Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Health Behavior Models and Regular Exercise Levels Among Workers in Taiwan
Authors Cheng HI, Hsu WT, Wang WH, Li RH, Tang FC, Huang SL
Received 18 September 2023
Accepted for publication 8 December 2023
Published 20 December 2023 Volume 2023:16 Pages 4149—4159
DOI https://doi.org/10.2147/JMDH.S435774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hsin-I Cheng,1,* Wei-Ting Hsu,2,3,* Wei-Hsun Wang,4,5 Ren-Hau Li,6,7 Feng-Cheng Tang,3,4,8 Shu-Ling Huang6,7
1Department of Rehabilitation, Taoyuan General Hospital, Ministry of Health and Welfare, Taoyuan, 330, Taiwan; 2Department of Construction Engineering, Chaoyang University of Technology, Taichung, 413, Taiwan; 3Department of Leisure Services Management, Chaoyang University of Technology, Taichung, 413, Taiwan; 4Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, 402, Taiwan; 5Department of Orthopaedics, Changhua Christian Hospital, Changhua, 500, Taiwan; 6Department of Psychology, Chung Shan Medical University, Taichung, 402, Taiwan; 7Room of Clinical Psychology, Chung Shan Medical University Hospital, Taichung, 402, Taiwan; 8Department of Occupational Medicine, Changhua Christian Hospital, Changhua, 500, Taiwan
*These authors contributed equally to this work
Correspondence: Shu-Ling Huang, Department of Psychology, Chung Shan Medical University, 110, Section 1, Jianguo North Road, South District, Taichung, 402, Taiwan, Tel +886-4-24730022 ext. 12301, Fax +886-4-23248191, Email [email protected] Feng-Cheng Tang, Department Occupational Medicine, Changhua Christian Hospital, 135 Nanhsiao Street, Changhua, 500, Taiwan, Tel +886-4-7286929, Fax +886-4-727-0910, Email [email protected]
Purpose: The present study aims to examine the disparate effects of health behavior models, namely exercise self-efficacy (ESE), health belief model (HBM), and planned behavior theory (PBT), applied to clarify the degree of regular exercise among workers in Taiwan.
Methods: A cross-sectional research design was adopted. A questionnaire was distributed to obtain information pertaining to regular exercise level, demographic characteristics, and the scores of ESE, HBM, and PBT. In total, 400 full-time workers voluntarily participated in this study.
Results: The results showed that only 20.5% of the participants exercised regularly, 37.3% exercised irregularly, and 42.3% did not exercise currently. “Perceived benefits” and “perceived barriers” pertaining to HBM; “attitude” and “perceived behavioral control” pertaining to PBT; and ESE were associated with regular exercise level in the multiple linear regression analyses of each health behavior model. When all three models were considered simultaneously, ESE provided the greatest explanation of the variances for regular exercise levels. PBT total made a smaller contribution in the prediction of regular exercise level, while the effect of HBM did not show statistical significance. In order to explore the practicality of moving beyond theoretical models and focusing on the components across health behavior models to enhance workers’ exercise behavior, the components showing statistical significance in separate analysis were put into the multiple linear regression simultaneously. The results showed that ESE, perceived barriers of health behavior, attitude, and perceived behavioral control were significantly associated with regular exercise level.
Conclusion: A low percentage of workers exercising regularly should be a notable issue for workplace health promotion. Neither utilizing cues to exercise nor advertising health threats of physical inactivity is sufficient to enable workers to exercise regularly. Enhancing workers’ ESE and behavior control and removing the exercise barriers would constitute efficient strategies for maintaining the exercise habit of workers.
Keywords: exercise, self-efficacy, health belief model, planned behavior theory, worker
Introduction
Issues related to health promotion began to receive attention in the 1970s, and have continued to expand ever since. In the Ottawa Charter for Health Promotion in 1986, the World Health Organization (WHO) considered health as a positive concept, emphasizing social/personal resources and physical capabilities, and viewed health as an everyday resource rather than a life goal. In the same period, the Ottawa Charter defined health promotion as “the process of enabling people to increase control over, and to improve, their health”.1 People can learn and practice healthy lifestyles in various settings, including schools, homes, workplaces, and the broader communities, to cope with all stages of life, chronic disease, and injury. In particular, workers spend one third of their life at work, so the workplace is one of the powerful settings wherein to manage health promotion activities. To promote workplace health, the purpose of this study is to explore the effects of applying health behavior models to workers’ exercise behaviors.
WHO defines exercise as planned, structured, and repetitive behavior by individuals, with the goal of improving or maintaining physical fitness. WHO2 states that regular exercise can not only reduce the risk of various chronic diseases, including hypertension, stroke, diabetes, depression, and cancer, but also improve bone and muscle health. Regular exercise and adequate physical activity help to prevent physical disorders and increase physiological benefits, such as enhancing cardiorespiratory fitness, and reducing the declining rate of skeletal muscle functionality and the risk of cognitive impairment.3–6 In addition to physical health, exercise also has many benefits for psychological health. Studies have found that exercise can reduce the risk of depression and its recurrence.7,8 Moreover, exercise can also create more positive outlooks on life among the elders, reduce dependence on others, and enhance their sense of dignity.9 For adolescent women, it provides better body image and improves women’s sense of self-worth.10
There have been several studies using various health behavior models to predict intention for exercise behavior. Commonly used health behavior models include the Exercise Self-Efficacy (ESE), the Health Belief Model (HBM), and the Planned Behavior Theory (PBT). Self-efficacy was first proposed by Bandura and refers to “an individual’s belief in his or her capacity to execute behaviors necessary to produce specific performance attainments”.11 It reflects confidence in the ability to exert control over one’s own behavior. Subsequently, ESE was proposed to examine the association between self-efficacy and the maintenance of exercise participation;12 it is defined as beliefs about one’s capability to successfully engage in incremental bouts of physical activity.13 Several studies, with the cross-sectional research design, have confirmed a positive correlation between ESE and exercise behavior indices, including frequency and intensity. The higher the ESE, the better the exercise behavior performance.14,15 Some studies, with the longitudinal research design, have also demonstrated that ESE is shown to be predictive of adherence in the early stages of an organized exercise program and to be the only variable to significantly predict adherence to exercise during follow-up.12,16
The Health Belief Model (HBM) was proposed by Rosenstock;17 it is expected to reduce the occurrence of diseases through early self-screening and prevention. HBM is composed of important components such as perceived susceptibility, perceived seriousness, perceived benefits, perceived barriers, and cues to action.17,18 “Perceived susceptibility” and “perceived seriousness” are often seen together and named as perceived threat of disease. “Perceived threat of disease” refers to an individual’s perception of disease-related information and the role of perceived threat to one’s own health. “Perceived benefits” refers to an individual’s subjective assessment of the possible benefits of a new behavior to lower the risk of disease. “Perceived barriers” refers to subjective cognitive evaluation of possible burden costs or obstacles in relation to the new behavior. “Cues to action” are the factors that trigger behavioral change when individuals are subjected to internal or external stimuli. HBM is often used to understand and predict the exercise performance of individuals with or without disease. The research results show that when HBM is applied to different types of individuals, each component has different effects on exercise behaviors.19–21 These inconsistent results are worth further research and investigation.
