Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Acupuncture for Early Parkinson’s Motor Symptoms: A Multicenter Randomized Controlled Trial Protocol
Authors Zhang J, Xie Y, Huang W, Wu J, Feng L, Li H, Jia X, Zhang X, Tang X, Yu F, Dong Z, Cui S ![]() , Liu W, Zhu X, Guo Z
, Liu W, Zhu X, Guo Z ![]() , Xu N, Wang L
, Xu N, Wang L
Received 10 March 2026
Accepted for publication 26 May 2026
Published 11 June 2026 Volume 2026:22 608205
DOI https://doi.org/10.2147/NDT.S608205
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Jiewen Zhang,1,2,* Yici Xie,1,2,* Weixin Huang,3 Junshang Wu,3 Lubao Feng,1 Hongtao Li,1 Xinyan Jia,4 Xie Zhang,5 Xiaorong Tang,1 Fangfei Yu,1 Zhengni Dong,6 Shaoyang Cui,2 Wenhao Liu,1 Xiaodong Zhu,7 Zining Guo,1 Nenggui Xu,1 Lin Wang1
1South China Research Center for Acupuncture and Moxibustion, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 2Department of Rehabilitation, Shenzhen Hospital (Fu Tian) of Guangzhou University of Chinese Medicine, Shenzhen, People’s Republic of China; 3Department of Acupuncture, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, People’s Republic of China; 4Department of Acupuncture, Shenzhen Bao’an Pure Traditional Chinese Medicine Hospital, Shenzhen, People’s Republic of China; 5School of Basic Medical Sciences, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 6Department of Acupuncture, The First Affiliated Hospital of Tianjin University of Chinese Medicine, Tianjin, People’s Republic of China; 7Department of Traditional Chinese Medicine, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Nenggui Xu, South China Research Center for Acupuncture and Moxibustion, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China, Email [email protected] Lin Wang, South China Research Center for Acupuncture and Moxibustion, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China, Email [email protected]
Background: Pharmacological treatment of motor disorders in early Parkinson (PD) has reached a bottleneck, and acupuncture as an important component of non-pharmacological therapy has demonstrated therapeutic potential. However, current evidence is limited in both quantity and quality, highlighting the need for further clarification of its efficacy.
Methods: A multi-center, investigator and participant blinded, randomized parallel group design was employed. 136 eligible participants were randomly assigned in a 1:1 ratio to either the acupuncture or sham acupuncture group via a central randomization system, received 12 sessions over 4 weeks. The primary outcome was motor function, assessed using the Unified Parkinson’s Disease Rating Scale-III (UPDRS-III). Secondary outcomes were objective gait metrics captured with the Ready system, disease stage assessed by the Hoehn and Yahr scale (HY), and quality of life measured by the Activities of Daily Living scale (ADL) and the Parkinson’s Disease Questionnaire 39 (PDQ 39). Levodopa dosage was recorded before and after treatment. Assessments were conducted at four time points (weeks 1, 2, 3, and 4), with 8 weeks follow up. Blood samples were collected before and after treatment for LC-MS/MS untargeted metabolomics and deep proteomics analysis.
Discussion: This study will aim to clarify the efficacy of acupuncture for early PD motor symptoms through an evidence-based randomized controlled trial (RCT), and explore the underlying mechanisms of acupuncture using multi-omics approaches.
Keywords: acupuncture, Parkinson, motor, randomized controlled trial, protocol
Introduction
Since Parkinson’s disease (PD) was first described, finding ways to overcome or slow its progression has become a major global health issue.1 Driven by factors such as aging, the prevalence of PD has increased by 118% over the past 30 years, making it the second most common neurodegenerative disease worldwide.1–3 Furthermore, the burden of PD on healthcare systems is expected to continue to increase, underscoring the need to develop effective health policies to address this challenge.1,2 The clinical manifestations of PD are primarily characterized by four core motor symptoms: tremor at rest (T), rigidity (R), akinesia (A), and postural instability (P).1,4 Additionally, PD also associated with a range of non-motor symptoms, which contribute to the significant symptom overlap between PD and other diseases.4,5 Despite the development of landmark diagnostic criteria by the Movement Disorder Society (MDS), diagnosing PD remains challenging.1,4,6 Moreover, due to the persistent progression of PD, once the disease reaches advanced stages, its core motor symptoms become increasingly difficult to manage, severely compromising patients’ quality of life and potentially leading to irreversible disability or even death in later stages.7,8 As a result, typical core motor symptoms continue to serve as key evidence for confirming a PD diagnosis and remain the primary focus of treatment.4,6,7 In such cases, timely identification of early PD core motor symptoms and intervention are particularly crucial.
Currently, the early core motor symptoms of Parkinson’s disease (PD) are primarily treated with dopamine replacement agents, represented by levodopa.9–11 However, prolonged use of levodopa leads to the “wearing-off phenomenon” (reduced duration of therapeutic effect) and the “on-off phenomenon” (sudden fluctuations in symptoms due to variations in drug efficacy).12 Furthermore, complications such as dyskinesia, which are associated with levodopa, may exacerbate the core symptoms of PD. In addition, the risk of adverse effects, including nausea and vomiting, has led some clinicians and patients with PD to hesitate to initiate this therapy in the early stages of the disease.9 Other available pharmacological treatments, such as dopamine receptor agonists and monoamine oxidase B inhibitors (MAOBIs), are commonly used as adjuncts to levodopa therapy, where negative consequences are inevitable with levodopa again.9,13–15 Against the backdrop of a bottleneck in the progress of pharmacological treatments, the development of non-pharmacological therapies has opened up new possibilities for the management of early motor symptoms in PD,16 further exploration of various non-pharmacological therapies for managing early PD motor symptoms holds considerable clinical value and is urgent.
Acupuncture therapy plays a critical role in non-pharmacological therapy; it emphasizes exerts therapeutic effects by stimulating specific acupoints to induce the sensation of “de qi”.8,17,18 Due to its distinct advantages, including safety, ease of administration, and cost-effectiveness, acupuncture has increased application in PD treatment,19,20 and has been recommended (Grade B) by clinical practice guidelines for symptom management of PD, indicating its considerable potential.8,16,17,21 Acupuncture has a history of application spanning thousands of years in its country of origin, China, and its global influence is rising.5 Therefore, demonstrating the efficacy of acupuncture for early PD core motor symptoms has significant implications for health policies. Therefore, demonstrating the efficacy of acupuncture for early PD core motor symptoms has significant implications for health policies. However, the application of acupuncture in this field still suffers from significant deficiencies in the level of evidence, which primarily stem from methodological flaws in research design. One such issue is randomization bias and the challenges associated with blinding. As a critical initiation procedure in RCTs, randomization bias leads to the infiltration of confounding factors that affect efficacy evaluation, causing issues such as baseline imbalance and weakening causal inference regarding acupuncture’s efficacy; it may even lead to the prediction of subject allocation, resulting in erroneous feedback on acupuncture’s efficacy. The challenges regarding blinding stem from the inherent difficulty of blinding acupuncturists in clinical research; previous studies have lacked effective blinding devices, causing loopholes regarding intervention bias to be infinitely magnified. Another issue is the questioning of the “placebo effect” caused by the setting of acupuncture control measures. Due to the lack of an ideal inert sham acupuncture control, there remains a prevalent view in the international academic community that the observed efficacy may stem from non-specific factors such as the therapeutic environment or the natural course of the disease. Furthermore, the insufficient feedback on the true efficacy of acupuncture caused by the lack of efficacy assessment tools further exacerbates the challenges regarding the level of evidence for acupuncture treatment. Therefore, establishing high-quality RCT evidence to verify the therapeutic value of acupuncture is crucial for confirming its future clinical relevance.22
Based on the above, this study will aim to (1) address the issues mentioned above and implement a self-developed randomization system to correct flaws in the randomization process, utilizing a Modular Multichannel Acupuncture Device (MoCAD) to ensure blinding throughout the process, and minimize placebo effects, (2) employ objective measurement tools to accurately assess the treatment effects of acupuncture in a rigorously designed, evidence-based randomized controlled trial (RCT) aimed at preliminarily evaluating the efficacy of acupuncture in treating core motor symptoms in early PD.23 Additionally, this study also will utilize multi-omics techniques to explore the mechanistic effects of acupuncture at the clinical level. The findings of this study will provide valuable reference for future research and help develop new strategies to improve PD treatment.
