")
Back to Journals » Journal of Blood Medicine » Volume 13
Anemia and Associated Factors Among Under Five Year Old Children Who Attended Bule Hora General Hospital in West Guji zone, Southern Ethiopia
Received 4 March 2022
Accepted for publication 29 June 2022
Published 5 July 2022 Volume 2022:13 Pages 395—406
DOI https://doi.org/10.2147/JBM.S363876
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Alqeer Aliyo,1 Abdurezak Jibril2
1Department of Medical Laboratory Science, Bule Hora University, Bule Hora, Ethiopia; 2Department of Nursing, Bule Hora University, Bule Hora, Ethiopia
Correspondence: Alqeer Aliyo, Department of Medical Laboratory Science, Bule Hora University, Bule Hora, Ethiopia, Tel +251 968-467458, Email [email protected]
Background: Anemia is a major global public health public health problem in the early stages of childhood, particularly in developing countries. In Africa, anemia causes higher morbidity and mortality among children less than five years old, especially in Ethiopia.
Objective: This study aimed to assess the prevalence of anemia and its associated factors among children under five years old attending Bule Hora General Hospital, West Guji Zone, southern Ethiopia.
Methods: A hospital-based quantitative cross-sectional study was conducted at Bule Hora General Hospital, Southern Ethiopia from October to November 2020. A convenience sampling technique was used to include 375 under five children enrolled in the study. The pretested structure questionnaire was used to collect socioeconomic and demographic characteristics of study individuals after taking appropriate written informed consent. Then, a venous blood sample was collected from each child and analyzed for hemoglobin determination using a Cell-DYN 1800 machine. Binary logistic regression models were used to identify associated factors of anemia. A P value ≤ 0.05 was considered statistically significant.
Results: The overall prevalence of anemia among under five children was 13.2% (50) [95% CI=5.2– 21.2%] of them anemic children, 11.1% (1) had mild anemia, and 33.3% (3) had moderate anemia and 55.6% (5) had severe anemia. In this study, anemia was significantly associated with recent intestinal protozoan infection [AOR=2.13, 95% CI=1.35– 9.270], malaria infection [AOR=5.42, 95% CI=0.307– 11.034] and soil-transmitted helminths infection [AOR=6.09, 95% CI=2.047– 27.54].
Conclusion: Anemia among under five children in this study was found to be a mild public health problem. It could be managed by preventing malaria infection, intestinal protozoa and soil-transmitted helminthic infection.
Keywords: anemia, under five, Bule Hora, general hospital, West Guji
Introduction
Anemia is a condition that causes a decline in erythrocyte concentration in circulation or hemoglobin in the blood and a concomitant impairment of oxygen transportation.1 The World
The Health Organization (WHO) defined hemoglobin (Hgb)<12 g/dL in adult nonpregnant women, Hgb <11 g/dL in pregnant females, Hgb <13 g/dL in adult men, Hgb <11 g/dl in children aged 6–59 months, Hgb <11.5 g/dl in children aged 5–11 years, Hgb<12 g/dl for children aged 12–14 years and Hgb <13 g/dL in newborns.2,3
Globally, 1.3 billion individuals suffer from anemia, making it one of the most important public health issues on the international agenda.4 Globally, on average, approximately 9.6 million children are severely anemic.5 It affects people in both developing and developed countries.6 By 2017, 293.1 million (47.4%) children under five years of age were anemic worldwide, and 67.6% of these children lived in Africa.1 In Ethiopia, 57% of children are anemic, and 6–59 months is anemic according to the Ethiopian Demographic and Health Survey (EDHS) report.7
Iron deficiency is the major cause of anemia in developing countries and results in insufficient red blood cell production. In some individuals, infections such as peptic ulcers may cause blood loss and anemia. In developing countries, iron deficiency impacts all vulnerable groups. Additionally, geographically specific infections such as malaria and helminthic contribute to excessive red blood cell destruction and cause excessive red blood cell loss. Other infectious diseases may also be at play.8
Anemia impairs mental, physical, and social development and causes negative behavioral and cognitive effects, resulting in poor school performance and work capacity in later years.9 In early childhood, poor feeding habits, especially during the weaning period, exacerbate the problem. Anemia frequently develops as breast milk is replaced by foods that are poor in iron and other nutrients, including vitamin B12 and folic acid. Low oxygenation of brain tissues, a consequence of anemia, may lead to impaired cognitive function, growth and psychomotor development, especially in children. Infants, children under 5 years old and pregnant women have greater susceptibility to anemia because of their increased iron requirements due to rapid body growth and expansion of red blood cells.9 Moreover, anemia leads to immune system compromise, resulting in a decreased ability to fight infections and increased mortality in African children, where resources to determine the basic etiology remain poor.10,11
However, there are national and regional data on the prevalence of anemia and its risk factors among children under five years of age in specific settings in Ethiopia.7 To our knowledge, no previous study has been undertaken in the study area of Bule Hora. Therefore, this study aimed to assess the prevalence of anemia and its associated factors among children from 6–59 months of age in Bule Hora Hospital, southern Ethiopia.
