Back to Journals » Journal of Pain Research » Volume 19
Abnormal Brain Structure and Function in People with Shoulder Pain: A Systematic Review of Neuroimaging Studies
Authors Fan B, Lam CS, Chen S ![]() , Hsu CL, Wong AYL
, Hsu CL, Wong AYL ![]() , McCreesh K, Wong TM, Leong HT
, McCreesh K, Wong TM, Leong HT ![]()
Received 30 March 2026
Accepted for publication 25 June 2026
Published 30 June 2026 Volume 2026:19 613135
DOI https://doi.org/10.2147/JPR.S613135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Alaa Abd-Elsayed
Bin Fan1, Ching Shan Lam1, Shuqi Chen1, Chun Liang Hsu1, Arnold Yu Lok Wong1,2, Karen McCreesh3, Tak Man Wong4, Hio Teng Leong1,2
1Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China; 2Research Institute for Smart Ageing, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China; 3School of Allied Health, and Health Research Institute, University of Limerick, Limerick, Ireland; 4Department of Orthopaedics and Traumatology, School of Clinical Medicine, LKS Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, People’s Republic of China
Correspondence: Hio Teng Leong, Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China, Tel +852 2766 6707, Email [email protected]
Background: Shoulder pain (SP) is a prevalent musculoskeletal disorder. Emerging evidence suggests maladaptive brain plasticity in individuals with SP. This systematic review summarized structural and functional brain abnormalities in individuals with SP and explored their associations with clinical outcomes.
Methods: PubMed, Web of Science, EBSCO, and EMBASE were searched from inception to June 2025. The risk of bias was assessed using JBI checklist, and the evidence was graded using the GRADE approach.
Results: Five cross-sectional studies were included. These studies demonstrated low to moderate risk of bias. Individuals with SP demonstrated lower volume and density of thalamus grey matter compared to healthy controls. Besides, lower grey matter (volume, density or thickness) was observed in regions such as the amygdala, prefrontal, postcentral, and temporal cortices. Functional neuroimaging studies reported both increased and decreased functional connectivity, as well as abnormalities in regional homogeneity (ReHo) and amplitude of low-frequency fluctuation (ALFF) in brain areas including thalamus, prefrontal, anterior cingulate, middle temporal, orbitofrontal, and sensorimotor cortices. These structural and functional brain changes were associated with higher pain intensity, lower pain threshold, longer pain duration, poor shoulder function and psychological outcomes. However, the overall certainty of evidence was rated as very low due to the small number of studies and methodological heterogeneity.
Conclusion: This systematic review provides preliminary, hypothesis-generating evidence on brain abnormalities in individuals with SP. Very low-certainty evidence suggests that SP may be associated with structural and functional abnormalities in brain regions involved in pain processing, emotion, and sensorimotor integration. Further longitudinal studies are needed to validate the findings.
Keywords: shoulder pain, magnetic resonance imaging, neuroimaging, brain alterations, central nervous system
Introduction
Shoulder pain (SP) is the third most prevalent musculoskeletal complaint in primary care, with an estimated prevalence of 1.0%–4.8%.1 The most common cause of SP is rotator cuff-related SP, which includes subacromial impingement syndrome, rotator cuff tendinitis, and rotator cuff tears, accounting for 80% of shoulder conditions.2,3 Other shoulder pathologies include adhesive capsulitis, bursitis, bicipital tendinitis, osteoarthritis, and labral lesions.4 Common clinical features include limited range of motion, weakness, and pain.5 Pain and functional impairment of shoulder negatively affect daily activities, quality of life, and psychosocial well-being.6 Emerging evidence suggested that damage of shoulder structures may not necessarily correlate with intensity and duration of SP.7,8 Previous reviews have reported widespread mechanical hyperalgesia, referred pain, and impaired conditioned pain modulation in individuals with SP,9,10 suggesting that hypersensitivity of the central nervous system plays a role beyond peripheral mechanisms. However, these reviews primarily summarized behavioral and psychophysical evidence without directly examining objective brain changes using neuroimaging techniques. Therefore, it is crucial to synthesize evidence regarding abnormalities on brain images in individuals with SP to better understand mechanisms underlying SP.
As neuroimaging technology advances, it is possible to investigate the complex pain perception and modulation in various musculoskeletal pain conditions.11 Several non-invasive modalities, such as magnetic resonance imaging (MRI), magnetoencephalography (MEG), positron emission tomography (PET), single-photon-emission computed tomography (SPECT/CT), functional near-infrared spectroscopy (fNIRS), and electroencephalogram (EEG), have been used to assess the structure and function of the brain.12 In recent years, MRI has been extensively used in pain research because it offers high spatial resolution for imaging both cortical and deep brain structures, is non-invasive and free of ionizing radiation, and is widely available.13 Numerous studies have revealed abnormal brain structure and function in musculoskeletal pain conditions, including lower back pain,14,15 neck pain,16 and knee osteoarthritis.17 The structural and functional abnormalities in the brain have been identified in regions involved in emotional regulation, attention, memory, and self-referential processing, including the prefrontal cortex,18 amygdala,19 and insula.20 Sensorimotor brain regions such as the precentral cortex21 and cerebellum22 also exhibit abnormalities. Although there are some common pain-processing brain regions,23 various musculoskeletal pain conditions present unique patterns of brain abnormalities.24
Recent research has examined the potential abnormalities of specific brain regions in individuals with SP, such as the thalamocortical pathway25 and prefrontal cortex.26 Neuroimaging studies often exhibit heterogeneity in imaging techniques, analytical methods, and patient populations (eg, distinct diagnoses such as rotator cuff-related SP or adhesive capsulitis, which involve different pathophysiological mechanisms)27,28 This methodological heterogeneity underscores the need for a systematic review to synthesize the existing evidence However, no systematic reviews have summarized the brain abnormality pattern in individuals with SP. This review aimed to: (1) summarize evidence regarding structural and functional abnormalities in the brain of individuals with SP; and (2) determine the relationships between brain abnormalities and clinical outcomes. Understanding the potential brain abnormalities may help clinicians develop more targeted interventions for SP, such as neuromodulation.
Materials and Methods
Protocol
This systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol has been registered with PROSPERO (CRD42023454587).
Search Strategy
The electronic databases of PubMed, Web of Science, EBSCO, and EMBASE were searched from inception to June 2025. The search strategy followed the PECO principle (Population: human adults; Exposure: SP; Comparison: healthy control; Outcome: the structural and functional abnormalities of the brain detected by brain imaging techniques such as MRI, fNIRS, EEG, MEG, PET and SPECT/CT, and the correlations between brain abnormalities and clinical outcomes such as pain intensity, pain duration, muscle strength, range of motion, and psychological outcomes). The reference lists of the included studies were also searched. Additionally, forward citation tracking was performed for the included studies using PubMed and Web of Science. The detailed search strategy is presented in Appendix S1.
Selection Strategy
All citations retrieved from each database were imported into Endnote. After duplicates were removed, three reviewers (B.F. and C.S.L.) independently screened the titles and abstracts for eligibility. Subsequently, the full texts were retrieved and assessed according to the inclusion and exclusion criteria. In case of disagreements between the three reviewers, a third reviewer (H.T.L.) was consulted to reach a consensus.
Studies were selected if they included: (1) participants with SP of any chronicity, including acute SP (duration of < 1 month), subacute SP (duration of 1–3 months), chronic SP (duration of > 3 months) and mixed chronicity;29 (2) one or more brain imaging techniques for assessing brain structure or function; and (3) were published as full-text original research reports. Studies were excluded if they: (1) were in vitro, animal or cadaveric studies; (2) had no comparison with a control group; (3) SP that did not originate from disorders within the shoulder joint (eg, pain due to neck problems, myofascial pain, fibromyalgia, complex regional pain syndrome, or other neurological disorders such as stroke); or (4) were study protocols, editorials, commentaries, opinion-based papers, reviews, or meta-analyses.
