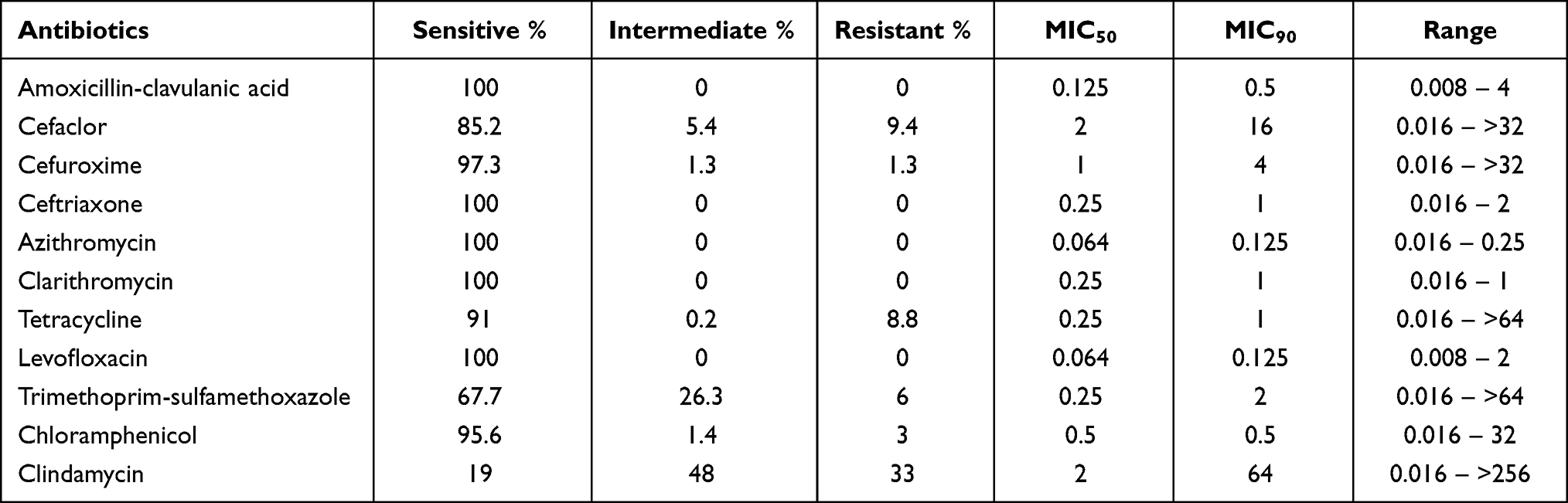 |
Table 6 The Overall Resistance Rate of M. catarrhalis to Different Antibacterial Agents, from 2010 to 2018 |
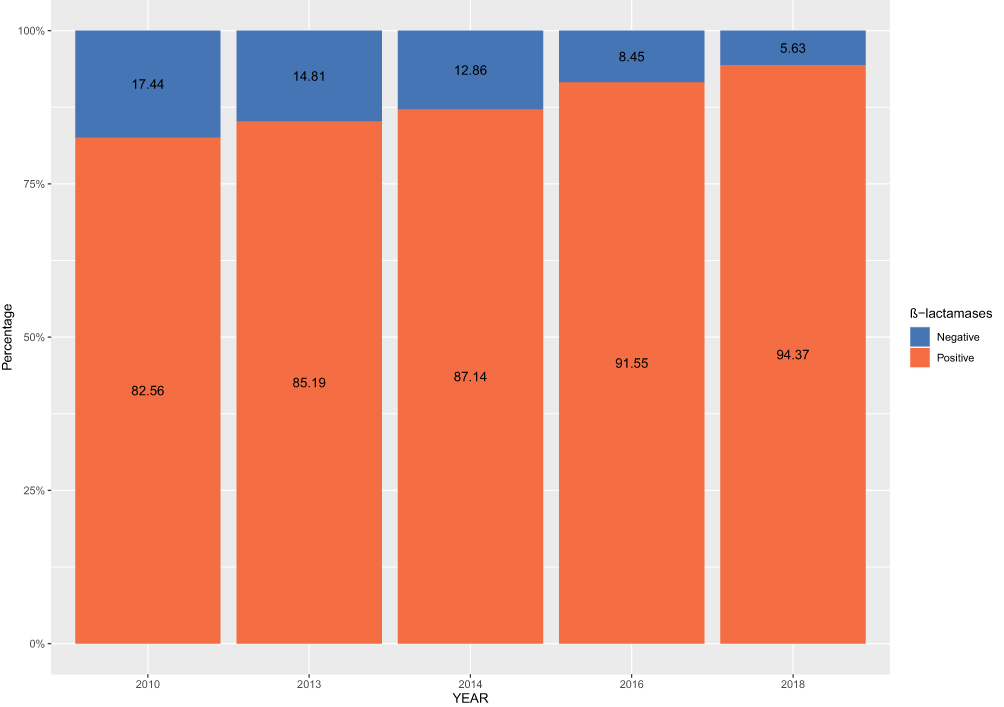 |
Figure 5 The prevalence of β-lactamase positive M. catarrhalis in different years. |
The three bacteria in this study showed different drug resistance in different regions, and the drug resistance rate in northwest China was higher than that in other regions, especially for β-lactams. Supplementary Figures 1–3 show the resistance rates of S. pneumoniae, H. influenzae and M. catarrhalis to different drugs, respectively.
Discussion
This study updated the antimicrobial resistance trend of the major pathogens that cause CARTI in Chinese adults. S. pneumoniae, H. influenzae and M. catarrhalis were the most frequently isolated bacterial pathogens associated with CARTIs and were becoming more and more resistant to commonly used antimicrobial agents, according to the findings of this long-term research. Successful management and treatment of CARTIs requires timely administration of effective therapeutic agents. At this juncture, clinical decisions on empirical therapy require knowledge of possible pathogens and their susceptibilities to antimicrobials. However, such knowledge can be gained in result of clinical practice experience over time, but more objectively and robustly through surveillance. Moreover, the prevalence of resistance rates to commonly used antimicrobials in the management of CARTIs is alarming. Furthermore, there are fewer drug resistance monitoring surveillance studies focused on CARTIs in China and the majority of studies reported results from nosocomial infections. The current monitoring of nosocomial infection shows that the drug resistance rate is also increasing year by year, especially the proportion of CRE (carbapenem resistant Enterobacteriaceae) is increasing.19 Although the pathogens of community-acquired infection and nosocomial infection are different, they all show a trend of increasing drug resistance.
