Back to Journals » Cancer Management and Research » Volume 18

Analyzing the Influence of Surgical Sequence on Perioperative Circulating Tumor Cells in Patients with Resectable Non-Small Cell Lung Cancer
Authors Chen H, He Y, Wang Y, Liu X, Zou G
Received 15 January 2026
Accepted for publication 14 May 2026
Published 3 June 2026 Volume 2026:18 596523
DOI https://doi.org/10.2147/CMAR.S596523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Haolin Chen,1,* Ying He,2,* Yun Wang,3 Xiaoming Liu,4 Guowen Zou4
1Department of Thoracic Surgery (Thyroid and Breast Surgery, Tumor Surgery), Kaiping Central Hospital, Jiangmen, Guangdong, 529300, People’s Republic of China; 2Department of Otorhinolaryngology Head and Neck Surgery, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330019, People’s Republic of China; 3Department of Dentistry, Kaiping Central Hospital, Jiangmen, Guangdong, 529300, People’s Republic of China; 4Department of Thoracic Surgery, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330019, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guowen Zou, Email [email protected] Xiaoming Liu, Email [email protected]
Objective: To investigate the impact of different surgical sequences on perioperative dynamic changes in circulating tumor cells (CTCs) in patients with resectable non-small cell lung cancer (NSCLC).
Methods: A total of 60 patients with resectable NSCLC were prospectively enrolled in this single-center, non-randomized observational study and divided into the lung-first group (n = 33) and the lymph node-first group (n = 27) according to surgical sequence.
Results: CTCs were detected in 97.5% of perioperative blood samples. In the overall cohort, total CTC counts did not differ significantly before and after surgery. However, surgical sequence was associated with distinct perioperative CTC dynamics. In the lung-first group, postoperative CTC counts were significantly lower than preoperative levels (median, 9 vs. 13 cells/5 mL; P = 0.007), whereas CTC counts increased significantly after surgery in the lymph node-first group (median, 20 vs. 9 cells/5 mL; P < 0.001). At the individual-patient level, CTC counts decreased in 66.7% of patients in the lung-first group, whereas they increased in 88.9% of patients in the lymph node-first group (P < 0.001). Postoperatively, the lung-first group showed a higher proportion of epithelial CTCs and a lower proportion of hybrid CTCs. Higher postoperative CTC counts were associated with pleural adhesion, lymphovascular invasion, and higher consolidation-to-tumor ratio.
Conclusion: Perioperative CTC dynamics in NSCLC are influenced by surgical sequence and clinicopathological characteristics. Prioritizing lung tumor resection before lymph node dissection may be associated with reduced perioperative CTC dissemination and a more favorable CTC phenotype; however, these preliminary findings require validation in larger prospective randomized studies.
Keywords: circulating tumor cells, non-small-cell lung carcinoma, surgical sequence, lymph node dissection, metastasis
Introduction
Lung cancer is one of the most common and deadly malignant tumors worldwide.1 Non-small cell lung cancer (NSCLC) accounts for 75% - 85% of lung cancers, and its prognosis is poor with a high mortality rate.2 Due to the lack of early symptoms, most patients are diagnosed at an advanced stage, and the 5-year survival rate is relatively low.3,4 Surgical resection remains the main treatment method for early and some locally advanced NSCLC patients,5 but 30% - 50% of patients still experience recurrence or metastasis after surgery,6,7 which may be related to pre-existing micrometastatic foci, tumor heterogeneity, and clonal evolution.8 Tumor micrometastasis is an important prerequisite for recurrent tumor metastasis,9 and accurately assessing the spread and recurrence risk of the tumor is crucial for postoperative management. Traditional imaging methods (such as CT, PET-CT) often have difficulty detecting early micrometastatic lesions,10 and the specificity and sensitivity of serum tumor markers (such as CEA, CA125) are usually limited.11 Although tissue biopsy remains the gold standard for diagnosis, its invasive nature makes it impossible to conduct repeated real-time monitoring. Therefore, new biomarkers are urgently needed for precise assessment. It is necessary to introduce new detection technologies and combine them with existing examination methods to more accurately assess the patient’s condition.
Circulating tumor cells (CTCs) are tumor cells that detach from the primary or metastatic tumor tissue and enter the bloodstream. They are a key step in distant tumor metastasis.12 CTCs are not a homogeneous population. Based on epithelial–mesenchymal transition (EMT), they can be classified into epithelial, mesenchymal, and hybrid types. Among them, hybrid-type CTCs, which co-express epithelial and mesenchymal features, are considered to have stronger invasive ability and higher metastatic potential, and have been associated with poorer clinical outcomes.13 In addition, CTC clusters have been reported to show higher metastatic efficiency and are linked to shorter survival. In contrast, epithelial-type CTCs are generally considered less aggressive. Therefore, both the number and the subtype composition of CTCs may have important clinical value in predicting tumor progression and prognosis. Previous studies have shown that CTC detection has value in evaluating prognosis and monitoring disease progression in various cancers.14–17 Surgical intervention itself may influence the dissemination of tumor cells. It has been reported that intraoperative tumor manipulation, vascular handling, and lung resection can promote the release of tumor cells into the circulation,18 In addition, perioperative changes in CTC levels have been observed in patients undergoing lung cancer surgery, suggesting that surgical manipulation may affect tumor cell dissemination. From a mechanistic perspective, manipulation of the tumor-bearing lung before vascular or lymphatic control may theoretically promote mechanical shedding of tumor cells into the circulation. Conversely, lymph node manipulation before tumor removal may disturb lymphatic drainage pathways, dislodge tumor cells from nodal deposits, or alter potential metastatic “landing sites.” Therefore, surgical sequence may influence perioperative CTC dissemination through different patterns of tumor, vascular, and lymphatic manipulation. However, current clinical evidence regarding the impact of surgical sequence on perioperative CTC dynamics in NSCLC remains limited.
From an oncological perspective, the concept of the “no-touch isolation” technique has been proposed to reduce intraoperative tumor cell dissemination. This principle emphasizes early vascular control and minimizing direct manipulation of the tumor-bearing tissue before isolation of the tumor from the systemic circulation. It has been widely discussed in the surgical management of solid tumors, particularly in colorectal cancer, where early ligation of tumor-draining vessels has been associated with reduced hematogenous spread of tumor cells. In this context, the sequence of surgical procedures in lung cancer surgery may also influence the extent of tumor cell release into the circulation. However, whether different operative sequences conform to this principle and affect perioperative CTC dynamics in NSCLC remains unclear.
Therefore, this study aimed to evaluate perioperative changes in CTC counts and subtypes in patients with resectable NSCLC undergoing different surgical sequences and to explore the potential association between surgical sequence and CTC dissemination.
Materials and Methods
Study Population
The patients were not randomly assigned. The choice of surgical sequence was determined according to preoperative imaging findings, tumor location, intraoperative anatomical exposure, operative feasibility, and the surgeon’s intraoperative judgment. In general, the lung-first approach was preferred when early control of the target lobe vessels and lung lesion was technically feasible, whereas the lymph-node-first approach was selected when initial lymph node dissection was required to improve exposure or facilitate subsequent lung resection These decisions were made by the operating surgeon according to intraoperative conditions. This study was conducted in accordance with the revised Helsinki Declaration and was approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University (Approval Number: IIT [2023] No. 267).
Inclusion and Exclusion Criteria
Inclusion Criteria
① Patients aged 18–80 years;
② Those who were first diagnosed with primary malignant tumours of the lungs, pathologically or cytologically confirmed as NSCLC;
③ No previous malignant tumour in other parts of the body;
④ No distant metastasis in preoperative imaging;
⑤ The patient’s heart, liver, lungs, kidneys and other important organs have normal or basically normal function. (Cardiac function includes: no obvious ventricular wall motion abnormality on cardiac ultrasound, left ventricular ejection fraction ≥60%, and no significant abnormality on electrocardiogram; hepatic function includes: total bilirubin ≤1.5 times the upper limit of the normal value, and glutamic oxidase and azelaic transaminase ≤2.5 times the upper limit of the normal value; pulmonary function test suggests that the expected value of FEV1 ≥40% after surgery, and DLCO ≥40%; renal function includes: creatinine ≤1.5 times the upper limit of the normal value, and DLCO ≥40%. (1.5 times the upper limit of normal value, and creatinine clearance ≥ 60 mL/min);
⑥ Patients or their authorised principals gave informed consent to the content and purpose of the study and participated voluntarily.
Exclusion Criteria (Fulfilling Any One of the Following)
①Patient’s age is less than 18 years old or more than 80 years old;
② Pathological or cytological confirmation of non-NSCLC;
③ Patients with important organ dysfunction and contraindications to surgery;
④ Combined autoimmune disease and coagulation-related diseases;
⑤ Previous history of malignant tumour;
⑥ Patients or their authorised principals who refuse the study.
Study Design and Endpoints
This was a prospective, non-randomized, two-arm exploratory study designed to evaluate the immediate perioperative dynamics of CTCs in resectable NSCLC patients undergoing different surgical sequences. Given the exploratory nature of the study and the relatively small sample size, no formal adjustment for multiple comparisons was applied.
