Back to Journals » Journal of Pain Research » Volume 15
An Advanced Practice Provider Guide to Peripheral Nerve Stimulation
Authors Hoffmann CM ![]() , D'Souza RS
, D'Souza RS ![]() , Hagedorn JM
, Hagedorn JM ![]()
Received 26 April 2022
Accepted for publication 23 July 2022
Published 7 August 2022 Volume 2022:15 Pages 2283—2291
DOI https://doi.org/10.2147/JPR.S370037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Andrea Tinnirello
Chelsey M Hoffmann,1 Ryan S D’Souza,1 Jonathan M Hagedorn2
1Department of Anesthesiology and Perioperative Medicine, Division of Pain Medicine, Mayo Clinic, Rochester, MN, USA; 2Department of Pain Medicine, iSpine Pain Physicians, Maple Grove, MN, USA
Correspondence: Chelsey M Hoffmann, Tel +1 507-422-6378, Fax +1 507-266-7732, Email [email protected]
Objective: To describe the team approach of an interventional pain management practice, with particular emphasis on advanced practice providers (APPs), in the selection, education, care, and management of peripheral nerve stimulation (PNS) patients.
Materials and Methods: We devised an APP guide to PNS based on an in-depth search of multiple databases for studies on neuromodulation, pain management, and APPs.
Results: Of 65 articles captured in the search strategy, three articles were pertinent to the topic of APP involvement in neuromodulation. More specifically, only one of the three publications on neuromodulation discussed APP involvement in PNS. This single publication was from 1995 and focused on electrical stimulation of the trigeminal ganglion using a permanent percutaneously placed electrode.
Conclusion: PNS is growing in clinical indication and use for both acute and chronic pain conditions. With the increasing need for APPs in both general and specialty medicine, it is imperative that APPs are well educated on PNS. Here, we have outlined ways in which APPs can optimize the care of PNS patients and how the skillset of the APP in a PNS practice can potentially improve patient outcomes.
Keywords: advanced practice provider, peripheral nerve stimulation, interventional pain management, nurse practitioner, physician assistant
Introduction
Peripheral nerve stimulation (PNS) is becoming a more frequent treatment modality for patients suffering from both acute and chronic pain conditions. Additionally, PNS has been utilized to offer substantial analgesia in challenging pain conditions including complex regional pain syndrome,1 postherpetic neuralgia,2 cranial neuralgias,3 migraines and cluster headaches,4 amputee pain,5 back pain,6 and cancer-related pain.7 PNS implants may be temporary (60 days) or permanent.
Most pain management practices utilize a comprehensive care team model consisting of nurses, APPs (ie, nurse practitioners (NPs) and physician assistants (PAs)), mental health specialists, and physicians. In the article The Team Approach to Spinal Cord and Dorsal Root Ganglion Stimulation: A Guide for the Advanced Practice Provider,8 the authors explored the role of APPs in the use and management of spinal cord and dorsal root ganglion stimulation. Furthermore, the paper explains how APPs are improving access for treatment of patients suffering from chronic pain.
In Contribution of physician assistants/associates to secondary care: a systematic review,9 the authors found PAs achieve the objective of increasing throughput of patients, while containing costs and without adversely affecting outcomes. Another article, Physician assistants reduce resident workload and improve care in an academic surgical setting, found the addition of PAs to the surgical team resulted in decreased late planned discharges, increased unplanned early discharges with earlier reassessment and/or coordination of care, decreased resident workload and improved resident rotation satisfaction. Specifically, implementation of PAs on a general surgery service resulted in a significant decrease in late discharges from 20% to 0.5% and increased unplanned early discharges from 0.5% to 16%.10 Lastly, Physician Assistants and Nurse Practitioners in Primary Care Plus: A Systematic Review investigated the use of a primary care plus (specialist care provided in the primary care/community care setting) services provided by a PA and/or NP. The authors found “the quality of care, both at the patient-level and professional-level, appears to be guaranteed with possibly better access to healthcare and fewer referrals to the hospital.”11
As PNS has increased in frequency of use, there has been a unique opportunity and need for a higher degree of APP involvement in the care and management of this patient population. Here, we will explore the specific role of APPs in a PNS implanting pain management practice while also discussing the findings of an in-depth literature review investigating APP involvement in neuromodulation.
Methods
A comprehensive search of several databases from each database’s inception to April 6th, 2022, was conducted and filtered to capture only articles in the English language. The databases included Ovid MEDLINE(R), Ovid EMBASE, Ovid Cochrane Central Register of Controlled Trials, and Ovid Cochrane Database of Systematic Reviews. The search strategy was designed and conducted by an experienced librarian, L.P. Database subject headings supplemented with keywords were used to search for “advanced practice providers”, “nurse practitioners”, “physician assistants”, “pain management”, and “neuromodulation”.
