Back to Journals » Drug Design, Development and Therapy » Volume 20
Anlotinib Plus Immune Checkpoint Inhibitors versus Chemotherapy in Elderly Patients with Extensive-Stage Small-Cell Lung Cancer: A Real World, Exploratory Study
Authors Lu BW, Zhao C, Wang DZ, Wang W
Received 28 March 2026
Accepted for publication 8 May 2026
Published 27 May 2026 Volume 2026:20 608659
DOI https://doi.org/10.2147/DDDT.S608659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Bing-Wei Lu,1,* Can Zhao,2,* Da-Zhong Wang,3 Wei Wang4
1Department of general Medicine, Liaoning Cancer Hospital & Institute, Cancer Hospital of China Medical University, Liaoning Cancer Hospital of Dalian University of Technology, Shenyang, Liaoning, People’s Republic of China; 2Department of Cardiothoracic Surgery, General Hospital of Fushun Mining Bureau of Liaoning Health Industry Group, Fushun, Liaoning, People’s Republic of China; 3Department of Pulmonology, Liaoning Cancer Hospital & Institute, Cancer Hospital of China Medical University, Liaoning Cancer Hospital of Dalian University of Technology, Shenyang, Liaoning, People’s Republic of China; 4Department of Thoracic surgery, Liaoning Cancer Hospital & Institute, Cancer Hospital of China Medical University, Liaoning Cancer Hospital of Dalian University of Technology, Shenyang, Liaoning, People’s Republic of China
*With equal contribution to the work
Correspondence: Da-Zhong Wang, Department of pulmonology, Liaoning Cancer Hospital & Institute, Cancer Hospital of China Medical University, Liaoning Cancer Hospital of Dalian University of Technology, Shenyang, Liaoning, People’s Republic of China, Tel +86 13555864808, Email [email protected] Wei Wang, Department of thoracic surgery, Liaoning Cancer Hospital & Institute, Cancer Hospital of China Medical University, Liaoning Cancer Hospital of Dalian University of Technology, Shenyang, Liaoning, People’s Republic of China, Tel +86 13940272712, Email [email protected]
Objective: This retrospective study aimed to compare the real-world effectiveness and safety of anlotinib plus immune checkpoint inhibitors (ICIs) combination therapy versus chemotherapy in elderly patients with extensive-stage small-cell lung cancer (ES-SCLC).
Methods: A total of 119 elderly patients (age ≥ 65 years) with ES-SCLC were screened and included in this study. Patients who received anlotinib plus ICIs (N = 59) were treated as observation group (OG). Subjects who received single-agent chemotherapy (irinotecan, docetaxel or paclitaxel) (N = 60) were deemed as control group (CG). Overall survival (OS) was the primary endpoint. Secondary endpoints included progression-free survival (PFS), objective response rate (ORR), disease control rate (DCR), Duration of response (DoR) and tolerability. Kaplan–Meier methods and Log rank tests were used to analyze OS/PFS/DoR with Cox proportional hazards modeling for multivariate analysis.
Results: Median age was comparable with 71 years in both groups. Anlotinib plus ICIs showed significantly prolonged survival: median OS was 11.9 months (95% CI: 8.93– 14.87) in OG versus 6.7 months (95% CI: 3.41– 9.99) in CG (HR=0.53, 95% CI: 0.35– 0.81, P=0.003). Median PFS was 5.5 months (95% CI: 4.43– 6.57) in OG and 3.1 months (95% CI: 2.82– 3.38) in CG (HR=0.56, 95% CI: 0.38– 0.83, P=0.003). ORR was higher in OG (33.9% vs 15.0%, P=0.016), as was DCR (79.7% vs 55.0%, P=0.004). Treatment-related adverse events (TRAEs) of grade ≥ 3 was 42.4% in anlotinib plus ICIs and 55.0% in chemotherapy group, and this difference was not statistically significant (P=0.168). The most common TRAEs in OG were fatigue (54.2%), hypertension (45.8%), nausea/vomiting (39.0%) and hand–foot syndrome (27.1%). The frequent TRAEs in CG included myelosuppression (55.0%), nausea/vomiting (48.3%), Fatigue (41.7%) and AST/ALT elevation (33.3%).
Conclusion: Anlotinib combined with ICIs demonstrated improved OS compared to single-agent chemotherapy with acceptable safety profile in elderly patients with ES-SCLC. These real-world findings were hypothesis-generating and required confirmation in prospective trials.
Keywords: elderly, extensive-stage small-cell lung cancer, anlotinib, immune checkpoint inhibitors, chemotherapy, effectiveness, safety
Introduction
Small-cell lung cancer (SCLC) is a highly aggressive malignancy that accounts for approximately 15% of all lung cancers.1 The vast majority of SCLC patients present with extensive-stage disease (ES-SCLC) at diagnosis (70%) due to rapid progression and early metastasis.2 ES-SCLC carries a dismal prognosis with historical 5-year survival rates under 5%.3 For decades, the standard first-line therapy for ES-SCLC has been platinum-based combination chemotherapy (typically cisplatin or carboplatin plus etoposide), which yields high initial response rates (60–65%) but only a short survival benefit.3 Relapse is almost universal and often rapid, reflecting the emergence of chemo-resistant tumor clones.4
Managing ES-SCLC is especially challenging in elderly patients, in whom limited physiologic reserve can constrain tolerable treatment options.5 Lung cancer predominantly affects older adults, and approximately 67% of SCLC patients are considered elderly.6 In these patients, coexistent comorbidities and age-related decline in organ function often limit the use of aggressive therapies.7 In the present study, age ≥65 years was selected as the elderly threshold because this cutoff was widely used in geriatric oncology research and clinical guidance, while recognizing that chronological age alone did not define physiologic fitness.8 Clinical trials in SCLC have historically imposed strict upper age limits or fitness criteria (usually <75 years), resulting in underrepresentation of patients ≥65–70 years.9 For example, the pivotal trials of new agents in SCLC enrolled relatively younger patients (median ages in the 50s–60s). As a consequence, evidence guiding optimal therapy in the elderly population is scarce, and clinicians must extrapolate from younger cohorts.10 Real-world patterns show that many very elderly SCLC patients receive no specific anticancer therapy due to frailty, leading to a median survival of only 1–3 months if untreated.11 Even among octogenarians who do receive chemotherapy, outcomes are poor (median survival of approximately 7 months), highlighting the need for more effective yet tolerable treatments for elderly patients.12
Recent therapeutic innovations in SCLC have introduced immune checkpoint inhibitors (ICIs) into first-line treatment. In 2019, the IMpower133 trial demonstrated that adding the anti–PD-L1 antibody atezolizumab to first-line platinum–etoposide significantly prolonged overall survival (OS) (median: 12.3 vs 10.3 months, HR=0.70) and increased 1-year survival from 38% to 51%.13 This established chemo-immunotherapy followed by maintenance immunotherapy as a new standard of care for ES-SCLC. Similarly, the CASPIAN trial showed improved outcomes with durvalumab (another PD-L1 inhibitor) plus platinum–etoposide.14 However, these advances, while important, have yielded only incremental survival gains of 2–3 months, and most patients still relapse within 6 months of first-line therapy.15 Moreover, the benefit of immunotherapy in the elderly remains uncertain, as elderly patients are underrepresented in trials (in one analysis, only 40% of patients in key immunotherapy trials were ≥65). There is concern that frail older individuals may not tolerate combination chemo-immunotherapy, leading some to receive attenuated regimens or immunotherapy alone in real-world practice.16
The later-line setting is further complicated by platinum sensitivity. Platinum-sensitive relapse, commonly defines as relapse ≥90 days after completion of platinum-based therapy, tends to be associated with better subsequent outcomes than platinum-resistant relapse. Nevertheless, both platinum-sensitive and platinum-resistant diseases have limited durable treatment options, especially in elderly patients.17 Although lurbinectedin and other newer agents have expanded the therapeutic landscape in some regions, access and elderly-specific evidence remain limited, and the optimal later-line strategy after platinum-based therapy and immunotherapy has not been established.18
Incorporating antiangiogenic therapy is a promising strategy. SCLC is highly vascular with VEGF expression reported in a large proportion of tumors (up to 80% in some series), and higher VEGF levels have been associated with poorer prognosis.19 This provides a rationale for targeting angiogenesis in SCLC. Early trials of antiangiogenic agents produced mixed results. The VEGF antibody bevacizumab modestly improved progression-free survival (PFS) when added to frontline chemotherapy in ES-SCLC, other randomized programs (including maintenance/continuation strategies) similarly failed to show a consistent survival advantage.20 Multiple tyrosine kinase inhibitors (TKIs) against VEGF receptors (vandetanib, sunitinib, sorafenib, pazopanib, apatinib, etc.) were tested in second-line settings, but most failed to show significant clinical benefit. One notable exception was anlotinib, a novel oral TKI targeting VEGFR-1–3, FGFR-1–4, PDGFR-α/β, c-Kit and RET. In the randomized Phase II ALTER 1202 trial, anlotinib as third-line therapy for relapsed SCLC significantly improved median PFS (4.1 vs 0.7 months for placebo) and OS (7.3 vs 4.9 months).21 These positive results led the China National Medical Products Administration (formerly CFDA) to approve anlotinib in 2019 as the standard of care for third-line treatment of SCLC. Subsequent studies confirmed that anlotinib monotherapy exhibited meaningful activity in refractory SCLC, including in elderly patients: for instance, anlotinib achieved an objective response rate (ORR) of 9% and median OS of 7 months in elderly (≥60) ES-SCLC patients who had failed ≥2 prior therapies.10 Although the ORR with single-agent anlotinib is modest, disease control rate (DCR) is seen in approximately 60–70% of patients.22 Combining antiangiogenic agents with ICIs is an attractive approach that may synergistically enhance anti-tumor efficacy. Mechanistically, VEGF/VEGFR signaling contributes not only to tumor angiogenesis but also to immune suppression within the tumor microenvironment. VEGF may impair immune-cell trafficking, limit T-cell infiltration, and promote suppressive immune-cell populations. Antiangiogenic therapy may partially normalize abnormal tumor vasculature, reduce hypoxia and facilitate immune-cell infiltration into tumor tissue. Therefore, anlotinib may provide a rational partner for PD-1/PD-L1 blockade by promoting vascular normalization, facilitating CD8+ T-cell infiltration and reshaping the tumor immune microenvironment toward a more immune-active state.23 Clinical experience in other cancers (eg. non-small cell lung cancer and hepatocellular carcinoma) demonstrated that combining anti-VEGF therapies with ICIs yielded superior outcomes compared to either alone, presumably via these complementary mechanisms of action. In SCLC, retrospective studies have begun to explore this strategy. For example, a recent real-world analysis reported that adding anlotinib to immunotherapy in relapsed SCLC achieved an ORR of 32% and prolonged median OS to 13.2 months, far exceeding historical results of single-agent immunotherapy or TKIs.1 Furthermore, a maintenance therapy study in ES-SCLC found that anlotinib plus ICIs after first-line chemo-immunotherapy led to promising survival (median OS of 19.5 months) with tolerable toxicity.23 The mechanism by which anlotinib plus ICIs might reshape the tumor microenvironment was summarized in Supplementary Figure S1.