Methods
This study adhered to the overall reporting guidelines of the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2025 checklist and Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA).24,25 The details of sham acupuncture are in accordance with the latest SHam Acupuncture REporting guidelines and a checklist in clinical trials (SHARE) guidelines.26
Involvement from Patients and the Public
During the protocol design phase, dedicated investigators conducted verbal consultations with patients presenting at the outpatient clinic with motor symptoms of PD to assess their willingness and previous experience with acupuncture therapy, as well as the frequency of treatment they would most readily accept. Additionally, the investigators inquired about their willingness to participate if this study were to be conducted. After completing the survey, the investigators compiled patient feedback, which was used to refine certain aspects of the protocol, including the estimated duration of the study and the number of acupuncture sessions. The planning and details of reporting the study results were not developed with direct involvement from patients or the public.
Study Design
This RCT was designed as a multicenter study with blinding to the principal investigators (study designers, outcome assessors, and statisticians) and participant, no blinding to the acupuncturists, parallel randomization, superiority trial design. A total of 136 eligible participants were randomly assigned in a 1:1 ratio to either the acupuncture group (n=68) or the sham acupuncture group (n=68) following baseline assessments (Table 1 and Figure 1). The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Tianjin University of Chinese Medicine and other participating centers (TYLL2025[K]) and registered with the International Traditional Medicine Clinical Trial Registry (ITMCTR2025001351).
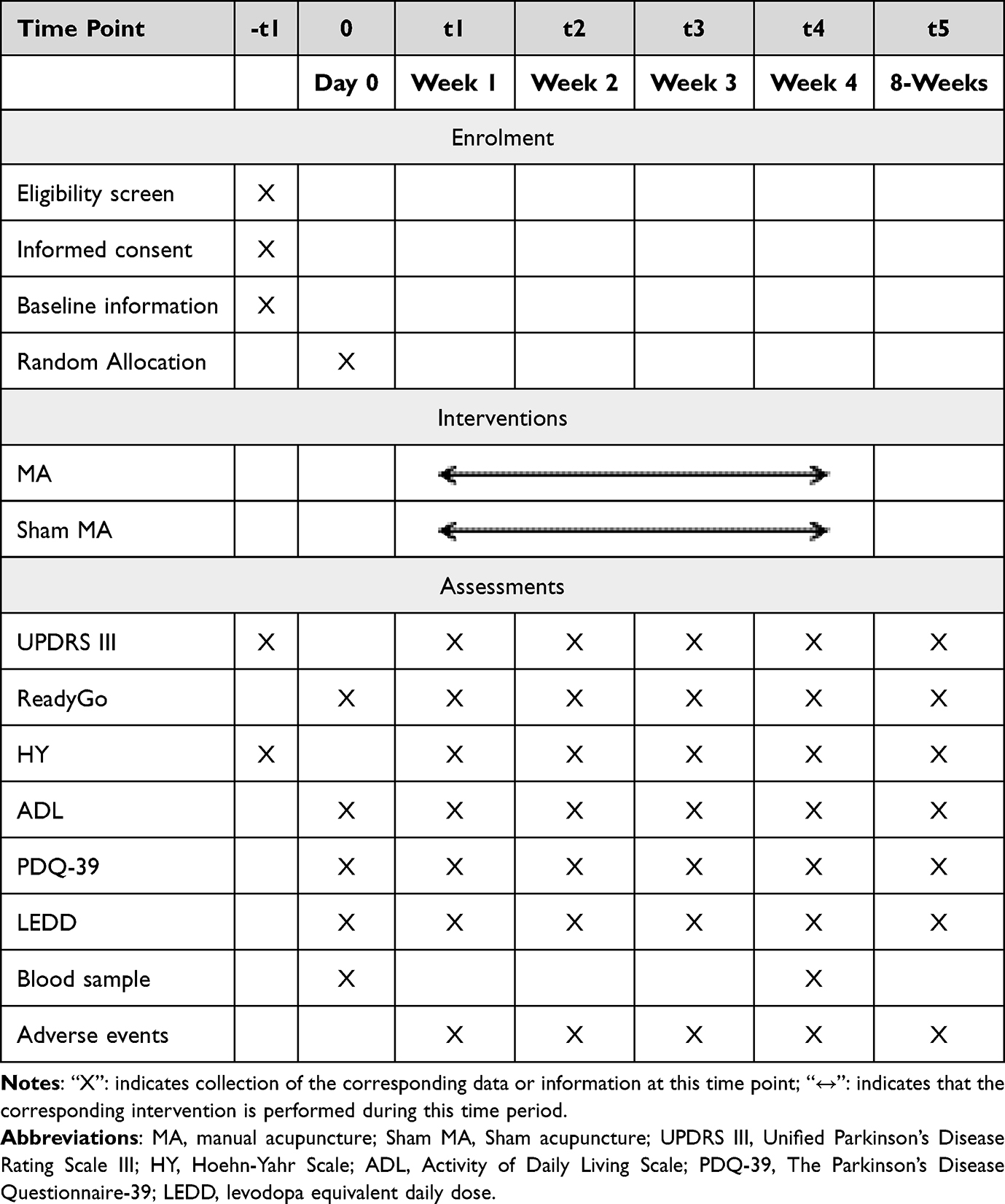 |
Table 1 Inclusion Criteria |
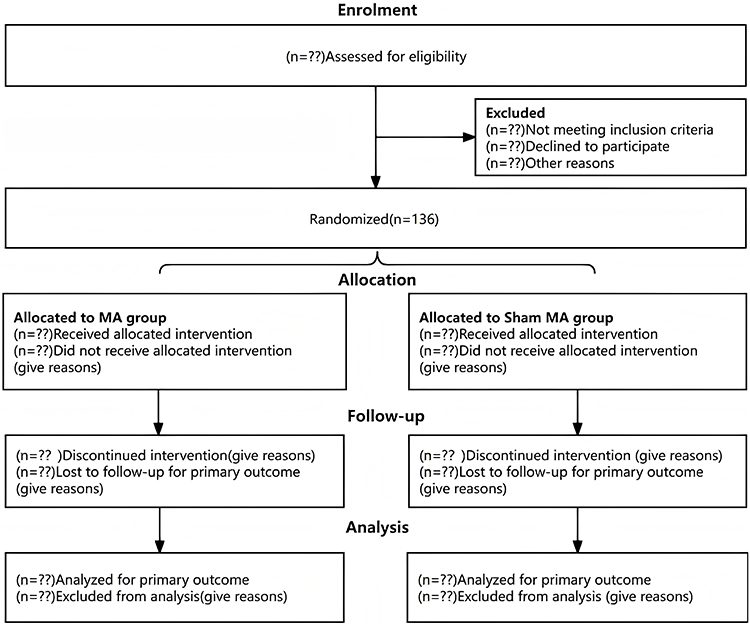 |
Figure 1 Study flow (The “??” symbol indicates the number of subjects who met this item). |
Trial Setting
This trial was conducted at five centers in China: the First Affiliated Hospital of Tianjin University of Chinese Medicine, Tianjin Huanhu Hospital, Tianjin Beichen District Chinese Medicine Hospital, Tianjin Medical University General Hospital, and Guangdong Provincial Hospital of Chinese Medicine. During the study period, acupuncture was administered in dedicated acupuncture rooms established in the outpatient or inpatient departments of each center. Each acupuncture bed was separated by curtains, ensuring privacy and independence of each subject during the acupuncture treatment, unaffected by the research environment.
