Back to Journals » Journal of Asthma and Allergy » Volume 19
Acupuncture for Persistent Asthma: Protocol for a Randomized, Sham-Controlled Trial with Neuroimaging
Authors Mao Y, Zhang P, Tian Z, Huang L, Yu S, He Z, Luo Z, Chen Z, Zhao R, Dong X, Gao J ![]() , Zeng F
, Zeng F
Received 8 April 2026
Accepted for publication 20 May 2026
Published 3 June 2026 Volume 2026:19 615234
DOI https://doi.org/10.2147/JAA.S615234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Yangke Mao,1– 3,* Pan Zhang,4,* Zilei Tian,1– 3,* Ling Huang,5 Siyi Yu,1– 3 Zhaoxuan He,1– 3 Zaiyi Luo,1– 3 Ziyi Chen,1– 3 Ruyi Zhao,6 Xiaohui Dong,6 Jing Gao,6 Fang Zeng1– 3
1Acupuncture and Tuina School, Chengdu University of Traditional Chinese Medicine, Chengdu, 610075, People’s Republic of China; 2Acupuncture and Brain Science Research Center, Chengdu University of Traditional Chinese Medicine, Chengdu, 610075, People’s Republic of China; 3Key Laboratory of Acupuncture for Senile Disease (Chengdu University of TCM), Ministry of Education, Chengdu, 610075, People’s Republic of China; 4Nervous System Disease Treatment Center, Traditional Chinese Medicine Hospital of Meishan, Meishan, Sichuan, 620032, People’s Republic of China; 5Department of Respiratory and Critical Care Medicine, Chengdu Fifth People’s Hospital, Chengdu University of Traditional Chinese Medicine, Chengdu, 611130, People’s Republic of China; 6School of Nursing, Chengdu University of Traditional Chinese Medicine, Chengdu, 610075, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohui Dong, School of Nursing, Chengdu University of Traditional Chinese Medicine, Chengdu, 610075, People’s Republic of China, Email [email protected] Jing Gao, School of Nursing, Chengdu University of Traditional Chinese Medicine, Chengdu, 610075, People’s Republic of China, Email [email protected]
Background: Although acupuncture has shown therapeutic potential for asthma, its clinical application is limited by insufficient high-quality evidence and an incomplete understanding of its neurophysiological mechanisms. This study aims to evaluate the efficacy and safety of acupuncture in patients with persistent asthma and to further investigate its central mechanisms.
Methods: This randomized, sham-controlled neuroimaging trial will enroll 72 patients with mild-to-moderate persistent asthma. Participants will be randomly assigned in a 1:1 ratio to receive either genuine or sham acupuncture. The intervention comprises 12 sessions over 4 weeks. The primary outcome is the change in the Asthma Control Test score from baseline to week 4. Secondary outcomes encompass scores from the Asthma Quality of Life Questionnaire, Self-Rating Anxiety Scale, Self-Rating Depression Scale, Pittsburgh Sleep Quality Index, Montreal Cognitive Assessment, along with forced expiratory volume in 1 second and fractional exhaled nitric oxide levels. Cerebral changes will be assessed via magnetic resonance imaging conducted before and after the treatment course. Statistical analyses will adhere to the intention-to-treat principle and will employ analysis of covariance and linear mixed-effects models. Furthermore, correlation and mediation analyses will be performed to investigate the relationships between clinical improvements and neuroimaging data, thereby exploring potential neurobiological mechanisms of acupuncture.
Discussion: This randomized controlled trial aims to evaluate the clinical efficacy and central neural mechanisms of acupuncture in patients with persistent asthma. The findings are expected to provide evidence supporting its therapeutic role. By elucidating the underlying neuroregulatory mechanisms, this study may contribute to a more mechanism-informed and optimized application of acupuncture in asthma management.
Trial Registration: This trial is registered on the International Traditional Medicine Clinical Trial Registry (http://itmctr.ccebtcm.org.cn/) on April 2025 (ITMCTR2025000737).
