Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Analysis of Determinants Based on the Health Belief Model: A Study Predicting Cognitive Impairment Among Community-Dwelling Older Adults in China
Authors Zhu Q, Xia J, Wang Q, Bai L, Shen C, Yang Y
Received 20 October 2025
Accepted for publication 15 January 2026
Published 22 January 2026 Volume 2026:19 568925
DOI https://doi.org/10.2147/JMDH.S568925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Veronica Swallow
Qingjiao Zhu,1,2,* Jinjing Xia,3,* Qing Wang,2 Lu Bai,4 Chunxian Shen,5 Ying Yang6
1School of Nursing, Jinzhou Medical University, Jinzhou, 121001, People’s Republic of China; 2Department One of Gynecology, Suizhou Hospital, Hubei University of Medicine (Suizhou Central Hospital), Suizhou, 441300, People’s Republic of China; 3Operating Room, Department of Anesthesiology and Perioperative Medicine, Suizhou Hospital, Hubei University of Medicine (Suizhou Central Hospital), Suizhou, 441300, People’s Republic of China; 4Department of Medical Aesthetics, Suizhou Hospital, Hubei University of Medicine (Suizhou Central Hospital), Suizhou, 441300, People’s Republic of China; 5Department of Infectious Diseases, Suizhou Hospital, Hubei University of Medicine (Suizhou Central Hospital), Suizhou, 441300, People’s Republic of China; 6Department of Rehabilitation Business, The Second Hospital of Huangshi City, Huangshi, 435002, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Yang, Department of Rehabilitation Business, The Second Hospital of Huangshi City, No. 102, Qingshanqiao, Huangshigang District, Huangshi, Hubei, 435002, People’s Republic of China, Email [email protected]
Introduction: To investigate the predictive value of psychosocial factors and the Health Belief Model (HBM) for cognitive impairment in community-dwelling older adults, develop a combined prediction model, analyze the mechanistic pathways linking social support, loneliness, and self-efficacy, and evaluate the efficacy of nursing interventions guided by the integrated HBM framework.
Methods: A single-center cross-sectional observational survey enrolled 158 older adults from a community. Participants were categorized into cognitively normal and cognitive impairment groups based on cognitive status. Data collected included demographics, HBM constructs (perceived susceptibility, severity, benefits, barriers, cues to action, and self-efficacy), and psychosocial factors (social support, loneliness). Multivariable logistic regression identified determinants of cognitive impairment. ROC curves assessed the predictive model’s performance, and mediation analysis explored pathways through which psychosocial factors and self-efficacy influence cognitive impairment.
Results: Multivariable analysis identified age, hypertension, perceived barriers, and loneliness as risk factors for cognitive impairment, while educational attainment, exercise ≥ 3 times/week, self-efficacy, and social support as protective factors (P < 0.05). The combined model demonstrated superior predictive accuracy (AUC = 0.951) to single-factor models. Mediation analysis revealed that social support and loneliness primarily exerted direct effects on cognitive impairment, though the mediating role of self-efficacy did not reach statistical significance.
Conclusion: Social support and self-efficacy are significant protective factors against cognitive impairment in community-dwelling older adults, whereas loneliness and perceived barriers are risk factors. A prediction model integrating HBM and psychosocial factors enhances early screening efficacy for community-based cognitive impairment. Nursing interventions leveraging the synergistic HBM framework warrant broader community implementation.
Keywords: cognitive impairment, health belief model, social support, loneliness, SELF-efficacy, combined prediction model
Introduction
The accelerating global aging population has led to a significant increase in the prevalence of cognitive impairment, particularly dementia such as Alzheimer’s disease, establishing it as a major public health challenge impacting the health and quality of life of older adults. According to the World Health Organization (WHO) statistics, approximately 10 million new dementia cases occur globally each year, with projections indicating that the global number of people living with dementia will reach 152 million by 2050.1 China, home to the world’s largest elderly population, is experiencing a rising trend in the incidence of cognitive impairment among community-dwelling older adults. Relevant research indicates a prevalence of cognitive impairment reaching 44.04% among individuals aged 60 years and above in China.2 Cognitive impairment not only diminishes the self-care capacity of older adults, increasing burdens on families and society, but also significantly elevates the risk of depression, anxiety, falls, and complications from other chronic conditions.3,4 Consequently, the early identification of high-risk individuals for cognitive impairment at the community level, alongside the development of scientifically robust diagnostic models and the implementation of effective interventions, has become a critical focus within clinical and public health domains.
Current approaches to screening and intervention for cognitive impairment in community settings often face challenges such as delayed initiation, low screening rates, and poor adherence. Singular medical or social intervention models have proven inadequate for achieving optimal outcomes. In recent years, the Health Belief Model (HBM) and social cognitive theory have emerged as significant theoretical foundations for research into cognitive impairment interventions.5–7 Substantial evidence suggests that psychosocial factors, including social support, loneliness, and self-efficacy, not only directly influence the health behaviors and cognitive function of older adults but may also impact the onset and progression of cognitive impairment through mediating mechanisms.8–11
Concurrently, traditional risk prediction for cognitive impairment has predominantly relied on singular clinical or epidemiological indicators, resulting in limited predictive efficacy. Recently, the construction of multifactorial prediction models incorporating multidimensional physiological, psychological, and social factors has become a research priority, demonstrating potential for significantly enhancing the accuracy of early cognitive impairment identification. Nevertheless, most existing Chinese prediction models emphasize demographic and medical variables, with relatively limited incorporation of health belief constructs or psychosocial pathways within a unified theoretical framework. Furthermore, interventions targeting high-risk populations based on the HBM hold promise for improving health behaviors and slowing cognitive decline in older adults. Relevant studies demonstrate that strengthening self-efficacy, enhancing social support, and reducing loneliness may contribute to lowering the risk of cognitive impairment, although the precise pathways of these mechanisms remain incompletely elucidated.12,13
Against this backdrop, the present study aimed to develop and evaluate a focused prediction model for cognitive impairment among Chinese community-dwelling older adults based on the Health Belief Model (HBM). Using a cross-sectional design, we integrated demographic factors, core HBM constructs, and key psychosocial variables, including social support and loneliness, to identify determinants of cognitive impairment and construct a multifactorial predictive model. In addition, we explored potential mediating pathways linking health beliefs, psychosocial factors, and cognitive impairment.
Unlike prior Chinese prediction models that have primarily relied on epidemiologic or isolated psychosocial factors, the present study uniquely incorporates HBM constructs and psychosocial variables within a unified theoretical and predictive framework. This approach addresses a key gap in existing research by linking health beliefs, social context, and cognitive outcomes simultaneously, rather than examining these dimensions independently.
Materials and Methods
Study Design
This study employed a single-center cross-sectional survey observational survey to systematically investigate the factors influencing cognitive impairment in community-dwelling older adults and to construct a prediction model based on the HBM. The study protocol received approval from the Ethics Committee of Suizhou Central Hospital (No. KY-2025-22-01), and written informed consent was obtained from all participants. All data were anonymized prior to analysis, strictly adhering to the Declaration of Helsinki and local ethical regulations to ensure participant privacy and data security.
Participants were included if they met the following criteria: (1) aged 60 years or older; (2) continuous residence in the study community for at least 6 months; (3) ability to complete questionnaires and cognitive assessments independently or with minimal assistance; and (4) voluntary participation with signed informed consent.
