Back to Journals » Infection and Drug Resistance » Volume 19
Antimicrobial Resistance in Somalia: Surveillance Gaps, Stewardship Barriers, and One Health Priorities
Authors Jimale AM ![]() , Ali MA, Osman NH
, Ali MA, Osman NH ![]() , Moallim AA, Mohamud AA, Ahmed ID, Abdi AM
, Moallim AA, Mohamud AA, Ahmed ID, Abdi AM ![]() , Adam AA
, Adam AA ![]() , Mohamud OM
, Mohamud OM ![]()
Received 28 March 2026
Accepted for publication 24 June 2026
Published 26 June 2026 Volume 2026:19 612836
DOI https://doi.org/10.2147/IDR.S612836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Abdirahman Mohamed Jimale,1,2 Mohamed Ahmed Ali,1 Nor Haji Osman,1 Aweis Ahmed Moallim,1 Abdirahman Ahmed Mohamud,1 Ismail Dahir Ahmed,1 Abdiweli Mohamed Abdi,3 Abdikarim Abdi Adam,4 Osman Mohamed Mohamud5
1Directorate of Health and Human Services, Research Section, Banaadir Regional Administration, Mogadishu, Somalia; 2Faculty of Health Science, University of Somalia (UNISO), Mogadishu, Somalia; 3Faculty of Health Science, Al Hayat Medical University, Mogadishu, Somalia; 4Department of Environmental health and Climate, IPC Section, Federal Ministry of Health, Mogadishu, Somalia; 5Faculty of Medicine and Health Sciences, Zamzam University of Science and Technology, Mogadishu, Somalia
Correspondence: Abdirahman Mohamed Jimale, Faculty of Health Science, University of Somalia (UNISO), Mogadishu, Somalia, Tel +252615654902, Email [email protected]
Abstract: This narrative review examines antimicrobial resistance (AMR) in Somalia, with emphasis on surveillance gaps, stewardship barriers, and One Health priorities. Peer-reviewed and selected grey literature published between 2010 and March 2026 was reviewed using major bibliographic databases and relevant policy sources. The available Somalia-specific evidence remains limited, heterogeneous, and concentrated mainly in facility-based studies from urban settings, particularly Mogadishu. Existing findings indicate concerning resistance patterns among major bacterial pathogens, while national surveillance systems, laboratory capacity, quality assurance, antimicrobial stewardship structures, and regulatory oversight remain underdeveloped. Evidence from animal health, food systems, and environmental sectors is also sparse, limiting operational implementation of a One Health response. Strengthening AMR control in Somalia requires phased investment in sentinel surveillance, microbiology and antimicrobial susceptibility testing, antimicrobial stewardship, pharmaceutical regulation, infection prevention and control, water, sanitation and hygiene, and multisectoral coordination. Addressing AMR in Somalia will depend on both AMR-specific interventions and broader health-system strengthening.
Keywords: antimicrobial resistance, Somalia, surveillance, antimicrobial stewardship, one health, fragile health systems, laboratory capacity
Introduction
Antimicrobial resistance (AMR) has emerged as a major threat to global health, undermining the effective treatment of common bacterial infections and jeopardizing gains in modern medicine. The most comprehensive global analysis to date estimated that bacterial AMR was associated with 4.95 million deaths in 2019, including 1.27 million deaths directly attributable to resistance, with the highest burdens concentrated in low-resource settings.1 More recent global modelling has shown that AMR remains a substantial cause of mortality worldwide and continues to reflect profound inequalities in health-system capacity, access to effective antimicrobials, infection prevention, and diagnostic services.2
Conflict, displacement, damaged infrastructure, environmental contamination, weak governance, interrupted medicine supply chains, and reduced access to microbiology services all create conditions that facilitate both the emergence and transmission of resistant organisms while simultaneously weakening the capacity to detect and contain them.3 Humanitarian settings are therefore not peripheral to the AMR agenda; rather, they represent some of the environments in which stewardship, surveillance, infection prevention and control, and laboratory strengthening are most urgently needed, even though these functions are often deprioritized in emergency response.4
In Somalia, decades of conflict, chronic underinvestment, fragmented governance, and dependence on external assistance have contributed to a health system characterized by uneven service delivery, weak regulatory oversight, and limited public health capacity.5,6 Recent analyses describe recurrent outbreaks of cholera, measles, and polio, widespread displacement, patchy surveillance, inadequate water, sanitation and hygiene (WASH) coverage, and severe workforce and infrastructure constraints, all of which complicate infection prevention and rational antimicrobial use.6,7 UNICEF Somalia reports that only about 52% of the population has access to a basic water supply and that open defecation remains common, affecting about 28% of the population; these figures illustrate the wider WASH constraints that can increase infection burden and antimicrobial demand.8 Diagnostic limitations remain particularly important for AMR: although laboratory capacity improved during and after the COVID-19 period, Somalia entered that period with insufficient national diagnostic capability, and bacteriology and susceptibility-testing capacity remain inadequate for routine, nationwide AMR surveillance.9 At the same time, Somali studies and reviews have identified inappropriate antibiotic access and use, including pharmacy- and community-level practices that may promote non-prescription use, empirical treatment, and weak stewardship.10
Despite these vulnerabilities, Somalia remains poorly represented in the AMR evidence base. AMR in Somalia has been described as a silent and under-prioritized public health crisis requiring urgent policy attention, stronger surveillance, and antimicrobial stewardship within a One Health framework.11 Recent studies consistently describe AMR in Somalia as severe but poorly documented, emphasizing that available data are sparse, geographically limited, and insufficient to support robust national estimates or context-specific treatment guidance.12 This evidence gap itself justifies a dedicated review. A Somalia-focused synthesis is needed not because the data are abundant, but because they are fragmented: bringing together the available literature is essential to clarify the current state of knowledge, identify major surveillance and research gaps, and inform realistic policy and programmatic responses in a setting where AMR control must be integrated with broader efforts to strengthen health systems, diagnostics, outbreak response, and medicines regulation.5,12,13 Therefore, this review aims to synthesize the available evidence on AMR in Somalia, identify major surveillance and stewardship gaps, and outline practical priorities for policy and implementation.
Methods
This study was conducted as a narrative review of published and grey literature, together with relevant policy and strategic documents, on antimicrobial resistance (AMR) in Somalia. Searches were performed in PubMed, Scopus, Web of Science, and Google Scholar using combinations of terms related to AMR and the Somali context, including “antimicrobial resistance,” “antibiotic resistance,” “antimicrobial stewardship,” “surveillance,” “laboratory capacity,” “One Health,” “policy,” “Somalia,” and “Somaliland,” with appropriate Boolean operators. Reference lists of relevant publications were also hand-searched to identify additional sources. The 2010-March 2026 period was selected to capture contemporary AMR evidence after the global expansion of AMR policy attention and to include Somalia’s more recent AMR policy and surveillance developments, including national action planning and GLASS enrolment.