Keywords: asthma, acupuncture, magnetic resonance imaging, neuroimaging, randomized controlled trial
Introduction
Asthma is a chronic inflammatory airway disorder characterized by bronchial hyperresponsiveness and recurrent symptoms such as wheezing, chest tightness, cough, and dyspnea.1 It affects approximately 300 million individuals worldwide, with a prevalence ranging from 4.1% to 32% across populations.2,3 Despite advances in pharmacological therapy, a substantial proportion of patients remain inadequately controlled, and approximately 40% experience persistent symptoms requiring long-term management.4 Poor asthma control is associated with impaired quality of life (QoL) and increased risks of disease progression, disability, and mortality.5 Current guidelines from the Global Initiative for Asthma (GINA) and European Respiratory Society/American Thoracic Society emphasize the goal of asthma treatment is to achieve total control or well-controlled asthma symptoms, including minimization of adverse outcomes risk and symptom burden.6,7 However, although inhaled corticosteroids combined with long-acting β2-agonists are effective, long-term use may be associated with adverse effects and does not fully address unmet clinical needs.8,9 Therefore, adjunctive non-pharmacological interventions are increasingly being explored.
Acupuncture, a key component of traditional Chinese medicine, has demonstrated potential benefits in respiratory conditions such as allergic rhinitis and chronic obstructive pulmonary disease (COPD).10,11 Emerging evidence suggests that acupuncture may improve asthma symptoms and QoL.12 However, current evidence remains inconclusive because previous acupuncture studies in asthma have often been limited by small sample sizes, insufficiently justified sample size calculations, heterogeneous intervention protocols, and reliance on patient-reported outcomes. In addition, few studies have incorporated objective physiological measures or mechanistic assessments, which limits the interpretation of both clinical efficacy and underlying biological pathways.13–15 Meanwhile, the underlying therapeutic mechanism has not been fully elucidated, thus limiting further application and promotion of acupuncture.
Although asthma has traditionally been regarded as a peripheral inflammatory airway disease, emerging evidence highlights the role of the lung–brain axis in its pathophysiology. Recent studies have demonstrated that asthma is associated with structural and functional alterations in the brain that correlate with disease severity and airway inflammation.16,17 Furthermore, neural regulation has become an increasingly important therapeutic target, as reflected by the use of interventions such as anticholinergic agents and non-invasive vagus nerve stimulation.18 The autonomic nervous system contributes to the regulation of bronchial smooth muscle tone, airway sensory perception, and neuroimmune interactions within the airway. Dysregulated afferent and efferent signaling between the airways and central nervous system may therefore amplify symptom perception and inflammatory responses. This provides a biological rationale for considering the brain and related neural circuits as potential therapeutic targets in asthma. Previous neuroimaging studies of acupuncture have shown that acupuncture stimulation may modulate activity and functional connectivity in brain regions.19 These findings suggest that acupuncture may exert systemic therapeutic effects partly through central modulation rather than through purely peripheral mechanisms. However, whether such brain changes are associated with improvements in asthma control has not been sufficiently investigated. In addition, identifying neuroimaging features associated with treatment response may help generate hypotheses regarding which patients are more likely to benefit from adjunctive acupuncture in future individualized asthma management.
Therefore, this randomized, sham-controlled trial incorporating neuroimaging is designed to (1) evaluate the efficacy and safety of acupuncture in patients with persistent asthma and (2) investigate its potential central mechanisms, particularly in relation to the lung–brain axis. We hypothesize that acupuncture, when used as an adjunctive intervention to routine pharmacological treatment, will produce a clinically meaningful improvement in asthma control compared with sham acupuncture in patients with mild-to-moderate persistent asthma. We further hypothesize that these clinical improvements will be associated with acupuncture-induced changes in brain function within neural systems related to respiratory perception, autonomic regulation, and affective processing, thereby providing preliminary evidence for a lung–brain axis mechanism.
Methods
Study Design
This study is a randomized, sham-controlled, single-blind clinical trial incorporating neuroimaging. The protocol adheres to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT 2025)20 statement (see Supplementary File) and the trial will be conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT 2025)21 and the Revised Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA)22 guidelines.