Primary Endpoint
The difference in dynamic changes in total CTC count from before to after surgery between the lung-first group and the lymph node-first group.
Secondary Endpoints
① Changes in the subtype composition (epithelial, hybrid, mesenchymal) of CTCs before and after surgery within and between groups.
② The correlation between perioperative CTC counts and clinicopathological characteristics (eg., pleural adhesion, lymphovascular invasion, consolidation-to-tumor ratio (CTR)).
③ The impact of specific surgical techniques (eg., wedge resection) on postoperative CTC levels.
Surgical Procedure
Preoperative Preparation
Preoperative investigations included general haematological tests such as blood count, blood group, liver and kidney function, electrolytes, and cardiopulmonary function tests. Preoperative staging tests are routinely performed, including enhanced CT scan of the chest, magnetic resonance imaging of the head, whole-body bone plane imaging, and ultrasound or CT examination of the abdomen.
Surgical Approach
All surgeries were performed by three experienced thoracic surgeons under general anesthesia with double-lumen endotracheal intubation. Patients were placed in the lateral decubitus position with one‑lung ventilation. Surgical access (single‑port or single‑utility‑port VATS) was selected based on preoperative planning and surgeon preference. Except for one conversion to open thoracotomy due to dense pleural adhesions, all other procedures (n=59) were performed minimally invasively, including lobectomy, segmentectomy, or wedge resection.
In the lung‑first group (Figure 1A), during lobectomy the vessels of the target lobe were ligated and divided first, followed by removal of the lobe. Hilar and mediastinal lymph nodes were systematically dissected afterward (right side: stations 2R, 3a, 3p, 4R, 7, 8, 9; left side: stations 4L, 5, 6, 7, 8, 9). For segmentectomy, 3D reconstruction was used for preoperative planning, and the segmental vessels and bronchus were ligated and divided accordingly, with systematic lymph node sampling performed. Prior to wedge resection, CT‑guided Hookwire localization was performed, and resection was completed within 1–2 h after localization.
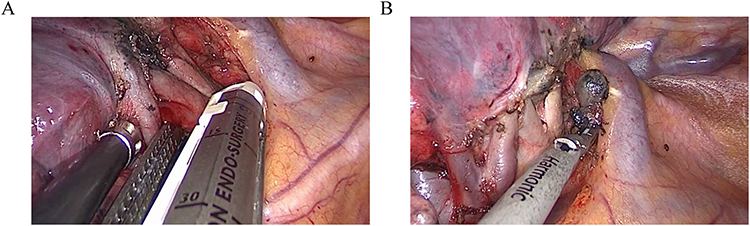 |
Figure 1 (A) Intraoperative prioritisation of target lungs. (B) Intraoperative prioritisation of lymph nodes. |
In the lymph node-first group (Figure 1B), the order was reversed: target lymph nodes were dissected or sampled first, followed by resection of the lung lesion. All procedures followed standardized institutional protocols for thoracoscopic lung resection and lymph node dissection.
Research Methods
Collection and Preservation of Samples
Before the operation (during skin incision) and after the operation (when thoracic cavity closure is completed), 5 mL of central venous blood was collected from the patient into EDTA anticoagulant tubes (Figure 2A and B). To avoid interference from residual drugs or liquids in the central venous pathway, 10 mL of venous blood was discarded before sampling, and then 5 mL of the required blood sample for the study was collected. After blood collection, the blood was gently inverted and mixed 10 times to ensure thorough mixing of the blood with the anticoagulant. The samples were pre-treated within 4 hours after collection; if not processed in time, they were stored in a 4°C refrigerator and sent for testing within 12 hours. All samples were quality-controlled by laboratory personnel before testing, and samples with hemolysis or other unqualified conditions were excluded and recorded.
 |
Figure 2 (A) EDTA anticoagulated blood collection tube. (B) Specimen collection site. |
Selection of CTCs Separation and Identification Techniques
Although separation techniques based on the physical (such as density, volume, diameter, charge) or biological (such as expression of cell surface antigens and protein markers) characteristics of CTCs have been widely used in clinical practice,19,20 these methods are difficult to effectively identify CTC subpopulations that are in the process of EMT.21 Therefore, in this study, the CanPatrol CTC Typing Detection System, which does not rely on specific markers, was used for CTC separation, identification and analysis.
Canpatrol CTCs Detection Principle and Process
The Canpatrol system consists of two parts: CTCs separation and typing identification. Separation stage: After the blood sample is lysed, it passes through an 8 μm pore size nanofilter membrane, and CTCs are captured by the size difference between tumor cells and white blood cells. This can enrich epithelial, mesenchymal, mixed CTCs and circulating tumor microthrombi (CTM). This system is applicable to most solid tumors, with a detection sensitivity of 1 CTC /5mL peripheral blood, enrichment efficiency ≥ 80%, and specificity > 90%. Typing identification stage: Using multiple mRNA in situ hybridization technology, specific nucleic acid labeling and typing of the enriched CTCs are performed using epithelial and mesenchymal cell markers (such as EpCAM, E-cadherin, Twist, etc). This technology significantly improves detection sensitivity through the hybridization of multiple RNA probes with target genes and amplification by a fluorescence signal system.22 The specific operation process is as follows (Figure 3).
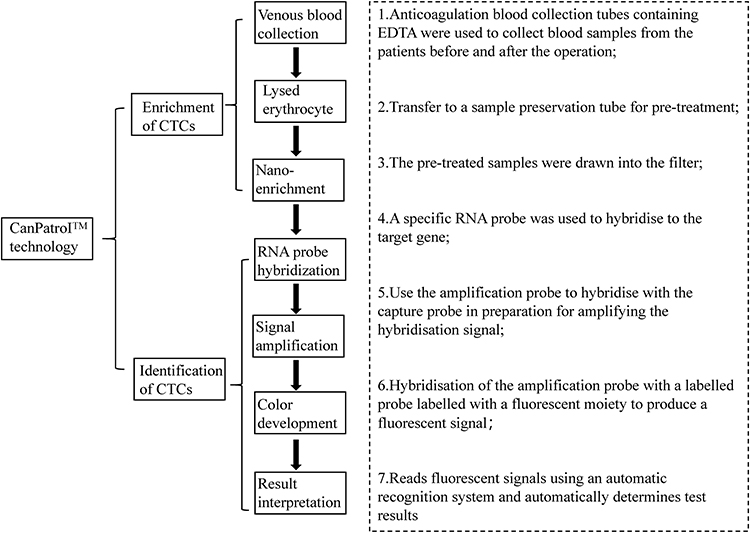 |
Figure 3 Flowchart of the operation of Canpatrol CTCs. |
Interpretation of Results
CTCs were further classified according to the fluorescence signals expressed by each subtype. Red fluorescence represented epithelial markers, including EpCAM and E-cadherin; green fluorescence represented mesenchymal markers, such as Twist; white fluorescence identified leukocytes; and DAPI indicated nuclear staining. Epithelial-type CTCs showed red fluorescence, mesenchymal-type CTCs showed green fluorescence, and hybrid-type CTCs showed both red and green fluorescence, as shown in Table 1 and Figure 4.