Participant Recruitment and Consent
Participant recruitment will be conducted through multiple channels at each trial center, including outpatient clinics, recruitment posters, and official WeChat accounts. For individuals who meet the eligibility criteria determined by clinical physicians, the researchers will provide a thorough explanation of the trial objectives, procedures, content, and relevant details. After ensuring complete understanding, the participants or their legally authorized representatives will provide informed consent before proceeding to the next phase.
Eligibility Criteria
Diagnostic Criteria
Diagnostic criteria for PD were based on the 2015 MDS Diagnostic Criteria. These diagnostic criteria have been validated in the population with PD in China and demonstrate higher sensitivity and specificity than alternative criteria.6,27
Inclusion Criteria
- Meeting the above diagnostic criteria.
- Aged 30–75.
- Hoehn & Yahr stage ≤ 2.
- The presence of one or more TRAP core motor symptoms was assessed using the Unified Parkinson’s Disease Rating Scale (UPDRS).
- Clear consciousness, normal cognition, and the ability to understand and cooperate with relevant assessments and examinations.
- Having been using a stable dose of levodopa for the past 30 days.
- Voluntarily signing and providing informed consent.
- Have not received acupuncture treatment within the past six months.
Exclusion Criteria
- Having motor symptoms attributable to other diseases.
- Having uncorrectable coagulopathy or bleeding tendency, leading to the inability to receive acupuncture.
- Previously underwent DBS or other surgery related to PD treatment.
- With a history of psychiatric disorders, substance-use disorders, or epilepsy, or current use of antipsychotics or antidepressants.
- Severe primary diseases of the circulatory or respiratory system (or other serious primary diseases).
- Currently participating in other clinical studies.
Dropout Criteria
Participants will be considered to drop out of the trial due to the following reasons:
- The participants withdrew their informed consent or were lost to follow-up owing to lack of treatment efficacy or other reasons.
- Participants were unable to continue participating in the study owing to adverse events (AEs), disease progression, or other uncontrollable factors.
Elimination Criteria
Participants will be eliminated from the trial due to the following reasons:
- A diagnosis error.
- Assignment to an incorrect group for any reason.
- Poor compliance and failure to cooperate in completing the acupuncture treatment course during the trial.
- The established protocol was violated during the study period, and other therapies that compromised the evaluation of the overall therapeutic effect were arbitrarily used.
Discontinuation Criteria
If a participant experiences a serious adverse events (SAEs) or other significant incident during the study, the clinical investigator will report it, and the Clinical Events Committee (CEC) will jointly determine whether continuation of the trial is inappropriate; if this were the case, the study would be discontinued.
Dropout, Discontinuation, and Exclusion Handling Procedures
In the event of a dropout, elimination, or discontinuation, the responsible investigator must document the reasons in detail, file them in the study records, and report them to the Data Monitoring Committee (DMC). For participants who experience special circumstances but are not lost to follow-up, the responsible investigator should encourage and provide multiple means, such as phone calls, to facilitate completion the follow-up and data collection. If a participant experiences special circumstances due to a AEs/SAE, the responsible investigator will implement appropriate measures based on the situation to ensure the safety of the participant.
Termination Criteria
Considering that the safety of acupuncture has been widely recognized, in consultation with the research team and DMC, pre-specified stopping criteria triggered by AEs related to acupuncture were not established. However, if any center commits a significant error, resulting in the full disclosure of blind information, the termination criteria for this trial will be activated. Only the DMC had the authority to terminate the entire study.
Randomization
A third party (responsible only for randomization) personnel will use a centralized randomization system developed by the research team, specifically for evidence-based acupuncture research, to randomly allocate 136 eligible participants according to a 1:1 ratio using stratified (by center) block randomization (block size set as four or six modules according to center sample size). The detailed randomization procedure involved randomization staff collecting the necessary participant information and entering it into a central randomization system. Upon receiving the data, the system automatically assigns groups. The randomized personnel then forwarded the group assignment to the designated acupuncturist via the backend of the system.
Blinding and Allocation Concealment
The trial employed a double-blind design for both the principal investigators (study designers, outcome assessors, and statisticians) and participants. Due to the specific nature of acupuncture clinical trials, the acupuncturists performing the treatments were not blinded in this study. Randomization was performed by independent personnel using a central randomization system. The allocation sequence was unpredictable and concealed prior to assignment, and the results were communicated to acupuncturists through the backend of the system, ensuring the rigor of allocation concealment. The principal investigators independently worked under rigorous allocation concealment to ensure that blinding was maintained throughout the study. Furthermore, owing to the lack of reliable tools in most previous acupuncture clinical trials, achieving complete blinding of the participants during the entire acupuncture procedure has been challenging. For this purpose, we developed MoCAD. The overall MoCAD enclosure is hemispherical, featuring five channels on the device shell: one at the top, two at a 45-degree angle, and two near the bottom, which can meet the diverse requirements of perpendicular, oblique, and horizontal acupuncture techniques in clinical practice. Meanwhile, the MoCAD includes two type, MoCAD-A and MoCAD-B. Among them, MoCAD-A’s base is hollow and is used for the acupuncture group, while the MoCAD-B’s base is impermeable and equipped with a disposable blunt acupuncture needle is used for the sham acupuncture group. When acupuncturist used the MoCAD-B to manipulate, simulates the sensation of needle insertion on the skin’s surface without penetrating the skin or acupuncture points to evoke the “de qi” sensation, thereby ensuring that subjects remain blinded during the acupuncture procedure. The details of the MoCAD have been documented in previous studies.23 Additionally, blinded study information will be stored in duplicate by independent randomization personnel and a central system. Should emergency unblinding be necessary during the study, it will be conducted in accordance with established protocols.