To date, however, there is a lack of published data specifically comparing anlotinib plus immunotherapy versus conventional chemotherapy in the second-line or later-line treatment of SCLC, particularly in elderly patients. In clinical practice, elderly ES-SCLC patients who progress after first-line therapy often have limited options. Many are not candidates for aggressive combination chemotherapy regimens due to age-related toxicity concerns. Although ICI monotherapy remains a treatment consideration in later-line SCLC (and was previously approved as third-line therapy in some settings), ORR are low (10–20%) and durable survival benefit has not been consistently demonstrated in refractory disease.24 Single-agent chemotherapy (such as topotecan, irinotecan or taxanes) remains a common palliative approach in second-line treatment, but its efficacy is quite limited (ORR of 10–20%, median OS of 5–6 months).17 Therefore, new combination strategies are needed to improve outcomes in this setting without unacceptable toxicity. Consequently, we performed a retrospective exploratory study to evaluate the real-world effectiveness and safety of anlotinib combined with ICIs versus single-agent chemotherapy in elderly patients with ES-SCLC in clinical practice.
Methods
Study Design and Screening Criteria
This was a retrospective cohort study, patients with SCLC who were hospitalized in Liaoning Cancer Hospital & Institute from January 2020 to August 2025 were screened retrospectively. The main inclusion criteria were: (1) Histologically or cytologically confirmed SCLC with extensive-stage disease (ES-SCLC); (2) Age ≥65 years according to previous criteria;8 (3) Eastern cooperative oncology group (ECOG) performance status ≤2 score; (4) received at least one cycle of either anlotinib plus ICIs or single-agent chemotherapy as subsequent line treatment for ES-SCLC in clinical practice when previous systemic treatment failure; (5) at least one measurable target lesion per RECIST v1.1; (6) adequate clinical data and follow-up information available. Key exclusion criteria included: (1) Prior treatment with anlotinib or any antiangiogenic TKI (to isolate the effect of anlotinib in this line); (2) Other concurrent cancers apart from SCLC; (3) serious or life-threatening comorbidities that, in the investigator’s judgment, might compromise patient safety, study compliance or the interpretation of study outcomes; (4) concurrent use of other systemic anticancer agents (including chemotherapy, targeted therapy or other immunotherapy) during treatment with anlotinib plus ICIs or chemotherapy monotherapy. However, local therapy was permitted; (5) substantially unavailable baseline characteristics, therapeutic outcomes or follow-up information. Finally, a total of 119 elderly patients met the eligible criteria were included in this study: 59 patients received anlotinib plus ICIs regimens and 60 patients were treated with single-agent chemotherapy, and the study profile was illustrated in Figure 1.
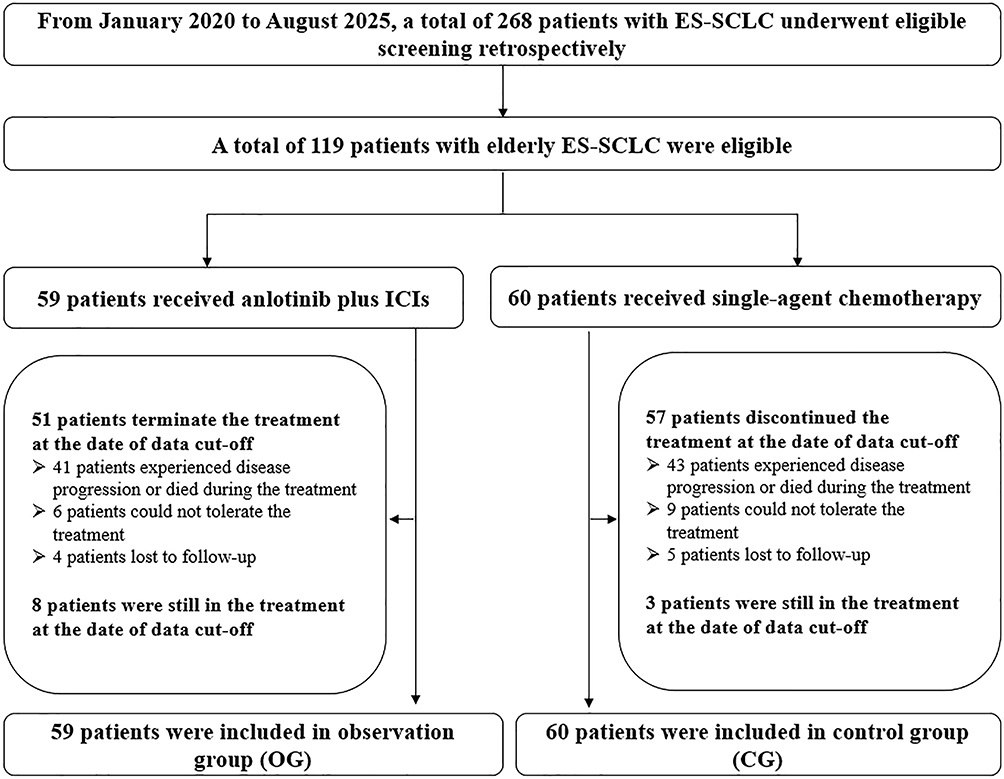 |
Figure 1 Study profile of this retrospective study. |
OS was the primary endpoint, ORR, DCR, duration of response (DoR), PFS and safety profile were secondary endpoints. The study was approved by the institutional ethics committee of Liaoning Cancer Hospital & Institute (approval number: KY20241016), which was conducted in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective design.
Therapeutic Regimens
The decision to administer anlotinib plus ICIs or single-agent chemotherapy in clinical practice was made by treating physicians based on the patient’s performance status, comorbidities, prior therapy and preference. Therefore, potential selection bias was inherent to the retrospective real-world design. Both platinum-sensitive relapse (relapse ≥90 days after first-line therapy) and platinum-resistant relapse (<90 days) were included to reflect real-world diversity. Eligible patients were categorized into two treatment cohorts: the anlotinib plus ICIs group and the single-agent chemotherapy group. The anlotinib+ICIs group was treated as observation group (OG), and received anlotinib in combination with a PD-1 or PD-L1 inhibitor. The single-agent chemotherapy group was deemed as control group (CG), and received a single cytotoxic agent (such as irinotecan, docetaxel, or paclitaxel).
Treatment details were retrieved from medical records, including dosing, schedule and duration. Anlotinib plus ICIs in OG: anlotinib was administered orally at a starting dose of 10–12 mg once daily on days 1–14 of a 21-day cycle (2 weeks on, 1 week off). The initial anlotinib dose was typically 12 mg daily for patients with good performance status and no contraindications; dose reductions to 10 mg or 8 mg were allowed for toxicity, per physician decision, with the lowest effective dose maintained. In combination, the specific ICIs agent was chosen according to availability and physician preference: Tislelizumab (200 mg intravenously every 3 weeks), pembrolizumab (200 mg intravenously every 3 weeks), Serplulimab (a PD-1 inhibitor, 4.5 mg/kg intravenously Q3W) and atezolizumab (PD-L1 inhibitor, 1200 mg intravenously Q3W). All ICIs were continued until disease progression or unacceptable toxicity. Single-agent chemotherapy in CG: the specific agent (irinotecan, docetaxel or paclitaxel) was selected by the treating oncologist based on prior therapy and patient factors. Irinotecan was administered intravenously at 100–125 mg/m2 on days 1 and 8 of a 21-day cycle. Docetaxel was administered intravenously at 60–75mg/m2 on day 1 of a 21-day cycle. Paclitaxel was administered as 175 mg/m2 intravenously on day 1 Q3W, depending on patient tolerance. Growth factor support (G-CSF) was provided per guidelines if neutropenia risk was high, particularly for patients receiving taxanes. Chemotherapy was continued until disease progression or unacceptable toxicity.
All patients in both cohorts received supportive care as needed, including antiemetics, prophylactic antibiotics (for neutropenia), transfusions, or management of symptoms.
Sample Size Calculation
Given the retrospective design, we performed a post hoc sample-size justification based on the primary endpoint of OS in this study using PASS software (version 15.0). Prior evidence indicated that single-agent chemotherapy (irinotecan, docetaxel or paclitaxel) achieved a median OS of approximately 6 months in previously treated ES-SCLC,17,25 which served as the reference value for the control arm assumption. This study assumed that anlotinib plus ICIs regimen might prolong the median OS from 6 months to 11 months. A two-sided Log rank test with an overall sample size of 101 subjects (50 in the OG and 51 in the CG) achieved 80% power at a two-sided α of 0.05 significance level to detect a hazard ratio (HR) of 0.54. The planned study duration was 48 months, including a 36-month retrospective identification (screening) period. Allowing for a 15% attrition rate, the target screening sample size was 59 patients per group. Ultimately, 59 and 60 patients were included in the OG and CG, respectively.
