Back to Journals » Journal of Pain Research » Volume 19
Comparative Effectiveness of Chinese Patent Medicines for Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Bayesian Network Meta-Analysis
Authors Lin S, Huang W, Liu R, Xu J, Li Y
Received 19 August 2025
Accepted for publication 23 December 2025
Published 14 January 2026 Volume 2026:19 560430
DOI https://doi.org/10.2147/JPR.S560430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor King Hei Stanley Lam
Shuai Lin,1,2,* Wenrui Huang,3,* Ruxin Liu,2 Juan Xu,2 Yanlin Li2
1Zhongshan Hospital of Traditional Chinese Medicine Affiliated to Guangzhou University of Traditional Chinese Medicine, Zhongshan, Guangdong, People’s Republic of China; 2Zhongshan Hospital of Traditional Chinese Medicine, Zhongshan, Guangdong, People’s Republic of China; 3Shenzhen Traditional Chinese Medicine Hospital, Shenzhen, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanlin Li, Email [email protected] Juan Xu, Email [email protected]
Objective: Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS) presents with persistent pelvic pain, urinary symptoms, and psychological burden, severely affecting patients’ quality of life. While antibiotics and α-blockers are commonly prescribed, their long-term efficacy is limited and adverse reactions are frequent. Chinese patent medicines (CPMs) have emerged as promising alternatives, yet the lack of head-to-head evidence among formulations hinders evidence-based clinical recommendations.
Methods: Eight databases—CNKI, WanFang, VIP, SinoMed, PubMed, Web of Science, Embase, and the Cochrane Library—were searched from inception to November 1, 2025. Randomized controlled trials enrolling adults with CP/CPPS treated with CPMs versus standard therapy (ST) were included. Bias was assessed with ROB 2, and evidence certainty with CINeMA. A Bayesian network meta-analysis was performed, and outcomes were summarized using forest plots, league tables, and SUCRA curves in RStudio.
Results: Seventy-six trials (n=8431) involving 12 CPMs were analyzed. All studies were conducted in China, and all CPMs outperformed ST in enhancing the total effective rate and reducing NIH-CPSI scores. Shuangshi Tonglin Capsules (SSTL) ranked highest for both overall efficacy (OR = 5.6; 95% CI [2.0, 17]; SUCRA 73.8%) and NIH-CPSI reduction (MD = − 8.0; 95% CI [− 11, − 4.8]; SUCRA 93.3%). SSTL also provided the largest improvements in pain (MD = − 5.4; 95% CI [− 8.0, − 2.8]) and quality of life (MD = − 4.3; 95% CI [− 5.7, − 2.9]).
Conclusion: Compared with ST, CPMs significantly improved CP/CPPS symptoms, with SSTL showing the greatest overall benefit. However, since all included studies originated from China, the generalizability of these findings to other populations may be limited.
Keywords: chronic prostatitis, chronic pelvic pain syndrome, Chinese patent medicines, network meta-analysis
Introduction
Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS) is a multifactorial disorder defined by pelvic pain persisting beyond three months. Symptoms frequently include discomfort in the prostate, perineum, penile root, testicles, lower abdomen, and sacral region, often accompanied by urinary disturbances such as urgency, frequency, and dysuria.1,2 The condition is further complicated by sexual dysfunction and psychological disturbances, including anxiety, depression, and sleep disorders, which together exert a profound impact on patients’ health and quality of life.3,4 Prevalence estimates range from 8.4% to 25% internationally and 6.0% to 32.9% in China.5,6
Although the exact etiology of CP/CPPS is unknown, multiple mechanisms—including infection, immune response, neuromuscular abnormalities, psychological stress, and lifestyle factors—are believed to contribute. The interplay of these factors complicates diagnosis and underscores the need for multifaceted management. Current treatments encompass antibiotics, α-blockers, anti-inflammatory drugs, 5α-reductase inhibitors, physical therapy, and herbal medicine. In this review, “standard therapy (ST)” refers to conventional Western medical regimens commonly used in CP/CPPS, typically including an α-blocker (eg, tamsulosin) with or without a short course of antibiotics (when infection is suspected) and/or non-steroidal anti-inflammatory drugs, consistent with contemporary guideline-based care. However, most offer only limited long-term benefit and carry potential adverse effects. Antibiotics may foster resistance and alter gut microbiota; α-blockers and anti-inflammatories can induce hypotension and gastrointestinal reactions; 5α-reductase inhibitors are associated with sexual dysfunction; physical therapy requires sustained commitment; and the efficacy and safety of herbal therapies remain uncertain.7 These challenges emphasize the urgency of individualized and sustainable treatment plans.
Produced with standardized manufacturing and rigorous quality control, Chinese patent medicines (CPMs) are regarded as safe therapeutic agents supported by both extensive clinical experience and growing scientific validation. Their ease of use, sustained pharmacological effect, and cost-effectiveness make them well-suited for CP/CPPS treatment, earning recommendations in multiple clinical guidelines.8 Evidence from randomized trials indicates that CPMs substantially reduce NIH-CPSI scores, relieving pain and urinary symptoms while improving quality of life.9–12 Recent mechanistic studies further suggest that CPMs may mitigate prostatic inflammation and oxidative stress via specific signaling pathways. For example, Ningmitai capsules attenuate inflammatory responses through the CCL2–MAPK axis and reduce oxidative stress in experimental prostatitis models; Shuangshi Tonglin capsules modulate SIRT1/AMPK and MAPK signaling, inhibiting oxidative stress and inflammation in CP/CPPS models; and Qianlie Jiedu–related investigations implicate IL-6/STAT3 and Th17-cell pathways. Additional component-level data (eg, dioscin, calycosin) show suppression of TLR4/NF-κB or p38MAPK/NF-κB signaling in prostatitis models, providing biological plausibility for CPM effects.13–16 Combination therapy integrating CPMs with Western medicine demonstrates superior efficacy and safety over Western medicine alone. Mechanistic studies suggest that CPMs may exert therapeutic effects by modulating signaling pathways, suppressing inflammation and oxidative stress, and regulating apoptosis in prostate tissue.17
Substantial clinical data support the safety and therapeutic potential of CPMs in CP/CPPS management. However, most trials have compared individual CPMs only with standard therapy, leaving their relative efficacy uncertain. Considering the diverse compositions and mechanisms of different CPMs, a comparative evaluation is clinically necessary to inform treatment choice. A Bayesian network meta-analysis was therefore employed to integrate direct and indirect evidence, allowing simultaneous comparison and ranking of multiple CPMs, which cannot be achieved through traditional pairwise meta-analysis. This study aims to provide robust comparative evidence to guide clinical decision-making. Notably, all included randomized controlled trials (RCTs) were conducted in China, where CPMs are widely used and regulated; thus, differences in drug availability and healthcare settings elsewhere may limit generalizability.