Based on the MIC breakpoints of oral penicillin, the percentage of PRSP in this study increased drastically from 24.2% in 2010 to 61.6% in 2018. Previous study suggested the high resistance due to clonal spread of resistance clones, such as 19F-ST271 and 19A-ST320 strains.20,21 In this study, S. pneumoniae strains demonstrated a high drug resistant rate to β-lactam drugs as well as to macrolides, which posed a severe challenge to actual clinical treatment and may cause clinical treatment failure in actual clinical practice. Fluoroquinolones maintained high sensitivity to S. pneumoniae in this study, and can be applied as the first choice for the treatment of CARTI in appropriate populations, such as adults.
In addition to the weak antibacterial activities of macrolides against S. pneumoniae in this study, macrolides showed strong antibacterial activity against both H. influenzae and M. catarrhalis isolates. Although the antibacterial activity against S. pneumoniae was relative weaker in this study, considering the higher safety boundary and strong tissue penetration of macrolides,22 especially in lung tissue, macrolides can be used as multi-therapy in combination with β-lactam or amoxicillin-clavulanate.23 The MIC results of erythromycin and clindamycin suggested MLSB phenotype was the most prevalent phenotype in China and this result was consistent with previous research.24,25
For the prevention and treatment of S. pneumoniae, in addition to the standardized application of conventional antibacterial regents, pneumococcal vaccine was also an important supplementary measurement, especially in groups with risk factors for pneumococcal infection.26 As the pneumococcal vaccine has not been included in the Chinese immunization program, the pneumococcal vaccine has not been widely used in China. PCV-7 vaccine had been introduced in China since 2008, and it was replaced by PCV-13 vaccine in 2016, which can prevent pneumococcal infection of 13 different serotypes.27,28 Previous studies have shown that the current pneumococcal vaccine PCV-13 can effectively cover the main drug-resistant serotypes in China, and the vaccine coverage rate in adults was 62%.21 If the vaccine were widely used, it will definitely impose a significant impact on the distribution of pneumococcal serotypes and resistant clones, and this will be a new opportunity for the rational use of antibacterial drugs.
