Back to Journals » Journal of Pain Research » Volume 19
Acupuncture-Related Interventions for Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Authors Liu X ![]() , Ren L, Xu W, Huang W, Wang R
, Ren L, Xu W, Huang W, Wang R
Received 1 April 2026
Accepted for publication 2 June 2026
Published 9 June 2026 Volume 2026:19 612867
DOI https://doi.org/10.2147/JPR.S612867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Houman Danesh
Xin Liu,1 Luqian Ren,2 Wei Xu,3 Wenrui Huang,4 Rui Wang5
1Chinese Medicine Department, The 903rd Hospital of the Joint Logistics Support Force, Hangzhou, Zhejiang Province, People’s Republic of China; 2Obstetrics and Gynecology, The 903rd Hospital of the Joint Logistics Support Force, Hangzhou, Zhejiang Province, People’s Republic of China; 3Pulmonology, The 903rd Hospital of the Joint Logistics Support Force, Hangzhou, Zhejiang Province, People’s Republic of China; 4Obstetrics and Gynecology, Shenzhen Traditional Chinese Medicine Hospital, Shenzhen, Guangdong Province, People’s Republic of China; 5Department of Stomatology, The 903rd Hospital of the Joint Logistics Support Force, Hangzhou, Zhejiang Province, People’s Republic of China
Correspondence: Xin Liu, Email [email protected] Rui Wang, Email [email protected]
Background: Chronic prostatitis (CP) is a common condition for which pharmacological therapies often provide unsatisfactory outcomes. Acupuncture has emerged as a promising supportive therapy. However, further comparative studies are needed to clarify the relative effectiveness of different acupuncture modalities versus standard pharmacological therapies, particularly because most existing trials used active rather than sham-controlled comparisons.
Methods: This network meta-analysis (PROSPERO: CRD420251180258) evaluated acupuncture-related therapies for CP. Randomized controlled trials (RCTs) published through October 2025 were identified. The primary outcome was the National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI). Analyses were conducted using Stata 17.0, with mean differences (MDs), 95% confidence intervals (CIs), and SUCRA rankings calculated. Most included studies compared acupuncture-related therapies with pharmacological treatments rather than sham controls.
Results: Forty-five RCTs involving 3534 participants were included. Acupuncture-related therapies, alone or combined with medication, were associated with greater improvements in NIH-CPSI outcomes than conventional medications in active-controlled trials. Warm needle acupuncture (WMA) ranked highest for total NIH-CPSI improvement (SUCRA 94.1%) and response rate (RR = 1.35, 95% CI 1.20– 1.51; SUCRA 91.4%). Electroacupuncture (EA) demonstrated favorable effects across multiple outcomes, ranking second for total NIH-CPSI improvement (SUCRA 86.2%) and showing benefits in pain relief and quality of life. EA combined with Western medicine ranked highest for pain relief, while auricular acupoint therapy showed advantages for urinary symptoms. Manual acupuncture combined with Chinese herbal medicine ranked highest for quality-of-life improvement.
Conclusion: Acupuncture-related therapies may serve as useful complementary approaches for improving CP symptoms in active-controlled trials. WMA showed the greatest overall improvement and response rates, whereas EA and EA combined with Western medicine demonstrated benefits across multiple symptom domains. However, these findings should be interpreted cautiously because most studies were conducted in Chinese populations, evidence certainty was predominantly low to moderate, and long-term follow-up data were limited.
Keywords: chronic prostatitis, network meta-analysis, acupuncture-related therapies, warm needle acupuncture, electroacupuncture
Introduction
Prostatitis is a common urological condition affecting adult men. Studies show about 35%–50% of men experience prostatitis-related symptoms during their lifetime.1–3 In urology clinics, prostatitis accounts for about 8%–25% of patient visits.1–3 In China, the reported incidence of chronic prostatitis (CP) ranges from 6.0% to 32.9%,4 while globally, between 1% and 14.2% of people are affected.3,5,6 Even though CP is common, primary-care doctors often miss it. Evidence also suggests a possible link between CP and an increased risk of benign prostatic hyperplasia (BPH) and prostate cancer.3,7 CP is primarily characterized by chronic pelvic pain, urinary symptoms, and varying degrees of sexual and psychological dysfunction, all of which can substantially impair quality of life.4,8–12
The causes of CP are not fully understood and likely involve many factors, including infection, immune dysfunction, nerve and hormone imbalances, and pelvic muscle problems.13,14 Current management of CP commonly includes alpha-blockers, antibiotics, and anti-inflammatory medications, with antibiotics commonly used in selected patients, often for treatment courses lasting at least four weeks.15–19 However, treatment responses remain variable, and long-term outcomes are often unsatisfactory, partly because of antibiotic resistance and individual differences in treatment response.19,20 In addition, pharmacological treatments may cause side effects such as dizziness, low blood pressure, and gastrointestinal discomfort, which can reduce patient adherence.17,18
Given these limitations, acupuncture has drawn interest as a potential non-drug treatment. Several clinical trials show acupuncture can relieve pelvic pain and urinary symptoms and improve NIH Chronic Prostatitis Symptom Index (NIH-CPSI) scores.21,22 The therapeutic benefits may persist over time, with better symptom control and quality of life compared to sham acupuncture.21,22 Acupuncture may work through several pathways: reducing inflammation, balancing immune function, improving antioxidant activity, influencing nerve signals, relaxing pelvic muscles, and modifying pain-related brain activities.23,24
It should be noted that acupuncture-related therapies include several distinct technical forms, including Manual Acupuncture (MA), Electroacupuncture (EA), Warm Needle Acupuncture (WMA), Heat-Sensitive Moxibustion (SMS), Acupoint Application Therapy (AAT), and Moxibustion (MOX). These modalities differ in stimulation characteristics and potential mechanisms of action, which may contribute to differences in clinical outcomes. However, direct head-to-head comparisons among different acupuncture-related therapies remain limited. Previous conventional meta-analyses could not adequately evaluate the relative efficacy of different acupuncture modalities.25 Network meta-analysis (NMA) is better suited to compare and rank different acupuncture-related therapies by using both direct and indirect evidence. Clearer classification of acupuncture stimulation types may also improve the interpretability and clinical applicability of comparative findings. This study aims to provide a clearer comparison of the effectiveness and safety of different acupuncture-related therapies for the treatment of CP and to help inform clinical practice.
Methods
This systematic review and network meta-analysis was conducted in accordance with the PRISMA 2020 statement and its extension for NMA.26,27 The study protocol was prospectively registered with PROSPERO (CRD420251180258). The registered protocol is publicly accessible through the PROSPERO database under registration number CRD420251180258. No amendments were made to the protocol after registration.
Research Question (PICOS)
The review question was defined according to the PICOS framework:
Population
Adult patients diagnosed with chronic prostatitis according to established clinical criteria.
Interventions
Acupuncture-related therapies (including manual acupuncture, electroacupuncture, warm needle acupuncture, heat-sensitive moxibustion, moxibustion, and auricular acupoint therapy), administered either as monotherapy or in combination with conventional Western medicine or Chinese herbal medicine.
Comparators
Western medicine alone, Chinese herbal medicine alone, or other eligible acupuncture modalities.
Outcomes
Primary outcomes were the NIH-CPSI total score and subscores (pain, urinary symptoms, quality of life); secondary outcome was the response rate.
Study Design
Randomized controlled trials published in Chinese or English.
Eligibility Criteria
Study Type
Eligible randomized controlled trials (RCTs) published in Chinese or English evaluated the effectiveness and safety of acupuncture-related therapies for prostatitis. Trials were eligible regardless of whether blinding or allocation concealment was used, as these procedures are often difficult to apply in acupuncture studies. Non-randomized studies, quasi-experimental studies, case reports, and reviews were excluded.
Participants
Eligible participants were adults diagnosed with CP according to established clinical criteria. There were no limits on age, CP subtype, disease duration, or severity, as long as the starting characteristics were similar between the treatment and control groups.
Interventions and Comparators
The intervention group received acupuncture-related therapies, given either as standalone treatments or in combination with conventional Western medicine (WM) or Chinese herbal medicine (CHM). Eligible approaches included AAT, EA, MA, MOX, SMS, and WMA, along with their combinations with oral medications (eg, EA + WM, EA + CHM). To maintain clinical consistency, included interventions were limited to: (i) acupuncture monotherapy or (ii) acupuncture combined with WM or CHM. We excluded trials that combined different acupuncture modalities or used sham acupuncture.
Control groups received WM alone, CHM alone, or one eligible acupuncture type. This design allowed for direct and indirect comparisons within a NMA.
Outcomes
The primary outcomes were the NIH-CPSI total score and its subscores for pain, urination, and quality of life. The secondary outcome was the response rate.
Search Strategy
English and Chinese databases were systematically searched for RCTs evaluating acupuncture-related therapies for CP. English databases included PubMed, Embase, Web of Science, and Cochrane Library; Chinese databases covered CNKI, Wanfang Data, VIP, and CBM. The search strategy followed the PICOS framework and combined Medical Subject Headings (MeSH) with free-text terms. We used Boolean operators (AND/OR) to connect synonyms and related concepts. Population terms included “chronic prostatitis,” “chronic pelvic pain syndrome,” and “CP/CPPS.” Intervention termscovered “acupuncture,” “electroacupuncture,” “moxibustion,” “heat-sensitivemoxibustion,” “warm acupuncture,” and “acupoint application therapy.” We focused on RCTs using keywords like “randomized controlled trial.” The search covered records from each database’s inception to October 1, 2025, without language restrictions. Two researchers independently checked the studies for eligibility and settled any disagreements through discussion or by consulting a third reviewer. Detailed search strategies are provided in Appendix 1.
Study Selection and Data Extraction
Two reviewers went through all the records on their own, using a two-stage method with pre-established criteria: initial title/abstract screening followed by full-text assessment. Duplicate records were removed using EndNote and checked manually. Clearly irrelevant studies were removed in the first screening, while those needing more assessment went on to a full-text review. Full-text articles were carefully checked to make sure they met the inclusion criteria for population, interventions, and outcomes. Studies with missing or unclear data were excluded if we could not get the necessary information from the authors. When there were duplicate publications, we kept the version with the most complete data and best methods. Any disagreements between reviewers were settled by discussion or with help from a third reviewer.