Methods
The study design complied with the PRISMA 2020 statement and PRISMA-NMA extension for network meta-analyses.18 The protocol was preregistered in PROSPERO (CRD42024574970), with full details presented in Appendix 1.
Search Strategy
A systematic search was conducted in CNKI, WanFang, VIP, SinoMed, PubMed, Web of Science, Embase, and the Cochrane Library to identify RCTs on CPMs for CP/CPPS from database inception to November 1, 2025, with no language or publication-type restrictions applied. Reference lists of included studies and relevant systematic reviews were also screened to capture additional eligible records. Study screening was performed independently by two reviewers, and any discrepancies were resolved in consultation with a third reviewer. Full search strategies are provided in Appendix 2.
Eligibility Criteria
RCTs evaluating CP/CPPS were eligible, irrespective of participants’ age or disease duration. The diagnosis of CP/CPPS was required to be based on the National Institutes of Health (NIH) classification or equivalent clinical criteria, characterized by pelvic pain persisting for at least 3 months and exclusion of bacterial infection.
Eligible interventions included CPMs administered alone or as adjuncts to standard Western therapy, with treatment durations of at least 1 week. No restrictions were placed on dosage, formulation, or administration route. Comparators consisted of ST such as antibiotics, α-blockers, and non-steroidal anti-inflammatory drugs, consistent with established CP/CPPS management protocols.
Studies were required to report at least one of the primary or secondary outcomes (eg, total effective rate, NIH-CPSI score, pain, urinary, or quality-of-life domains) measured at the end of treatment or at the last follow-up point. The “Total Effective Rate” refers to the proportion of patients who achieve predefined clinical improvement categories (eg, cured, markedly effective, or effective). Although not an internationally standardized or patient-reported endpoint, TER is widely used in Chinese clinical trials as a pragmatic composite measure of overall therapeutic benefit. Only peer-reviewed RCTs published in English or Chinese were included; conference abstracts, duplicate publications, crossover trials, and studies lacking accessible outcome data were excluded.
Screening Process
All retrieved records were imported into EndNote for duplicate removal. Two reviewers (Reviewer A and Reviewer B) independently screened all titles and abstracts according to predefined eligibility criteria, documenting inclusion decisions and specific reasons for exclusion. Full-text articles meeting initial criteria were then reviewed independently and in duplicate to confirm eligibility. Any discrepancies between reviewers were first discussed to reach a consensus; if disagreement persisted, a third senior reviewer (Reviewer C) was consulted to make the final decision.
Data Extraction
A structured extraction form was developed to collect: (i) study characteristics (author, publication year, country, and design); (ii) participant demographics (sample size, age, sex, and diagnostic criteria); (iii) intervention and control details (treatment protocol, dosage, and duration); (iv) outcomes, including primary measures (overall efficacy and NIH-CPSI total score) and secondary measures (pain and urinary symptom scores, quality-of-life score, expressed prostatic secretion [EPS] white blood cell count, and adverse events); (v) follow-up data; and (vi) methodological quality indicators (randomization, allocation concealment, blinding, and data integrity). Data extraction was conducted independently and in duplicate by two reviewers using the predefined form. Extracted data were then cross-checked for consistency, and any discrepancies were discussed and resolved by consensus or, when necessary, adjudicated by a third reviewer.
Quality Assessment of Evidence
We evaluated methodological quality using the Cochrane RoB 2 tool,19 focusing on five domains: randomization and allocation concealment, fidelity to intended interventions, management of missing data, reliability of outcome measurement, and completeness of outcome reporting. Trials fulfilling criteria across these domains were rated as low risk of bias. Two reviewers independently assessed each study, with disagreements resolved through consensus. The overall certainty of evidence in the network meta-analysis was assessed with the CINeMA framework,20 which systematically examines within-study bias, reporting bias, indirectness, imprecision, heterogeneity, and inconsistency to determine evidence confidence levels.
Methods for Evidence Synthesis
Evidence synthesis was conducted through a Bayesian network meta-analysis implemented in R (gemtc, rjags). An evidence network was constructed, with nodes representing interventions, scaled to sample size, and edges weighted by standard errors. Consistency between direct and indirect estimates was evaluated using inconsistency models and the node-splitting technique.
Bayesian estimation was performed via Markov Chain Monte Carlo (MCMC) to obtain Odds Ratios (ORs) or Mean Differences (MDs), which were summarized in league tables. Between-study heterogeneity was quantified using the I2 statistic and P-values; fixed-effect models were used when P≥0.1 and I2≤50%, whereas random-effects models or narrative synthesis were applied when P<0.1 and I2>50%. Treatment rankings were derived from surface under the cumulative ranking curve (SUCRA) values, with higher SUCRA indicating greater effectiveness.
Results
Literature Selection and Study Characteristics
From the 6825 retrieved records, 236 articles underwent full-text review, and 76 RCTs including 8431 adults met eligibility criteria (Figure 1). All trials were conducted in China, with sample sizes ranging from 30 to 138 and intervention periods lasting 2–12 weeks. The mean age of participants was 40.0 years (SD = 6.32), and the mean disease duration was 5.98 years (SD = 1.56). 12 CPMs were investigated as adjuncts to standard treatment, resulting in 13 network interventions: Qianlie Shutong (QLST), Ningmitai (NMT), Qianlie Antong (QLAT), Sanjin (SJ), Qianlie Jiedu (QLJD), Qianlie Beixi (QLBX), Relinqing (RLQ), Qianlie Tongyu (QLTY), Qianlieping (QLP), Qianlie Anshuan (QLAS), and Shuangshi Tonglin (SSTL). Detailed characteristics of the trials and CPM formulations are summarized in Appendix 3.