Participants were excluded based on any of the following criteria: (1) a prior diagnosis of severe psychiatric disorders (eg, schizophrenia, major depressive disorder); (2) a prior diagnosis of Alzheimer’s disease or other severe neurodegenerative disorders; (3) severe hearing or visual impairment precluding completion of questionnaires or cognitive assessments; (4) concurrent severe acute physical illness that could compromise the accuracy of cognitive assessment; or (5) current participation in other clinical research related to cognitive impairment.
Study Setting and Participants
The study was conducted in a single urban community, China. Community-dwelling older adults aged 60 years and above were invited to participate through community health service centers. Participants were recruited using a convenience sampling strategy based on voluntary participation during routine community health activities. As this was a single-community, single-center study, the sample may not be fully representative of the broader older adult population. Therefore, the generalizability of the findings should be interpreted with caution.
Data Collection and Quality Control
All research personnel underwent standardized training prior to data collection to ensure consistency in questionnaire administration and cognitive assessment procedures. A pilot study was conducted to test the feasibility and comprehensibility of the instruments before the formal survey commenced. During the formal data collection phase, on-site research coordinators monitored the process in real-time to verify data quality. Data entry was performed via dual independent entry, with any discrepancies identified promptly resolved through verification against source documents. Completed paper questionnaires were assigned unique identification numbers, sealed, and securely archived. Electronic data were managed using a password-protected and encrypted electronic data capture (EDC) system, with regular backups implemented and strict access permissions enforced.
Variable Definitions
The primary outcome variable was cognitive impairment, determined based on predefined clinical diagnostic criteria during the survey visit. All enrolled participants underwent face-to-face cognitive assessments conducted by uniformly trained personnel. Cognitive impairment was diagnosed based on comprehensive clinical evaluation conducted by trained clinicians during the survey visit. The diagnostic criteria incorporated: (1) cognitive complaints reported by participants or their caregivers; (2) observable deficits in cognitive domains during face-to-face assessment, including orientation, attention, memory, and executive functioning; and (3) evidence of impaired daily functioning attributable to cognitive decline. Participants were classified as having cognitive impairment if the clinicians determined that cognitive deficits were present and interfered with normal daily activities, or if a prior clinical diagnosis of cognitive impairment or dementia was documented in the medical records.
Primary predictor variables encompassed several domains: demographic characteristics (age, sex, educational attainment, marital status, income level, and living alone), history of chronic diseases (hypertension, diabetes mellitus, coronary heart disease, stroke, and depression), lifestyle factors (smoking status, alcohol consumption, exercise frequency, sleep duration, and dietary diversity), psychosocial factors [social support measured by the Social Support Rating Scale (SSRS), loneliness assessed by the University of California, Los Angeles Loneliness Scale (UCLA-LS), and life satisfaction], and HBM dimensions (perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy). All HBM dimensions were assessed using the validated Chinese version of the HBM scale, employing a 5-point Likert scale for scoring. Missing data for key variables were addressed using multiple imputation (MI), with sensitivity analyses performed to evaluate the robustness of the imputation approach.
Measurement Instruments
Health beliefs were evaluated using a validated Chinese version of the HBM questionnaire. This instrument measured six core dimensions: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy, utilizing a 5-point Likert scale for responses.
Social support was measured with the SSRS. This 10-item instrument comprised three subscales: subjective support (reflecting perceived emotional support), objective support (indicating tangible assistance received), and support utilization (assessing the individual’s active use of available support resources). Items were scored on a graded scale, yielding a total score ranging from 12 to 66, with higher scores denoting greater perceived social support. The SSRS demonstrated good internal consistency in this study (Cronbach’s α = 0.82).
Subjective loneliness was assessed using the 20-item UCLA-LS, version 3. Participants rated the frequency of their loneliness experiences on a 4-point Likert scale (1 = never, 4 = often), resulting in a total score between 20 and 80. Higher scores indicated greater loneliness severity. This scale encompassed facets such as perceived deficits in social connectedness and the intensity of loneliness experiences, demonstrating established construct and content validity. The UCLA-LS typically exhibited high internal consistency (Cronbach’s α > 0.89), confirming its robust psychometric properties.
Statistical Analysis
Statistical analyses were performed using [SPSS 26.0/R 4.5.2]. Continuous variables are presented as means and standard deviations or medians and interquartile ranges, and categorical variables as frequencies and percentages; group comparisons used independent-samples t tests or Mann–Whitney U-tests for continuous variables and chi-square tests for categorical variables. Univariate analyses were conducted to identify factors associated with cognitive impairment (P<0.05), followed by multivariable logistic regression including predictors selected based on theoretical relevance and univariate results; multicollinearity was assessed using variance inflation factors (VIF<5). Given the modest number of outcome events, the potential risk of overfitting was acknowledged, and model stability was evaluated using bootstrap resampling with 1,000 iterations; model discrimination was assessed using the area under the receiver operating characteristic curve (AUC), and model calibration using calibration-in-the-large and the calibration slope. Mediation analyses were conducted as exploratory and hypothesis-generating; because the data were cross-sectional, temporal ordering and causal inference could not be established. All tests were two-sided, and a p value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
Significant differences (P < 0.05) were observed between the cognitive impairment group and the cognitively normal group regarding age, educational attainment, hypertension prevalence, sleep duration, and weekly exercise frequency. Specifically, participants in the cognitive impairment group were significantly older than those in the cognitively normal group [median age 79 years (interquartile range, IQR: 71, 86) vs 70 years (IQR: 65, 79); P = 0.001]. Educational attainment also differed significantly: the cognitive impairment group exhibited a higher proportion of individuals with junior high school education (45.10% vs 20.56%) and a lower proportion of illiterate individuals (25.49% vs 47.66%; P = 0.003). Hypertension was more prevalent in the cognitive impairment group (60.78% vs 41.03%; P = 0.003). Concerning sleep duration, a significantly higher proportion of participants in the cognitive impairment group reported sleeping less than 6 hours per night compared to the cognitively normal group (54.90% vs 33.64%; P = 0.039). Furthermore, the proportion of individuals engaging in exercise at least three times per week was significantly lower in the cognitive impairment group (23.53% vs 52.34%; P = 0.001). No statistically significant differences (all P > 0.05) were found between the two groups for the remaining variables, including sex, body mass index (BMI), living arrangement, diabetes mellitus, coronary heart disease, smoking history, or alcohol consumption. Comprehensive baseline characteristics are presented in Table 1.