Eligible materials included peer-reviewed original articles, review papers, surveillance reports, policy documents, strategic frameworks, and selected grey literature from the World Health Organization, the Federal Government of Somalia, and other relevant national and international agencies. Sources were included if they addressed AMR burden, antimicrobial use, stewardship, surveillance systems, laboratory capacity, regulatory challenges, or One Health issues in Somalia. Both qualitative and quantitative sources were considered when they contributed directly to the review objectives. Sources were excluded if they did not address Somalia or Somaliland, did not relate to AMR, antimicrobial use, laboratory capacity, stewardship, surveillance, policy, or One Health, were duplicate records, or were commentaries without Somalia-specific relevance beyond general background. English-language sources were prioritized because they were the accessible sources identified during the searches. Relevant literature from other fragile and conflict-affected settings was considered only where it provided contextual insight and was not used to estimate the Somali AMR burden. As a narrative review, sources were selected purposively based on relevance to the review objectives, contextual importance, and contribution to understanding AMR in Somalia. No formal meta-analysis or quantitative synthesis was undertaken because the available evidence is limited, heterogeneous, and not methodologically comparable across settings, specimen types, laboratory methods, and populations.
Study quality was considered descriptively rather than through a formal risk-of-bias tool. During synthesis, each source was assessed for relevance to the review question, study setting, population, specimen type, laboratory or data-collection approach, clarity of reporting, and limitations affecting generalizability. These limitations are summarized in the text and in Table 1. This approach was considered appropriate for a narrative review whose purpose was to map fragmented evidence, identify gaps, and generate policy-relevant priorities rather than produce pooled prevalence estimates.
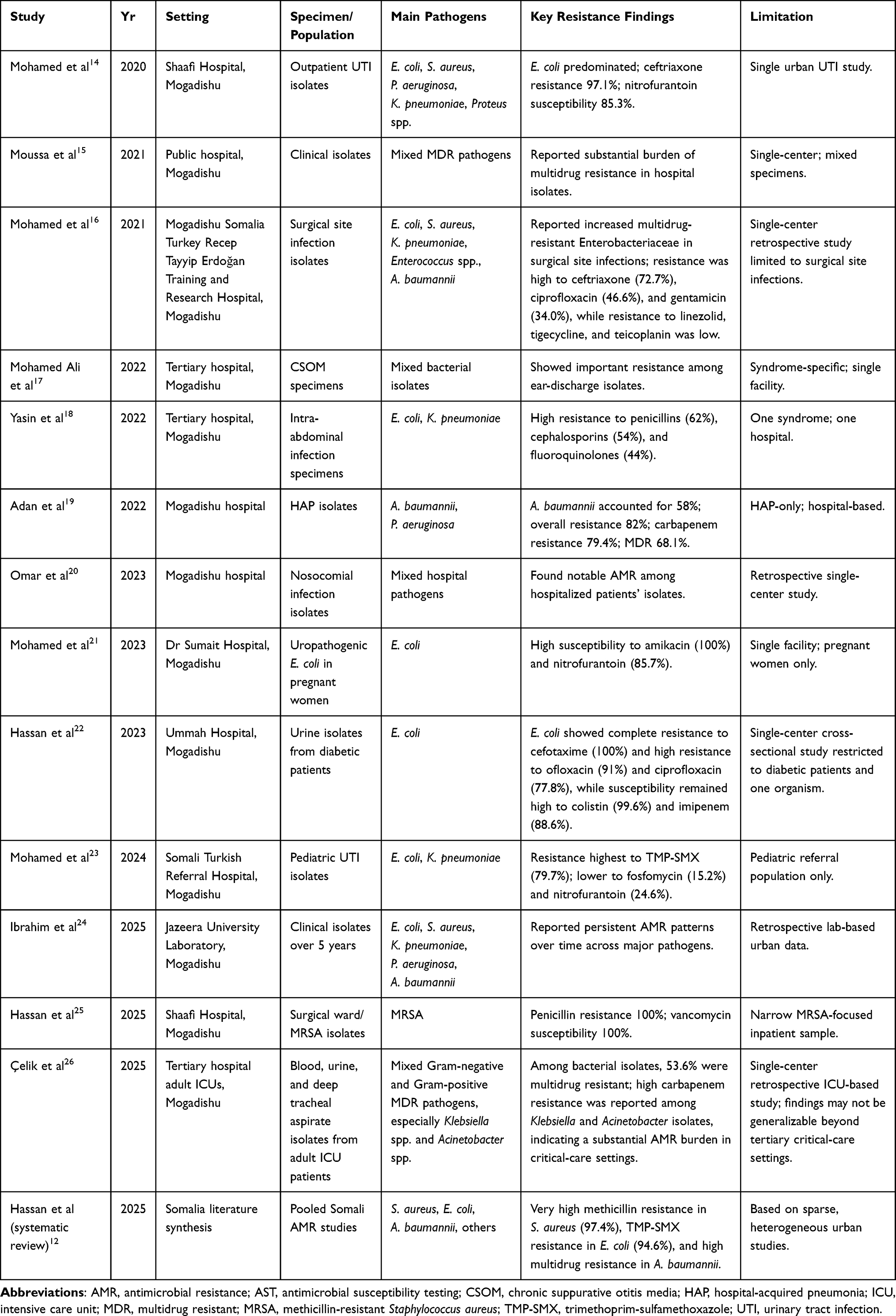 |
Table 1 Summary of Published Antimicrobial Resistance Studies in Somalia |
Country and Health-System Context
Somalia’s health system is best understood through the lens of prolonged fragility. Decades of conflict, political fragmentation, recurrent climatic shocks, and chronic underinvestment have left the country with weak governance, uneven service availability, and limited core public health capacity. Recent analyses describe Somalia as having fragmented health governance, weak surveillance, major workforce shortages, and poor preparedness indicators; one 2025 assessment reported an International Health Regulations compliance score of 31/100 and highlighted fragmented governance and low preparedness across surveillance and laboratory functions.5 Earlier qualitative work on health-system strengthening similarly found that Somalia’s national health system had to be rebuilt after years of institutional decline and disintegration, with stakeholders emphasizing governance, financing, human resources, and engagement with the expanding private sector as central priorities. Together, these studies depict a system in recovery, but one still constrained by chronic instability and limited state capacity.5,27
A defining feature of the Somali health sector is its heavy dependence on external financing and non-state provision. Recent literature notes that Somalia relies heavily on international and private sources for health support because domestic public financing remains limited.28 This financing structure is not merely supplementary; it has shaped how the system operates. A 2026 analysis of post-conflict health governance reported that more than 80% of donor health funding is delivered through UN agencies, international non-governmental organizations, and the Red Cross/Red Crescent, largely outside government financial systems; in 2020, 96.8% of these funds were managed off-budget and off-treasury, with only 3% reaching Somali government entities directly.29 The same study argued that parallel systems for procurement, human resources, and data management weaken national stewardship and limit institutional ownership.29 In practice, this donor-dependent architecture coexists with a highly privatized care landscape. A recent study in presents that federalism and health-system implementation in Somalia describes the current system as privatized and urban-centred, with limited capacity for national authorities to regulate private providers or effectively coordinate service expansion into rural areas.28 This combination of donor dependence and strong private-sector presence complicates continuity of care, standard setting, and nationwide implementation of stewardship or surveillance interventions.28,29
Laboratory and pharmaceutical oversight remain especially weak, with important implications for AMR. Even before COVID-19, Somalia’s national laboratory services had insufficient diagnostic capacity, and the country had to build SARS-CoV-2 molecular testing and sequencing capacity rapidly during the pandemic.9 Although this expansion improved national health security and created useful platforms for epidemic detection, the same study makes clear that the baseline was extremely limited.9 More broadly, Somalia’s public health literature continues to identify weak surveillance and limited laboratory confirmation as major barriers to effective outbreak control.5,7,30 Pharmacy regulation is similarly constrained. Somalia-specific AMR reviews consistently point to weak regulatory oversight, insufficient diagnostic capability, poor infection control practices, and overuse of antimicrobials as central drivers of resistance.6 Evidence from Mogadishu also suggests that irrational antimicrobial use is not confined to informal assumptions: in a survey of 202 doctors at a training and research hospital, physicians identified antibiotic misuse in society, inappropriate prescribing, and the lack of infectious disease specialists as leading contributors to resistance in Somalia.31 Regionally, a 2024 survey covering pharmacists in 19 Arab countries found concerning attitudes and practices around non-prescription antibiotic supply and concluded that regulation and education must be strengthened to address resistance; Somalia was included in that regional analysis.32 Taken together, the literature suggests that laboratory scarcity encourages empiric prescribing, while weak pharmacy oversight and inconsistent stewardship enable unnecessary or inappropriate antibiotic exposure.6,9,31,32
The demand for antimicrobials in Somalia is also shaped by a persistently high burden of infectious disease. Recent reviews describe Somalia’s epidemiological profile as dominated by endemic and epidemic-prone infections, including tuberculosis, malaria, cholera, measles, polio, and a range of zoonoses.7,30,33 A 2025 public health review noted that cholera is concentrated in riverine areas and internally displaced person settlements, while tuberculosis burden is amplified in overcrowded urban settings and areas with malnutrition.30 Another 2025 narrative review linked recurrent outbreaks of cholera, measles, and polio to conflict, drought, flooding, displacement, and the destruction of health infrastructure since the early 1990s.7 Laboratory-based measles data from January to June 2024 showed that 58.4% of 1266 suspected cases tested at the national reference laboratory were confirmed, with 98.3% of cases occurring among unvaccinated individuals.34 Zoonotic disease research further suggests an under-recognized infectious burden: a 2023 scoping review documented 22 zoonotic infections in the Somali literature, but found that only 18 studies had undertaken laboratory analysis within Somalia, underscoring how much of the country’s infection burden remains poorly characterized.33 In such an environment, antimicrobials are likely to be used frequently, often before definitive diagnosis, increasing selective pressure for resistance.6,9,33
