Back to Journals » Journal of Hepatocellular Carcinoma » Volume 11
Adjuvant Transarterial Chemoembolization Plus Immunotherapy for Huge Hepatocellular Carcinoma: A Propensity Score Matching Cohort Study
Authors Huang H ![]() , Liao W, Zhang K, Wang H, Cheng Q
, Liao W, Zhang K, Wang H, Cheng Q ![]() , Mei B
, Mei B
Received 20 December 2023
Accepted for publication 29 March 2024
Published 8 April 2024 Volume 2024:11 Pages 721—735
DOI https://doi.org/10.2147/JHC.S455878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Manal Hassan
Hongwei Huang,* Wei Liao,* Kaiyue Zhang, Hao Wang, Qi Cheng, Bin Mei
Hepatic Surgery Center, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Mei; Qi Cheng, Hepatic Surgery Center, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, No. 1095 Jie Fang Avenue, Qiaokou, Wuhan, 430030, People’s Republic of China, Email [email protected]; [email protected]
Purpose: The prognosis of patients with huge hepatocellular carcinoma (huge HCC, diameter ≥ 10 cm) is poor owing to the high early recurrence rate. This study aimed to explore the clinical value of postoperative adjuvant transarterial chemoembolization (PA-TACE) plus programmed cell death-1 (PD-1) inhibitors for huge HCC.
Patients and Methods: Data from consecutive huge HCC patients treated with hepatectomy during June 2017 and July 2022 were retrospectively collected. Baseline differences were balanced between huge HCC patients who underwent PA-TACE with (AIT group) or without PD-1 inhibitors (AT group) by propensity-score matching (PSM). We compared recurrence-free survival (RFS), overall survival (OS) and recurrence patterns between the two groups. Independent risk factors for RFS and OS were confirmed by Cox regression analysis, and subgroup analysis was also conducted.
Results: A total of 294 patients were enrolled, and 77 pairs of patients in the AIT and AT groups were matched by PSM. The 1-year and 2-year RFS were 49.9% and 35.7% in the AIT group compared to 24.7% and 15.5% in the AT group respectively (p< 0.001). The 1-year and 2-year OS were 83.6% and 66.9% in the AIT group compared to 50.6% and 36.8% in the AT group respectively (p< 0.001). There were no significant differences in recurrence patterns between the two groups. Multivariable analysis demonstrated that combined therapy of PA-TACE plus PD-1 inhibitors was a protective factor related to both RFS and OS.
Conclusion: PA-TACE plus PD-1 inhibitors could improve survival outcomes for huge HCC patients.
Keywords: hepatocellular carcinoma, postoperative adjuvant therapy, programmed cell death-1 inhibitors, transarterial chemoembolization, early recurrence
Introduction
Hepatocellular carcinoma (HCC) is the most common type of liver cancer, accounting for 75–86% of cases.1 Many HCC patients were diagnosed with huge sizes (exceeding 10 cm in diameter) owing to insidious symptoms and lacking of well-organized screening programs.2,3 Although hepatectomy demonstrated quite high feasibility and cost-effectiveness and was the only curative treatment for huge HCC, the oncological outcomes were still poor for early recurrence following surgery.4,5 The recurrence rates remained as high as 32.1–54% at 1 year and 57–70% at 3 years.2,3,6,7
Therefore, postoperative adjuvant treatment is necessary to reduce early recurrence rate and improve oncological prognosis for patients with huge HCC. Postoperative adjuvant treatment includes locoregional treatments such as transarterial chemoembolization (TACE), hepatic artery infusion chemotherapy, radiotherapy, and systemic therapy such as antiviral treatment, tyrosine kinase inhibitors (TKIs), and immune checkpoint inhibitors (ICIs).8–12 Up to date, postoperative adjuvant TACE (PA-TACE) has demonstrated its importance in reducing recurrence rate, improving recurrence-free survival (RFS) and overall survival (OS) for HCC patients with high recurrence risks, including huge HCC.8,13,14 Therefore, PA-TACE was recommended in guidelines of China. However, the effect of PA-TACE is still unsatisfactory. TACE, as a kind of locoregional treatment, can be used in combination with systemic therapy to further improve oncological prognosis of HCC. ICIs are being explored as postoperative adjuvant treatment for HCC in several Phase III clinical trials, such as EMERALD-2, KEYNOTE-937, IMbrave 050, CheckMate 9DX. Recently, ICIs were recommended as adjuvant therapy for patients with HCC by the latest guidelines of American Association for the Study of Liver Diseases (AASLD) according to the interim results of IMbrave 050 which showed that adjuvant atezolizumab plus bevacizumab was associated with significantly improved RFS compared with active surveillance (1-year RFS, 78% vs 65%).15,16 However, to the best of our knowledge, there is still no study about PA-TACE plus adjuvant immunotherapy for huge HCC.
In this study, two cohorts were established according to different postoperative adjuvant treatments. All included patients with huge tumor underwent R0 hepatectomy. The short-term oncological outcomes of the two methods were compared, providing a high level of evidence by using propensity-score matching (PSM) to overcome selection bias.
Materials and Methods
Patient Selection
This study was conducted in accordance with the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the institutional ethics committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (TJ-IRB20221125). Consecutive patients who were diagnosed with huge HCC and underwent hepatectomy with curative intent from June 2017 to July 2022 at our center were retrospectively analyzed.
The inclusion criteria were as follows: 1) pathologically diagnosed as HCC; 2) tumor diameter ≥10 cm; 3) R0 resection; 4) receipt of PA-TACE with or without ICIs; 5) Child-Pugh class A or B7; 6) absence of extrahepatic metastasis in preoperative radiological imaging; 8) no history of other malignant diseases; 9) good cardiopulmonary function and Eastern Cooperative Oncology Group (ECOG) score <2. The exclusion criteria were as follows: 1) recurrent HCC; 2) patients who died within 30 days after surgery; 3) recurrence in the first month after surgery; 4) underwent other anti-recurrence treatments before and/or after surgery; 5) incomplete clinical or follow-up data. These patients were divided into two cohorts of adjuvant immunotherapy plus TACE (AIT group) or adjuvant TACE (AT group) according to treatment. The choice of treatment was based on every patient’s wish after he/she discussed with his/her doctors in detail.
Preoperative Assessment, Hepatectomy
Each patient underwent a comprehensive preoperative assessment including laboratory examinations and medical imaging evaluations. In detail, laboratory examinations included full blood cell tests, coagulation tests, liver function tests, viral load (hepatitis B virus and/or hepatitis C virus, HBV and/or HCV), serum alpha-fetoprotein (AFP) level, thyroid function tests, hypertensive cardiac troponin I tests, myoglobin tests and adrenal gland function tests. Medical imaging, including chest computed tomography (CT), abdominal ultrasonography, abdominal enhanced CT, and/or abdominal magnetic resonance imaging (MRI), was performed to assess tumor resectability. An indocyanine green 15-min retention test was performed on every patient to assess his/her hepatic functional reserve. Three-dimensional reconstruction of the liver was routinely performed to evaluate the residual liver volume. A multidisciplinary team meeting, which included liver surgeons, gastroenterologists, hepatologists, oncologists, radiologists and pathologists, was held every week to discuss a comprehensive treatment scheme for every patient. Hepatectomy would not be performed unless these criteria were met simultaneously: 1) indocyanine green 15-min retention rate <15%; 2) sufficient remnant liver volume >40% standard liver volume; 3) viral load of HBV DNA and/or HCV RNA <1*10^4 IU/mL.17,18
The surgical procedures of hepatectomy have been reported previously.19 Intraoperative ultrasound was routinely performed to identify any potential tumor nodules that were not detected before surgery and to help rule out parenchymal transection plane. Pringle’s maneuver and the low central venous pressure technique were performed if necessary. Liver parenchymal transection was performed by an ultrasonic scalpel. After surgery, full blood cell counts, coagulation tests, liver and renal function tests were routinely performed on the first, third and fifth days.