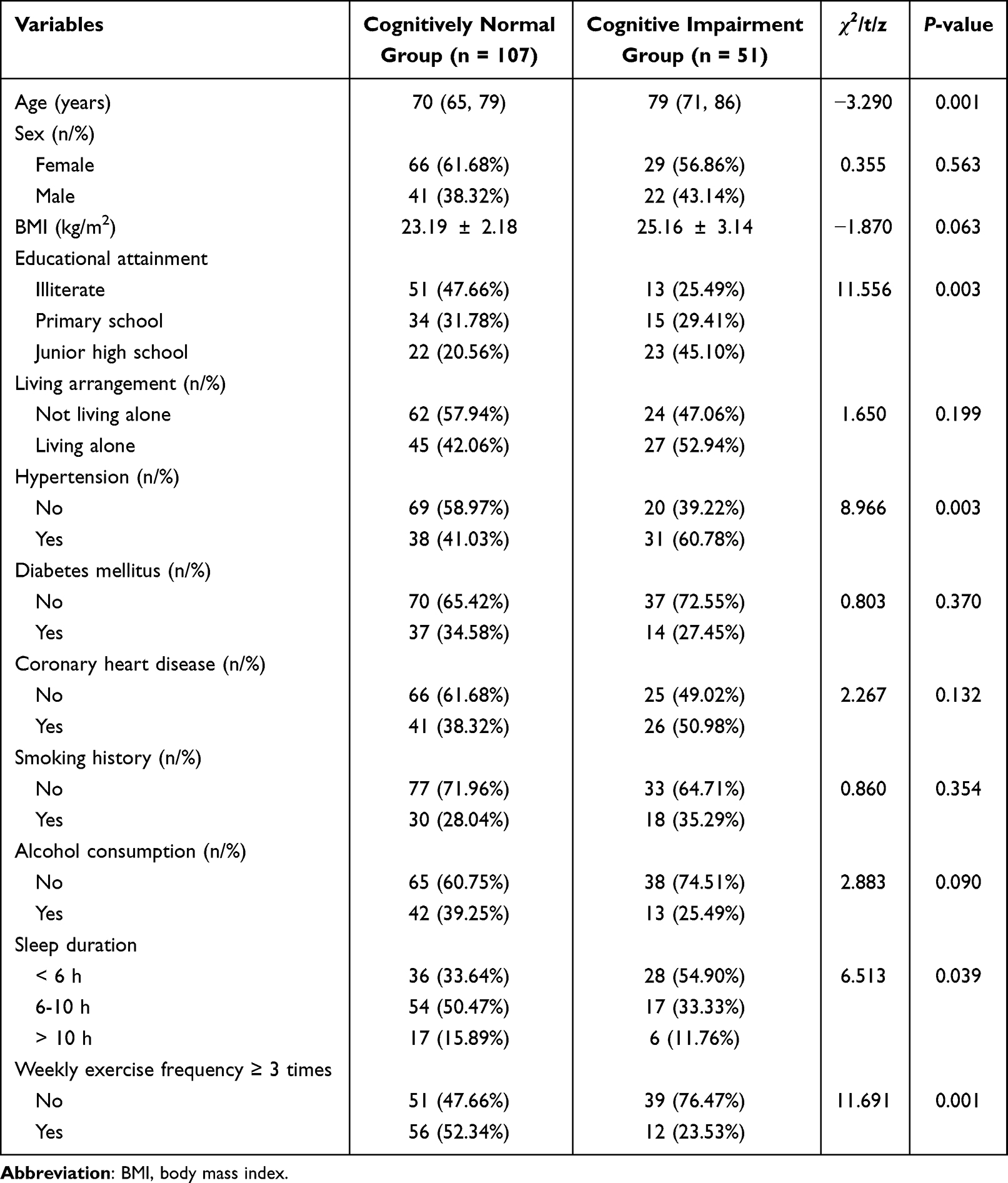 |
Table 1 Baseline Characteristics |
Intergroup Differences in HBM Dimensions and Psychosocial Factors
Significant differences in scores across the dimensions of the HBM and psychosocial factors were observed between the cognitively normal group and the cognitive impairment group (as seen in Table 2). Compared to the cognitively normal group, participants with cognitive impairment demonstrated significantly elevated scores for perceived severity (3.57 ± 0.59 vs 3.32 ± 0.58; P = 0.014), perceived barriers (3.63 ± 0.50 vs 3.15 ± 0.66; P < 0.001), and loneliness (49.20 ± 7.86 vs 41.22 ± 8.57; P < 0.001). Conversely, the cognitive impairment group exhibited significantly reduced scores for perceived benefits (2.94 ± 0.72 vs 3.31 ± 0.59; P = 0.001), self-efficacy (2.67 ± 0.54 vs 3.21 ± 0.56; P < 0.001), and social support (29.12 ± 6.35 vs 33.30 ± 5.36; P < 0.001). No statistically significant differences (P > 0.05) were detected between the groups for perceived susceptibility or cues to action. Detailed comparative results are presented in Table 2.
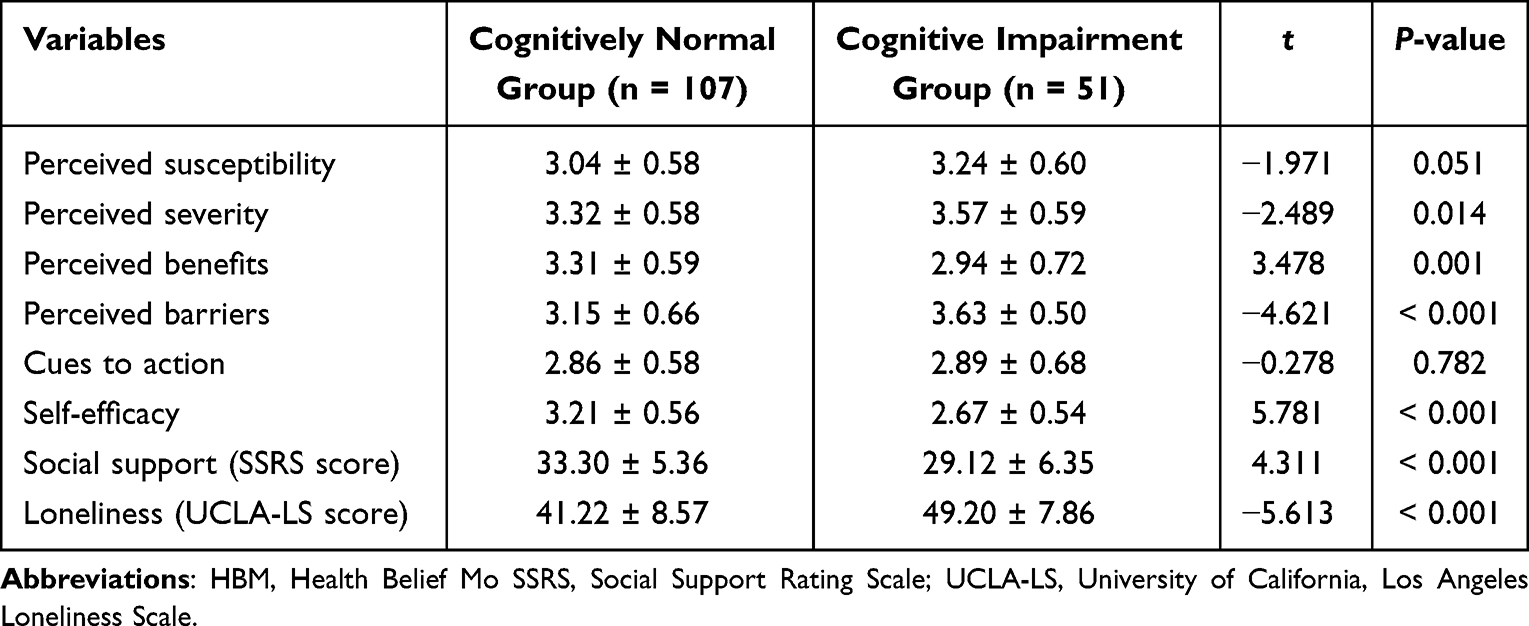 |
Table 2 Intergroup Differences in HBM and Psychosocial Factors |
Multivariable Logistic Regression Model
Variables demonstrating significant intergroup differences underwent collinearity diagnostics, revealing variance inflation factor (VIF) values below 5 for all included variables. Following appropriate variable coding (as detailed in Table 3), these variables were entered into a multivariable logistic regression analysis. The results identified several independent risk factors for cognitive impairment: advanced age [odds ratio (OR) = 1.068, 95% confidence interval (CI): 1.002–1.138, P = 0.043], hypertension (OR = 3.504, 95% CI: 1.027–11.960, P = 0.045), higher perceived barriers (OR = 3.828, 95% CI: 1.147–12.781, P = 0.029), and elevated loneliness scores (UCLA-LS; OR = 1.116, 95% CI: 1.036–1.204, P = 0.004). Conversely, protective factors significantly associated with a reduced risk of cognitive impairment included higher educational attainment (primary education: OR = 0.110, 95% CI: 0.025–0.475, P = 0.003), engaging in exercise at least three times per week (OR = 0.262, 95% CI: 0.071–0.968, P = 0.045), greater self-efficacy (OR = 0.145, 95% CI: 0.050–0.420, P < 0.001), and higher social support scores (SSRS; OR = 0.854, 95% CI: 0.768–0.950, P = 0.004). Variables such as perceived severity and perceived benefits, while significant in univariate analyses, did not retain statistical significance in the multivariable model (both P > 0.05). Complete multivariable analysis results are presented in Table 4.