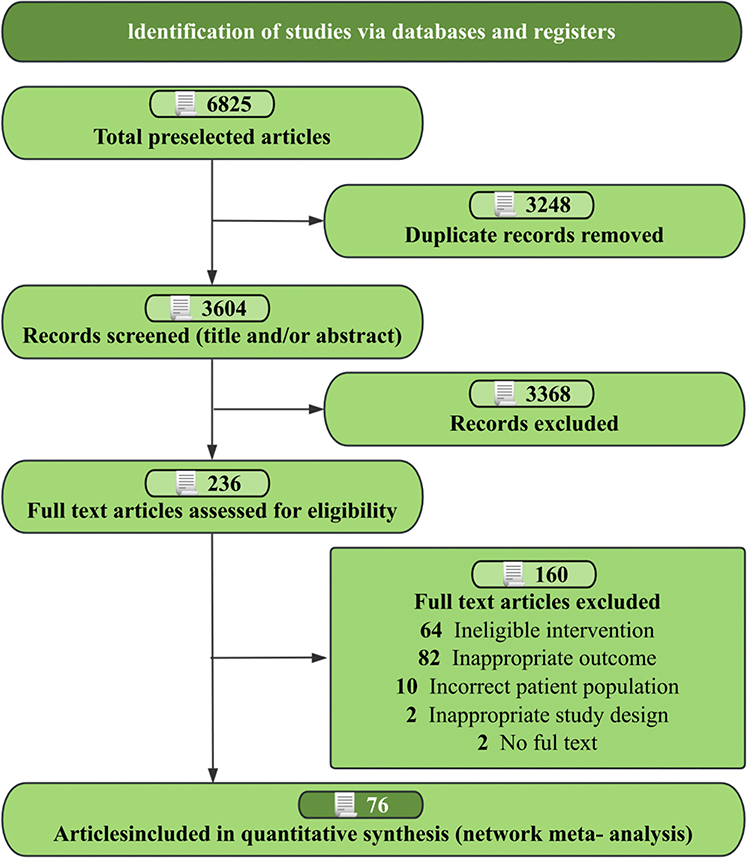 |
Figure 1 Flow diagram of preferred reporting items identified, included, and excluded for systematic reviews and meta-analyses (PRISMA). |
Risk of Bias, Certainty of Evidence, and Consistency
Appendix 4 summarizes the risk-of-bias evaluation. The main methodological concern was insufficient reporting of blinding procedures and loss-to-follow-up data. Of the 76 trials, 69 (90.7%) were judged low risk for randomization, 65 (85.5%) for deviations from intended interventions, 70 (92.1%) for missing data, 74 (97.3%) for outcome measurement, and 70 (92.1%) for selective reporting. Nine trials (11.8%) were classified as high risk, and 4 (5.2%) were rated as having some concerns.
Network consistency was high, as indicated by concordance between direct and indirect estimates (Appendix 6 and 7), and I2 statistics confirmed low heterogeneity (Appendix 5). All networks satisfied transitivity, ensuring valid indirect comparisons (Appendix 8, Figure S1 and Table S1). CINeMA analysis showed most pairwise comparisons had low confidence, with a minority reaching moderate or high levels (Appendix 8, Figure S2 and Table S2). Funnel plots demonstrated no evidence of small-study effects (Appendix 9). Together, these results confirm the methodological soundness and credibility of the synthesized evidence.
Total Effective Rate
The analysis of total effective rate included 73 RCTs with 8032 participants. Compared with ST, all CPMs yielded significant improvements (Figures 2 and 3). SSTL achieved the highest effect size (OR = 5.6; 95% CI [2.0, 17]; SUCRA 73.8%), followed by QLBX (OR = 5.4; 95% CI [2.8, 11]; SUCRA 74.7%) and QLST (OR = 4.8; 95% CI [3.7, 6.1]; SUCRA 74.1%) (Appendix 11 and Table S3). Pairwise comparisons showed that QLST (OR = 2.21; 95% CI [1.08, 4.53]) and QLJD (OR = 2.24; 95% CI [1.00, 5.06]) were significantly more effective than WLT (Appendix 12 and Table S10). CINeMA assessment indicated predominantly moderate-to-high certainty for this endpoint (Appendix 8 and Table S2).
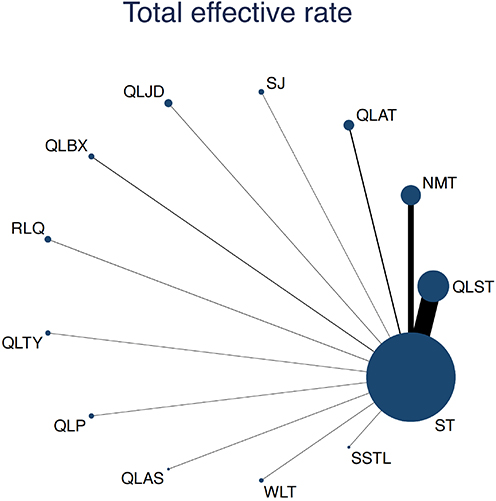 |
Figure 2 Network plot of available comparisons of CPMs for CP/CPPS. |
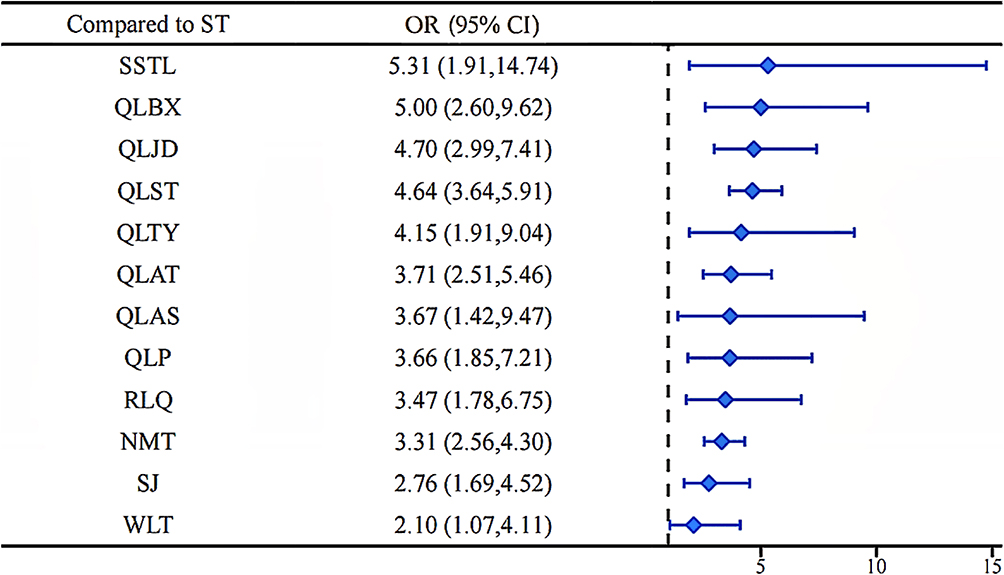 |
Figure 3 Forest plot of available comparisons of CPMs for CP/CPPS. Abbreviations: QLST, Qianlie Shutong Capsules; NMT, Ningmitai Capsules; QLAT, Qianlie Antong Tablets/Capsules; SJ, Sanjin Tablets; QLJD, Qianlie Jiedu Capsules; QLBX, Qianlie Beixi Capsules; RLQ, Relinqing Granules; QLTY, Qianlie Tongyu Capsules; QLP, Qianlieping Capsules; QLAS, Qianlie Anshuan Tablets; WLT, Wenglitong Capsules; SSTL, Shuangshi Tonglin Capsules; ST, Standard treatment. |
Pain Symptom Score
Pain symptom scores were analyzed across 47 RCTs involving 5137 participants. SSTL ranked highest for pain reduction (MD = −5.4; 95% CI [−8.0, −2.8]; SUCRA 95.3%). Compared with ST, all CPMs except QLBX, QLTY, and QLP produced significant improvements. Indirect network estimates confirmed SSTL’s superiority over NMT (MD = 3.37; 95% CI [0.64, 6.13]), QLAT (MD = 2.95; 95% CI [0.10, 5.82]), QLBX (MD = 4.14; 95% CI [0.94, 7.35]), and QLP (MD = 3.64; 95% CI [0.44, 6.84]) (Appendix 10 and Figure S3). Full SUCRA rankings and pairwise data are presented in Appendix 11 (Table S4) and Appendix 12 (Table S11).