Treatment Protocol
All the participants underwent foundational treatment administered by clinicians in accordance with the American Academy of Neurology’s Clinical Practice guidelines for early PD and the 2020 Chinese “Parkinson’s Disease Treatment (4th edition)”. Foundational treatment included medications, such as levodopa and levodopa combination therapies, to alleviate PD symptoms.28 The responsible personnel record the initial dose of the medication and information on any changes, documenting these details in the Case Report Form (CRF). Furthermore, manual acupuncture (MA) will be used as the acupuncture type in this trial, given its demonstrated effectiveness in previous research.8,17 Both MA and sham MA procedures will be administered by licensed acupuncturists with at least five years of experience at each center, with no more than two practitioners involved to reduce operator bias. Acupoint selection was based on the clinical practice of the research team and related evidence, utilizing Yintang (GV24+), Shenting (GV24), Baihui (GV20), Dazhui (GV14), bilateral Fengfu (GV16), and Jiaji (EX-B2), among them, the EX-B2 points include all the EX-B2 acupoints on both sides of the spinous processes from the 1st thoracic to the 5th lumbar vertebra. All acupoint localizations were referred to the 2021 Chinese publication of “Nomenclature and Location of Meridian Points” (Table 2 and Figure 2).
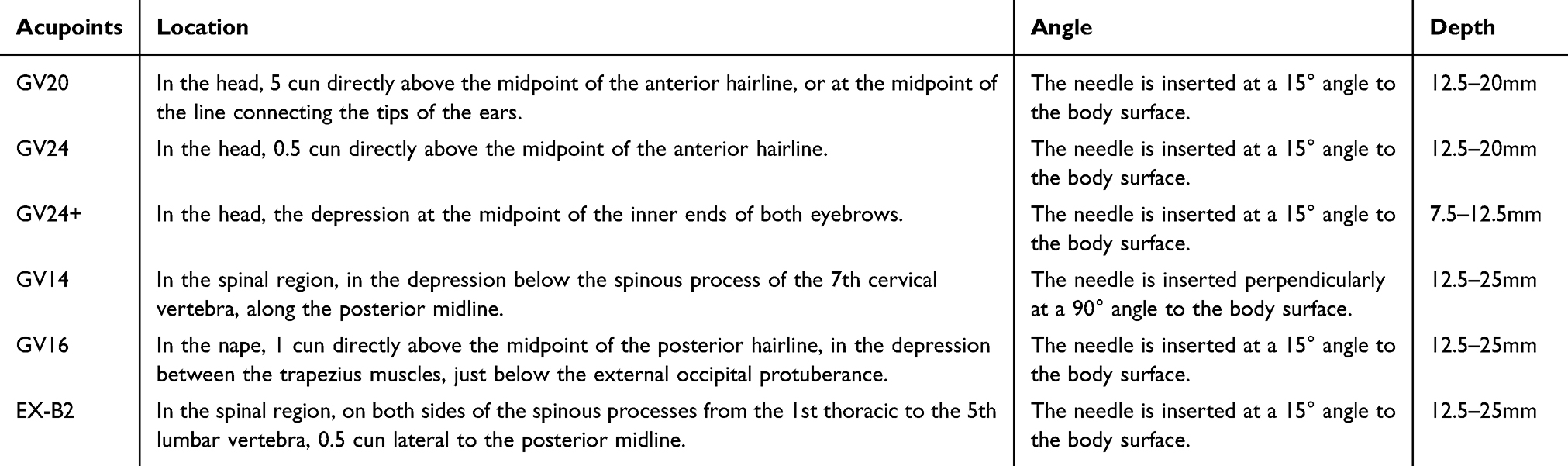 |
Table 2 Acupoints Detail |
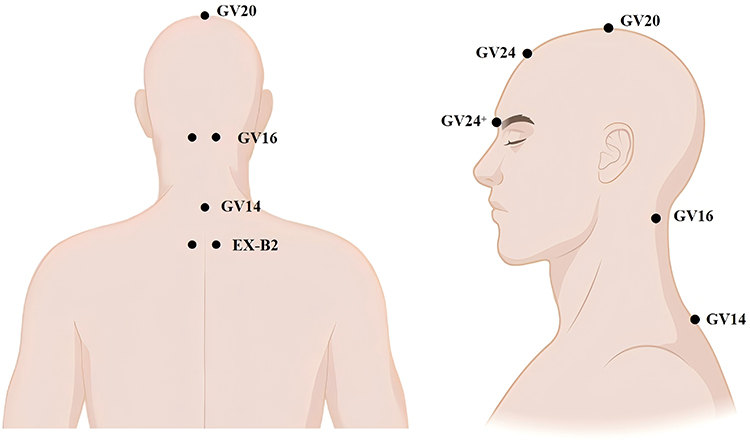 |
Figure 2 Detail of acupoints. |
Acupuncture Group
The responsible acupuncturist performed acupuncture treatment daily at 10:00 AM ± 30 min in the dedicated acupuncture room at each center. Patients were instructed to relax and assume a sitting position while avoiding unnecessary communication. The total acupuncture treatment cycle lasted four weeks, with three sessions per week, and the needle retention time was 30 min per session. Specific details are listed as follows. The acupuncturist performed routine disinfection using alcohol swabs to disinfect areas at the GV24+, GV24, GV14, GV16, and EX-B2 acupoints. The adhesive pad at the bottom of MoCAD-A was peeled off and applied to the selected acupuncture points on the skin. The corresponding needle catheter was inserted depending on the insertion angle for each acupoint. It should be noted that the MoCAD-A device covers insertion angles from 0° to 180° and has a circular hollow design at the bottom, which does not interfere with the acupuncturist’s needle insertion technique. The acupuncturist then selected a disposable stainless steel acupuncture needle (0.25 mm × 40 mm or 0.25 mm × 25 mm, Suzhou Medical Supplies Factory, Huatuo brand), placed it into the catheter, and used the Flick-finger needle insertion technique to insert the needle into the acupoints. The depth was adjusted to locally induce the sensation of “de qi”. Specific details of the insertion direction, angle, and depth are listed in Table 2.
Sham Acupuncture Group
Given that the efficacy of acupuncture has been questioned due to the “placebo” effect, we established a sham acupuncture group in this study. To maximize the demonstration of the specific therapeutic effects of acupuncture, the duration of treatment, communication information, course of treatment, and detailed procedures in the sham acupuncture group were kept consistent with those in the acupuncture group, and the same was applied to acupoint selection. The only difference was that the sham acupuncture group used MoCAD-B and 0.25 mm×40 mm or 0.25 mm×25 mm sterile stainless steel blunt-tip needles (Suzhou Medical Supplies Factory, China) in the specific acupuncture procedures. The functions of MoCAD-B have been previously described. In brief, it does not induce the sensation of “de qi” and prevents unblinding.
Outcomes
Primary Outcome
The primary outcome was assessed using the UPDRS-III, evaluated by clinical physicians. The UPDRS-III includes 16 items, each item with professional guidelines for standardizing the assessment process and offers five response options: 0 (normal, no disability), 1 (mild, symptoms noticeable but without impact on physical function), 2 (moderate, affecting independent activities), 3 (moderate, affecting normal life), and 4 (severe, unable to perform normal activities), with lower scores indicating better functioning. Additionally, the UPDRS-III includes supplementary items for recording medication and “on-off” phase information. The validity and reliability of the UPDRS-III have been extensively validated, and the minimum clinically important difference (MCID) is 3.25 points.29–31 Currently, the UPDRS-III has become the core tool for assessing motor symptoms of PD and, therefore, served as the primary outcome in this study.