Data Extraction and Data Synthesis
Two independent reviewers (B.F. and C.S.L.) extracted data using a standardized form that included: (1) study characteristics (authors, year of publication, study design); (2) participants’ characteristics (sample size, age, sex, diagnosis, duration of symptoms, dominant hand, pain side); (3) characteristics of controls (sample size, age, sex, dominant hand); (4) methods used to assess brain structure or function (eg, functional magnetic resonance imaging (fMRI), etc); (5) outcome measures (eg, brain structure/region, brain function/activity, etc); and (6) clinical outcomes (eg, pain intensity, pain duration, shoulder function, and psychological outcomes, etc) for assessing the correlation with brain findings Extracted data was synthesized through qualitatively description and summary tables according to brain structure, brain function, and clinical relationships.
Assessments of Risk of Bias and Certainty of Evidence
Two reviewers (B.F. and S.Q.C.) independently assessed the risk of bias using the Joanna Briggs Institute (JBI) checklist for analytical cross-sectional studies or JBI checklist for cohort studies.30 This consists of eight questions regarding eligibility criteria, study sample, exposure measures, condition criteria, confounding factors, outcome measures, and statistical analysis. Each item is rated as either: yes, no, unclear, or not applicable. To determine the risk of bias of the included studies, an answer of “yes/no/unclear” was scored as “2/0/1”, respectively, and the percentage of the score in the total score was calculated. Items rated as “not applicable” were not included in the total score calculation. Scores of 75% or above, 55%–75%, and 55% or below were considered as low, moderate, and high risk of bias, respectively.31 Scoring disagreements were resolved by consensus between the two reviewers or, if necessary, by a third reviewer (H.T.L). The intraclass correlation coefficient (ICC), using two-way mixed effects analysis for absolute agreement, was calculated using IBM SPSS Statistics 27.0 for Windows (IBM Corp., Armonk, NY, USA) to determine the inter-rater agreement between the two reviewers.
The certainty of evidence for brain findings and their correlations with clinical outcomes were determined using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE).32,33 Outcomes were rated as having high, moderate, low, or very low certainty evidence according to the GRADE criteria.32,33 The certainty of evidence was downgraded by one level (serious) or two levels (very serious) based on the following domains: (1) risk of bias: downgraded when the evidence was derived from more than 50% (serious) or 75% (very serious) of studies classified as having a moderate or high risk of bias (assessed using the JBI checklist); (2) inconsistency: downgraded when results were inconsistent across more than 50% (serious) or 75% (very serious) of the studies regarding the direction or magnitude of effect, or methodological heterogeneity; (3) indirectness: downgraded when more than 50% (serious) or 75% (very serious) of the included studies differed significantly from the primary review question in terms of populations or outcome measures; (4) imprecision: downgraded by one level (serious) when the total sample size contributing to an outcome was less than 400,34 or by two levels (very serious) when the outcomes was based on a single study; and (5) publication bias: downgraded by a maximum of one level when there was clear evidence of selective reporting.
Results
Study Selection
A total of 2,927 articles were retrieved from the databases. After the removal of duplicates, 2,293 titles and abstracts were screened, with 14 included for full-text screening. The full text of one potential study was not available despite contacting the corresponding author who did not reply. Of the 13 remaining articles, five met the inclusion criteria. The reasons for exclusion were: (1) no comparison with healthy controls (n = 4); (2) disorder unrelated to the shoulder joint (n = 1); (3) no brain imaging (n = 3). The detailed screening flow diagram is shown in Figure 1.
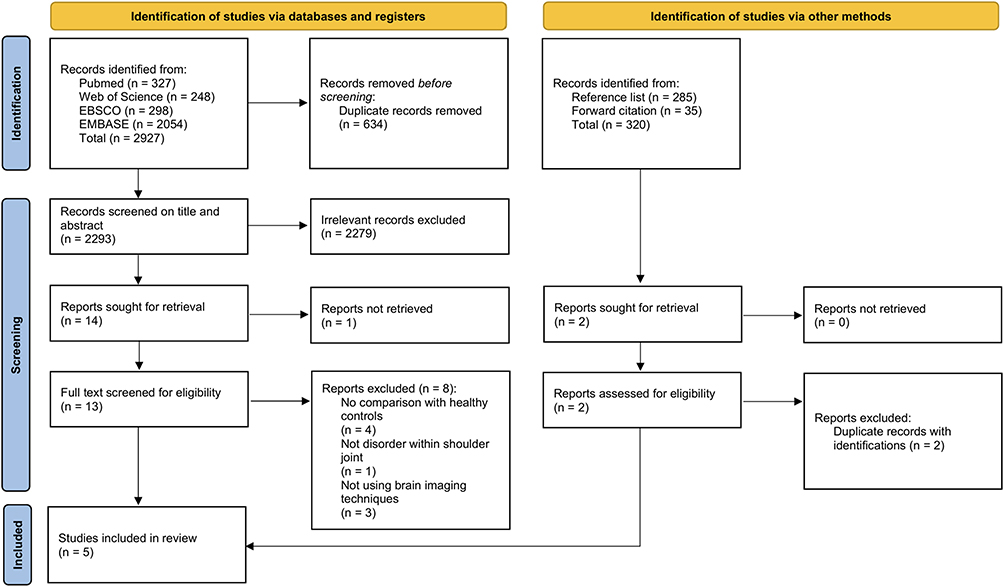 |
Figure 1 The detailed screening flow diagram. |
Study Characteristics
The characteristics of the included studies are summarized in Table 1. The five included studies used a cross-sectional design. It is noteworthy that the healthy control groups in Li et al 202035 and Wei et al 202236 shared identical demographic characteristics, indicating potential overlap in control participants. Therefore, a total of 345 unique participants (199 individuals with SP and 146 healthy controls) were included in these studies after accounting for the shared healthy control cohort (n = 24) between Li et al35 and Wei et al36 The non-unique total number of participants was 369. The sample size per study ranged from 39 to 104. Their mean age ranged from 43.2 to 76.3 years. The diagnoses of SP included rotator cuff-related SP,37 adhesive capsulitis,25,26 and SP for which the specific diagnosis was not reported in the original studies.35,36 Among the five studies, only one study reported a mean pain duration of 6.38 ± 6.05 months for SP participants,35 and the remaining four studies did not report the mean pain duration for SP group.25,26,36,37