Results
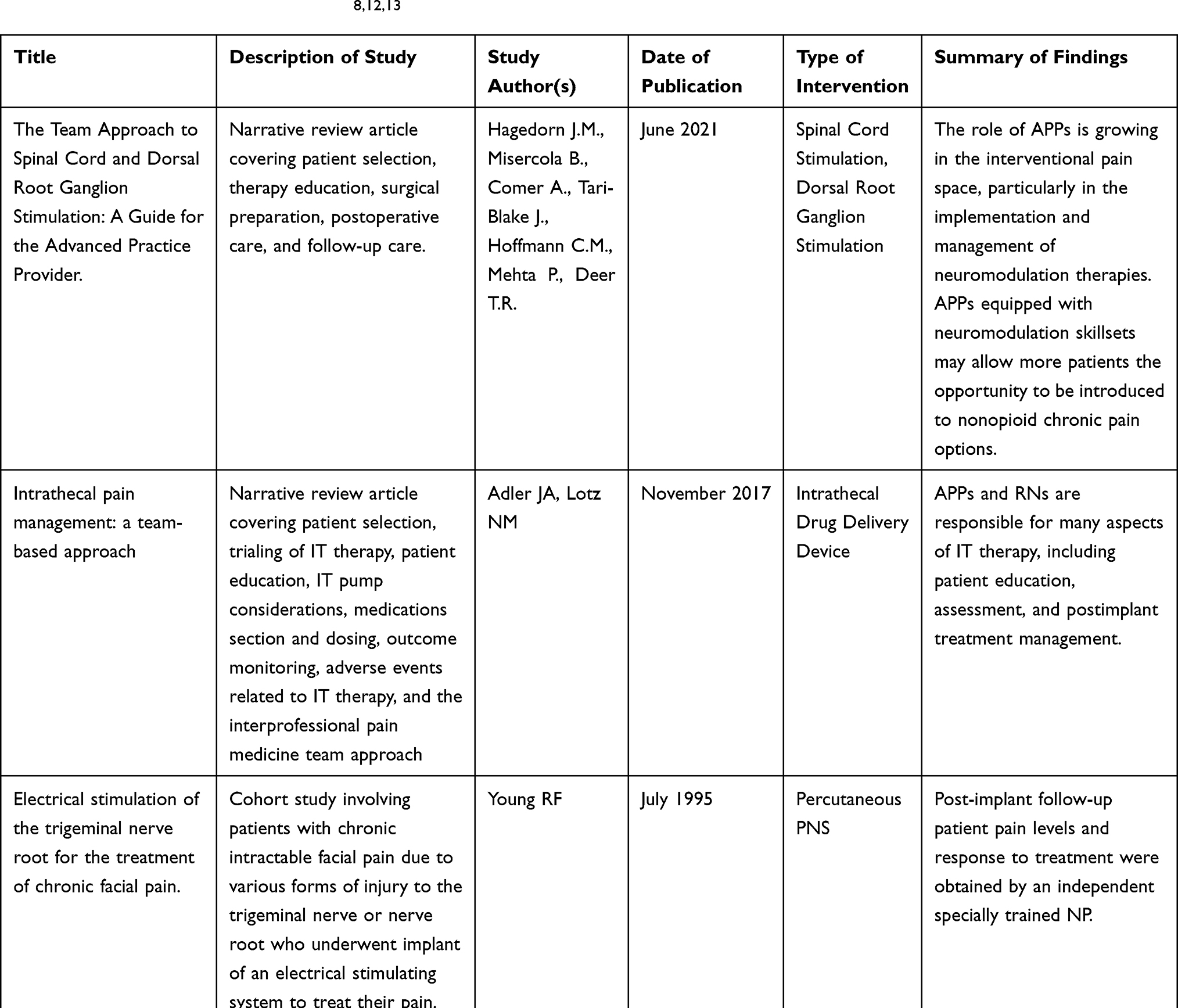
The literature review resulted in 65 articles pertinent to neuromodulation, pain management and APPs. Of these articles, only three were pertinent to the topic of APP involvement in neuromodulation (see Table 1). More specifically, only one of the three publications on neuromodulation discussed APP involvement in PNS. This single publication was from 1995 and focused on electrical stimulation of the trigeminal ganglion using a permanent percutaneously placed electrode. In the study, the NP was involved in following patients post-implant to obtain pain levels and response to treatment. The other two studies well-describe the importance of APP involvement and the role of the APP in caring for patients with implanted intrathecal drug delivery devices, spinal cord, or dorsal root ganglion stimulators. All three studies agree that APPs play a significant role in the post-implant follow-up of patients with neuromodulation devices.
 |
Patient Selection
The first opportunity for APPs to be involved in the care of PNS patients is at the time of appropriate patient selection. In many practices, APPs triage pain management consult requests and are the first to review a patient’s past medical and surgical history, medications, allergies, and prior imaging. It is during this initial step when APPs may recognize and identify patients with a pain diagnosis who may benefit from PNS. It is imperative that the APP is educated on proper indications for PNS (ie, mononeuropathy is preferable rather than polyneuropathy or widespread pain distributions). In the setting of more diffuse pain in an extremity, the APP may identify the area that is most painful and consider offering PNS to target up to two separate nerves that innervate that region. Prognostic risk factors associated with outcomes from PNS are lacking. However, the general neuromodulation literature on dorsal column spinal cord stimulation and dorsal root ganglion spinal cord stimulation highlights potential predictors of poor pain relief including younger age, history of tobacco use, history of substance use disorder, mental health disorders (posttraumatic stress disorder, depression, anxiety), history of litigation or worker’s compensation, and other variables.14–17 Consultation with a psychiatrist or psychologist is important to determine if a patient has uncontrolled mental health or behavioral health issues that may make the patient a poor candidate for an implanted PNS device. However, solely having a formal diagnosis of a mental health or behavioral issue is not a contraindication to PNS implantation if those conditions are adequately treated and optimized.