Data were extracted independently using standard forms. Extracted information included: study characteristics (authors, publication year, sample size, randomization methods, blinding procedures, participant demographics), intervention details (acupuncture modality, combination therapies, treatment duration and frequency), and comparator information. The main outcomes were the NIH-CPSI total score and its subscales (pain, urinary symptoms, and quality of life), while the response rate was a secondary outcome. All the collected data were double-checked before analysis to make sure they were accurate and complete. In addition to outcome data, we extracted prespecified study-level variables including publication year, country, diagnostic criteria, sample size, participant age, intervention type, comparator type, treatment duration, treatment frequency, and methodological characteristics relevant to risk-of-bias assessment. For studies with unclear or incomplete information, attempts were made to determine the necessary information from the published report; when outcome data remained unavailable or could not be derived in a usable form, the study was excluded from the corresponding quantitative synthesis. No imputation of missing outcome data across trials was performed.
Risk of Bias and Certainty of Evidence Assessment
A rigorous approach was used to assess the quality of the evidence. Two reviewers independently evaluated the risk of bias in each included study using the RoB 2.0 tool,28 which examines five domains: the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selective reporting. Any disagreements were resolved through discussion or consultation with a third reviewer. Studies meeting the predefined criteria were considered low risk. The certainty of evidence for the main outcomes was further assessed using the CINeMA framework, which is based on GRADE, through its online platform. The assessment covered six domains: within-study bias, reporting bias, indirectness, imprecision, heterogeneity, and inconsistency. Final confidence ratings were then generated for the evidence.
Statistical Analysis
NMA was performed using Stata 17.0 with the mvmeta command under a frequentist framework. For continuous outcome measures, including the NIH-CPSI total score and its subdomain scores for pain, urinary symptoms, and quality of life, pooled mean differences along with 95% confidence intervals were calculated. The response rate was analyzed using risk ratios and 95% confidence intervals. All analyses used random-effects models, with heterogeneity estimated by restricted maximum likelihood and reported as τ2 values.29–31To evaluate consistency between direct and indirect evidence, we applied the node-splitting method. Network diagrams were used to show evidence structures, and treatment efficacy was ranked using the surface under the cumulative ranking curve (SUCRA).32 Finally, we assessed potential publication bias and small-study effects through adjusted funnel plots. Study selection was summarized using a PRISMA flow diagram. Characteristics of included studies are summarized in Table 1. Network geometry was presented using network plots, and synthesis results were presented using forest plots, league tables, SUCRA-based treatment rankings, and Supplementary Appendices where appropriate. Prior to synthesis, interventions were grouped into clinically meaningful treatment nodes according to acupuncture modality and whether they were administered alone or in combination with Western medicine or Chinese herbal medicine. We assessed statistical heterogeneity using the between-study variance (τ2) estimated under the random-effects model and interpreted heterogeneity in conjunction with the distribution of study characteristics across comparisons. We also examined inconsistency between direct and indirect evidence using node-splitting analyses. Because the included studies were limited for several direct comparisons and the network structure was relatively sparse for some outcomes, no additional subgroup analyses or formal meta-regression analyses were undertaken. No sensitivity analyses were conducted.
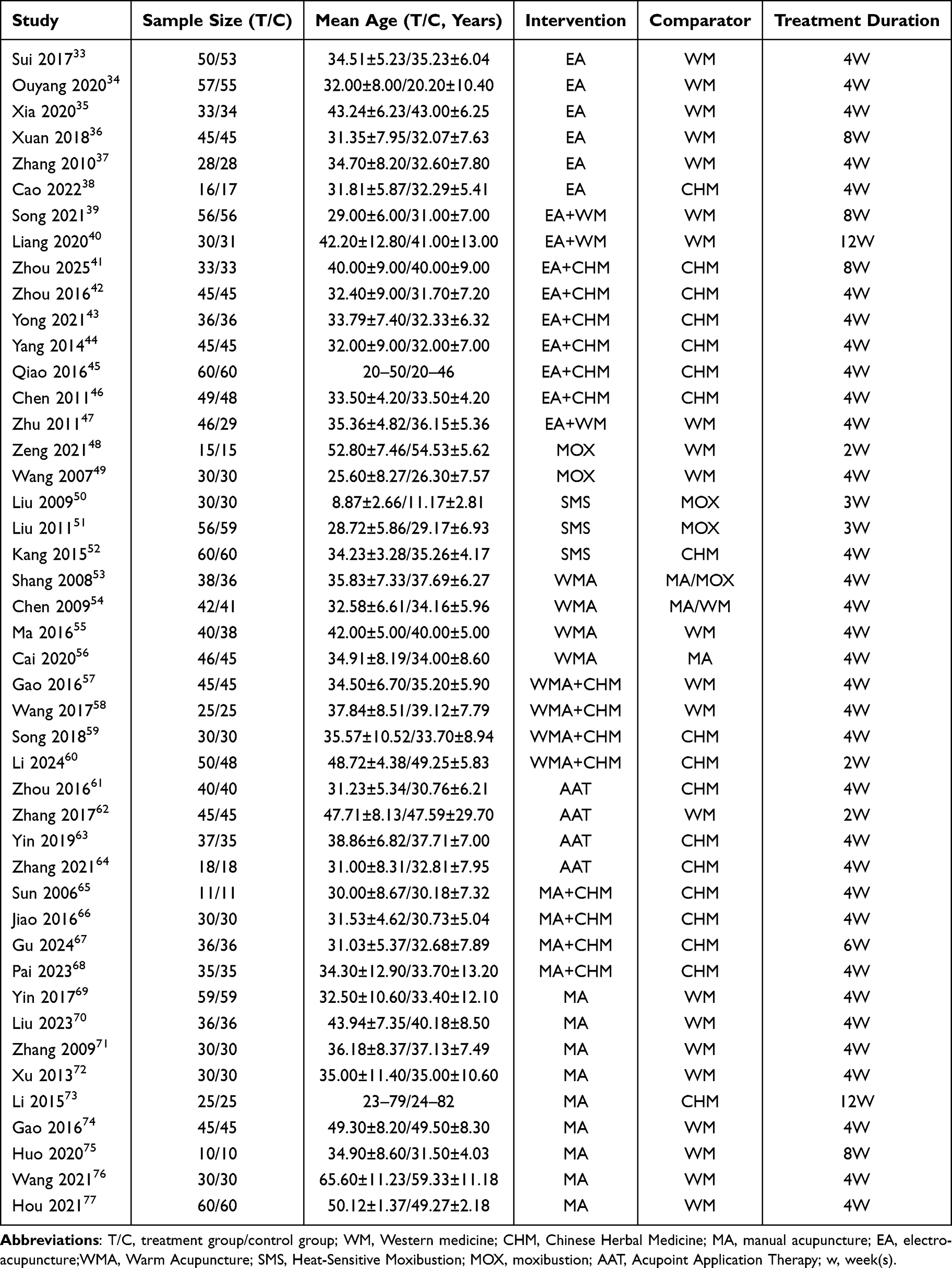 |
Table 1 Characteristics of Included Studies |
Results
Literature Search Results
The initial search identified 1,924 records from nine databases: PubMed (n=113), Embase (n=159), Cochrane Library (n=52), Web of Science (n=122), CNKI (n=426), VIP (n=210), Wanfang Data (n=361), and CBM (n=481). After removal of 959 duplicates, 965 unique records remained for title and abstract screening, of which 700 were excluded as clearly irrelevant. The remaining 265 reports underwent full-text assessment for eligibility. Of these, 220 reports were excluded because of non-randomized design, ineligible population, ineligible intervention or comparator, insufficient outcome data, duplicate publication, or failure to meet other predefined eligibility criteria. Finally, 45 RCTs33–77 were included in the quantitative synthesis and network meta-analysis (Figure 1).
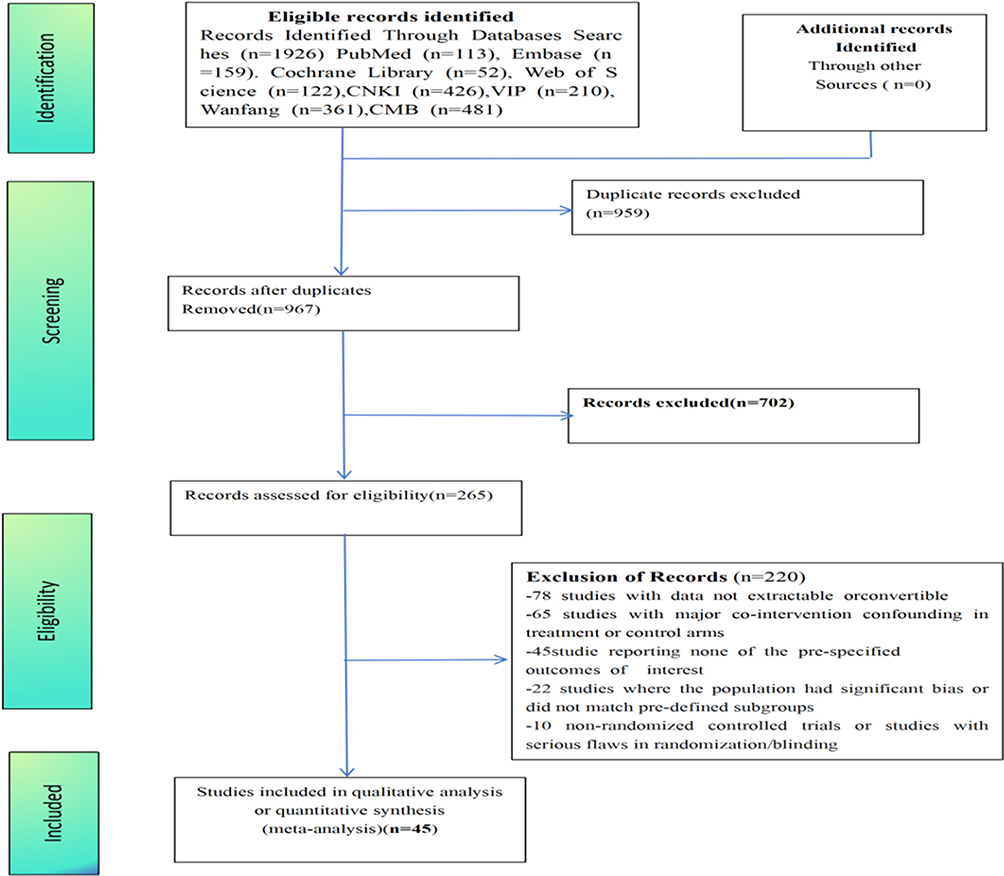 |
Figure 1 Flow chart of the search for eligible RCTs. |
Included Study Characteristics
This analysis examined 45 RCTsprimarily conducted in China between 2007 and 2025. The sample sizes generally ranged from 10 to 60 participants per study arm, with most trials enrolling 30 to 45 patients. There was a wide age range among participants, with the majority aged 30 to 50. Several studies included older adults, such as Wang et al (2021), where the mean age was around 60 years. The investigated interventions encompassed various acupuncture modalities, including EA, WMA, SMS, MOX, AAT, and MA, applied either as monotherapy or in combination with WM or CHM. The control groups received WM, CHM, or different acupuncture methods. Treatment duration was typically 4 weeks, though some trials implemented courses lasting 2, 3, 6, 8, or 12 weeks. All these studies formed a connected network of comparisons between treatments and controls, with participants having comparable starting characteristics (Table 1). The main characteristics and outcome domains reported by individual studies are summarized in Table 1.