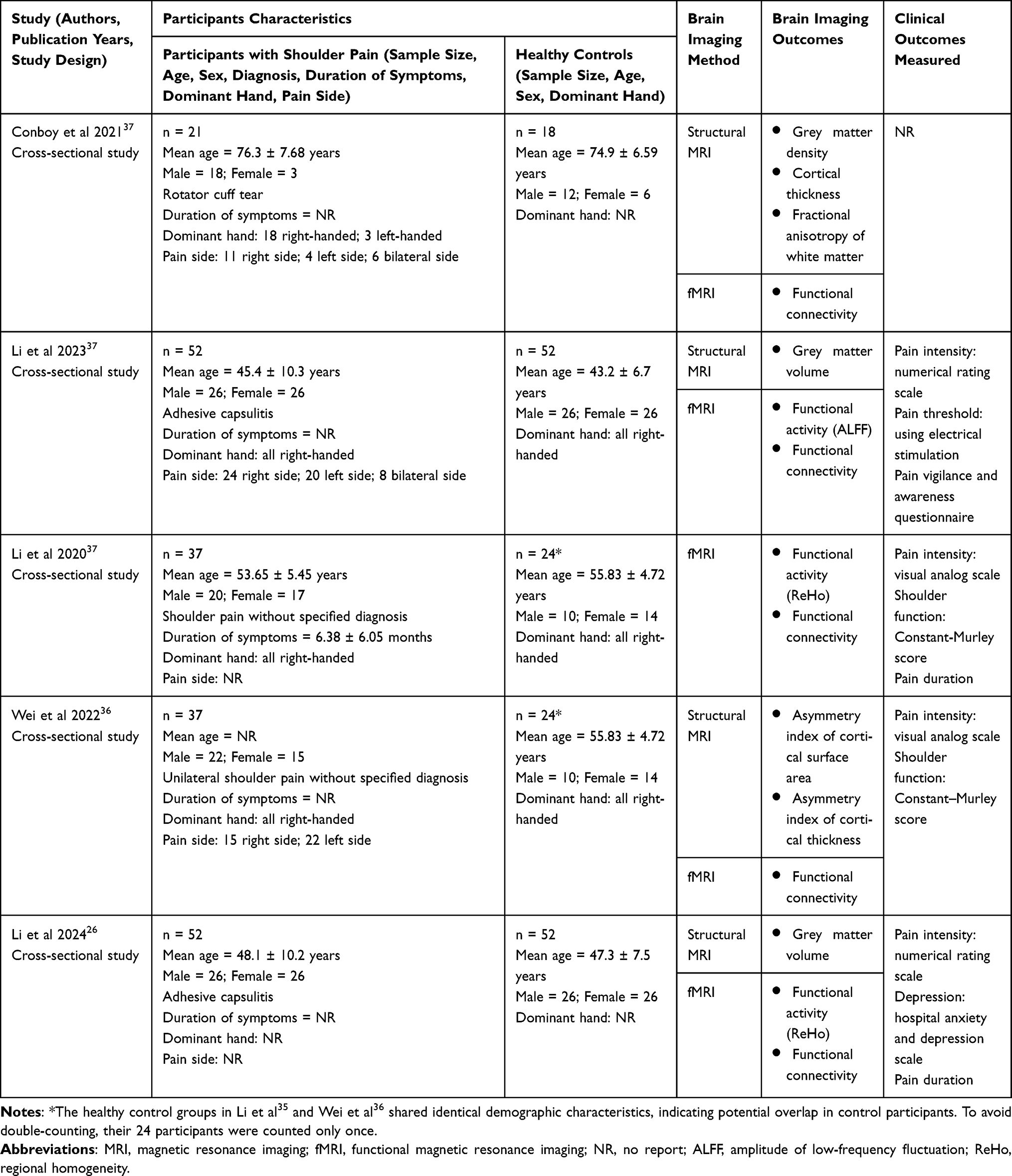 |
Table 1 Study Characteristics |
All included studies used MRI to compare brain structure and function between individuals with SP and healthy controls.25,26,35–37 Four studies assessed the structural differences in grey matter (measured as volume, density, cortical thickness, asymmetry index of cortical surface area, and asymmetry index of cortical thickness),25,26,36,37 and one study assessed the structural differences of white matter37 (measured as fractional anisotropy reflecting the integrity and orientation of white matter).38 All five studies assessed brain function using resting-state fMRI.25,26,35–37 For the resting-state analyses, all five studies examined functional connectivity,25,26,35–37 which reflects functional synergy across brain regions;39 two studies measured regional homogeneity (ReHo),26,35 which represents the functional coordination of local brain regions,40 and one study measured the amplitude of low-frequency fluctuation (ALFF),25 which reflects the intensity of regional spontaneous neural activity.41
Four included studies explored the correlation between brain abnormalities and clinical outcomes.25,26,35,36 Specifically, four assessed pain intensity,25,26,35,36 one examined pain threshold,25 three measured pain duration,26,35 two assessed shoulder function,35,36 one examined pain vigilance and awareness,25 and one assessed depressive symptoms.26
Regarding correction for multiple comparisons, all the five included studies applied appropriate correction methods (such as threshold-free cluster enhancement with family-wise error correction, false discovery rate, and Gaussian random field theory) for the analysis examining structural and functional differences between individuals with SP and healthy controls. However, for the correlation analyses between brain imaging measures and clinical outcomes, only one study (Li et al 2024) explicitly reported using Bonferroni correction.26 The remaining three studies that examined clinical correlations did not report applying correction for multiple comparisons.25,35,36 The methodological characteristics of the included studies were shown in Appendix S2.
Risk of Bias Assessments
Table 2 shows the JBI score of each article. The scores ranged from 62.5% to 81.25%. There was no “not applicable” answer for any items in the included studies. Three studies showed low risk of bias25,26,37 and two studies35,36 showed moderate risk of bias. The ICC for the inter-rater reliability was 0.75. All discrepancies identified during the initial stage were subsequently resolved through discussion involving a third reviewer. The results of the certainty of evidence assessment using GRADE are shown in Appendix S3.
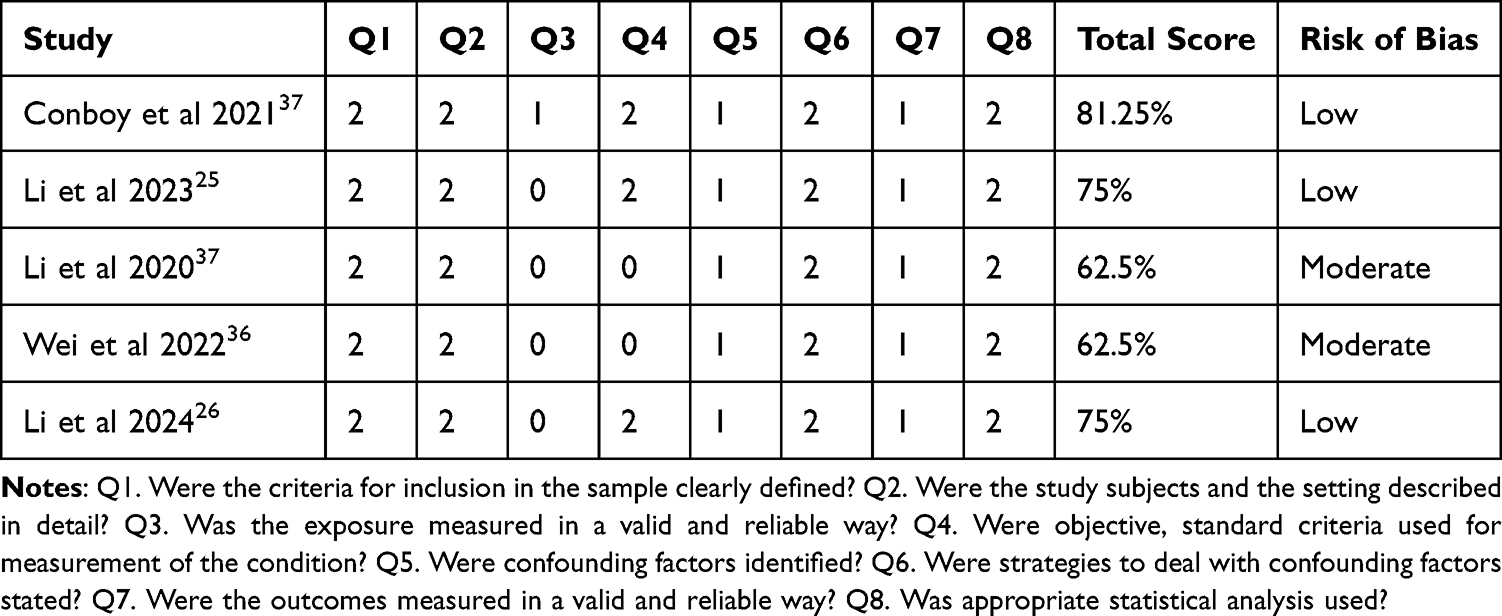 |
Table 2 Results of Risk of Bias Assessment Using Joanna Briggs Institute Checklist |
Syntheses of Results
Abnormalities in Brain Structure
Grey Matter
The results of structural abnormalities are shown in Table 3. Among the four studies that compared the differences in grey matter between individuals with SP and healthy controls,25,26,36,37 two studies reported significant lower grey matter volume in bilateral thalamus,25 left amygdala,26 and right ventromedial prefrontal cortices26 in individuals with SP. One study reported significantly lower grey matter density in the left thalamus, left postcentral gyrus, left anterior intra-parietal sulcus, left inferior parietal lobule, and right temporal-parietal junction in individuals with SP compared to healthy controls.37 One study found significantly smaller cortical thickness in the right temporal-parietal junction, right superior temporal sulcus, and right inferior temporal cortex in individuals with SP compared to healthy controls.37 Another study examined the asymmetry index of cortical surface area and the asymmetry index of cortical thickness and reported no significant differences in the precentral and postcentral cortex in individuals with unilateral left or right SP compared to healthy controls.36 In summary, although two studies with low risk of bias consistently reported smaller volume and density of thalamus grey matter in individuals with SP, the certainty of evidence was very low due to the small sample size, heterogeneous measures and the observational study design. Very low-certainty evidence also supported grey matter structural abnormalities in other brain regions that are responsible for sensory integration, emotion, and cognitive processing, such as the postcentral cortex, amygdala, ventromedial prefrontal cortices, and parietal and temporal cortices.