Once an appropriate PNS candidate is identified during the triage process, the APP may be able to provide guidance to scheduling staff regarding appointment arrangements, such as offering the patient a consultation with an APP or implanting physician, arranging for a diagnostic peripheral nerve block targeting the region of the patient’s pain (if this is standard of care in the practice), scheduling a mental health assessment, and providing resources for PNS education (eg, education session with nursing staff).
Consultation with APP and Implanting Physician
At the time of initial consultation with a patient who is a potential candidate for PNS implant, the APP plays a primary role in obtaining a thorough past medical history and description of the patient’s pain symptoms. The APP should properly diagnose and assess the patient’s neuropathic pain. This begins with awareness of the neuropathic grading system (ie, possible, probable, or definite neuropathic pain), associated criteria and available screening instruments.18 Screening instruments for the diagnosis of neuropathic pain include, but are not limited to, the Leeds assessment of neuropathic symptoms and signs (LANSS) Pain Scale,19 the neuropathic pain questionnaire,20 the douleur neuropathique 4 questions (DN4),21 the painDETECT questionnaire (PD-Q),22 and ID-Pain.23
During the initial consult, the APP should screen for contraindications for the use of PNS, which include coagulopathy, current infections, significant behavioral or mental health issues that are not optimized, a failed diagnostic trial, requirement of periodic MRIs, and complete sensory loss.24 Most targets for PNS therapy are superficial peripheral nerves and are considered low risk for bleeding complications; thus, exceptions may be made to pursue PNS therapy in patients who are on anticoagulation therapy for low-risk targets, which are consistent with published guidelines.25,26 Furthermore, failed diagnostic peripheral nerve blockade is not an absolute contraindication to pursuing PNS therapy. Due to both peripheral and central neuromodulation mechanisms, patients may still benefit from PNS therapy despite not achieving adequate analgesia from the anesthetic phase from diagnostic trial blocks.
Additionally, the APP should be able to identify the specific peripheral nerve targets for potential PNS implant. In more generalized painful conditions, with regions innervated by several peripheral nerves, the APP is tasked with determining which specific peripheral nerve targets contribute most to the patient’s pain. Lastly, the APP should ensure the patient has updated imaging of the peripheral nerve target area and assess if electrodiagnostic studies reveal abnormalities in nerve conduction of the target peripheral nerve.
The APP may follow the suggested criteria for PNS patient selection, displayed in Table 2, which have been revised from the article titled Current Innovations in Peripheral Nerve Stimulation published in 2018 by Raghavendra Nayak and Ratan K. Banik.24
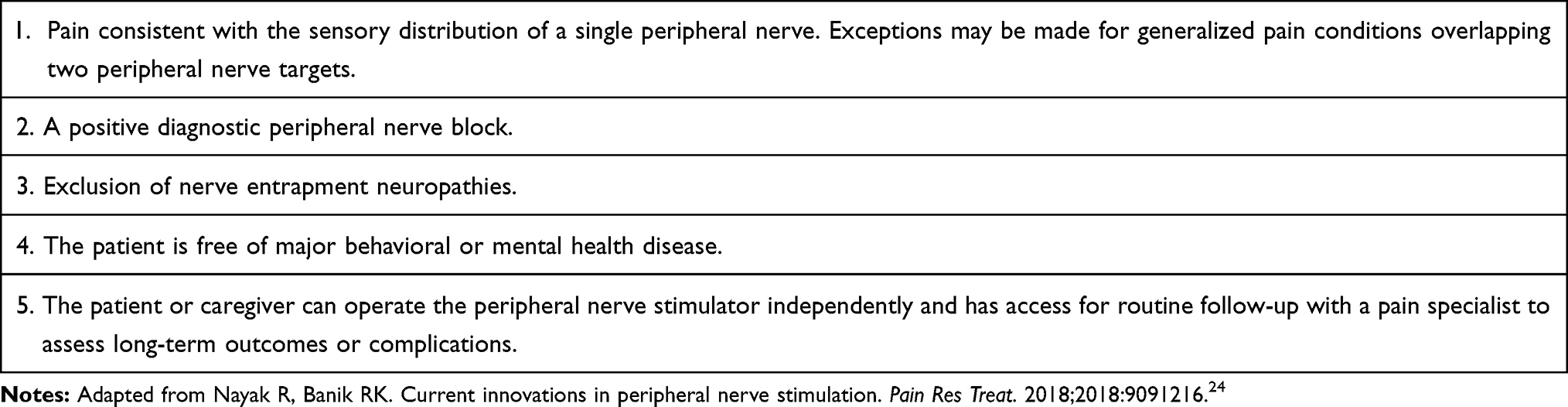 |
Table 2 Suggested Criteria for Peripheral Nerve Stimulator Patient Selection |
Here, a suggestion is made to add a fifth criteria for PNS patient selection – that of the ability to operate the device remote and navigate device charging requirements (if applicable). Occasionally, patients with severely arthritic hands or underlying medical conditions may not have the dexterity to operate these devices on their own without support from a family member or caregiver. Also, patients need to have a baseline level of cognition to allow for device education and optimization, and the ability to self-adjust device settings based on pain and activity levels. Moreover, many PNS devices require the patient to routinely change dressings, which again may be difficult depending upon the site of device placement, the patient’s range of motion, and cognitive status.
The APP can document prior treatments which may include conservative treatments (physical therapy, acupuncture, massage, and topical creams/ointments), oral medications (narcotics and non-narcotics), interventional treatments (diagnostic and therapeutic nerve blocks). This information can be extremely important when attempting to obtain insurance coverage of the PNS implant.