Postoperative Treatment Regimen
The AIT group: Patients in the AIT group began to undergo immunotherapy when recovered well from the surgery and alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were both less than 80 U/L and total bilirubin was less than 30 μmol/L. Patients in this group received 200mg programmed cell death-1 (PD-1) inhibitors once every 3 weeks for 9 cycles. PD-1 inhibitors include pembrolizumab, tislelizumab, sintilimab and camrelizumab. The specific agents of PD-1 inhibitors were determined by the patients’ wishes and consultation with their attending physicians. It would be terminated when disease progressed or intolerable toxicity occurred. Patients would undergo PA-TACE 1–1.5 months after surgery.8 A hepatic arterial catheter was selectively placed into the proper hepatic artery through the femoral artery by the Seldinger technique, and then hepatic angiography was performed. If tumor staining was not found, an emulsion was prepared by mixing oxaliplatin with lipiodol at a volume ratio of 1:1. Approximately 5–10 mL of emulsion was slowly injected into the hepatic artery.
The AT group: The patients in this group only underwent PA-TACE 1–1.5 months after surgery. Similarly, the indications and procedure have been stated above.
Follow Up
All follow-up was performed in our clinic to obtain unified and unabridged data. For the AIT group, abdominal ultrasound, full blood cell counts, coagulation tests, liver function tests, renal tests, serum AFP level, thyroid function tests, hypertensive cardiac troponin I tests, myoglobin tests, adrenal gland function tests and electrocardiogram were performed once every 3 weeks before injecting PD-1inhitors during the 9 cycles, and once every three months thereafter. Chest CT, abdominal CT and/or MRI and bone imaging would be performed if tumor recurrence was suspected. For the AT group, abdominal ultrasound, full blood cell counts, coagulation tests, liver function tests, renal tests and serum AFP levels were performed once every month during the first six months after surgery and then once every three months. The follow-up continued until two years after surgery or death. Patients who suffered from recurrence underwent microwave ablation, repeat hepatectomy, TACE, radiotherapy or systemic therapy depending on tumor size, location, number of tumors, liver function, ECOG scores and patient wishes.
Outcomes
The primary endpoints of the study were to clarify oncological outcomes of RFS and OS. Recurrence patterns and adverse events (AEs) were considered as the secondary endpoints of the study.
Definition
MVI was defined as the presence of tumor cell nests in vessels of the surrounding hepatic tissue lined by endothelium which was visible only on microscopy.20 Satellites were defined as tumor cell nests with similar histological features of the primary tumor located around but separated from the main tumor.21 RFS was defined as the period from the date of surgery to the date of the first diagnosis of disease recurrence or censored at the last follow-up or death by any cause. OS was defined from the date of surgery to the date of death for any reason or the last follow-up. The grades of AEs were based on the National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0.
Statistical and Survival Analysis
Continuous variables were expressed as medians and ranges while categorical variables were expressed as frequency and percentage. An independent samples t-test (normal distribution) or Mann‒Whitney U-test (abnormal distribution) was used to compare continuous variables as appropriate while the Chi-square test or Fisher’s exact test was used for categorical variables.
We performed PSM to overcome possible selection bias between the AIT group and AT group. All clinicopathological parameters associated with survival outcomes were included in the propensity score model to draw more reliable outcomes. We established a multivariable logistic regression model with the covariates to calculate propensity scores from 0 to 1 including age, sex, basic liver disease, HBV load, Child‒Pugh class, AST, ALT, total bilirubin, albumin, platelets, neutrophil-to-lymphocyte ratio (NLR), prothrombin time, AFP, tumor size, Barcelona Clinic Liver Cancer (BCLC) stage, multiple tumors, satellites, MVI, ruptured tumor, Edmonson-Steiner (E-S) grade III–IV and intrahepatic blood transfusion. A one-to-one match without replacement was performed by nearest neighbor matching. The caliper of match was 0.20 in the study.