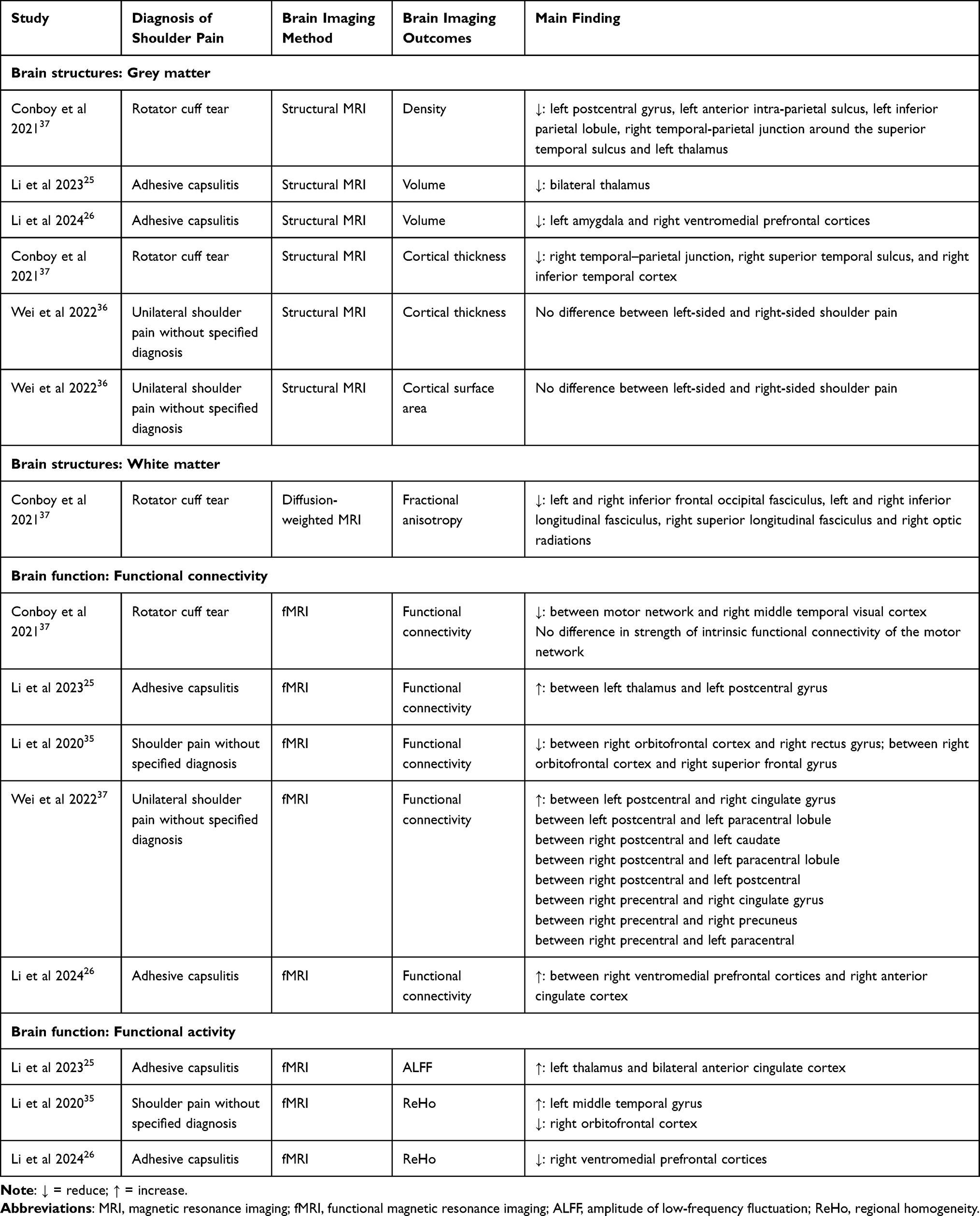 |
Table 3 Summary of Magnetic Resonance Imaging (MRI) Findings of the Included Studies That Compared Brain Structure/Function Between Individuals with Shoulder Pain and Controls |
White Matter
Only one included study compared the white matter structure between individuals with and without SP by calculating fractional anisotropy.37 This study found lower fractional anisotropy of white matter in the bilateral inferior frontal occipital fasciculus, bilateral inferior longitudinal fasciculus, right superior longitudinal fasciculus, and right optic radiations in individuals with SP37 despite the very low-certainty of evidence.
Abnormalities in Brain Function
The results of resting-state fMRI are presented in Table 3. Of the five studies that assessed functional connectivity, heterogeneous findings were reported, showing both greater and lower intensity of functional connectivity in various brain regions.25,26,35–37 Individuals with SP demonstrated significantly lower functional connectivity between the motor network and right middle temporal visual cortex,37 between the right orbitofrontal cortex and right rectus gyrus,35 and between the right orbitofrontal cortex and right superior frontal cortex.35 Other studies showed significantly greater functional connectivity in the left postcentral gyrus with the left thalamus,25 right cingulate gyrus,36 left paracentral lobule,36 and right postcentral gyrus;36 in the right postcentral gyrus with the left caudate36 and left paracentral lobule;36 in the right precentral gyrus with the right cingulate cortex,36 right precuneus,36 and left paracentral lobule;36 and between the right ventromedial prefrontal cortices and right anterior cingulate cortex37 when compared to healthy individuals. Among the five studies examining functional connectivity abnormalities, only one reported directional variations in functional connectivity, showing that individuals with SP presented a negative correlation in functional activity between the motor network and right middle temporal visual cortex, rather than a positive correlation observed in healthy controls.37 Two studies found varied patterns of ReHo between groups.26,35 Individuals with SP demonstrated lower ReHo in the right orbitofrontal cortex35 and right ventromedial prefrontal cortices,26 while there was greater ReHo in the left middle temporal gyrus in individuals with SP.35 Only one study found a greater ALFF in the left thalamus and bilateral anterior cingulate cortex in individuals with SP.25 In summary, very low-certainty evidence supported heterogenous brain functional abnormalities (such as the thalamus, ventromedial prefrontal cortices, anterior cingulate cortex, middle temporal cortex, orbitofrontal cortex, and precentral and postcentral cortex) in individuals with SP.
Correlations with Clinical Outcomes
Pain Intensity
Two included studies revealed a significant association between pain intensity and brain structural abnormalities in individuals with SP25,36 (Table 4). Higher pain intensity was associated with smaller grey matter volume of bilateral thalamus (r = −0.32, p = 0.02)25 and a smaller asymmetry index of the cortical surface area in the precentral cortex for left SP (r = −0.57, p = 0.01).36 However, it should be noted that these studies did not report applying correction for multiple comparisons in their correlation analyses25,36 and the risk of false-positive findings is increased. Functionally, higher pain intensity was associated with greater functional connectivity between right ventromedial prefrontal cortex and right anterior cingulate cortex (r = 0.44, p = 0.005).26 However, the certainty of evidence was very low as only one cross-sectional study reported the correlation.