Fragility therefore shapes both the emergence of AMR and the capacity to respond to it. The mechanisms are increasingly well described in the broader literature on conflict and AMR: conflict, forced displacement, environmental disruption, damaged infrastructure, and failed governance can increase the spread of resistant organisms while simultaneously weakening stewardship, diagnostics, surveillance, and infection prevention capacity.3 Humanitarian actors have likewise argued that AMR cannot be treated as separate from crisis response, because the settings with the greatest barriers to diagnostics and infection prevention are often those where resistant infections are hardest to detect and treat.4,35 Somalia exemplifies this problem. Its fragmented governance, donor-dependent financing, large private sector, limited capture of private-sector data, weak laboratory systems, and recurrent outbreaks all reduce the state’s ability to monitor antimicrobial consumption, standardize prescribing, detect resistance patterns, or translate AMR policy into operational practice.5,6,28 The result is a setting in which the biological drivers of AMR and the institutional barriers to controlling it reinforce one another. For AMR, the Somali context is therefore not a peripheral backdrop but a central explanatory factor. Health-system fragility increases infection burden, encourages empiric and poorly regulated antimicrobial use, constrains microbiological confirmation, and weakens surveillance and stewardship. Any interpretation of AMR patterns in Somalia must account for these structural realities, because they shape both the emergence of resistance and the limited response capacity available to contain it.3,6,9,35
Current Evidence on AMR in Somalia
The published evidence on AMR in Somalia remains limited, heterogeneous, and concentrated in a small number of facility-based studies. Although the search covered 2010 to March 2026, the Somalia-specific primary AMR studies summarized in Table 1 were published between 2020 and 2026. No relevant Somalia-specific primary antimicrobial susceptibility studies from 2010–2019 were identified among the included sources; earlier materials were used only where they provided contextual or policy background. A 2025 systematic review concluded that AMR in Somalia is severe but poorly documented, with the available literature consisting largely of antimicrobial susceptibility studies from clinical specimens rather than coordinated surveillance datasets.12 The primary studies identified to date have been conducted almost entirely in Mogadishu, especially at Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Shaafi Hospital, Dr Sumait Hospital, Ummah Hospital, and the Jazeera University Laboratory Department. The available work spans several clinical syndromes and specimen types, including outpatient urinary tract infection isolates from Shaafi Hospital,14 multidrug-resistant clinical isolates from a public hospital in Mogadishu,15 chronic suppurative otitis media at a tertiary hospital in Mogadishu,17 surgical site infections caused by multidrug-resistant bacterial pathogens,16 complicated intra-abdominal infections,18 hospital-acquired pneumonia due to non-fermentative Gram-negative bacilli,19 nosocomial infections in hospitalized patients,20 pediatric urinary tract infections,23 uropathogenic Escherichia coli among pregnant women at Dr Sumait Hospital,21 Escherichia coli isolates from diabetic patients at Ummah Hospital in Mogadishu,22 a recent 5-year laboratory retrospective analysis from Jazeera University Laboratory,24 and multidrug-resistant bacterial isolates from adult intensive care units in a tertiary hospital in Mogadishu.26 As shown in Table 1, these studies highlight the key resistance patterns, the main pathogens identified and the limitations of each study.
Across these studies, the most commonly reported bacterial pathogens are Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii.12,14,15,17–21,23,24 In urinary isolates from outpatients at Shaafi Hospital, E. coli was the leading pathogen, followed by S. aureus, P. aeruginosa, K. pneumoniae, and Proteus spp.14 In pediatric urinary tract infections at the Mogadishu Somali Turkish referral hospital, E. coli accounted for 48% of isolates and K. pneumoniae for 16.2%.23 In complicated intra-abdominal infection, E. coli was again the most common organism, followed by K. pneumoniae.18 Hospital-acquired pneumonia data from Mogadishu highlighted non-fermenters, with A. baumannii comprising 58% of isolates and P. aeruginosa 34%.19 Meanwhile, studies of wound or mixed hospital specimens have repeatedly identified S. aureus as a major pathogen.15,20,25
The major resistance patterns reported are concerning and suggest reduced reliability of commonly used empirical antibiotics. The 2025 systematic review found near-universal methicillin resistance in S. aureus based on pooled Somali data, with cefoxitin resistance of 97.4%.12 In the same review, E. coli showed very high resistance to trimethoprim-sulfamethoxazole (94.6%), while A. baumannii was reported to exhibit 100% resistance to multiple drug classes, including carbapenems in some datasets.12 Individual primary studies broadly support this pattern of extensive resistance, although estimates vary by population and specimen type. Among outpatients UTI isolates at Shaafi Hospital, E. coli showed very high resistance to ceftriaxone (97.1%), while retaining relatively better susceptibility to nitrofurantoin (85.3%).14 Among pregnant women at Dr Sumait Hospital, E. coli isolates remained largely susceptible to amikacin (100%), nitrofurantoin (85.7%), amoxicillin-clavulanate, and meropenem.21 Among diabetic patients at Ummah Hospital in Mogadishu, E. coli isolates showed complete resistance to cefotaxime (100%) and high resistance to ofloxacin (91%) and ciprofloxacin (77.8%), while susceptibility remained high to colistin (99.6%) and imipenem (88.6%).22 In adult intensive care units, a later six-year retrospective study reported that 53.6% of bacterial isolates were multidrug resistant, with particularly high carbapenem resistance among Klebsiella and Acinetobacter species, reinforcing concern about severe AMR in critical-care settings.26 In children with UTI in Mogadishu, resistance among uropathogens was high for trimethoprim-sulfamethoxazole (79.7%), with lower resistance reported for fosfomycin (15.2%) and nitrofurantoin (24.6%).23 For complicated intra-abdominal infections, resistance was high to penicillins (62%), cephalosporins (54%), and fluoroquinolones (44%).18 In hospital-acquired pneumonia, A. baumannii showed an overall resistance level of 82%, and 79.4% of non-fermentative Gram-negative bacilli were carbapenem resistant; 68.1% were multidrug resistant.19 Similarly, ICU-based data from Mogadishu documented a substantial burden of multidrug resistance across Gram-negative and Gram-positive pathogens, with over half of all bacterial isolates classified as multidrug resistant.26 In surgical wound infections at Shaafi Hospital, MRSA isolates were 100% resistant to penicillin but remained 100% susceptible to vancomycin.25
Overall, the evidence base is strongest for selected urban hospital settings and weakest for federal member states outside Mogadishu, district hospitals, primary care, community pharmacies, pastoralist populations, and internally displaced persons camps.12,14,15,17–21,23,24 Therefore, the current literature should be interpreted as a signal of important resistance among major pathogens rather than as a nationally representative estimate of AMR prevalence or trends.