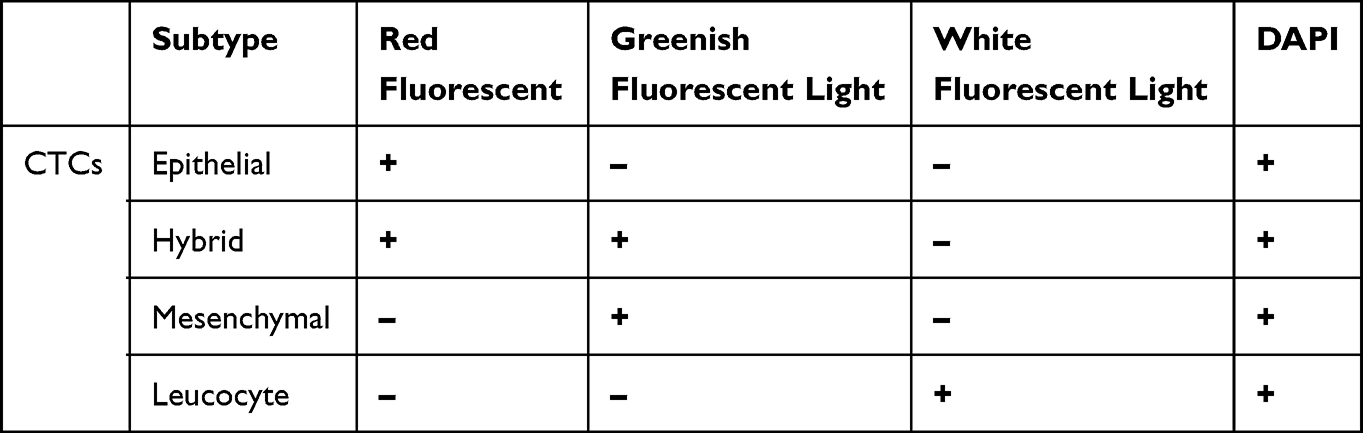 |
Table 1 Fluorescence Signal Characteristics and Corresponding Biomarkers Used for Classification of CTC Subtypes. Red Fluorescence Represents Epithelial Markers (EpCAM, E-Cadherin); Green Fluorescence Represents Mesenchymal Markers (E.g., Twist); White Fluorescence Identifies Leukocytes; DAPI Indicates Nuclear Staining. CTC Subtypes Were Classified Based on the Combination of These Fluorescence Signals |
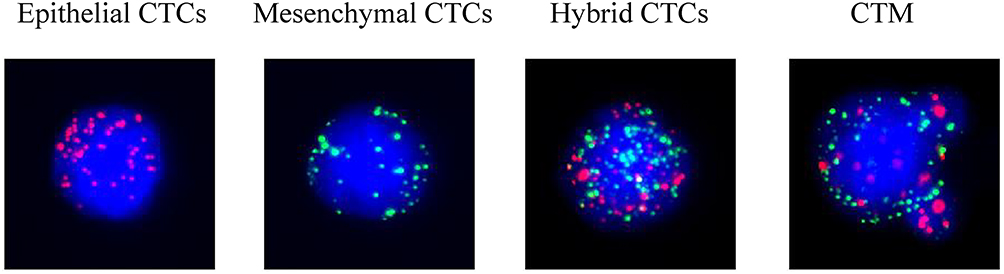 |
Figure 4 Representative fluorescence images of circulating tumor cell (CTC) subtypes identified by RNA in situ hybridization. Epithelial-type CTCs show red fluorescence corresponding to epithelial markers (EpCAM, E-cadherin). Mesenchymal-type CTCs show green fluorescence corresponding to mesenchymal markers (e.g., Twist). Hybrid-type CTCs co-express epithelial and mesenchymal markers and therefore display both red and green fluorescence. Nuclei are stained with DAPI, and leukocytes are identified by white fluorescence. |
Observation Indicators
① General condition of patients, such as gender, age, etc;
② Tumour location, length and diameter, solid tumour ratio (CTR), pathological type, degree of differentiation, clinical staging;
③ Serum tumour markers: carcinoembryonic antigen (CEA) (reference range 0.00–5.00 ng/mL), ferritin (reference range 13.00–150.00 U/mL), cytokeratin 19 fragment (CYFRA) (reference range 0.00–3.30 ng/mL), neuron-specific enolase (NSE) (reference range 0.00–16.30 ng/mL). 16.30 ng/mL), squamous cell carcinoma antigen (SCCA) (reference range 0.00–3.00 ng/mL), and so on;
④ Surgical method, intraoperative operation sequence, pleural adhesion, duration of surgery, and postoperative hospitalisation days;
⑤ Changes in preoperative and postoperative levels of CTCs (CTCs > 0 /5mL is considered positive, CTCs = 0 /5mL is considered negative) and staging.
Statistical Methods
Data were analysed using IBM SPSS Statistics 25.0 and Excel 2016. CTC counts and other continuous variables are presented as median (interquartile range). The nonparametric Mann–Whitney U-test was used for comparisons between two independent groups, the Wilcoxon signed-rank test was used for paired comparisons before and after surgery, and the Kruskal–Wallis test was used for comparisons among three or more groups. Given the non-randomized design and the observed imbalance in surgical methods between groups, subgroup analyses were performed according to surgical approach. Categorical variables are expressed as number of cases (percentage) and were analysed using the chi-square test; Fisher’s exact test was applied when the expected frequency was less than 5, including for the comparison of surgical methods between groups. Missing data were minimal and were not imputed. For each analysis, percentages were calculated based on the number of available cases for the corresponding variable. Cases with missing values were excluded only from the specific analysis in which that variable was required, while other available data from these patients were retained. Therefore, the denominators may vary slightly across different analyses. A p value < 0.05 was considered statistically significant.
Results
Basic Information
A total of 60 patients with NSCLC were included in this study, providing 120 perioperative blood samples. Among them, 33 patients were assigned to the lung-first group (18 males and 15 females; median age, 61 years), and 27 patients to the lymph node-first group (10 males and 17 females; median age, 59 years). Most patients in both groups had stage I disease, with a small proportion of stage II cases. Lung adenocarcinoma was the predominant pathological subtype in both groups, followed by squamous cell carcinoma, and lesions included pure ground-glass, mixed ground-glass, and solid nodules. Summary data on CTC detection are presented in Supplementary Table 1. Among the 120 blood samples, CTCs were detected in 117 samples, with an overall detection rate of 97.5%.
As shown in Table 2, most baseline demographic and clinicopathological characteristics were comparable between the lung-first and lymph node-first groups. No significant differences were observed in sex, age, tumor location, tumor diameter, CTR, lesion type, serum tumor marker status, pathological subtype, degree of differentiation, clinical stage, pleural adhesion, lymphovascular invasion, operation time, postoperative hospital stay, or perioperative complications (all P > 0.05). However, the distribution of surgical methods differed significantly between the two groups (P = 0.047), with segmentectomy more common in the lymph node-first group and wedge resection performed only in the lung-first group. To minimize the potential confounding effect of wedge resection, a sensitivity analysis excluding wedge resection cases was performed. After exclusion, the perioperative difference in total CTC changes remained significant between the two surgical-sequence groups (P = 0.038). Postoperative CTC counts showed a decreasing trend in the lung-first group (median, 8 vs. 11 cells/5 mL; P = 0.075) and remained significantly increased in the lymph node-first group (median, 20 vs. 9 cells/5 mL; P < 0.001), suggesting that the main findings were not solely attributable to wedge resection cases (Supplementary Table 2).
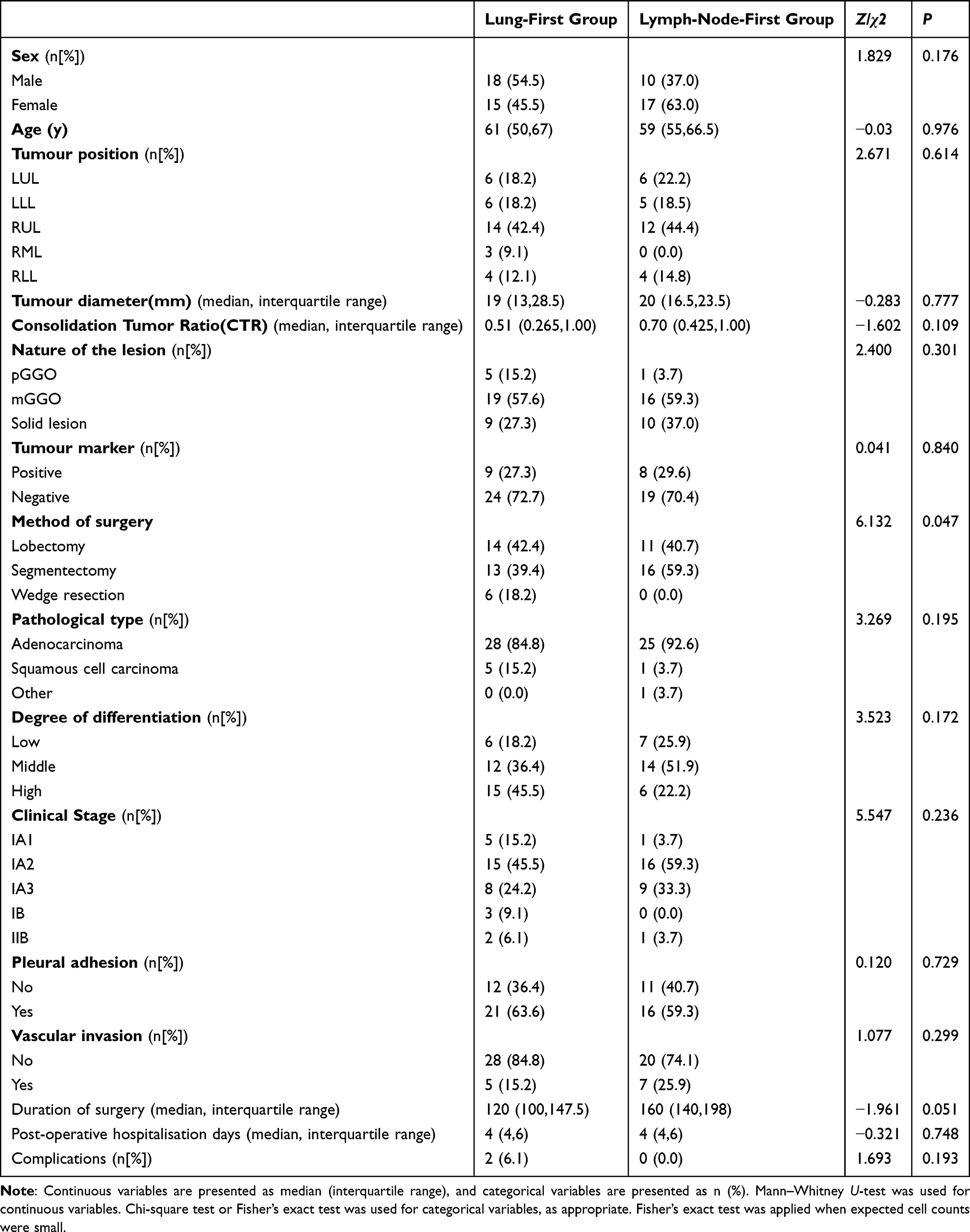 |
Table 2 Basic Information on Patients in the Lung-First Group and Patients in the Lymph-Node-First Group |
Relationship Between CTC Counts and Various Clinical Data
To explore the relationship between clinical characteristics and CTC counts before and after surgery in lung cancer patients, analyses were performed both within groups (preoperative vs. postoperative) and between groups.