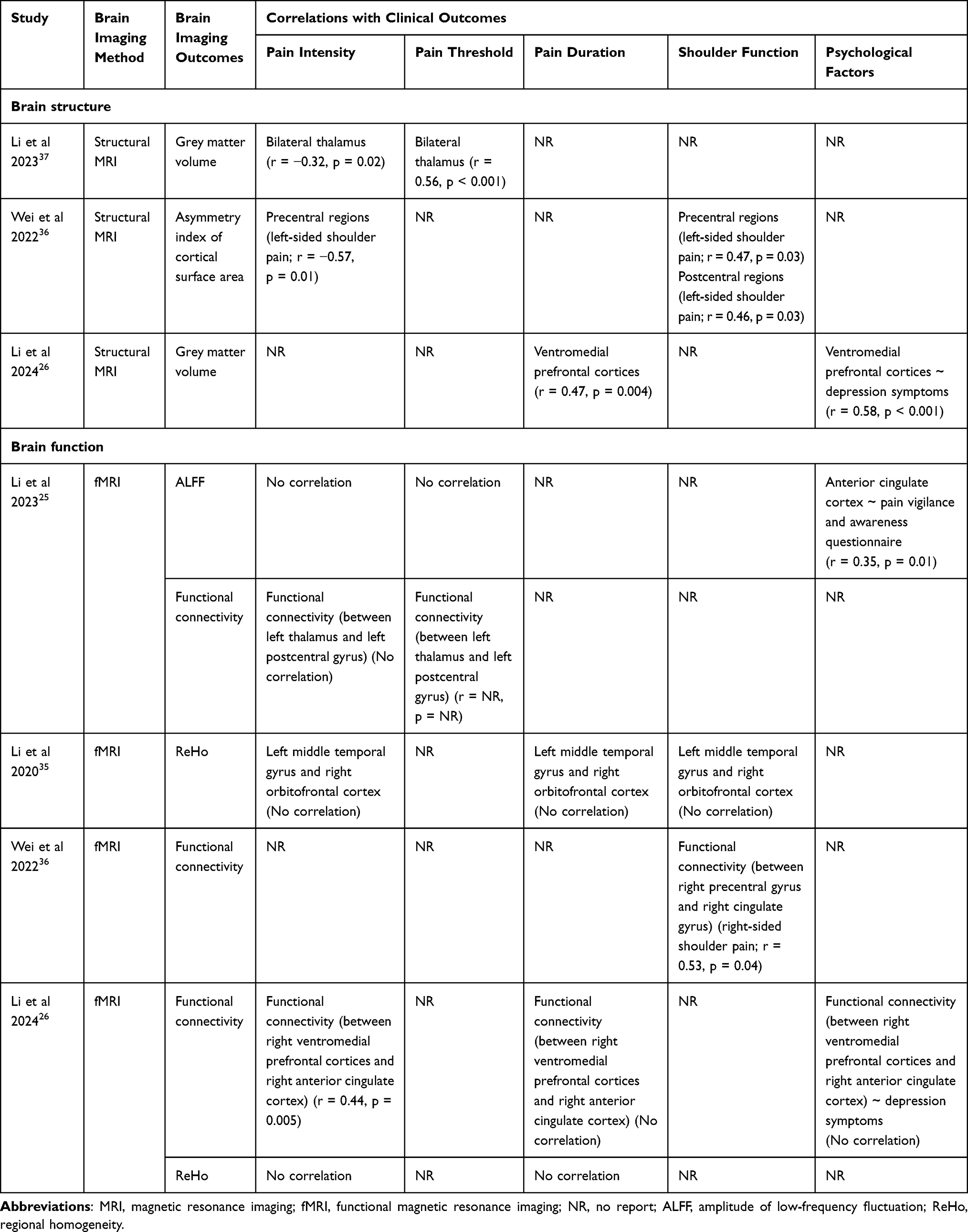 |
Table 4 Correlations Between Brain Abnormalities and Clinical Outcomes |
Pain Threshold
There was only one study reporting that lower pain thresholds were related to a smaller grey matter volume of the bilateral thalamus in people with SP (r = 0.56, p < 0.001)25 and associated with functional connectivity between the left thalamus and left postcentral gyrus (not reporting the direction of the association),25 without correction for multiple comparisons in the correlation analyses. The certainty of evidence was very low.
Pain Duration
One structural MRI study revealed that longer pain duration was correlated with greater grey matter volume in the ventromedial prefrontal cortices (r = 0.47, p = 0.004).26 However, the certainty of evidence was also very low.
Shoulder Function
Very low-certainty evidence from one MRI study showed that36 poorer shoulder function of individuals with left SP was correlated with a smaller asymmetry index of the cortical surface area in the precentral (r = 0.47, p = 0.03) and postcentral cortex (r = 0.46, p = 0.03). Additionally, functional MRI analyses demonstrated worse shoulder function of individuals with right SP was associated with lower functional connectivity linking the right precentral gyrus and right cingulate gyrus (r = 0.53, p = 0.04).36 However, the risk of false-positive findings was increased due to the lack of correction for multiple comparisons and the certainty of evidence was very low.
Psychological Factors
Two included studies found brain structural and functional abnormalities were related to psychological factors, such as depressive symptoms,26 and pain vigilance and awareness.25 Greater grey matter volume in the ventromedial prefrontal cortices was associated with more severe depressive symptoms (r = 0.58, p < 0.001).26 More severe pain vigilance and awareness was reported to be correlated with greater ALFF within the anterior cingulate cortex (r = 0.35, p = 0.01) without correction for multiple comparisons.25 Again, the certainty of evidence was very low.
Discussion
This systematic review was the first to synthesize evidence regarding brain abnormalities in individuals with SP compared to healthy controls. The overall certainty of evidence was rated as very low due to the small number and heterogeneity of studies. Very low-certainty evidence suggests possible structural and functional alterations in brain regions responsible for pain processing, emotional regulation, and sensorimotor integration compared with healthy controls. These brain abnormalities may be associated with higher pain intensity, lower pain threshold, longer pain duration, as well as poor shoulder function and psychological outcomes.
Pain Processing
This review found that individuals with SP have less grey matter in the thalamus compared to healthy controls,25,37 which is correlated with higher pain intensity and lower pain thresholds (uncorrected for multiple comparison, with increased risk of false positives).25 Additionally, greater spontaneous activity of thalamus and functional connectivity between postcentral cortex and thalamus have been observed in individuals with SP.25 The thalamus serves as an important relay station of nociceptive signal transmission, integrating sensory input and regulating pain perception.42 Overactivation of the thalamus may lead to excitatory toxicity and subsequent atrophy.25,43,44 Therefore, the observed smaller thalamic grey matter in those with SP raises the possibility of maladaptive plasticity resulting from shoulder nociceptive inputs.45 These structural abnormalities may disrupt the role of thalamus in modulating sensory signals, which leads to the amplification of pain signals and contributes to central sensitization.46,47 Indeed, central sensitization has been identified in individuals with SP,9 which may involve the maladaptive plasticity of the thalamus. These findings raise the possibility that the thalamus could be a potential treatment target in future neuromodulation studies.
Although these abnormalities in the thalamus are relatively consistent across two MRI studies,25,37 one study measured grey matter volume (Li et al 2023)25 and the other measured grey matter density (Conboy et al 2021).37 Therefore, the certainty of evidence remains very low, given the heterogenous methodologies, small sample sizes, and the cross-sectional study design. Further high-quality, prospective MRI studies with larger sample sizes and long follow-up are needed to confirm the causal relationships between the thalamic abnormalities and clinical outcomes of SP, as well as its role and potential as a biomarker and therapeutic target.