Secondary Outcomes
- ReadyGo Motion Function Quantitative Evaluation System: The ReadyGo system (Beijing Zhongke Ruiyi Information Technology Co., China) was equipped with independent capture cameras and time-of-flight sensors. It incorporates tracking and recognition algorithms into the system and a deep neural network algorithm based on long short-term memory (LSTM) for enhanced analysis.32 Based on these characteristics, without requiring participants to wear any devices, ReadyGo can precisely identify and capture the spatiotemporal characteristics of up to 32 joint points in three-dimensional space in patients with PD, and further extract frame-by-frame motion sequences of each joint point during the walking process from tracking images. Spatiotemporal and kinematic parameters are input into the algorithm and iteratively calculated to derive refined gait outcomes, such as stride length, gait speed, and swing velocity.32,33
- Hoehn and Yahr (HY) Scale: The HY scale is a clinician-assessed tool primarily designed to evaluate motor dysfunction and deficits in patients with PD, aiming to reflect the overall severity of PD.34 The HY scale has been validated for its effectiveness in assessing motor function and has the characteristics of simple operation, making it a widely accepted and authoritative tool internationally. The scale includes eight stages ranging from Stage 0 (no symptoms) to Stage 5 (requiring a wheelchair or being bedridden), with higher stages indicating more severe disabilities.
- Activities of Daily Living Scale (ADL): The ADL scale includes 10 items designed to assess the ability to perform daily activities, such as dressing, washing, and other seven dimensions of normal living. The total score ranged from 0 to 100, with higher scores indicating greater independence in daily activities.
- Parkinson’s Disease Questionnaire-39 (PDQ-39): The PDQ-39 is a patient-reported outcome (PRO) tool specifically designed to assess the quality of life of patients with PD. It is currently the most widely used tool in the field of PD and has been proven to effectively focus on issues that are most important to patients in clinical settings. Its reliability and validity have been well-established.35,36 The PDQ-39 consists of 39 items that reflect eight major areas of life, including motor function, social situations, and communication. It uses a four-point scoring system with a total score ranging from 0 to 48, with higher scores indicating poorer quality of life.35,36
- Levodopa Equivalent Daily Dose (LEDD): A change in LEDD was observed before and after treatment. LEDD was calculated by recording the daily doses of anti-Parkinsonian medications throughout the study period, converting each dose to its levodopa equivalent dose (LED), and summing the daily LEDs to obtain the LEDD.37
- Bang’s Blinding Index (BBI): A BBI assessment was conducted after treatment to evaluate the success of participant masking. Participants were asked to report whether they believed they had received real acupuncture, sham acupuncture, or were uncertain. BBI was calculated according to the participants’ treatment guesses to quantify the degree of blinding, with values close to 0 indicating random guessing and successful blinding.
Outcome Assessments
All outcome assessments were performed by independent qualified, assessors at weeks 1, 2, 3, and 4, with a total of four assessment points. The assessors were blinded to participants group. Primary outcomes were followed up until 8 weeks post-treatment.
Additional Outcome-Omics Sample Collection and Analysis
Peripheral blood samples were drawn from participants by a nurse at baseline and after treatment completion at 6:30 AM and were collected in EDTA anticoagulant tubes. A third-party technician separated the serum samples by centrifugation at 4000 rpm, 4°C for 15 min, aliquoted 200 µL of the supernatant into each cryovial tube, and stored the samples at −80°C. Upon completion of the study, serum samples were sent to the Shanghai OuYi Biological Company for LC-MS/MS full-spectrum metabolomics and deep blood proteomics analyses, with specific testing procedures described in previous studies.38,39
AEs and Safety Assessment
Common AEs with acupuncture include hematoma, bruising, and pain. AEs were reported by the participants or discovered by acupuncturists and researchers. Once an AE occurs, the acupuncturist or researcher must immediately manage it to ensure it does not progress and inform the subject of potential impacts that may result from the AE. Meanwhile, it will be reported to the CEC for causality assessment according to the World Health Organization Uppsala Monitoring Centre standard (WHO-UMC).40 The CEC will be composed of acupuncturists selected by each center independently of the research. Additionally, AEs will be documented in detail by researchers in the CRF, including the name, onset and resolution time, management approach, causality assessment, and severity classification. SAEs were defined as death, hospitalization, prolonged hospitalization, or any other severe impairment of function or life-threatening condition during the study period. The handling process for SAEs was the same as that for AEs. The DMC reviewed both AEs and SAEs every 6 months.
Data Entry and Management
Data assessors and entry personnel used both paper forms and an Electronic Data Capture (EDC) system for CRF data entry. To ensure the accuracy and completeness of data evaluation and entry, an independent monitoring assistant oversaw the process throughout the assessment and data entry phases. All CRF data were stored at the Clinical Quality Management (GCP) center during the study period and uniformly archived at the GCP Center of the First Affiliated Hospital of Tianjin University of Chinese Medicine upon completion of the trial. The DMC will review the completeness and accuracy of the data every six months to ensure compliance with the study requirements and relevant regulations.
Quality Assurance
All established procedures in this trial, including informed consent communication and signing by the responsible investigators, randomization steps performed by independent personnel, and communication and treatment processes conducted by acupuncturists underwent standardized training in accordance with Standard Operating Procedures (SOPs).
Sample Size
The sample size was calculated using the Power Analysis and Sample Size (PASS) version 15 superiority module based on the primary outcome of the UPDRS III. The parameters were set as follows: significance level (α) = 0.05 and power (β) = 0.9. According to previous research, the mean difference (MD) and standard deviation (SD) between the acupuncture group and the control group were 16.4±20. The superiority margin was determined to be five points based on the MCID of the UPDRS III, combined with consensus opinions from the research team.31,41 Considering a 20% dropout rate, 68 participants per group (136 participants in total) provided 90% of the statistical power, meeting the requirements of this trial.
Statistical Analysis
Data analysis for this study was performed using R, Version 4.3.3, with α set to 0.05. The analysis sets in the data analysis plan include the modified intention-to-treat (mITT) and per-protocol set (PPS). The mITT group was defined as participants who were randomized and received at least one treatment, and the PPS group was defined as participants who successfully completed the treatment protocol. Baseline characteristics were analyzed descriptively. Continuous variables were tested for normal distribution; normally distributed data were presented as MD±SD, while non-normally distributed data were expressed as median and interquartile range (M[P25, P75]). Categorical variables were analyzed using the chi-square test and reported as counts (percentages). The primary outcome was analyzed using the Linear Mixed-Effects Model (LMM) according to a predefined analysis plan. The dependent variable was the UPDRS III score, with fixed effects including group-time interaction, age, sex. Random effects included individual random intercepts and study center effects. Under the assumption of missing completely at random (MCAR) or missing at random (MAR), the LMM provides a valid statistical inference without the need for the imputation of missing values.42 For nonrandom missing data (MNAR), appropriate imputation methods were applied depending on the extent of missingness. The primary outcome analysis results were reported as least squares means (MD) and 95% confidence intervals (95% CI). Secondary outcomes were analyzed using the same model as the primary outcomes, and the results were presented in an identical format. Sensitivity analysis was performed by comparing the outcomes of the mITT and PPS analysis sets to verify the reliability of the results.