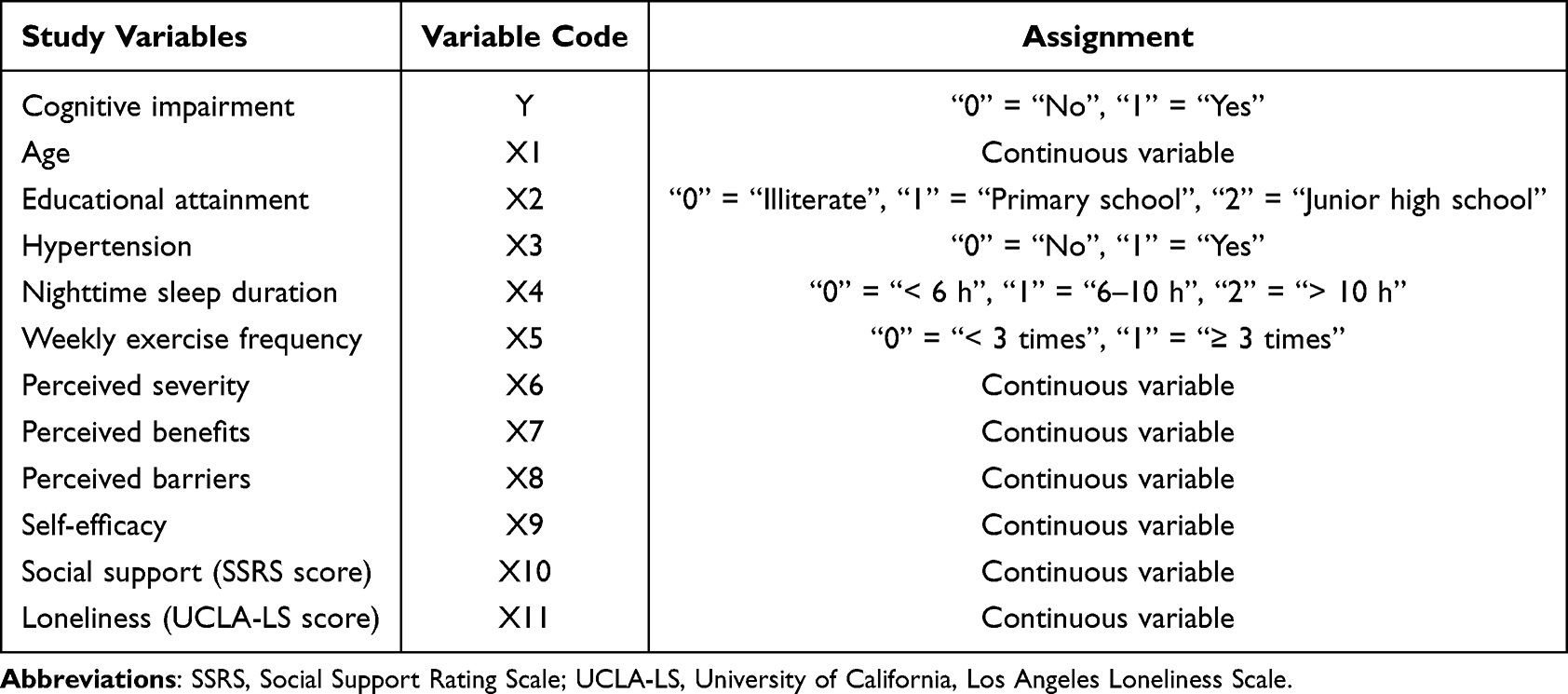 |
Table 3 Variable Coding Scheme |
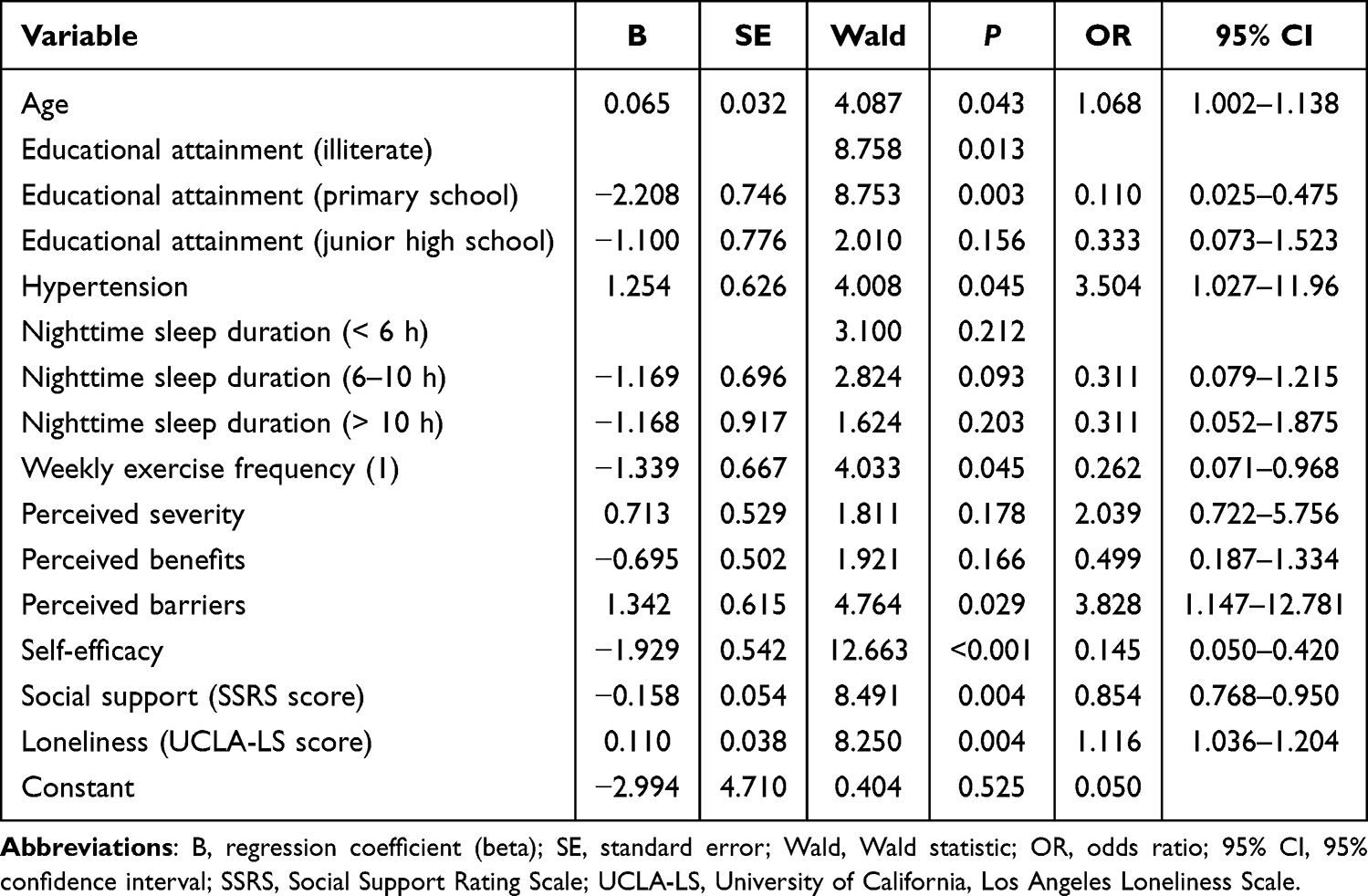 |
Table 4 Results of Multivariable Analysis |
Predictive Model Performance Analysis
ROC curve analysis revealed limited predictive capacity for cognitive impairment when using individual indicators. Among single predictors, self-efficacy demonstrated relatively higher discriminatory power [area under the curve (AUC) = 0.7609, 95% CI: 0.6848–0.8369; Youden’s index = 0.4198), followed by perceived barriers (AUC = 0.7270, 95% CI: 0.6447–0.8092; Youden’s index = 0.3546) and loneliness (AUC = 0.6909, 95% CI: 0.6057–0.7761; Youden’s index = 0.301). Moderate predictive value was observed for age (AUC = 0.6620), weekly exercise frequency (AUC = 0.6440), and social support (AUC = 0.6582). Hypertension exhibited the lowest discriminatory ability (AUC = 0.5544, 95% CI: 0.4582–0.6506), indicating limited predictive utility. Notably, the combined prediction model integrating multiple significant factors demonstrated substantially enhanced performance, achieving an AUC of 0.9514 (95% CI: 0.9214–0.9815) with a sensitivity of 84.31% and specificity of 93.46%. The corresponding Youden’s index was 0.7777, indicating superior predictive accuracy for cognitive impairment compared to any single predictor.
The multivariable logistic regression model demonstrated good discrimination, with an area under the receiver operating characteristic curve (AUC) of 0.92 (95% CI: 0.87–0.96). Internal validation using bootstrap resampling with 1,000 repetitions suggested that model performance was relatively stable.
Model calibration was assessed using bootstrap-corrected calibration plots. The bias-corrected calibration curve showed reasonable agreement with the ideal line across most of the predicted probability range. The mean absolute calibration error was 0.041, and the Brier score was 0.10, indicating acceptable overall calibration. Detailed performance metrics are presented in Table 5 and Figures 1, 2.