The APP is in a unique position during initial PNS consultation to discuss the patient’s goals. Emphasis on functional goals in addition to pain reduction goals is extremely important. Functional goal examples include sleep habits, walking distance, work status, and patient-specific goals. Goal discussion and documentation are extremely valuable to ensure the patient has realistic expectations following PNS implant. For example, APPs may need to re-emphasize that achievement of 100% pain relief may be difficult and the APP may need to work further with the patient to develop and document the patient’s defined meaningful pain relief, expressed as a percentage. This information is also helpful to review post-PNS implant or at the end of temporary PNS treatment to record the degree of success with therapy. It is also important to explain evidence-based PNS outcomes to patients based upon current research. For example, APPs can discuss available research supporting sustained pain relief follow end of therapy for 60-day temporary percutaneous PNS.27,28
APPs can receive education on currently available PNS systems via virtual or face-to-face webinars, workshops, continuing education conferences, etc. Based upon this foundational knowledge, APPs should be able to have an informed discussion with patients regarding currently available PNS systems and weigh the risks versus benefits of each system for the specific needs of the patient. Some patients express a preference in receiving a temporary versus permanent PNS system and the APP should be prepared to answer any questions on the differences between devices.
The APP can provide initial patient education regarding the use of PNS at the time of the initial consult or at a subsequent return visit. Additional pre- and post-implant education is sometimes provided by other care team members as well. Once it is certain the patient is a good candidate for PNS and the patient agrees they are interested in this therapy, an appointment can be arranged with a PNS implanting physician. A diagnostic peripheral nerve block (ideally performed by the implanting physician) can also be arranged. Lastly, a mental health assessment should be pursued.
Post-PNS Implant
After PNS implant, the APP plays an important role in patient follow-up. At each follow-up appointment, the patient’s device usage should be documented (ie, number of hours used per day, device settings, etc.). The patient’s pain numeric rating scale (NRS) score and percentage pain relief should be documented, in addition to progress towards meeting their pre-implant functional goals. If the patient requires device interrogation or programming adjustment, the APP should coordinate an appointment with the device representative for this to occur.
Other metrics should also be assessed including physical functioning, emotional functioning, patient satisfaction, and adverse events. These metrics fall under the auspices of the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) guidelines highlighting the six core domains of pain, physical functioning, emotional functioning, satisfaction, adverse events, and disposition (eg, treatment adherence).29 Furthermore, the National Institutes of Health’s Patient Reported Outcome Measurement Information System (PROMIS) measures pain, fatigue, negative affect, physical function, and social function. PROMIS demonstrates validity in both real-world clinical settings and in comparative effectiveness research.30 These measurements from multiple core domains should be inputted into neuromodulation registries to ensure that services and standards of care are benchmarked. Additionally, abstraction of these outcomes over time may identify positive and negative predictors of long-term success with PNS, which may be subsequently improve APP education and inform future optimal patient selection.
At follow-up appointments, the APP needs to be aware of potential PNS complications which may fall under two categories: hardware-related complications and biological complications. These complications are listed in Table 3, which has been developed from Complications of Spinal Cord Stimulation and Peripheral Nerve Stimulation Techniques: A Review of the Literature by Eldabe et al.31
The Food and Drug Administration (FDA) manages the Manufacturer and User Facility Device Experience (MAUDE) database, which mandates manufacturers, importers, and device user facilities to report any adverse events related to medical devices including PNS. Voluntary reports from healthcare professionals are also encouraged to uphold patient safety and facilitate benchmarking of services and standards of care.32 APPs should engage with the PNS device company to troubleshoot low-risk complications such as mild skin irritation from adhesive (which may be as simple as providing the patient with hypoallergenic Tegaderm). Should the APP encounter more severe skin reactions with associated systemic symptoms or abnormal laboratory findings (ie, elevated white blood cell count, erythrocyte sedimentation rate or C-reactive protein), consideration should be given to ordering a consultation with infectious disease for expert opinion.