Risk of Bias, Consistency and Certainty of Evidence
We assessed the methodological quality of the included studies using the Cochrane Risk of Bias 2.0 tool (RoB 2.0). Of the 45 randomized controlled trials, 38 (84.4%) were judged as low risk in the randomization process, whereas 7 (15.6%) raised some concerns because the methods used for sequence generation or allocation concealment were insufficiently described. For deviations from intended interventions, 44 studies (97.8%) were judged as having some concerns, mainly because blinding of participants and personnel is difficult to implement in acupuncture trials, while 1 study (2.2%) was rated as low risk. All studies were judged as low risk for missing outcome data, outcome measurement, and selective reporting. Overall, 1 study (2.2%) was rated as low risk of bias, 35 (77.8%) as having some concerns, and 9 (20.0%) as high risk. Detailed domain-level assessments are presented in Figure 2 and Appendix 2, Table S1.
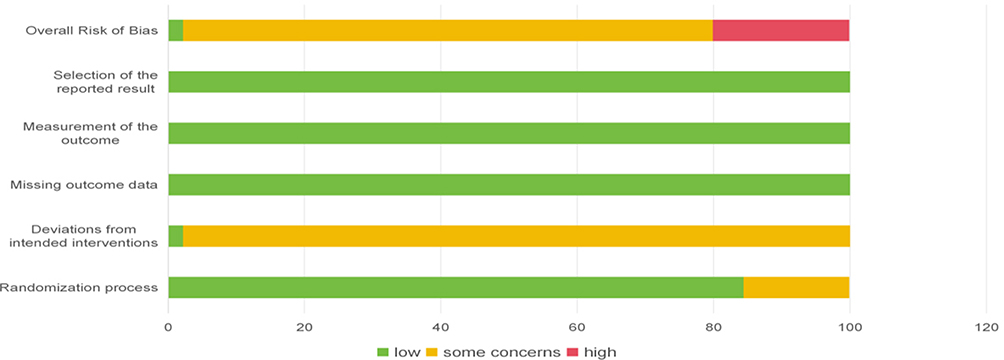 |
Figure 2 Risk-of-bias assessment of included studies using the RoB 2.0 tool. Green indicates low risk, yellow indicates some concerns, and red indicates high risk of bias. |
For network assumptions, both global and local consistency assessments supported the use of the consistency model (Appendix 3, Table S2). Node-splitting analyses showed no statistically significant disagreement between direct and indirect evidence across evaluated comparisons (all P > 0.05; Appendix 3, Table S3, Table S4). Between-study heterogeneity, expressed as τ2, was low to moderate across outcomes and remained within an acceptable range for interpretation. Adjusted funnel plots did not show major asymmetry, suggesting no strong evidence of small-study effects or major reporting bias (Appendix 4, Figure S1–S5). Confidence in the evidence, assessed using the CINeMA framework, was generally low to moderate for many comparisons, although some comparisons were rated very low and some key comparisons were supported by higher-certainty evidence. Overall, these findings suggest that the network estimates are reasonably robust in parts of the network, but several comparisons still warrant cautious interpretation because of study limitations, imprecision, heterogeneity, and incoherence (Appendix 5, Figures S6–S13 and Tables S5–S8). No additional subgroup analyses, meta-regression analyses, or sensitivity analyses were performed. Accordingly, the robustness of the findings was judged primarily on the basis of network consistency, heterogeneity estimates, and certainty-of-evidence assessment.
Network Diagrams of NIH-CPSI Scores
The NIH-CPSI total score and subscales formed well-connected networks with WM and CHM as central nodes, connected to various acupuncture therapies including MA, EA, WMA, and their combinations. This design allowed for complete comparisons of the treatments, with edge thickness representing study numbers and node size indicating sample size (Figure 3).
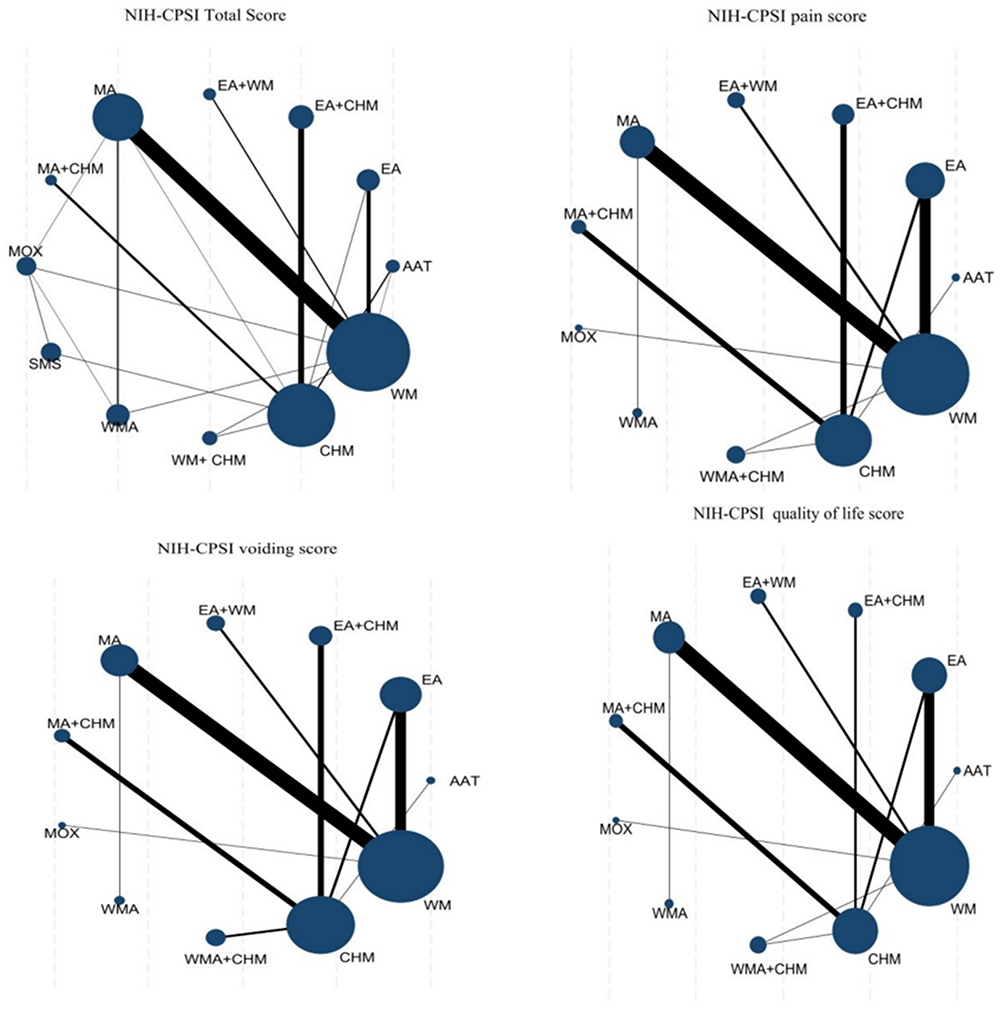 |
Figure 3 Network plots for the primary outcomes. Node size represents the sample size of each intervention, and line thickness represents the number of direct comparisons. |
NIH-CPSI Total Score
Analysis of the forest plot (Figure 4) showed that acupuncture therapies, whether used alone or combined with conventional oral medications, consistently reduced NIH CPSI total scores compared to oral drug controls. The treatments led to notable improvements, especially over CHM. WMA, EA, and EA with WM were the most effective. Specific results showed WMA versus CHM (MD −6.81, 95% CI −9.14 to −4.48; SUCRA 94.1%; high certainty evidence) and WMA versus WM (MD −5.55, 95% CI −7.27 to −3.83; SUCRA 94.1%; high certainty evidence). EA was effective compared with CHM (MD −6.05, 95% CI −8.15 to −3.95; SUCRA 86.2%; low certainty evidence) and with WM (MD −4.78, 95% CI −6.30 to −3.72; SUCRA 86.2%; low certainty evidence). EA plus WM showed effectiveness versus CHM (MD −6.00, 95% CI −8.80 to −3.21; SUCRA 84.1%; low certainty evidence) and versus WM (MD −4.74, 95% CI −6.94 to −2.54; SUCRA 84.1%; low certainty evidence) (Appendix 6, Figure S14, Table S9; Appendix 5, Table S5).