The Planned Behavior Theory (PBT) was extended from the Theory of Reasoned Action to predict and understand human behavior.22 PBT includes three components: attitude, subjective norms, and perceived behavioral control. This theory declares that behavior is directly affected by behavioral intention, and perceived behavioral intention in turn is determined by one’s attitude, subjective norms, and perceived behavioral control.23 “Attitude” refers to an individual’s subjective cognition, whether positive or negative, and value judgment regarding engagement in a regular behavior. “Perceived behavioral control” refers to abilities, resources, and opportunities that an individual believes he or she needs to possess in order to successfully enact a behavior. “Subjective behavioral norms” refers to a personal perception of the social pressures and expectations imposed to perform a particular behavior. The comprehensive review article points out that attitude and perceived behavioral control are important factors affecting exercise intention, and that exercise behavior could be greatly improved by proactively providing exercise plans to individuals when they have a positive attitude toward exercise and assisting them in overcoming obstacles when they think exercise is difficult to carry out.24
Physical inactivity significantly contributes to non-communicable diseases and significantly impacts mental health and overall quality of life. A comprehensive analysis of 358 surveys spanning 168 countries, examining insufficient physical activity trends globally from 2011 to 2016, revealed a notable global age-standardized prevalence of insufficient physical activity, reaching 27.5% in 2016. This insufficiency has notably increased in high-income countries over time, rising from 31.6% in 2001 to 36.8% in 2016.25 Moreover, the emergence of the coronavirus disease 2019 (COVID-19) has adversely affected engagement in physical activity.26–28 Seeking the essential components aimed at increasing the level of physical activity among workers is imperative.
Theoretical frameworks such as ESE, HBM, and PBT emphasize distinct dimensions of health behavior. ESE accentuates internal confidence regarding the execution of health behaviors, while HBM underscores the necessity and accessibility of adopting health-promoting behaviors. PBT primarily centers on the components of behavioral intention. These models comprehensively encompass fundamental aspects of health behavior. Previous research has explored the associations between exercise behavior and various individual theories or models.14,15,29,30 In contrast, the current study has simultaneously integrated these three models, aiming to identify the most suitable health behavior models and their corresponding components conducive to fostering regular exercise behavior among workers. These findings could provide a robust foundation for the effective and adaptable application of pivotal models and components in future workplace health promotion endeavors.
Materials and Methods
Participants and Recruitment
This study adopted a cross-sectional research design; it was conducted according to the Declaration of Helsinki and was approved by the Institutional Review Board of Chung-Shan University Hospital in Taiwan (CSHIRB No: CS18263). The researchers visited workplaces to explain the purpose of this study and randomly selected 465 full-time workers. The researchers explained the purpose of this study to the workers, respected respondents’ wishes, and promised to keep the information confidential. The workers who agreed to participate in this study were invited to a meeting room at their workplaces to complete a consent form and the study questionnaire. Trained researchers were available to assist in case of any questions. The process took approximately 30 minutes for each participant. Ultimately, a total of 400 workers agreed to participate in this study.
Measures
The present study uses a questionnaire survey method to collect data. The study questionnaire includes demographic characteristics, the degree of ESE, the HMB scale, the PBT scale, and the level of regular exercise behavior. In the personal background variable section, the questions included gender, age, education level, marital status, whether the worker works in shifts, and occupational category.
Self-Efficacy for Exercise
This study uses the Chinese version of the Self-Efficacy for Exercise to measure the degree of ESE. The Self-Efficacy for Exercise Scale was originally developed by Resnick and Jenkins.31 The scale contains nine question items to evaluate ESE and to understand an individual’s confidence in maintaining a regular exercise in the face of exercise obstacles. The extent of confidence for each item ranges from 1 to 10. Higher scores indicate better ESE. The Chinese version of the Self-Efficacy for Exercise Scale was verified and confirmed to have both reliability and validity.32 The Cronbach’s alpha value of this ESE scale in this study was 0.92, indicating good reliability.
Health Belief Model
This study uses the valid and reliable Chinese version of Health Belief Model Scale for Exercise, designed for the assessment of the workers’ health belief in the exercise behavior.33 This scale has 21 items with four components: perceived threat of disease, perceived benefits, perceived barriers, and cues to action. The Likert-type five-point scale was used for scoring. Participants reported their subjective feelings by selecting “strongly disagree”, “disagree”, “neutral”, “agree”, or “strongly agree”. Each answer has one score of 1, 2, 3, 4, and 5 for selection; higher scores indicate greater subject agreeability for the item. The high score for perceived barriers means that it is difficult to exercise. For the other three factors, a high score means that individuals are more likely to exercise regularly. The HBM total score is calculated by deducting the score of perceived barriers from the sum of the scores of perceived threat of disease, perceived benefits, and cues to action. This scale has been tested for reliability and validity, and the Cronbach’s alpha for the four subscales in this study was between 0.75 and 0.87.33
Planned Behavior Theory
This study adopts the planned behavior theory scale developed for the Taiwanese population to measure the intention of regular exercise behavior.34 The scale consists of three components (attitude, perceived behavioral control, and subjective norms) for a total of 21 items. The Likert-type five-point scale was used for scoring, as participants selected an answer, from “strongly disagreeing” to “strongly agreeing”, for each item according to their subjective feelings. Each answer has one score of 1 to 5 for selection; higher scores indicate greater subject agreeability for the item. The PBT total and three subscale scores can be thereby be obtained. The Cronbach’s alpha value of each component ranged from 0.87 to 0.96, with good discriminant validity.34 The Cronbach’s alpha values for the three subscales in this study range from 0.82 to 0.94.