Response Assessment and Data Collection
Treatment responses were typically assessed every 6–8 weeks with imaging (contrast-enhanced CT scans of chest and abdomen plus brain MRI if clinically indicated). Patients who progressed on this study’s treatment could receive further lines of therapy at the physicians’ discretion.
Trained investigators reviewed electronic medical records to extract data on baseline patient characteristics, treatment delivery, tumor response, survival status and adverse events. Baseline variables collected included: age, gender, smoking history, ECOG performance status, comorbid conditions, baseline weight loss and laboratory values, sites of metastases (eg. liver, bone, brain) and prior first-line treatment details (including whether immunotherapy was part of first-line). We also noted the chemotherapy agent used in the single-agent group and the specific ICIs agent in the combination group.
The primary endpoint was OS, defined as the time from initiation of the treatment (anlotinib plus ICIs or single-agent chemotherapy) to death from any cause. Surviving patients were censored at the date of data cut-off. PFS was a secondary endpoint, measured from treatment initiation to the first documented disease progression (radiologic or clinical) or death, whichever occurred first. Patients alive without progression were censored at last disease assessment. ORR was defined as the proportion of patients achieving a complete response (CR) or partial response (PR) as their best response, according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. DCR was defined as the proportion achieving CR, PR or stable disease (SD). DoR was defined as the time from the first documented CR or PR to disease progression or any-cause death. Tumor responses were assessed by the local investigators/radiologists; for consistency, the response assessments documented in the clinical charts or radiology reports were accepted. Where imaging was available, an independent investigator performed a verification of response classification according to RECIST 1.1 criteria. The data cut-off date of this study was January 10, 2026.
Safety profile was evaluated by reviewing recorded treatment-related adverse events (TRAEs), laboratory results, and dose modifications. TRAEs were graded per the National Cancer Institute’s Common Terminology Criteria for Adverse Events (CTCAE), version 5.0. We specifically captured all grade 3 or higher TRAEs, and selected lower-grade AEs of clinical interest (eg. immune-related AEs).
Statistical Analysis
Statistical analyses in this study were performed using SPSS Statistics (Version 25.0) and Stata (Version 14.0). Descriptive statistics to summarize baseline characteristics and treatment exposure were adopted. Continuous variables were reported as median (range) and compared between groups using the Mann–Whitney U-test. Categorical variables were summarized as counts and percentages, and compared using the chi-square test or Fisher’s exact test (if expected counts were <5). The Kaplan–Meier method was employed to estimate survival distributions for OS, PFS and DoR in each treatment group using Stata 14.0 to generate survival curves. The Log rank test was used for univariate comparison of survival curves. Median OS and PFS with two-sided 95% confidence interval (CI) were reported for each cohort. Cox proportional hazards model was constructed to estimate the hazard ratio (HR) and 95% CI for treatment effect (anlotinib plus ICIs vs single-agent chemotherapy) on OS, PFS and DoR, both without adjustment and with multivariable adjustment for covariates. Pre-specified covariates in multivariate analyses included factors that might influence outcomes: age, ECOG performance status (0–1 vs 2), platinum-sensitivity of disease (sensitive vs resistant relapse), presence of liver metastases and whether previous treatment included immunotherapy. Proportional hazards assumptions were tested by examination of log(-log) survival plots. For ORR and DCR, group differences were assessed by chi-square test.
Propensity score matching was not performed because of the modest sample size, the need to retain as many elderly patients as possible, and the comparable distribution of measured baseline factors between the two cohorts. Instead, multivariable Cox models were used to adjust for clinically relevant covariates. Accordingly, the findings were interpreted as exploratory associations rather than definitive causal effects. All statistical tests were two-sided, P<0.05 was considered statistically significant. Given the exploratory nature of the study, P-values were not adjusted for multiple comparisons.
Results
Patient Characteristics
A total of 119 elderly patients with ES-SCLC met the inclusion criteria and were included in the analysis (59 in the OG, 60 in the CG). As shown in Table 1, the median age was 71 years (range: 65–86) in the OG and 71 years (range: 65–88) in the CG (no significant difference, P=0.518). All patients had extensive-stage disease by definition and the distribution of metastases was similar: about 40% had liver metastases. By inclusion criteria, all patients had received at least one lines of systemic chemotherapy. Approximately 34–42% patients had also received an ICIs previously. At the time of initiating study treatment, 22 patients (37.3%) were classified as platinum-sensitive relapse (progression ≥3 months after completing first-line), whereas 37 (62.7%) had platinum-resistant disease (progression within <3 months). The split was similar in CG (35.0% and 65.0%, respectively).
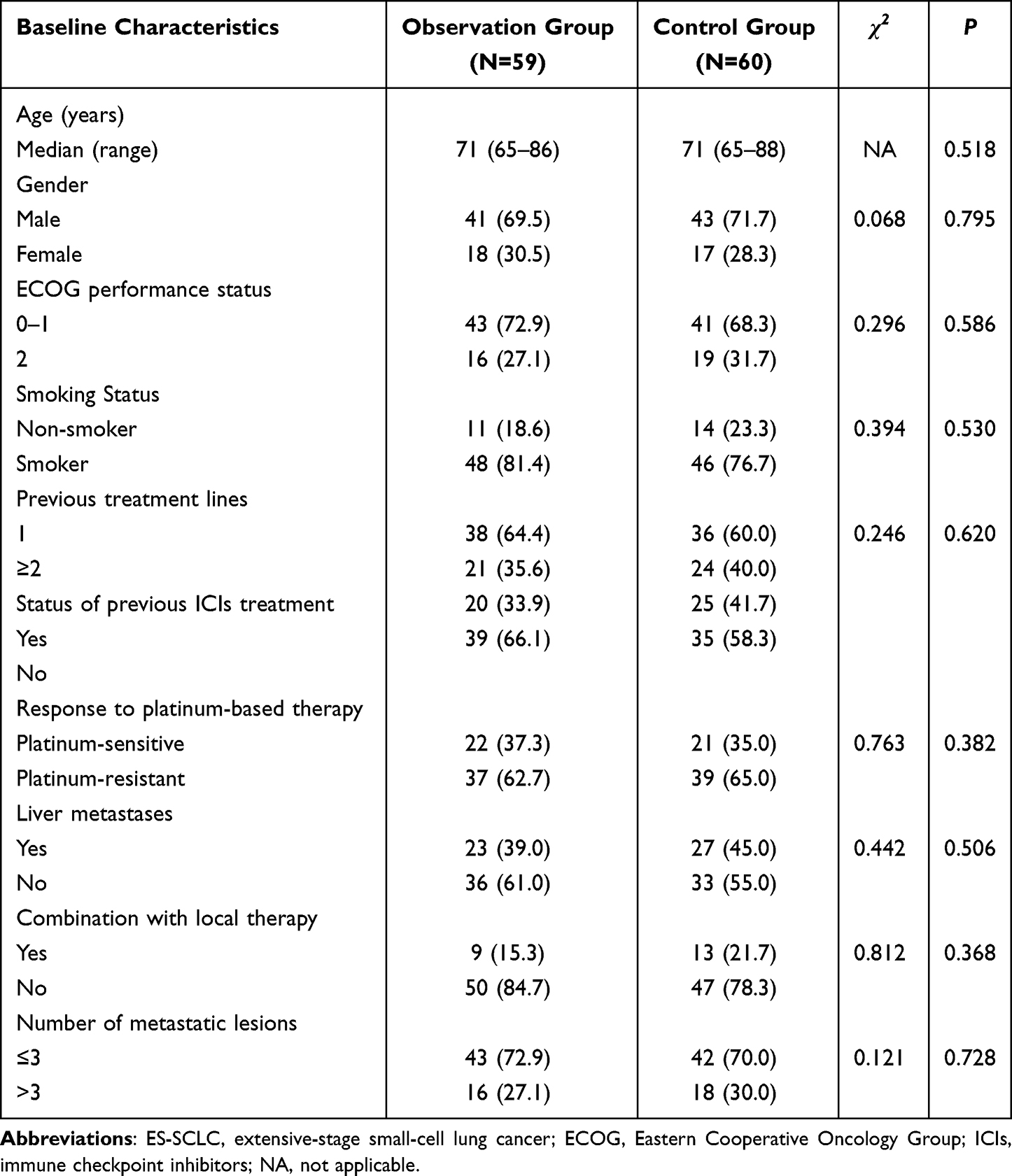 |
Table 1 Comparison of Baseline Clinical Characteristics Between Observation Group and Control Group Among the 119 Elderly Patients with ES-SCLC |
In the single-agent chemotherapy group, the agents used were: paclitaxel in 22 patients (36.7%), docetaxel in 20 patients (33.3%) and irinotecan in 18 patients (30.0%). In the anlotinib plus ICIs group, the breakdown of ICIs agents was: PD-1 inhibitors in 50 patients (84.7%) including Tislelizumab (n=27), pembrolizumab (n=12) and Serplulimab (n=11). And PD-L1 inhibitors in 9 patients (15.3%): atezolizumab (n=9).
Anlotinib was started at 12 mg daily in 45 patients (76.3%) and at a reduced dose of 10 mg in 14 patients (23.7%) (often due to low body weight or physician’s precaution in very elderly). No patient started at 8 mg initially, but dose reductions to 8 mg occurred later in 10 patients.
Therapeutic Exposure and Compliance
Patients in anlotinib plus ICIs group received a median of 6 cycles of therapy corresponding to approximately 4.2 months of treatment. In contrast, the chemotherapy group received a median of 4 cycles of their regimen. At data cutoff, 8 patients (13.6%) in anlotinib plus ICIs arm were still on treatment, whereas only 3 patients (5.0%) in the chemotherapy arm remained on therapy (others had discontinued due to progression or intolerance).