Survival rates were calculated by the Kaplan‒Meier method and compared between two groups by the Log rank test. Then, we used a univariate Cox regression model to explore the potential recurrence and survival factors in matched patients. Only the significant variables in the univariate Cox regression model were included in the multivariable Cox regression analysis. Subgroup survival analysis was conducted using univariable Cox regression, stratified by different clinical variables (sex, age, etiology, AFP, macrovascular invasion, multiple tumors, E-S grade, ruptured tumor, MVI, satellites, blood transfusion), and forest plots were drawn with hazard ratio (HR) and 95% confidence interval (CI). A p value <0.05 was defined as statistically significant.
All statistical analyses were conducted with SPSS version. 24.0 (IBM Corp., Armonk, NY, USA), R program (version 4.3.2, R foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
From June 2017 to July 2022, 372 patients with huge HCC underwent hepatectomy. As shown in Figure 1, 78 patients were excluded and 294 patients who received adjuvant therapy were enrolled in the study, with 83 patients in the AIT group and the other 211 patients in the AT group. The significant differences between two groups were that more patients with younger age, macrovascular invasion, MVI and satellites existed in the AIT group. After a 1:1 match, 77 pairs of patients were matched, and balanced baseline characteristics of the two groups are shown in Table 1.
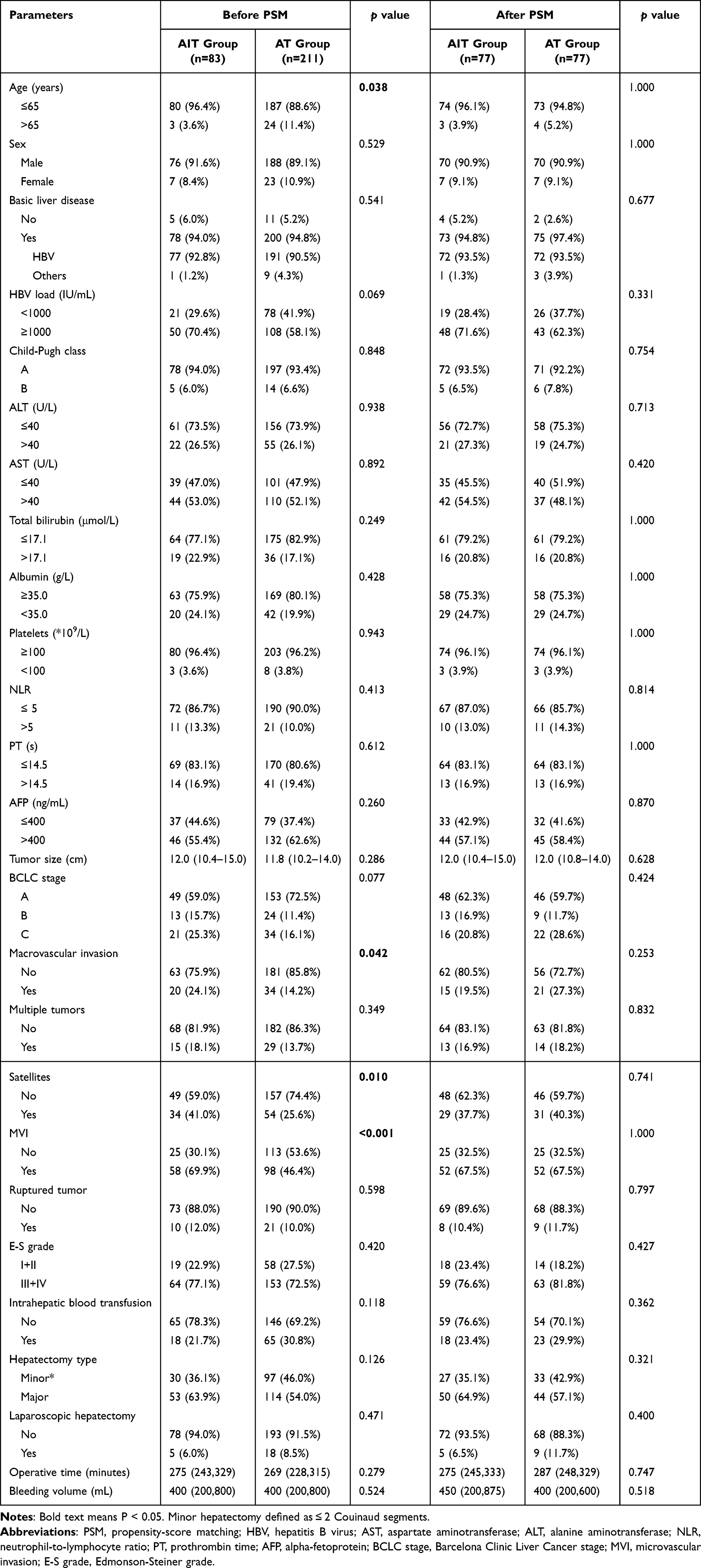 |
Table 1 Baseline Characteristics of the AIT Group Compared with the at Group Before and After PSM |
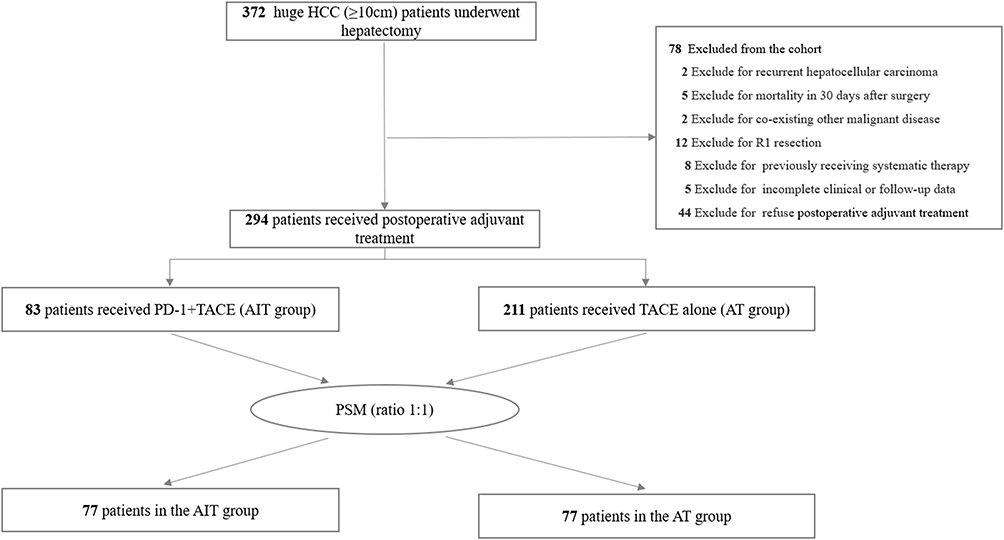 |
Figure 1 Flowchart of patients’ enrollment for comparison. Abbreviation: PSM, propensity score matching. |
Recurrence‑free Survival and Overall Survival
With the follow-up time of two years, recurrences occurred in 50 patients in the AIT group and 155 patients in the AT group, while mortality occurred in 24 patients in the AIT group and 98 patients in the AT group before PSM (Table 2). The corresponding 1-year and 2-year RFS were 48.7% and 35.8% in the AIT group compared with 33.9% and 25.1% in the AT group respectively (p=0.035; Supplementary Figure 1A). The median RFS was 11.7 months (95% CI: 8.0~19.3 months) in the AIT group while it was 6.9 months (95% CI: 5.6~8.9 months) in the AT group. The 1-year and 2-year OS in the AIT group were superior to those in the AT group (83.7%, 63.1% vs 67.1%, 51.8%, p=0.025, Supplementary Figure 1B). The median OS did not reach both in two groups.
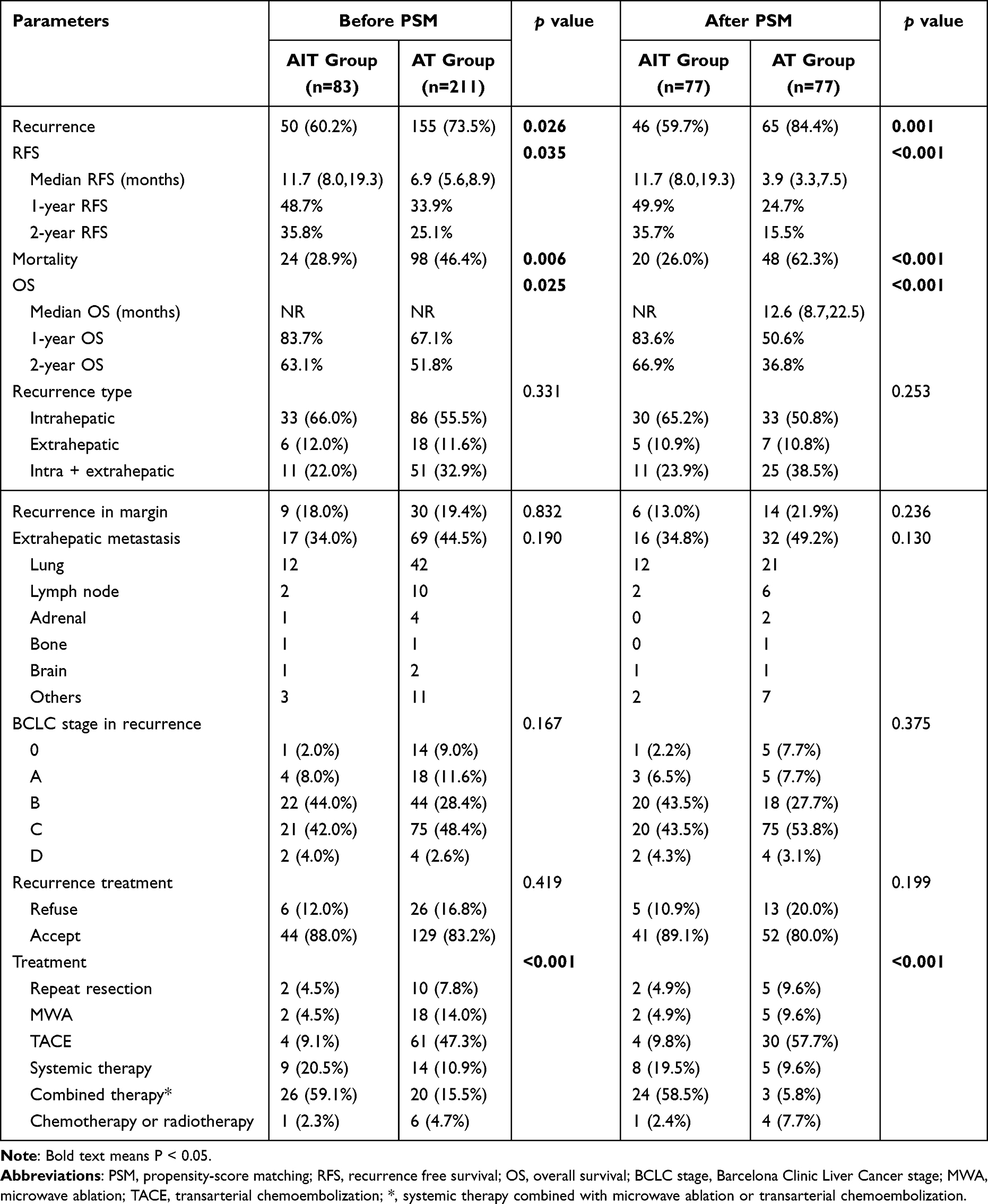 |
Table 2 Recurrence and Survival Data Before and After PSM |
After PSM, 46 patients underwent recurrence and 20 patients died in the AIT group, while 65 patients underwent recurrence and 48 patients died in the AT group (Table 2). The corresponding 1-year and 2-year RFS were 49.9% and 35.7% in the AIT group compared with 24.7% and 15.5% in the AT group respectively (p<0.001; Figure 2A). The median RFS was also 11.7 months (95% CI: 8.0~19.3 months) in the AIT group while it was 3.9 months (95% CI: 3.3~7.5 months) in the AT group. The 1-year and 2-year OS were 83.6% and 66.9% in the AIT group compared with 50.6% and 36.8% in the AT group respectively (p<0.001; Figure 2B). The median OS was 12.6 months (95% CI: 8.7~22.5 months) in the AT group while did not reach in the AIT group. There were no significant differences between the two groups in terms of recurrence type or recurrence location. Intrahepatic recurrence was the most common type. There was also no significant difference in recurrence rates at resection margins and stages of recurrence. Most recurrences were in median or advanced stage, especially the advanced stage which accounted for nearly half of the recurrences. Forty-one patients underwent treatment for recurrence in the AIT group and 52 patients in the AT group (p=0.199). There were significant differences in treatments after recurrence between the two groups as more patients in the AIT group received combined therapy of locoregional treatment plus systemic therapy while more patients in the AT group received TACE alone (p<0.001).