Urination Disorder Score
Results of the Urination Disorder Score network meta-analysis are shown in Appendix 10 (Figure S4). Following consistency evaluation, several CPMs significantly outperformed ST: QLST (MD = −1.8; 95% CI [−2.3, −1.4]), NMT (MD = −1.2; 95% CI [−1.7, −0.68]), QLAT (MD = −1.1; 95% CI [−1.8,−0.33]), QLJD (MD = −1.3; 95% CI [−2.1, −0.46]), QLBX (MD = −2.3; 95% CI [−3.4, −1.1]), RLQ (MD = −2.3; 95% CI [−3.3, −1.4]; SUCRA 90.6%), and QLTY (MD = −1.8; 95% CI [−3.6, −0.04]). Additional rankings and indirect effect estimates are available in Appendix 11 (Table S5) and Appendix 12 (Table S12).
Quality of Life Score
Quality-of-life outcomes were analyzed across 41 RCTs comprising 4550 participants. All CPMs except QLAS significantly improved quality of life compared with ST. SSTL demonstrated the largest effect size (MD = −4.3; 95% CI [−5.7, −2.9]; SUCRA 99.6%) (Appendix 10 and Figure S5). Network estimates further confirmed SSTL’s advantage over nearly all CPMs, with QLTY being the only formulation without a significant difference. Full SUCRA rankings and indirect comparisons are available in Appendix 11 (Table S6) and Appendix 12 (Table S13).
NIH-CPSI Score
Analysis of NIH-CPSI scores included 58 RCTs with 6515 participants. Compared with ST, all CPMs except QLAS and WLT produced significant reductions. SSTL demonstrated the largest effect (MD = −8.0; 95% CI [−11, −4.8]; SUCRA 93.3%), followed by QLBX (MD = −6.2; 95% CI [−8.5, −3.9]; SUCRA 77.8%) and SJ (MD = −6.1; 95% CI [−8.8, −3.3]; SUCRA 73.4%) (Appendix 10 and Figure S6). Network comparisons confirmed SSTL’s superiority over QLJD, QLAS, and WLT. Notably, the observed mean reductions exceeded the minimally important difference (MID) of approximately 6 points established for the NIH-CPSI total score in prior validation studies,97,98 suggesting that these improvements are not only statistically significant but also clinically meaningful for patients. Complete SUCRA rankings and pairwise estimates are reported in Appendix 11 (Table S7) and Appendix 12 (Table S14).
EPS White Blood Cell Counts
Significant reductions in EPS white blood cell counts were observed for QLST (MD = −5.59; 95% CI [−7.65, −3.52]), NMT (MD = −5.67; 95% CI [−9.12, −2.22]), SJ (MD = −8.33; 95% CI [−14.88, −1.92]), QLJD (MD = −8.91; 95% CI [−13.54, −4.46]), and QLBX (MD = −6.34; 95% CI [−10.27, −2.40]) compared with ST (Appendix 10 and Figure S7). No statistically significant differences were identified among the remaining CPMs in indirect network comparisons. Detailed results are provided in Appendix 11 (Table S8) and Appendix 12 (Table S15).
Adverse Events
A total of 24 RCTs documented adverse events. The network meta-analysis revealed no significant differences across interventions in both direct and indirect estimates (Appendix 10 and Figure S8). Complete adverse event data are presented in Appendix 11 (Table S9) and Appendix 12 (Table S16).
Sensitivity Analyses and Meta-Regressions
To assess result stability, sensitivity analyses were performed by omitting one study at a time. No exclusions materially changed the pooled effects, and findings remained consistent with the primary analyses (Appendix 13). Meta-regression was used to evaluate potential baseline modifiers, including disease duration, follow-up length, and participant age. None demonstrated a statistically significant association with the primary outcomes (Appendix 14).
Discussion
Principal Findings
In this comprehensive network meta-analysis, we synthesized evidence from 76 RCTs including 8431 participants to assess the comparative efficacy and safety of 12 CPMs for CP/CPPS. Across all included formulations, significant improvements were observed in total effective rate and NIH-CPSI scores relative to ST. SSTL emerged as the top-ranked intervention, yielding the greatest benefits for total efficacy and NIH-CPSI reduction with high-certainty evidence. It also demonstrated the most substantial effects on pain alleviation and quality-of-life enhancement in adults with CP/CPPS.
Shuangshi Tonglin Capsules (SSTL)
Underpinned by TCM theory, CPMs are manufactured using standardized processes and are widely adopted in clinical practice due to their demonstrated efficacy and affordability. While previous meta-analyses have confirmed their benefit in improving CP/CPPS outcomes,11,99 head-to-head evidence comparing different formulations has been lacking. This study employs a network meta-analysis to address this limitation, identifying SSTL as the most effective intervention.
SSTL is traditionally prescribed to regulate qi and blood and to dispel damp-heat, aligning with the typical presentation of CP/CPPS.100 Pharmacodynamic studies indicate that SSTL exerts multi-component, multi-target, and multi-pathway effects. Its principal compounds—including quercetin, luteolin, tanshinone IIA, stigmasterol, and berberine—target inflammatory mediators such as PTGS2, HSP90AA1, IL-1B, and IL-6, and modulate IL-17, TNF, and PI3K-Akt signaling pathways, providing a mechanistic rationale for its clinical efficacy.101
Strengths and Limitations of This Study
This work represents the most comprehensive and up-to-date Bayesian network meta-analysis of CPMs for CP/CPPS and applies the CINeMA framework to ensure transparent and robust evidence grading. Nevertheless, several limitations should be acknowledged.