The results of the within-group analysis are shown in Table 3. There was no significant association between clinical stage, lesion nature, or tumor differentiation and changes in CTC counts before and after surgery (P > 0.05). Regarding surgical methods, the postoperative CTC count in patients who underwent wedge resection was significantly lower than the preoperative level (median: 10.5 vs. 18 cells per 5 mL; P = 0.027). In the segmentectomy group, the postoperative CTC count showed a numerical increase compared with the preoperative level (median: 12 vs. 11 cells per 5 mL); however, this difference did not reach statistical significance (P = 0.066). No significant perioperative change was observed in the lobectomy group. In patients with pleural adhesions, the postoperative CTC count was significantly higher than the preoperative level (median: 12 vs. 11 cells per 5 mL; P = 0.038), whereas no significant change was observed in patients without pleural adhesions (P > 0.05). Similarly, in patients with vascular invasion, the postoperative CTC count was significantly higher than the preoperative level (median: 27 vs. 21 cells per 5 mL; P = 0.040), while no significant difference was found in patients without vascular invasion (P > 0.05).
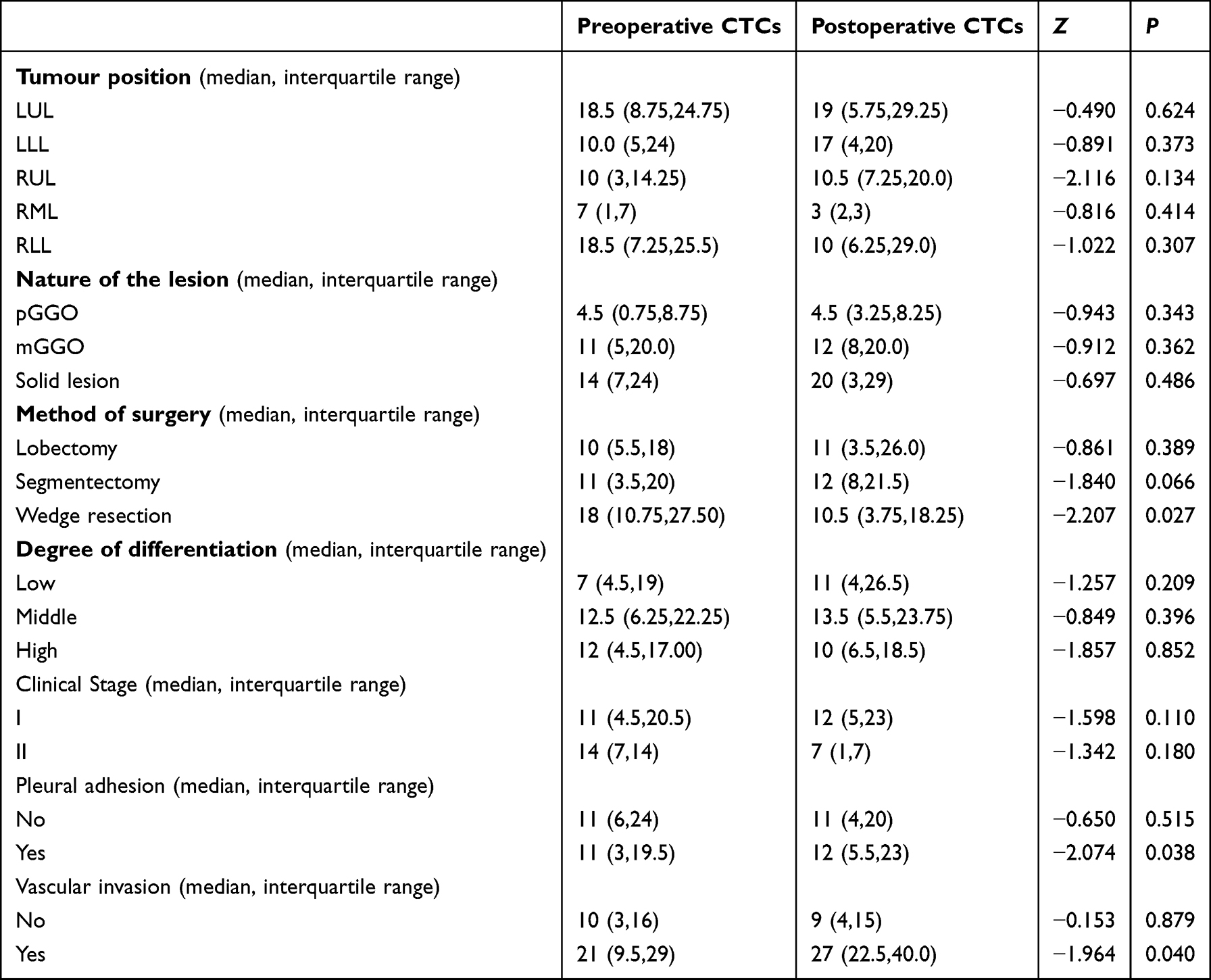 |
Table 3 Within-Group Comparison of Preoperative and Postoperative CTC Counts According to Clinicopathological Characteristics |
The results of the between-group analysis are shown in Table 4. There were no significant differences in preoperative or postoperative CTC counts according to tumor location, clinical stage, lesion nature, surgical method, tumor differentiation, or pleural adhesion (P > 0.05). In contrast, patients with vascular invasion had significantly higher CTC counts both before and after surgery compared with those without vascular invasion (P < 0.05).
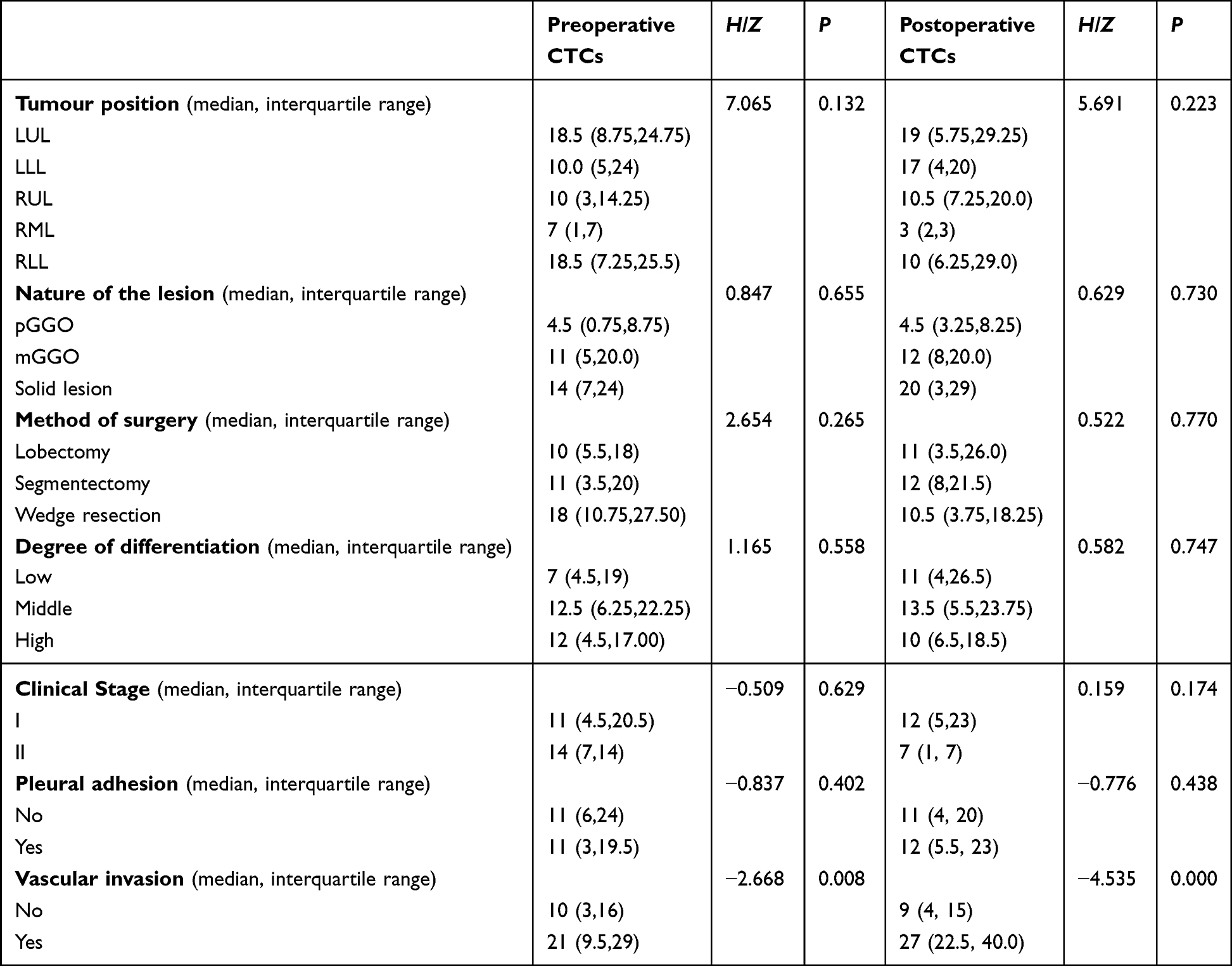 |
Table 4 Between-Group Comparison of CTC Counts According to Clinicopathological Characteristics |
Analysis of the Correlation Between CTCs and Some Clinical Data
The correlation analysis is shown in Table 5. The CTC counts before and after the surgery were not significantly correlated with tumor long diameter, degree of pleural adhesion, differentiation degree, or clinical stage (all P > 0.05), but were significantly positively correlated with vascular invasion and CTR (P < 0.05). Further subgroup analysis was performed in patients with sub-solid lesions, including pure ground-glass opacity lesions (pGGO, n = 6) and mixed ground-glass opacity lesions (mGGO, n = 35). When analysed as a combined subgroup, CTR was not significantly correlated with preoperative CTC counts but showed a significant positive correlation with postoperative CTC counts (r = 0.493, P = 0.003), and postoperative CTC levels increased with higher CTR (Supplementary Table 3). When analysed separately, no statistically significant correlation between CTR and CTC counts was observed within the pGGO subgroup, which may be related to the small sample size. In the mGGO subgroup, a similar positive trend between CTR and postoperative CTC counts was observed; however, the correlation did not reach statistical significance. These findings suggest that the overall association is mainly driven by the combined subgroup analysis.