Methodology
Study Area, Period and Design
The health facility-based quantitative cross-sectional study was conducted from October 26 to November 20, 2020, at Bule Hora General Hospital, Guji Zone: Oromia Region, southern Ethiopia. The hospital found in Bule Hora town 467 km from Addis Ababa capital city of Ethiopia. According to the 2007 national census, the total population of Bule Hora town is 27,820. Geographically, the town is located between latitude 5°35ʹN and longitude 38°15ʹE and an altitude of 1716 meters above sea level. Regarding Bule Hora General Hospital, the hospital provides different services, including pediatrics, emergency, delivery, outpatient, patient, laboratory, pharmacy, medical and surgical services. Currently, the hospital has given the service for 5 million people in the area.
Study Population and Selection
All children aged between 6 months and 59 months who attended Bule Hora General Hospital during the data collection period and fulfilled the selection criteria were included in the study. Children who were recently treated or who took iron supplements were excluded from the study.
Sample Size and Sampling Technique
The sample size was determined using a single population proportion formula considering the prevalence of anemia from a previous study 66.8%.12

where d=Margin of error between the sample and the population (d=5%), n=Sample size, Z α/2=95% confident interval (1.96), P=66.8% Prevalence. Then, a 15% nonresponse rate was added considering the response rate of a previous study; thus, the final sample size was 392. A convenience sampling technique was used for all under five children who fulfilled the inclusion criteria during the study period.
Data Collection Instruments and Procedure
The data were collected using a structured questionnaire adapted from previous literature.13 The questionnaire was prepared in English in written form, orally translated into the Afan Oromo and Amharic languages, and then returned to English to ensure its consistency. Five percent of the total sample respondents were interviewed during the pretest in another health institution. After this, the questionnaire was edited accordingly, and then the final version of the questionnaire was adapted to interview children’s parents/caregivers. The data collectors explained the objective of the study to the children’s parents/caregivers. Highlighting on the benefit of being tested for Hgb and what would be done if the child is anemic. The data collectors were given details to the patient/caregiver that no name of participant written on the questionnaire and confidentiality were protected, and verbal consent was obtained. Data were collected through pretested and structured questionnaires by face-to-face interviews with the children’s patients/caregivers (Annex 1). The questionnaire was used to collect sociodemographic data and associated factors.
Blood Sample Collection
By strictly following the standard operating procedure (SOPs), a 3 mL venous blood sample was collected. Experienced laboratory technicians collected the samples in tubes containing ethylenediaminetetraacetic acid (EDTA). The complete blood count (CBC) reports from the hematology analyzer (Cell-DYN 1800) in the hospitals, including hemoglobin (Hgb) analysis, were performed as per the manufacturer’s instructions (Annex 2).
Operational Definitions
Anemia - Hemoglobin (Hgb) <11 g/dL in children whose age is 6–59 months.14
Mild anemia: The Hgb value is 10–10.9 g/dL.14
Moderate anemia: Hgb value 7–9.9 g/dL for children 6–59 months.14
Severe anemia: Hgb value <7 g/dL for children aged 6–59 months.14
Low income: family monthly income less than 750 birr (ETB).15
Moderate income: family monthly income from 750–1500 ETB15
High income: family monthly income greater than 1500 ETB15
Recent infection: Children diagnosed with helminthic, intestinal protozoa and malaria within the last two weeks.
Data Quality Control
To assure data quality, 5% of the estimated sample was pretested at the Bule Hora health center before the data collection to determine whether the questionnaires were simple and understandable. After every data collection, the completeness and consistency of the questionnaire were checked. Data collector training and daily supervision were performed before and during the data collection period.
During blood sample analysis, the standard operating procedures (SOPs) and manufacturers’ instructions were strictly followed for all laboratory activities. The sample was checked for hemolysis, clotting and enough volume before running the test. When the machine passed the control, the samples were analyzed. Finally, the laboratory test result was recorded, and the specimens were managed properly.
Data Processing and Analysis
Data were entered, sorted and categorized. Data cleaning was performed to check for completeness, accuracy, and missed values, and any errors identified were corrected. Then, the data were analyzed using SPSS version 22. Descriptive statistics (mean, frequency) were carried out to describe the sociodemographic status of the participants presented by table, pie chart and graph. A binary logistic regression model was fitted to identify factors associated with anemia. Variables with a P value ≤ 0.25 in the bivariate analysis were considered candidates for the multivariate analysis. Multivariate logistic regression was performed to control for possible confounding and identify the true effect of the selected predictor variables. The model fitness was checked with the Hosmer–Lemeshow test. The extant association between the different variables related to anemia was measured using AOR at 95% CI. A P value ≤ 0.05 was considered statistically significant.
Results
Sociodemographic and Economic Status
Of the 392 children under the age of five, 375 participated in this study, with a 95.7% response rate. The participants’ ages ranged from 6 to 59 months, with a mean (SD) age of 3.3 (± 2.195) months. Among 375 children under the age of five, 54.4% (204) were female, and the majority 39.7% (149) of children’s mothers/caregivers were farmers. More than half, 54.4% (204), were from rural areas. Approximately 29.4% (110) of child caregivers were unable to read and write. Out of 375 children under the age of five, approximately 55.9% (210) were protestants. Almost half of them (44.3%, 166) were living in a household with 3 family members, and the majority of households (36.8%, 138) had incomes less than 750 Ethiopian birr (Table 1).