Ampicillin and amoxicillin were the drugs of choice for the treatment of H. influenzae infection. The data of this study showed that the resistance rate of H. influenzae to ampicillin rose rapidly from 17.2% in 2010 to 43.9% in 2018. This study showed that the resistance rate of H. influenzae to ampicillin was 32.2%, and the positive rate of β-lactamase was 26.3%. There were 79 β-lactamase-negative ampicillin resistant (BLNAR) strains in this study, which were considered to be resistant to β-lactams such as AMC, ampicillin-sulbactam, cefaclor and cefuroxime, although they were susceptible to some of the antimicrobials in vitro.29 In this study, ceftriaxone, levofloxacin, moxifloxacin, azithromycin, chloramphenicol and tetracycline showed high activity against BLNAR strains, with susceptibility rates of >92.2%.
In the case of M. catarrhalis, although the rate of β-lactamase positivity was very high, the antibacterial drug susceptibility testing results show that M. catarrhalis strains were still highly susceptible to β-lactam agents, indicating that the effect used for the β-lactamase produced by M. catarrhalis was relatively weak and that current β-lactam drugs remained stable against it, thus allowing for the application of such antibiotics in empirical clinical treatment. Further research and testing is needed to determine exactly what type of β-lactamases are produced by M. catarrhalis in China.
In this study, strains from the north-western region showed high resistance rates, while strains isolated from the east and south showed relatively low resistance rates. The possible reasons for this phenomenon are, firstly, the small number of hospitals participated in the north-west included in the study, such differences being due to random errors, and secondly, the association with antibiotics use habits and vaccination rates (especially for S. pneumoniae). The north-western region of China is relatively economically less developed, whereas in the eastern and southern coastal regions the level of economic development is high. S. pneumoniae vaccination is not included in the national immunization in China and vaccines need to be paid for themselves. The serotypes covered by the PCV13 are mostly those with high resistance rates, and because of the relatively high vaccination rates in the east and south, the proportion of S. pneumoniae with high resistance serotypes decreases, resulting in lower resistance rates. Previous studies have also confirmed the impact of the level of economic development on S. pneumoniae antibiotic resistance rates.21
Although this research mainly focused on the changes in the drug resistance of the main pathogens in community-acquired respiratory infections, it was difficult to conduct standardized pathogenic diagnosis in communities. The pathogens collected in this study are mainly from large medical centers in huge cities. Strains may not fully represent the true resistance properties of strains from communities especially in remote rural areas. For example, relatively serious infections that the community cannot deal with will be finally diagnosed and treated in a sophisticated hospital. The pathogens isolated in this way may be more resistant than the strains in the real communities. This is called survivorship bias and results of this study could overestimate the actual resistance rate of pathogens in the real community.
In conclusion, the results of this study confirmed the excellent activities of fluoroquinolones, including levofloxacin and moxifloxacin, against S. pneumoniae, H. influenzae and M. catarrhalis. However, the susceptibilities to azithromycin, clarithromycin, erythromycin and β-lactams among these pathogens were on the decrease. Regional variations were also found in the antimicrobial susceptibilities of these CARTI pathogens. Given the high rate of resistance and limited data from rural areas, continuous national surveillance of the epidemiology of CARTIs is strongly warranted in China.