In the OG, anlotinib dose reductions were required in 12 patients (20.3%): 8 patients reduced from 12 mg to 10 mg, and 4 patients from 10 mg to 8 mg, mostly owing to hypertension or hand-foot syndrome after 1–2 cycles. Temporary anlotinib interruptions occurred in 15 patients (25.4%) for management of adverse events, typically for one week beyond the scheduled break clinically. In the CG, 18 patients (30.0%) had ≥1 dose reduction of the chemotherapy agent (eg. docetaxel reduced to 40 mg/m2, or paclitaxel reduced by 20%) due to toxicity such as neutropenia or neuropathy. Approximately 25% of patients in CG required cycle delays of >7 days at least once. These data indicate that while both regimens needed dose adjustments in some elderly patients, overall treatment delivery was feasible, with the combination therapy showing a somewhat longer continuation.
Prognosis Outcomes
At the date of data cut-off (January 10, 2026), the median follow-up duration was 11.3 months (range: 1.1–33.5 months) in OG and 6.5 months (range: 0.7–30.3 months) in CG. A total of 90 deaths events (deaths) were observed: 39 in the anlotinib plus ICIs group (66.1%), 51 in the chemotherapy group (85.0%). The Kaplan–Meier curve for OS was shown in Figure 2, the median OS for patients receiving anlotinib plus ICIs was 11.9 months (95% CI: 8.93–14.87 months), which was significantly longer than the median OS of 6.7 months (95% CI: 3.41–9.99 months) for those receiving single-agent chemotherapy. And the 24-month OS rate was 34.7% (95% CI: 22.5–47.3%) and 15.5% (95% CI: 7.2–26.7%), respectively. The difference in OS between the two groups was statistically significant by Log rank test (χ2=9.078, P=0.003). The HR for OS with anlotinib plus ICIs versus chemotherapy was 0.53 (95% CI: 0.35–0.81).
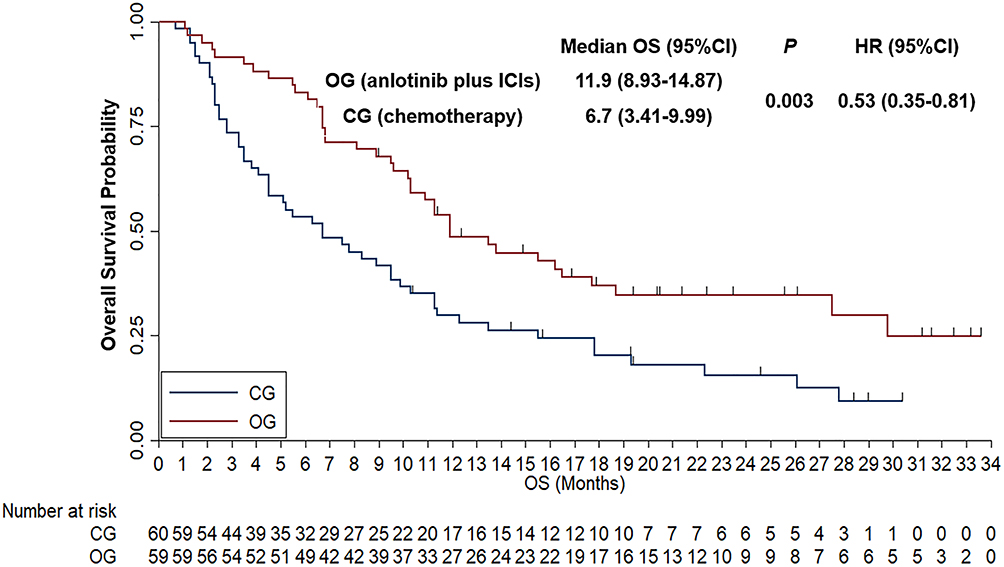 |
Figure 2 Comparison of Kaplan-Meier Overall survival curve between anlotinib plus ICIs regimens and single-agent chemotherapy. |
With regard to the PFS analysis. Most patients experienced progression or death at the time of data cut-off. In the anlotinib plus ICIs group, 49 progression or death events (83.1%) were observed, whereas in the chemotherapy group, 55 progression or death events (91.7%) were detected. As illustrated in Figure 3, the median PFS was 5.5 months (95% CI: 4.43–6.57 months) with anlotinib plus ICIs and 3.1 months (95% CI: 2.82–3.38 months) with single-agent chemotherapy. And the 12-month PFS rate was 25.4% (95% CI: 15.2–37.0%) and 13.1% (95% CI: 6.0–23.0%), respectively. This difference was statistically significant (χ2=8.896, P=0.003). HR of PFS was 0.56 (95% CI: 0.38–0.83) favoring OG.
 |
Figure 3 Comparison of Kaplan-Meier Progression-free survival curve between anlotinib plus ICIs regimens and single-agent chemotherapy. |
Additionally, a multivariate Cox regression analysis for OS was constructed to identify the independent significance in the context of another prognostic factors: ECOG performance status, age, previous treatment lines, status of previous ICIs treatment, response to platinum-based therapy, liver metastases and number of metastatic lesions. As exhibited in Table 2, after multivariate adjustment, therapeutic regimen (OG vs CG) was still independent factor influencing OS (adjusted HR=0.58, 95% CI: 0.41–0.89, P=0.011). Other covariates with significant impact on OS in multivariate analysis were ECOG performance status (HR=0.52, P=0.009), response to platinum-based therapy (HR=0.64, P=0.021), liver metastases (HR=1.38, P=0.025) and number of metastatic lesions (HR=0.61, P=0.015). Importantly, there was no significant influence of age for OS (>71 vs ≤71, P=0.218).
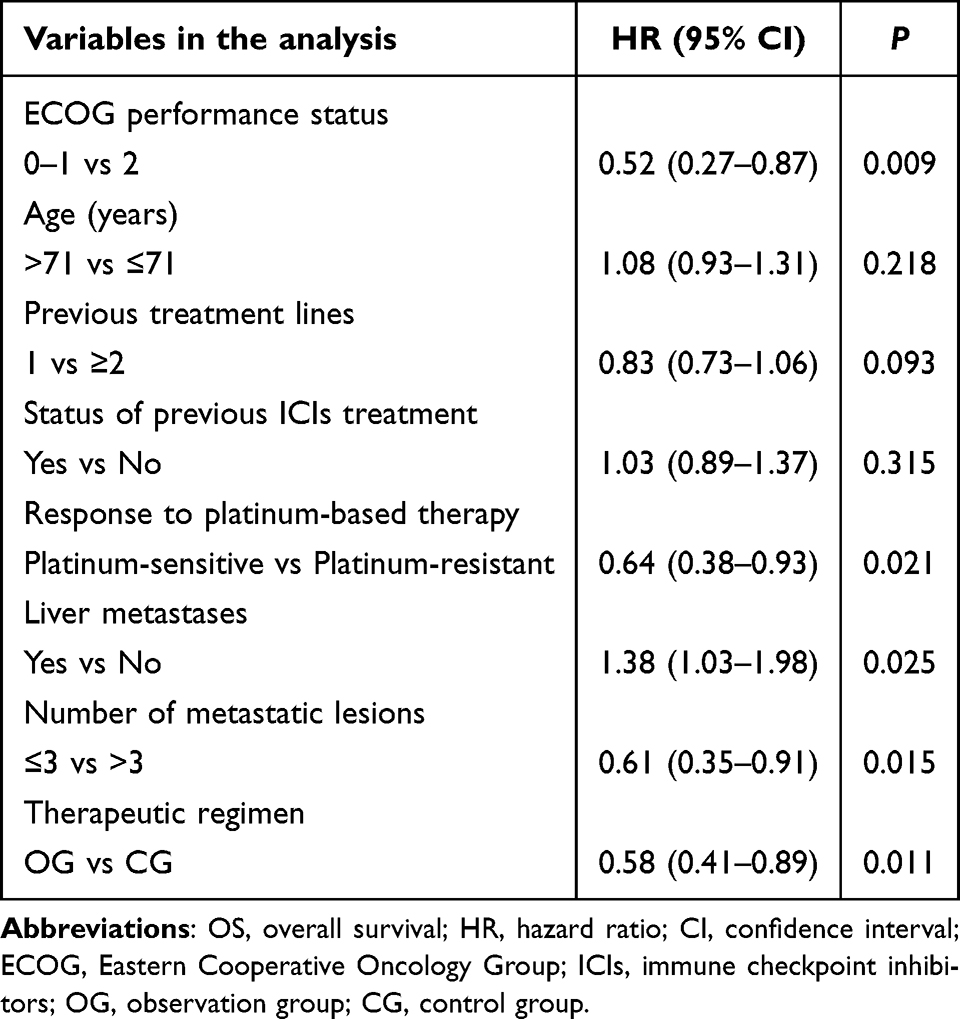 |
Table 2 Multivariate Cox Regression Adjustment for OS Analysis |
Tumor Response
Therapeutic response outcomes were summarized in Table 3. No CR were observed, 20 PR was detected, 27 SD was noted, 7 PD was found and 5 patients were not available in OG. 9 PR was observed, 24 SD was reported, 21 PD was detected and 6 patients were not available in CG. Therefore, ORR was 33.9% (95% CI: 22.1–47.4%) for anlotinib plus ICIs and 15.0% (95% CI: 7.1–26.6%) for single-agent chemotherapy, respectively, which showed a statistically significant difference (P=0.016). And DCR was 79.7% (95% CI: 67.2–89.0%) for anlotinib plus ICIs and 55.0% (95% CI: 41.6–67.9%) for single-agent chemotherapy (P=0.004). Specifically, the best percentage change in target lesion from baseline of the two groups was illustrated in Figure 4, each bar represented an individual patient. The waterfall plot illustrated that 54 patients in OG demonstrated a more dramatical reduction of target lesions compared with 54 patients in CG (mean: −18.1% vs 9.7%).