The study will be conducted at the Hospital of Chengdu University of Traditional Chinese Medicine from April 2025 to June 2027. The trial consists of a 2-week baseline period, a 4-week treatment phase, and an 8-week follow-up period. A total of 72 participants with persistent asthma will be randomly assigned in a 1:1 ratio to either the acupuncture group or the sham acupuncture group.
Demographic characteristics will be collected during the enrollment and screening period (week −2). Patient-reported outcome measures (PROMs) will be evaluated at baseline (week 0), after treatment (week 4), 1st follow-up (week 8) and 2nd follow-up (week 12). Magnetic resonance imaging (MRI) scan, forced expiratory volume in 1 second (FEV1) and fractional exhaled nitric oxide (FeNO) will be performed at the baseline and the end of the treatment. Figure 1 and Table 1 provide the detailed information of the study design.
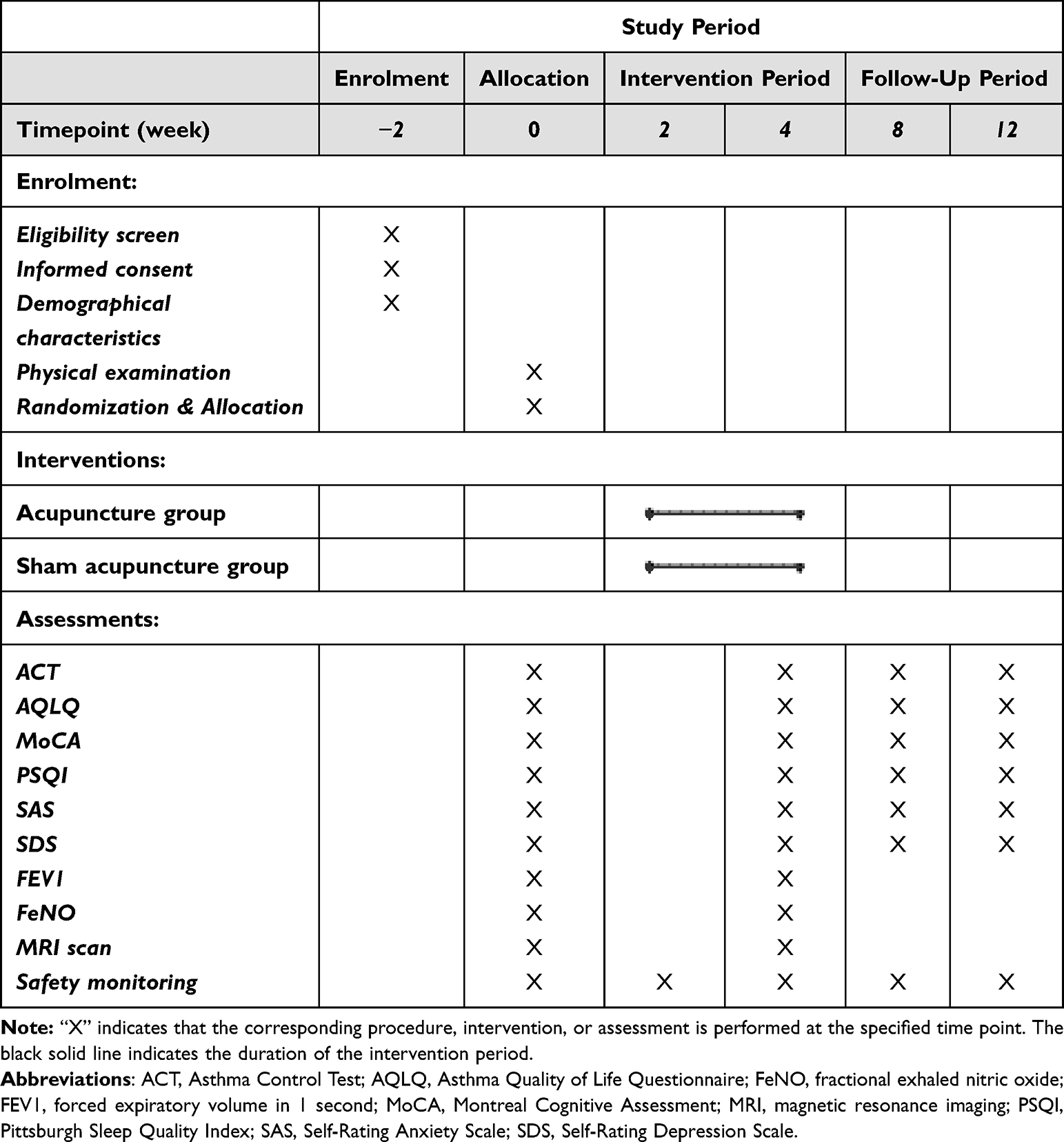 |
Table 1 Schedule of Enrolment, Interventions, and Assessments |
 |
Figure 1 Schematic diagram. Abbreviations: FEV1, forced expiratory volume in 1 second; FeNO, fractional exhaled nitric oxide; MRI, magnetic resonance imaging. |
Participants
Participants will be recruited from the outpatient department of the Hospital of Chengdu University of Traditional Chinese Medicine and from the community through advertisements and health promotion activities. Eligibility will be assessed by a respiratory specialist. All eligible participants will receive a detailed explanation of the study procedures, risks, and benefits, and written informed consent will be obtained prior to enrollment.