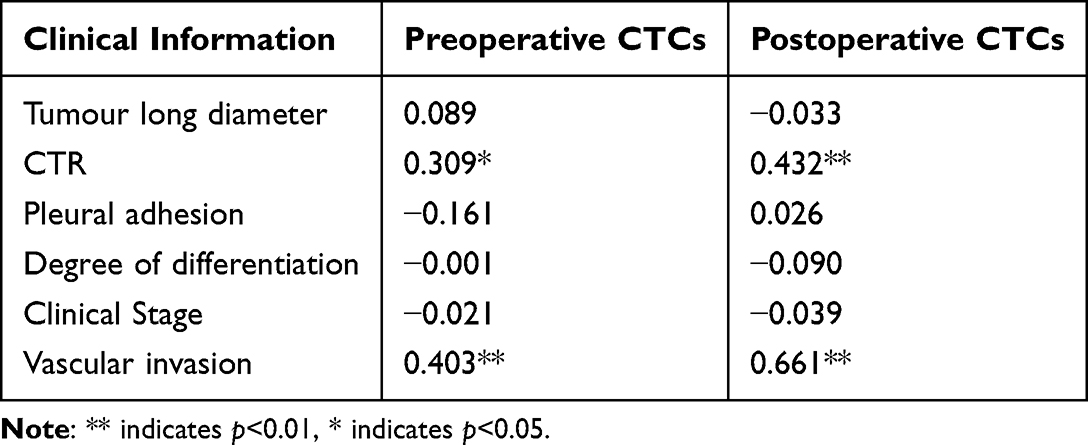 |
Table 5 Correlation Analysis of Selected Clinical Data with CTCs |
Effect of Surgery on CTCs
Effect of Surgery on the Number and Typing of CTCs
In 60 NSCLC patients, a total of 835 CTCs were detected preoperatively, including 483 epithelial CTCs, 340 mixed CTCs, and 10 mesenchymal CTCs; a total of 909 CTCs were detected postoperatively, including 555 epithelial CTCs, 350 mixed CTCs, and 4 mesenchymal CTCs (Supplementary Table 4). As summarized in Table 6, the median total CTC count was 11 per 5 mL both before and after surgery. The median counts for epithelial CTCs were 5 and 6 per 5 mL pre- and postoperatively, respectively, while those for hybrid CTCs remained at 3.5 per 5 mL. Mesenchymal CTCs were rarely detected (median 0 per 5 mL). Statistical analysis revealed no significant differences in the total number of CTCs or in the counts of each subtype between the preoperative and postoperative periods (all P > 0.05).
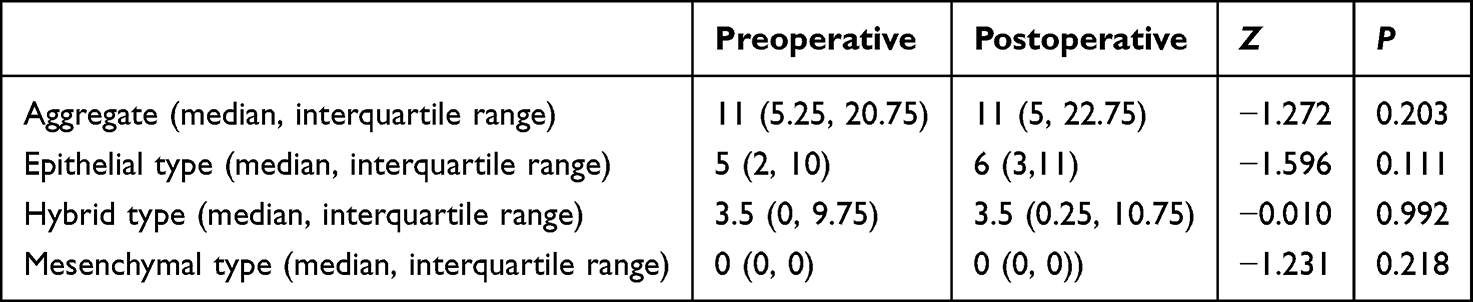 |
Table 6 Analysis of Changes in the Number and Typology of CTCs Preoperatively and Postoperatively |
Comparison of Differences in the Composition of CTCs Before and After Different Surgical Sequences
As shown in Table 7, in the lung-first group, the postoperative CTC count was significantly lower than the preoperative level (median: 9 vs. 13 per 5 mL; P = 0.007). In contrast, in the lymph node-priority group, the postoperative CTC count significantly increased compared with the preoperative value (median: 20 vs. 9 per 5 mL; P < 0.001). In addition, to further assess patient-level changes, the perioperative difference in CTC counts (ΔCTCs) was calculated. The lung-first group showed a decrease, whereas the lymph node-first group exhibited a marked increase, further supporting the differential impact of surgical sequence on tumor cell dissemination.
 |
Table 7 Changes in the Number of CTCs Before and After Different Operation Sequences |
As shown in Table 8, there was no significant difference in the composition of CTC subtypes between the preoperative lung-first group and the lymph node-first group (P > 0.05). However, postoperatively, the proportion of epithelial-type CTC in the lung-first group was higher than that in the lymph node-first group, while the proportion of mixed-type CTC was significantly lower in the lung-first group than in the lymph node-first group (P < 0.05).