The findings of the thalamic abnormalities are consistent with previous systematic reviews reporting lower grey matter volume of the thalamus in individuals with complex regional pain syndrome48 and low back pain.49 In contrast, greater thalamus grey matter volume has been observed in individuals with temporomandibular pain.50 These differences may be due to the specific locations of pain, supporting the previous observation that pain-related brain abnormalities are location-specific.51
Emotional Regulation
Functional MRI studies may indicate functional reorganization in brain regions involved in the emotional and cognitive dimensions of pain in individuals with SP. Specifically, this review identified functional abnormalities in the cingulate cortex, including greater spontaneous activity;25 greater functional connectivity with the ventromedial prefrontal cortex;26 and enhanced functional connectivity with precentral and postcentral gyrus.36 The cingulate cortex is a key region mediating the affective-motivational and cognitive-evaluative components of pain experience, and it plays an essential role in encoding the emotional distress of pain.52–54 Overactivation of the cingulate cortex may amplify the perceived threat of pain, driving catastrophic cognition and avoidance behaviour towards pain.52,55 This is consistent with the observed correlations between anterior cingulate cortex activity and pain vigilance and awareness in the individuals with SP (uncorrected for multiple comparison, with increased risk of false positives).25 The activation of the cingulate cortex has been observed across various musculoskeletal pain conditions, including low back pain56,57 and fibromyalgia.58
Structural and functional abnormalities were also reported in the ventromedial prefrontal cortex, orbitofrontal cortex, and amygdala,26,35 which are the brain regions responsible for emotion regulation in pain conditions.59,60 Interestingly, longer pain duration and more severe depressive symptoms appeared to be correlated with greater grey matter volume in the ventromedial prefrontal cortices of individuals with SP,26 which seemed to contradict the finding of lower grey matter volume of the ventromedial prefrontal cortices in those with SP compared with healthy controls.26 Ventromedial prefrontal cortices are also involved in descending antinociceptive pathways.61 Antinociceptive compensatory reorganization of the brain was found in response to nociceptive stimulation,62 indicating the possibility that such compensation may mitigate the grey matter volume reduction of ventromedial prefrontal cortices within the SP group, although the overall grey matter volume in the SP group was lower than healthy controls. However, more studies are warranted to clarify this.
These results should be interpreted with considerable caution given the small number of studies, heterogenous methodologies, cross-sectional study design, and very low certainty of evidence. These findings raise the possibility that addressing emotional problems may be beneficial in SP management, such as mindfulness and cognitive behavioral therapy.63–65 However, whether these interventions can modulate these brain regions and improve outcomes in individuals with SP remains to be investigated in future high-quality studies.
Sensorimotor Integration
This review found structural and functional reorganization within the sensorimotor networks of individuals with SP, although the certainty of evidence is very low.25,36,37 Studies have reported greater functional connectivity between the sensorimotor cortex and both the thalamus and cingulate cortices,25,36 as well as lower grey matter density in the postcentral cortex and temporal-parietal junction.37 Importantly, abnormalities in the structure and function of the sensorimotor cortex appeared to be associated with impaired shoulder function (uncorrected for multiple comparison, with increased risk of false positives).36 Similar reviews in other pain conditions reported evidence for grey matter abnormalities in the postcentral gyrus of those with low back pain57 and abnormal motor cortex function in those with temporomandibular pain.50 Abnormalities in these brain regions, which are responsible for multisensory integration and motor planning, may support the sensorimotor impairments observed in individuals with SP.66 Conboy et al 2021 also used behavioural testing conducted to demonstrate the sensory integration impairment and disruption of movement perception in individuals with SP.37 Individuals with SP are found to modify their movement patterns and avoid pain-provoking activities due to fear-avoidance belief.67,68 Evidence indicates that immobilization can lead to cortical reorganization,69–71 supporting the hypothesis that maladaptive abnormalities in sensorimotor networks may reflect cortical plasticity in response to a pain-induced protective movement strategy.
These observations should be viewed as hypothesis-generating, due to limited number of studies, cross-sectional study design, and methodological heterogeneity. These results may suggest that maladaptive changes in sensorimotor networks might correlate to functional impairment in those with SP. They could provide a theoretical rationale for exploring whether interventions targeting sensorimotor reorganization, such as graded motor imagery,72 could be beneficial in individuals with SP.
Limitations and Future Research
This study has several limitations. Firstly, there are only five included studies with potentially overlapping cohorts and small sample sizes, and most identified abnormalities in the various brain regions were only reported by a single study. Therefore, the generalizability of these results was limited, and should be interpreted with caution. Secondly, there was significant heterogeneity in the analytical metrics (such as voxel-based morphometry and surface morphology) and patient populations (such as rotator cuff tears, adhesive capsulitis, and SP without specified diagnosis) of the included studies, which precluded direct results comparisons across these studies. The clinical heterogeneity limits the generalizability of our findings to the entire SP population. Future work should prioritize standardizing imaging protocols and data analysis frameworks to enable comparisons across studies. Thirdly, dominant hand and symptom duration of included participants were not reported in some studies. These variables are related to interpreting potential lateralization effects and the influence of pain chronicity on brain changes. Future studies should prioritize standardized reporting of these characteristics to enable comparisons. Fourthly, three included studies did not use correction for multiple comparisons in clinical correlation analysis, thereby increasing the risk of false positives. Consequently, the observed associations between brain alterations and clinical outcomes should be regarded as hypothesis-generating rather than definitive. Fifthly, all included studies used a cross-sectional design, which prevents the determination of causal association between brain abnormalities and pain. It remains unclear whether the observed neural abnormalities in individuals with SP are the cause or results of pain. Therefore, the translational implications of MRI findings require cautious interpretation. Future large-sample prospective studies are needed to clarify the causal relationship between neural abnormalities and pain progression.
Conclusions
Very low-certainty evidence suggests that SP may be associated with structural and functional brain abnormalities in regions involved in pain processing, emotional regulation, and sensorimotor integration. These abnormalities appeared to correlate with pain intensity, pain threshold, pain duration, shoulder function, and psychological outcomes. However, given the methodological heterogeneity, small sample sizes, and the cross-sectional design of the included studies, these findings should be considered preliminary and hypothesis-generating. The causal association and clinical translational potential of these results remain to be clarified. The findings suggest a potential rationale for future high-quality longitudinal and interventional studies to confirm these observations and to explore whether targeting neuroplasticity (such as targeting the thalamus) could be beneficial in SP management.
Funding
The work described in this paper was fully supported by a grant from the Research Grants Council of the Hong Kong Special Administrative Region, China (RGC Project No: 24122024).
Disclosure
All authors have no conflicts of interest to declare.