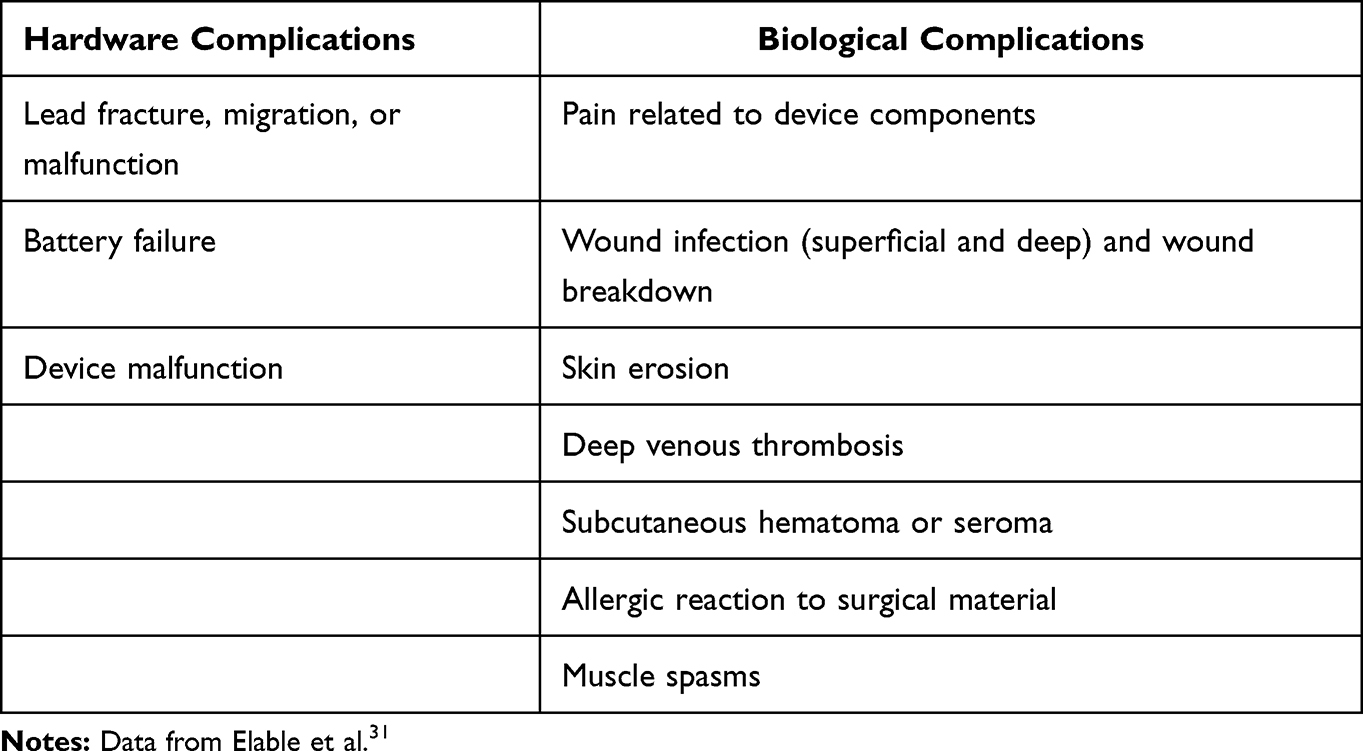 |
Table 3 Peripheral Nerve Stimulator Complications |
Device Removal
The APP needs to be aware of the critical thought-process involved in deciding whether to explant both temporary and permanent PNS devices. Indications for device removal may include patient preference, device infection, therapy failure, persistent pain at the site of hardware, or skin erosion.31 If any of these indications for device removal are met, the APP should involve the implanting physician in the decision-making process. A permanent PNS device will need to be removed by the implanting physician in a sterile operating room setting, while a temporary PNS device can be removed by an APP in the office setting.
Whether the patient has reached the end of intentional 60-day treatment with a temporary PNS device or they are having temporary PNS device-related complications and require early lead pull, this can be accomplished in the office setting by the APP. Lead removal should be performed utilizing sterile technique, though published research on outcomes of sterile vs unsterile removal of PNS leads is currently lacking.
Keys to proper lead pull technique can be remembered using the acronym P.A.T.H as outlined in Table 4. Additional measures sometimes utilized during the temporary PNS lead pull include massage at the site to “loosen” the lead and disrupt any adhesions and potential injection of local anesthetic into the area of the lead as it is removed to “lubricate” the tissues near the implanted lead.
 |
Table 4 P.A.T.H for Suggested Temporary Peripheral Nerve Stimulator Lead Removal* |
Similarities vs Differences Between NPs and PAs
While a thorough discussion on the similarities and differences between NPs and PAs is beyond the scope of this manuscript, it is important to note how these similarities or differences might play a role in the care of PNS patients.
Some institutions utilize NPs and PAs interchangeably for pre-operative, intra-operative, or post-operative patient care needs. Certainly, many of the skills for APP involvement in neuromodulation can be learned via on-the-job training during “onboarding” or “orientation”. Additionally, the prior career of the NP or PA may lend itself well to certain “phases” of patient care (ie, pre-operative, intra-operative, or post-operative). For example, a Registered Nurse (RN) working on a surgical floor who then trains to become an NP may have a particularly high skillset for post-operative care of neuromodulation patients. Similarly, a surgical first assistant who continues their training to become a PA may have a very advanced skill set for assisting in the intra-operative care for neuromodulation patients.