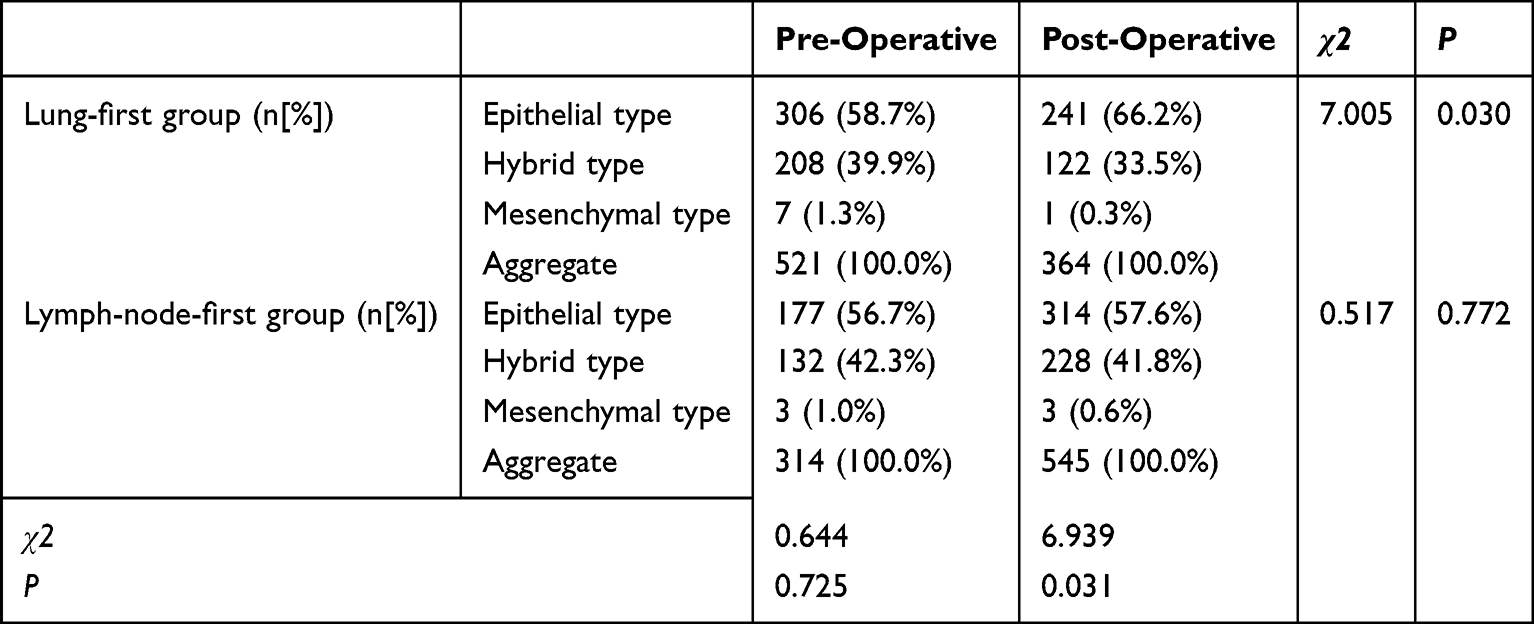 |
Table 8 Changes in the Percentage of CTCs and Typing Before and After Different Operation Sequences |
The intra-group analysis further revealed that in the lung-first group, the proportion of postoperative epithelial-type CTC significantly increased, while the proportion of mixed-type CTC decreased accordingly (P < 0.05). In contrast, in the lymph node-first group, no significant changes were observed in the CTC subtype composition during and after the operation.
Discussion
This study demonstrates that surgical sequence is associated with dynamic changes in circulating tumor cells (CTCs) during the perioperative period in NSCLC patients. In our cohort, prioritizing lung resection was associated with a reduction in postoperative CTC counts and a shift in CTC phenotype toward a higher proportion of epithelial-type cells, whereas prioritizing lymph node dissection was associated with an increase in postoperative CTC counts. These findings support the potential role of CTCs as a real-time biomarker for monitoring tumor cell dissemination during the perioperative period.
The incidence and mortality rates of lung cancer rank first among all malignant tumors,23 and it has become one of the major public health problems in China.3,24 Even if the tumor lesions can be completely removed through surgery, most patients will experience recurrence and metastasis, which may be related to the mutation of tumor cells and their survival selection.25
CTCs are tumor cells that detach from the primary lesion and enter the circulation. They are a key step in distant metastasis.12 CTCs are closely related to the clinical stage, postoperative recurrence, and long-term survival of lung cancer patients. They can serve as a relatively independent prognostic indicator26 and may influence the decision-making of adjuvant therapy.27 The CTC detection technology combined with low-dose CT scanning can improve the accuracy of lung cancer screening to a certain extent and has real-time monitoring capabilities.28 It is helpful for the early detection of tumor micrometastases and prognosis assessment, and plays an important role in individualized treatment and post-treatment efficacy monitoring. Therefore, it is necessary to consider the dynamic changes in the number of circulating CTCs as a new tumor monitoring indicator, and determine the risk of recurrence and metastasis of patients by detecting their high or low levels.29
It has been reported in the literature that the number of CTCs may vary depending on the disease stage of the patient. Li30 and Wei31 et al found that the count of CTCs would be higher in advanced lung cancer, but Hofman32 et al discovered that the count of CTCs was not correlated with the clinical stage or the pathological type of the tumor. In this study, we found that the count of CTCs in lung cancer patients increased as the clinical stage progressed; in terms of detection rate, the detection rate of CTCs in patients at stage II was also higher than that in patients at stage I, but the count or detection rate of CTCs in stage II patients was not correlated with that in stage I patients. However, there was no statistically significant difference between the count and detection rate of CTCs and the clinical stage of patients, indicating that there may be no correlation between the count of CTCs and the clinical stage. Regarding the correlation between the clinical stage of NSCLC patients and CTCs, there is currently no unified view, which may be due to differences in research methods, patient inclusion criteria, the time of CTC sample collection and detection techniques. These factors may be related to the methodological design of each study, patient inclusion criteria, the time of CTC sample collection and detection techniques, thereby resulting in differences in CTC detection results.
The surgical procedure is considered to be a potential factor that may cause tumor cells to transfer from the body to the circulatory system. Previous studies have shown that both open surgery and minimally invasive surgery may increase the release of CTCs during the perioperative period in patients with lung and other solid malignant tumors.33–35 Our research results indicate that in the lung-first resection group, postoperative CTCs were lower than those before the operation; in the lymph node-first resection group, postoperative CTCs were higher than those before the operation. This may suggest that, in NSCLC surgery, prioritizing resection of the target lung area where the tumor is located may reduce the possibility of CTCs entering the circulatory system. This strategy is more consistent with oncological principles. At the same time, in actual clinical practice, the choice of surgical sequence is influenced by multiple factors, including tumor location, anatomical exposure, pleural adhesions, operative difficulty, and surgeon judgment. Therefore, surgical sequence should be selected according to the specific intraoperative situation rather than applied as a fixed strategy in all patients. In addition, the imbalance in surgical methods between groups, such as the higher proportion of wedge resections in the lung-first group, may have independently influenced perioperative CTC dynamics. Therefore, the observed differences may not be solely attributable to surgical sequence, and the potential contribution of these confounding factors should be considered.
In addition to the number of cells, phenotypic heterogeneity is also increasingly regarded as having biological significance. Through EMT, cells may acquire stronger migration and invasion capabilities.36–38 Particularly, mixed-type cells, as previously studied, have been shown to be associated with higher metastasis efficiency and poor prognosis.39,40 In this study, the inter-group analysis revealed that the postoperative epithelial-type CTC proportion in the lung-first group was higher than that in the lymph node-first group, while the proportion of mixed-type CTC was lower than that in the lymph node-first group. The intra-group analysis showed that the postoperative epithelial-type CTC proportion in the lung-first group significantly increased, while the proportion of mixed-type CTC significantly decreased; while the proportions of each subtype of CTC in the lymph node-first group did not show significant changes before and after the surgery. This finding is consistent with that of Lin41 - external interference or stimulation may directly or indirectly promote the EMT process of CTCs, thereby causing changes in their subtype composition. This also suggests that compared with the lymph node-first resection surgery, the surgical sequence of prioritizing the resection of the target lung may bring greater benefits to patients.
Surgical approach may also influence perioperative tumor cell dissemination. In the present study, wedge resection was associated with a reduction in postoperative CTC counts, suggesting that limited tumor manipulation may help reduce surgery-related tumor cell release. This observation is biologically plausible and is consistent with the “no-touch isolation” principle, which emphasizes early vascular control and minimization of tumor manipulation to reduce intraoperative tumor cell dissemination. Similar concepts have been applied in several solid tumors and have been reported to reduce hematogenous tumor cell spread.42–49 However, this finding should be interpreted cautiously because the number of wedge resection cases was limited, wedge resection was performed only in the lung-first group, and no significant overall difference in CTC counts was observed among different surgical methods. Although sensitivity analysis was performed to reduce the potential confounding effect of wedge resection, the non-randomized design and imbalance in surgical methods preclude definitive conclusions regarding the independent effect of surgical approach. Further studies with larger sample sizes, balanced surgical subgroups, and long-term follow-up are needed to determine whether specific surgical strategies can reduce perioperative tumor dissemination and improve oncological outcomes. This interpretation is consistent with the findings reported by Yasukawa et al.50
Pleural adhesions also seem to affect the dynamic changes of CTCs during the perioperative period. Adhesions increase the complexity of the surgery and may require more complex tissue handling, which may promote the spread of tumor cells.51 The data from this study show that the postoperative count of CTCs in patients with pleural adhesions is significantly higher than that before the surgery; while there is no significant difference in the pre- and post-operative CTC counts in patients without pleural adhesions, suggesting that the presence of pleural adhesions may promote the dissemination of tumors to the circulatory system.
Lymphatic vessel invasion (LVI) is a well-established pathway for tumor spread and is associated with recurrence and poor prognosis in NSCLC.52,53 In this study, patients with LVI had significantly higher levels of CTCs in the perioperative period compared to before surgery, and patients with vascular invasion had higher CTC counts after surgery than those without vascular invasion. This supports the view that vascular invasion facilitates the entry of tumor cells into the bloodstream and increases the susceptibility to intraoperative spread.