All included trials were conducted in China, where CPMs are most widely used, which may limit the generalizability of the findings to broader populations and introduce potential geographic and publication bias. Moreover, most studies did not incorporate syndrome differentiation, a cornerstone of traditional Chinese medicine, which may have influenced treatment response heterogeneity. The intervention durations varied from 2-12 weeks, restricting the ability to evaluate long-term efficacy or sustained benefits. Variations in sample size, baseline symptom severity, and background therapy (antibiotics, α-blockers, or NSAIDs) may also have contributed to clinical heterogeneity, despite the overall low statistical heterogeneity in the pooled results.
Because CPMs were administered either alone or in combination with different standard treatments, the transitivity assumption underlying indirect comparisons may not have been fully satisfied. Although consistency testing supported the validity of the network, the relative effects between certain interventions should still be interpreted with caution. Some CPMs were supported by only a few trials, reducing confidence in their relative rankings. Finally, methodological deficiencies persisted in several studies, including incomplete reporting of randomization, allocation concealment, blinding procedures, and loss-to-follow-up data, which could lead to performance and attrition bias, although attempts were made to obtain clarifying information from the study authors.
Conclusions
CPMs showed greater symptom improvement than standard therapy in patients with CP/CPPS. SSTL ranked among the more effective options; however, the certainty of evidence—assessed using the CINeMA framework—was generally low to moderate, given the small sample sizes, limited head-to-head comparisons, and short intervention durations. SUCRA rankings were interpreted descriptively, and results should be viewed with caution. Further large, high-quality, multicenter RCTs are needed to confirm these findings and strengthen confidence in the evidence base.
Funding
This work was supported by the University – Hospital Joint Fund Project of Guangzhou University of Chinese Medicine (No. GZYZS2024U19); Research Project of Guangdong Provincial Administration of Traditional Chinese Medicine (20251436); and National Key Specialty of Traditional Chinese Medicine Program (Nephrology Department, Zhongshan Hospital of Traditional Chinese Medicine).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Franco JVA, Turk T, Jung JH, et al. Pharmacological interventions for treating chronic prostatitis/chronic pelvic pain syndrome: a Cochrane systematic review. BJU Int. 2020;125(4):490–11. doi:10.1111/bju.14988
2. Nickel JC, Nyberg LM, Hennenfent M. Research guidelines for chronic prostatitis: consensus report from the first National Institutes of Health International Prostatitis Collaborative Network. Urology. 1999;54(2):229–233. doi:10.1016/S0090-4295(99)00205-8
3. Zhang JM, Bin B, Shang XJ, et al. Expert consensus on integrated traditional Chinese and Western medicine diagnosis and treatment of chronic prostatitis. Chin J Integr Tradit West Med. 2015;35(8):9.
4. Strauss AC, Dimitrakov JD. New treatments for chronic prostatitis/chronic pelvic pain syndrome. Nat Rev Urol. 2010;7(3):127–135. doi:10.1038/nrurol.2010.4
5. Zhang J, Liang C, Shang X, Li H. Chronic prostatitis/chronic pelvic pain syndrome: a disease or symptom? Current perspectives on diagnosis, treatment, and prognosis. Am J Mens Health. 2020;14(1):1557988320903200. doi:10.1177/1557988320903200
6. Mi H, Chen K, Mo ZN. Epidemiological characteristics of chronic prostatitis in China. Zhonghua Nan Ke Xue. 2012;18(7):4.
7. Chinese Urological Association, Chronic Prostatitis/Chronic Pelvic Pain Syndrome Diagnosis and Treatment Guidelines Writing Group, Shang XJ, et al. Guidelines for the diagnosis and treatment of chronic prostatitis/chronic pelvic pain syndrome. Zhonghua Nan Ke Xue. 2022;2022(006):028.
8. Li HS. Expert consensus on integrated traditional Chinese and Western medicine treatment of chronic prostatitis. Chin J Androl. 2021;35(04):55–58.
9. Dong YH, Sun BG, Cao JH, et al. Clinical efficacy of Ningmitai capsules on various phenotypes of chronic prostatitis/chronic pelvic pain syndrome based on the UPOINT(S) system. Chin J Androl. 2022.
10. Geng Q, Chen SF, Li Z, et al. Clinical observation of Huang E capsules in the treatment of chronic prostatitis/chronic pelvic pain syndrome with damp-heat and blood stasis syndrome. Chin J Androl. 2023;37(6):101–104.
11. Xu HS, Li HS, Li BZ, et al. Meta-analysis on the efficacy and safety of Relinqing granules in the treatment of chronic prostatitis with damp-heat downward flow syndrome. Chin J Androl. 2022;36(2):6.
12. Zhang CH, Wang YW, Sun PP, et al. Reevaluation of the clinical efficacy of Longjin Tonglin capsules in the treatment of chronic prostatitis based on a multicenter real-world study. Zhonghua Nan Ke Xue. 2022;28(9):831–836.
13. Liu H, Wang Z, Xie Q, et al. Ningmitai capsules have anti-inflammatory and pain-relieving effects in the chronic prostatitis/chronic pelvic pain syndrome mouse model through systemic immunity. Front Pharmacol. 2022;13:949316. doi:10.3389/fphar.2022.949316
14. Liu Q, Zhang X, Mao P, et al. Shuangshi Tonglin capsule improves chronic prostatitis through the SIRT-1/AMPK and MAPK signalling pathways. Heliyon. 2023;9(11):e21745. doi:10.1016/j.heliyon.2023.e21745
15. Jia Z, Lv D, Chen T, et al. Network pharmacology and in vivo experiment-based strategy for investigating the mechanism of chronic prostatitis/chronic pelvic pain syndrome in QianLieJinDan tablets. Heliyon. 2024;10(9):e29975. doi:10.1016/j.heliyon.2024.e29975
16. Long Y, Ge X, Ma L, Guo J, Zhu Y. Dioscin protects against chronic prostatitis through the TLR4/NF-κB pathway. Open Med. 2024;19(1):20241036. doi:10.1515/med-2024-1036
17. Hong ZM, Guo J, He ZP, et al. Study on the mechanism of Xia Li Qi capsules in treating chronic prostatitis based on network pharmacology. Chin J Androl. 2023;37(04):67–73+96.
18. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/M14-2385
19. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
20. Nikolakopoulou A, Higgins JPT, Papakonstantinou T, et al. CINeMA: an approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020;17(4):e1003082. doi:10.1371/journal.pmed.1003082
21. Wang YH, Fan YX, Li F, et al. Clinical study of Qianlie Shutong Capsules combined with Pursuitai Tablets in the treatment of chronic prostatitis. Mod Drugs Clin. 2023;38(11):2825–2830.
22. Zhang KZ, Wu YJ, Zhao XW, et al. Effects of Qianlie Shutong Capsules combined with Minocycline on erectile function and inflammatory factors in patients with chronic prostatitis. Med Forum J. 2023;44(17):97–100.