It should be noted that the education, initial certification, maintenance of certification, and licensure requirements are different between NPs and PAs. Table 5 illustrates these differences in a side-by-side comparison, with information obtained from the American Academy of Physician Assistants (AAPA) and the American Association of Nurse Practitioners (AANP).33,34
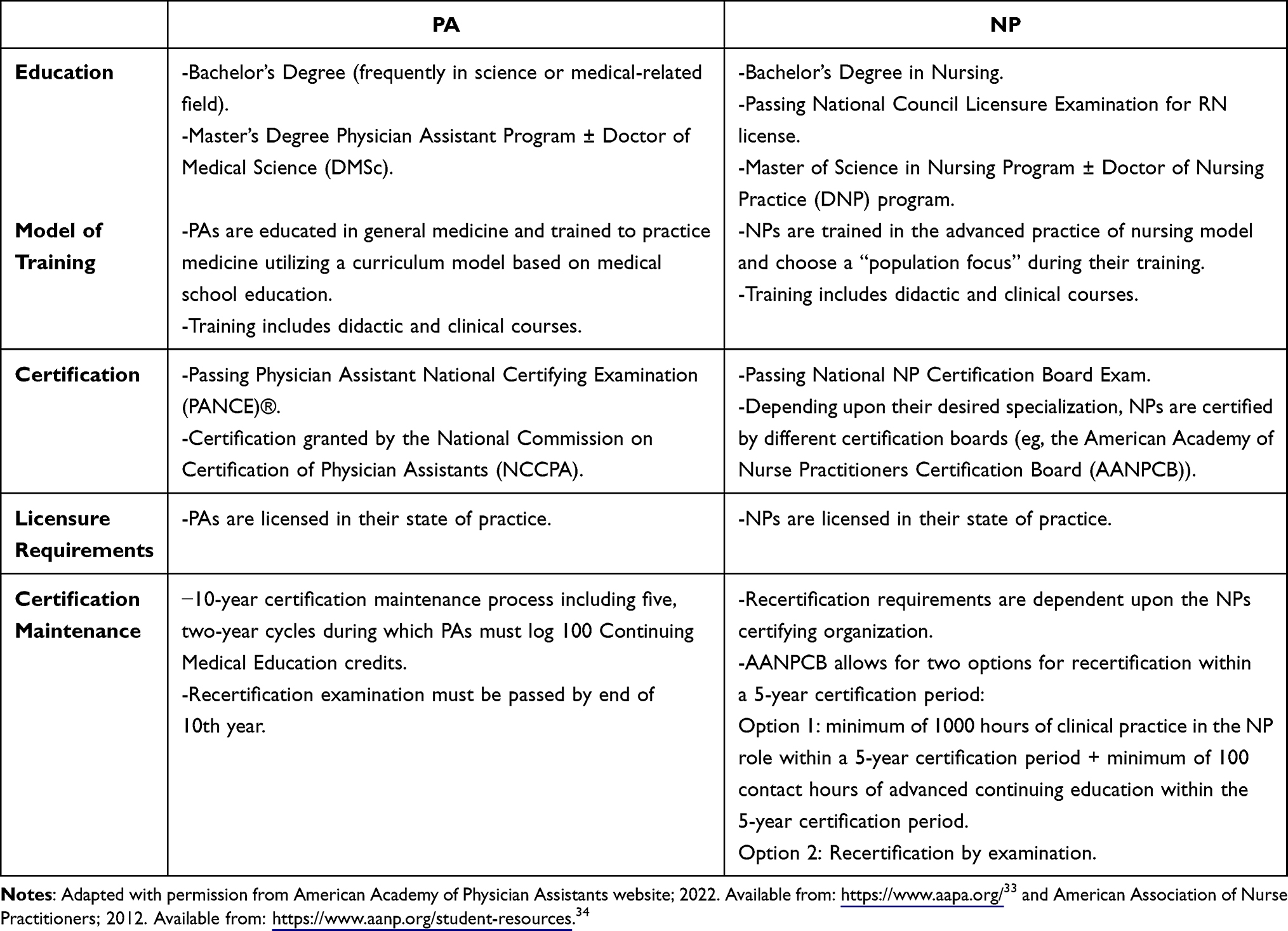 |
Table 5 NPs and PAs Education, Certification, Maintenance of Certification, and Licensure Requirements |
Future Directions
More research is needed regarding the optimal stimulation waveforms for PNS and the safety of continuous PNS at various frequencies.35,36 It is possible that PNS waveforms could be changed to provide improved relief in patients or potentially used as salvage PNS therapy in those who have lost efficacy.
Remote monitoring of PNS patients is another area of research being further developed. Research has already been published regarding the use of remote programming for spinal cord stimulation patients with chronic pain, and it is possible that similar methods could be utilized with PNS patients to improve patient outcomes.37
PNS technology is continuing to develop and advance, including changes to MRI labeling of PNS devices.38–41 Therefore, patients who previously may not have been ideal candidates for PNS, due to the expected future or lifetime need of advanced imaging, may now be better suited to receive this therapy.
Lastly, further research is needed regarding the role of APPs related to neuromodulation patient outcomes (ie, patient satisfaction, post-operative complications, etc.). An April 2020 study titled A Hybrid SWOT Analysis of the Neuromodulation Process for Chronic Pain found that utilization of advanced practice registered nurses as “neuromodulation nurses” freed up neurosurgeon time by offloading responsibilities such as preparing patients for surgery, examining stimulators, and determining possible problems with stimulation therapy, etc. The paper reports the use of neuromodulation nurses “yielded significant shorter queuing times and better patient satisfaction.”42 Specific to PNS, the role of the APP could be measured via patient or implanting provider satisfaction surveys. Additionally, analysis of PNS patient outcomes (ie, pain relief, functional improvement, post-operative complications, etc.) could be further analyzed to determine if there is a correlation between outcomes and treatment by an APP provider.
Conclusion
The APP is an integral member of the clinical care team in pain management clinics, particularly those practices utilizing PNS. At all stages of the patient experience, the APP can optimize outcomes and assist in avoidance of complications. This guide should serve as a framework for proper resource allocation in pain management clinics. It will be imperative, moving forward, that APPs continue to stay up to date on evidence-based research regarding PNS therapies, best practices related to care of PNS patients and new PNS device offerings.
Author Contributions
Chelsey M. Hoffmann, Ryan S. D’Souza, Jonathan M. Hagedorn: All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
CMH provides general consulting for SPR Therapeutics and Nalu Medical. RSD has an investigator-initiated grant with Nevro Corp. JMH is a consultant for Abbott, Boston Scientific, Medtronic, Nevro, and Saluda. He has funded research with Abbott, Medtronic, and Saluda.
