Back to Journals » Advances in Medical Education and Practice » Volume 17
Preparing Nurse Practitioners and Physician Assistants for Effective Roles in Graduate Medical Education: A Framework for Onboarding, Role Clarity, and Patient Safety
Received 15 April 2026
Accepted for publication 3 June 2026
Published 5 June 2026 Volume 2026:17 616800
DOI https://doi.org/10.2147/AMEP.S616800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
Sarah Sofka,1,* Josephine Reece2,*
1Department of Medical Education, West Virginia University School of Medicine, Morgantown, WV, USA; 2Department of Medicine, West Virginia University School of Medicine, Morgantown, WV, USA
*These authors contributed equally to this work
Correspondence: Sarah Sofka, Department of Medical Education, PO Box 9160, West Virginia University School of Medicine, Morgantown, West Virginia, USA, Email [email protected]
Abstract: Health care delivery models have increasingly integrated nurse practitioners (NPs) and physician assistants (PAs) as essential members of interprofessional teams within graduate medical education (GME). While initially utilized to support clinical coverage and duty-hour compliance, NP and PA roles have expanded to include meaningful contributions to trainee education, healthcare team function, and continuity of patient care. This article proposes a structured framework for NP and PA onboarding and professional development across five key domains: accreditation requirements, role clarification and supervision, interprofessional teamwork and communication, patient safety and handoffs, and ongoing educational development. Enhancing NP and PA understanding of GME expectations and regulatory standards, particularly those outlined by the ACGME, may optimize their impact on both trainee learning and patient outcomes. Strengthening NP and PA integration through targeted education and development opportunities may improve team-based care, promote patient safety, and enrich the clinical learning environment.
Keywords: advance practice providers, nurse practitioner, physician assistant, professional development, handoff, supervision
Introduction
Health care models have rapidly evolved in recent years to include both the role of physician assistant (PA) and nurse practitioner (NP) as integral members of the interprofessional team. The clinical learning environment for both residents and fellows, herein referred to as trainees, is no exception to this evolution. Early in the integration of NPs and PAs into academic medical settings, they were often utilized as trainee substitutes to help programs comply with duty-hour restrictions and to maintain clinical coverage during protected educational time. This remains an essential role for NPs and PAs, but emerging evidence seems to show that their contributions have expanded to include an educational component, especially as it relates to interprofessional teamwork. As trainees and faculty frequently rotate through services and clinical experiences, NPs and PAs often remain as a constant team member, offering stability for both patient care and team logistics.1 However, this potential cannot be fully realized without NPs and PAs understanding the goals, expectations, and regulatory requirements of graduate medical education (GME). Another consideration is the differences in education and training, licensure, and scope of practice between NPs and PAs. PAs complete graduate-level medical education programs and undergo broad clinical training across multiple specialties before obtaining national certification and state licensure. Their scope of practice is determined by state regulations and institutional policies, and most commonly require collaboration with a supervising physician.2 NPs complete advanced graduate nursing education at the master’s or doctoral level that builds upon registered nursing training and emphasizes both clinical care and nursing-based models of patient management. Their scope of practice varies by state law and may include independently or collaboratively evaluating and treating patients.3 Both roles bring unique skills as well as potential gaps that need bridged for safe and effective education of trainees. With much of the emphasis of onboarding and professional development on faculty physicians and trainees, there is a unique opportunity to strengthen and further expand the NP and PA role within GME by also providing them with focused educational opportunities.
The proposed framework for NP and PA onboarding and professional development within the clinical learning environment was developed from a synthesis of Accreditation Council for Graduate Medical Education (ACGME) program requirements,4 published literature on interprofessional education and patient safety,5–7 and the authors’ experience in GME administration and clinical education. NP and PA onboarding and professional development within the clinical learning environment can be divided into 5 categories: Accreditation Requirements, Role Clarification and Supervision, Interprofessional Teaming and Communication, Patient Safety and Handoffs, and Educational Opportunities and Ongoing Professional Development (Figure 1).