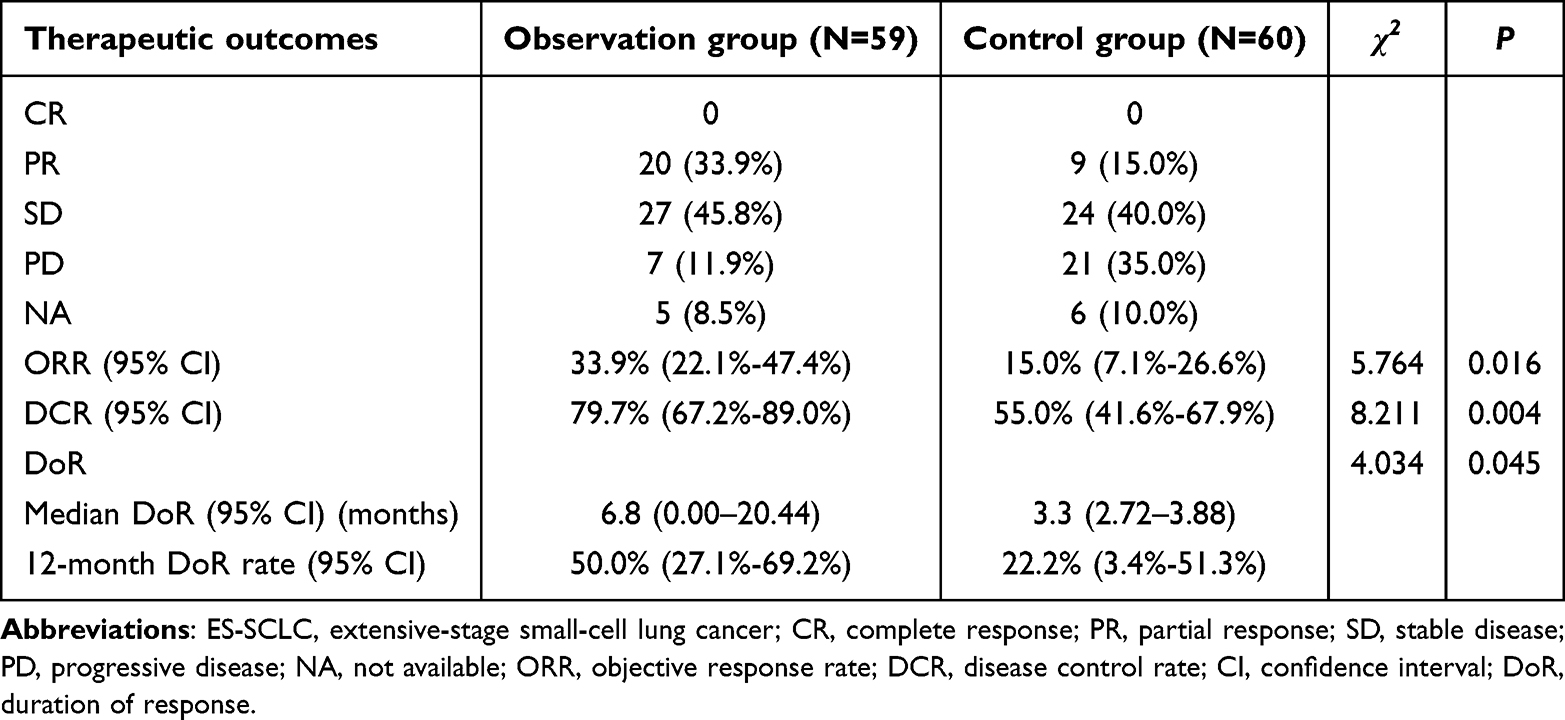 |
Table 3 Comparison of Therapeutic Outcomes Between Observation Group and Control Group Among the 119 Elderly Patients with ES-SCLC |
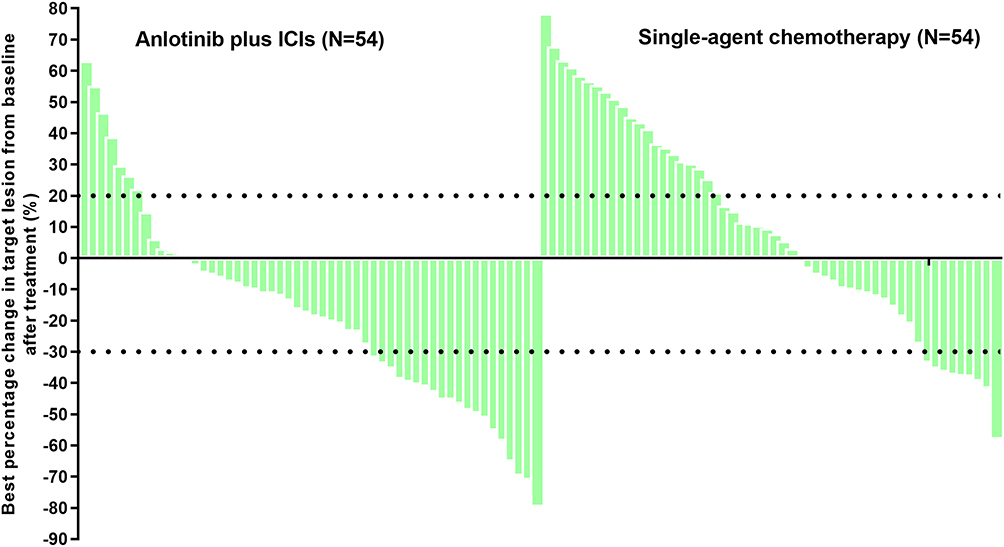 |
Figure 4 Waterfall plot of the best percentage in target lesion from baseline after treatment of anlotinib plus ICIs regimens and single-agent chemotherapy. |
Additionally, DoR was also evaluated in this study among patients who achieved CR or PR. As exhibited in Figure 5, the median DoR of the 20 responders in OG and 9 responders in CG was 6.8 months (95% CI: 0.00–20.44 months) and 3.3 months (95% CI: 2.72–3.88 months), respectively. And the 12-month DoR rate in OG and CG was 50.0% (95% CI: 27.1–69.2%) and 22.2% (95% CI: 3.4–51.3%), which showed a trend toward marginal statistical significance (χ2=4.034, P=0.045).
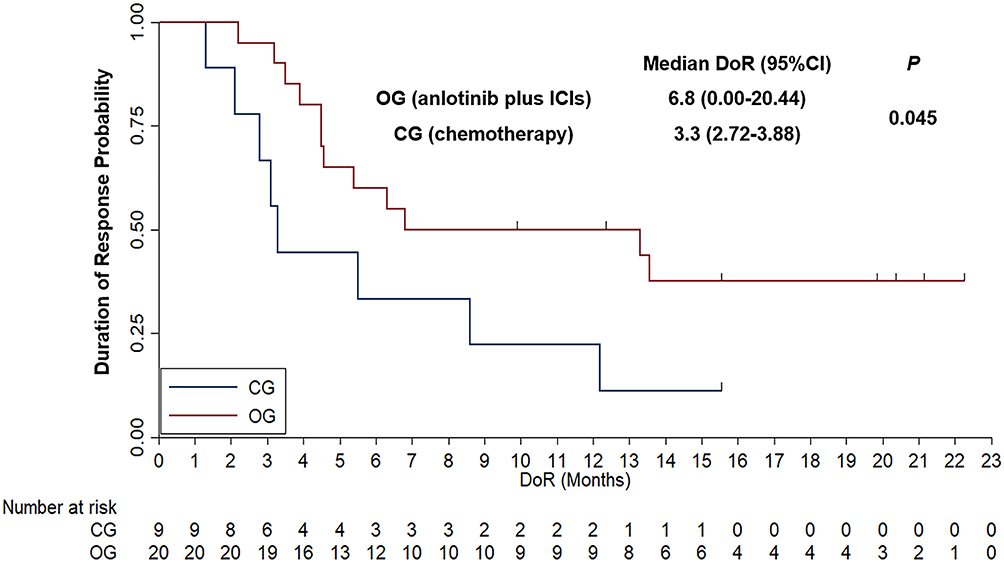 |
Figure 5 Comparison of Kaplan-Meier Duration of response survival curve between anlotinib plus ICIs regimens and single-agent chemotherapy among responders. |
Tolerability
All patients were evaluable for safety profile. Overall, both treatment approaches were tolerable in this elderly cohort, but they exhibited distinct TRAE profiles consistent with their different mechanisms. As shown in Table 4, in OG, 52 patients (88.1%) who received anlotinib plus ICIs regimens experienced any-grade TRAEs, which was similar to the 56 patients (93.3%) in the chemotherapy group. The incidence of grade ≥3 TRAEs was slightly higher in OG at 42.2% compared to 55.0% in CG, but this difference was not statistically significant (χ2=1.898, P=0.168).