Inclusion Criteria
Patients will be enrolled if they fulfill all of the following criteria: (1) age from 18 to 65 years; (2) diagnosis of mild-to-moderate persistent asthma according to GINA 2024, defined by: a) a documented history of variable respiratory symptoms, including wheeze, shortness of breath, chest tightness, or cough; b) objective evidence of variable expiratory airflow limitation, such as an increase in FEV1 of >12% and >200 mL after bronchodilator administration. c) mild asthma is defined as asthma that can be controlled with low-intensity treatment, such as as-needed low-dose ICS–formoterol or low-dose ICS-containing controller therapy. Moderate asthma is defined as asthma that is well controlled with Step 3 or Step 4 treatment, such as low- or medium-dose ICS/LABA; (3) right-handedness; (4) absence of concurrent participation in other trials and no history of acupuncture therapy within the previous 30 days; (5) provision of written informed consent.
Exclusion Criteria
Patients will be excluded if they meet any of the following criteria: (1) presence of other significant respiratory diseases (eg., bronchiectasis, tuberculosis, lung abscess, or restrictive lung disease); (2) active malignancy or severe systemic diseases that may compromise safety; (3) asthma symptoms occurring exclusively after exposure to specific allergens or chemical irritants; (4) pregnancy, lactation, or planned pregnancy within the next 6 months; (5) contraindications to acupuncture (eg., local skin infection or bleeding disorders); (6) contraindications to MRI (eg., ferromagnetic implants or pacemakers).
Randomization, Allocation Concealment, and Blinding
An independent statistician will generate the randomization sequence using PASS software (version 15.0; NCSS, LLC, USA) with a 1:1 allocation ratio. Allocation concealment will be ensured using sequentially numbered, opaque, sealed envelopes prepared by an independent researcher. The allocation will be revealed only after enrollment, immediately prior to the first treatment session.
Due to the nature of the intervention, acupuncturist cannot be blinded. However, participants, outcome assessors, and data analysts will remain blinded to group allocation. To minimize potential bias, treatments will be administered in separate rooms to prevent communication between participants. To evaluate the success of participant blinding, participants will be asked after the final treatment session to guess their group allocation.
Interventions
Participants will continue their routine pharmacological treatment throughout the study. Permitted medications include maintenance therapies such as inhaled corticosteroid/long-acting β2-agonist combinations (eg., salmeterol/fluticasone or formoterol/budesonide), and salbutamol metered-dose inhaler (100 μg per puff) will be provided as rescue medication. Participants will be instructed to maintain stable medication regimens during the study. Any additional treatments will be allowed only in emergency situations and will be fully documented.
Medication use will be monitored throughout the trial. At each study visit, research staff will review the diary and verify changes in medication use. Participants will be instructed not to change their regular controller medication during the study unless clinically necessary. Any change in controller medication, rescue medication use, or additional treatment for asthma exacerbation will be documented in the case report form. Changes in maintenance therapy or frequent rescue medication use will be considered in sensitivity analyses where appropriate.