The available studies also differ in design, specimen type, patient population, and antibiotic panels, and they are heavily weighted toward cultures obtained in better-resourced urban laboratories.12,14,15,17–21,23,24 Several studies focus on specific syndromes, such as urinary tract infection, chronic ear infection, surgical wound infection, hospital-acquired pneumonia, or intra-abdominal infection, which further limits comparability and generalizability.17–21,23,25 The best-supported conclusion is therefore that the small amount of published evidence already shows substantial resistance among major bacterial pathogens, while large geographic and epidemiologic gaps remain unresolved.12
Surveillance Landscape and Gaps
AMR surveillance in Somalia remains underdeveloped and fragmented. Recent studies have improved understanding of resistance patterns in selected institutions, but the current evidence base still does not constitute a representative national surveillance system.6,12,17,20,22,24
One of the principal barriers to effective surveillance is the limited availability of microbiology services. Existing Somali AMR studies are concentrated in tertiary or referral hospital settings, including work on nosocomial infections, urinary pathogens, otitis media, and other facility-based bacterial isolates.17,20 This pattern strongly suggests that routine bacteriology capacity is restricted to a small number of better-resourced institutions, while much of the country remains outside systematic microbiological testing. In practical terms, this limits confirmation of bacterial infection, reduces opportunities for culture-guided treatment, and constrains the generation of surveillance-quality data.6,12
Antimicrobial susceptibility testing (AST) capacity is similarly weak and uneven. Several Somali studies have reported AST data using standard laboratory methods, but these findings come from isolated facilities rather than from a harmonized national testing network.17,20 Consequently, AST in Somalia is better described as episodic and institution-specific than as part of a coordinated surveillance architecture. Without broader and standardized AST capacity, it is difficult to produce comparable antibiograms across facilities, monitor emerging resistance trends consistently, or use local data to guide empiric treatment policies.6,12
Effective AMR surveillance requires much more than laboratory testing alone; it also depends on standardized isolate-level recording, denominator data, case classification, data aggregation, and timely national reporting. The Somali literature repeatedly characterizes AMR as a serious but poorly documented problem, reflecting the weakness of the country’s surveillance infrastructure and the scarcity of integrated national datasets.6,12 This interpretation is reinforced by hospital-based retrospective work, which notes that healthcare-associated infection data in Somalia remain limited because of resource shortages, funding constraints, and weak research capacity.20
Quality assurance is another major limitation. Reliable AMR surveillance depends on consistent specimen handling, organism identification, susceptibility testing methods, trained personnel, and external quality assessment. Somalia’s National Action Plan on AMR explicitly recognized these constraints and proposed progressive strengthening of laboratory quality systems, including external quality control and phased development of surveillance sites.13 The same document indicates that early surveillance would rely on sentinel facilities and available hospital data while national capacity expanded, underscoring that quality-assured routine surveillance was not yet fully operational at the time of planning.13
Somalia’s enrolment in the WHO Global Antimicrobial Resistance Surveillance System (GLASS) from October 2020 marked an important policy step toward integration into the global AMR surveillance framework.36 WHO documented that from October 2020 onward Somalia had been enrolled in GLASS, following support for development of the national AMR action plan and promotion of rational medicine use.36 However, enrolment in GLASS should not be interpreted as equivalent to full nationwide operational surveillance. Peer-reviewed reviews published after this milestone still describe the Somali AMR evidence base as sparse, fragmented, and heavily dependent on isolated hospital reports rather than on a mature national surveillance platform.6,12 The gap between formal enrolment and operational nationwide surveillance therefore remains substantial.6,12,36
This gap has important clinical and policy consequences. Without broader microbiology coverage, stronger AST capacity, better laboratory information systems, and credible quality assurance, Somalia cannot yet generate a reliable national picture of priority resistant pathogens across regions and levels of care. The resulting dependence on isolated facility data weakens empiric prescribing guidance, limits benchmarking across hospitals, and reduces the capacity of the health system to respond strategically to AMR.6,12,13,20,31
Antimicrobial Stewardship in Somalia
Antimicrobial stewardship in Somalia is constrained by structural weaknesses across the health system, pharmaceutical market, and public health environment. The available literature suggests that inappropriate antibiotic use is driven not only by prescriber behaviour, but also by over-the-counter access, self-medication, limited diagnostics, weak institutional governance, medicine quality concerns, and insufficient public awareness.6,12,37,38
A major stewardship challenge is the widespread availability of antibiotics outside regulated prescribing pathways. Somalia’s AMR literature has repeatedly linked the resistance problem to weak pharmaceutical regulation and easy access to antibiotics without prescription.6,37 WHO’s country cooperation strategy for Somalia similarly notes substantial irrational medicine use, including antibiotic overprescribing in public facilities and widespread purchase of medicines, including antibiotics, without prescription in the private sector.39 In such an environment, antibiotic use frequently begins before any clinical assessment or diagnostic consideration, undermining stewardship at the community level.6,37,39
A cross-sectional study from Mogadishu demonstrated a high prevalence of self-medication practices, showing that unsupervised medicine use is common in the Somali context.38 Although that study focused on self-medication during the COVID-19 period, its findings align with the broader Somali AMR literature, which identifies community misuse of medicines as an important contributor to irrational antimicrobial consumption.37,38 Self-medication increases the risk of inappropriate drug selection, under-dosing, incomplete treatment courses, and antibiotic use for illnesses that are not bacterial.37,38
Another major obstacle to stewardship is empiric prescribing in the absence of diagnostics. Because microbiology services and AST capacity remain limited, clinicians often have little choice but to prescribe antibiotics empirically, especially in hospital settings and severe infections.6,12 This practice is understandable in a constrained health system, but it weakens stewardship because therapy cannot easily be refined on the basis of culture or susceptibility results. In effect, the weakness of the surveillance and laboratory system feeds directly into antibiotic overuse and inappropriate exposure.6,12
Weak prescribing guidance and limited institutional support also contribute to inappropriate antibiotic use. In a study of doctors in a training and research hospital in Mogadishu, respondents identified misuse of antibiotics in society, unnecessary prescribing by doctors, and the absence of infectious disease specialists in most institutions as leading contributors to resistance in Somalia.31 The same study found that many physicians relied on infectious disease consultation or existing antimicrobial guidance when such support was available, suggesting that rational prescribing is hindered by the absence of strong stewardship infrastructure rather than by lack of concern alone.31