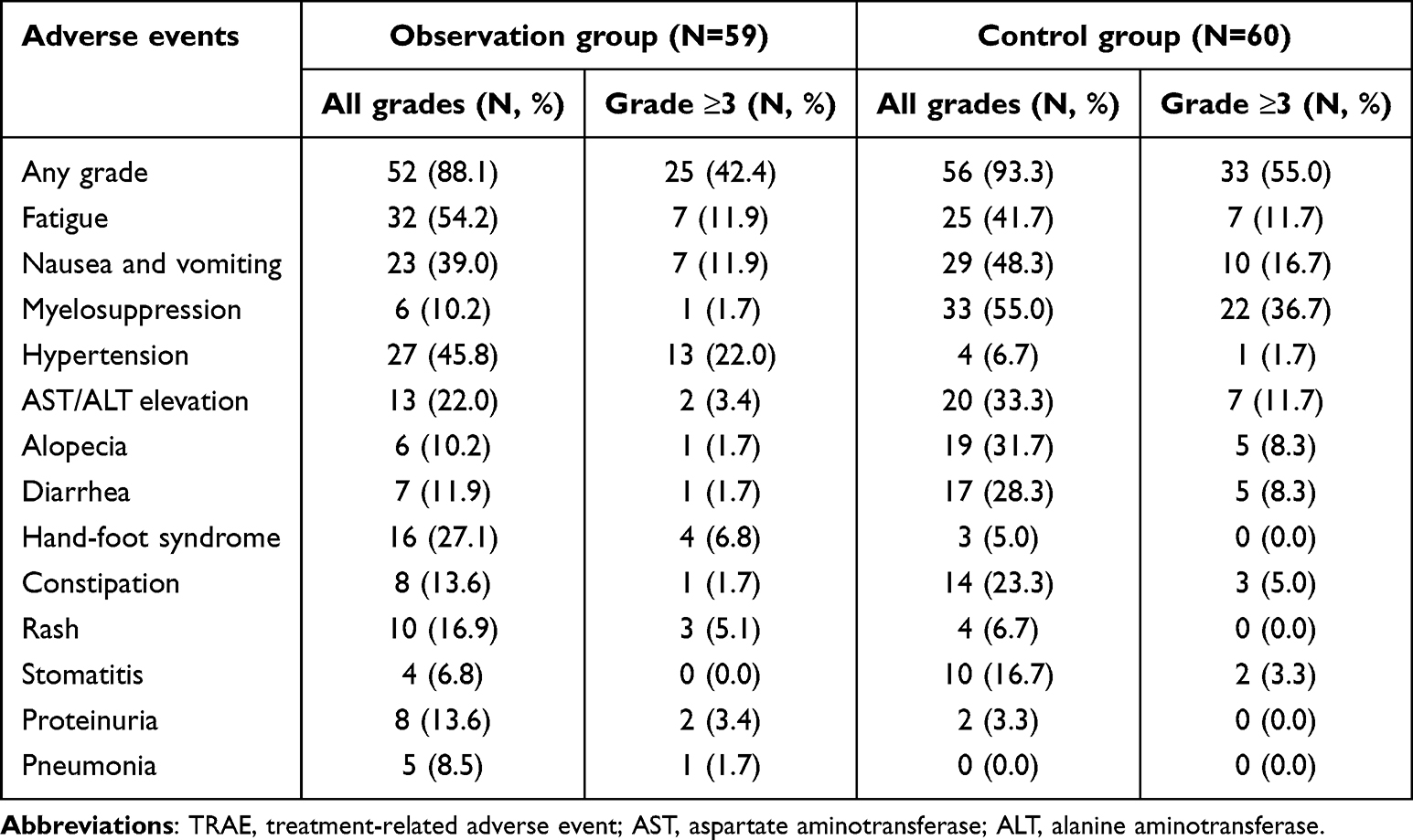 |
Table 4 Safety Profile of Patients in Observation Group and Control Group |
The most frequent TRAEs in anlotinib plus ICIs group were fatigue (54.2%), hypertension (45.8%), nausea/vomiting (39.0%) and hand–foot syndrome (27.1%). And clinically relevant grade ≥3 events mainly included hypertension (22.0%), fatigue (11.9%), nausea/vomiting (11.9%) and hand-foot syndrome (6.8%). In contrast, the chemotherapy group showed a toxicity profile dominated by cytotoxic-related events, with higher rates of myelosuppression (55.0%; grade ≥3=36.7%), nausea/vomiting (48.3%; grade ≥3=16.7%), Fatigue (41.7%; grade ≥3=11.7%) and AST/ALT elevation (33.3%; grade ≥3=11.7%), along with alopecia (31.7%) and diarrhea (28.3%). Rash, proteinuria, and pneumonia were observed only in the observation group, whereas grade ≥3 rash, proteinuria, and pneumonia were uncommon (≤5.1%). Overall, safety profile findings suggested that anlotinib plus ICIs was feasible in elderly patients with a toxicity spectrum distinct from and in some respects more favorable than that of single-agent chemotherapy.
Discussion
From a novelty perspective, although antiangiogenic agents combined with ICIs were explored previously in SCLC, direct comparative evidence in elderly patients with relapsed ES-SCLC remained limited. By focusing on an elderly population and using single-agent chemotherapy as a direct comparator, the present study provided clinically relevant real-world evidence. Nevertheless, given its retrospective design, these findings should be considered hypothesis-generating and required prospective validation.
These findings were significant given the historically poor outcomes of second-line treatments in SCLC. For context, traditional second-line chemotherapy options (such as topotecan, the only FDA-approved second-line drug for SCLC until recently) yielded median OS of approximately 6 months and ORRs below 15%.26 Our control arm results were consistent with this: median OS of 6.7 months and ORR 15% with single agents like irinotecan or taxanes, reflecting the limited efficacy of chemotherapy in refractory SCLC, especially among elderly patients.27 In contrast, the anlotinib plus ICIs combination in our study achieved an ORR of 34% and extended median OS to nearly 12 months, essentially doubling survival time. Although cross-trial comparisons must be cautious, it was notable that the OS of 11.9 months with the combination approached the survival durations seen in some first-line immunochemotherapy trials (for instance, atezolizumab plus chemotherapy in first-line gave median OS of 12.3 months in a broader population).28 Achieving a similar magnitude of survival in a subsequent-line elderly cohort was remarkable and underscored the potential efficacy of this combination. Our results aligned with and built upon emerging evidence from other studies exploring angiogenesis inhibition plus immunotherapy in SCLC. Chen et al (2025) reported a retrospective series of 68 ES-SCLC patients who received anlotinib plus PD-1/PD-L1 inhibitors after prior immunotherapy failure.1 They observed an ORR of 32.4%, median PFS of 5.6 months, and median OS of 13.2 months, which were very close to the efficacy outcomes in our combination arm (ORR=33.9%, median PFS=5.5 months, and median OS of 11.9 months). This convergence of data strongly suggested that adding anlotinib might substantially enhance the activity of immunotherapy in SCLC, even after prior exposure. Another real-world study by Yang et al (2024) evaluated anlotinib plus immunotherapy as maintenance after first-line chemo-ICI in 12 ES-SCLC patients29 they found a median PFS of 13.6 months and median OS of 19.5 months in that small cohort, while not directly comparable (given maintenance setting and highly selected patients), indicated the combination’s potential to extend survival beyond what immunotherapy alone might achieve. Taken together, these studies and our current analysis painted a consistent picture: the synergistic combination of antiangiogenic therapy and ICIs might provide durable disease control in SCLC, surpassing historical benchmarks of either modality alone. The multivariable Cox analysis highlighted that therapeutic regimen remained independently associated with survival, anlotinib plus ICIs demonstrated a significantly lower hazard of death than chemotherapy (HR=0.58, 95% CI: 0.41–0.89, P=0.011). Clinically, this benefit was observed after adjusting for key disease and host-related factors that were particularly relevant in elderly ES-SCLC. Better performance status (ECOG 0–1 vs 2) was a strong favorable factor (HR=0.52, P=0.009), consistent with real-world ES-SCLC data showing ECOG status as a major determinant of outcomes.30 Likewise, platinum-sensitive relapse (vs platinum-resistant) predicted improved OS (HR=0.64; P=0.021), in line with the established prognostic and treatment-selection role of platinum sensitivity status in relapsed SCLC.31 Conversely, liver metastases status was independently associated with worse survival (HR=1.38; P=0.025), aligning with contemporary evidence that liver involvement was a negative prognostic feature in ES-SCLC.32 A lower metastatic burden (≤3 vs >3 lesions) also correlated with longer OS (HR=0.61; P=0.015), supporting the concept that tumor burden adversely impacted prognosis.33 Notably, chronologic age (>71 vs ≤71) and prior ICIs exposure were not independently associated with OS in this model, suggesting that in an elderly population, functional status and disease biology (platinum sensitivity, liver involvement, metastatic burden) might be more informative than age alone for risk stratification and treatment selection.
Mechanistically, this synergy likely arose from multiple factors. Anlotinib’s inhibition of VEGFR and related receptors not only exerted direct anti-tumor and antiangiogenic effects (starving the tumor of blood supply and slowing growth), but also might modulate the tumor microenvironment in ways that enhanced immune response.34 Antiangiogenic TKIs might normalize the abnormal tumor vasculature, improving perfusion and immune-cell trafficking into tumor sites.35 VEGF pathway blockade also reversed immunosuppressive signals. For instance, VEGF inhibition might decrease myeloid-derived suppressor cells and regulatory T-cells, while increasing cytotoxic T-cell infiltration in tumors.36 These changes created a more favorable milieu for ICIs to activate an anti-tumor immune attack. In essence, anlotinib might convert previously “cold” tumors (with low immune activity) into “hotter” tumors more susceptible to immune-mediated killing.37 Our finding that some patients in OG had very prolonged responses (with a tail of the survival curve at 2+ years) was suggestive of the kind of durable benefit one might expect from immune mechanism engagement. This was in stark contrast to chemotherapy, where responses were rarely durable in SCLC. From a clinical standpoint, these results might inform treatment decisions in subsequent-line ES-SCLC. Currently, there was no globally accepted standard for second-line systemic therapy in ES-SCLC, especially after failure of platinum and immunotherapy.18 Topotecan was a traditional option (with poor efficacy and significant toxicity). In 2020, lurbinectedin (a novel DNA minor-groove binder) received accelerated approval as a second-line treatment based on a 35% ORR in platinum-sensitive disease, but subsequent trials had tempered enthusiasm and access to lurbinectedin was limited in some regions.38 Anlotinib was approved in China for third-line SCLC and was included in Chinese guidelines. Our data suggested that combining it with PD-1/PD-L1 blockade might be a superior paradigm to monotherapy. Perhaps the future of SCLC management might involve triplet combinations (chemotherapy plus immunotherapy plus antiangiogenic TKI) in fit patients, or dual combinations (immunotherapy plus antiangiogenic TKI) in those who could not tolerate chemotherapy. Our study contributed real-world evidence that, in practice, this strategy yielded better survival than chemotherapy in elderly, previously treated population.