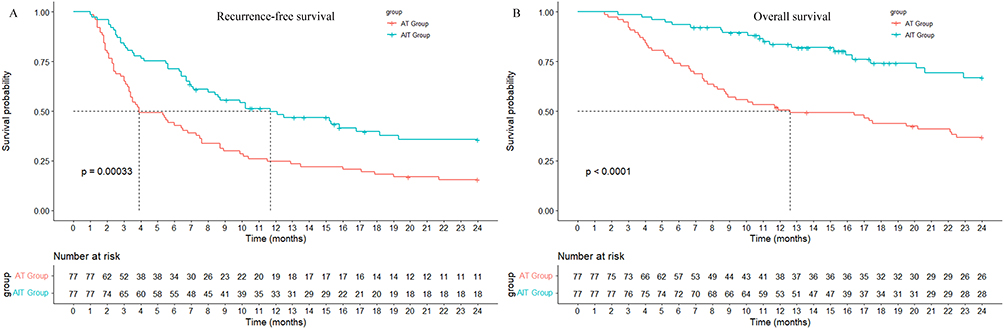 |
Figure 2 Comparison of RFS (A) and OS (B) between the AIT group and AT group after PSM. |
Safety
Transient AEs during TACE treatment were not recorded. Of the 83 patients in the AIT group, AEs of any grade occurred in 34 patients (41.0%) and grades 3/4 AEs occurred in 5 patients (6.0%). All patients with grades 3/4 AEs recovered after discontinuing immunotherapy and receiving corticosteroids There were no treatment-related deaths. The common AEs included rash or pruritus, neutropenia, decreased platelets, hypothyroidism, increased ALT or AST. Detailed AEs are summarized in Table 3.
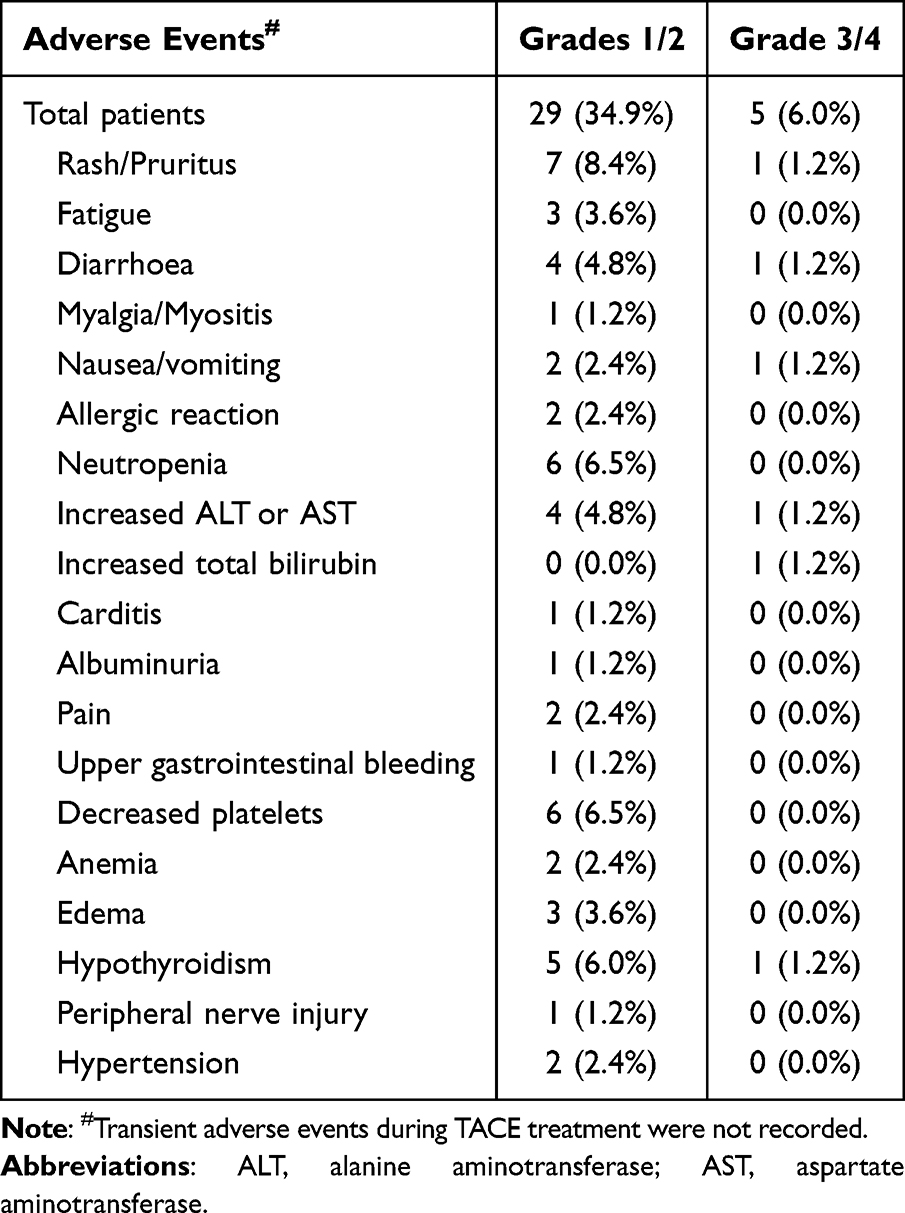 |
Table 3 Adverse Events in Regard to Immunotherapy |
Univariable and Multivariable Analysis
After PSM, univariable analysis revealed that AFP >400 ng/mL (HR=1.715; 95% CI: 1.167~2.522; p=0.006), macrovascular invasion (HR=1.824; 95% CI: 1.202~2.768; p=0.005), multiple tumors (HR=1.863; 95% CI: 1.183~2.934; p=0.007), satellites (HR=2.189; 95% CI: 1.499~3.197; p<0.001), and AIT (HR=0.507; 95% CI: 0.347~0.741; p<0.001) were factors significantly related to RFS. Multivariable analysis showed that macrovascular invasion (HR=1.703; 95% CI: 1.091~2.656; p=0.019), multiple tumors (HR=1.672; 95% CI: 1.009~2.770; p=0.046), satellites (HR=1.719; 95% CI: 1.112~2.657; p=0.015), and AIT (HR=0.445; 95% CI: 0.302~0.656; p<0.001) were independent predictors of RFS (Table 4).