Abbreviations
CARTIs, community-acquired respiratory tract infections; CARTIPS, community-acquired respiratory tract infection pathogen surveillance; BALF, bronchoalveolar lavage fluid; CSF, cerebrospinal fluid; WBC, white blood cells; CLSI, Clinical and Laboratory Standards Institute; MIC, minimum inhibitory concentration; PSSP, penicillin-susceptible S. pneumoniae; PISP, penicillin-intermediate S. pneumoniae; PRSP, penicillin-resistant S. pneumoniae; AMC, amoxicillin and clavulanic acid; SXT, sulfamethoxazole and trimethoprim.
Funding
This study was sponsored by Bayer China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ho J, Ip M. Antibiotic-resistant community-acquired bacterial pneumonia. Infect Dis Clin North Am. 2019;33:1087–1103. doi:10.1016/j.idc.2019.07.002
2. Song J-H, Huh K, Chung DR. Community-acquired pneumonia in the Asia-Pacific region. Semin Respir Crit Care Med. 2016;37:839–854. doi:10.1055/s-0036-1592075
3. Dunne EM, Murad C, Sudigdoadi S, et al. Carriage of Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, and Staphylococcus aureus in Indonesian children, A cross-sectional study. PLoS One. 2018;13:e0195098. doi:10.1371/journal.pone.0195098
4. Hirai J, Kinjo T, Koga T, Haranaga S, Motonaga E, Fujita J. Clinical characteristics of community-acquired pneumonia due to Moraxella catarrhalis in adults, a retrospective single-centre study. BMC Infect Dis. 2020;20:821. doi:10.1186/s12879-020-05564-9
5. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. an official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200:e45–e67. doi:10.1164/rccm.201908-1581ST
6. Bush K, Bradford PA. β-Lactams and β-Lactamase inhibitors, an overview. Cold Spring Harb Perspect Med. 2016;6:a025247. doi:10.1101/cshperspect.a025247
7. Thakuria B, Lahon K. The beta lactam antibiotics as an empirical therapy in a developing country, an update on their current status and recommendations to counter the resistance against them. J Clin Diagn Res. 2013;7:1207–1214. doi:10.7860/JCDR/2013/5239.3052
8. Xiao Y. Antimicrobial stewardship in China, systems, actions and future strategies. Clin Infect Dis. 2018;67 suppl_2:S135–S141. doi:10.1093/cid/ciy641
9. Zhang Y, Zhang F, Wang H, et al. Antimicrobial susceptibility of Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis isolated from community-acquired respiratory tract infections in China, results from the CARTIPS antimicrobial surveillance program. J Glob Antimicrob Resist. 2016;5:36–41. doi:10.1016/j.jgar.2016.03.002
10. Wang H, Chen M, Xu Y, et al. Antimicrobial susceptibility of bacterial pathogens associated with community-acquired respiratory tract infections in Asia, report from the Community-Acquired Respiratory Tract Infection Pathogen Surveillance (CARTIPS) study, 2009–2010. Int J Antimicrob Agents. 2011;38:376–383. doi:10.1016/j.ijantimicag.2011.06.015
11. Prestinaci F, Pezzotti P, Pantosti A. 10 Antimicrobial resistance, a global multifaceted phenomenon. Pathog Glob Health. 2015;109:309–318. doi:10.1179/2047773215Y.0000000030
12. Inoue M, Farrell DJ, Kaneko K, et al. Antimicrobial susceptibility of respiratory tract pathogens in Japan during PROTEKT years 1–5 (1999–2004). Microb Drug Resist. 2008;14:109–117. doi:10.1089/mdr.2008.0806
13. CLSI. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved St Andard.
14. Cao B, Huang Y, She D-Y, et al. Diagnosis and treatment of community-acquired pneumonia in adults, 2016 clinical practice guidelines by the Chinese Thoracic Society, Chinese Medical Association. Clin Respir J. 2018;12:1320–1360. doi:10.1111/crj.12674
15. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
16. CLSI. Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria; Approved Guideline.
17. Khan S, Sallum UW, Zheng X, Nau GJ, Hasan T. Rapid optical determination of β-lactamase and antibiotic activity. BMC Microbiol. 2014;14:84. doi:10.1186/1471-2180-14-84
18. Wickham H. ggplot2, Elegant Graphics for Data Analysis. Springer; 2016.
19. Wang Q, Wang X, Wang J, et al. Phenotypic and genotypic characterization of carbapenem-resistant Enterobacteriaceae: data from a longitudinal large-scale CRE Study in China (2012–2016). Clin Infect Dis. 2018;67(suppl_2):S196–S205. doi:10.1093/cid/ciy660
20. Zhao C, Xie Y, Zhang F, et al. Investigation of antibiotic resistance, serotype distribution, and genetic characteristics of 164 invasive Streptococcus pneumoniae from North China Between April 2016 and October 2017. Infect Drug Resist. 2020;13:2117–2128. doi:10.2147/IDR.S256663
21. Zhao C, Li Z, Zhang F, et al. Serotype distribution and antibiotic resistance of Streptococcus pneumoniae isolates from 17 Chinese cities from 2011 to 2016. BMC Infect Dis. 2017;17:804. doi:10.1186/s12879-017-2880-0
22. Blyth CC, Gerber JS. Macrolides in Children with community-acquired pneumonia, panacea or placebo? J Pediatric Infect Dis Soc. 2018;7:71–77. doi:10.1093/jpids/pix083
23. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. Am J Respir Crit Care Med. 2019;200:E45–67. doi:10.1164/rccm.201908-1581ST
24. Li Y, Tomita H, Lv Y, et al. Molecular characterization of erm(B)- and mef(E)-mediated erythromycin-resistant Streptococcus pneumoniae in China and complete DNA sequence of Tn2010. J Appl Microbiol. 2011;110:254–265. doi:10.1111/j.1365-2672.2010.04875.x
25. Tiemei Z, Xiangqun F, Youning L. Resistance phenotypes and genotypes of erythromycin-resistant Streptococcus pneumoniae isolates in Beijing and Shenyang, China. Antimicrob Agents Chemother. 2004;48:4040–4041. doi:10.1128/AAC.48.10.4040-4041.2004
26. Berical AC, Harris D, Dela Cruz CS, Possick JD. Pneumococcal vaccination strategies. an update and perspective. Ann Am Thorac Soc. 2016;13:933–944. doi:10.1513/AnnalsATS.201511-778FR
27. Zheng Y, Rodewald L, Yang J, et al. The landscape of vaccines in China, history, classification, supply, and price. BMC Infect Dis. 2018;18:502. doi:10.1186/s12879-018-3422-0
28. Zhang T, Zhang J, Shao X, et al. Effectiveness of 13-valent pneumococcal conjugate vaccine against community acquired pneumonia among children in China, an observational cohort study. Vaccine. 2021;39:4620–4627. doi:10.1016/j.vaccine.2021.06.075
29. García-Cobos S, Arroyo M, Pérez-Vázquez M, et al. Isolates of β-lactamase-negative ampicillin-resistant Haemophilus influenzae causing invasive infections in Spain remain susceptible to cefotaxime and imipenem. J Antimicrob Chemother. 2014;69:111–116. doi:10.1093/jac/dkt324
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Hospital-Based and Cross-Sectional Investigation on Clinical Characteristics of Pediatric Streptococcus pneumoniae Isolates in Beijing from 2015 to 2021
Lyu Z, Li J, Zhen J, Shi W, Meng Q, Zhou W, An J, Yao K, Dong F
Infection and Drug Resistance 2023, 16:499-508
Published Date: 26 January 2023
Antibacterial Activity of Thesium chinense Turcz Extract Against Bacteria Associated with Upper Respiratory Tract Infections

Wei J, Zhang C, Ma W, Ma J, Liu Z, Ren F, Li N
Infection and Drug Resistance 2023, 16:5091-5105
Published Date: 8 August 2023