Regular Exercise Levels
The level of regular exercise behavior is described using the Transtheoretical Model.35 It is a 5-stage measure assessing the following exercise behavior: 1) Precontemplation (I am not exercising, and I have no plans to exercise in the next six months.), 2) Contemplation (I am not exercising, but I plan to start exercising in the next six months.), 3) Preparation (I am currently exercising, but not regularly. In the next month, I plan to start exercising regularly.), 4) Action (I am currently exercising regularly, but I have been doing so for less than six months.), 5) Maintenance (I have been engaging in regular exercise for more than six months.). The higher the score, the higher the degree of regular exercise.
Statistical Analysis
The demographic characteristics of the participants, along with their data pertaining to regular exercise levels were summarized using descriptive statistics. The Chi-square test was adopted to compare the differences in regular exercise levels by demographic characteristics and job-related variables. Pearson’s correlation was used to analyze the relationships between the continuous variables. For the research purpose, gender, age, shift work, and occupational category were controlled for in multiple linear regressions. The categorical covariates, including gender, whether taking shift work, and occupational category, were transformed into dummy variables beforehand. Female, without shift work, and white-collar worker were coded as referents. The relationships between health behavior models and regular exercise levels were investigated by multiple linear regression analysis with some specific variables controlled. The relationships of regular exercise levels with ESE, HBM, and PBT were examined respectively in models 1, 2, and 3. These three health behavior models were then investigated simultaneously in model 4. Finally, in order to explore the practicality of moving beyond theoretical models and focusing on the components across health behavior models to enhance workers’ exercise behavior, the components with statistical significance in models 1, 2, and 3 were put into the multiple linear regression simultaneously in model 5. All statistical procedures were performed using SPSS-20.0 software for Microsoft Windows (IBM Corp., Armonk, NY, USA); a p-value less than 0.05 was considered statistically significant.
Results
Of the 465 questionnaires distributed, 400 were successfully collected, representing a response rate of 86.0%. Of the participants, 89.8% were males and 10.3% were females. The average age was 37.72 years (SD = 6.14). The majority of the participants were married (65.5%), with a bachelor’s degree (76.8%), without shift work (71.8%), and white-collar worker (80.8%). The prevalence across the levels of regular exercise behavior was as follows: 13.8% for precontemplation, 28.5% for contemplation, 37.3% for preparation, 9.5% for action, and 11.0% for maintenance. The precontemplation and contemplation stages could be viewed as not currently engaging in exercise (42.3%). The preparation stage indicates irregular exercise (37.3%). The action and maintenance stages signify regular exercise (20.5%). Table 1 lists the regular exercise levels by demographic characteristics and job-related variables. Neither demographic characteristics nor job-related variables showed significant difference on the regular exercise level.
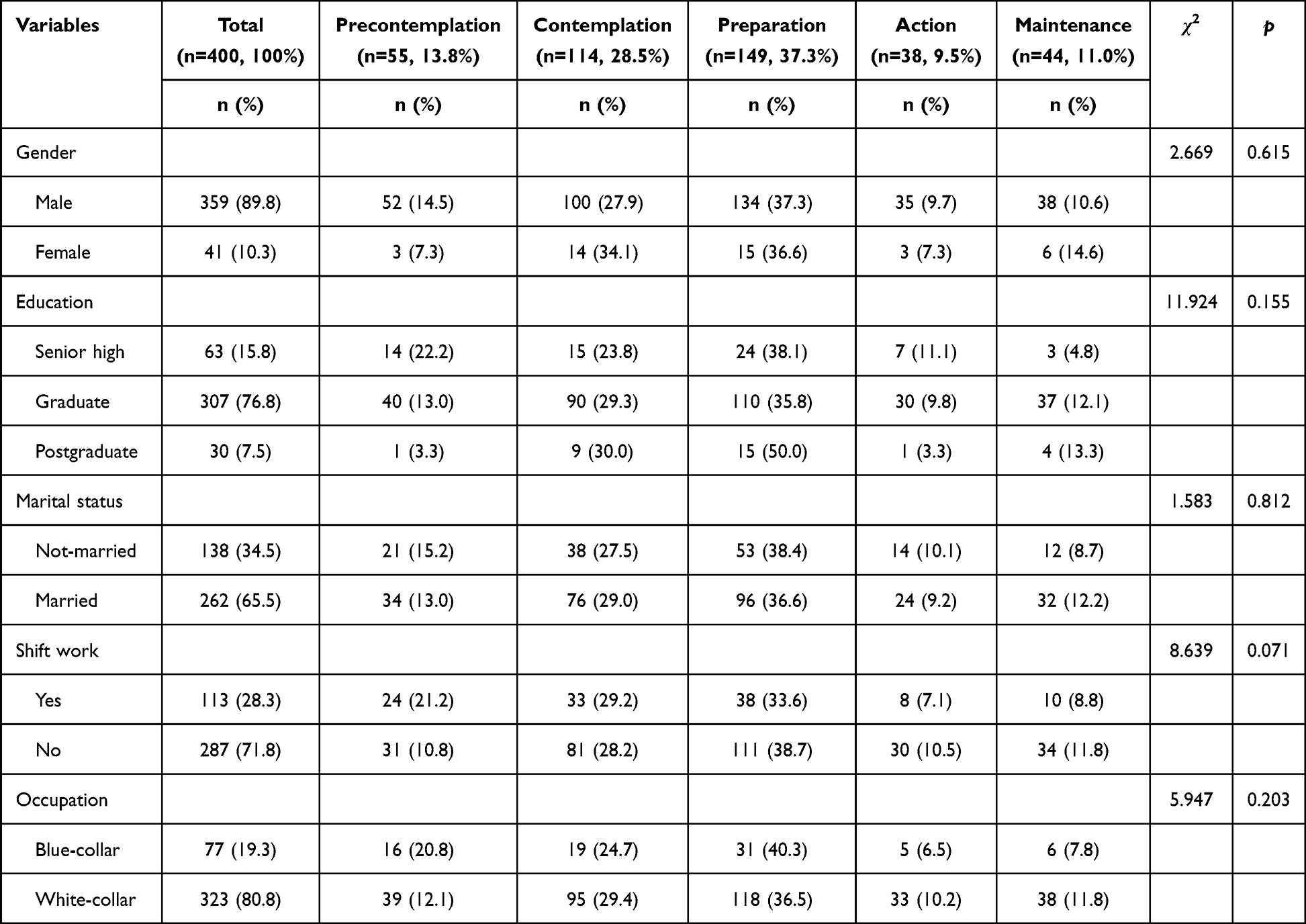 |
Table 1 The Comparisons of Regular Exercise Levels by Demographic Variables |
Table 2 lists the bivariate correlations of the research variables. The level of regular exercise behavior was significantly associated with the main behavior factors, including ESE total, HBM total, perceived threat, perceived benefits, perceived barriers, PBT total, attitude, and perceived behavioral control, except for other research variables, such as age, cues to action, and subjective norm. Among these correlations, the ESE total correlated highly with the level of regular exercise behavior (r = 0.510, p < 0.001). In addition, the correlation coefficients were statistically significant between the main components of all three health behavior models, with the exceptions of the relationships between perceived barriers and other behavior factors, such as perceived threat, perceived benefits, PBT total, and attitude. Moreover, the ESE total was not significantly correlated with subjective norm.