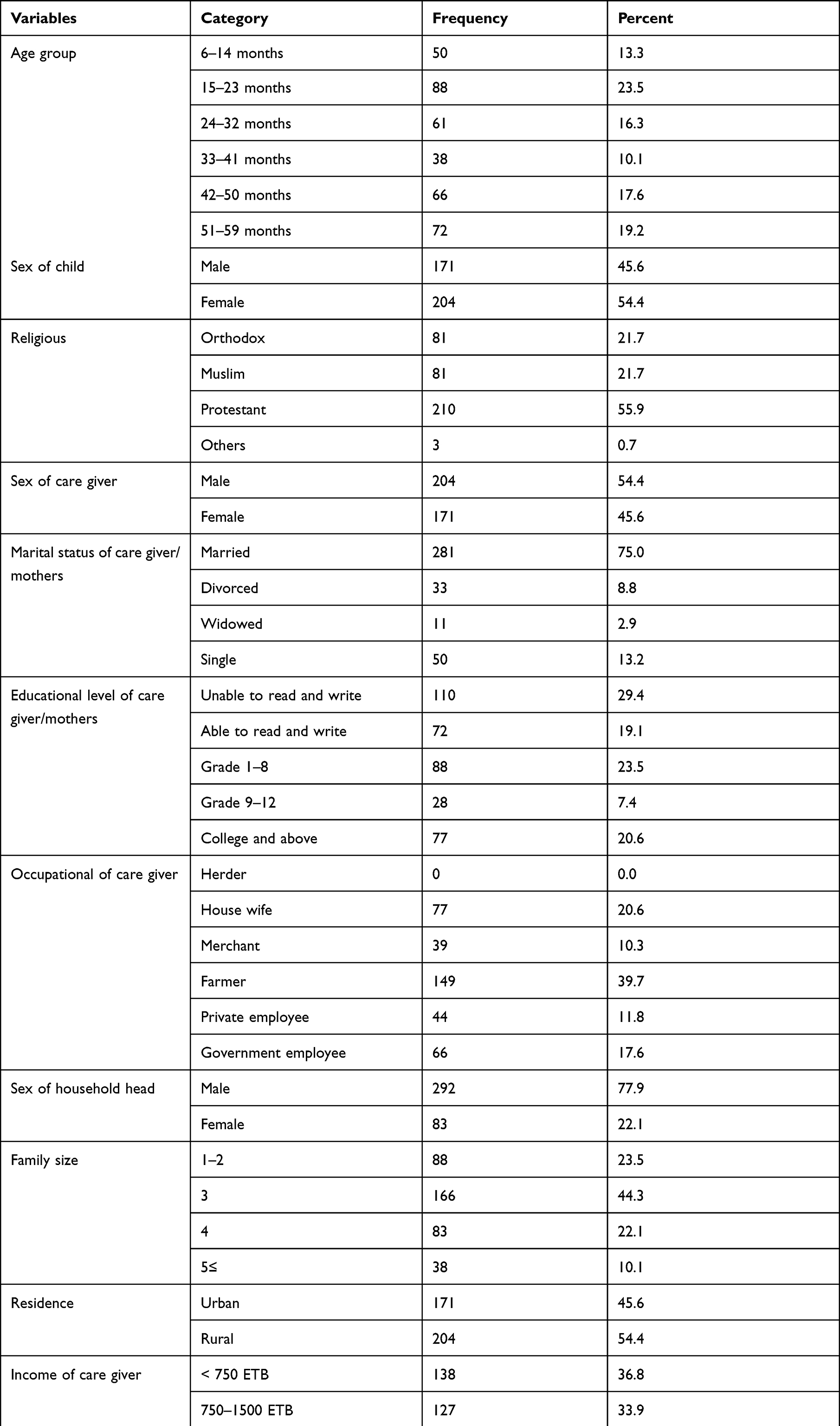 |
Table 1 Sociodemographic and Other Selected Characteristics of Under Five Year Old Children Attended Bule Hora General Hospital |
Feeding-Related Factors
Regarding feeding practices, among 375 under five children 69.1% (259) dietary diversity practice, 79.4% (298) introduction of complementary food after 6 months, 61.8% (232) mothers/caregivers do not have nutritional knowledge, 23.5% (88) faces food insecurity within four weeks, 69.2% (259) had meal three times feed per day while majority 80.8% (303) breastfeeding practice at 6–12 months (Table 2).