Hospital antimicrobial stewardship structures also appear limited. Current Somali peer-reviewed literature does not describe widespread, institutionalized stewardship programmes with routine audit and feedback, multidisciplinary stewardship committees, antibiotic time-outs, or systematic post-prescription review. Where such structures are absent, practical roles would need to be distributed across stakeholders: hospital leaders would establish stewardship committees and authorize prescribing guidance; clinicians would apply syndrome-specific guidelines and review antibiotic duration; pharmacists would monitor antibiotic consumption and dispensing practices; laboratories would provide culture and AST results to support de-escalation; IPC teams would reduce preventable infection and transmission; and regulators would strengthen prescription-only access and medicine quality oversight.6,12 WHO policy material also frames rational drug use in Somalia as an ongoing area requiring support, which is consistent with the interpretation that stewardship systems remain developmental rather than fully embedded across the health sector.36,39
Medicine quality and regulatory weaknesses further complicate stewardship. Somali AMR analyses have highlighted the risks posed by poor pharmaceutical regulation, weak market oversight, and uncontrolled access to antimicrobials.6,37 Where regulatory control is weak, the circulation of substandard or poor-quality medicines becomes more likely, exposing patients to ineffective therapy and potentially promoting resistance through subtherapeutic drug concentrations. Stewardship in Somalia must therefore be understood not only as a prescribing issue, but also as a pharmaceutical governance issue requiring stronger regulation, procurement oversight, and medicine quality assurance.6,37,39
Clinician and public awareness barriers remain important, even though awareness alone is not the core problem. Physicians in Mogadishu have demonstrated recognition that AMR is a serious concern, yet the persistence of misuse, unnecessary prescribing, self-medication, and limited specialist support indicates a substantial gap between awareness and feasible practice.31,37,38 At public level, antibiotics are still often used in contexts of weak health literacy, fragmented care-seeking, and retail access without adequate counselling.38,39 Thus, the challenge in Somalia is not simply a lack of knowledge, but the inability of current health-system and regulatory arrangements to translate awareness into consistent stewardship behaviour.31,37–39 Overall, antimicrobial stewardship in Somalia remains constrained by a combination of over-the-counter antibiotic access, self-medication, empiric prescribing without diagnostics, weak prescribing guidance, limited hospital stewardship structures, medicine quality and regulatory problems, and persistent awareness barriers. Addressing these gaps will require a systems approach that links laboratory strengthening, national surveillance development, regulatory reform, hospital stewardship mechanisms, and sustained professional and public education.
Concrete national estimates on the proportion of facilities without antimicrobial stewardship programmes or the exact frequency of non-prescription antibiotic sales are not yet available in the reviewed Somali literature. This absence is itself an important surveillance and implementation gap. Future stewardship monitoring should therefore measure facility-level availability of stewardship committees, prescribing guidelines, antibiotic review practices, pharmacy dispensing compliance, antimicrobial consumption, and public self-medication behaviours.
One Health Dimensions of AMR in Somalia
Antimicrobial resistance in Somalia is best viewed through a One Health lens because human health, animal health, food systems, and the environment are closely interconnected. This is particularly relevant in Somalia, where livestock and pastoral livelihoods remain central to household income, food security, and daily life.40 Close and continuous contact between people, animals, and shared environments creates conditions in which resistant organisms, antimicrobial residues, and other health risks can move across sectors rather than remain confined to clinical settings.40
Livestock and pastoral production are therefore directly relevant to AMR. In settings where veterinary oversight is limited and access to animal health services is uneven, antimicrobial use in animals may occur with little regulation.40 Although the Somali evidence base on veterinary antimicrobial use remains limited, available studies have detected antibiotic residues in raw milk and in meat sold in Mogadishu markets, indicating that antimicrobial exposure in food-animal systems is already a measurable concern.41,42 These findings suggest that AMR in Somalia is not only a human health problem, but also a food safety and livestock systems issue.40–42
Food systems and environmental contamination add another important dimension. Poor slaughter hygiene, weak meat inspection, inadequate waste disposal, and unsafe water and sanitation conditions may all facilitate the circulation of resistant organisms between animals, food products, people, and the environment.40,43 WHO documentation from Somalia has also highlighted broader weaknesses in public health functions, including infection prevention and control, waste management, and WASH-related gaps, all of which are relevant to AMR containment.43
A major challenge is the poor integration of human, animal, and environmental sectors. Somalia’s One Health architecture is still evolving, and existing efforts have been described as fragmented and heavily dependent on external support.40 Practical barriers include limited financing, weak routine data-sharing between ministries and sectors, uneven laboratory infrastructure, limited veterinary and environmental testing capacity, weak food-safety inspection systems, and the absence of a fully institutionalized platform for joint AMR planning and reporting.40 As a result, AMR-related issues that cut across sectors, including antimicrobial use in animals, food contamination, zoonotic risk, and environmental exposure, are not yet addressed through a fully coordinated system.40 At the same time, emerging One Health policy opportunities are visible. Recent analyses point to increasing recognition of One Health as a useful framework for addressing complex health threats in Somalia, including AMR.40 Operationalizing this approach would require joint surveillance of human clinical isolates, animal antimicrobial use, residues in meat and milk, food-market contamination, and environmental exposure pathways; shared reporting between human health, livestock, food safety, and environmental authorities; and inclusion of AMR indicators within broader zoonoses, food safety, environmental health, and health security platforms.
Policy Response and Implementation Challenges
Somalia’s main policy response to antimicrobial resistance is its National Action Plan (NAP) on AMR, which provides the country’s formal strategic framework for action.13,44 The plan is aligned with the global AMR agenda and emphasizes awareness, surveillance, infection prevention, rational antimicrobial use, and multisectoral coordination.13 In policy terms, this is an important step because it places AMR within a national One Health framework and establishes a basis for surveillance and stewardship development.13,44
However, implementation remains constrained by major structural weaknesses. Financing is a central barrier, as Somalia’s health system remains heavily dependent on external support and must manage AMR alongside many competing public health priorities.39,40 This limits the country’s ability to sustain investments in laboratory capacity, surveillance systems, stewardship structures, and regulatory enforcement.39
Workforce limitations also remain significant. Effective implementation of the NAP depends on trained laboratory personnel, pharmacists, clinicians, veterinary professionals, and regulatory staff, yet both WHO and peer-reviewed literature indicate important shortages across these areas.6,12,39,40 These gaps weaken surveillance quality, stewardship, and medicine oversight.
Regulatory weakness is another major challenge. Antibiotics are widely accessed without prescription, and both WHO reports and Somali studies link AMR to overuse, self-medication, and weak pharmaceutical control.6,12,39 Without stronger enforcement of prescribing and dispensing rules, the policy goals of rational antimicrobial use will remain difficult to achieve.
Governance and multisectoral coordination are similarly fragile. Although the NAP recognizes the need for collaboration across human, animal, and environmental sectors, implementation of this vision is still limited.39 Somalia’s One Health structures remain at an early stage, and coordination across sectors has yet to become routine or institutionalized.39 This weakens the country’s ability to operationalize a comprehensive AMR response.