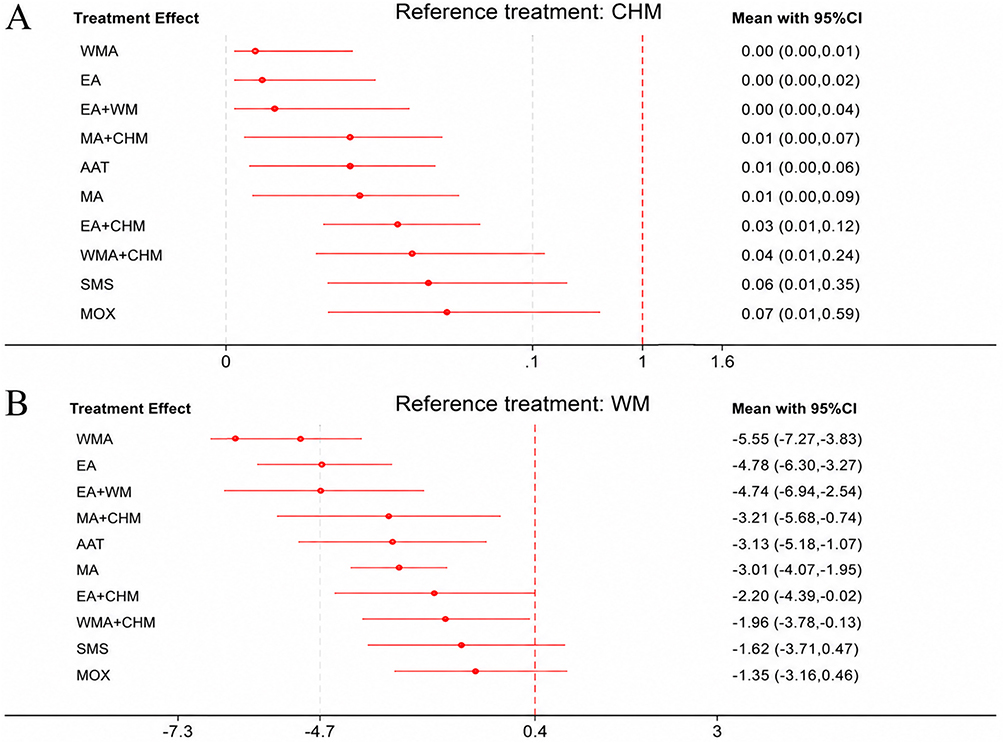 |
Figure 4 Forest plots for NIH-CPSI total score. (A) Compared with CHM; (B) compared with WM. |
The league table (Appendix 7, Table S14) suggestedthat EA and EA+WM were more effective compared to other interventions. EA showed better results than several other treatments: EA+CHM (−2.58, −5.09 to −0.07, 86.2%), MOX (−3.43, −5.74 to −1.13, 86.2%), SMS (−3.16, −5.64 to −0.69, 86.2%), and WMA+CHM (−2.83, −5.11 to −0.55, 86.2%). Additionally, EA+WM showed significant improvements compared with MOX (−3.39, −6.24 to −0.55, 84.1%) and SMS (−3.12, −6.16 to −0.08, 84.1%). None of the remaining comparisons were statistically significant.
NIH-CPSI Pain Subscore
Forest plot analysis (Figure 5) showed that acupuncture therapies, either as monotherapy or combined with oral medications, consistently produced greater reductions in NIH-CPSI pain subscores than oral drug controls. Specifically, when compared with CHM, three interventions showed statistically significant improvements: AAT (MD −2.24, 95% CI −4.26 to −0.58; SUCRA 76.6%), EA (MD −2.07, 95% CI −3.90 to −0.25; SUCRA 71.5%), and MA+CHM (MD −2.06, 95% CI −3.41 to −0.72; SUCRA 69.3%) (Appendix 6, Figure S15, Table S10; Appendix 5, Table S6).
Compared to WM, several interventions presented enhanced effects: EA+WM (MD −3.28, −5.02 to −1.55; 80.4%), AAT (MD −3.13, −5.78 to −0.48; 76.6%), EA (MD −2.78, −3.82 to −1.75; 71.5%), MA+CHM (MD −2.78, −5.11 to −0.44; 69.3%), WMA (MD −2.37, −4.51 to −0.23; 58.2%), and MA (MD −1.84, −2.87 to −0.81; 42.9%). The league table (Appendix 7, Table S15) showed no other statistically significant differences between intervention pairs.
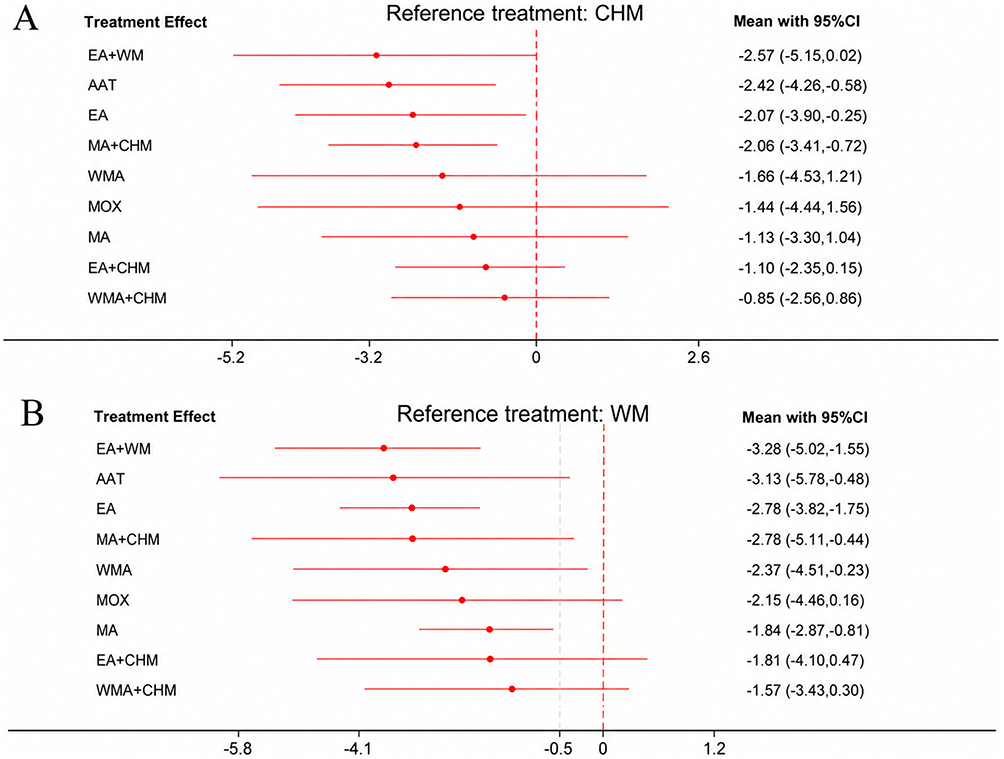 |
Figure 5 Forest plots for NIH-CPSI pain score. (A) Compared with CHM; (B) compared with WM. |
NIH-CPSI Urinary Subscore
Forest plot analysis (Figure 6) showed that acupuncture treatments, whether used alone or with oral medications, reliably improved NIH-CPSI urinary subscores compared with oral medication alone. When compared with CHM, three interventions showed statistically significant benefits: AAT (MD −1.60, 95% CI −3.11 to −0.09; SUCRA 83.4%), MA+CHM (MD −1.20, 95% CI −2.18 to −0.22; SUCRA 73.7%), and EA+CHM (MD −1.16, 95% CI −2.13 to −0.19; SUCRA 72.8%) (Appendix 6, Figure S16, Table S11; Appendix 5, Table S7).
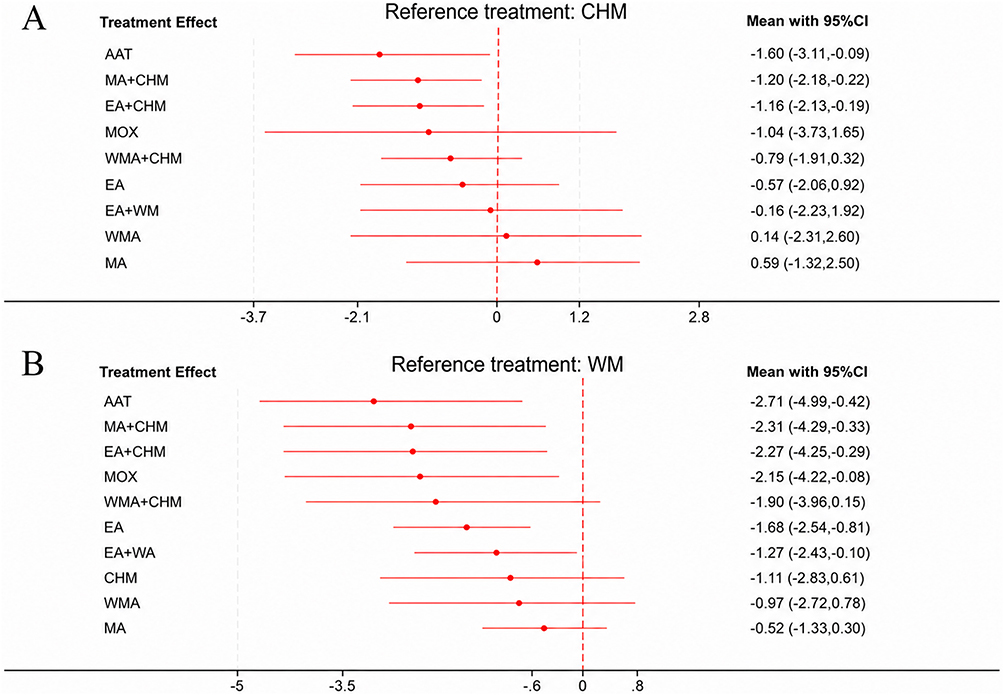 |
Figure 6 Forest plots for NIH-CPSI urinary score. (A) Compared with CHM; (B) compared with WM. |
Compared to WM, multiple interventions showed advantages: AAT (MD −2.71, −4.99 to −0.42; 83.4%), MA+CHM (MD −2.32, −4.29 to −0.33; 73.7%), EA+CHM (MD −2.27, −4.25 to −0.29; 72.8%), MOX (MD −2.15, −4.22 to −0.08; 67.5%), EA (MD −1.68, −2.54 to −0.81; 56.5%), and EA+WM (MD −1.27, −2.43 to −0.10; 43.2%). The league table (Appendix 7, Table S16) presented no other statistically significant differences between intervention pairs.
NIH-CPSI Quality of Life Subscore
Forest plot analysis (Figure 7) indicated that most acupuncture interventions, whether used alone or in combination with conventional oral medications, showed improving trends in NIH-CPSI quality of life subscores compared to CHM, though these were not statistically significant. The exception was MA+CHM (MD −1.79, 95% CI −2.93 to −0.66; SUCRA 83.6%), which showed both clinically meaningful improvement and statistical significance.