Discussion
PD is a common progressive neurodegenerative disorder that severely affects patients’ quality of life and daily functioning, and early intervention is of great significance for delaying disease progression, maintaining motor function, and improving long-term outcomes. Currently, although acupuncture therapy has been confirmed to have potential clinical value in ameliorating early motor and non-motor symptoms of PD and improving quality of life. However, current clinical evidence for acupuncture in treating PD remains inconsistent; previous studies generally suffer from issues such as flaws in research design and methodology, high heterogeneity in acupuncture protocols, and insufficient reporting of efficacy outcomes, limiting the reliability and generalizability of the research results. Furthermore, although some studies have revealed the potential mechanisms of acupuncture in treating PD, most have focused on basic research and lack clinical data for more direct verification of their therapeutic mechanisms. Therefore, addressing the problems generally existing in current research, this study adopted a more rigorous research design. It aims to clarify the efficacy of acupuncture on motor symptoms in early PD through an evidence-based RCT, providing high-quality evidence for the management of motor symptoms in early PD using acupuncture, while further utilizing multi-omics approaches to investigate the potential mechanisms of acupuncture in treating PD.
Firstly, regarding the methodological rigor of the study design, particularly in terms of randomization and blinding, this study employs a self-developed randomization system and a MoCAD device to address these issues. Regarding randomization, it is a key process for initiating high-quality RCTs and a crucial link for inferring the causal strength of acupuncture efficacy; flaws in randomization will lead to between-group differences in confounding factors that affect efficacy evaluation, thereby reducing the credibility of the study results.43,44 Based on this, this study adopts a self-developed randomization system, in which the built-in stratified block randomization method can compensate for randomization flaws. Regarding blinding, due to the inherent specificities of acupuncture clinical research, it is difficult to blind acupuncturists, making blinding setup long regarded as a formidable challenge.45 Analysis of existing high-quality evidence-based acupuncture research indicates that the most appropriate method for blinding is to ensure that principal investigators and participants remain blinded throughout the process.8,17 In this trial, we not only use the self-developed randomization system to ensure allocation concealment, but also developed a MoCAD device capable of simulating the sensation of acupuncture stimulation, making it difficult for the sham acupuncture group to guess their group assignment, thereby reducing the risk of subject bias to ensure the rigor of blinding.45 Sham acupuncture devices such as MoCAD, currently widely used in research, face problems such as limited needle insertion angles that restrict clinical practice operations and invasive procedures that amplify the placebo effect; the self-developed MoCAD device used in this study addresses the aforementioned two problems,23,46 further enhancing the rigor of the study design.
Secondly, addressing the issue of high heterogeneity in acupuncture protocols, this study adopted a standardized acupuncture intervention protocol to enhance the consistency and reproducibility of the intervention. Integrating traditional Chinese medicine theory with modern clinical practice, this study used the acupoints such as GV24 and GV14; existing evidence indicates that acupuncture at GV24, GV14, and related points can improve UPDRS scores by approximately 40% compared to baseline, while also reducing the risk of falls.22,47 Furthermore, the study standardized the qualifications of acupuncturists while implementing standardized training to minimize operator bias. Through the standardization of acupoint selection, acupuncturist qualifications, and procedures, the therapeutic effects were maximized.
Secondly, addressing the issue of high heterogeneity in acupuncture protocols, this study adopted a standardized acupuncture intervention protocol to enhance the consistency and reproducibility of the intervention. Integrating traditional Chinese medicine theory with modern clinical practice, this study used the acupoints such as GV24 and GV14; existing evidence indicates that acupuncture at GV24, GV14, and related points can improve UPDRS scores by approximately 40% compared to baseline, while also reducing the risk of falls.22,47 Furthermore, the study standardized the qualifications of acupuncturists while implementing standardized training to minimize operator bias. Through the standardization of acupoint selection, acupuncturist qualifications, and procedures, the therapeutic effects were maximized.
Additionally, addressing the issue of insufficient feedback on therapeutic efficacy, this study introduced the Ready system. Although current research primarily relies on the subjective assessment tool UPDRS III to evaluate therapeutic outcomes, it remains susceptible to factors such as rater bias, leading to variability in efficacy.29,31 Previous studies have confirmed that acupuncture treatment can ameliorate balance symptoms among typical core motor symptoms of Parkinson’s disease, such as gait speed and stride length.48 Therefore, we introduced the Ready system to quantify gait-related outcomes in balance and combined it with UPDRS III, thereby combining subjective and objective assessment tools to provides more comprehensive feedback on the efficacy of acupuncture. Ultimately, through a rigorous design, comprehensive feedback, and study implementation, this study aims to strengthen the evidence chain for acupuncture treatment of early PD motor symptoms.
It is worth noting that regarding that the pathogenesis of motor symptoms in PD involves microglial polarization and the dysregulation of apoptosis-related proteins. And existed studies have shown that acupuncture at the chorea control area near GV24 can, on one hand, inhibit the polarization of the M1 microglial subtype by mediating glucose metabolic pathways,49 and on the other hand, regulate the ratio of apoptosis-related proteins Bax/Bcl-2 by inhibiting the SIRT1/AMPK signaling pathway,50 thereby ameliorating PD-related symptoms through multiple pathways. However, most existing studies on the metabolic and protein-related mechanisms of acupuncture for PD motor symptoms are basic research, and studies providing direct evidence in a clinical setting are still lacking. Against this background, this study intends to further employ full-spectrum metabolomics and deep proteomics, and apply high-throughput sequencing methods to fill this gap.
Overall, this study addressed the limitations regarding the rigor of randomization and blinding in previous studies and further utilized the validated subjective assessment tool UPDRS III, combined with objectively quantified gait results from the Ready system, to comprehensively and clearly elucidate the efficacy of acupuncture in treating motor symptoms of early PD. Morever, multi-omics approaches will be use to provide neurobiological evidence at the metabolic and protein levels regarding the clinical dimensions of acupuncture in treating motor symptoms of early PD. However, this study has limitations; most participants will come from fixed regions, such as and Tianjin and Guangdong Province, and due to budget constraints, the sample size is relatively small, which may affect the generalizability of the study results.
Reporting Checklist
The authors have completed the SPIRIT reporting checklist.
Data Sharing Statement
The CRFs will be preserved in a locked cabinet at the participating hospitals and can be accessed by the research team only. Patient identifiable data will be used to provide clinical care and follow-up merely, and the trial database will be anonymized. The aggregated research findings will be submitted for publication in a peer-reviewed clinical journal to have widespread dissemination. The original paper files and electronic data will be preserved for at least 5 years after publication, which can be accessible from the corresponding author, Lin wang, with appropriate reasons.
Ethical Approval and Consent to Participate
The study followed the ethical standards established in the 1961 Declaration of Helsinki. This protocol has been registered in International Traditional Medicine Clinical Trial Registry (ITMCTR2025001351) and approved by the Ethics Committee of the First Affiliated Hospital of Tianjin University of Chinese Medicine and other participating centers. Written informed consent will be obtained from all participants.