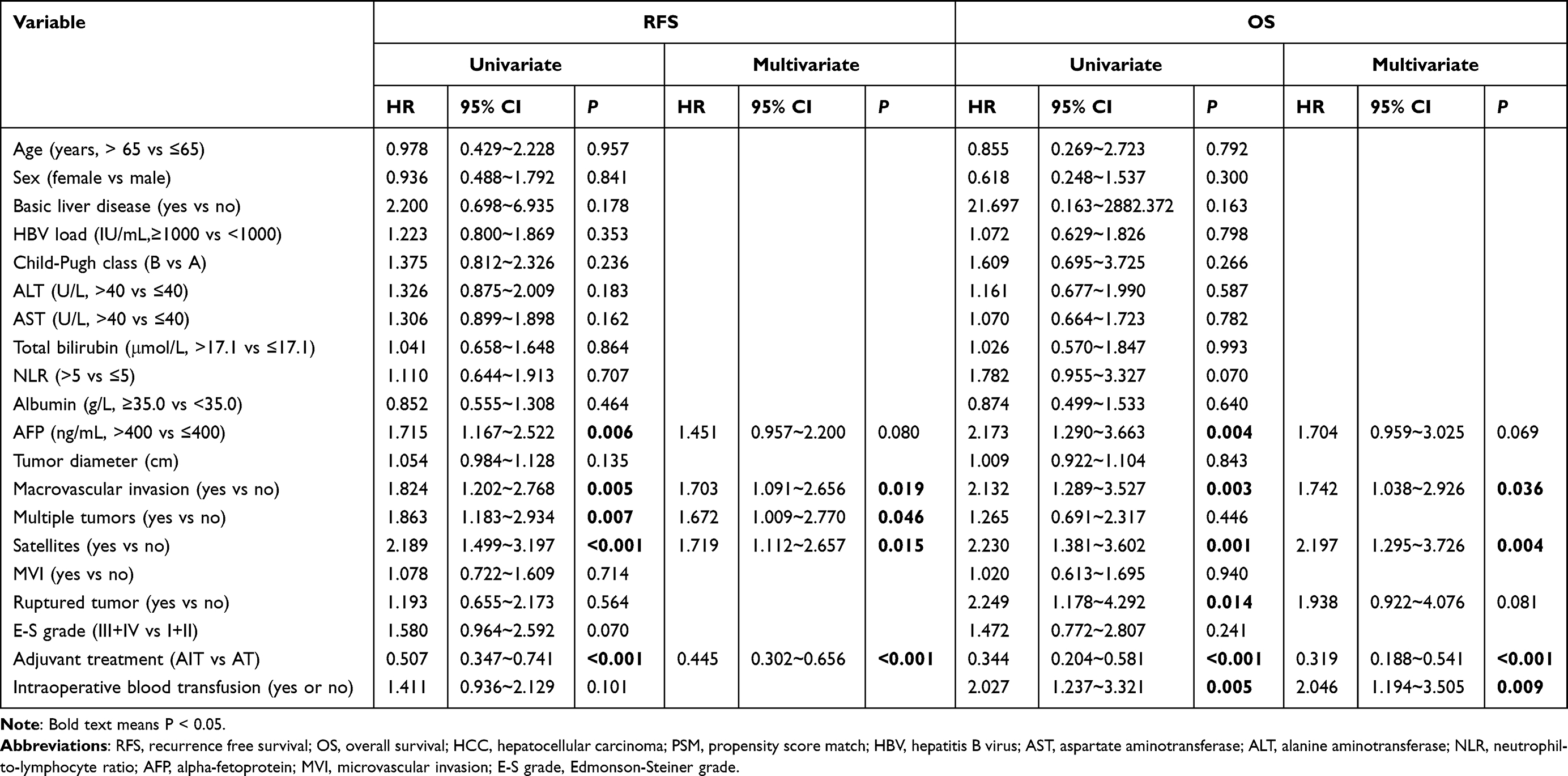 |
Table 4 Univariate and Multivariate Analysis of RFS and OS for Huge HCC After PSM |
Univariable analysis revealed that AFP >400 ng/mL (HR=2.173; 95% CI: 1.290~3.663; p=0.004), macrovascular invasion (HR=2.132; 95% CI: 1.289~3.527; p=0.003), satellites (HR=2.230; 95% CI: 1.381~3.602; p=0.001), ruptured tumor (HR=2.249; 95% CI: 1.178~4.292; p=0.014), intraoperative blood transfusion (HR=2.027; 95% CI: 1.237~3.321; p=0.005) and AIT (HR=0.344; 95% CI: 0.204~0.581; p<0.001) were factors significantly related to OS. Similarly, multivariable analysis showed that macrovascular invasion (HR=1.742; 95% CI: 1.038~2.926; p=0.036), satellites (HR=2.197; 95% CI: 1.295~3.726; p=0.004), intraoperative blood transfusion (HR=2.046; 95% CI: 1.194~3.505; p=0.009) and AIT (HR=0.319; 95% CI: 0.188~0.541; p<0.001) were independent predictors for OS (Table 4).