References
1. Lucas J, van Doorn P, Hegedus E, Lewis J, Van der Windt D. A systematic review of the global prevalence and incidence of shoulder pain. BMC Musculoskelet Disord. 2022;23(1):1073. doi:10.1186/s12891-022-05973-8
2. Gray M, Wallace A, Aldridge S. Assessment of shoulder pain for non-specialists. BMJ. 2016;355:i5783. doi:10.1136/bmj.i5783
3. Ottenheijm RPG, Joore MA, Walenkamp GHIM, et al. The maastricht ultrasound shoulder pain trial (MUST): ultrasound imaging as a diagnostic triage tool to improve management of patients with non-chronic shoulder pain in primary care. BMC Musculoskelet Disord. 2011;12:154. doi:10.1186/1471-2474-12-154
4. Hodgetts C, Walker B. Epidemiology, common diagnoses, treatments and prognosis of shoulder pain: a narrative review. Int J Osteopath Med. 2021;42:11–14. doi:10.1016/j.ijosm.2021.10.006
5. Crookes T, Wall C, Byrnes J, Johnson T, Gill D. Chronic shoulder pain. Aust J Gen Pract. 2023;52(11):753–758. doi:10.31128/AJGP-04-23-6790
6. Ackerman IN, Fotis K, Pearson L, et al. Impaired health-related quality of life, psychological distress, and productivity loss in younger people with persistent shoulder pain: a cross-sectional analysis. Disabil Rehabil. 2022;44(15):3785–3794. doi:10.1080/09638288.2021.1887376
7. Alaiti RK, Caneiro JP, Gasparin JT, et al. Shoulder pain across more movements is not related to more rotator cuff tendon findings in people with chronic shoulder pain diagnosed with subacromial pain syndrome. Pain Rep. 2021;6(4):e980. doi:10.1097/PR9.0000000000000980
8. Unruh KP, Kuhn JE, Sanders R, et al. The duration of symptoms does not correlate with rotator cuff tear severity or other patient-related features: a cross-sectional study of patients with atraumatic, full-thickness rotator cuff tears. J Shoulder Elbow Surg. 2014;23(7):1052–1058. doi:10.1016/j.jse.2013.10.001
9. Sanchis MN, Lluch E, Nijs J, Struyf F, Kangasperko M. The role of central sensitization in shoulder pain: a systematic literature review. Semin Arthritis Rheum. 2015;44(6):710–716. doi:10.1016/j.semarthrit.2014.11.002
10. Noten S, Struyf F, Lluch E, D’Hoore M, Van Looveren E, Meeus M. Central pain processing in patients with shoulder pain: a review of the literature. Pain Pr. 2017;17(2):267–280. doi:10.1111/papr.12502
11. Martucci KT, Mackey SC. Neuroimaging of pain: human evidence and clinical relevance of central nervous system processes and modulation. Anesthesiology. 2018;128(6):1241–1254. doi:10.1097/ALN.0000000000002137
12. Schmidt-Wilcke T. Neuroimaging of chronic pain. Best Pract Res Clin Rheumatol. 2015;29(1):29–41. doi:10.1016/j.berh.2015.04.030
13. Luo J, Zhu HQ, Gou B, Wang XQ. Neuroimaging assessment of pain. Neurotherapeutics. 2022;19(5):1467–1488. doi:10.1007/s13311-022-01274-z
14. Heukamp NJ, Moliadze V, Mišić M, et al. Beyond the chronic pain stage: default mode network perturbation depends on years lived with back pain. Pain. 2025;166(1):160–170. doi:10.1097/j.pain.0000000000003335
15. Zhou Z, Hui ES, Kranz GS, et al. Potential mechanisms underlying the accelerated cognitive decline in people with chronic low back pain: a scoping review. Ageing Res Rev. 2022;82:101767. doi:10.1016/j.arr.2022.101767
16. Ni X, Zhang J, Sun M, et al. Abnormal dynamics of functional connectivity density associated with chronic neck pain. Front Mol Neurosci. 2022;15:880228. doi:10.3389/fnmol.2022.880228
17. Iwabuchi SJ, Drabek MM, Cottam WJ, et al. Medio-dorsal thalamic dysconnectivity in chronic knee pain: a possible mechanism for negative affect and pain comorbidity. Eur J Neurosci. 2023;57(2):373–387. doi:10.1111/ejn.15880
18. Murillo C, López-Sola M, Cagnie B, et al. Gray matter adaptations to chronic pain in people with whiplash-associated disorders are partially reversed after treatment: a Voxel-Based Morphometry Study. J Pain. 2024;25(6):104471. doi:10.1016/j.jpain.2024.01.336
19. Asada M, Shibata M, Hirabayashi N, et al. Association between chronic low back pain and regional brain atrophy in a Japanese older population: the Hisayama Study. Pain. 2022;163(11):2185–2193. doi:10.1097/j.pain.0000000000002612
20. Sanchis-Alfonso V, Beser-Robles M, Ten-Esteve A, et al. Brain network functional connectivity changes in patients with anterior knee pain: a resting-state fMRI exploratory study. Eur Radiol Exp. 2023;7(1):60. doi:10.1186/s41747-023-00378-1
21. De Zoete RMJ, McMahon KL, Coombes JS, Sterling M. The effects of physical exercise on structural, functional, and biochemical brain characteristics in individuals with chronic whiplash-associated disorder: a pilot randomized clinical trial. Pain Pract. 2023;23(7):759–775. doi:10.1111/papr.13240
22. Zhang S, Zhang G, Bao S, et al. Resting-State functional connectivity of the cerebellum in patients with chronic low back pain. Am J Phys Med Rehabil. 2024. doi:10.1097/PHM.0000000000002583
23. Lindsay N, Chen C, Gilam G, Mackey S, Scherrer G. Brain circuits for pain and its treatment. Sci Transl Med. 2021;13(619):eabj7360. doi:10.1126/scitranslmed.abj7360
24. Coppieters I, Meeus M, Kregel J, et al. Relations between brain alterations and clinical pain measures in chronic musculoskeletal pain: a systematic review. J Pain. 2016;17(9):949–962. doi:10.1016/j.jpain.2016.04.005
25. Li T, Li J, Zhao R, Zhou J, Chu X. Deficits in the thalamocortical pathway associated with hypersensitivity to pain in patients with frozen shoulder. Front Neurol. 2023;14:1180873. doi:10.3389/fneur.2023.1180873
26. Li J, Zhao R, Wang C, et al. Structural and functional abnormalities in the medial prefrontal cortex were associated with pain and depressive symptoms in patients with adhesive capsulitis. Pain Rep. 2024;9(2):e1139. doi:10.1097/PR9.0000000000001139
27. Zhang LB, Chen YX, Li ZJ, et al. Advances and challenges in neuroimaging-based pain biomarkers. Cell Rep Med. 2024;5(10):101784. doi:10.1016/j.xcrm.2024.101784
28. Lowry V, Lavigne P, Zidarov D, Matifat E, Cormier AA, Desmeules F. A systematic review of clinical practice guidelines on the diagnosis and management of various shoulder disorders. Arch Phys Med Rehabil. 2024;105(2):411–426. doi:10.1016/j.apmr.2023.09.022
29. Dowell D. CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recomm Rep. 2022;71. doi:10.15585/mmwr.rr7103a1
30. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: Systematic Reviews of Etiology and Risk. JBI; 2020.