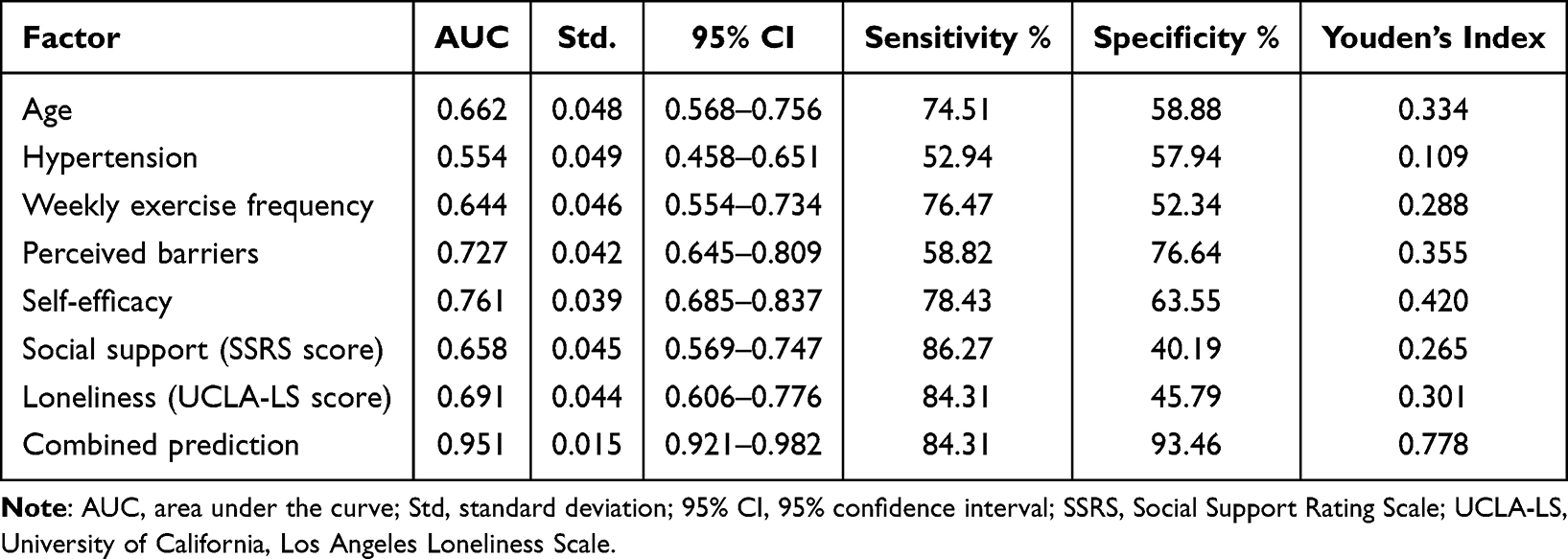 |
Table 5 Predictive Model Performance Analysis |
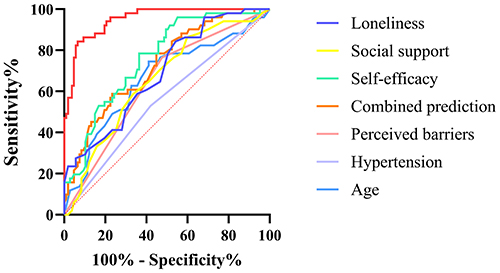 |
Figure 1 ROC curves for various variables and the combined prediction model. |
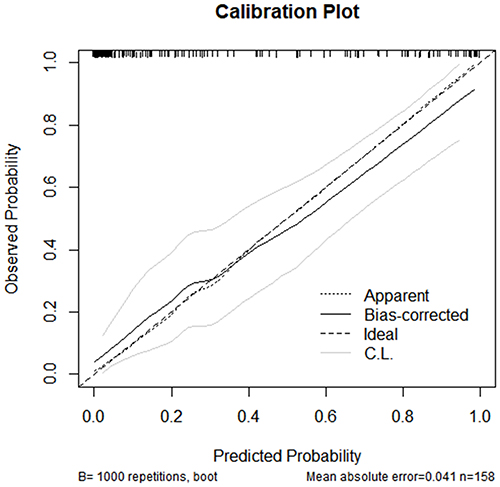 |
Figure 2 Bootstrap-corrected calibration plot of the multivariable logistic regression model. |
Mediation Effect Analysis of Psychosocial-HBM Factors
Based on health behavior theory and relevant literature, social support, loneliness, and self-efficacy were included in the mediation analysis. Univariate and multivariate results confirmed significant associations between all three factors and the risk of cognitive impairment (P < 0.05), while statistically significant correlations were also observed between social support/loneliness and self-efficacy (P < 0.05). Mediation analysis revealed that the indirect mediating effect of self-efficacy on the relationships between social support and cognitive impairment, and between loneliness and cognitive impairment, was not statistically significant (P > 0.05). However, social support exerted a significant negative direct effect on cognitive impairment [estimate (est) = −0.016, P = 0.002], and loneliness demonstrated a significant positive direct effect (est = 0.017, P < 0.001). The total effects of both social support and loneliness on cognitive impairment were also statistically significant. Furthermore, self-efficacy itself served as a significant independent negative predictor of cognitive impairment (est = −0.281, P < 0.001). Therefore, in this sample, social support and loneliness were primarily associated with cognitive impairment through statistically significant direct effects, whereas the indirect effects via self-efficacy were not statistically supported. Given the cross-sectional design, these findings should be interpreted as exploratory and do not establish temporal or causal pathways. Detailed mediation analysis results are presented in Table 6 and illustrated in Figure 3.