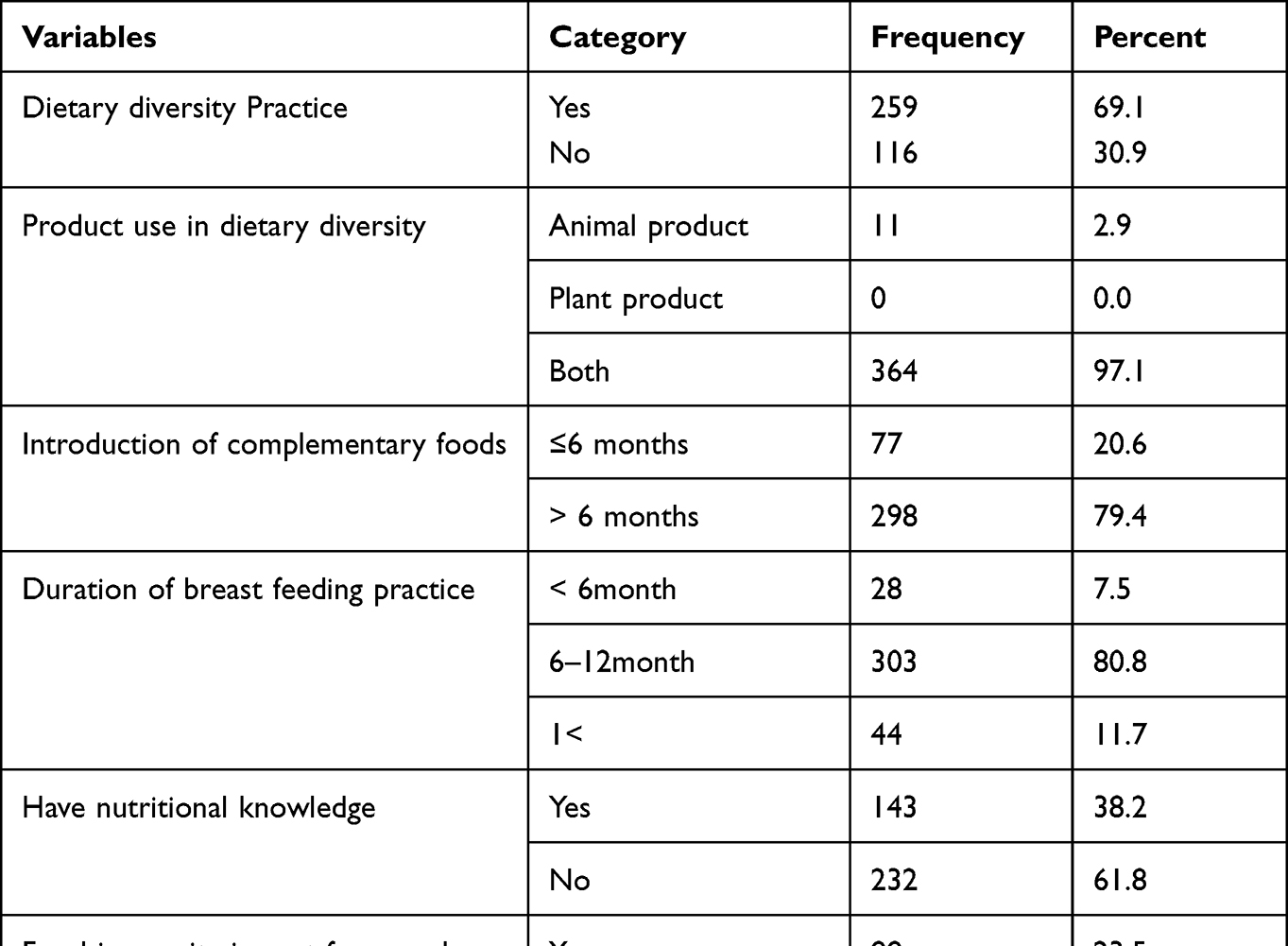 |
Table 2 Feeding-Related Factor Characteristics of Children Attended Bule Hora General Hospital |
Health Care and Disease Characteristics
Out of 375 under five children enrolled in the study, 17.6% (66) had intestinal protozoa followed by soil-transmitted helminthic infection 16.2% (61) and malaria infection 14.7% (55) (Table 3).
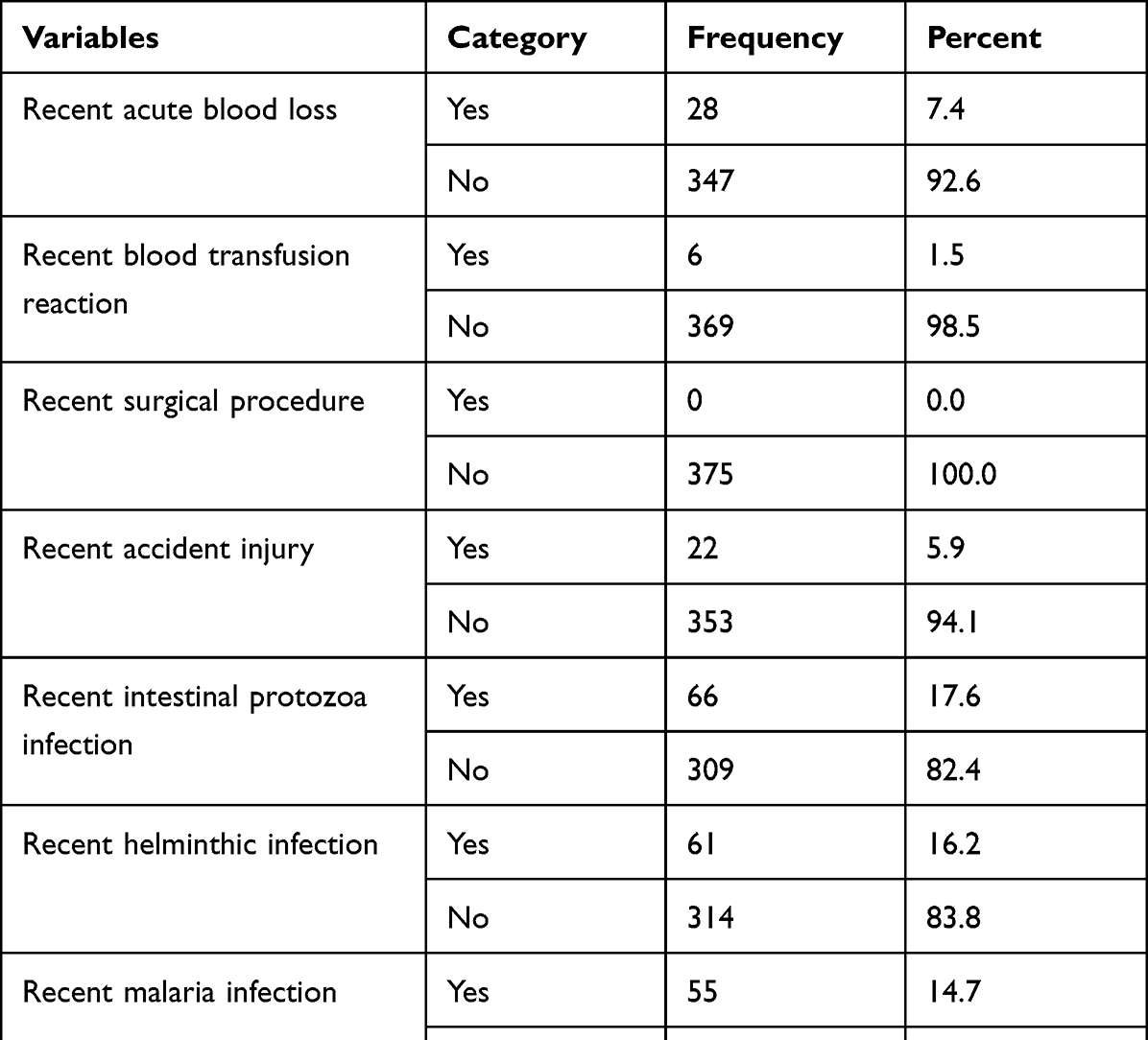 |
Table 3 Clinical Characteristics of Children Who Attended Bule Hora General Hospital |
Prevalence of Anemia
Based on the hemoglobin cutoff value, less than 11 g/dL was categorized as anemic, and Hgb values of 10–10.9 g/dl, 7–9.9 g/dl, and less than 7 g/dL were determined to be mild, moderate and severe, respectively.16 The overall prevalence of anemia was 13.2% (50) (Figure 1). Among anemic children under five years of age, 12% (6) were mild, 32% (16) were moderate and 56% (28) were severe (Figure 2).
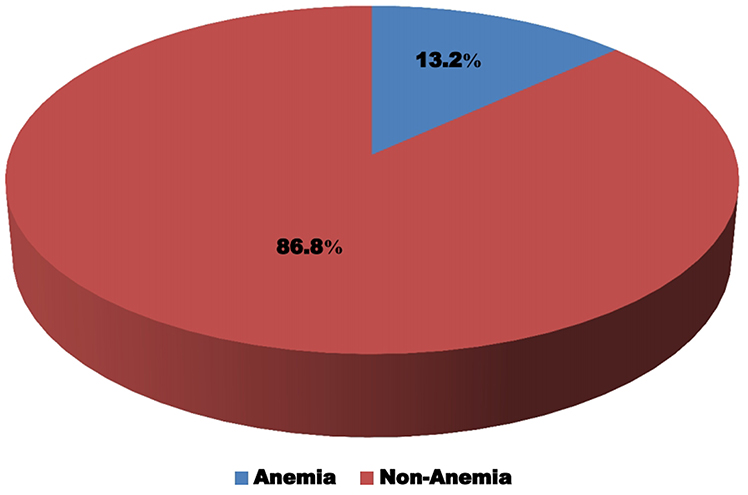 |
Figure 1 This figure shows the anemia among under five year old children attended Bule Hora General Hospital. Anemia is children scores hemoglobin less than 11 g/dL and non-anemia children score hemoglobin greater than or equal to11 g/dL. |
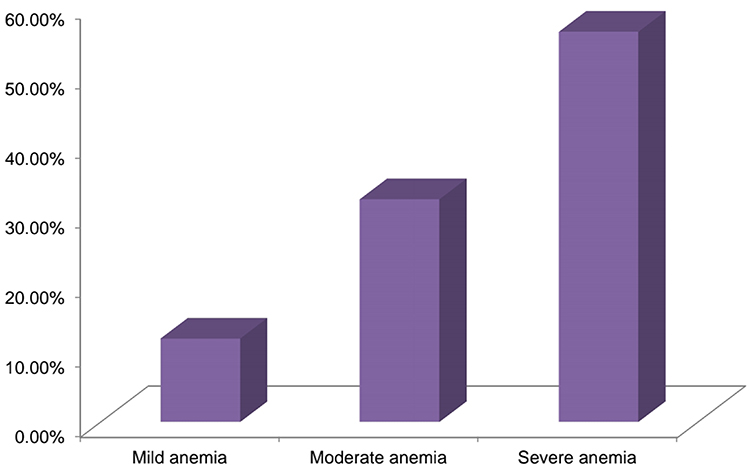 |
Figure 2 Anemic level among under five year old children attended Bule Hora General Hospital. Anemic children scores hemoglobin values of 10–10.9 g/dl were mild anemia, 7–9.9 g/dl were moderate anemia, and less than 7 g/dL were determined severe anemia. |
Factor Associated with Prevalence of Anemia
In bivariate analysis, variables such as child age group, child sex, family size, income of caregiver, dietary diversity practice, breastfeeding practice, nutritional knowledge, meal frequency, recent intestinal protozoan infection, recent helminthic infection, and recent malaria infection had a p value of <0.25 and were considered candidates for multivariate analysis. In multivariate analysis, the chance of having anemia was approximately 2 times higher among children under the age of five who had recent intestinal protozoan infection [AOR= 2.13, 95% CI =1.35–9.270] than among their counterparts. Additionally, children who had recent soil-transmitted helminths infections were 6 times more likely to have anemia [AOR=6.09, 95% CI=2.047–27.54] than their counterparts. Similarly, the children who had recent malaria infection were nearly 5 times more likely [AOR=5.42, 95% CI=0.307–11.034] to have anemic than those who did not have recent malaria infection (Table 4).