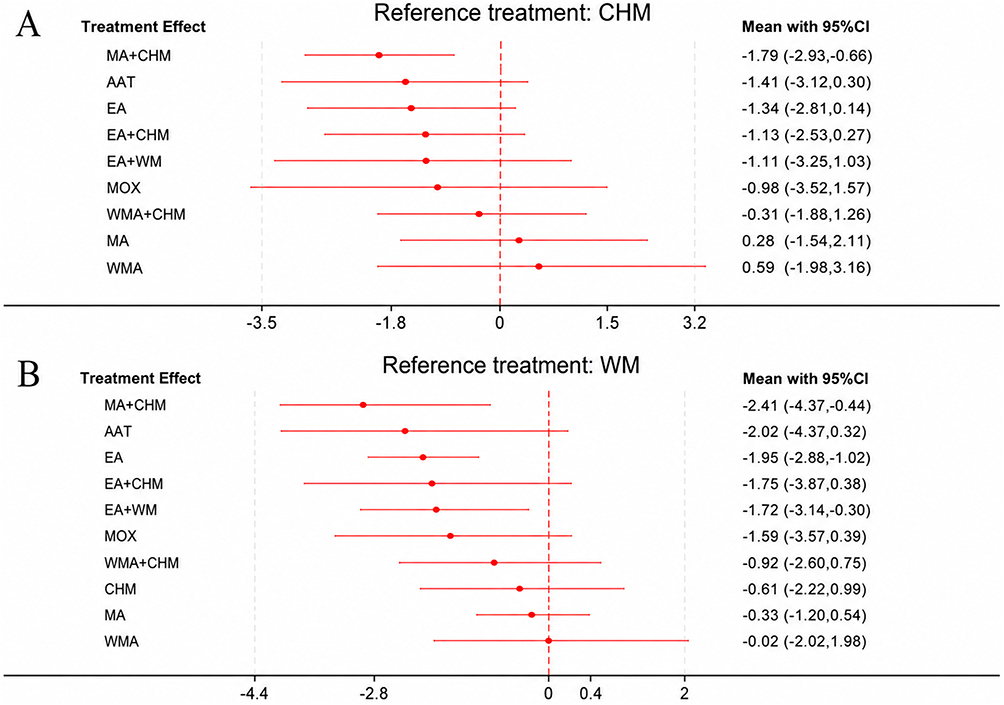 |
Figure 7 Forest plots for NIH-CPSI quality-of-life score. (A) Compared with CHM; (B) compared with WM. |
Compared to WM, showed statistically significant benefits: MA+CHM (MD −2.41, −4.37 to −0.44; 83.6%), EA (MD −1.95, −2.88 to −1.02; 74.6%), and EA+WM (MD −1.72, −3.14 to −0.30; 66.1%) (Appendix 6, Figure S17, Table S12; Appendix 5, Table S8). The league table (Appendix 7, Table S17) showed no other significant differences in direct comparisons between treatment pairs.
Whether used alone or in combination with conventional medications (either CHM or WM), most treatments showed clear advantages over oral medication alone in reducing the total NIH-CPSI score and its subscale scores, with advantages particularly evident for WMA, EA (either as monotherapy or combined with conventional oral medications), and AAT compared to control groups receiving oral drugs.
Response Rate
The network structure (Figure 8) showed high connectivity, with WM and CHM acting as central nodes that connected multiple acupuncture interventions including MA, EA, WMA, SMS, AAT, MOX, and their combination therapies. This configuration allowed for thorough direct and indirect comparisons of treatments. Forest plot analysis (Figure 9) indicated that most acupuncture-related therapies showed improved response rates compared to CHM and WM. Significant improvements were seen with WMA (RR 1.34, 95% CI 1.12 to 1.60; SUCRA 91.4%), EA+CHM (1.05, 0.86 to 1.27; 77.6%), MA +CHM (1.20, 1.03 to 1.39; 65.3%), and SMS (1.18, 1.01 to 1.38; 61.7%). Compared to WM, all acupuncture therapies, particularly WMA (1.35, 1.20 to 1.51; SUCRA 91.4%), EA+CHM (1.25, 1.06 to 1.48; 77.6%), SMS (1.19, 1.01 to 1.39; 61.7%) showed improved response rates, with statistically significant effects (Appendix 6, Figure S18, Table S13). The analysis in the league table (Appendix 7, Table S18) showed that WMA was better than EA, EA plus WM, MA, and MOX, with significant statistical differences.
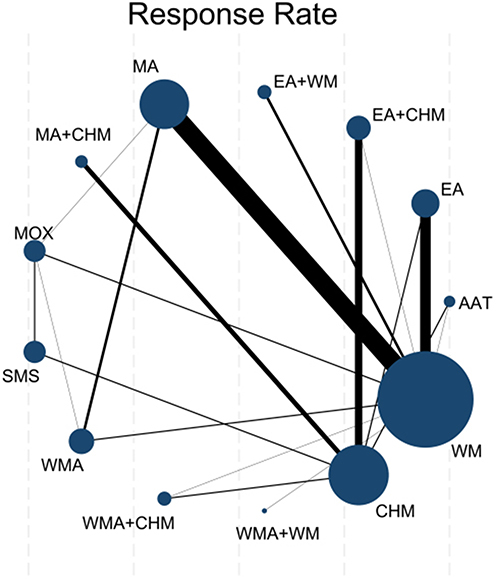 |
Figure 8 Network plots for response rate. Node size represents the sample size of each intervention, and line thickness represents the number of direct comparisons. |
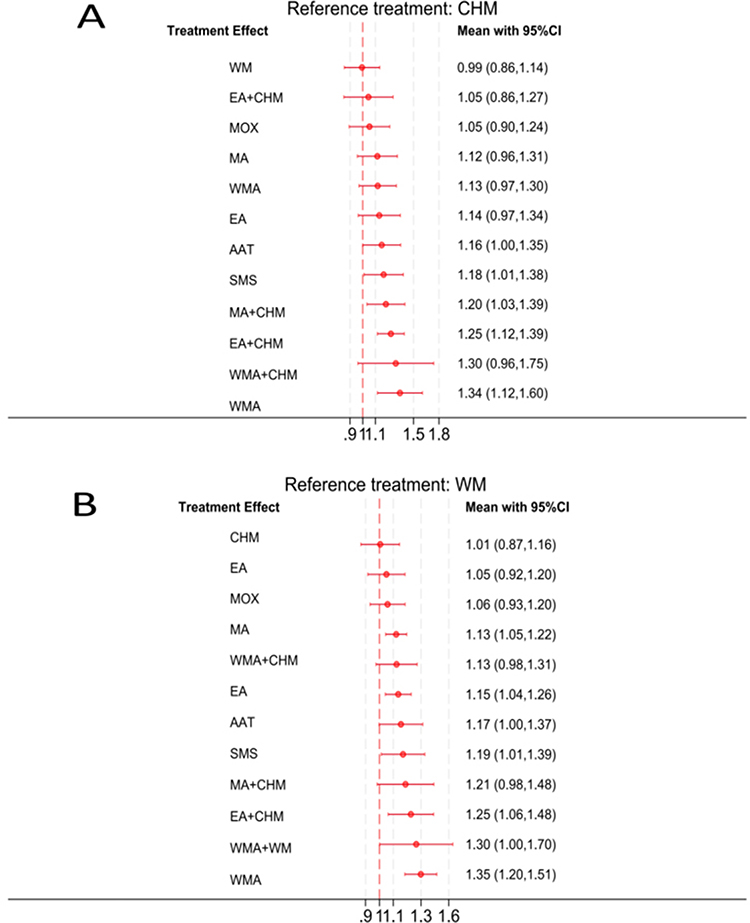 |
Figure 9 Forest plots for response rate. (A) Compared with CHM; (B) compared with WM. |
Adverse Events
The included clinical studies on CP showed that MA, EA, MOX, and CHM were generally safe, with no serious side effects reported. Minor and short-lived reactions happened occasionally, including acupuncture-related vasovagal responses (eg, dizziness or sweating), localized bleeding or needle retention, gastrointestinal discomfort associated with herbal medicine, and local skin reactions following acupoint application. These reactions were generally mild, self-limiting, and did not require stopping therapy. Furthermore, there were no significant differences in side effect rates between the intervention and control groups, indicating that these therapies are well tolerated and generally safe for managing CP.
Discussion
Primary Findings
This NMA of 45 RCTs suggests most acupuncture-related therapies were associated with greater symptom improvement than medication alone in active-controlled trials.78 WMA and EA showed relatively consistent benefits across several major symptom domains. WMA showed the most consistent improvements in overall symptom scores and response rates, while EA, either alone or combined with WM, was associated with improvements in pain relief and quality of life. Nevertheless, these findings should be interpreted with caution because many included studies had methodological limitations and relied predominantly on active-controlled rather than sham-controlled designs. Further high-quality sham-controlled studies are still needed to confirm these findings.
Comparison with Previous Evidence
The present findings are consistent with previous systematic reviews and meta-analyses.79,80 Current evidence indicates that acupuncture significantly improves NIH-CPSI scores, pain, and urinary symptoms in CP/CPPS patients.80 Specifically, verum acupuncture has been associated with greater reductions in NIH-CPSI total scores (MD = −6.41)25 and higher response rates compared to sham acupuncture and WM,78 which the present NMA further supports. Regarding safety, observed minor adverse events, including subcutaneous hematoma and temporary pain, are in line with previous reports25 and are far less severe than potential systemic reactions associated with oral medications.25 The present findings contrast with a 2024 NMA by Qin et al81 which found long-needle and thumb-tack needles to be the most effective, but had serious flaws in its methods. The “thumb-tack needle paradox” shows that while these needles appear effective, their mechanism seems unlikely,81 suggesting possible statistical errors.25 Furthermore, the study confused needle length with stimulation method, because long needles are frequently used for EA or WMA,82 which likely led to wrongly assigning the effects of stimulation to needle length. In comparison, our NMA used clear definitions of interventions, separating thermal and electrical stimulation, and identified WMA and EA as the most favorable modalities based on solid methods and results that can be applied in practice.