In this elderly ES-SCLC cohort, the safety profile of anlotinib plus ICIs was clinically manageable and mechanistically distinct from single-agent chemotherapy with broadly comparable rates of any-grade TRAEs (88.1% vs 93.3%) and a numerically lower incidence of grade ≥3 events in OG (42.4% vs 55.0%). The OG toxicity spectrum was dominated by VEGFR-pathway/on-target adverse events, particularly hypertension (45.8%), hand–foot syndrome (27.1%) and proteinuria (13.6%), alongside fatigue and nausea/vomiting—patterns consistent with established VEGFR-TKI toxicity.39 In contrast, the CG toxicity profile was driven by cytotoxic-typical toxicities, most notably myelosuppression (55.0%) with higher gastrointestinal toxicity and alopecia, reflecting the expected burden of irinotecan and taxanes in later-line settings.40 Notably, events such as rash, proteinuria and pneumonia in OG were infrequently severe, reinforcing the need for routine monitoring (blood pressure, urinalysis, and respiratory symptoms) and timely supportive management rather than suggesting new safety signals.41 From a geriatric-oncology perspective, several adverse events warranted heightened surveillance and proactive management when using anlotinib plus ICIs in elderly ES-SCLC. Hypertension, proteinuria and AST/ALT elevation were more common among elderly patients and proactive symptom-directed supportive care should be implemented throughout administration of anlotinib plus ICIs among elderly patients.10,42 It was worth noting that no new safety signals emerged from combining anlotinib with ICIs in our study. The toxicities were largely predictable from each component and did not appear to synergize to produce worse outcomes. Specifically, although both anlotinib and ICIs might independently cause pneumonitis (TKI-induced or immune-related pneumonitis),43 we saw pneumonitis was only 8.5% of patients, a manageable incidence. Thus, the combination appeared to be not only effective but also tolerable for elderly patients as long as they were monitored and managed appropriately.
This study specifically focused on an elderly cohort with a median age of 71 years and including patients up to 88 years old. This was a group often underrepresented in clinical trials and sometimes undertreated in practice due to concerns about frailty. Importantly, the survival advantage of the combination was seen even in patients ≥75, and the toxicity did not seem prohibitive in this subgroup. In fact, one could argue that avoiding intensive chemotherapy in favor of a targeted plus immunotherapy approach might be preferable for many elderly patients. Our findings thereby stressed that age alone should not exclude patients from receiving potentially effective therapies like anlotinib plus ICIs. With careful patient selection (eg. those with ECOG 0–2 and without uncontrolled comorbidities) and supportive measures, even septuagenarians and octogenarians might tolerate and benefit from this regimen. This was consistent with other real-world observations in lung cancer that chronological age was less important than biological fitness in determining treatment tolerability.44 It also resonated with a prior analysis that showed even very elderly SCLC patients (≥80) who received some active treatment (chemotherapy or radiotherapy) doubled their survival compared to those untreated,11 implying that offering therapy was crucial, and our results suggested that offering a more efficacious therapy (anlotinib plus ICIs) might substantially improve outcomes in this group.
Several limitations should be acknowledged. First, the retrospective design introduced risks of selection bias and residual confounding. Although measured baseline characteristics were balanced and multivariable adjustment was performed, unmeasured factors might have influenced treatment selection. For example, physicians might have preferentially selected anlotinib plus ICIs for patients with better functional reserve, stronger treatment motivation, or better access to ICIs, which might result in improved outcomes. Second, propensity score matching was not performed. We chose not to apply matching because the sample size was modest and matching might have excluded clinically informative elderly patients, but the absence of PSM limited causal inference. Third, the treatment arms were heterogeneous: the chemotherapy group included irinotecan, docetaxel and paclitaxel, while the combination group included several PD-1/PD-L1 inhibitors. This heterogeneity reflected real-world practice but might introduce variability. Fourth, the sample size was limited, and the study was underpowered for definitive subgroup comparisons. Fifth, follow-up duration was still relatively short to fully assess long-term survival tail or late toxicities, especially for those on immunotherapy (immune-related effects like endocrinopathies might occur late among elderly patients).45 Continued follow-up was important to determine if any long-term survivors emerged predominantly from the combination treatment.
Prospective validation was warranted. A suitable next step would be a multicenter randomized phase II trial comparing anlotinib plus a predefined PD-1/PD-L1 inhibitor versus investigator’s choice standard single-agent chemotherapy in elderly patients with previously treated ES-SCLC. Stratification factors should include platinum sensitivity, prior ICI exposure, ECOG performance status, liver metastases and age subgroup. In addition to OS and PFS, future trials should incorporate independent radiologic review, geriatric assessment, patient-reported quality of life, comorbidity burden and prospective toxicity monitoring. If positive, such a trial could support a larger Phase III confirmatory study.
Conclusion
Anlotinib plus ICIs was associated with improved survival and tumor control compared with single-agent chemotherapy with manageable toxicity in elderly patients with previously treated ES-SCLC. The observed benefit appeared clinically relevant and was not limited by chronological age or prior ICIs exposure in the adjusted analysis. Nevertheless, the present real-world evidence should be considered hypothesis-generating because of the retrospective design, treatment heterogeneity and potential selection bias. Careful patient selection, particularly regarding ECOG performance status, comorbidities and the ability to tolerate antiangiogenic and immune-related toxicities, remained essential. Prospective randomized trials were needed to confirm whether anlotinib plus ICIs might become a standard later-line option for elderly patients with ES-SCLC subsequently.
Consent Statement
Despite the informed consent was waived by the Ethics Committee of Liaoning Cancer Hospital & Institute, we confirmed that the data of the patients included in this study was anonymized or maintained with confidentiality.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Chen T-F, Li Z-J, Zhao H-S, Yang R. Feasibility and safety of anlotinib combined with immune checkpoint inhibitors in patients with previously immunotherapy-treated extensive-stage small cell lung cancer: a retrospective exploratory study. Drug Des Devel Ther. 2025;19:4991–16. doi:10.2147/dddt.s525481
2. Paz-Ares L, Borghaei H, Liu SV, et al. Efficacy and safety of first-line maintenance therapy with lurbinectedin plus atezolizumab in extensive-stage small-cell lung cancer (IMforte): a randomised, multicentre, open-label, Phase 3 trial. Lancet. 2025;405(10495):2129–2143. doi:10.1016/s0140-6736(25)01011-6
3. Cheng Y, Zhang W, Wu L, et al. Toripalimab plus chemotherapy as a first-line therapy for extensive-stage small cell lung cancer: the phase 3 EXTENTORCH randomized clinical trial. JAMA Oncol. 2025;11(1):16–25. doi:10.1001/jamaoncol.2024.5019
4. Kim SY, Park HS, Chiang AC. Small cell lung cancer: a review. JAMA. 2025;333(21):1906–1917. doi:10.1001/jama.2025.0560
5. Bonn O, Schmidt-Wolf G, Risse F, Glasmacher A, Kleinschmidt R, Schmidt-Wolf IG. Vindesine and etoposide: a practical and well-tolerated therapy for elderly patients or patients in reduced clinical condition with extensive-stage small-cell lung cancer (SCLC). Med Sci Monit. 2005;11(2):Pi19–21.