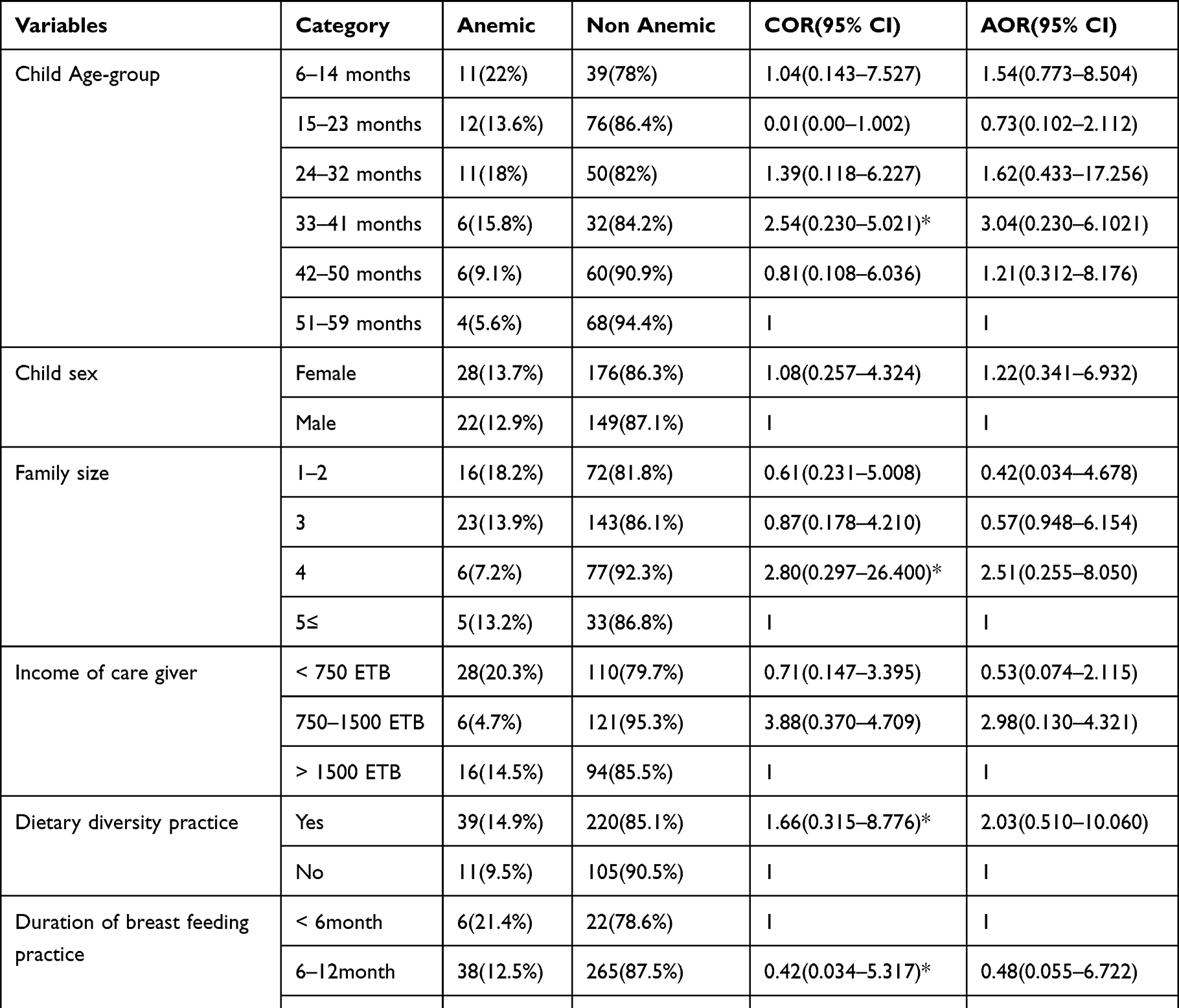 |
Table 4 Bivariate and Multivariate Analyses of Factors Associated with the Prevalence of Anemia in Among Under five Children Attended at Bule Hora General Hospital, Southern Ethiopia |
Discussion
In this study, the overall prevalence of anemia among under five children attending Bule Hora General Hospital was 13.2% (50) (95% CI=5.2–21.2%). According to the WHO definition, anemia can be defined as a mild, moderate and severe public health problem when the prevalence is 5–19.9%, 20–39.9% and greater than 40%, respectively. Therefore, the prevalence of anemia in this study is considered a mild public health concern.17
This is lower than the previous study conducted in Western China (51.2%),18 Eastern Sudan (86%),19 Cape Verde West Africa (51.8%),20 Nigeria (70.5%),21 Tanzania (77.2%),22 Gonder town Ethiopia (66.8%),23 Gonder, Ethiopia (58.6%),24 Wagmra zone, Ethiopia (66.6%),25 and South Wollo, Northeast Ethiopia (41.1%).15 The difference in prevalence might be due to variations in the number of participants, sample analysis equipment, hemoglobin cutoff points, and cultural, geographical and behavioral characteristics of the community. In contrast, this finding was higher than reports from Brazil (10.2%)26 and Sub-Sahara Africa (9.7%).27 The possible reason might be due to the age difference of the study participants. In our study, the study participants were aged from 6–59 months, but in Sub-Saharan Africa, the study participants were aged below 36 months.