Radiological characteristics also showed an association with CTC dynamics. The consolidation-to-tumor ratio (CTR), which reflects tumor invasiveness,54,55 was positively correlated with postoperative CTC levels, particularly in patients with sub-solid lesions (Supplementary Table 2). This finding is consistent with evidence indicating that tumors with a higher solid component have stronger invasive potential.56 However, subgroup analyses of pGGO and mGGO lesions should be interpreted with caution due to the limited sample size, especially in the pGGO subgroup. Interestingly, elevated CTC levels were observed in some patients with early ground-glass-like lesions, suggesting that hematogenous dissemination may occur even in early-stage disease.57
Several limitations should be considered. First, this was a single-center study with a relatively small sample size, and most patients were in stage I, which may limit statistical power, particularly in subgroup analyses. As a result, non-significant findings should be interpreted with caution, as they may reflect insufficient power rather than a true absence of association. Second, the study was not randomized. The choice of surgical sequence was based on preoperative imaging, intraoperative conditions, and surgeon judgment, which may introduce selection bias. In addition, there were imbalances in surgical methods between groups, which may act as potential confounding factors and cannot be fully accounted for in the current analysis. Third, central venous blood was used for CTC detection to ensure consistency in perioperative sampling and to better reflect tumor cell release during surgical manipulation. However, differences between central and peripheral blood sampling may influence CTC measurements, which represents a potential source of bias. Fourth, the CTC detection method used in this study is based on size-dependent filtration and may miss smaller tumor cells, which could affect the accuracy of CTC quantification. Fifth, long-term follow-up data are not yet available. Therefore, the relationship between perioperative CTC changes and clinical outcomes, including recurrence and survival, cannot be determined. Finally, given the exploratory nature of the study and the relatively small sample size, no formal adjustment for multiple comparisons was applied. Accordingly, the findings should be interpreted as hypothesis-generating, and further validation in larger, well-designed prospective studies is required.
Conclusion
Perioperative CTC dynamics in patients with resectable NSCLC were associated with clinicopathological characteristics and surgical factors. Prioritizing lung tumor resection before lymph node dissection was associated with lower postoperative CTC counts and a more favorable CTC phenotype. However, given the non-randomized design, limited sample size, and potential confounding factors, particularly the imbalance in surgical methods, these findings should be interpreted cautiously. Surgical sequence should be individualized according to patient characteristics and intraoperative conditions. These preliminary findings generate the hypothesis that prioritizing lung tumor resection before lymph node dissection may help minimize perioperative tumor cell dissemination, a concept that requires further validation in larger prospective randomized studies with long-term follow-up.
Abbreviations
CTCs, Circulating tumor cells; NSCLC, Non-small cell lung cancer; SCLC, Small cell lung cancer; EpCAM, Epithelial cell adhesion molecule; FISH, Fluorescence in situ hybridization; mRNA, Messenger RNA; EMT, Epithelial-mesenchymal transition; E-cad, E-cadherin; CEA, Carcino-embryonic antigen; CA125, Carbohydrate antigen; RT-PCR, Real time-polymerase chain reaction; VATS, Video-assisted thoracoscopic surgery; DFS, Disease-free survival; OS, Overall survival; RFS, Recurrence-free survival; AJCC, American Joint Committee on Cancer; LVI, lymphovascular invasion; LN, lymph node; CTM, circulating tumor microemboli; CTR, consolidation-to-tumor ratio.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author Guowen Zou ([email protected]) on reasonable request. This study was registered in the ISRCTN registry (The UK’s Clinical Study Registry) under the registration number ISRCTN17981262.
Ethical Statement
This study was conducted in accordance with the revised Helsinki Declaration and was approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University (Approval Number: IIT [2023] No. 267).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by grants from the National Key R&D Program of China (No. 2023YFC2508604).
Disclosure
The authors declare that they have no competing interests.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–16. doi:10.3322/caac.21660
2. Santucci C, Carioli G, Bertuccio P, et al. Progress in cancer mortality, incidence, and survival: a global overview. Eur J Cancer Prev. 2020;29(5):367–381. doi:10.1097/CEJ.0000000000000594
3. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
4. Zeng H, Chen W, Zheng R, et al. Changing cancer survival in China during 2003–15: a pooled analysis of 17 population-based cancer registries. Lancet Glob Health. 2018;6(5):e555–e567. doi:10.1016/S2214-109X(18)30127-X
5. Gabriel MT, Calleja LR, Chalopin A, Ory B, Heymann D. Circulating Tumor Cells: a Review of Non–EpCAM-Based Approaches for Cell Enrichment and Isolation. Clin Chem. 2016;62(4):571–581. doi:10.1373/clinchem.2015.249706
6. Asamura H, Nishimura KK, Giroux DJ, et al. IASLC lung cancer staging project: the new database to inform revisions in the ninth edition of the TNM classification of lung cancer. J Thorac Oncol. 2023;18(5):564–575. doi:10.1016/j.jtho.2023.01.088
7. Bhatti I, Patel M, Dennison AR, Thomas MW, Garcea G. Utility of postoperative CEA for surveillance of recurrence after resection of primary colorectal cancer. Int J Surg. 2015;16(Pt A):123–128. doi:10.1016/j.ijsu.2015.03.002
8. Margonis GA, Gani F, Buettner S, et al. Rates and patterns of recurrence after curative intent resection for gallbladder cancer: a multi-institution analysis from the US extra-hepatic biliary malignancy consortium. HPB. 2016;18(11):872–878. doi:10.1016/j.hpb.2016.05.016
9. Deng XF, Jiang L, Liu QX, et al. Lymph node micrometastases are associated with disease recurrence and poor survival for early-stage non-small cell lung cancer patients: a meta-analysis. J Cardiothorac Surg. 2016;11(1):28. doi:10.1186/s13019-016-0427-x
10. Lawrence R, Watters M, Davies CR, Pantel K, Lu Y-J. Circulating tumour cells for early detection of clinically relevant cancer. Nat Rev Clin Oncol. 2023;20(7):487–500. doi:10.1038/s41571-023-00781-y
11. Wu H, Wang Q, Liu Q, et al. The serum tumor markers in combination for clinical diagnosis of lung cancer. Clin Lab. 2020;66(03/2020). doi:10.7754/Clin.Lab.2019.190533
12. Boya M, Chu CH, Liu R, Ozkaya-Ahmadov T, Sarioglu AF. Circulating tumor cell enrichment technologies. Recent Results Cancer Res. 2020;215:25–55.
13. Gurzu S, Kobori L, Fodor D, Jung I. Epithelial mesenchymal and endothelial mesenchymal transitions in hepatocellular carcinoma: a review. Biomed Res Int. 2019;2019:2962580. doi:10.1155/2019/2962580
14. Dong S, Liang S, Cheng Z, et al. ROS/PI3K/Akt and Wnt/β-catenin signalings activate HIF-1α-induced metabolic reprogramming to impart 5-fluorouracil resistance in colorectal cancer. J Exp Clin Cancer Res. 2022;41(1):15. doi:10.1186/s13046-021-02229-6
15. Andergassen U, Kolbl AC, Mahner S, Jeschke U. Real-time RT-PCR systems for CTC detection from blood samples of breast cancer and gynaecological tumour patients. Oncol Rep. 2016;35(4):1905–1915. doi:10.3892/or.2016.4608
16. Cabel L, Proudhon C, Gortais H, et al. Circulating tumor cells: clinical validity and utility. Int J Clin Oncol. 2017;22(3):421–430. doi:10.1007/s10147-017-1105-2
17. Abdalla TSA, Meiners J, Riethdorf S, et al. Prognostic value of preoperative circulating tumor cells counts in patients with UICC stage I-IV colorectal cancer. PLoS One. 2021;16(6):e0252897. doi:10.1371/journal.pone.0252897
18. Hashimoto M, Tanaka F, Yoneda K, et al. Significant increase in circulating tumour cells in pulmonary venous blood during surgical manipulation in patients with primary lung cancer. Interact Cardiovasc Thorac Surg. 2014;18(6):775–783. doi:10.1093/icvts/ivu048
19. Gonvers S, Tabrizian P, Melloul E, et al. Is liquid biopsy the future commutator of decision-making in liver transplantation for hepatocellular carcinoma? Front Oncol. 2022;12:940473. doi:10.3389/fonc.2022.940473