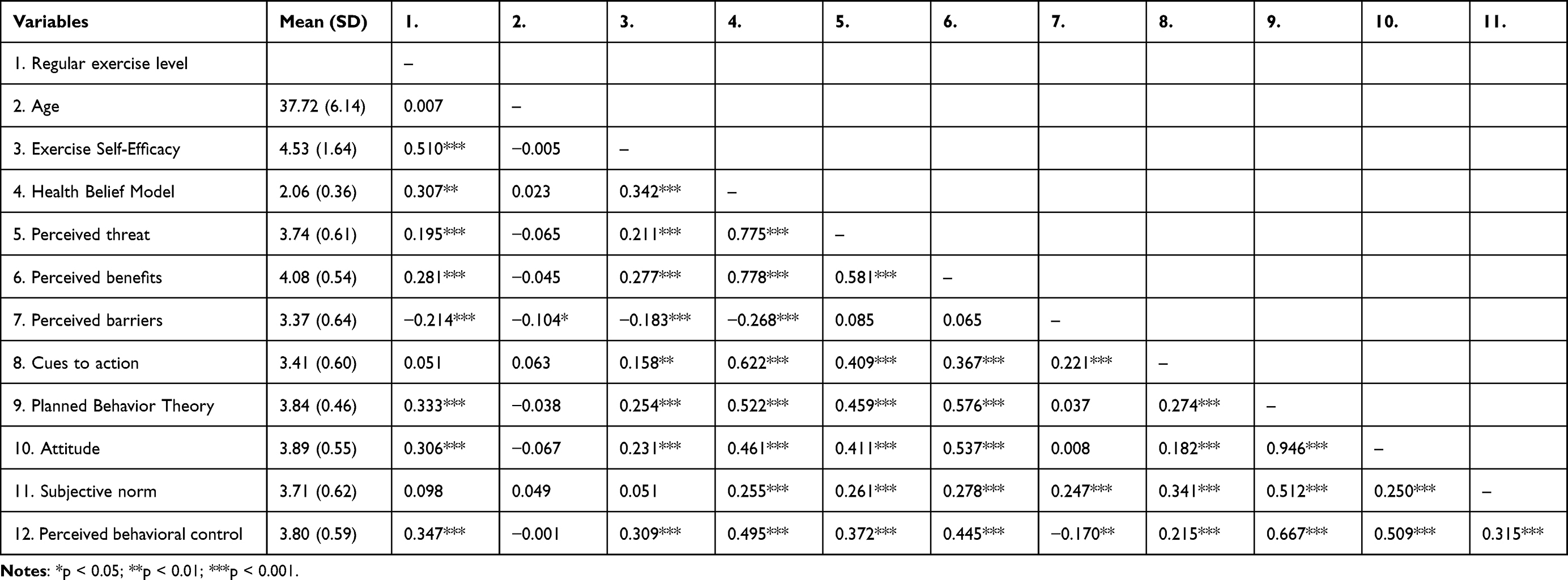 |
Table 2 The Correlations Between Research Variables |
Table 3 summarizes the multiple linear regressions predicting regular exercise level by each health behavior model. In model 1, with gender, age, shift work, and occupational category controlled, the model was significant (F = 30.163, p < 0.001; adjusted R2 = 0.268); ESE showed a significantly positive relation with regular exercise level (β = 0.514, p < 0.001). In model 2, with the same covariates controlled (F = 8.439, p < 0.001; adjusted R2 = 0.130), perceived benefits was positively associated with regular exercise level (β = 0.260, p < 0.001); perceived barriers was negatively associated with regular exercise level (β = −0.229, p < 0.001). In model 3, with covariates controlled (F = 10.303, p < 0.001; adjusted R2 = 0.142), attitude (β = 0.169, p < 0.01) and perceived behavioral control (β = 0.269, p < 0.001) were positively associated with regular exercise level.