Subgroup Analysis
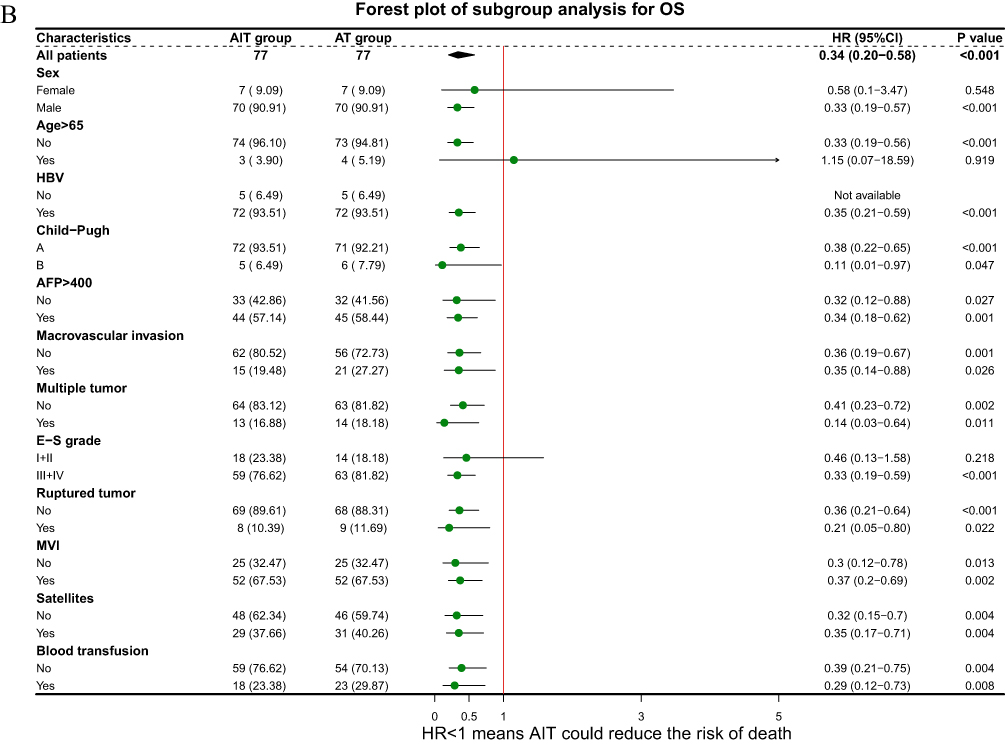
To further explore the potential value of AIT for improving RFS and OS, subgroup analysis was performed. The results indicated that AIT could significantly improve RFS in huge HCC patients with HBV infection, AFP >400 ng/mL, E-S grade III+IV, regardless of multiple tumors, satellites or vascular invasion (Figure 3A). In addition, AIT significantly improved OS in patients with E-S grade III+IV, regardless of AFP >400 ng/mL, multiple tumors, satellites or vascular invasion (Figure 3B). Figure 3 Continued. Figure 3 Forest plot for subgroup survival analysis for RFS (A) and OS (B). Abbreviations: AFP, alpha-fetoprotein; E-S, Edmonson-Steiner; MVI, microvascular invasion.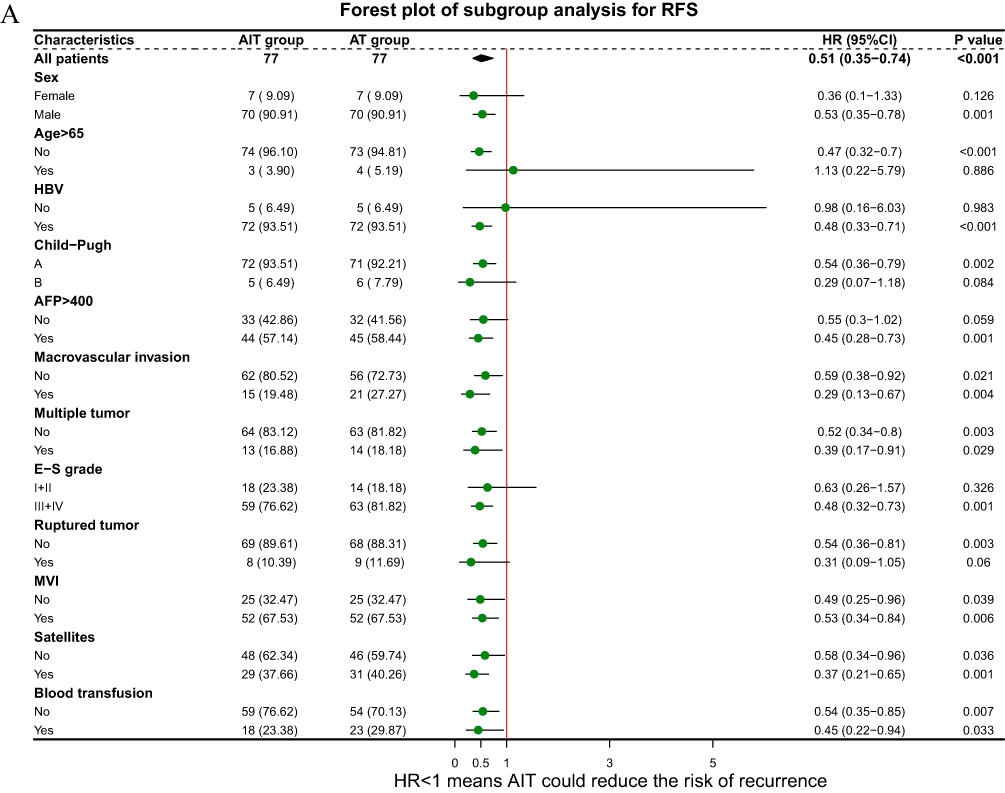
Discussion
Thanks to the development of surgical technic, hepatectomy has been conducted for many patients with huge HCC regardless of challenges and demonstrated as the only curative approach.4,5,22 Unfortunately, the high postoperative recurrence rate impaired the long-term oncological outcomes, especially for those with early recurrence.2,3,6 It is always a pursuit for hepatic surgeons to reduce early recurrence rates and gain a satisfactory oncological outcome by effective postoperative adjuvant therapies. Several studies showed that PA-TACE could significantly improve RFS and OS with well-tolerated toxicities for huge HCC patients.8,13,14,23 However, the early recurrence rates were still unsatisfactory. Recently, some studies and the guidelines of AASLD recommended that postoperative adjuvant PD-1 treatment could improve short-term survival outcomes for HCC patients with high recurrence risk, including large tumors, MVI, satellites, poor tumor differentiation.12,15,16,24 However, it is still uncertain whether the combined therapy of PA-TACE plus PD-1 inhibitors could achieve better anti-recurrence effect than PA-TACE alone. The study cohorts were established by PSM with well-balanced baseline characteristics, providing a more reliable comparison of short-term outcomes. As expected, we obtained a better survival outcome of RFS and OS with well-tolerated AEs in huge HCC patients who underwent combined therapy. This study was the first to evaluate the efficacy and safety of AIT for huge HCC patients.
Large tumors were associated with poor oncological prognosis due to early recurrence and distant metastasis. Early recurrence is possibly related to both the residual tumor cells and a dysfunctional tumor-immune microenvironment.25,26 PA-TACE could lead to necrosis of tumor cells by lipiodol embolization, which is related to the unique rich arterial blood supply of early micro-tumor nodules.13 However, TACE had no ability to suppress immune evasion. This might be the reason why TACE alone for huge HCC could not achieve a satisfactory outcome. A variety of studies have demonstrated the rationale of the combined therapy of TACE plus TKIs and PD-1 inhibitors for unresectable HCC, with better progression-free survival (9.7 vs 7.0 months), OS (24.0 vs 21.4 months) and objective response rate (52.4% vs 17.8%) compared to TACE plus TKIs.27,28 PD-1 inhibitors could block the tumor immune escape pathway and maintain the T cells’ tumor cell-killing activity by binding to PD-1 on the surface of T cells. TACE can effectively cause tumor necrosis, resulting in the release of tumor-specific antigens, which subsequently improves immunotherapy due to better antigen presentation.29
The recurrence of HCC is classified as early recurrence (within two years) and late recurrence (after two years) as early recurrence is generally considered to be metastasis via residual cancer related to the biologic features of tumors and late recurrence is considered to be newborn cancer related to underlying liver disease background.30,31 The primary endpoint should be set in early phase of recurrence to increase the statistical power if the efficacy of the treatment modalities, such as immunotherapy and TACE, lie in preventing the recurrence of residual cancer. Both in the crude and PSM cohorts, AIT showed a strong association with reduced early recurrence rate and prolonged OS in patients with huge HCC. The subgroup analysis showed that huge HCC patients could achieve benefit from AIT in most subgroups except female patients, older patients, patients with AFP ≤400ng/mL, E-S grade I+II or ruptured tumor or patients without HBV infection. Further studies to explore the efficacy in subgroups should be conducted because the number of patients in some subgroups was small, which may affect the results of the subgroup analysis.