References
1. Taylor SS, Noor N, Urits I, et al. Complex regional pain syndrome: a comprehensive review. Pain Ther. 2021;10(2):875–892. doi:10.1007/s40122-021-00279-4
2. Kurklinsky S, Palmer SC, Arroliga MJ, Ghazi SM. Neuromodulation in postherpetic neuralgia: case reports and review of the literature. Pain Med. 2018;19(6):1237–1244. doi:10.1093/pm/pnx175
3. Slavin KV, Nersesyan H, Colpan ME, Munawar N. Current algorithm for the surgical treatment of facial pain. Head Face Med. 2007;3(30). doi:10.1186/1746-160X-3-30
4. Antony AB, Mazzola AJ, Dhaliwal GS, Hunter CW. Neurostimulation for the treatment of chronic head and facial pain: a literature review. Pain Physician. 2019;22(5):447–477. doi:10.36076/ppj/2019.22.447
5. Rauck RL, Cohen SP, Gilmore CA, et al. Treatment of post-amputation pain with peripheral nerve stimulation. Neuromodulation. 2014;17(2):188–197. doi:10.1111/ner.12102
6. Knotkova H, Hamani C, Sivanesan E, et al. Neuromodulation for chronic pain. Lancet. 2021;397(10289):2111–2124. doi:10.1016/S0140-6736(21)00794-7
7. Mainkar O, Solla CA, Chen G, Legler A, Gulati A. Pilot study in temporary peripheral nerve stimulation in oncologic pain. Neuromodulation. 2020;23(6):819–826. doi:10.1111/ner.131398
8. Hagedorn JM, Misercola B, Comer A, et al. The team approach to spinal cord and dorsal root ganglion stimulation: a guide for the advanced practice provider. Mayo Clin Proc Innov Qual Outcomes. 2021;5(3):663–669. doi:10.1016/j.mayocpiqo.2021.05.002
9. Halter M, Wheeler C, Pelone F, et al. Contribution of physician assistants/associates to secondary care: a systematic review. BMJ Open. 2018;8(6):e019573. doi:10.1136/bmjopen-2017-019573
10. Dies N, Rashid S, Shandling M, Swallow C, Easson AM, Kennedy E. Physician assistants reduce resident workload and improve care in an academic surgical setting. JAAPA. 2016;29(2):41–46. doi:10.1097/01.JAA.0000476214.34937.50
11. van Erp RMA, van Doorn AL, van den Brink GT, Peters JWB, Laurant MGH, van Vught AJ. Physician assistants and nurse practitioners in primary care plus: a systematic review. Int J Integr Care. 2021;21(1):6. doi:10.5334/ijic.5485
12. Adler JA, Lotz NM. Intrathecal pain management: a team-based approach. J Pain Res. 2017;10:2565–2575. doi:10.2147/JPR.S142147
13. Young RF. Electrical stimulation of the trigeminal nerve root for the treatment of chronic facial pain. J Neurosurg. 1995;83(1):72–78. doi:10.3171/jns.1995.83.1.0072
14. Dougherty MC, Woodroffe RW, Wilson S, Gillies GT, Howard MA
15. Patel SK, Gozal YM, Saleh MS, Gibson JL, Karsy M, Mandybur GT. Spinal cord stimulation failure: evaluation of factors underlying hardware explantation. J Neurosurg Spine. 2019;1–6. doi:10.3171/2019.6.SPINE181099
16. JM Hagedorn, D’Souza RS, D’Souza RS, et al. Explantation of 10 kHz spinal cord stimulation devices: a retrospective review of 744 patients followed for at least 12 months. Neuromodulation. 2021;24(3):499–506. doi:10.1111/ner.13359
17. Taylor RS, Desai MJ, Rigoard P, Taylor RJ. Predictors of pain relief following spinal cord stimulation in chronic back and leg pain and failed back surgery syndrome: a systematic review and meta-regression analysis. Pain Pract. 2014;14(6):489–505. doi:10.1111/papr.12095
18. Finnerup NB, Haroutounian S, Kamerman P, et al. Neuropathic pain: an updated grading system for research and clinical practice. Pain. 2016;157(8):1599–1606. doi:10.1097/j.pain.0000000000000492
19. Bennett M. The LANSS pain scale: the Leeds assessment of neuropathic symptoms and signs. PAIN. 2001;92(1):147–157. doi:10.1016/S0304-3959(00)00482-6
20. Krause SJ, Backonja MM. Development of a neuropathic pain questionnaire. Clin J Pain. 2003;19(5):306–314. doi:10.1097/00002508-200309000-00004
21. Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). PAIN. 2005;114(1):29–36. doi:10.1016/j.pain.2004.12.010
22. Freynhagen R, Baron R, Gockel U. To¨ lle TR. painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin. 1911–20;2006:22.