Mechanisms of Acupuncture Therapies for CP
WMA achieves its effects by using both needling and moxibustion. The thermal component induces vasodilation that significantly improves prostatic microcirculation and enhances inflammatory mediator clearance,83 while simultaneously downregulating local pro-inflammatory cytokines and relaxing hypertonic pelvic floor muscles.81 EA shows clear benefits in reducing central sensitization and improving neuromuscular function,84 while both EA and WMA offer overall pain relief and anti-inflammatory effects.
Dual Synergistic Mechanisms of Warm Needle Acupuncture
WMA combines the mechanical effect of needling with the heat from moxibustion, creating a combined effect that improves treatment outcomes.14 The thermal component induces vasodilation that significantly improves local prostatic microcirculation,83 enhances inflammatory mediator clearance, and consequently reduces tissue congestion and edema, advantages not achieved by MA alone. At the same time, the heat from moxibustion (around 47–52°C)17 works together with needling to reduce local pro-inflammatory cytokines (including TNF-α and IL-1β)81 while relaxing hypertonic pelvic floor musculature, thereby providing direct pain relief and anti-inflammatory effects.81
Multi-Level Neuroregulatory Mechanisms of EA
As a therapy that acts on the nervous system outside the central nervous system, EA affects CP/CPPS processes in different ways through specific electrical frequency stimulation.85 Locally, EA suppresses inflammatory responses and oxidative stress in prostatic tissue, reducing levels of pro-inflammatory factors (eg, IL-1β, IL-6, TNF-α) and oxidative stress markers (COX-2, iNOS, MDA).86 At the spinal level, EA directly inhibits hyperactivation of dorsal horn glial cells, downregulates activation markers (including GFAP and Iba1), and decreases release of chemokines such as CXCL1, thereby calming central sensitization and increasing pain tolerance.86,87 Systemically, EA affects the neuro-endocrine-immune system,88 helping to correct T-cell imbalances associated with CP/CPPS and other immune dysfunctions while promoting restoration of immune homeostasis.83
In summary, WMA and EA act through two different pathways that complement each other in producing their effects—“thermodynamic-microcirculatory” and “electrophysiological-neuromodulatory”—that precisely target the core pathological mechanisms of CP/CPPS. These mechanisms may partly explain the favorable clinical effects observed for WMA and EA in the present NMA.
Clinical Implications
This NMA provides comparative evidence that may help inform clinical decision-making and future guideline development in CP. Current guidelines provide only broad recommendations for acupuncture because past evidence is varied and there are few direct comparisons between different acupuncture methods.25,89 This study suggests that WMA and EA may represent useful acupuncture-related therapies for patients with insufficient response to conventional medications. Besides, combining acupuncture with standard medications may provide additional benefits. While medications primarily target local organ structures, previous studies suggest that WMA and EA may also influence neuroimmune regulation and central sensitization pathways.85 However, because most included studies were based on active-controlled comparisons and the overall certainty of evidence was predominantly low to moderate, these findings should not yet be interpreted as definitive evidence of superiority over other therapeutic approaches. This multimodal approach may support the use of acupuncture as a complementary strategy in CP management.
Strengths and Limitations
To our knowledge, this is the first network meta-analysis based on a relatively large evidence base (45 RCTs) to distinguish WMA, EA, and MA as separate intervention nodes while also treating combination regimens as independent comparators within the network. By revisiting the methodological limitations in Qin et al,81 this study further clarified the so-called “thumb-tack needle paradox” and highlighted the importance of defining intervention nodes according to stimulation type rather than needle form alone. These design features improve the interpretability and clinical relevance of the present findings.
Several limitations should also be considered. Clinical heterogeneity remained substantial across studies, including differences in acupoint selection, treatment frequency, treatment duration, and co-interventions.90 The methodological quality of many RCTs was also limited, particularly regarding blinding, allocation concealment, and incomplete reporting of intention-to-treat analyses.91,92 In addition, most studies compared acupuncture-related therapies with active medications rather than sham controls, making it difficult to fully distinguish specific treatment effects from contextual or nonspecific effects. Most included studies were conducted in China, which may limit generalizability and increase the risk of location-related publication bias or selective reporting of positive findings.93 Response rate outcomes should also be interpreted cautiously because definitions of clinical response varied across studies. Some network comparisons relied mainly on indirect evidence or a limited number of small studies, reducing the precision of certain treatment contrasts. Furthermore, because no additional subgroup analyses, meta-regression analyses, or sensitivity analyses were performed, the influence of specific clinical or methodological factors on treatment rankings could not be explored further. Therefore, although the overall findings support the potential value of acupuncture-related therapies, particularly WMA and EA, the rankings should still be interpreted with caution.
Future studies should prioritize rigorously designed head-to-head randomized trials comparing WMA and EA, with standardized diagnostic criteria, harmonized treatment protocols, and longer follow-up periods. Improved methodological transparency and broader geographic representation will also be important for strengthening the evidence base and improving the reliability of future treatment rankings.
Conclusions
This NMA suggests that WMA and EA may serve as useful complementary approaches for improving core CP symptoms in active-controlled trials. WMA showed the most favorable overall results, while EA demonstrated benefits in pain relief and quality of life. By re-evaluating the methodological limitations in Qin et al,81 the findings further suggest that the “thumb-tack needle paradox” may partly result from inappropriate node classification.25,82 These findings highlight the importance of clearly defining stimulation types in future NMAs. Nevertheless, the current findings should be interpreted with caution because most included studies were active-controlled trials with predominantly low-to-moderate certainty evidence and limited long-term follow-up. Further high-quality head-to-head and sham-controlled studies are needed.
Abbreviations
AAT, auricular acupoint therapy; CHM, Chinese herbal medicine; CI, confidence interval; CP, chronic prostatitis; EA, electroacupuncture; MA, manual acupuncture; MD, mean difference; MOX, moxibustion; NIH-CPSI, National Institutes of Health Chronic Prostatitis Symptom Index; NMA, network meta-analysis; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, randomized controlled trial; RR, risk ratio; SMS, heat-sensitive moxibustion; SUCRA, surface under the cumulative ranking curve; WM, Western medicine; WMA, warm needle acupuncture.
Data Sharing Statement
The data used in this systematic review and network meta-analysis were derived from published studies cited in the manuscript. Extracted study data and analysis materials are available from the corresponding author Rui Wang upon reasonable request.
Ethical Approval
Human Ethics and Consent to Participate declarations: not applicable.
Acknowledgments
The authors thank all the researchers and clinicians whose work contributed to this systematic review. We also thank the participants of the original trials included in this network meta-analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Zhejiang Traditional Chinese Medicine Science and Technology Program (Grant No. 2026ZL0112) and the Scientific Research Project of the 903rd Hospital (Grant No. Y202405). The funders had no role in the study design, literature search, data extraction, statistical analysis, interpretation of the results, manuscript preparation, or the decision to submit the manuscript for publication.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Rizzo M, Marchetti F, Travaglini F, et al. Prevalence, diagnosis and treatment of prostatitis in Italy: a prospective urology outpatient practice study. BJU Int. 2003;92(9):955–19. doi:10.1111/j.1464-410X.2003.04520.x
2. Liang CZ. Strengthening epidemiological research on chronic prostatitis in China. Zhonghua Miniao Waike Zazhi. 2006;27(8):509–511.
3. Krieger JN, Lee SW, Jeon J, et al. Epidemiology of prostatitis. Int J Antimicrob Agents. 2008;31(Suppl 1):S85–S90. doi:10.1016/j.ijantimicag.2007.08.028
4. Zhang MJ, Chang DG, Bin B, et al. Guidelines for integrated traditional Chinese and Western medicine diagnosis and treatment of chronic prostatitis. Zhongguo Nankexue Zazhi. 2023;37(1):3–17.
5. Barry MJ, Link CL, McNaughton-Collins MF, et al. Overlap of different urological symptom complexes in a racially and ethnically diverse, community-based population of men and women. BJU Int. 2008;101(1):45–51. doi:10.1111/j.1464-410X.2007.07191.x
6. Roberts RO, Jacobson DJ, Girman CJ, et al. Low agreement between previous physician diagnosed prostatitis and National Institutes of Health Chronic Prostatitis Symptom Index pain measures. J Urol. 2004;171(1):279–283. doi:10.1097/01.ju.0000100088.70887.29
7. Zhang J, Zhang X, Cai Z, et al. The lifetime risk and prognosis of chronic prostatitis/chronic pelvic pain syndrome in the middle-aged Chinese males. Am J Mens Health. 2019;13(4):1557988319865380. doi:10.1177/1557988319865380
8. Mo MQ, Long LL, Xie WL, et al. Sexual dysfunctions and psychological disorders associated with type IIIa chronic prostatitis: a clinical survey in China. Int Urol Nephrol. 2014;46(12):2255–2261. doi:10.1007/s11255-014-0810-2
9. Schoor RA. Prostatitis and male infertility: evidence and links. Curr Urol Rep. 2002;3(4):324–329. doi:10.1007/s11934-002-0058-8
10. Li HJ, Xu P, Liu JS, et al. Investigation on the incidence of chronic prostatitis in infertile men and its impact on fertility. Zhonghua Yixue Zazhi. 2004;84(5):21–23.
11. Björn R, Christian AB, Sascha A, et al. Assessing psychological factors, social aspects and psychiatric co-morbidity associated with chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) in men - a systematic review. J Psychosom Res. 2014;77(5):333–350. doi:10.1016/j.jpsychores.2014.09.012
12. Huang X, Qin Z, Cui H, et al. Psychological factors and pain catastrophizing in men with chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS): a meta-analysis. Transl Androl Urol. 2020;9(2):485–493. doi:10.21037/tau.2020.01.25
13. Zhang MJ, Chang DG, Bin B, et al. Expert consensus on integrated traditional Chinese and Western medicine diagnosis and treatment of chronic prostatitis. Zhongguo Nankexue Zazhi. 2023;37(1):3–17.