Laboratory scale-up remains another major implementation challenge. National AMR policy cannot function effectively without broader microbiology services, stronger antimicrobial susceptibility testing capacity, quality assurance, and reliable data systems.6,12 Yet current Somali AMR evidence still comes mainly from a small number of facility-based studies, highlighting the gap between policy intent and operational capacity.6,12 Overall, Somalia has made important policy progress on AMR, but implementation continues to be limited by financing constraints, workforce shortages, weak regulation, fragile governance, slow laboratory expansion, and insufficient multisectoral coordination.
Practical Recommendations for Somalia
A practical AMR response in Somalia should focus on feasible, phased priorities that address the most immediate system gaps while building a stronger long-term foundation. One priority is to strengthen sentinel surveillance. Given the current limitations in diagnostic infrastructure and national data systems, a sentinel approach remains more realistic than immediate nationwide surveillance and would help generate more consistent evidence for policy and clinical use.
A second priority is to expand laboratory capacity. Wider access to microbiology services, antimicrobial susceptibility testing, specimen referral systems, and quality assurance is essential not only for surveillance, but also for reducing reliance on empiric treatment and supporting better stewardship. Without this expansion, both surveillance and clinical decision-making will remain constrained by limited diagnostic evidence.
Regulation of antibiotic sales should also be strengthened. Over-the-counter access, self-medication, and weak control of medicine distribution continue to undermine rational antimicrobial use in Somalia. More effective enforcement of prescription-only access and stronger oversight of medicine quality and pharmaceutical sales are therefore central to AMR containment.
Hospital stewardship programs should be developed in parallel. Even in resource-limited settings, practical stewardship measures such as prescribing guidance, review of antibiotic use, audit and feedback, and targeted clinician training can improve antibiotic practice. These approaches are especially important where specialist support is limited and empiric prescribing is common.
Infection prevention and control (IPC) and water, sanitation, and hygiene (WASH) also need greater attention. Reducing infection burden lowers antibiotic demand and limits the spread of resistant organisms. In Somalia, improvement in hand hygiene, sanitation, waste management, environmental cleaning, and basic IPC systems would support AMR control while strengthening broader health system resilience. Recent nationwide HHFA-based evidence further supports this priority: an analysis of 1,219 Somali health facilities found substantial IPC readiness gaps, including limited availability of standard precautions policies, healthcare waste-management guidance, staff training, hand-hygiene supplies, and sterilization equipment, with marked regional disparities across states.45
AMR should also be integrated more explicitly into Somalia’s emerging One Health platforms. Because antimicrobial use, resistant organisms, food contamination, and environmental exposure cut across sectors, an effective response cannot remain confined to human health institutions alone. Stronger linkage with livestock, food safety, and environmental systems would make AMR policy more consistent with the Somali risk context.
Finally, Somalia would benefit from stronger local research and routine data use. The current evidence base remains narrow, and more locally generated research is needed on prescribing practices, animal antimicrobial use, residues in food, environmental contamination, and operational stewardship. At the same time, routine facility and subnational data should be used more actively to inform local decision-making rather than serving only as fragmented reports.
Priority data needs include standardized resistance patterns for priority pathogens, antimicrobial consumption and prescribing data, facility-level stewardship capacity, pharmacy dispensing practices, veterinary antimicrobial use, antibiotic residues in food products, and environmental contamination indicators. Priority settings for expanded surveillance include tertiary hospitals, district hospitals, private laboratories and pharmacies, internally displaced persons settlements, livestock markets, slaughter points, and food-production chains. These priorities would help Somalia move from fragmented evidence toward routine data use for clinical guidance, regulation, and One Health action.
Figure 1 presents a conceptual framework linking surveillance gaps, stewardship barriers, and One Health priorities for AMR control in Somalia.
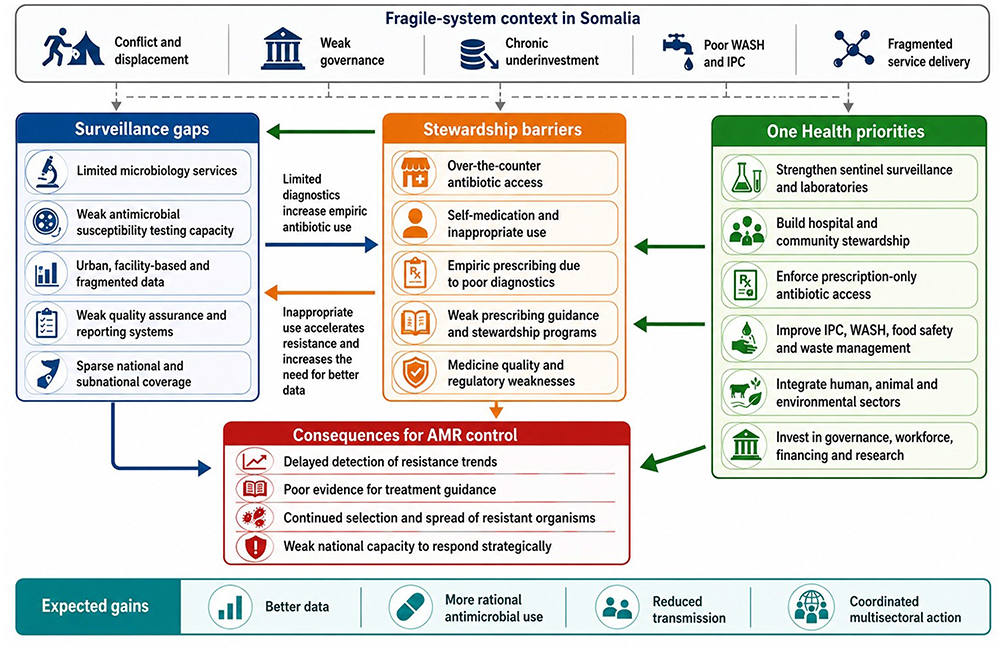 |
Figure 1 Conceptual framework linking surveillance gaps, antimicrobial stewardship barriers, and One Health priorities for antimicrobial resistance control in Somalia. This figure illustrates how Somalia’s fragile health-system context contributes to limited microbiology services, weak antimicrobial susceptibility testing capacity, fragmented surveillance data, over-the-counter antibiotic access, self-medication, empiric prescribing, and weak stewardship structures. It also highlights how One Health priorities, including sentinel surveillance, laboratory strengthening, hospital and community stewardship, prescription-only antibiotic access, IPC, WASH, food safety, environmental management, and multisectoral coordination, can support improved AMR detection, more rational antimicrobial use, reduced transmission, and coordinated national action. |
Limitations
This review should be interpreted in light of several limitations. First, the available literature on antimicrobial resistance in Somalia remains sparse, reflecting the broader underdevelopment of AMR surveillance and research in the country. Second, much of the existing evidence is derived from cross-sectional and single-center studies, often conducted in a limited number of urban or tertiary-care settings, which restricts the generalizability of the findings to the national level. Third, publication bias cannot be excluded, as studies reporting notable resistance patterns or originating from better-resourced institutions may be more likely to reach publication than data from smaller or less visible settings. Fourth, evidence from the animal health and environmental sectors was limited, reducing the ability of this review to assess AMR comprehensively from a fully operational One Health perspective. Fifth, because this was a narrative review, no formal risk-of-bias scoring, meta-analysis, or pooled estimate was undertaken. Finally, the studies included in the Somali AMR literature used inconsistent laboratory methods, antimicrobial susceptibility testing approaches, specimen selection, and reporting practices, which limited direct comparison across reports and made it difficult to draw standardized conclusions regarding the magnitude and trends of resistance.