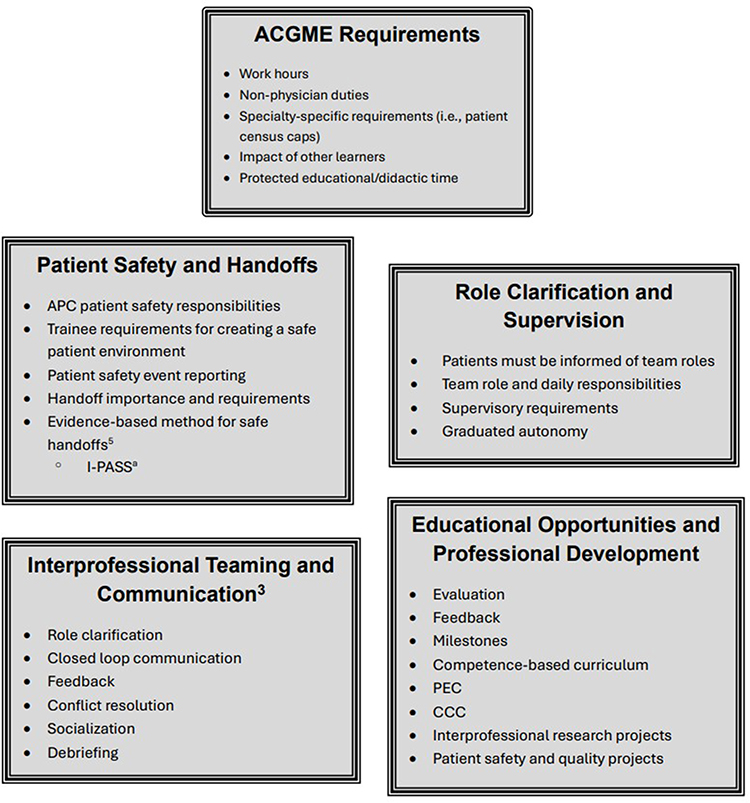 |
Figure 1 Five categories of APC onboarding and professional development within the clinical learning environment. aI-PASS: Illness Severity, Patient Summary, Action List, Situation Awareness and Contingency Planning, Synthesis by Receiver.5 |
Discussion
The ACGME requirements for trainees can be a complex and confusing resource to understand fully. NP and PA education should focus on relevant areas that would be applicable in the day-to-day interactions with trainees. A thorough understanding of work-hour limits and the importance of maintaining compliance is an essential component. Additionally, knowledge of specialty-specific requirements, such as patient census caps, would be important if the NP or PA works primarily with trainees from that program. NPs and PAs should also be aware of the ACGME requirement that prohibits trainees from routinely performing non-physician duties that interfere with the educational experience.4 Additional areas of focus are illustrated in Figure 1. Also of note, the other major areas of focus are in alignment with the ACGME requirements.
Role Clarification and Supervision are also components of ACGME core program requirements,4 but expanding beyond the requirements may create more learning opportunities for trainees and may promote effective interprofessional teaming. ACGME requires that all members of the health care team and patients be informed of each team members’ roles.4 Clearly defining one’s role on the team, as well as outlining daily responsibilities, may help provide an important foundation for effective team functioning. Although an attending physician is always ultimately responsible for supervisory care, a common misconception is that an NP or PA cannot provide supervision to trainees. Clarifying the ACGME requirements around supervision, as well as any specialty-specific requirements, is necessary to remain in accreditation compliance and to maximize teaching potential where NPs and PAs may have a nuanced or advanced skill set. Common examples would be procedures or specialized patient care workflows. Lastly, graduated autonomy is another critical concept for NPs and PAs to put into action so that trainees may grow into independent physicians.