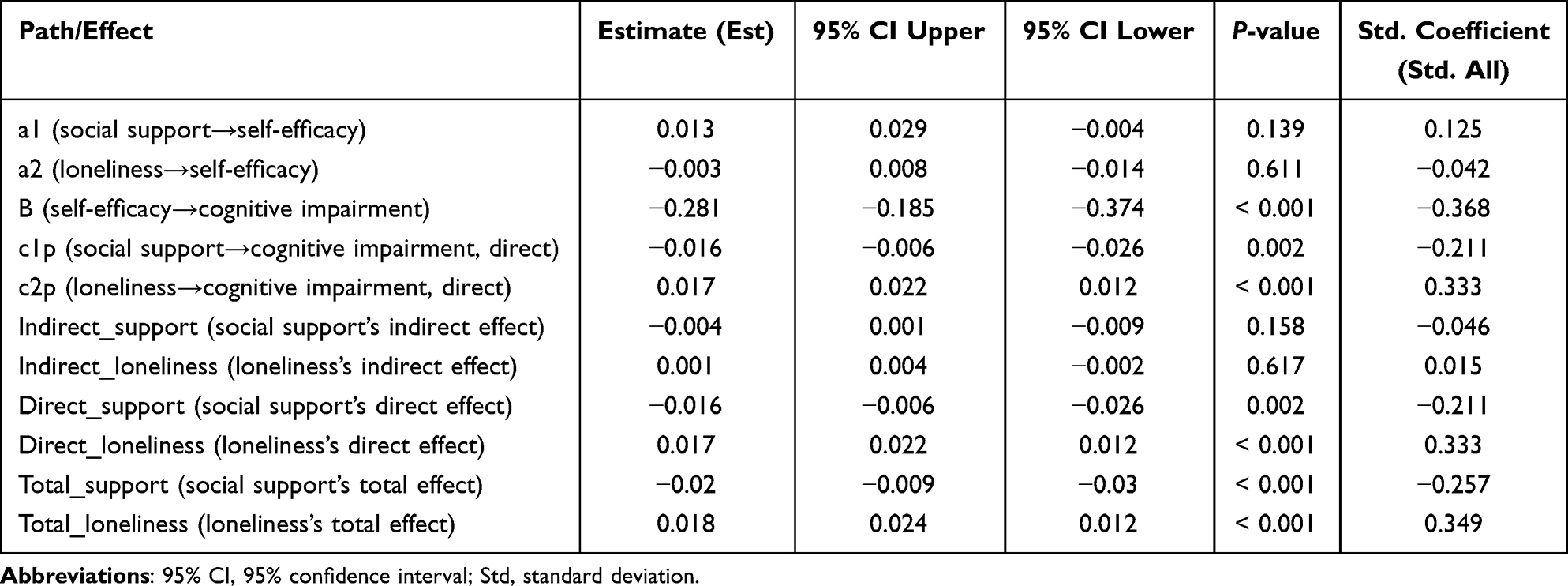 |
Table 6 Mediation Effect Analysis of Psychosocial-HBM Pathways |
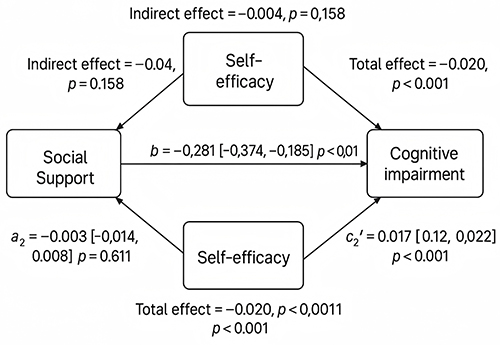 |
Figure 3 Mediation model illustrating the direct and indirect effects of social support and loneliness on cognitive impairment through self-efficacy. |
Discussion
The findings of the present study demonstrated significant negative associations between social support, self-efficacy, and cognitive impairment, while loneliness emerged as an independent risk factor. Furthermore, the multifactorial prediction model demonstrated good discriminative performance (AUC = 0.9514), supporting its potential utility for identifying individuals at higher risk of cognitive impairment in community settings rather than establishing causal relationships. These findings align closely with the study objectives of identifying psychosocial correlates of cognitive impairment and developing a community-oriented prediction model to support early risk identification. Particularly among rural residents and individuals with lower levels of education, the protective effect of social support may play an even more pivotal role, underscoring the need for tailored interventions that integrate educational background with strategies to enhance social and emotional connections.
Consistent with numerous domestic and international studies, social support has been frequently identified as a protective factor for cognitive function. A meta-analysis encompassing 2.37 million individuals revealed that weak social networks were associated with a significantly increased risk of dementia, and lack of social support also elevated this risk.14 A longitudinal follow-up study further indicates lower dementia risk among individuals with high social participation and frequent social contact.15 The significant negative direct effect of social support on cognitive impairment observed in our study aligns with these reports, supporting the crucial role of emotional and functional social connections in maintaining cognitive health. Evidence from an urban sample in Jilin Province demonstrated that higher levels of education were significantly associated with reduced risk of cognitive impairment (P < 0.001), whereas the effects of occupational or cognitive activities appeared limited.9 Moreover, analyses based on the Chinese Longitudinal Healthy Longevity Survey (CLHLS) indicated that socioeconomic disparities represent a critical predictor of cognitive decline among older adults in China, with educational attainment accounting for approximately 40% of the observed inequality. Emotional support also emerged as a significant factor contributing to the unequal distribution of cognitive impairment.16
Conversely, loneliness has consistently been implicated as a significant risk factor for cognitive impairment.17 Our results confirmed a significant positive direct effect of loneliness on cognitive impairment. A meta-analysis involving 600,000 individuals in PubMed suggested that loneliness increased the risk of cognitive impairment by approximately 42%.14 Another meta-analysis incorporating 31 cohort studies found significant associations between social isolation and dementia incidence [eg, relative risk (RR) = 1.57 for reduced social contact, RR = 1.58 for loneliness].17 Mechanistically, loneliness may impair neurological health by increasing psychological stress, inflammatory responses, and negative affect.18–20 Therefore, our findings reinforce the importance of addressing emotional isolation and mitigating loneliness within community-based interventions.