20. Costa C, Muinelo-Romay L, Cebey-Lopez V, et al. Analysis of a real-world cohort of metastatic breast cancer patients shows circulating tumor cell clusters (CTC-clusters) as predictors of patient outcomes. Cancers. 2020;12(5):1111. doi:10.3390/cancers12051111
21. Zarour LR, Anand S, Billingsley KG, et al. Colorectal cancer liver metastasis: evolving paradigms and future directions. Cell Mol Gastroenterol Hepatol. 2017;3(2):163–173. doi:10.1016/j.jcmgh.2017.01.006
22. Banys-Paluchowski M, Witzel I, Riethdorf S, et al. The clinical relevance of serum vascular endothelial growth factor (VEGF) in correlation to circulating tumor cells and other serum biomarkers in patients with metastatic breast cancer. Breast Cancer Res Treat. 2018;172(1):93–104. doi:10.1007/s10549-018-4882-z
23. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J. 2022;135(5):584–590. doi:10.1097/CM9.0000000000002108
24. Feng R-M, Zong Y-N, Cao S-M, Xu R-H. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics? Cancer Commun. 2019;39(1):22. doi:10.1186/s40880-019-0368-6
25. Lee S-Y, Chae D-K, An J, et al. Combinatory analysis of cell-free and circulating tumor cell DNAs provides more variants for cancer treatment. Anticancer Res. 2019;39(12):6595–6602. doi:10.21873/anticanres.13875
26. Lindsay CR, Faugeroux V, Michiels S, et al. A prospective examination of circulating tumor cell profiles in non-small-cell lung cancer molecular subgroups. Ann Oncol. 2017;28(7):1523–1531. doi:10.1093/annonc/mdx156
27. Markou A, Tzanikou E, Lianidou E. The potential of liquid biopsy in the management of cancer patients. Semin Cancer Biol. 2022;84:69–79. doi:10.1016/j.semcancer.2022.03.013
28. Manjunath Y, Upparahalli SV, Suvilesh KN, et al. Circulating tumor cell clusters are a potential biomarker for detection of non-small cell lung cancer. Lung Cancer. 2019;134:147–150. doi:10.1016/j.lungcan.2019.06.016
29. Li W, Liu J-B, Hou L-K, et al. Liquid biopsy in lung cancer: significance in diagnostics, prediction, and treatment monitoring. Mol Cancer. 2022;21(1):25. doi:10.1186/s12943-022-01505-z
30. Li J. Significance of circulating tumor cells in nonsmall-cell lung cancer patients: prognosis, chemotherapy efficacy, and survival. J Healthc Eng. 2021;2021:2680526. doi:10.1155/2021/2680526
31. Wei T, Zhu D, Yang Y, Yuan G, Xie H, Shen R. The application of nano-enrichment in CTC detection and the clinical significance of CTCs in non-small cell lung cancer (NSCLC) treatment. PLoS One. 2019;14(7):e0219129. doi:10.1371/journal.pone.0219129
32. Hofman V, Ilie MI, Long E, et al. Detection of circulating tumor cells as a prognostic factor in patients undergoing radical surgery for non-small-cell lung carcinoma: comparison of the efficacy of the CellSearch Assay™ and the isolation by size of epithelial tumor cell method. Int J Cancer. 2011;129(7):1651–1660. doi:10.1002/ijc.25819
33. Duan X, Zhu Y, Cui Y, et al. Circulating tumor cells in the pulmonary vein increase significantly after lobectomy: a prospective observational study. Thorac Cancer. 2019;10(2):163–169. doi:10.1111/1759-7714.12925
34. Lv C, Zhao B, Wang L, et al. Detection of circulating tumor cells in pulmonary venous blood for resectable non-small cell lung cancer. Oncol Lett. 2018;15(1):1103–1112. doi:10.3892/ol.2017.7405
35. Murlidhar V, Reddy RM, Fouladdel S, et al. Poor prognosis indicated by venous circulating tumor cell clusters in early-stage lung cancers. Cancer Res. 2017;77(18):5194–5206. doi:10.1158/0008-5472.CAN-16-2072
36. Gui Y, Khan MGM, Bobbala D, et al. Attenuation of MET-mediated migration and invasion in hepatocellular carcinoma cells by SOCS1. World J Gastroenterol. 2017;23(36):6639–6649. doi:10.3748/wjg.v23.i36.6639
37. Buscail E, Chiche L, Laurent C, et al. Tumor-proximal liquid biopsy to improve diagnostic and prognostic performances of circulating tumor cells. Mol Oncol. 2019;13(9):1811–1826. doi:10.1002/1878-0261.12534
38. Debnath P, Huirem RS, Dutta P, Palchaudhuri S. Epithelial–mesenchymal transition and its transcription factors. Biosci Rep. 2022;42(1). doi:10.1042/BSR20211754
39. Wu J-S, Jiang J, Chen B-J, Wang K, Tang Y-L, Liang X-H. Plasticity of cancer cell invasion: patterns and mechanisms. Transl Oncol. 2021;14(1):100899. doi:10.1016/j.tranon.2020.100899
40. Dong J, Zhu D, Tang X, et al. Detection of circulating tumor cell molecular subtype in pulmonary vein predicting prognosis of stage I–III non-small cell lung cancer patients. Front Oncol. 2019;9:1139. doi:10.3389/fonc.2019.01139
41. Lin D, Shen L, Luo M, et al. Circulating tumor cells: biology and clinical significance. Signal Transduct Target Ther. 2021;6(1):404. doi:10.1038/s41392-021-00817-8
42. Alix-Panabieres C, Pantel K. Challenges in circulating tumour cell research. Nat Rev Cancer. 2014;14(9):623–631. doi:10.1038/nrc3820
43. Sales J-P, Wind P, Douard R, Cugnenc P-H, Loric S. Blood dissemination of colonic epithelial cells during no-touch surgery for rectosigmoid cancer. Lancet. 1999;354(9176):392. doi:10.1016/S0140-6736(99)92164-5
44. Gall TMH, Jacob J, Frampton AE, et al. Reduced dissemination of circulating tumor cells with no-touch isolation surgical technique in patients with pancreatic cancer. JAMA Surg. 2014;149(5):482–485. doi:10.1001/jamasurg.2013.3643
45. Lee J-M, Lee K-W, Kim H-C, Yi N-J, Suh K-S. No touch isolation technique for the prevention of postoperative recurrence of hepatocellular carcinoma after liver transplantation-combined with trans-arterial radioembolization. Surg Oncol. 2020;35:189–190. doi:10.1016/j.suronc.2020.08.024
46. Li Y, Xu KS, Li JS, et al. The research of no-touch isolation technique on the prevention of postoperative recurrence and metastasis of hepatocellular carcinoma after hepatectomy. Hepatogastroenterology. 2014;61(131):784–791.
47. Sznurkowski JJ. En bloc pelvic resection for advanced ovarian cancer preceded by central ligation of vessels supplying the tumor bed: a description of surgical technique and a feasibility study. World J Surg Oncol. 2016;14(1):133. doi:10.1186/s12957-016-0894-5
48. Yasukawa M, Sawabata N, Kawaguchi T, Taniguchi S. Effectiveness of intraoperative pulmonary wedge resection of tumor site before lobectomy for early lung adenocarcinoma. Anticancer Res. 2019;39(12):6829–6834. doi:10.21873/anticanres.13899
49. Kitagawa H, Tajima H, Nakagawara H, et al. A modification of radical antegrade modular pancreatosplenectomy for adenocarcinoma of the left pancreas: significance of en bloc resection including the anterior renal fascia. World J Surg. 2014;38(9):2448–2454. doi:10.1007/s00268-014-2572-5
50. Yasukawa M, Sawabata N, Kawaguchi T, Taniguchi S. Wedge resection of tumor before lobectomy for lung cancer could be a no-touch isolation technique. In Vivo. 2020;34(2):779–785. doi:10.21873/invivo.11838
51. Kouritas VK, Kefaloyannis E, Tcherveniakov P, et al. Do pleural adhesions influence the outcome of patients undergoing major lung resection?†. Interact Cardiovasc Thorac Surg. 2017;25(4):613–619. doi:10.1093/icvts/ivx173
52. Li P, He H-Q, Zhu C-M, et al. The prognostic significance of lymphovascular invasion in patients with resectable gastric cancer: a large retrospective study from Southern China. BMC Cancer. 2015;15(1):370. doi:10.1186/s12885-015-1370-2
53. Mei D, Zhao B, Zhang J, et al. Impact of lymphovascular invasion on survival outcome in patients with gastric cancer. Am J Clin Pathol. 2020;153(6):833–841. doi:10.1093/ajcp/aqaa021
54. Hansell DM, Bankier AA, MacMahon H, McLoud TC, Muller NL, Remy J. Fleischner society: glossary of terms for thoracic imaging. Radiology. 2008;246(3):697–722. doi:10.1148/radiol.2462070712
55. Moon Y, Sung SW, Lee KY, Park JK. Clinicopathological characteristics and prognosis of non-lepidic invasive adenocarcinoma presenting as ground glass opacity nodule. J Thorac Dis. 2016;8(9):2562–2570. doi:10.21037/jtd.2016.08.46
56. Xing X, Yang F, Huang Q, et al. Decoding the multicellular ecosystem of lung adenocarcinoma manifested as pulmonary subsolid nodules by single-cell RNA sequencing. Sci Adv. 2021;7(5). doi:10.1126/sciadv.abd9738
57. Kongsgaard A, Boye K, Fodstad Ø, et al. Detection of disseminated tumor cells in lymph nodes from patients with early stage non-small cell lung cancer. Diagn Pathol. 2016;11(1):50. doi:10.1186/s13000-016-0504-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comprehensive Genomic Profiling Identifies FAT1 as a Negative Regulator of EMT, CTCs, and Metastasis of Hepatocellular Carcinoma
Huang ZL, Zhang PB, Zhang JT, Li F, Li TT, Huang XY
Journal of Hepatocellular Carcinoma 2023, 10:369-382
Published Date: 7 March 2023