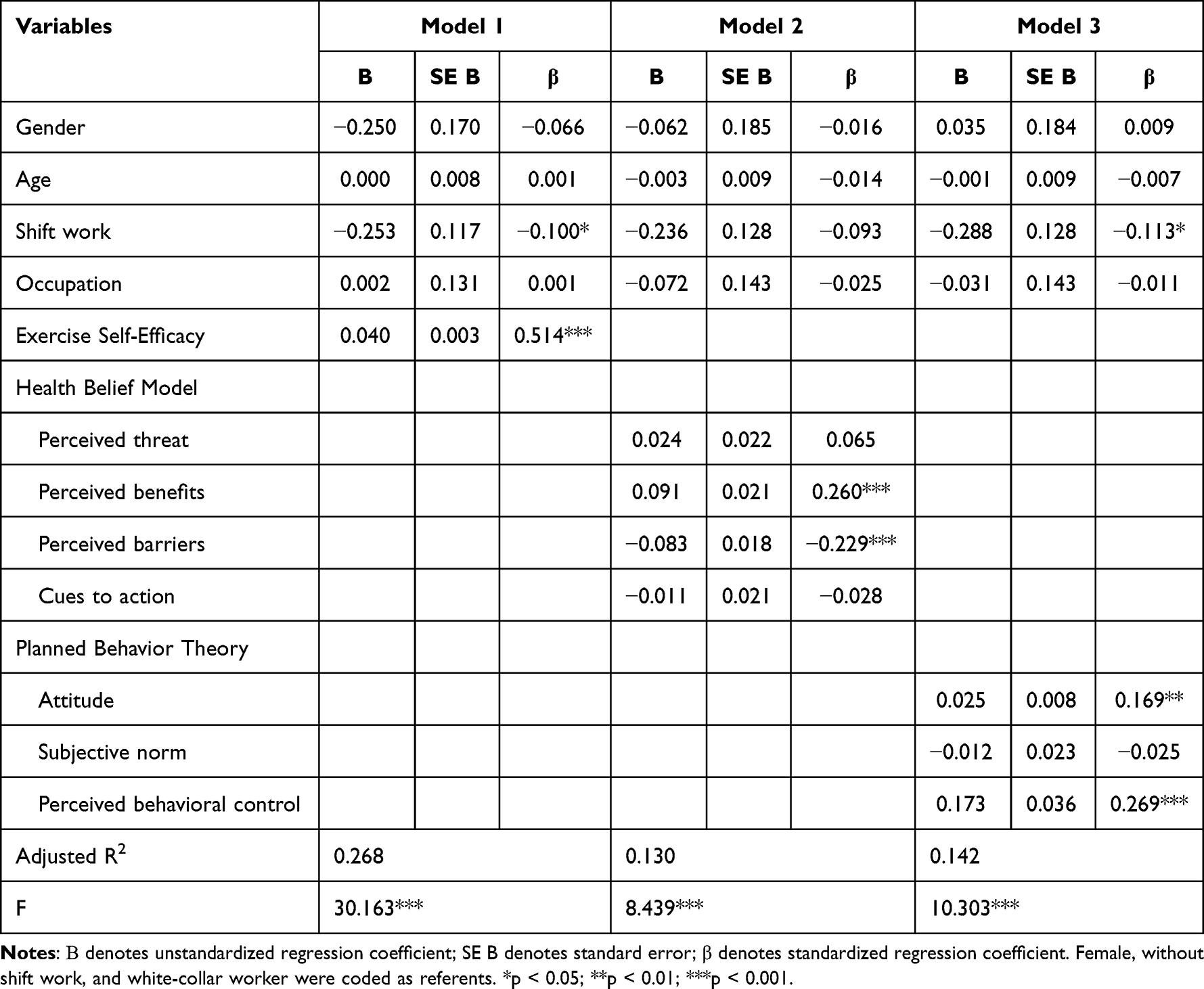 |
Table 3 Summary of Multiple Linear Regressions Predicting Regular Exercise Levels by Health Behavior Models Separately |
Table 4 lists the results of multiple linear regressions predicting regular exercise level by ESE, HBM, and PBT simultaneously. In model 4, when the three health behavior models were taken into consideration simultaneously with covariates controlled (F = 25.690, p < 0.001; adjusted R2 = 0.304), the ESE total (β = 0.450, p < 0.001) and the PBT total (β = 0.190, p < 0.001) were positively associated with regular exercise level. However, the HBM total did not show a significant effect (β = 0.045, p > 0.05). In model 5, with covariates controlled as well, the components with statistical significance in models 1, 2, and 3 were put into the multiple linear regression (F = 22.084, p < 0.001; adjusted R2 = 0.325). The results show that the ESE total (β = 0.414, p < 0.001), perceived barriers (β = −0.126, p < 0.01), attitude (β = 0.117, p < 0.05), and perceived behavioral control (β = 0.119, p < 0.01) were significantly associated with regular exercise level.
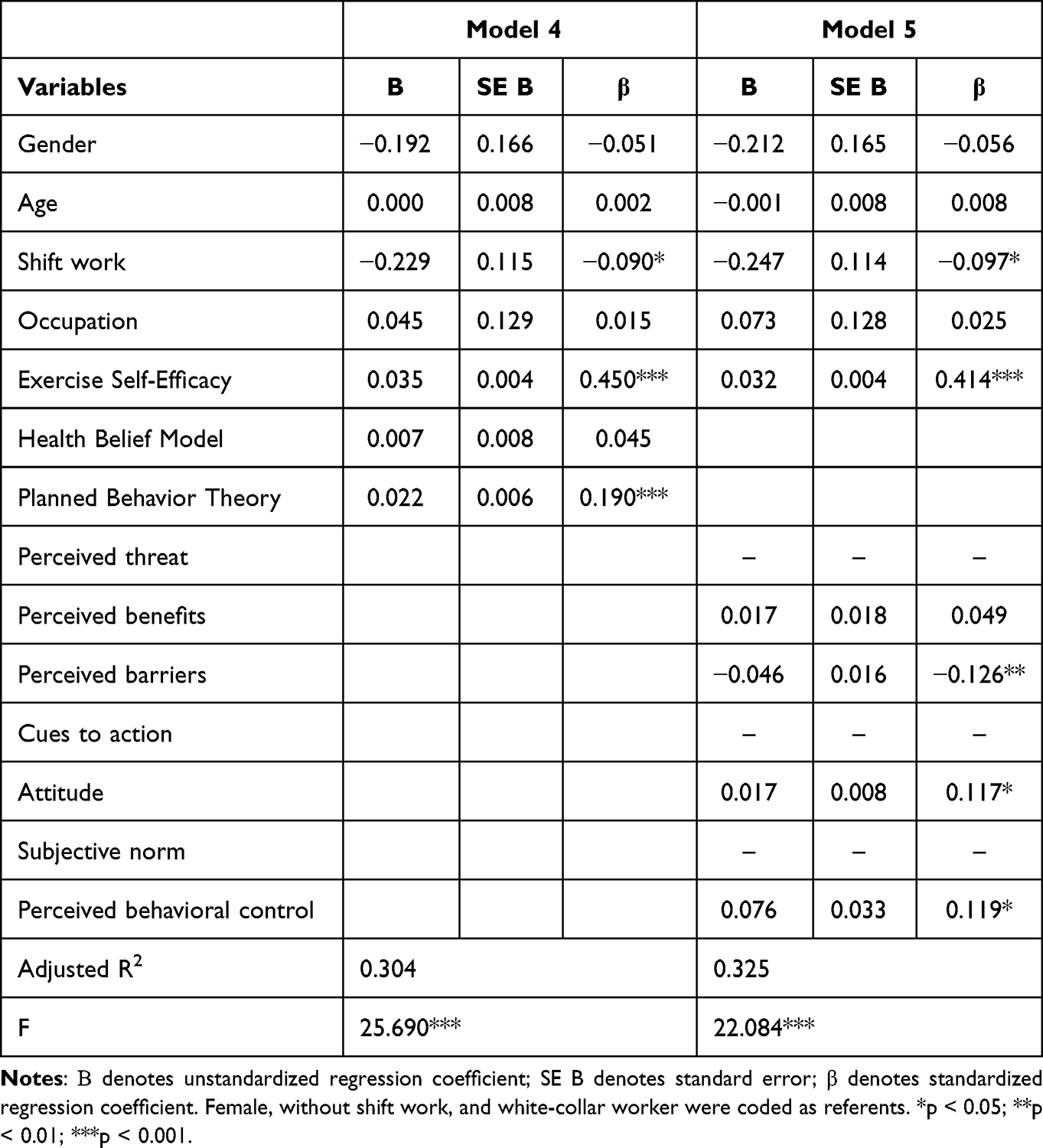 |
Table 4 Summary of Multiple Linear Regressions Predicting Regular Exercise Levels by Three Health Behavior Models Simultaneously |
Discussion
The purpose of this study was to assess the relationship between regular exercise levels and three health behavior models: ESE, HBM, and PBT, among full-time Taiwanese workers. The results showed that only 20.5% of the participants exercised regularly, 37.3% exercised irregularly, and 42.3% did not exercise currently. In the separate multiple linear regression analysis for each health behavior model, ESE, perceived benefits, perceived barriers, attitude, and perceived behavior control have statistically significant relations with workers’ regular exercise behavior. However, perceived threat of disease, cues to action, and subjective norms were not significantly correlated with exercise behavior. In addition, when the three models were considered simultaneously, ESE best explained the variation of regular exercise behavior, followed by PBT, while HBM did not have statistically significant predictive power.
Compared to HBM and PBT, the relationship between ESE and regular exercise behavior was the most statistically significant in this study not only in simple correlation and single-model regression analysis, but also when other models were considered simultaneously. The correlation coefficient and regression coefficient were relatively the highest, showing that the contribution of self-efficacy to the regular exercise behavior would be largest, signifying that when individuals are aware of their abilities to overcome obstacles that may be encountered during the exercise process, they are more likely to maintain regular exercise behavior. Many previous studies have confirmed a positive correlation between ESE and exercise behavior. The higher the ESE, the better the exercise behavior performance.14,15,36 The results of this study once again support the importance of self-efficacy in exercising. Future research should explore how to improve individual ESE.