A core ACGME competency is interpersonal communication skills and trainees must be able to work effectively in an interprofessional team.4 Part of that competency is optimizing the NP and PA skill set to maximize the functionality and efficiency of the team to care for patients in a safe manner. Learning to do this in training is key to transitioning to an independent practice that will likely utilize NPs and PAs in some form or another. Both trainees and NPs and PAs therefore may benefit from education in this area. Skills such as role clarification, closed-loop communication, conflict resolution, and debriefing are a few of the strategies that trainees and NPs and PAs should learn.5
A clinical learning environment where patient safety is prioritized is a requirement for all GME programs,4 and each of the previously described domains above contributes to this goal. Each major area of focus above supports patient safety. Handoffs are one area of vulnerability when it comes to patient safety.6 Trainees are required to have education around safe handoff procedures,4 but we have and literature has observed deficits in NP handoff practices.7,8 These deficits may lead to incomplete, inadequate, and unsafe transitions of care.6 Structured, evidence-based education on the necessary components of an effective patient handoff, such as I-PASS,5 should be a required component of any NP and PA onboarding process.
The last major area of focus is other educational opportunities and professional development. The ACGME common program requirements allow for NPs and PAs serving in educational roles to serve as core faculty and to serve on key GME committees such as the Program Evaluation Committee and Clinical Competency Committee if the program director deems that they play a significant role in the educational program.4 NPs and PAs serving in these roles should receive the same type of faculty development that physicians would receive around learner evaluation, feedback, milestones, and competency-based curriculum. NPs and PAs may contribute to trainee interprofessional research projects or quality and patient safety projects with their unique perspective within the health care system.
Conclusion
NPs and PAs will continue to play a major role in American health care systems. It is essential that trainees learn to effectively work in a safe and efficient team-based care model that includes NPs and PAs. Additionally, health care systems that educate medical residents and fellows may benefit from ensuring that NPs and PAs are well trained on the necessary components of the clinical learning environment that contributes to both patient safety and high-quality physician education.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Barker AM, Konopasky AW, Varpio L, Soh M, Poole BR, Stalmeijer RE. How advanced practice clinicians support education for and contribute to education of graduate medical education trainees: a critical literature review. Acad Med. 2024;99(11):1286–4. doi:10.1097/ACM.0000000000005858
2. American Academy of Physician Associates. What is a PA? AAPA. Available from: https://www.aapa.org/about/what-is-a-pa/.
3. American Association of Nurse Practitioners. Scope of practice for nurse practitioners. AANP. Available from: https://www.aanp.org/advocacy/advocacy-resource/position-statements/scope-of-practice-for-nurse-practitioners.
4. Accreditation Council for Graduate Medical Education. ACGME common program requirements (Residency). 2026. Available from: https://www.acgme.org/globalassets/pfassets/programrequirements/2026-prs/cprresidency_2026_feb_revision.pdf.
5. Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371(19):1803–1812. doi:10.1056/NEJMsa1405556
6. Agency for Healthcare Research and Quality. TeamSTEPPS® 3.0: team strategies & tools to enhance performance and patient safety—pocket guide. 2023. Available from: https://www.ahrq.gov/sites/default/files/wysiwyg/teamstepps-program/teamstepps-pocket-guide.pdf.
7. Vanderzwan KJ, Kilroy S, Burt L, O’Rourke J. Don’t interrupt me! Development of a handoff education bundle to simulate the real world. Int J Nurs Educ Scholarship. 2024;21(1):20230092. doi:10.1515/ijnes-2023-0092
8. Song Y, McCreary LL. New graduate nurses’ self-assessed competencies: an integrative review. Nurse Educ Pract. 2020;45:102801. doi:10.1016/j.nepr.2020.102801
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Advanced Practice Provider Guide to Peripheral Nerve Stimulation
Hoffmann CM, D'Souza RS, Hagedorn JM
Journal of Pain Research 2022, 15:2283-2291
Published Date: 7 August 2022
The American Society of Pain and Neuroscience (ASPN) Guidelines for Advanced Practice Providers in Interventional Spine and Pain Management Practice
Grillo C, Abd-Elsayed A, Yousef TA, Misercola B, Hussaini Z, Rabii M, Comer A, Durkin K, McGinn P, Deer T
Journal of Pain Research 2025, 18:6319-6344
Published Date: 26 November 2025