23. Qi WM, Xu YT, Lu XZ, et al. Evaluation of the effect of Qianlie Shutong Capsules combined with Tamsulosin Hydrochloride Sustained-Release Capsules in the treatment of prostatitis. Marriage Health. 2023;29(05):82–84.
24. Liu QL. Effect of Qianlie Shutong Capsules combined with Tamsulosin Hydrochloride Sustained-Release Capsules in the treatment of patients with chronic prostatitis. China Health Care Nutr. 2022;34(20):92–94+98.
25. Liu KX. Analysis of the effect of Qianlie Shutong Capsules combined with Tamsulosin Hydrochloride Sustained-Release Capsules in the treatment of prostatitis. Med Theory Pract. 2022;35(15):2603–2605. doi:10.19381/j.issn.1001-7585.2022.15.033
26. Zhang ZJ. Effect of Qianlie Shutong Capsules combined with Tamsulosin Capsules on postoperative patients after transurethral resection of the prostate and its impact on inflammatory factors. Chin J Integr Tradit West Med Surg. 2021;27(03):447–450.
27. Ba DRG, Bai SX, Wen YH. Evaluation of the efficacy of Qianlie Shutong Capsules combined with Fosfomycin Trometamol in the treatment of chronic bacterial prostatitis. Chin Prescr Drug. 2021;19(06):87–88.
28. Wang XP. Exploration of the efficacy of Tadalafil combined with Qianlie Shutong Capsules in the treatment of chronic prostatitis complicated with erectile dysfunction and premature ejaculation. Chin Foreign Med Res. 2021;40(17):81–83. doi:10.16662/j.cnki.1674-0742.2021.17.081
29. Wang YJ, Fan YT. Analysis of the efficacy of quinolone antibiotics combined with Qianlie Shutong Capsules in the treatment of chronic bacterial prostatitis. Prim Med Forum. 2021;25(14):1960–1962. doi:10.19435/j.1672-1721.2021.14.017
30. Lu QH, Chen YD. Efficacy of Qianlie Shutong combined with Tamsulosin in the treatment of chronic prostatitis. Shenzhen J Integr Tradit Chin West Med. 2020;30(23):174–176. doi:10.16458/j.cnki.1007-0893.2020.23.082
31. Liu X, Luo HL, Zhou DP, et al. Efficacy of Qianlie Shutong Capsules in the treatment of type III prostatitis of damp-heat and stasis type and its effect on IFN-γ and IL-10 in prostatic fluid. Chin Mod Dr. 2020;2020(36):74–76, 80.
32. Wang Q, Yang YT, Zeng XB. Exploration of the effect of Tamsulosin combined with Qianlie Shutong Capsules in the treatment of chronic prostatitis. North Pharm. 2020;17(08):111–112.
33. Zhang P, Zhao FL, Miao XY, et al. Therapeutic effect of Qianlie Shutong Capsules combined with quinolone antibiotics in the treatment of chronic bacterial prostatitis. North Pharm. 2019;16(07):73–74.
34. Su DJ, Liu Y. Clinical efficacy of Qianlie Shutong Capsules combined with quinolone antibiotics in the treatment of chronic bacterial prostatitis. Med Equip. 2019;32(05):59–61.
35. Jing ZM, Zhu HS, Xu HL, et al. Clinical study of Qianlie Shutong Capsules combined with Tamsulosin Capsules in the treatment of prostatitis of damp-heat and stasis type. Shaanxi J Tradit Chin Med. 2019;40(3):294–296. doi:10.3969/j.issn.1000-7369.2019.03.006
36. Zeng DS, He Y, Xiao YH, et al. Effect of Qianlie Shutong Capsules combined with Tamsulosin Capsules on inflammatory factors in chronic non-bacterial prostatitis and its clinical efficacy. Int J Urol. 2017;37(06):865–869. doi:10.3760/cma.j.issn.1673-4416.2017.06.020
37. Wu QR. Clinical value of Qianlie Shutong Capsules combined with Moxifloxacin in the treatment of chronic prostatitis. Clin Res. 2017;25(2):123–124. doi:10.3969/j.issn.1004-8650.2017.02.107
38. Cai JL. Clinical effect analysis of Qianlie Shutong Capsules combined with Levofloxacin in the treatment of prostatitis. Cap Food Med. 2017;24(12):99–100.
39. Yu M. Observation of the effect of Qianlie Shutong Capsules combined with Moxifloxacin in the treatment of chronic prostatitis. J Clin Rational Drug Use. 2016;9(20):57–58. doi:10.15887/j.cnki.13-1389/r.2016.20.038
40. Sang Q. Clinical efficacy of Qianlie Shutong Capsules combined with quinolone antibiotics in the treatment of chronic bacterial prostatitis. J Mudanjiang Med Coll. 2016;37(03):106–107.
41. Chang CY. Observation of the clinical effect of Qianlie Shutong combined with Levofloxacin in the treatment of type III prostatitis. J Clin Rational Drug Use. 2015;8(24):138–139.
42. Zhang MX. Clinical observation of Levofloxacin combined with Qianlie Shutong Capsules in the treatment of chronic prostatitis. China Natl Folk Med. 2015;24(13):47.
43. He B, Dai EL. Clinical observation of Qianlie Shutong Capsules combined with α-1A receptor blockers in the treatment of type III prostatitis of damp-heat and stasis type. Int J Urol. 2014;34(5):704–708. doi:10.3760/cma.j.issn.1673-4416.2014.05.023
44. Zhu HM, Jia L, Hu HL. Clinical observation of Qianlie Shutong Capsules combined with Moxifloxacin in the treatment of chronic prostatitis. Chin J Hospital Pharm. 2013;33(02):137–139.
45. Xiao L, Chen X, Feng XH. Clinical observation of Qianlie Shutong combined with Sparfloxacin in the treatment of type IIIA prostatitis. J Hunan Univ Tradit Chin Med. 2013;33(12):29–30.
46. Liu J. Clinical study of Levofloxacin combined with Qianlie Shutong Capsules in the treatment of chronic prostatitis. Hebei Med. 2012;18(03):378–379.
47. Wang JS. Clinical effect of Ningmitai Capsules combined with Levofloxacin in the treatment of chronic prostatitis in elderly patients. J Clin Rational Drug Use. 2022;15(35):116–118.
48. Lin L. Study on the clinical efficacy of Levofloxacin Capsules combined with Ningmitai Capsules in the treatment of prostatitis and its effect on serum factors. Harbin Med. 2022;42(05):120–121.
49. Liu HW, Tian HS, Liu JJ, et al. Observation of the efficacy of Ningmitai Capsules combined with Tamsulosin Sustained-Release Tablets in the treatment of type IIIB prostatitis. J Pract Chin Med. 2021;37(08):1322–1323.