14. Mandar R, Korrovits P, Rahu K, et al. Dramatically deteriorated quality of life in men with prostatitis-like symptoms. Andrology. 2020;8(1):101–109. doi:10.1111/andr.12647
15. Shoskes DA, Nickel JC. Classification and treatment of men with chronic prostatitis/chronic pelvic pain syndrome using the UPOINT system. World J Urol. 2013;31(4):755–760. doi:10.1007/s00345-013-1075-6
16. Nickel JC, Shoskes DA, Wagenlehner FM. Management of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS): the studies, the evidence, and the impact. World J Urol. 2013;31(4):747–753. doi:10.1007/s00345-013-1062-y
17. Wei SZ, Xiong KL, Zhang WG, et al. Therapeutic effect of alpha-blocker combined with Cox-2 inhibitor on patients with type IIIb prostatitis. Di-san Junyi Daxue Xuebao. 2015;37(11):1166–1170.
18. Qin Z, Mo M, He CB, et al. Discussion on clinical advantage diseases of traditional Chinese medicine: chronic prostatitis. Zhongguo Shiyan Fangjixue Zazhi. 2024;30(24):152–158. doi:10.13422/j.cnki.syfjx.20242392
19. Chinese Society of Andrology. Chinese guidelines for the diagnosis and treatment of chronic prostatitis/chronic pelvic pain syndrome. Zhonghua Nankexue Zazhi. 2022;28(6):544–559.
20. Zhu H. Effect of Qian Yan Qing Formula on TCM syndrome and specific inflammatory cytokines in patients with chronic prostatitis. Xin Zhongyi. 2022;54(15):84–87.
21. Li ZH, Hu JW, Li X, et al. Research progress on the mechanism of acupuncture and moxibustion in treating chronic prostatitis. World J Acupunct Moxibust. 2021;31(4):309–313. doi:10.1016/j.wjam.2021.08.004
22. Gong QK, Huang XF, Chen Y, et al. Clinical evaluation of acupuncture for chronic prostatitis/chronic pelvic pain syndrome and research progress on its central nervous mechanism. Zhonghua Nankexue Zazhi. 2020;26(6):559–563.
23. Qin Z, Zang Z, Zhou K, et al. Acupuncture for chronic prostatitis/chronic pelvic pain syndrome: a randomized, sham acupuncture-controlled trial. J Urol. 2018;200(4):815–822. doi:10.1016/j.juro.2018.05.001
24. Zhou J, Liu Y, Li C, et al. Comparison of 3 assessment modes of acupuncture effect on patients with chronic prostatitis/chronic pelvic pain syndrome: a study protocol for a randomized controlled trial. Medicine. 2018;97(42):e12887. doi:10.1097/MD.0000000000012887
25. Pan J, Jin S, Xie Q, et al. Acupuncture for chronic prostatitis or chronic pelvic pain syndrome: an updated systematic review and meta-analysis. Pain Res Manag. 2023;2023:7754876. PMID: 36960418; PMCID: PMC10030225. doi:10.1155/2023/7754876
26. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
27. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/M14-2385
28. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l48–98. doi:10.1136/bmj.l4898
29. Turner RM, Davey J, Clarke MJ, Thompson SG, Higgins JP. Predicting the extent of heterogeneity in meta-analysis, using empirical data from the Cochrane Database of Systematic Reviews. Int J Epidemiol. 2012;41(3):818–827. doi:10.1093/ije/dys041
30. Chawla N, Anothaisintawee T, Charoenrungrueangchai K, et al. Drug treatment for panic disorder with or without agoraphobia: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2022;376:e066–084. doi:10.1136/bmj-2021-066084
31. da Costa BR, Juni P. Systematic reviews and meta-analyses of randomized trials: principles and pitfalls. Eur Heart J. 2014;35(47):3336–3345. doi:10.1093/eurheartj/ehu424
32. Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. 2011;64(2):163–171. doi:10.1016/j.jclinepi.2010.03.016
33. Sui L, Zhang XX. Clinical observation of electroacupuncture at Baliao points for treating chronic pelvic pain syndrome. J Zhejiang Chin Medical Univ. 2017;41(8):707–710. doi:10.16466/j.issn1005-5509.2017.08.018
34. Ou YF, Xie ZG, Chen SY, et al. Observation on the therapeutic effect of electroacupuncture for type IIIA prostatitis. Shanghai J Acupuncture Moxibust. 2020;39(11):1380–1384. doi:10.13460/j.issn.1005-0957.2020.13.1055
35. Xia SY, Wang SL, Fang ST, et al. Clinical study on mind-regulating acupuncture for chronic prostatitis/chronic pelvic pain syndrome. J Clin Acupuncture Moxibust. 2020;36(03):11–15.
36. Xuan LH. Acupuncture at Conception Vessel acupoints for type IIIA prostatitis. Jilin J Tradit Chin Med. 2018;38(3):335–338. doi:10.13463/j.cnki.jlzyy.2018.03.025
37. Zhang J, Liu CD, Ding Y, et al. Observation on the therapeutic effect of electroacupuncture for chronic prostatitis and its impact on urethral sphincter electromyography. Chin Acupuncture Moxibust. 2010;30(1):13–17. doi:10.13703/j.0255-2930.2010.01.011
38. Cao W. Clinical Study on Point Electroacupuncture for Chronic Non-Bacterial Prostatitis. Anhui University of Chinese Medicine; 2022. doi:10.26922/d.cnki.ganzc.2022.000178
39. Song GP, Wang XM, Chen F, et al. Observation on the efficacy of electroacupuncture combined with medication for chronic non-bacterial prostatitis. Shanghai J Acupuncture Moxibust. 2021;40(9):1070–1074. doi:10.13460/j.issn.1005-0957.2021.09.1070
40. Liang QF. Clinical Observation on Electroacupuncture Combined with Tamsulosin in the Treatment of Chronic Prostatitis with Dampness-Heat and Blood Stasis Syndrome [Dissertation]. Guangzhou University of Chinese Medicine; 2020. DOI: 10.27044/d.cnki.ggzzu.2020.000577.
41. Zhou SN, Chen BH, Wang GP. Observation on the efficacy of sacral four-needle electroacupuncture combined with Wenglitong Capsules for chronic prostatitis/chronic pelvic pain syndrome with dampness-heat and blood stasis syndrome. Shanghai J Acupuncture Moxibust. 2025;44(4):464–470. doi:10.13460/j.issn.1005-0957.2025.04.0464
42. Zhou P, Wang Y, Wang Y, et al. Clinical study on Chinese herbal medicine acupoint application for 40 cases of chronic prostatitis with dampness-heat and blood stasis syndrome. Jiangsu J Tradit Chin Med. 2016;48(9):58–60.
43. Yong SS. Clinical Efficacy Evaluation of Electroacupuncture Combined with Qianmitong Tablets for Chronic Prostatitis/Chronic Pelvic Pain Syndrome with Qi Stagnation and Blood Stasis Syndrome [Dissertation]. Chengdu University of Traditional Chinese Medicine; 2021. DOI: 10.26988/d.cnki.gcdzu.2021.000001.
44. Yang MY, Ying J, Li JX, et al. Clinical observation on electroacupuncture at Baihuanshu (BL30) and Huiyang (BL35) for chronic prostatitis. Shanghai J Acupuncture Moxibust. 2014;33(10):913–915. doi:10.13460/j.issn.1005-0957.2014.10.0913
45. Qiao LL. Observation on the Clinical Efficacy of Electroacupuncture Combined with Compound Niuling Granules in Treating Chronic Prostatitis [Master’s thesis]. Anhui University of Chinese Medicine; 2016.
46. Chen ZL, Wang GW, Yang RY. Electroacupuncture combined with Chinese herbal medicine for chronic non-bacterial prostatitis. J Clin Acupuncture Moxibust. 2011;27(8):35–36.
47. Zhu W, He QH, Wang SQ, et al. Clinical observation on acupuncture-medication combination for chronic non-bacterial prostatitis. J Traditional Chinese Med Pharm. 2011;17(5):70–72. doi:10.13862/j.cnki.cn43-1446/r.2011.05.029
48. Zeng L, Tan SH, Fang Y, et al. Moxibustion combined with tamsulosin sustained-release capsules for chronic prostatitis: a summary of 15 cases. Hunan J Tradit Chin Med. 2021;37(11):76–78. doi:10.16808/j.cnki.issn1003-7705.2021.11.024
49. Wang WC, Ma WJ, Hu R, et al. Efficacy observation of heat-sensitive moxibustion at acupoints for 30 cases of type IIIB prostatitis. J New Chin Med. 2007;(4):50–51. doi:10.13457/j.cnki.jncm.2007.04.027
50. Liu HS, Reheman A, Fu Y, et al. Efficacy observation of suspended moxibustion at heat-sensitive acupoints combined with medication for chronic prostatitis. Chin Acupuncture Moxibust. 2009;29(7):543–546. doi:10.13703/j.0255-2930.2009.07.011
51. Liu HS, Xu HB, Kang MF, et al. Multicenter clinical study on heat-sensitive moxibustion combined with Chinese herbal enema for chronic prostatitis. Jiangxi J Tradit Chin Med. 2011;42(1):56–58.
52. Kang MF, Zhang HF, Fu Y, et al. Clinical efficacy evaluation of different moxibustion dosage regimens using heat-sensitive moxibustion for chronic prostatitis. Lishizhen Med Materia Medica Res. 2015;26(1):125–127.
53. Shang YJ, Cui XM. Clinical observation on warm needle acupuncture at Guanyuan (CV4) and Zhongji (CV3) for chronic non-bacterial prostatitis. Heilongjiang J Tradit Chin Med. 2008;(2):39–40.
54. Chen ZX. Therapeutic effect of warm needle acupuncture as the main treatment for chronic non-bacterial prostatitis. World J Acupuncture-Moxibust. 2009;19(3):19–24.
55. Ma GZ, Chen L, Feng XX, et al. Observation on the therapeutic effect of warm needle acupuncture for chronic prostatitis with kidney yang deficiency pattern. Shanghai J Acupuncture Moxibust. 2016;35(7):820–822. doi:10.13460/j.issn.1005-0957.2016.07.0820
56. Cai GZ (Kuo-Chen Tsai). Clinical Study on Warm Needle Acupuncture for Chronic Prostatitis with Kidney Yang Deficiency Pattern [Dissertation]. Guangzhou University of Chinese Medicine; 2020. DOI: 10.27044/d.cnki.ggzzu.2020.000732.