In the regression analysis of HBM components, perceived barriers and perceived benefits had significant effects in predicting regular exercise behavior, whereas perceived threat of disease and cues to action did not. The statistically significant results of perceived barriers were consistent with most domestic and international studies. When individuals perceive that they will encounter various obstacles and difficulties in executing regular movements, they will significantly reduce their exercise behavior.19,33,36 Regarding the relationship between perceived benefits and exercise behaviors, previous studies have shown inconsistent results. Some studies argue that there is no significant correlation between these two factors, even in those suffering concerned conditions, whose physical health could benefit from exercising.19,37,38 However, other studies with workers as subjects found that perceived benefits and exercise behavior are related with statistical significance.33 The level of regular exercise behavior can be improved by the awareness of health benefits derived by exercise behavior.
The relationship between the perceived threat of disease and exercise was not statistically significant; this is consistent with many studies, of which study subjects included various kinds of population, such as students, workers, elders, or patients.19,33,36 However, prior studies have found that when individuals suffered from a disease and perceived the severity of the health threats, they would more readily adopt beneficial health behaviors.20 Exercise, in general, requires more physical effort, time, and commitment than other healthy lifestyle behaviors. Of health belief factors, perceiving the threat of disease alone seems insufficiently strong enough to motivate individuals to do regular exercise. Like perceived threat of disease, cues to action also appeared to exhibit no significant association with regular exercise behaviors. Cues to action can be internal cues (such as disease symptoms) or external cues (such as mass media reports, interpersonal interactions, and physician recommendations) that trigger the decision-making process to adopt the recommended health behaviors. Taiwan’s Sports Administration has promoted “physical fitness 3-3-3” (exercise at least 3 times a week; at least 30 minutes each time; the heart rate above 130 beats per minute during exercise) for decades. The necessity of exercise for health has been widely advocated for a long time. The effect of stimulus-driven cue might be gradually reduced and cues to prompt action seem no longer to be an important factor in triggering the behavior of exercise.
Perceived behavior control and attitude of the PBT-related components show significant effects in predicting regular exercise behavior. In contrast, subjective norms have no significant effect in predicting regular exercise behavior. The significant findings of this study are consistent with the results of several previous studies.29,30 Furthermore, perceived behavioral control is more closely related to exercise than attitude. Another study with a sample of Taiwanese workers also shows that the stronger the perceived behavioral control ability of the workers toward certain behavior, the stronger their intention to engage in that behavior.39 The effect of perceived behavior control is similar to that of self-efficacy. This perception focuses on an individual’s sense of control over things. On the other hand, subjective norms refer to the perceptions of the social pressures other than an individual sense to shape one’s exercise behavior. In this study, not only subjective norms, but also cues to action have no significant relations to exercise behavior; this finding may indicate that it is more difficult for full-time workers to promote regular exercise behavior through extrinsic feedback.