Self-efficacy demonstrated a strong independent negative predictive value for cognitive impairment in this study, with an AUC of 0.7609. This concurs with findings from studies conducted in the US and Europe, where enhancing self-efficacy in individuals with mild cognitive impairment (MCI) or mild dementia has been associated with improvements in depression, anxiety, and quality of life.21,22 Bandura’s social cognitive theory posits that self-efficacy influences an individual’s behavioral beliefs in response to situations, thereby modifying health behavior pathways such as exercise, social engagement, and cognitive training.23 Randomized controlled intervention trials have shown that self-efficacy training can enhance cognitive performance and brain function responses in older adults,24 which resonates with the independent predictive role of self-efficacy identified here.
Regarding the theoretical pathway proposing that social support and loneliness influence cognition indirectly through self-efficacy, our mediation analysis did not detect statistically significant indirect effects. This suggests that this specific mediating mechanism was not statistically supported within our samples. Potential explanations include the cross-sectional design, cultural factors, measurement limitations, and sample size constraints. In contrast, some European studies, such as the German AgeWell.de project,25 found that self-efficacy partially mediated the relationship between social participation and cognitive maintenance. This discrepancy implies that the mediating role of self-efficacy may depend on specific sample characteristics or study designs, warranting further investigation through longitudinal or intervention studies.
The superior predictive performance of the combined model underscores that integrating multidimensional variables significantly outperforms reliance on single indicators for community-based early screening. Similar conclusions were drawn by the Rush University Memory and Aging Project in the US, which found a positive association between social engagement and cognitive ability. Chen et al26 also reported that the most socially active individuals had a 38% reduced risk of dementia and a 21% reduced risk of MCI, with dementia onset delayed by approximately 5 years on average. Community screening practices should therefore consider integrating psychosocial indicators like social support, loneliness, and self-efficacy with traditional physiological measures to enhance early identification accuracy.
From an intervention perspective, our findings provide practical guidance for community strategies. Enhancing emotional support through initiatives such as neighborhood mutual assistance, interest groups, and volunteer companionship represents one key approach. Concurrently, developing self-efficacy training programs incorporating goal setting, task feedback, and cognitive exercises holds promise for improving older adults’ capacity for autonomous health management. Empirical support for such multidimensional strategies comes from community intervention trials like the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER)27 and the US Study to Protect Brain Health Through Lifestyle Intervention to Reduce Risk (US POINTER).28 In the FINGER intervention group, combining dietary guidance, physical activity, cognitive training, and social activities resulted in an average 25% improvement in global cognitive function post-intervention, with significant advantages over the control group in subdomains including executive function, processing speed, and memory (improvements in executive function reached as high as 83%). The US POINTER study further demonstrated the feasibility of this model within US communities, indicating that long-term interventions can improve cognitive performance and maintain adherence rates. From a practical perspective, these findings suggest that community nurses and public health practitioners could incorporate brief psychosocial screening for social support and loneliness into routine community cognitive screening. In addition, community-based brain health programs may benefit from integrating self-efficacy-enhancing components, along with targeted outreach to older adults with limited physical activity or uncontrolled hypertension, to support early, non-pharmacological prevention efforts.
Nevertheless, several limitations warrant consideration. First, the cross-sectional design precludes causal inference and temporal ordering; accordingly, the mediation analysis should be interpreted as exploratory and hypothesis-generating rather than confirmatory evidence of causal mechanisms, and future longitudinal or intervention studies are needed to verify the proposed pathways. Second, participants were recruited from a single community, which may limit representativeness and generalizability and may also have contributed to the counterintuitive distribution of educational attainment observed in the baseline characteristics; this pattern likely reflects cohort effects, as participants with junior high school education tended to be younger than illiterate participants, and age is a strong determinant of cognitive impairment. Third, the modest sample size may have limited statistical power to detect mediation effects. Fourth, several potentially relevant factors, including depression, physiological markers, biomarkers, and the severity or progression of cognitive impairment, were not assessed, which may have constrained the explanatory scope of the model. Future studies incorporating larger samples, longitudinal designs, and severity-based assessments are warranted.
Conclusion
In summary, this study provides evidence of associations between social support, loneliness, self-efficacy, and cognitive impairment, and presents a preliminary combined prediction model for community-based risk identification. The mediation analysis did not demonstrate significant indirect effects and should be interpreted as exploratory and hypothesis-generating. Self-efficacy showed an independent negative association with cognitive impairment, suggesting its relevance as a potential intervention target. Future longitudinal and intervention studies are needed to validate the proposed relationships and further refine and externally validate the prediction model.
Data Sharing Statement
The datasets generated and analyzed in the current study are available on request from the corresponding author.
Ethics Approval and Consent to Participate
The study protocol received approval from the Ethics Committee of Suizhou Central Hospital (No. KY-2025-22-01), and written informed consent was obtained from all participants. All data were anonymized prior to analysis, strictly adhering to the Declaration of Helsinki and local ethical regulations to ensure participant privacy and data security.
Funding
There is no funding to report.
Disclosure
Qingjiao Zhu and Jinjing Xia are co-first authors for this study. The authors declare no competing interests in this work.