57. Gao XY, Li JY. Observation on the efficacy of Lishen Zhuyu Decoction combined with warm needle acupuncture for chronic non-bacterial prostatitis. J Traditional Chinese Med Pharm. 2016;22(2):91–93. doi:10.13862/j.cnki.cn43-1446/r.2016.02.036
58. Wang K, Yang LL. Warm needle acupuncture combined with Western medicine for chronic non-bacterial prostatitis with kidney yang deficiency: a clinical study. J Clin Acupuncture Moxibust. 2017;33(7):35–37.
59. Song XL, Zhao JP, Xu SQ. Efficacy observation of warm needle acupuncture at Guanyuan (CV4) combined with Qianliexin Capsules for chronic non-bacterial prostatitis. Chin J Human Sexuality. 2018;27(3):92–95.
60. Li YC, Cui WF. Effects of warm needle acupuncture combined with Jisheng Shenqi pills on chronic non-bacterial prostatitis with kidney yang deficiency. Tradit Chin Med Res. 2024;37(12):62–66.
61. Zhou P, Wang Y, Wang Y, et al. Clinical study on acupoint application of chinese herbal medicine for chronic prostatitis with dampness-heat stasis syndrome: an analysis of 40 cases. Jiangsu J Tradit Chin Med. 2016;48(9):58–60.
62. Zhang R. Magnetic acupoint application therapy combined with tamsulosin hydrochloride sustained-release tablets for chronic prostatitis: 90 cases analysis. Shandong J Tradit Chin Med. 2017;36(10):853–855. doi:10.16295/j.cnki.0257-358x.2017.10.009
63. Yin Z. Clinical Observation of Zishen Quyu Decoction Combined with Acupoint Application in Treating Chronic Non-Bacterial Prostatitis (Dampness-Heat Stasis with Kidney Deficiency Syndrome). Heilongjiang University of Chinese Medicine; 2019. doi:10.27127/d.cnki.ghlzu.2019.000448
64. Zhang L. A Randomized Double-Blind Controlled Clinical Trial on the Additive Therapeutic Effect of Acupoint Application Therapy for Chronic Prostatitis/Chronic Pelvic Pain Syndrome with Dampness-Heat Stasis Syndrome. Chengdu University of Traditional Chinese Medicine; 2021. doi:10.26988/d.cnki.gcdzu.2021.000681
65. Sun C. Clinical Observation on Acupuncture-Medication Combination for Chronicnon-Bacterial Prostatitis. Nanjing University of Chinese Medicine; 2006.
66. Jiao GL. Clinical Observation on Prostatitis No. 1 Formula Combined with Acupuncture for Type III Prostatitis (Dampness-Heat Stasis Syndrome). Nanjing University of Chinese Medicine; 2016.
67. Gu Y. Thumb-Tack Needle Therapy Combined with Qianlie Shutong Capsules for Type III Prostatitis: A Clinical Study. Beijing University of Chinese Medicine; 2024. doi:10.26973/d.cnki.gbjzu.2024.000654
68. Pai N, Wang Z, Li J, et al. Clinical study on acupuncture combined with aromatherapy for chronic prostatitis. J External Ther Tradit Chin Med. 2023;32(1):38–40.
69. Yin J, Sun JG, Zhang PH, et al. Observation on the efficacy of acupuncture combined with extracorporeal microwave thermotherapy for chronic prostatitis/chronic pelvic pain syndrome. J Sichuan Tradit Chin Med. 2017;35(1):204–206.
70. Liu Z. Clinical Observation on Warm Needle Acupuncture Combined with Acupoint Application Therapy for Chronic Prostatitis with Kidney Yang Deficiency. Shandong University of Traditional Chinese Medicine; 2023. doi:10.27282/d.cnki.gsdzu.2023.000174
71. Zhang L. Clinical Observation on Acupuncture for Chronic Non-Bacterial Prostatitis. Nanjing University of Chinese Medicine; 2009.
72. Xiumei XU, Yanlong XU. Matrix acupuncture combined with needling at Sanyin points for chronic non-bacterial prostatitis: 31 cases report. Western J Tradit Chin Med. 2013;26(12):57–59.
73. Li Q, Wang LL. Circular acupuncture technique for chronic prostatitis. Xinjiang J Tradit Chin Med. 2015;33(4):36–38.
74. Gao F, Cong XL. Efficacy observation of acupuncture and moxibustion for chronic prostatitis. Shaanxi J Tradit Chin Med. 2016;37(6):726–727.
75. Huo J. Acupuncture for Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Clinical Study. Guangzhou University of Chinese Medicine; 2020. doi:10.27044/d.cnki.ggzzu.2020.000530
76. Wang M. “Golden Hook Fishing” Needle Technique for Type IIIB Prostatitis: A Controlled Clinical Trial. Gansu University of Chinese Medicine; 2021. doi:10.27026/d.cnki.ggszc.2021.000155
77. Hou J, Zhu Q, Lei JJ, et al. Efficacy observation of acupuncture-based clinical therapy for chronic prostatitis. Contemp Med. 2021;27(23):61–63.
78. Fang W, Wang S, Dong JK, et al. Evaluation of clinical effect of acupuncture on chronic prostatitis: meta analysis. Am J Mens Health. 2025;19(1):15579883241290035. doi:10.1177/15579883241290035
79. Wang Z, Wu J, Deng C, et al. Efficacy and brain modulation mechanisms of acupuncture for chronic prostatitis/chronic pelvic pain syndrome revealed by structural MRI changes. Front Neurol. 2025;16:1579484. doi:10.3389/fneur.2025.1579484
80. Qin Z, Guo J, Chen H, Wu J. Acupuncture for chronic prostatitis/chronic pelvic pain syndrome: a GRADE-assessed systematic review and meta-analysis. Eur Urol Open Sci. 2022;46:55–67. doi:10.1016/j.euros.2022.10.005
81. Qin P, Cao X, Ni H, et al. Efficacy of different acupuncture therapies for chronic prostatitis/chronic pelvic pain syndrome: a network meta-analysis. J Pain Res. 2025;18:3653–3673. doi:10.2147/JPR.S530646
82. Wu XL, Cheng K, Xu C, et al. Effect of electroacupuncture on cyclic adenosine monophosphate-protein kinase A-vanillic acid receptor subtype 1 of the transient receptor potential/PLK-protein kinase C-vanillic acid receptor subtype 1 of the transient receptor potential pathway based on RNA-seq analysis in prostate tissue in rats with chronic prostatitis/chronic pelvic pain syndrome. Front Neurosci. 2022;16:938200. PMID: 36090261; PMCID: PMC9449126. doi:10.3389/fnins.2022.938200
83. Wu X, Cheng K, Xu C, et al. Mechanism of acupuncture and moxibustion on chronic prostatitis/chronic pelvic pain syndrome: a narrative review of animal studies. Pain Res Manag. 2021;2021:2678242. doi:10.1155/2021/2678242
84. Kim HY, Wang J, Lee I, Kim HK, Chung K, Chung JM. Electroacupuncture suppresses capsaicin-induced secondary hyperalgesia through an endogenous spinal opioid mechanism. Pain. 2009;145(3):332–340. doi:10.1016/j.pain.2009.06.035
85. Yu Y, Peng X. Acupuncture for chronic prostatitis/chronic pelvic pain syndrome: a narrative review of therapeutic techniques and mechanisms. J Clin Question. 2025;2(5):e87. doi:10.69854/jcq.2025.0027
86. Zhang C, Li D. Effects of electroacupuncture on alleviating prostatodynia and inflammation in rats with chronic nonbacterial prostatitis. J Pain Res. 2021;14:2757–2765. PMID: 34522134; PMCID: PMC8434923. doi:10.2147/JPR.S321119
87. Su Y, Yang F, Xie JC, et al. Electroacupuncture neural stimulation mitigates bladder dysfunction and mechanical allodynia in cyclophosphamide induced cystitis through downregulation of the BDNF-TrkB signaling pathway. eNeuro. 2025;12(3):ENEURO.0329–24.2025. PMID: 40064496; PMCID: PMC11913400. doi:10.1523/ENEURO.0329-24.2025
88. Chang XU, Na LI, Xiaoling WU, et al. Effect of electroacupuncture on inflammatory signal expression in local tissues of rats with chronic pelvic pain syndrome based on purinergic 2X7 receptor/NOD-like receptor pyrin domain-containing 3 signal pathway. J Tradit Chin Med. 2022;42(6):965–971. PMID: 36378055; PMCID: PMC9924754. doi:10.19852/j.cnki.jtcm.20220928.003
89. Lai HH, Pontari MA, Argoff CE, et al. Male chronic pelvic pain: AUA guideline: part I evaluation and management approach. J Urol. 2025. doi:10.1097/JU.0000000000004564
90. Qin Z, Wu J, Zhou J, Liu Z. Systematic review of acupuncture for chronic prostatitis/chronic pelvic pain syndrome. Medicine. 2016;95(11):e3095. PMID: 26986148; PMCID: PMC4839929. doi:10.1097/MD.0000000000003095
91. Kim TH, Lee MS, Alraek T, Birch S. Acupuncture in sham device controlled trials may not be as effective as acupuncture in the real world: a preliminary network meta-analysis of studies of acupuncture for hot flashes in menopausal women. Acupunct Med. 2020;38(1):37–44. PMID: 31517500; PMCID: PMC7041625. doi:10.1136/acupmed-2018-011671
92. Kim Y, Park HI, Chu H, Jin H, Leem J. Effectiveness and safety of acupuncture modalities for overweight and obesity treatment: a systematic review and network meta-analysis of RCTs. Front Med. 2024;11:1446515. doi:10.3389/fmed.2024.1446515
93. Pratt M, Wieland S, Ahmadzai N, et al. A scoping review of network meta-analyses assessing the efficacy and safety of complementary and alternative medicine interventions. Syst Rev. 2020;9(1):97. PMID: 32354348; PMCID: PMC7191816. doi:10.1186/s13643-020-01328-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Effectiveness of Chinese Patent Medicines for Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Bayesian Network Meta-Analysis
Lin S, Huang W, Liu R, Xu J, Li Y
Journal of Pain Research 2026, 19:560430
Published Date: 14 January 2026