31. Maricot A, Dick E, Walravens A, et al. Brain neuroplasticity related to lateral ankle ligamentous injuries: a systematic review. Sports Med. 2023;53(7):1423–1443. doi:10.1007/s40279-023-01834-z
32. Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, Luque-Suarez A. Pain-Related fear, pain intensity and function in individuals with chronic musculoskeletal pain: a systematic review and meta-analysis. J Pain. 2019;20(12):1394–1415. doi:10.1016/j.jpain.2019.04.009
33. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
34. Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines 6. Rating the quality of evidence—imprecision. J Clin Epidemiol. 2011;64(12):1283–1293. doi:10.1016/j.jclinepi.2011.01.012
35. Li JL, Yan CQ, Wang X, et al. Brain functional alternations of the pain-related emotional and cognitive regions in patients with chronic shoulder pain. J Pain Res. 2020;13:575–583. doi:10.2147/jpr.S220370
36. Wei X, Shi G, Tu J, et al. Structural and functional asymmetry in precentral and postcentral gyrus in patients with unilateral chronic shoulder pain. Front Neurol. 2022;13:792695. doi:10.3389/fneur.2022.792695
37. Conboy V, Edwards C, Ainsworth R, et al. Chronic musculoskeletal impairment is associated with alterations in brain regions responsible for the production and perception of movement. J Physiol. 2021;599(8):2255–2272. doi:10.1113/jp281273
38. Zhang J, Tian L, Zhang L, et al. Relationship between white matter integrity and post-traumatic cognitive deficits: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2019;90(1). doi:10.1136/jnnp-2017-317691
39. T D, W R, Gj W, Nd V. Functional connectivity and brain activation: a synergistic approach. Cereb Cortex. 2014;24(10). doi:10.1093/cercor/bht119
40. Jiang L, Zuo XN. Regional homogeneity: a multimodal, multiscale neuroimaging marker of the human connectome. Neurosci Rev J. 2016;22(5):486–505. doi:10.1177/1073858415595004
41. Zou QH, Zhu CZ, Yang Y, et al. An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: fractional ALFF. J Neurosci Methods. 2008;172(1):137–141. doi:10.1016/j.jneumeth.2008.04.012
42. Yen CT, Lu PL. Thalamus and pain. Acta Anaesthesiol Taiwan. 2013;51(2):73–80. doi:10.1016/j.aat.2013.06.011
43. Silberstein SD. Neurotoxins in the neurobiology of pain. Headache J Head Face Pain. 2003;43(s1):2–8. doi:10.1046/j.1526-4610.43.7s.2.x
44. Feraco P, Bacci A, Pedrabissi F, et al. Metabolic abnormalities in pain-processing regions of patients with fibromyalgia: a 3T MR spectroscopy study. AJNR Am J Neuroradiol. 2011;32(9):1585–1590. doi:10.3174/ajnr.A2550
45. Kuner R, Flor H. Structural plasticity and reorganisation in chronic pain. Nat Rev Neurosci. 2017;18(1):20–30. doi:10.1038/nrn.2016.162
46. Apkarian AV, Sosa Y, Sonty S, et al. Chronic back pain is associated with decreased prefrontal and thalamic gray matter density. J Neurosci. 2004;24(46):10410–10415. doi:10.1523/JNEUROSCI.2541-04.2004
47. Domin M, Strauss S, McAuley JH, Lotze M. Complex regional pain syndrome: thalamic GMV atrophy and associations of lower GMV with clinical and sensorimotor performance data. Front Neurol. 2021;12. doi:10.3389/fneur.2021.722334
48. Ma T, Li ZY, Yu Y, et al. Gray matter abnormalities in patients with complex regional pain syndrome: a systematic review and meta-analysis of voxel-based morphometry studies. Brain Sci. 2022;12(8):1115. doi:10.3390/brainsci12081115
49. Ng SK, Urquhart DM, Fitzgerald PB, Cicuttini FM, Hussain SM, Fitzgibbon BM. The relationship between structural and functional brain changes and altered emotion and cognition in chronic low back pain brain changes: a systematic review of MRI and fMRI studies. Clin J Pain. 2018;34(3):237–261. doi:10.1097/AJP.0000000000000534
50. Yin Y, He S, Xu J, et al. The neuro-pathophysiology of temporomandibular disorders-related pain: a systematic review of structural and functional MRI studies. J Headache Pain. 2020;21(1):78. doi:10.1186/s10194-020-01131-4
51. Zaki J, Wager TD, Singer T, Keysers C, Gazzola V. The anatomy of suffering: understanding the relationship between nociceptive and empathic pain. Trends Cognit Sci. 2016;20(4):249–259. doi:10.1016/j.tics.2016.02.003
52. Jee HJ, Zhu E, Sun M, Liu W, Zhang Q, Wang J. Anterior cingulate cortex regulates pain catastrophizing-like behaviors in rats. Mol Brain. 2023;16(1):71. doi:10.1186/s13041-023-01060-8
53. Lee J, Protsenko E, Lazaridou A, et al. Encoding of self-referential pain catastrophizing in the posterior cingulate cortex in fibromyalgia. Arthritis Rheumatol. 2018;70(8):1308–1318. doi:10.1002/art.40507
54. Vogt BA. Pain and emotion interactions in subregions of the cingulate gyrus. Nat Rev Neurosci. 2005;6(7):533–544. doi:10.1038/nrn1704
55. Haythornthwaite JA, Campbell CM, Edwards RR. When thinking about pain contributes to suffering: the example of pain catastrophizing. PAIN. 2024;165(11S):S68. doi:10.1097/j.pain.0000000000003372
56. Hazra S, Handa G, Nayak P, Sahu S, Sarkar K, Venkataraman S. A dysfunctional descending pain modulation system in chronic nonspecific low back pain: a systematic review and ALE Meta-Analysis. Neurol India. 2022;70(4):1344–1360. doi:10.4103/0028-3886.355137
57. Kregel J, Meeus M, Malfliet A, et al. Structural and functional brain abnormalities in chronic low back pain: a systematic review. Semin Arthritis Rheum. 2015;45(2):229–237. doi:10.1016/j.semarthrit.2015.05.002
58. Cagnie B, Coppieters I, Denecker S, Six J, Danneels L, Meeus M. Central sensitization in fibromyalgia? A systematic review on structural and functional brain MRI. Semin Arthritis Rheum. 2014;44(1):68–75. doi:10.1016/j.semarthrit.2014.01.001
59. Yang S, Chang MC. Chronic pain: structural and functional changes in brain structures and associated negative affective states. Int J Mol Sci. 2019;20(13):13. doi:10.3390/ijms20133130
60. Hashmi JA, Baliki MN, Huang L, et al. Shape shifting pain: chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain J Neurol. 2013;136(Pt 9):2751–2768. doi:10.1093/brain/awt211
61. Huang J, Gadotti VM, Chen L, et al. A neuronal circuit for activating descending modulation of neuropathic pain. Nat Neurosci. 2019;22(10):1659–1668. doi:10.1038/s41593-019-0481-5
62. Russo A, Tessitore A, Esposito F, et al. Pain processing in patients with migraine: an event-related fMRI study during trigeminal nociceptive stimulation. J Neurol. 2012;259(9):1903–1912. doi:10.1007/s00415-012-6438-1
63. Dahlke LAM, Sable JJ, Andrasik F. Behavioral therapy: emotion and pain, a common anatomical background. Neurol Sci. 2017;38(1):157–161. doi:10.1007/s10072-017-2928-3
64. Lee J, Lazaridou A, Paschali M, et al. A randomized controlled neuroimaging trial of cognitive behavioral therapy for fibromyalgia pain. Arthritis Rheumatol. 2024;76(1):130–140. doi:10.1002/art.42672
65. Ploesser M, Martin D. Mechanism of action of mindfulness-based interventions for pain Relief-A systematic review. J Integr Complement Med. 2024;30(12):1162–1178. doi:10.1089/jicm.2023.0328
66. Ceylan İ, Canlı M, Kuzu Ş, Alkan H, Özüdoğru A. Predictors of balance in individuals with adhesive capsulitis: a cross-sectional study. J Occup Ther Rehabil. 2024;12(2):97–104. doi:10.30720/ered.1328675
67. Lethem J, Slade PD, Troup JD, Bentley G. Outline of a fear-avoidance model of exaggerated pain perception--I. Behav Res Ther. 1983;21(4):401–408. doi:10.1016/0005-7967(83)90009-8
68. Chung YC, Chen CY, Chang CM, et al. Altered corticospinal excitability of scapular muscles in individuals with shoulder impingement syndrome. PLoS One. 2022;17(5):1–12. doi:10.1371/journal.pone.0268533
69. Clouette J, Potvin-Desrochers A, Seo F, Churchward-Venne TA, Paquette C. Reorganization of brain resting-state functional connectivity following 14 days of elbow immobilization in young females. Neuroscience. 2024;540:77–86. doi:10.1016/j.neuroscience.2024.01.005
70. Karumattu Manattu A, Borrell JA, Copeland C, Fraser K, Zuniga JM. Motor cortical functional connectivity changes due to short-term immobilization of upper limb: an fNIRS case report. Front Rehabil Sci. 2023;4:1156940. doi:10.3389/fresc.2023.1156940
71. Fortuna M, Teixeira S, Machado S, et al. Cortical reorganization after hand immobilization: the beta qEEG spectral coherence evidences. PLoS One. 2013;8(11):e79912. doi:10.1371/journal.pone.0079912
72. Flor H, Diers M. Sensorimotor training and cortical reorganization. NeuroRehabilitation. 2009;25(1):19–27. doi:10.3233/NRE-2009-0496
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acupuncture for Persistent Asthma: Protocol for a Randomized, Sham-Controlled Trial with Neuroimaging
Mao Y, Zhang P, Tian Z, Huang L, Yu S, He Z, Luo Z, Chen Z, Zhao R, Dong X, Gao J, Zeng F
Journal of Asthma and Allergy 2026, 19:615234
Published Date: 3 June 2026