Conclusion
Antimicrobial resistance in Somalia is a serious but still under-documented public health concern. The most important Somalia-specific takeaway is that available studies already indicate substantial resistance among clinically important pathogens, yet the evidence comes mainly from a small number of urban hospital and laboratory settings and cannot define national AMR prevalence or trends. The most urgent priorities are therefore to expand sentinel surveillance beyond Mogadishu, strengthen microbiology and AST capacity, generate routine antimicrobial use and prescribing data, regulate antibiotic sales, and embed stewardship within hospitals and pharmacies. One Health surveillance should also be prioritized in livestock production, food markets, milk and meat safety, environmental contamination, and settings where human-animal-environment contact is intense, including pastoralist and displacement-affected communities. Progress will depend not only on AMR-specific interventions, but also on broader investment in laboratory systems, pharmaceutical regulation, infection prevention and control, WASH, and multisectoral governance.
Data Sharing Statement
Data sharing is not applicable to this article as no data were created or analyzed in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was obtained for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Murray CJ, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–14. PubMed PMID: 35065702. doi:10.1016/S0140-6736(21)02724-0
2. Naghavi M, Vollset SE, Ikuta KS, et al. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. Lancet. 2024;404(10459):1199–1226. doi:10.1016/S0140-6736(24)01867-1
3. Abbara A, Shortall C, Sullivan R, et al. Unravelling the linkages between conflict and antimicrobial resistance. NPJ Antimicrobials Resist. 2025;3(1). doi:10.1038/s44259-025-00099-y
4. Naim C, Pokorny J, Uyen A, Shortall C, Farra A, Moussally K. The role of humanitarian actors in global governance for AMR. Lancet Glob Health. 2024:e1752–3. PubMed PMID: 39074476. doi:10.1016/S2214-109X(24)00319-X
5. Hussein SA, Osman MM, Hassan YSA, et al. Strengthening Somalia’s health system: pathways to achieving International Health Regulations core capacities at points of entry by 2025. Trop Med Int Health. 2025. doi:10.1186/s41182-025-00836-z
6. Hassan SA, Mohamed Dirie A, Ahmed NR, Omar AI. Update on antimicrobial resistance in Somalia: current status, challenges, opportunities, and future perspectives. Heliyon. 2024. doi:10.1016/j.heliyon.2024.e39434
7. Hussein SA, Osman MM, Hassan MM, et al. Combating infectious disease outbreaks in Somalia’s fragile health system: the impact of climate change-narrative review. Trop Med Int Health. 2025. doi:10.1186/s41182-025-00816-3
8. Water, sanitation and hygiene | UNICEF Somalia. [Cited June 14, 2026]. Available from: https://www.unicef.org/somalia/water-sanitation-and-hygiene.
9. Figuereo S, Mohamed SI, Takele D, et al. Laboratory capacity-building during COVID-19 in Somalia: improving access to essential diagnostics for national health security in a fragile setting. J Epidemiol Glob Health. 2025;15(1). PubMed PMID: 39909951. doi:10.1007/s44197-025-00350-9
10. Mohamed MA, Tahlil AA, Osman MM, et al. Knowledge, attitudes and practices regarding antibiotic use and resistance among pharmacists in the Banadir region of Mogadishu Somalia. 2023. Available from: https://www.researchsquare.com/article/rs-3473448/v1.
11. Jimale AM, Osman NH, Abdi AM, Adam AA, Moallim AA. Antimicrobial resistance in Somalia: a silent public health crisis demanding immediate action. Infect Drug Resist. 2026;19. doi:10.2147/IDR.S592399
12. Hassan SA, Osman MH, Mohamed MA. Prevalence of antimicrobial resistance in Somalia: a systematic review. IJID Regions. 2025. doi:10.1016/j.ijregi.2025.100800
13. Federal Government of Somalia M of HWHO. Somalia National Action Plan on Combating Antimicrobial Resistance. 2022 [Cited March 22, 2026]. Available from: https://cdn.who.int/media/docs/default-source/antimicrobial-resistance/amr-spc-npm/nap-library/somalia-nap-amr.pdf?download=true&sfvrsn=2b101444_3.
14. Mohamed MA, Abdifetah O, Hussein FA, Karie SA. Antibiotic resistance pattern of Escherichia coli isolates from outpatients with urinary tract infections in Somalia. J Infect Dev Ctries. 2020;14(3):284–289. PubMed PMID: 32235089. doi:10.3855/jidc.12189
15. Moussa AA, Abdi AA, Awale MA, Garba B. Occurrence and phenotypic characterization of multidrug-resistant bacterial pathogens isolated from patients in a public hospital in Mogadishu, Somalia. Infect Drug Resist. 2021;14:825–832. doi:10.2147/IDR.S275090
16. Mohamed AH, Mohamud HA, Arslan E. Epidemiological characteristics and predisposing factors for surgical site infections caused by bacterial pathogens exhibiting multidrug-resistant patterns. Antibiotics. 2021;10(6). doi:10.3390/antibiotics10060622
17. Mohamed Ali I, Duman C, Bozdağ İ, et al. Microbiology and drug susceptibility pattern of bacterial isolates from patients with chronic suppurative otitis media at a tertiary care hospital in Somalia. Infect Drug Resist. 2022;15:7733–7739. doi:10.2147/idr.s390886
18. Yasin NA, Ali AM, Ahmed MA, Keleşoğlu Sİ. Epidemiological characteristics, antimicrobial susceptibility profile, and surgical outcome of complicated intra-abdominal infection at a tertiary hospital in Somalia. Int J Gen Med. 2022;15:7427–7434. doi:10.2147/IJGM.S379711
19. Adan FN, Jeele MOO, Omar NMS. Epidemiology of multidrug resistant non-fermentative gram negative bacilli in patients with hospital acquired pneumonia: an alarming report from Somalia. Infect Drug Resist. 2022;15:6297–6305. doi:10.2147/IDR.S387370
20. Omar NMS, Erismis B, Osman MM, Garba B, Hassan MA, Akuku IG. Retrospective evaluation of nosocomial bacterial infections and their antimicrobial resistance patterns among hospitalized patients in Mogadishu, Somalia. Infect Drug Resist. 2023;16:705–720. doi:10.2147/IDR.S398387
21. Mohamed FY, Dahie HA, Mohamoud JH, Adam MH, Dirie HM. Prevalence, antimicrobial susceptibility profile, and associated risk factors of uropathogenic Escherichia coli among pregnant women attending Dr. Sumait Hospital Mogadishu, Somalia. Front Public Health. 2023:11. PubMed PMID: 38328535. doi:10.3389/fpubh.2023.1203913
22. Hassan SA, Ahmed YMA, Hassan GD. Antimicrobial susceptibility of Escherichia coli isolated from diabetic patients in Mogadishu, Somalia. Front Microbiol. 2023;14. doi:10.3389/fmicb.2023.1204052
23. Mohamed AA, Bastug Y, Senol C, Kassim MM, Yusuf AA, Mohamed AH. Antimicrobial resistance pattern and uropathogens distribution in children visiting a referral hospital in Mogadishu. Future Sci OA. 2024;10(1). doi:10.2144/fsoa-2023-0298