Compared to the study of H. Wang et al related to huge HCC with PA-TACE, our results of RFS and OS were worse.23 The possible reasons were as follows: 1) our study subjects contained patients with macrovascular invasion; 2) the interval of follow-up was one month in our study but two months in the study of H. Wang et al. Compared to non-huge HCC, a more powerful risk of recurrence in huge HCC was extrahepatic metastasis. A study performed by Kenji demonstrated that more than 40% of patients with huge HCC relapsed in distant organs, especially in lung, while only 7% patients with non-huge HCC relapsed in distant organs.32 Our results were consistent with the results of previous study and the AIT group showed a lower extrahepatic metastasis rate, although without statistical significance. Another significant difference in the post-recurrence treatments was that more patients in the AT group underwent TACE alone again while more patients in the AIT group underwent TKIs followed repeat TACE and PD-1 inhibitors. This might be due to economic factors because the patients in the AIT group might have more wealth to receive systemic therapy. Differences in post-recurrence treatment also had an important impact on OS, which need to be considered. The median OS was longer in patients who underwent combined therapy compared with those underwent repeated TACE alone after recurrence (16.3 vs 11.1 months, p=0.21, Supplementary Figure 2)
The combined treatment of AIT was safe as a postoperative adjuvant modality for huge HCC. PA-TACE was demonstrated to be safe as adjuvant treatment.8,13 In our study, most patients experienced transient AEs and recovered well without severe AEs and treatment-related deaths during TACE treatment. Regard to immunotherapy, the occurrence rate of grade 3/4 AEs was 6.0%. According to the results of previous studies, the common AEs of PD-1 inhibitors, such as increased ALT or AST, fatigue, hypothyroidism, pruritus and asthenia, occurred in 64%~73% of HCC patients while grade ≥3 AEs occurred in 15%~24% of patients.33,34 The occurrence rates of AEs in our study were lower than the reported results. This might be attributed to the fewer injection circles of PD-1 inhibitors in this study. This study demonstrated the well-tolerated toxicity of PD-1 inhibitors as adjuvant treatment for HCC patients.
Analysis of associated risk factors showed that patients with macrovascular invasion, multiple tumors, satellites, and intraoperative blood transfusion had a poor prognosis. Cox regression analysis proved further that AIT was a protective factor related to RFS and OS. Multiple tumors or tumors with macrovascular invasion mean that the stage of HCC is more advance and the prognosis of patients is worse. Many studies showed that the presence of poor pathology performances, such as MVI, satellites, low-grade differentiation, were important predictors of postoperative recurrence and poor prognosis.30,31,35,36 Our results only supported satellites as an independent risk factor for the prognosis of huge HCC. Blood transfusion was associated with poor prognosis of HCC after surgery owing to the immunosuppressive effect, which has been reported in previous studies.37 The subgroup analysis showed that AIT could further reduce the risks of recurrence and mortality in subgroups of macrovascular invasion, multiple tumors, satellites, and intraoperative blood transfusion.
There are several limitations in our study. First, although we applied PSM to balance the baseline characteristics, potential biases were still inevitable due to the retrospective nature of our study. For instance, the types of PD-1 inhibitors could not be standardized. However, it is somewhat more consistent with the real-world applications of PD-1 inhibitors. Second, a control arm without any adjuvant treatment failed to be established owing to highly frequent loss to follow-up. Third, patients with HBV infection accounted for most of the cohorts. Whether the results obtained in this study can be generalized to HCV-related or alcohol-related HCC needs further investigation. Additionally, this was a single-center clinical study so that the sample size of this study was limited, and the duration of follow-up was relatively short. Thus, a multicenter, randomized controlled study with a large sample size is necessary to validate the conclusion of the study.
Conclusion
This study demonstrated that AIT, associated with better survival outcomes, would be a potentially effective adjuvant treatment with tolerable toxicities for huge HCC. However, a multicenter, randomized controlled study with a large sample size is necessary to further validate the conclusion of the study.
Abbreviations
AASLD, American Association for the Study of Liver Diseases; AEs, adverse events; AFP, alpha-fetoprotein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCLC, Barcelona Clinic Liver Cancer; CI, confidence interval; CT, computed tomography; ECOG, Eastern Cooperative Oncology Group; E-S, Edmonson-Steiner; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; HR, hazard ratio; ICIs, immune checkpoint inhibitors; MRI, magnetic resonance imaging; MVI, microvascular invasion; NLR, neutrophil-to-lymphocyte ratio; OS, overall survival; PA-TACE, postoperative adjuvant transarterial chemoembolization; PD-1, programmed cell death-1; PSM, propensity score matching; RFS, recurrence-free survival; TACE, transarterial chemoembolization; TKIs, tyrosine kinase inhibitors.
Data Sharing Statement
The data that support the findings of this study are not publicly available due to privacy or ethical restrictions but are available on request from the corresponding author.
Ethics Approval and Informed Consent
This study was approved by the institutional ethics committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (TJ-IRB20221125). Informed consent for all patients was waived by the committee due to the retrospective nature of this study. All included patients’ personal information is strictly confidential.
Funding
This study was supported by the Chen Xiao-ping Foundation for the Development of Science and Technology of Hubei Province (Grant numbers: CXPJJH1200008-21).
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Elhanafy E, Aboelinin M, Said R, et al. Outcomes of liver resection for huge hepatocellular carcinoma exceeding 10 cm in size: a single center experience. Am J Surg. 2023;225(6):1013–1021. doi:10.1016/j.amjsurg.2022.12.005
3. Wang J-C, Hou J-Y, Chen J-C, et al. Development and validation of prognostic nomograms for single large and huge hepatocellular carcinoma after curative resection. Eur J Cancer. 2021;155:85–96. doi:10.1016/j.ejca.2021.07.009
4. Wei C-Y, Chen P-C, Chau G-Y, et al. Comparison of prognosis between surgical resection and transarterial chemoembolization for patients with solitary huge hepatocellular carcinoma. Ann Transl Med. 2020;8(5):238. doi:10.21037/atm.2019.12.157
5. Bogdanovic A, Bulajic P, Masulovic D, Bidzic N, Zivanovic M, Galun D. Liver resection versus transarterial chemoembolization for huge hepatocellular carcinoma: a propensity score matched analysis. Sci Rep. 2021;11(1):4493.
6. Fang Q, Xie Q-S, Chen J-M, et al. Long-term outcomes after hepatectomy of huge hepatocellular carcinoma: a single-center experience in China. Hepatobiliary Pancreat Dis Int. 2019;18(6):532–537. doi:10.1016/j.hbpd.2019.09.001
7. Wang L, Liu Z, Liu X, Zeng Y, Liu J. The hepatectomy efficacy of huge hepatocellular carcinoma and its risk factors: a meta analysis. Medicine. 2017;96(52):e9226. doi:10.1097/MD.0000000000009226
8. Wang Z, Ren Z, Chen Y, et al. Adjuvant transarterial chemoembolization for HBV-related hepatocellular carcinoma after resection: a randomized controlled study. Clin Cancer Res. 2018;24(9):2074–2081. doi:10.1158/1078-0432.CCR-17-2899