References
1. Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP. The global prevalence of dementia: a systematic review and metaanalysis. Alzheimers Dement. 2013;9(1):63–12. doi:10.1016/j.jalz.2012.11.007
2. Wu X, Tang Y, He Y, Wang Q, Wang Y, Qin X. Prevalence of cognitive impairment and its related factors among Chinese older adults: an analysis based on the 2018 CHARLS data. Front Public Health. 2024;12:1500172. doi:10.3389/fpubh.2024.1500172
3. Ma L. Depression, anxiety, and apathy in mild cognitive impairment: current perspectives. Front Aging Neurosci. 2020;12:9. doi:10.3389/fnagi.2020.00009
4. Zu B, Wang N, Fan L, et al. A study on the impact of chronic diseases and depressive symptoms comorbidity on the risk of cognitive impairment in middle-aged and older adults people based on the CHARLS database. Front Public Health. 2025;13:1558430. doi:10.3389/fpubh.2025.1558430
5. Zhang J, Liu X, Gong D, Peng Y, Li H, Yang Y. Health beliefs, lifestyle, and cognitive aging among Chinese community residents: a structural equation model analysis. Front Public Health. 2022;10:1028679. doi:10.3389/fpubh.2022.1028679
6. Huang Y, Wang T, Wang H, Zeng Y, Xie L. Health beliefs mediates the association between the number of non-communicable diseases and preventive behaviors in middle-aged and older adults in southern China. Aging Clin Exp Res. 2025;37(1):49. doi:10.1007/s40520-025-02939-3
7. Mo PK, Xie L, Fong VWI, et al. Efficacy of a theory-based and setting-based intervention in promoting strength training among older adults in Hong Kong: a clustered randomized controlled trial. Appl Psychol Health Well Being. 2024;16(4):1731–1756. doi:10.1111/aphw.12548
8. O’Neil-Pirozzi TM. Cognitive exercise self-efficacy of community-dwelling older adults: measurement and associations with other self-reported cognitive exercise factors. Brain Sci. 2021;11(6):672. doi:10.3390/brainsci11060672
9. Li B, Guo Y, Deng Y, et al. Association of social support with cognition among older adults in China: a cross-sectional study. Front Public Health. 2022;10:947225. doi:10.3389/fpubh.2022.947225
10. Wang Y, Li J, Fu P, Jing Z, Zhao D, Zhou C. Social support and subsequent cognitive frailty during a 1-year follow-up of older people: the mediating role of psychological distress. BMC Geriatr. 2022;22(1):162. doi:10.1186/s12877-022-02839-5
11. Kwon S, Benoit E, Windsor L. The effects of social support and self-efficacy on hopefulness in low-income older adults during COVID-19 pandemic. BMC Geriatr. 2024;24(1):305. doi:10.1186/s12877-024-04915-4
12. Cui X, Zheng X, Lu Y. Prediction model for cognitive impairment among disabled older adults: a development and validation study. Healthcare. 2024;12(10):1028. doi:10.3390/healthcare12101028
13. Wang X, Zhou S, Ye N, et al. Predictive models of Alzheimer’s disease dementia risk in older adults with mild cognitive impairment: a systematic review and critical appraisal. BMC Geriatr. 2024;24(1):531. doi:10.1186/s12877-024-05044-8
14. Penninkilampi R, Casey AN, Singh MF, Brodaty H. The association between social engagement, loneliness, and risk of dementia: a systematic review and meta-analysis. J Alzheimers Dis. 2018;66(4):1619–1633. doi:10.3233/JAD-180439
15. Wang S, Molassiotis A, Guo C, Leung ISH, Leung AYM. Association between social integration and risk of dementia: a systematic review and meta-analysis of longitudinal studies. J Am Geriatr Soc. 2023;71(2):632–645. doi:10.1111/jgs.18094
16. Deng Q, Liu W. Inequalities in cognitive impairment among older adults in China and the associated social determinants: a decomposition approach. Int J Equity Health. 2021;20(1):82. doi:10.1186/s12939-021-01422-5
17. Kuiper JS, Zuidersma M, Oude Voshaar RC, et al. Social relationships and risk of dementia: a systematic review and meta-analysis of longitudinal cohort studies. Ageing Res Rev. 2015;22:39–57. doi:10.1016/j.arr.2015.04.006
18. Cardona M, Andres P. Are social isolation and loneliness associated with cognitive decline in ageing? Front Aging Neurosci. 2023;15:1075563. doi:10.3389/fnagi.2023.1075563
19. Zhang Y, Tatewaki Y, Liu Y, et al. Perceived social isolation is correlated with brain structure and cognitive trajectory in Alzheimer’s disease. Geroscience. 2022;44(3):1563–1574. doi:10.1007/s11357-022-00584-6
20. Smith KJ, Gavey S, RIddell NE, Kontari P, Victor C. The association between loneliness, social isolation and inflammation: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2020;112:519–541. doi:10.1016/j.neubiorev.2020.02.002
21. Lee J, Cho E, Kim H, Lee KH, Kim E, Ye BS. The development and evaluation of a self-efficacy enhancement program for older adults with mild cognitive impairment. Appl Nurs Res. 2023;73:151726. doi:10.1016/j.apnr.2023.151726
22. Kurasz AM, DeFeis B, Locke DEC, et al. Psychometric properties of the self-efficacy for managing mild cognitive impairment scale. Int J Geriatr Psychiatry. 2021;36(1):174–181. doi:10.1002/gps.5411
23. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52(1):1–26. doi:10.1146/annurev.psych.52.1.1
24. Rotenberg S, Anderson ND, Binns MA, et al. Effectiveness of a meta-cognitive group intervention for older adults with subjective cognitive decline or mild cognitive impairment: the ASPIRE randomized controlled trial. J Prev Alzheimers Dis. 2024;11(6):1534–1548. doi:10.14283/jpad.2024.166
25. Wittmann FG, Pabst A, Zulke A, et al. Adherence to a lifestyle intervention - just a question of self-efficacy? Analysis of the AgeWell.de-intervention against cognitive decline. Alzheimers Res Ther. 2024;16(1):133. doi:10.1186/s13195-024-01499-4
26. Chen Y, Grodstein F, Capuano AW, Wang T, Bennett DA, James BD. Late-life social activity and subsequent risk of dementia and mild cognitive impairment. Alzheimers Dement. 2025;21(1):e14316. doi:10.1002/alz.14316
27. Kivipelto M, Solomon A, Ahtiluoto S, et al. The finnish geriatric intervention study to prevent cognitive impairment and disability (FINGER): study design and progress. Alzheimers Dement. 2013;9(6):657–665. doi:10.1016/j.jalz.2012.09.012
28. Baker LD, Snyder HM, Espeland MA, et al. Study design and methods: u.S. study to protect brain health through lifestyle intervention to reduce risk (U.S. POINTER). Alzheimers Dement. 2024;20(2):769–782. doi:10.1002/alz.13365
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Social Support and Daytime Sleepiness Among Chinese Medical Students: Mediating Roles of Loneliness and Problematic Smartphone Use
Chen S, Li H, Wen D
Psychology Research and Behavior Management 2023, 16:4083-4093
Published Date: 5 October 2023
Health Behavior Models and Regular Exercise Levels Among Workers in Taiwan
Cheng HI, Hsu WT, Wang WH, Li RH, Tang FC, Huang SL
Journal of Multidisciplinary Healthcare 2023, 16:4149-4159
Published Date: 20 December 2023
Pathways of Media Contact to Health Literacy in Middle-Aged and Older People: The Chain Mediation Effect of Perceived Social Support and Self-Efficacy
Jiang MM, Xiao YW, Liao ZL
Journal of Multidisciplinary Healthcare 2024, 17:111-121
Published Date: 6 January 2024
The Serial Mediation Effects of Social Support and Self-Efficacy on Health Literacy and Self-Management Behaviors Among Young and Middle-Aged Cardiac Patients After Percutaneous Coronary Intervention: A Cross-Sectional Study in China
Liu W, Qian S, Hu Y, Zhang R
Risk Management and Healthcare Policy 2024, 17:2893-2906
Published Date: 22 November 2024
Mediating Effects of Health Literacy, Self-Efficacy, and Social Support on the Relationship Between Disease Knowledge and Patient Participation Behavior Among Chronic Ill Patients: A Cross-Sectional Study Based on the Capability-Opportunity-Motivation and Behavior (COM-B) Model
Wu M, Wang W, He H, Bao L, Lv P
Patient Preference and Adherence 2025, 19:1337-1350
Published Date: 8 May 2025