23. Portenoy R. Development and testing of a neuropathic pain screening questionnaire: ID Pain. Curr Med Res Opin. 2006;22(8):1555–1565. doi:10.1185/030079906X115702
24. Nayak R, Banik RK. Current innovations in peripheral nerve stimulation. Pain Res Treat. 2018;2018:9091216. doi:10.1155/2018/9091216
25. Deer TR, Narouze S, Provenzano DA, et al. The Neurostimulation Appropriateness Consensus Committee (NACC): recommendations on bleeding and coagulation management in neurostimulation devices. Neuromodulation. 2017;20(1):51–62. doi:10.1111/ner.12542
26. Narouze S, Benzon HT, Provenzano D, et al. Interventional spine and pain procedures in patients on antiplatelet and anticoagulant medications (second edition): guidelines from the American Society of Regional anesthesia and pain medicine, the European Society of Regional anaesthesia and pain therapy, the American Academy of Pain Medicine, the International Neuromodulation Society, the North American Neuromodulation Society, and the World Institute of Pain. Reg Anesth Pain Med. 2018;43(3):225–262. doi:10.1097/AAP.0000000000000700
27. Gilmore CA, Ilfeld BM, Rosenow JM, et al. Percutaneous 60-day peripheral nerve stimulation implant provides sustained relief of chronic pain following amputation: 12-month follow-up of a randomized, double-blind, placebo-controlled trial. Reg Anesth Pain Med. 2019:
28. Deer TR, Gilmore CA, Desai MJ, et al. Percutaneous peripheral nerve stimulation of the medial branch nerves for the treatment of chronic axial back pain in patients after radiofrequency ablation. Pain Med. 2021;22(3):548–560. doi:10.1093/pm/pnaa432
29. Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain. 2003;106(3):337–345. doi:10.1016/j.pain.2003.08.001
30. Cook KF, Jensen SE, Schalet BD, et al. PROMIS measures of pain, fatigue, negative affect, physical function, and social function demonstrated clinical validity across a range of chronic conditions. J Clin Epidemiol. 2016;73:89–102. doi:10.1016/j.jclinepi.2015.08.038
31. Eldabe S, Buchser E, Duarte RV. Complications of spinal cord stimulation and peripheral nerve stimulation techniques: a review of the literature. Pain Med. 2016;17(2):325–336. doi:10.1093/pm/pnv025
32. D’Souza RS, Olatoye OO, Butler CS, Barman RA, Ashmore ZM, Hagedorn JM. Adverse events associated with 10-kHz dorsal column spinal cord stimulation: a 5-year analysis of the manufacturer and user facility device experience (MAUDE) database. Clin J Pain. 2022;38(5):320–327. doi:10.1097/AJP.0000000000001026
33. American Academy of Physician Assistants website; Become a PA. Available from: https://www.aapa.org/career-central/become-a-pa/.
34. American Association of Nurse Practitioners. Student Resources. Available from: https://www.aanp.org/student-resources.
35. Günter C, Delbeke J, Ortiz-Catalan M. Safety of long-term electrical peripheral nerve stimulation: review of the state of the art. J NeuroEngineering Rehabil. 2019;16(13). doi:10.1186/s12984-018-0474-8
36. Finch P, Price L, Drummond P. High-frequency (10 kHz) electrical stimulation of peripheral nerves for treating chronic pain: a double-blind trial of presence vs absence of stimulation. Neuromodulation. 2019;22(5):529–536. doi:10.1111/ner.12877
37. Han Y, Lu Y, Wang D, et al. The use of remote programming for spinal cord stimulation for patients with chronic pain during the COVID-19 outbreak in China. Neuromodulation. 2021;24(3):441–447. doi:10.1111/ner.13382
38. Ruais J. Nalu receives FDA clearance for 1.5T full-body MRI scanning in patients with nalu neurostimulation system implants. Cision PRWeb; 2022. Available from: https://www.prweb.com/releases/nalu_receives_fda_clearance_for_1_5t_full_body_mri_scanning_in_patients_with_nalu_neurostimulation_system_implants/prweb17590348.htm.
39. Business Wire. Glodow Nead Communications. stimwave receives FDA 510(k) clearance for the first full-body MRI scan ready wireless Peripheral Nerve Stimulator (PNS) System; 2017. Available from: https://www.businesswire.com/news/home/20170809005263/en/Stimwave-Receives-FDA-510-k-Clearance-for-the-First-Full-Body-MRI-Scan-Ready-Wireless-Peripheral-Nerve-Stimulator-PNS-System.
40. Stimwave Technologies. MRI safety conditions for stimwave stimulators. Available from: https://stimwavefreedom.com/about-us/mri-information.
41. StimRouter. MRI safety. Available from: https://stimrouter.com/physicians/mri-safety-following-stimrouter-implant/.
42. Puurunen A, Ikäheimo TM, Nissen M, et al. A hybrid SWOT analysis of the neuromodulation process for chronic pain. Br J Neurosci Nurs. 2020;16(2):76–85. doi:10.12968/bjnn.2020.16.2.76
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Birds of a Feather Redux: Defining Ways to Stimulate the Peripheral Nervous System
Deer T, Shah A, Slavin K, Vorenkamp KE, Shah S, Leong M, McRoberts WP
Journal of Pain Research 2023, 16:1219-1224
Published Date: 8 April 2023
The American Society of Pain and Neuroscience (ASPN) Guidelines for Advanced Practice Providers in Interventional Spine and Pain Management Practice
Grillo C, Abd-Elsayed A, Yousef TA, Misercola B, Hussaini Z, Rabii M, Comer A, Durkin K, McGinn P, Deer T
Journal of Pain Research 2025, 18:6319-6344
Published Date: 26 November 2025
Preparing Nurse Practitioners and Physician Assistants for Effective Roles in Graduate Medical Education: A Framework for Onboarding, Role Clarity, and Patient Safety
Sofka S, Reece J
Advances in Medical Education and Practice 2026, 17:616800
Published Date: 5 June 2026