50. Yi JS. Clinical efficacy of Tamsulosin Capsules combined with Ningmitai Capsules in the treatment of type III prostatitis. J Clin Rational Drug Use. 2021;14(18):142–144.
51. Han JC. Effect of Ningmitai Capsules combined with Pursuitai Tablets in the treatment of prostatitis. Clin Med. 2021;41(04):115–117. doi:10.19528/j.issn.1003-3548.2021.04.048
52. Zhou R, Zhu JS, Chen ZJ, et al. Clinical efficacy of Ningmitai Capsules combined with Levofloxacin in the treatment of bacterial prostatitis. Drug Eval Res. 2021;44(02):403–406.
53. Qian YH, Wang K. Clinical efficacy of Ningmitai Capsules in the treatment of chronic prostatitis. J Clin Rational Drug Use. 2020;13(36):97–99. doi:10.15887/j.cnki.13-1389/r.2020.36.040
54. Zhao SX, Li ZQ. Efficacy of Ningmitai Capsules combined with Moxifloxacin in the treatment of chronic prostatitis and its effect on serum inflammatory factors. Mod J Integr Tradit West Med. 2020;29(03):291–294.
55. Peng YP, Huang W, Xing YT, et al. Observation of the efficacy of Ningmitai Capsules combined with Levofloxacin in the treatment of chronic prostatitis. Chin J Integr Tradit West Med Surg. 2019;25(03):366–369.
56. Liu LH, Wang Y, Zhang Y, et al. Clinical efficacy of Ningmitai Capsules combined with Moxifloxacin in the treatment of patients with chronic prostatitis and its effect on serum TNF-α, IL-1β, and M-CSF. Mod Prog Biomed Sci. 2018;18(07):1318–1321. doi:10.13241/j.cnki.pmb.2018.07.025
57. Ma CJ. Observation of the efficacy of Ningmitai Capsules combined with Tamsulosin Sustained-Release Capsules in the treatment of chronic prostatitis. Med Theory Pract. 2017;30(18):2738–2739.
58. Mei XF, Xia YG, Tian Y, et al. Analysis of the efficacy of Ningmitai Capsules combined with Levofloxacin Tablets in the treatment of type III chronic prostatitis. New Chin Med. 2017;49(06):74–76.
59. Chen MS. Observation of the efficacy of antibiotics combined with Ningmitai Capsules in the treatment of chronic prostatitis. Electron J Clin Med Lit. 2016;3(35):7056–7057. doi:10.16281/j.cnki.jocml.2016.35.104
60. Su JX, Chen SQ, Xie ZX. Clinical efficacy analysis of Ningmitai Capsules combined with Levofloxacin Capsules in the treatment of chronic prostatitis. Clin Res Tradit Chin Med. 2016;8(23):107–108.
61. Zhou RC. Observation of the clinical efficacy of Ningmitai Capsules combined with Levofloxacin Capsules in the treatment of chronic prostatitis. Prim Med Forum. 2015;19(09):1161–1162.
62. Luo XJ, Yang NQ, Peng SL. Clinical effect of Meloxicam combined with Tamsulosin Sustained-Release Capsules and Qianlie Antong Tablets in the treatment of type III prostatitis. Contemp Med. 2018;24(10):112–113.
63. Li JK. Analysis of the effect of Tamsulosin combined with Qianlie Antong Tablets in the treatment of chronic prostatitis. China Med Guide. 2017;15(8):89–90.
64. Zhang YJ. Clinical observation of integrated traditional Chinese and Western medicine in the treatment of 58 cases of chronic non-bacterial prostatitis. World J Integr Tradit West Med. 2016;11(2):198–200203.
65. Li CH. Qianlie Antong Tablets combined with Tamsulosin and Levofloxacin in the treatment of 45 cases of chronic non-bacterial prostatitis. China Pharm. 2015;24(08):86–87.
66. Liu LH, Wang Y, Pu YC. Effect of Qianlie Antong Capsules on the treatment of chronic prostatitis and the immune function of patients. West Med. 2014;26(11):1490–1492.
67. Zhang ZD, Chen G. Observation of the efficacy of Qianlie Antong Tablets combined with Tamsulosin Sustained-Release Tablets in the treatment of type IIIB chronic prostatitis. Tradit Chin Med Herald. 2011;17(07):23–25.
68. Sun YY, Chen ZG. Clinical observation of Qianlie Antong Tablets combined with Terazosin Hydrochloride in the treatment of chronic non-bacterial prostatitis. Chin J Inf Tradit Chin Med. 2008;15(6):65–66.
69. Fan SQ, Li J. Observation of the efficacy of Tamsulosin Capsules combined with Sanjin Tablets in the treatment of chronic non-bacterial prostatitis. China Pract Med. 2015;10(03):160–161.
70. Jiang SG, Zhang XH. Clinical experience of Sanjin Tablets in the treatment of chronic prostatitis of damp-heat type. Eval Anal Drug Use Hosp China. 2009;9(09):702–703. doi:10.14009/j.issn.1672-2124.2009.09.001
71. Li MK, Li SQ, Cui QL. Observation of the efficacy of Sanjin Tablets combined with Levofloxacin and Tamsulosin in the treatment of chronic prostatitis. Eval Anal Drug Use Hosp China. 2009;9(12):930–931.
72. Wu XJ, Lou CM, Tian WJ, et al. Clinical study of Tamsulosin combined with Qianlie Jiedu Capsules in the treatment of chronic non-bacterial prostatitis. Zhejiang J Trauma Surg. 2017;22(01):131–132.
73. Qiao YH, Zuo SS, Li DS, et al. Observation of the efficacy of Qianlie Jiedu Capsules combined with Tamsulosin Sustained-Release Capsules and Levofloxacin in the treatment of chronic prostatitis. Inner Mong J Tradit Chin Med. 2013;32(22):34–35. doi:10.16040/j.cnki.cn15-1101.2013.22.171
74. Qiao YH. Clinical observation of Qianlie Jiedu Capsules combined with Levofloxacin in the treatment of type III chronic prostatitis. Hebei Med. 2012;34(20):3168–3169.
75. Ji DL, Han RX, Liu SM, et al. Clinical observation of Qianlie Jiedu Capsules combined with Levofloxacin in the treatment of type IIIA prostatitis. Hebei Med. 2010;32(08):944–945.