Multivariate analysis showed that having a previous intestinal protozoan infection was significantly associated with the prevalence of anemia among under five children. This finding is in line with a study conducted in Pawe town, Benishangul Gumuz, region28 and Gonder, Ethiopia.24 Similarly, children who had previous malaria infection were significantly associated with anemia among under five children. This finding agrees with a study conducted in Ghana.29
In addition, anemia was 6 times more likely among children with previous soil-transmitted helminthic infections than among their counterparts. This finding is consistent with a study conducted in Gonder, Ethiopia.23 Possible justification could be due to intestinal wall bleeding, erythrocyte lysis, reduction of iron and damaged organs involved in hematopoiesis.
Out of 375 children under five years of age involved in the study, nearly half (48.5%, 182) were infected with at least one of the following species of parasites: Plasmodium spp., Entamoeba histolytical, Giardia lambia, Ascaris lumbricoides, Strongyloides stercoralis, Trichuris trichuria, Enterobius vermicularis and Hookworm. Of those children infected with recent malaria, 22 (40%), soil-transmitted helminths, 22 (36.1%) and intestinal protozoa 11 (16.7%) were found to be anemic. The parasite species may deplete red blood cells through loss of blood in the time of diarrhea and gastrointestinal bleeding.
Strength of the Study
This research could elaborate the important part of health accessibility issues, especially in child health, and identified associated factors of anemia.
Limitations of the Study
As a hospital-based study with convenience sampling technique was applied, and a small sample size was used, the result cannot be extrapolated to a larger community. Additionally, this study does not differentiate the types of anemia such as hemolytic, sickle cell, thalassemia and so on.
Conclusion
The present study demonstrated a 13.2% overall prevalence of anemia among children under the age of 5 who attended Bule Hora General Hospital. This finding was low compared with previous studies conducted in different parts of Ethiopia. The factors significantly associated with anemia were recent intestinal protozoan infections, soil-transmitted helminths, and malaria infection. Therefore, early diagnosis, treatment and prevention of parasite infection should be important in the reduction of anemia among under five children.
Abbreviations
CBC, complete blood count; EDTA, ethylene diamine tetraacetic acid; HGB, hemoglobin; g/dL, gram per deciliter; SOPS, standard operation procedures; AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; WHO, World Health Organization; EDHS, Ethiopian Demographic Health Survey; SPSS, Statistical Package for Social Science; ETB, Ethiopian Birr.
Data Sharing Statement
Data essential for the conclusion are included in this manuscript. Additional data can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was conducted after ethical approval from the Bule Hora University Research and Ethical Review Committee. The official letter was written to Bule Hora General Hospital. Informed, voluntary, written signed consent was obtained from the study participant, parent/caregiver and institution. The children’s parents/caregivers were informed about the purpose of the study, and written informed consent was obtained before the questionnaire was administered based on Helsinki declaration. Then, blood samples were collected from the study participant. Participation in the study was voluntary. The participants were informed of their right to quite/refuse their participation at any stage of the study if they did not want to participate. To ensure confidentiality of participant information, codes were used, and any identifier of participants was not written on the questionnaire on the test tube. Any abnormal test results of participants were communicated to the concerned body.
Acknowledgments
First, we would like to thank Bule Hora University, College of Medicine and Health Sciences, Department of Nursing for giving us the chance to undertake this research. Next, we would like to extend our thanks to Bule Hora University nursing department staff Mr. Yonas Dessie who guided and provided us with different information for enriching our research development and Bule Hora General Hospital staff for their unlimited cooperation in giving us information to develop the research. Finally, we would like to extend gratitude to our beloved family and friends for valuable patience during research development.
Author Contributions
All authors made a significant contribution in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no specific funding for this study.
Disclosure
We declare that we do not have any conflicts of interest related to this work or any activities pertaining to this research work.
References
1. McLean E, Cogswell M, Egli I, Wojdyla D, De Benoist B. Worldwide prevalence of anemia, WHO vitamin and mineral nutrition information system, 1993–2005. Public Health Nutr. 2009;12(4):444–454. doi:10.1017/S1368980008002401
2. Kratz A, Ferraro M, Sluss PM, Lewandrowski KB. Normal reference laboratory values. N Engl J Med. 2004;351(15):1548–1563. doi:10.1056/NEJMcpc049016
3. Uthman E. Understanding Anemia. Univ. Press of Mississippi; 2009.
4. Allen LH. Biological mechanisms that might underlie iron’s effects on fetal growth and preterm birth. J Nutr. 2001;131(2):581S–589S. doi:10.1093/jn/131.2.581S
5. World Health Organization. The Global Prevalence of Anemia in 2011. Geneva: World Health Organization; 2015.
6. Mainasara A, Ibrahim K, Uko E, et al. Prevalence of anemia among children attending pediatrics department of UDUTH, Sokoto, North-Western Nigeria. IBRR. 2017;7(1):1. doi:10.9734/IBRR/2017/29225
7. Central Statistical Agency [Ethiopia], ICF International. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: Central Statistical Agency [Ethiopia], ICF International; 2017.