Author Contributions
Jiewen Zhang and Yici Xie are the co-first authors. Nenggui Xu and Lin Wang are corresponding authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Open Project of National Clinical Research Center for Acupuncture and Moxibustion in Chinese Medicine (NCRCOP2024006), Guangdong Province Higher Education Innovation (2024KCXTD027), Guangdong Basic and Applied Basic Research Project (2023A1515110322), Guangzhou University of Chinese Medicine 2024 Young Top-notch Talent (Team) Cultivation “Challenge Tackling” Project (2025A04J38760), Solid Foundation Project for Enhancing the Capabilities of the Primary Discipline Level of Guangzhou University of Chinese Medicine (GZY2025GB0209), The major achievement project of the “Innovation Enhancement” program of Guangzhou University of Chinese Medicine (GZY2025ZJ05), Outstanding Young Talents (Teams) Cultivating Project of Guangzhou University of Chinese Medicine through the “Open Competition Mechanism to Select the Best Candidates”, Sanming Project of Medicine in Shenzhen (SZZYSM202311015).
Disclosure
No potential conflict of interest was reported by the author(s).
References
1. Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008;79(4):368–14. doi:10.1136/jnnp.2007.131045
2. Xu L, Wang Z, Li Q. Global trends and projections of Parkinson’s disease incidence: a 30-year analysis using GBD 2021 data. J Neurol. 2025;272(4):286. doi:10.1007/s00415-025-13030-2
3. Dorsey ER, Sherer T, Okun MS, Bloem BR. The emerging evidence of the Parkinson pandemic. J Park Dis. 2018;8(s1):S3–S8. doi:10.3233/JPD-181474
4. Cao F, Vogel AP, Gharahkhani P, Renteria ME. Speech and language biomarkers for Parkinson’s disease prediction, early diagnosis and progression. NPJ Park Dis. 2025;11(1):57. doi:10.1038/s41531-025-00913-4
5. Liu X, Fan J, Leong II, et al. Efficacy of acupuncture (Jin’s three-needle) on motor symptoms and anxiety in patients with Parkinson’s disease: protocol for a multicentre, randomised, assessor-blinded clinical trial. BMJ Open. 2024;14(3):e081312. doi:10.1136/bmjopen-2023-081312
6. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease: MDS-PD clinical diagnostic criteria. Mov Disord. 2015;30(12):1591–1601. doi:10.1002/mds.26424
7. Tolosa E, Garrido A, Scholz SW, Poewe W. Challenges in the diagnosis of Parkinson’s disease. Lancet Neurol. 2021;20(5):385–397. doi:10.1016/S1474-4422(21)00030-2
8. Zhao Y, Zhang Z, Qin S, et al. Acupuncture for Parkinson’s disease: efficacy evaluation and mechanisms in the dopaminergic neural circuit. Neural Plast. 2021;2021:1–23. doi:10.1155/2021/9926445
9. Jankovic J, Tan EK. Parkinson’s disease: etiopathogenesis and treatment. J Neurol Neurosurg Psychiatry. 2020;91(8):795–808. doi:10.1136/jnnp-2019-322338
10. Elsworth JD. Parkinson’s disease treatment: past, present, and future. J Neural Transm. 2020;127(5):785–791. doi:10.1007/s00702-020-02167-1
11. Höglinger G, Trenkwalder C; German Parkinson’s Guidelines Committee. Diagnosis and treatment of Parkinson´s disease (guideline of the German Society for Neurology). Neurol Res Pract. 2024;6(1):30. doi:10.1186/s42466-024-00325-4
12. Trenkwalder C, Kuoppamäki M, Vahteristo M, Müller T, Ellmén J. Increased dose of carbidopa with levodopa and entacapone improves “off” time in a randomized trial. Neurology. 2019;92(13):e1487–e1496. doi:10.1212/WNL.0000000000007173
13. De Bie RMA, Katzenschlager R, Swinnen BEKS, et al. Update on treatments for Parkinson’s disease motor fluctuations – an international Parkinson and movement disorder society evidence-based medicine review. Mov Disord. 2025;40(5):776–794. doi:10.1002/mds.30162
14. Pd Med Collaborative Group. Long-term effectiveness of dopamine agonists and monoamine oxidase B inhibitors compared with levodopa as initial treatment for Parkinson’s disease (PD MED): a large, open-label, pragmatic randomised trial. Lancet. 2014;384(9949):1196–1205. doi:10.1016/S0140-6736(14)60683-8
15. Hattori N, Mochizuki H, Hasegawa K, et al. Ropinirole patch versus placebo, ropinirole extended-release tablet in advanced Parkinson’s disease. Mov Disord. 2020;35(9):1565–1573. doi:10.1002/mds.28071
16. Deuschl G, Antonini A, Costa J, et al. European academy of neurology/movement disorder society-European section guideline on the treatment of Parkinson’s Disease: I. Invasive Therapies. Mov Disord. 2022;37(7):1360–1374. doi:10.1002/mds.29066
17. Yan M, Fan J, Liu X, et al. Acupuncture and sleep quality among patients with Parkinson disease: a randomized clinical trial. JAMA Network Open. 2024;7(6):e2417862. doi:10.1001/jamanetworkopen.2024.17862
18. Lu L, Zhang Y, Tang X, et al. Evidence on acupuncture therapies is underused in clinical practice and health policy. BMJ. 2022;376:e067475. doi:10.1136/bmj-2021-067475
19. Deuel LM, Seeberger LC. Complementary therapies in Parkinson disease: a review of acupuncture, tai chi, qi gong, yoga, and cannabis. Neurotherapeutics. 2020;17(4):1434–1455. doi:10.1007/s13311-020-00900-y
20. Donley S, McGregor S, Wielinski C, Nance M. Use and perceived effectiveness of complementary therapies in Parkinson’s disease. Parkinsonism Relat Disord. 2019;58:46–49. doi:10.1016/j.parkreldis.2018.08.003
21. Fan JQ, Lu WJ, Tan WQ, et al. Effectiveness of acupuncture for anxiety among patients with Parkinson disease. JAMA Network Open. 2022;5(9):e2232133. doi:10.1001/jamanetworkopen.2022.32133
22. Li K, Xu S, Wang R, et al. Electroacupuncture for motor dysfunction and constipation in patients with Parkinson’s disease: a randomised controlled multi-centre trial. EClinicalMedicine. 2023;56:101814. doi:10.1016/j.eclinm.2022.101814
23. Wang L, Guo Z, Zhang J, et al. Efficacy of acupuncture on upper limb dysfunction after stroke: a randomized controlled trial protocol with surface electromyography evaluation. Front Med. 2025;12:1615762. doi:10.3389/fmed.2025.1615762
24. Chan AW, Boutron I, Hopewell S, et al. SPIRIT 2025 statement: updated guideline for protocols of randomised trials. BMJ. 2025;389:e081477. doi:10.1136/bmj-2024-081477
25. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. PLoS Med. 2010;7(6):e1000261. doi:10.1371/journal.pmed.1000261