9. Li S, Mei J, Wang Q, et al. Postoperative adjuvant transarterial infusion chemotherapy with FOLFOX could improve outcomes of hepatocellular carcinoma patients with microvascular invasion: a preliminary report of a Phase III, randomized controlled clinical trial. Ann Surg Oncol. 2020;27(13):5183–5190. doi:10.1245/s10434-020-08601-8
10. Wang W-H, Wang Z, J-X W, et al. Survival benefit with IMRT following narrow-margin hepatectomy in patients with hepatocellular carcinoma close to major vessels. Liver Int. 2015;35(12):2603–2610. doi:10.1111/liv.12857
11. Zhang X-P, Chai Z-T, Gao Y-Z, et al. Postoperative adjuvant sorafenib improves survival outcomes in hepatocellular carcinoma patients with microvascular invasion after R0 liver resection: a propensity score matching analysis. HPB. 2019;21(12):1687–1696. doi:10.1016/j.hpb.2019.04.014
12. Chen W, Hu S, Liu Z, et al. Adjuvant anti-PD-1 antibody for hepatocellular carcinoma with high recurrence risks after hepatectomy. Hepatol Int. 2023;17(2):406–416. doi:10.1007/s12072-022-10478-6
13. Wei W, Jian P-E, S-h L, et al. Adjuvant transcatheter arterial chemoembolization after curative resection for hepatocellular carcinoma patients with solitary tumor and microvascular invasion: a randomized clinical trial of efficacy and safety. Cancer Commun. 2018;38(1):61. doi:10.1186/s40880-018-0331-y
14. Chen W, Ma T, Zhang J, et al. A systematic review and meta-analysis of adjuvant transarterial chemoembolization after curative resection for patients with hepatocellular carcinoma. HPB. 2020;22(6):795–808. doi:10.1016/j.hpb.2019.12.013
15. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
16. Qin S, Chen M, Cheng A-L, et al. Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): a randomised, open-label, multicentre, Phase 3 trial. Lancet. 2023;402(10415):1835–1847. doi:10.1016/S0140-6736(23)01796-8
17. Kubota K, Makuuchi M, Kusaka K, et al. Measurement of liver volume and hepatic functional reserve as a guide to decision-making in resectional surgery for hepatic tumors. Hepatology. 1997;26(5):1176–1181. doi:10.1053/jhep.1997.v26.pm0009362359
18. Zhang B, Xu D, Wang R, et al. Perioperative antiviral therapy improves safety in patients with hepatitis B related HCC following hepatectomy. Int J Surg. 2015;15:1–5. doi:10.1016/j.ijsu.2014.12.030
19. Chen XP, Qiu FZ, Wu ZD, Zhang BX. Chinese experience with hepatectomy for huge hepatocellular carcinoma. Br J Surg. 2004;91(3):322–326. doi:10.1002/bjs.4413
20. Xu X, Zhang H-L, Liu Q-P, et al. Radiomic analysis of contrast-enhanced CT predicts microvascular invasion and outcome in hepatocellular carcinoma. J Hepatol. 2019;70(6):1133–1144. doi:10.1016/j.jhep.2019.02.023
21. Cong W-M, Bu H, Chen J, et al. Practice guidelines for the pathological diagnosis of primary liver cancer: 2015 update. World J Gastroenterol. 2016;22(42):9279–9287. doi:10.3748/wjg.v22.i42.9279
22. Min YW, Lee JH, Gwak G-Y, et al. Long-term survival after surgical resection for huge hepatocellular carcinoma: comparison with transarterial chemoembolization after propensity score matching. J Gastroenterol Hepatol. 2014;29(5):1043–1048. doi:10.1111/jgh.12504
23. Wang H, Yu H, Qian Y-W, Cao Z-Y, Wu M-C, Cong W-M. Postoperative adjuvant transcatheter arterial chemoembolization improves the prognosis of patients with huge hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int. 2021;20(3):232–239. doi:10.1016/j.hbpd.2020.12.018
24. Li J, Wang W-Q, Zhu R-H, et al. Postoperative adjuvant tyrosine kinase inhibitors combined with anti-PD-1 antibodies improves surgical outcomes for hepatocellular carcinoma with high-risk recurrent factors. Front Immunol. 2023;14:1202039. doi:10.3389/fimmu.2023.1202039
25. Rabinovich GA, Gabrilovich D, Sotomayor EM. Immunosuppressive strategies that are mediated by tumor cells. Annu Rev Immunol. 2007;25(1):267–296. doi:10.1146/annurev.immunol.25.022106.141609
26. Zhu X-D, K-s L, Sun H-C. Adjuvant therapies after curative treatments for hepatocellular carcinoma: current status and prospects. Genes Dis. 2020;7(3):359–369. doi:10.1016/j.gendis.2020.02.002
27. Jiang N, Zhong B, Huang J, et al. Transarterial chemoembolization combined with molecularly targeted agents plus immune checkpoint inhibitors for unresectable hepatocellular carcinoma: a retrospective cohort study. Front Immunol. 2023;14:1205636. doi:10.3389/fimmu.2023.1205636
28. Zhang J-X, Chen P, Liu S, Q-q Z, Shi H-B, Zhou C-G. Safety and efficacy of transarterial chemoembolization and immune checkpoint inhibition with camrelizumab for treatment of unresectable hepatocellular carcinoma. J Hepatocell Carcinoma. 2022;9:265–272. doi:10.2147/JHC.S358658
29. Sangro B, Sarobe P, Hervás-Stubbs S, Melero I. Advances in immunotherapy for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18(8):525–543.
30. J-c W, Huang Y-H, Chau G-Y, et al. Risk factors for early and late recurrence in hepatitis B-related hepatocellular carcinoma. J Hepatol. 2009;51(5):890–897. doi:10.1016/j.jhep.2009.07.009
31. Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003;38(2):200–207. doi:10.1016/S0168-8278(02)00360-4
32. Wakayama K, Kamiyama T, Yokoo H, et al. Huge hepatocellular carcinoma greater than 10 cm in diameter worsens prognosis by causing distant recurrence after curative resection. J Surg Oncol. 2017;115(3):324–329.
33. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label Phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
34. Ren Z, Ducreux M, Abou-Alfa GK, et al. Tislelizumab in patients with previously treated advanced hepatocellular carcinoma (RATIONALE-208): a multicenter, non-randomized, open-label, Phase 2 trial. Liver Cancer. 2023;12(1):72–84. doi:10.1159/000527175
35. Hwang S, Lee Y-J, Kim K-H, et al. Long-term outcome after resection of huge hepatocellular carcinoma ≥ 10 cm: single-institution experience with 471 patients. World J Surg. 2015;39(10):2519–2528. doi:10.1007/s00268-015-3129-y
36. Ercolani G, Grazi GL, Ravaioli M, et al. Liver resection for hepatocellular carcinoma on cirrhosis: univariate and multivariate analysis of risk factors for intrahepatic recurrence. Ann Surg. 2003;237(4):536–543. doi:10.1097/01.SLA.0000059988.22416.F2
37. Harada N, Shirabe K, Maeda T, Kayashima H, Ishida T, Maehara Y. Blood transfusion is associated with recurrence of hepatocellular carcinoma after hepatectomy in Child-Pugh class A patients. World J Surg. 2015;39(4):1044–1051. doi:10.1007/s00268-014-2891-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Early TACE Refractoriness on Survival in Patients with Hepatocellular Carcinoma: A Real-World Study
Yang C, Luo YG, Yang HC, Yao ZH, Li X
Journal of Hepatocellular Carcinoma 2022, 9:621-631
Published Date: 21 July 2022
Comparison of the Efficacy and Safety of Transarterial Chemoembolization with or without Lenvatinib for Unresectable Hepatocellular Carcinoma: A Retrospective Propensity Score–Matched Analysis
Chen YX, Zhang JX, Zhou CG, Liu J, Liu S, Shi HB, Zu QQ
Journal of Hepatocellular Carcinoma 2022, 9:685-694
Published Date: 1 August 2022
Retrospective Study of the Efficacy and Safety of Chemoembolization with Drug-Eluting Microspheres Combined with Intra-Arterial Infusion of Bevacizumab for Unresectable Hepatocellular Carcinoma
Ueda S, Hori S, Hori A, Makitani K, Wan K, Sonomura T
Journal of Hepatocellular Carcinoma 2022, 9:973-985
Published Date: 12 September 2022
High Platelet Count is a Potential Prognostic Factor of the Early Recurrence of Hepatocellular Carcinoma in the Presence of Circulating Tumor Cells
Lu Z, Huang Y, Huang J, Ni HH, Luo T, Wei X, Bai X, Qi L, Xiang B
Journal of Hepatocellular Carcinoma 2023, 10:57-68
Published Date: 14 January 2023
Early Recurrent Hepatocellular Carcinoma with CK19 Positive Receiving Transarterial Chemoembolization After Surgical Resection: A Novel Risk Model Study
Zhu D, Yang W, Zhou HF, Liu S, Zhou WZ, Shao ZF, Shi HB, Feng Q
Journal of Hepatocellular Carcinoma 2026, 13:563631
Published Date: 27 February 2026