When the three health behavior models are considered at the same time, the explanatory power of ESE is the best, followed by PBT. HBM was not significant. Self-efficacy has been the most extensively studied and has been regarded as universal for many theories.40–42 Although HBM has been successfully applied to various health behaviors,43,44 HBM cannot fully predict physical activity, especially in young and healthy people.45 HBM has also been found to weakly predict the increases in stages of readiness for physical activities in older adults.36 It may be feasible to go beyond theoretical models and consider the included components of health behavior models when it comes to improving workers’ exercise behavior. In short, when implementing the health promotion program, to be effective, it needs to greatly enhance the individual’s self-confidence in exercise, to strengthen the sense of self-control over things needed to enact the exercise, and to assist in removing obstacles that may be encountered in the implementation of the exercise behavior.
This study follows a rigorous design, but there are still some limitations to be noted. The participants for this study came from the manufacturing industry only, and the sample size is not big. In addition, the workers in this study are mostly white-collar, which produces a gap between the size of the blue-collar worker sample and that of the white-collar worker sample. As a result, it was difficult to avoid the problem of under-represented survey respondents and this study’s generalizability of results may be limited. Furthermore, as this study is a cross-sectional survey, it can only explore the correlation of variables, and cannot infer clear causal relationships; nor can this study represent the long-term conditions of the subjects. Therefore, caution must be exercised in applying the findings.
Conclusion
The present study has delineated the most appropriate health behavior models and their respective elements conducive to establishing a consistent exercise regimen among employed individuals. When all three models were simultaneously considered, ESE emerged as the most suitable model for elucidating variations in regular exercise behavior, followed by PBT, while HBM did not exhibit statistically significant predictive capacity. These findings underscore the potential of transcending theoretical models and emphasize the components embedded within health behavior models to enhance the exercise behavior of workers. Given that ESE, perceived barriers, attitude, and perceived behavioral control significantly correlated with regular exercise levels, practical strategies can be considered. On an individual level, substantial attention should be directed towards bolstering individuals’ self-assurance in engaging in exercise and reinforcing their self-regulation to facilitate exercise participation. Regarding the environment, workplace health promotion initiatives should aim to mitigate barriers that impede the implementation of exercise. Additionally, it is imperative to recognize that solely relying on external stimuli to encourage exercise, social pressures, or highlighting the health risks associated with physical inactivity proves insufficient in fostering consistent exercise habits among employees.
Ethics Approval
This study was approved by the Institutional Review Board of the Chung Shan Medical University Hospital (CSHIRB No: CS18263). Also, the study was conducted in accordance with the guidelines outlined in the Declaration of Helsinki including.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Ottawa charter for health promotion. Available from: https://www.who.int/publications/i/item/WH-1987.
2. World Health Organization. Physical activity. Available from: https://www.who.int/news-room/fact-sheets/detail/physical-activity.
3. Cordes T, Bischoff LL, Schoene D, et al. A multicomponent exercise intervention to improve physical functioning, cognition and psychosocial well-being in elderly nursing home residents: a study protocol of a randomized controlled trial in the PROCARE (prevention and occupational health in long-term care) project. BMC Geriatr. 2019;19(1):369. doi:10.1186/s12877-019-1386-6
4. Galloway MT, Jokl P. Aging successfully: the importance of physical activity in maintaining health and function. J Am Acad Orthop Surg. 2000;8(1):37–44. doi:10.5435/00124635-200001000-00004
5. Hong Y, Li JX, Robinson P. Balance control, flexibility, and cardiorespiratory fitness among older Tai Chi practitioners. Br J Sports Med. 2000;34(1):29–34. doi:10.1136/bjsm.34.1.29
6. Colcombe SJ, Kramer AF, Erickson KI, et al. Cardiovascular fitness, cortical plasticity, and aging. Proc Natl Acad Sci USA. 2004;101(9):3316–3321. doi:10.1073/pnas.0400266101
7. Jonsdottir IH, Rödjer L, Hadzibajramovic E, Börjesson M, Ahlborg G. A prospective study of leisure-time physical activity and mental health in Swedish health care workers and social insurance officers. Prev Med. 2010;51(5):373–377. doi:10.1016/j.ypmed.2010.07.019
8. P-W K, Fox KR, Chen L-J, Chou P. Physical activity and depressive symptoms in older adults: 11-year follow-up. Am J Prev Med. 2012;42(4):355–362. doi:10.1016/j.amepre.2011.11.010
9. Kosteli MC, Williams SE, Cumming J. Investigating the psychosocial determinants of physical activity in older adults: a qualitative approach. Psychol Health. 2016;31(6):730–749. doi:10.1080/08870446.2016.1143943
10. Richman EL, Shaffer DR. If you let me play sports: how might sport participation influence the self‐esteem of adolescent females? Psychol Women Q. 2000;24(2):189–199. doi:10.1111/j.1471-6402.2000.tb00200.x
11. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191. doi:10.1037/0033-295X.84.2.191
12. McAuley E, Lox C, Duncan TE. Long-term maintenance of exercise, self-efficacy, and physiological change in older adults. J Gerontol. 1993;48(4):218–224. doi:10.1093/geronj/48.4.P218
13. Blacklock R, Rhodes R, Blanchard C, Gaul C. Effects of exercise intensity and self-efficacy on state anxiety with breast cancer survivors. Oncol Nurs Forum. 2010;37(2):206–212. doi:10.1188/10.Onf.206-212
14. Rodgers WM, Hall CR, Blanchard CM, McAuley E, Munroe KJ. Task and scheduling self-efficacy as predictors of exercise behavior. Psychol Health. 2002;17(4):405–416. doi:10.1080/0887044022000004902
15. Lane AM, Hall R, Lane J. Self‐efficacy and statistics performance among Sport Studies students. Teach High Educ. 2004;9(4):435–448. doi:10.1080/1356251042000252372
16. McAuley E. The role of efficacy cognitions in the prediction of exercise behavior in middle-aged adults. J Behav Med. 1992;15(1):65–88. doi:10.1007/BF00848378
17. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–335. doi:10.1177/109019817400200403
18. Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice. John Wiley & Sons; 2008.