24. Ibrahim AM, Mohamed LM, Aweis ADH, et al. A five-year retrospective analysis of antimicrobial resistance patterns in clinical bacterial isolates from the Jazeera University Laboratory in Mogadishu, Somalia. BMC Microbiol. 2025;25(1). PubMed PMID: 41299227. doi:10.1186/s12866-025-04519-x
25. Hassan SA, Mohamed MA, Salad ZA, et al. Prevalence of Methicillin-Resistant Staphylococcus Aureus and Associated Factors From Surgical Ward Inpatients at Shaafi Hospital, Mogadishu, Somalia. IJID Regions. 2025 Sep 1;16. doi:10.1016/j.ijregi.2025.100717
26. Çelik AK, Türkan M, Ali TA, et al. Prevalence and antimicrobial susceptibility of multi drug-resistant bacteria isolates in adult intensive care units: a six-year retrospective study from a tertiary hospital in Mogadishu, Somalia. BMC Infect Dis. 2025. PubMed PMID: 41422141. doi:10.1186/s12879-025-12315-1
27. Warsame A, Handuleh J, Patel P. Prioritization in Somali health system strengthening: a qualitative study. Int Health. 2016;8(3):204–210. PubMed PMID: 26420848. doi:10.1093/inthealth/ihv060
28. Said AS, Kicha DI. Implementing health system and the new federalism in Somalia: challenges and opportunities. Front Public Health. 2024:12. PubMed PMID: 38362207. doi:10.3389/fpubh.2024.1205327
29. Hussein SA, Ali AJA, Osman MM, et al. Prolonged multisectoral aid-driven reliance on health systems and governance post-conflict era in Somalia. Trop Med Int Health. 2026. doi:10.1186/s41182-025-00861-y
30. Abdi YH, Abdi MS, Bashir SG, Ahmed NI, Abdullahi YB. The State of Public Health in Somalia: Top 5 Challenges and Strategies for Improvement. Public Health Challenges. John Wiley and Sons Ltd; 2025; doi:10.1002/puh2.70138
31. Kıratlı K, Aysin M, Ali MA, Ali AM, Zeybek H, Köse Ş. Evaluation of doctors’ knowledge, attitudes, behaviors, awareness and practices on rational antimicrobial stewardship in a training and research hospital in Mogadishu-Somalia. Infect Drug Resist. 2024;17:2759–2771. doi:10.2147/IDR.S463197
32. Hafez H, Rakab MS, Elshehaby A, et al. Pharmacies and use of antibiotics: a cross sectional study in 19 Arab countries. Antimicrob Resist Infect Control. 2024;13(1). PubMed PMID: 39294829. doi:10.1186/s13756-024-01458-6
33. Mumin FI, Fenton A, Osman AY, Mor SM. Zoonoses research in Somalia: a scoping review using a One Health approach. One Health. 2023. doi:10.1016/j.onehlt.2023.100626
34. Siad AS, Yusuf AM, Otorkpa OJ, et al. Epidemiological investigation of measles outbreaks in Somalia: a Retrospective Study. Infect Drug Resist. 2025;18:2589–2595. doi:10.2147/IDR.S507063
35. Garcia-Vello P, Naim C, Langendorf C, et al. Not forgetting the humanitarian contexts in the fight against antimicrobial resistance: operational-driven reflection on knowledge and research gaps by Médecins Sans Frontières. PLOS Global Public Health. 2025. doi:10.1371/journal.pgph.0005498
36. WHO EMRO - our work in pictures during 2020. [Cited Mar 23, 2026]. Available from: https://who-j40.corephp.org/somalia/information-resources/our-work-in-pictures-during-2020.html.
37. Ayan Aden MOUSSA, Bashiru GARBA. How misuse of antimicrobial agents is exacerbating the challenges facing Somalia’s Public Health. Afr J Lab Med. 2022;(2):26–32.
38. Moussa AA, Omar FD, Fiidow OA, Ali FH, Babatunde SM. Self-medication practices against COVID-19 infection and awareness among residents of Mogadishu, Somalia: a cross-sectional analysis. PLoS One. 2023;18. PubMed PMID: 37379300. doi:10.1371/journal.pone.0284854
39. World Health Organization. Country cooperation strategy for WHO and Somalia 2021–2025. Cairo; 2021 [Cited Mar 23, 2026]. Available from: https://applications.emro.who.int/docs/9789290211280-eng.pdf.
40. Hassan-Kadle AA, Osman AM, Ibrahim AM, Mohamed AA, de Oliveira CJB, Vieira RFC. One Health in Somalia: present status, opportunities, and challenges. One Health. 2024;18. doi:10.1016/j.onehlt.2023.100666
41. Mohamed MA, Ali AM, Shair MA, et al. Detection of antibiotic residues in camel and goat meat from markets in Mogadishu city, Somalia. Pan African Med J One Health. 2022;9. doi:10.11604/pamj-oh.2022.9.8.36704
42. Mohamed MA, Elmi AAS, Dubad AB, Hassan YHS, Osman AM, Bitrus AA. Antibiotic residue in raw milk collected from dairy farms and markets in Benadir, Somalia. Pan African Med J One Health. 2020;2. doi:10.11604/pamj-oh.2020.2.19.24814
43. World Health Organization. Rapid build-up of essential public health functions in Somalia: utilizing the COVID-19 response to improve preparedness and readiness for health security threats in complex emergency situation. Cairo; 2023 [Cited March 23, 2026]. Available from: https://www.emro.who.int/images/stories/somalia/documents/strengthening-public-health-systems-case-study-august-1_2023.pdf.
44. World Health Organization. Somalia: national action plan on combating antimicrobial resistance. Geneva; 2022 [Cited March 23, 2026]. Available from: https://cdn.who.int/media/docs/default-source/antimicrobial-resistance/amr-spc-npm/nap-library/somalia-nap-amr.pdf?download=true&sfvrsn=2b101444_3.
45. Adam AA, Mohamed MH, Osman NH. Critical gaps in infection prevention and control in somalia: insights from the 2024 nationwide harmonized health facility assessment data. Infect Drug Resist. 2026;19. doi:10.2147/IDR.S581753
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinicians’ Intention to Submit Microbiological Pathogenic Test Before Antibiotics Use and Its Influencing Factors: New Evidence from the Perspective of Hospital Management
Wang Q, Zhang X, Zheng F, Wang L, Yu T
Infection and Drug Resistance 2022, 15:3013-3023
Published Date: 11 June 2022
Antimicrobial Resistance Rates and Surveillance in Sub-Saharan Africa: Where Are We Now?
Kariuki S, Kering K, Wairimu C, Onsare R, Mbae C
Infection and Drug Resistance 2022, 15:3589-3609
Published Date: 7 July 2022
Investigating Knowledge of Antibiotics, Antimicrobial Resistance and Antimicrobial Stewardship Concepts Among Final Year Undergraduate Pharmacy Students in Northern Nigeria
Abdu-Aguye SN, Barde KG, Yusuf H, Lawal BK, Shehu A, Mohammed E
Integrated Pharmacy Research and Practice 2022, 11:187-195
Published Date: 23 December 2022
Antimicrobial Resistance in Somalia: A Silent Public Health Crisis Demanding Immediate Action
Jimale AM, Osman NH, Abdi AM, Adam AA, Moallim AA
Infection and Drug Resistance 2026, 19:592399
Published Date: 25 February 2026
Antimicrobial Resistance in Somalia: A Growing Public Health Crisis in a Fragile Health System—A Narrative Review of Challenges, Healthcare Gaps, and Policy Recommendations
Hassan WM
Infection and Drug Resistance 2026, 19:624197
Published Date: 10 July 2026