6. Shah C, Hong YR, Bishnoi R, Jones D, Huo J. Utilization of antineoplastic agents and medicare spending in elderly patients with extensive-stage small-cell lung cancer between 2001 and 2013. JCO Oncol Pract. 2020;16(7):e610–e621. doi:10.1200/jop.19.00559
7. Hatfield LA, Huskamp HA, Lamont EB. Survival and toxicity after cisplatin plus etoposide versus carboplatin plus etoposide for extensive-stage small-cell lung cancer in elderly patients. J Oncol Pract. 2016;12(7):666–673. doi:10.1200/jop.2016.012492
8. Bergerot CD, Temin S, Verduzco-Aguirre HC, et al. Geriatric assessment: ASCO global guideline. JCO Glob Oncol. 2025;11:e2500276. doi:10.1200/go-25-00276
9. Paz-Ares L, Dvorkin M, Chen Y, et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929–1939. doi:10.1016/s0140-6736(19)32222-6
10. Song PF, Xu N, Li Q. Efficacy and safety of anlotinib for elderly patients with previously treated extensive-stage SCLC and the prognostic significance of common adverse reactions. Cancer Manag Res. 2020;12:11133–11143. doi:10.2147/cmar.s275624
11. Schild SE, Zhao L, Wampfler JA, et al. Small-cell lung cancer in very elderly (≥ 80 Years) patients. Clin Lung Cancer. 2019;20(4):313–321. doi:10.1016/j.cllc.2019.05.007
12. Misumi Y, Okamoto H, Sasaki J, et al. Phase I/II study of induction chemotherapy using carboplatin plus irinotecan and sequential thoracic radiotherapy (TRT) for elderly patients with limited-disease small-cell lung cancer (LD-SCLC): TORG 0604. BMC Cancer. 2017;17(1):377. doi:10.1186/s12885-017-3353-y
13. Liu SV, Reck M, Mansfield AS, et al. Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with atezolizumab, carboplatin, and etoposide (IMpower133). J Clin Oncol. 2021;39(6):619–630. doi:10.1200/jco.20.01055
14. Goldman JW, Dvorkin M, Chen Y, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2021;22(1):51–65. doi:10.1016/s1470-2045(20)30539-8
15. Zhang T, Li W, Diwu D, Chen L, Chen X, Wang H. Efficacy and safety of first-line immunotherapy plus chemotherapy in treating patients with extensive-stage small cell lung cancer: a Bayesian network meta-analysis. Front Immunol. 2023;14:1197044. doi:10.3389/fimmu.2023.1197044
16. Wu JT, Corrigan J, Su C, et al. The performance status gap in immunotherapy for frail patients with advanced non-small cell lung cancer. Cancer Immunol Immunother. 2024;73(9):172. doi:10.1007/s00262-024-03763-w
17. Zhao Y, Wan B, Zhang T, et al. Irinotecan, topotecan, paclitaxel or docetaxel for second-line treatment of small cell lung cancer: a single-center retrospective study of efficiency comparation and prognosis analysis. Transl Lung Cancer Res. 2019;8(6):829–837. doi:10.21037/tlcr.2019.10.21
18. Meriggi F. Second-line treatment options for small-cell lung cancer: a light at the end of the tunnel. Cancers. 2024;16(2). doi:10.3390/cancers16020255
19. Geng N, Ding CM, Liu ZK, Song S, Hu WX. Influence of VEGFR2 gene polymorphism on the clinical outcomes of apatinib for patients with chemotherapy-refractory extensive-stage SCLC: a real-world retrospective study. Int J Clin Oncol. 2021;26(4):670–683. doi:10.1007/s10147-020-01849-w
20. Spigel DR, Townley PM, Waterhouse DM, et al. Randomized phase II study of bevacizumab in combination with chemotherapy in previously untreated extensive-stage small-cell lung cancer: results from the SALUTE trial. J Clin Oncol. 2011;29(16):2215–2222. doi:10.1200/jco.2010.29.3423
21. Cheng Y, Wang Q, Li K, et al. Anlotinib for patients with small cell lung cancer and baseline liver metastases: a post hoc analysis of the ALTER 1202 trial. Cancer Med. 2022;11(4):1081–1087. doi:10.1002/cam4.4507
22. Hong X, Qiu S, Wu X, et al. Efficacy and safety of anlotinib in overall and disease-specific advanced gynecological cancer: a real-world study. Drug Des Devel Ther. 2023;17:2025–2033. doi:10.2147/dddt.s408304
23. Yang J, Yan J, Liu B. Targeting VEGF/VEGFR to modulate antitumor immunity. Front Immunol. 2018;9:978. doi:10.3389/fimmu.2018.00978
24. Chung HC, Piha-Paul SA, Lopez-Martin J, et al. Pembrolizumab after two or more lines of previous therapy in patients with recurrent or metastatic SCLC: results from the KEYNOTE-028 and KEYNOTE-158 studies. J Thorac Oncol. 2020;15(4):618–627. doi:10.1016/j.jtho.2019.12.109
25. Chouaïd C, Baize N, Monnet I. Second-line therapy for disseminated small-cell lung cancer: optimal management remains to be defined. Transl Lung Cancer Res. 2020;9(5):1732–1735. doi:10.21037/tlcr-20-362
26. Blackhall F, Jao K, Greillier L, et al. Efficacy and safety of rovalpituzumab tesirine compared with topotecan as second-line therapy in DLL3-high SCLC: results from the phase 3 TAHOE study. J Thorac Oncol. 2021;16(9):1547–1558. doi:10.1016/j.jtho.2021.02.009
27. Igawa S, Naoki K, Shintani Y, et al. Survival and prognostic factors in elderly patients receiving second-line chemotherapy for relapsed small-cell lung cancer: results from the Japanese Joint Committee of Lung Cancer Registry. Lung Cancer. 2020;146:160–164. doi:10.1016/j.lungcan.2020.05.038
28. Reck M, Dziadziuszko R, Sugawara S, et al. Five-year survival in patients with extensive-stage small cell lung cancer treated with atezolizumab in the Phase III IMpower133 study and the Phase III IMbrella A extension study. Lung Cancer. 2024;196:107924. doi:10.1016/j.lungcan.2024.107924
29. Yang P, Luo H, Zhao L, Xiong F, Tang C. Effectiveness and safety of anlotinib plus anti-programmed cell death 1/ligand 1 (anti-PD-1/PD-L1) antibodies as maintenance therapy after first-line chemotherapy combined with anti-PD-1/PD-L1 antibodies in extensive-stage small cell lung cancer: a real-world study. J Thorac Dis. 2024;16(7):4391–4399. doi:10.21037/jtd-24-394
30. Dawe DE, Rittberg R, Syed I, et al. Real-world predictors of survival in patients with extensive-stage small-cell lung cancer in Manitoba, Canada: a retrospective cohort study. Front Oncol. 2023;13:1191855. doi:10.3389/fonc.2023.1191855
31. Lara PN Jr, Moon J, Redman MW, et al. Relevance of platinum-sensitivity status in relapsed/refractory extensive-stage small-cell lung cancer in the modern era: a patient-level analysis of southwest oncology group trials. J Thorac Oncol. 2015;10(1):110–115. doi:10.1097/jto.0000000000000385
32. Kaira K, Kurata Y, Imai H, et al. Prognostic factors of liver metastases in extensive-stage small cell lung cancer receiving chemo-immunotherapy. Transl Lung Cancer Res. 2025;14(5):1569–1581. doi:10.21037/tlcr-2024-1091
33. Oliver DE, Donnelly OG, Grass GD, et al. Extracranial metastatic burden in extensive-stage small cell lung cancer: implications for prophylactic cranial irradiation. J Thorac Dis. 2018;10(7):4321–4327. doi:10.21037/jtd.2018.06.92
34. Huang Y, Goel S, Duda DG, Fukumura D, Jain RK. Vascular normalization as an emerging strategy to enhance cancer immunotherapy. Cancer Res. 2013;73(10):2943–2948. doi:10.1158/0008-5472.can-12-4354
35. Zhang Y, Brekken RA. Direct and indirect regulation of the tumor immune microenvironment by VEGF. J Leukoc Biol. 2022;111(6):1269–1286. doi:10.1002/jlb.5ru0222-082r
36. Huang Y, Yuan J, Righi E, et al. Vascular normalizing doses of antiangiogenic treatment reprogram the immunosuppressive tumor microenvironment and enhance immunotherapy. Proc Natl Acad Sci U S A. 2012;109(43):17561–17566. doi:10.1073/pnas.1215397109
37. Su Y, Luo B, Lu Y, et al. Anlotinib induces a T cell-inflamed tumor microenvironment by facilitating vessel normalization and enhances the efficacy of pd-1 checkpoint blockade in neuroblastoma. Clin Cancer Res. 2022;28(4):793–809. doi:10.1158/1078-0432.ccr-21-2241
38. Singh S, Jaigirdar AA, Mulkey F, et al. FDA approval summary: lurbinectedin for the treatment of metastatic small cell lung cancer. Clin Cancer Res. 2021;27(9):2378–2382. doi:10.1158/1078-0432.ccr-20-3901
39. Shyam Sunder S, Sharma UC, Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. 2023;8(1):262. doi:10.1038/s41392-023-01469-6
40. Schuette W. Chemotherapy as treatment of primary and recurrent small cell lung cancer. Lung Cancer. 2001;33 Suppl 1:S99–107. 10.1016/s0169-5002(01)00309-9.
41. Si X, Zhang L, Wang H, et al. Management of anlotinib-related adverse events in patients with advanced non-small cell lung cancer: experiences in ALTER-0303. Thorac Cancer. 2019;10(3):551–556. doi:10.1111/1759-7714.12977
42. Mohile SG, Dale W, Somerfield MR, et al. Practical assessment and management of vulnerabilities in older patients receiving chemotherapy: ASCO guideline for geriatric oncology. J Clin Oncol. 2018;36(22):2326–2347. doi:10.1200/jco.2018.78.8687
43. Li X, Zhou Z, Hu Y, Chen H. Efficacy and safety of anlotinib combined with immunotherapy as first-line treatment in elderly patients with advanced non-small cell lung cancer. J Thorac Dis. 2025;17(6):3547–3558. doi:10.21037/jtd-2025-236
44. Almodovar T, Teixeira E, Barroso A, et al. Elderly patients with advanced NSCLC: the value of geriatric evaluation and the feasibility of CGA alternatives in predicting chemotherapy toxicity. Pulmonology. 2019;25(1):40–50. doi:10.1016/j.pulmoe.2018.07.004
45. Husebye ES, Castinetti F, Criseno S, et al. Endocrine-related adverse conditions in patients receiving immune checkpoint inhibition: an ESE clinical practice guideline. Eur J Endocrinol. 2022;187(6):G1–g21. doi:10.1530/eje-22-0689
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Current Insights into the Risks of Using Melatonin as a Treatment for Sleep Disorders in Older Adults
Tuft C, Matar E, Menczel Schrire Z, Grunstein RR, Yee BJ, Hoyos CM
Clinical Interventions in Aging 2023, 18:49-59
Published Date: 12 January 2023
Effectiveness and Safety of Anlotinib Combined with PD-1 Blockades in Patients with Previously Immunotherapy Treated Advanced Non-Small Cell Lung Cancer: A Retrospective Exploratory Study
Dou XJ, Ma RY, Ren DW, Liu Q, Yan P
Lung Cancer: Targets and Therapy 2024, 15:29-40
Published Date: 25 March 2024
Feasibility and Safety of Anlotinib Combined with Immune Checkpoint Inhibitors in Patients with Previously Immunotherapy-Treated Extensive-Stage Small Cell Lung Cancer: A Retrospective Exploratory Study
Chen TF, Li ZJ, Zhao HS, Yang R
Drug Design, Development and Therapy 2025, 19:4991-5005
Published Date: 9 June 2025
Effectiveness and Safety of Anlotinib-Related Therapeutic Regimens in Patients with Previously Immune Checkpoint Inhibitors-Treated Advanced NSCLC: A Real-World Exploratory Study
Fang XS, Zhang TS, Li SJ, Zhao YL, Li JB, Xia H, Wang RT
Drug Design, Development and Therapy 2025, 19:7527-7540
Published Date: 29 August 2025
Real-World Outcomes and Safety of PD-1 Blockade Rechallenge Strategies After Prior Immunotherapy in Advanced NSCLC: A Retrospective Cohort Study
Zheng LJ, Shen YL, Zhao HW, Ma YC, Wang AF
Drug Design, Development and Therapy 2026, 20:572625
Published Date: 18 February 2026