19. Al-Ali N, Haddad LG. The effect of the health belief model in explaining exercise participation among Jordanian myocardial infarction patients. J Transcult Nurs. 2004;15(2):114–121. doi:10.1177/1043659603262484
20. Brownlee-Duffeck M, Peterson L, Simonds JF, Goldstein D, Kilo C, Hoette S. The role of health beliefs in the regimen adherence and metabolic control of adolescents and adults with diabetes mellitus. J Consult Clin Psychol. 1987;55(2):139. doi:10.1037/0022-006X.55.2.139
21. Wu S, Feng X, Sun X. Development and evaluation of the health belief model scale for exercise. Int J Nurs Sci. 2020;7:S23–S30.
22. Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: an Introduction to Theory and Research. Phil Rhet. 1977;10(2):130–132.
23. Ajzen I. From Intentions to Actions: A Theory of Planned Behavior. Action Control: From Cognition to Behavior. Springer; 1985:11–39.
24. Blue CL. The predictive capacity of the theory of reasoned action and the theory of planned behavior in exercise research: an integrated literature review. Res Nurs Health. 1995;18(2):105–121. doi:10.1002/nur.4770180205
25. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1· 9 million participants. Lancet Glob Health. 2018;6(10):e1077–e1086. doi:10.1016/S2214-109X(18)30357-7
26. Gülü M, Ayyıldız E. Effect of the COVID-19 pandemic on barriers to middle-aged adults’ participation in physical activity in Turkey: a cross-sectional study. J Mens Health. 2022;18(3):60. doi:10.31083/j.jomh1803060
27. Castañeda-Babarro A, Arbillaga-Etxarri A, Gutiérrez-Santamaría B, Coca A. Physical activity change during COVID-19 confinement. Int J Env Res Public Health. 2020;17(18):6878. doi:10.3390/ijerph17186878
28. Bentlage E, Ammar A, How D, et al. Practical recommendations for maintaining active lifestyle during the COVID-19 pandemic: a systematic literature review. Int J Env Res Public Health. 2020;17(17):6265. doi:10.3390/ijerph17176265
29. Caperchione CM, Duncan MJ, Mummery K, Steele R, Schofield G. Mediating relationship between body mass index and the direct measures of the theory of planned behaviour on physical activity intention. Psychol Health Med. 2008;13(2):168–179. doi:10.1080/13548500701426737
30. Fortier MS, Kowal J, Lemyre L, Orpana HM. Intentions and actual physical activity behavior change in a community‐based sample of middle‐aged women: contributions from the theory of planned behavior and self‐determination theory. Int J Sport Exerc Psychol. 2009;7(1):46–67. doi:10.1080/1612197X.2009.9671892
31. Resnick B, Jenkins LS. Testing the reliability and validity of the self-efficacy for exercise scale. Nurs Res. 2000;49(3):154–159. doi:10.1097/00006199-200005000-00007
32. Lee -L-L, Perng S-J, C-C H, Hsu H-M, Lau S-C, Arthur A. A preliminary reliability and validity study of the Chinese version of the self-efficacy for exercise scale for older adults. Int J Nurs Stud. 2009;46(2):230–238. doi:10.1016/j.ijnurstu.2008.09.003
33. Lin C-W, Hsiao T-H. Applying health belief model to investigate factors influencing behavior intention of exercise among employees in high-tech industry. NCYU Phys Educ Health Recreat J. 2015;14(3):57–73.
34. Lin H-L. Regular exercise behavior of university teachers: a perspective of planned behavior theory. Leis Exerc J. 2006;5:9–19.
35. Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol. 1992;47(9):1102–1114. doi:10.1037//0003-066x.47.9.1102
36. Sas-Nowosielski K, Hadzik A, Górna J, Grabara M. Applying the health belief model in explaining the stages of exercise change in older adults. Pol J Sport Tour. 2016;23(4):221–225. doi:10.1515/pjst-2016-0029
37. Jorvand R, Sadeghirad K, Haeri Mehrizi AA, Ghofranipour F, Tavousi M. Determinants of daily exercises among employees with overweight or obesity: the application of health belief model. J Research Health. 2019;9(5):387–393. doi:10.29252/jrh.9.5.387
38. Hatefnia E, Kimiafar M, Moghimbeigi A, Safari-Moradabadi A. Factors predicting physical activity behaviors related to hypertension in overweight male employees: application of health belief model. Health Educ Health Promot. 2023;11(2):311–316.
39. Wu Y-S, Hung W-C, C-H H, Shyu M-L, Huang S-J. A study on physical activity of the employees in financial industry. Health Promot Health Educ. 2013;36:23–40.
40. Rgn AH, Rgn HEW. Role of self efficacy and behaviour change. Int J Nurs Pract. 2002;8(2):106–115. doi:10.1046/j.1440-172x.2002.00352.x
41. Maddux JE, Stanley MA. Self-efficacy theory in contemporary psychology: an overview. J Soc Clin Psychol. 1986;4(3):249–255. doi:10.1521/jscp.1986.4.3.249
42. Strecher VJ, McEvoy DeVellis B, Becker MH, Rosenstock IM. The role of self-efficacy in achieving health behavior change. Health Educ Q. 1986;13(1):73–92. doi:10.1177/109019818601300108
43. Daddario DK. A review of the use of the health belief model for weight management. Medsurg Nurs. 2007;16(6):363.
44. Ross TP, Ross LT, Rahman A, Cataldo S. The bicycle helmet attitudes scale: using the health belief model to predict helmet use among undergraduates. J Am Coll Health. 2010;59(1):29–36. doi:10.1080/07448481.2010.483702
45. Sas-Nowosielski K, Grabara M, Hadzik A. Health Belief Model variables as predictors of light, moderate and vigorous physical activity among young adults. New Educ Rev. 2013;32(2):194.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pain Catastrophizing, Kinesiophobia and Exercise Adherence in Patients After Total Knee Arthroplasty: The Mediating Role of Exercise Self-Efficacy
Zhou Y, Gao W, Gao S, Guo X, Liu M, Cao C
Journal of Pain Research 2023, 16:3993-4004
Published Date: 21 November 2023
Analysis of Determinants Based on the Health Belief Model: A Study Predicting Cognitive Impairment Among Community-Dwelling Older Adults in China
Zhu Q, Xia J, Wang Q, Bai L, Shen C, Yang Y
Journal of Multidisciplinary Healthcare 2026, 19:568925
Published Date: 22 January 2026