8. Knowledge SUCCESS. Anemia prevalence, causes, and consequences. Available from: https://www.k4health.org/toolkits/anemia-prevention/anemia-causes-prevalence-impact.
9. Santos RF, Gonzalez ES, Albuquerque EC, et al. Prevalence of anemia in under five-year-old children in a children’s hospital in Recife, Brazil. Rev Bras Hematol Hemoter. 2011;33(2):100–104. doi:10.5581/1516-8484.20110028
10. Alderman H, Behrman JR, Kohler HP, Maluccio JA, Watkins SC. Attrition in longitudinal household survey data: some tests for three developing-country samples. Demogr Res. 2001;5:79–124. doi:10.4054/DemRes.2001.5.4
11. Brabin BJ, Premji Z, Verhoeff F. An analysis of anemia and child mortality. J Nutr. 2001;131(2):636S–48S. doi:10.1093/jn/131.2.636S
12. Abdisa B, Dessalegn N. Prevalence of anemia and associated factor among under five children in Bedele Hospital, Iluababor Zone, Oromia Regional State South West Ethiopia. Int J Dev Res. 2016;8:14652.
13. Gebereselassie Y, BirhanSelassie M, Menjetta T, Alemu J, Tsegaye A. Magnitude, severity, and associated factors of anemia among under-five children attending Hawassa University Teaching and Referral Hospital, Hawassa, Southern Ethiopia, 2016. Anemia. 2020;2020:1–6. doi:10.1155/2020/7580104
14. Rodak BF, Keohane EM, Fritsma GA. Hematology-E-Book: clinical Principles and Applications. Elsevier Health Sciences; 2013.
15. Gebreweld A, Ali N, Ali R, Fisha T, Adu-Afarwuah S. Prevalence of anemia and its associated factors among children under five years of age attending at Guguftu health center, South Wollo, Northeast Ethiopia. PLoS One. 2019;14(7):e0218961. doi:10.1371/journal.pone.0218961
16. Longanbach S, Miers MK, Keohane EM, Smith LJ, Walenga JM. Rodak’s hematology: clinical principles and applications. 2016:208–234.
17. Ahmed RA, Osman IM. Clinical and hematological pattern of chronic lymphocytic leukemia in sudanese patients. Int Blood Res Rev. 2017;7(1):1–10. doi:10.9734/IBRR/2017/31359
18. Gao W, Yan H, Dang S, Pei L, Pei L. Severity of anemia among children under 36 months old in rural western China. PLoS One. 2013;8(4):e62883. doi:10.1371/journal.pone.0062883
19. Mahmoud H, Muddathir A, Osman S, et al. Iron deficiency anemia among children under three years in Kassala, Eastern Sudan. Sudanese J Pub Health. 2014;9:33–37.
20. Semedo RM, Santos MM, Baião MR, Luiz RR, da Veiga GV. Prevalence of anemia and associated factors among children below five years of age in Cape Verde, West Africa. J Health Popul Nutr. 2014;32(4):646.
21. Oladeinde BH, Omoregie R, Olley M, Anunibe JA, Onifade AA, Oladeinde OB. Malaria and anemia among children in a low resource setting in Nigeria. Iran J Parasitol. 2012;7(3):31.
22. Simbauranga RH, Kamugisha E, Hokororo A, Kidenya BR, Makani J. Prevalence and factors associated with severe anemia among underfive children hospitalized at Bugando Medical Centre, Mwanza, Tanzania. BMC Hematol. 2015;15(1):1–9. doi:10.1186/s12878-015-0033-5
23. Getaneh Z, Enawgaw B, Engidaye G, et al. Prevalence of anemia and associated factors among school children in Gondar town public primary schools, northwest Ethiopia: a school-based cross-sectional study. PLoS One. 2017;12(12):e0190151. doi:10.1371/journal.pone.0190151
24. Enawgaw B, Workineh Y, Tadesse S, Mekuria E, Addisu A, Genetu M. Prevalence of anemia and associated factors among hospitalized children attending the University of Gondar Hospital, Northwest Ethiopia. EJIFCC. 2019;30(1):35.
25. Woldie H, Kebede Y, Tariku A. Factors associated with anemia among children aged 6–23 months attending growth monitoring at Tsitsika Health Center, Wag-Himra Zone, Northeast Ethiopia. J Nutr Metab. 2015;2015:1–9. doi:10.1155/2015/928632
26. Novaes TG, Gomes AT, Silveira KC, et al. Prevalence and factors associated with anemia in children enrolled in daycare centers: a hierarchical analysis. Revista Paulista de Pediatria. 2017;35:281–288. doi:10.1590/1984-0462/;2017;35;3;00008
27. Muoneke VU, Ibekwe RC, Nebe-Agumadu HU, Ibe BC. Factors associated with mortality in underfive children with severe anemia in Ebonyi, Nigeria. Indian Pediatr. 2012;49(2):119–123. doi:10.1007/s13312-012-0026-4
28. Birhanu M, Gedefaw L, Asres Y. Anemia among school-age children: magnitude, severity and associated factors in Pawe town, Benishangul-Gumuz region, Northwest Ethiopia. Ethiop J Health Sci. 2018;28(3):259–266. doi:10.4314/ejhs.v28i3.3
29. Parbey PA, Tarkang E, Manu E, et al. Risk factors for anemia among children under five years in the Hohoe municipality, Ghana: a case control study. Anemia. 2019;2019:1–9. doi:10.1155/2019/2139717
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.