76. Xu JC, Lu QM, Fu LJ, et al. Randomized double-blind controlled clinical observation of Qianlie Jiedu Capsules combined with Lomefloxacin in the treatment of chronic prostatitis. Natl J Androl. 2010;16(02):183–186. doi:10.13263/j.cnki.nja.2010.02.020
77. Cao ZH, Liu L. Effect of Tamsulosin combined with Qianlie Beixi Capsules in the treatment of chronic prostatitis and its impact on NIH-CPSI scores and white blood cell count. Clin Med Res Pract. 2023;8(20):37–40. doi:10.19347/j.cnki.2096-1413.202320010
78. Wang HY, Nie WH, Qiu L, et al. Observation of the efficacy of Tamsulosin combined with Qianlie Beixi Capsules in the treatment of prostatitis. Mod Drugs Clin. 2018;33(07):1775–1778.
79. Luo CH. Effect of Tamsulosin Sustained-Release Tablets combined with Qianlie Beixi Capsules in the treatment of prostatitis and observation of NIH-CPSI scores, white blood cells, and lecithin bodies. North Pharm. 2022;19(10):131–133.
80. Liu SM, Huang CT, Jia YS, et al. Clinical observation of Qianlie Beixi Capsules combined with Doxazosin Mesylate Sustained-Release Tablets in the treatment of 30 cases of type III prostatitis. Chin J Hum Sex. 2014;23(12):54–57.
81. Qin S, Shan M, Zeng TB, et al. Clinical observation of Qianlie Beixi Capsules combined with α-receptor blockers in the treatment of chronic prostatitis/chronic pelvic pain syndrome. West China Med J. 2009;24(06):1395–1397.
82. Sun FL, Li HB, Li GZ. Clinical study of Relinqing Granules combined with Tamsulosin in the treatment of chronic prostatitis. Mod Drugs Clin. 2021;36(08):1659–1663.
83. Nan HF, Liu J, Wu D, et al. Clinical observation of Relinqing Granules combined with Cefodizime Sodium in the treatment of chronic gonorrheal prostatitis. Chin J Hum Sex. 2021;30(08):121–124.
84. Wang JX. Effect of Relinqing Granules on inflammatory factors and sexual dysfunction in patients with chronic prostatitis. Chin J Hum Sex. 2020;29(10):129–132.
85. Xu L, Che XP, Gu J, et al. Observation of the efficacy of Relinqing Granules combined with Doxazosin and Levofloxacin in the treatment of chronic bacterial prostatitis. China J Tradit Chin Med Pharm. 2018;36(07):1711–1713. doi:10.13193/j.issn.1673-7717.2018.07.047
86. Zheng DX. Clinical observation of 120 cases of chronic prostatitis treated with Qianlie Tongyu Capsules combined with Sheni Tong. China Natl Folk Med. 2015;24(06):67–68.
87. Zhu ZH. Clinical observation of Qianlie Tongyu Capsules combined with Tamsulosin in the treatment of 42 cases of chronic non-bacterial prostatitis. J Yunnan Univ Tradit Chin Med. 2011;32(04):23–24. doi:10.16254/j.cnki.53-1120/r.2011.04.058
88. Wu ZW. Clinical observation of Tamsulosin combined with Qianlieping Capsules in the treatment of chronic prostatitis. New Chin Med. 2014;46(05):79–81. doi:10.13457/j.cnki.jncm.2014.05.031
89. Zhu QH, Liu WH. Clinical observation of integrated traditional Chinese and Western medicine in the treatment of chronic prostatitis. China J Tradit Chin Med Pharm. 2014;32(12):3064–3066. doi:10.13193/j.issn.1673-7717.2014.12.080
90. Cheng YL. Study on the inflammation mechanism and efficacy analysis of Qianlieping Capsules combined with Western medicine in the treatment of chronic prostatitis. Int Med Health Guid News. 2016;22(18):2764–2767.
91. Zhang GQ, Zhang Q, Li J, et al. Observation of the efficacy of Qianliean Suppository combined with Tamsulosin in the treatment of chronic non-bacterial prostatitis. Gansu Med J. 2015;34(07):512–514.
92. Xu WB, Zhao XL, Chang JK, et al. Clinical observation of Tamsulosin Sustained-Release Tablets combined with Qianliean Suppository and Gatifloxacin in the treatment of chronic pelvic pain syndrome. Shanxi Med J. 2014;43(12):1436–1438.
93. Lin QT, Chen ZC, Rao DP. Efficacy and safety of Wenglitong Tablets in the treatment of patients with chronic prostatitis. Liaoning J Tradit Chin Med. 2015;42(03):543–545.
94. Hao CH, Qu XW, Shan ZJ, et al. Evaluation of the clinical efficacy of Wenglitong Capsules combined with α-receptor blockers in the treatment of CP/CPPS. Contemp Med. 2012;18(05):150–151.
95. Zhou SY, He SM, Chen N. Clinical observation of Shuangshi Tonglin Capsules combined with Tamsulosin in the treatment of type IIIB prostatitis with non-liquefied semen. Chin J Hum Sex. 2021;30(08):28–31.
96. Zhu JW, Luo HQ. Observation of the efficacy of Shuangshi Tonglin Capsules combined with Levofloxacin in the treatment of chronic prostatitis. New Chin Med. 2016;48(02):72–73. doi:10.13457/j.cnki.jncm.2016.02.029
97. Litwin MS, Saigal CS, Lubeck DP, et al. Health-related quality of life in men with metastatic prostate cancer: the misleading effect of lead-time bias. BJU Int. 2003;91:9–13. doi:10.1046/j.1464-410X.2003.04010.x
98. Nickel JC, True LD, Krieger JN, et al. Consensus development of a histopathological classification system for chronic prostatic inflammation. BJU Int. 2001;87:797–805. doi:10.1046/j.1464-410x.2001.02193.x
99. Zhang C, Xi JB, Luo RX, et al. Meta-analysis of Ningmitai combined with levofloxacin in the treatment of chronic prostatitis. Chin J Integr Tradit West Med Surg. 2021. doi:10.3969/j.issn.1007-6948.2021.03.013
100. Zhu XR, Cao PJ. Analysis of the origin and clinical application of Bi Xie Fen Qing Yin. J Clin Tradit Chin Med. 2019;31(3):4. doi:10.16448/j.cjtcm.2019.0126
101. Dai JF, Zhang AP, Ye QY, et al. Study on the mechanism of Shuangshi Tonglin capsules in treating prostatitis based on network pharmacology and molecular docking. Clin Res Tradit Chin Med. 2023;15(23):8–16.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Bibliometric Analysis of Urologic Chronic Pelvic Pain Syndrome From 2000 to 2022
Wang J, Cao B, Lin S, Wang Y, Zhang Q, Jiang Y, Li W, Zhu Y
Journal of Pain Research 2023, 16:1225-1241
Published Date: 10 April 2023
Acupuncture-Related Interventions for Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Liu X, Ren L, Xu W, Huang W, Wang R
Journal of Pain Research 2026, 19:612867
Published Date: 9 June 2026