26. Ma P, Liu X, Liu Z, et al. The SHARE: sHam acupuncture REporting guidelines and a checklist in clinical trials. J Evid-Based Med. 2023;16(4):428–431. doi:10.1111/jebm.12560
27. Li J, Jin M, Wang L, Qin B, Wang K. MDS clinical diagnostic criteria for Parkinson’s disease in China. J Neurol. 2017;264(3):476–481. doi:10.1007/s00415-016-8370-2
28. Pringsheim T, Day GS, Smith DB, et al. Dopaminergic therapy for motor symptoms in early Parkinson disease practice guideline summary: a report of the AAN guideline subcommittee. Neurology. 2021;97(20):942–957. doi:10.1212/WNL.0000000000012868
29. Goetz CG, Tilley BC, Shaftman SR, et al. Movement disorder society-sponsored revision of the unified Parkinson’s disease rating scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008;23(15):2129–2170. doi:10.1002/mds.22340
30. Stebbins GT, Goetz CG, Burn DJ, Jankovic J, Khoo TK, Tilley BC. How to identify tremor dominant and postural instability/gait difficulty groups with the movement disorder society unified Parkinson’s disease rating scale: comparison with the unified parkinson’s disease rating scale. Mov Disord. 2013;28(5):668–670. doi:10.1002/mds.25383
31. Horváth K, Aschermann Z, Ács P, et al. Minimal clinically important difference on the motor examination part of MDS-UPDRS. Parkinsonism Relat Disord. 2015;21(12):1421–1426. doi:10.1016/j.parkreldis.2015.10.006
32. Chen H, Du H, Yi F, et al. Artificial intelligence–assisted oculo-gait measurements for cognitive impairment in cerebral small vessel disease. Alzheimers Dement. 2024;20(12):8516–8526. doi:10.1002/alz.14288
33. Li C, Ye C, Sun R, et al. Discrepant spatiotemporal characteristics of gait impairments in thalamic infarction patients. Brain Behav. 2025;15(5):e70582. doi:10.1002/brb3.70582
34. Martinez-Martin P, Skorvanek M, Rojo-Abuin JM, et al. Validation study of the hoehn and yahr scale included in the MDS-UPDRS. Mov Disord. 2018;33(4):651–652. doi:10.1002/mds.27242
35. Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The Parkinson’s disease questionnaire (PDQ-39): development and validation of a parkinson’s disease summary index score. Age Ageing. 1997;26(5):353–357. doi:10.1093/ageing/26.5.353
36. Neff C, Wang MC, Martel H. Using the PDQ-39 in routine care for Parkinson’s disease. Parkinsonism Relat Disord. 2018;53:105–107. doi:10.1016/j.parkreldis.2018.05.019
37. Julien C, Hache G, Dulac M, et al. The clinical meaning of levodopa equivalent daily dose in Parkinson’s disease. Fundam Clin Pharmacol. 2021;35(3):620–630. doi:10.1111/fcp.12646
38. Blume JE, Manning WC, Troiano G, et al. Rapid, deep and precise profiling of the plasma proteome with multi-nanoparticle protein Corona. Nat Commun. 2020;11(1):3662. doi:10.1038/s41467-020-17033-7
39. Wu Y, Shen S, Chen J, et al. Metabolite asymmetric dimethylarginine (ADMA) functions as a destabilization enhancer of SOX9 mediated by DDAH1 in osteoarthritis. Sci Adv. 2023;9(6):eade5584. doi:10.1126/sciadv.ade5584
40. The use of the WHO-UMC system for standardised case causality assessment. Available from: https://www.who.int/publications/m/item/WHO-causality-assessment.
41. Keller DL. Neurostimulation for Parkinson’s disease with early motor complications. N Engl J Med. 2013;368(21):2037–2038. doi:10.1056/NEJMc1303485
42. Mallinckrodt CH, Lane PW, Schnell D, Peng Y, Mancuso JP. Recommendations for the primary analysis of continuous endpoints in longitudinal clinical trials. Drug Inf J. 2008;42(4):303–319. doi:10.1177/009286150804200402
43. Lim CY, In J. Randomization in clinical studies. Korean J Anesthesiol. 2019;72(3):221–232. doi:10.4097/kja.19049
44. Broglio K. Randomization in clinical trials: permuted blocks and stratification. JAMA. 2018;319(21):2223–2224. doi:10.1001/jama.2018.6360
45. Fei YT, Cao HJ, Xia RY, et al. Methodological challenges in design and conduct of randomised controlled trials in acupuncture. BMJ. 2022;376:e064345. doi:10.1136/bmj-2021-064345
46. Luo XC, Liu JL, Yao MH, et al. Specific effect of inserted sham acupuncture and its impact on the estimation of acupuncture treatment effect in randomized controlled trials: a systematic survey. J Integr Med. 2025:S2095–4964(25)00113–X. doi:10.1016/j.joim.2025.07.011
47. Toosizadeh N, Lei H, Schwenk M, et al. Does integrative medicine enhance balance in aging adults? – proof of concept for benefit of electro-acupuncture therapy in Parkinson’s disease. Gerontology. 2015;61(1):3–14. doi:10.1159/000363442
48. Lei H, Toosizadeh N, Schwenk M, et al. A pilot clinical trial to objectively assess the efficacy of electroacupuncture on gait in patients with Parkinson’s disease using body worn sensors. PLoS One. 2016;11(5):e0155613. doi:10.1371/journal.pone.0155613
49. Zou Y, Huang T, Pang A, Zhou H, Geng X. Electroacupuncture regulates glucose metabolism by inhibiting SGLT1 levels, inhibiting microglial polarization, and alleviating Parkinson’s disease. Exp Gerontol. 2024;196:112558. doi:10.1016/j.exger.2024.112558
50. Geng X, Zou Y, Huang T, Li S, Pang A, Yu H. Electroacupuncture improves neuronal damage and mitochondrial dysfunction through the TRPC1 and SIRT1/AMPK signaling pathways to alleviate Parkinson’s disease in mice. J Mol Neurosci. 2024;74(1):1–13. doi:10.1007/s12031-023-02186-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Hu H, Li Z, Cheng Y, Gao H
Journal of Pain Research 2022, 15:1939-1947
Published Date: 13 July 2022
The Effectiveness of Pharmacopuncture in Patients with Lumbar Spinal Stenosis: A Protocol for a Multi-Centered, Pragmatic, Randomized, Controlled, Parallel Group Study
Lee JY, Park KS, Kim S, Seo JY, Cho HW, Nam D, Park Y, Kim EJ, Lee YJ, Ha IH
Journal of Pain Research 2022, 15:2989-2996
Published Date: 23 September 2022
A Systematic Review and Meta-Analysis Protocol on How Best to Use Non-Pharmacologic Therapies to Manage Chronic Low Back Pain and Associated Depression
Guo Y, Ma Q, Zhou X, Yang J, He K, Shen L, Zhao C, Chen Z, Tan CIC, Chen J
Journal of Pain Research 2022, 15:3509-3521
Published Date: 4 November 2022
Central Mechanism of Acupuncture Treatment in Patients with Migraine: Study Protocol for Randomized Controlled Neuroimaging Trial
Jia J, Yan C, Zheng X, Shi A, Li Z, Xu L, Hui Z, Chen Y, Cao Z, Wang J
Journal of Pain Research 2023, 16:129-140
Published Date: 18 January 2023