The acupuncture and sham acupuncture groups select the same acupoints including bilateral Taiyuan (LU9), Lieque (LU7), and Chize (LU5). Details of each acupoint are shown in Figure 2 and Table 2. Treatments will be administered three times per week for 4 weeks, totaling 12 sessions. All procedures will be performed by a licensed acupuncturist with at least 5 years of clinical experience and standardized training.
 |
Table 2 Locations of Acupoints |
 |
Figure 2 Locations of acupoints | LU5 (Chize), on the cubital crease, on the radial side of the tendon of biceps brachii; LU7 (Lieque), on the radial margin of the forearm, 1.5 cun above the transverse crease of the wrist, between the brachioradial muscle tendon and the long abductor muscle tendon of thumb; LU9 (Taiyuan), on the radial side of the transverse crease of the wrist, where the radial artery pulsates. |
Acupuncture Intervention
Participants will be treated in a supine position. After skin disinfection, adhesive pads will be applied to the acupoints, and sterile disposable needles (0.25 × 25 mm and 0.25 × 40 mm; Suzhou Hua Tuo Medical Instruments Co., Ltd., China) will be inserted through the pads. Needles will be inserted to depths of 5–10 mm at LU9 and LU7, and 20–30 mm at LU5 (Figure 3A). Manual stimulation will be applied using bidirectional rotation (90°–180°) combined with vertical movements (3–5 mm amplitude) at a frequency of 60–90 cycles per minute to elicit the deqi sensation (eg., soreness, numbness, distension, or heaviness). Needles will be retained for 30 minutes, with manual stimulation repeated every 10 minutes.
 |
Figure 3 Acupuncture device: (A) acupuncture; (B) sham acupuncture | a. acupuncture needle; b. blinding plastic cover; c. body skin; d. sharp needle tip; e. blunt needle tip. |
The acupoints LU9, LU7, and LU5 were selected because they are key acupoints of the Lung meridian and are commonly used for respiratory disorders in traditional acupuncture practice. The selection of these acupoints was finalized through expert consensus among licensed acupuncturists and respiratory physicians and was informed by previous clinical use of acupuncture for asthma and respiratory symptoms.
Sham Acupuncture Intervention
The sham acupuncture procedure will follow the same protocol as the acupuncture group, except that non-penetrating blunt-tipped needles will be used. These will be placed against the skin at the same acupoints to produce a minimal sensation without skin penetration (Figure 3B). The same treatment duration and procedural schedule will be maintained, but no attempt will be made to elicit the deqi sensation. Although non-penetrating sham acupuncture may not be physiologically inert, it is considered an appropriate control for reducing expectation-related and contextual effects in acupuncture trials.
Outcome Measures
Baseline demographic and clinical data will be collected prior to randomization. Outcome measures will be assessed at baseline, post-treatment, and during follow-up (weeks 8 and 12), except where otherwise specified. MRI, FEV1, and FeNO will be assessed at baseline and after treatments. An overview of all measurements is presented in Table 1.
Primary Outcome
The primary outcome is the change in the Asthma Control Test (ACT)23 score from baseline to week 4. The ACT is a validated instrument consisting of five items assessing activity limitation, shortness of breath, nocturnal symptoms, use of rescue medication, and overall asthma control. Scores range from 5 to 25, with lower scores indicating poorer asthma control.
Secondary Outcomes
The secondary outcomes include asthma-related quality of life, lung function, airway inflammation, cognitive function, sleep quality, anxiety, depression, and the durability of asthma control after treatment.
The Asthma Quality of Life Questionnaire (AQLQ)24 will be used to assess asthma-specific quality of life. It includes domains related to symptoms, activity limitation, emotional function, and environmental stimuli. Higher scores indicate better asthma-related quality of life. The AQLQ has been widely used and validated in asthma clinical studies. FEV1 will be measured by spirometry and used as an objective indicator of airway function. Higher FEV1 values indicate better expiratory airflow. FeNO will be measured as a non-invasive marker of type 2 airway inflammation, with higher values generally indicating greater eosinophilic airway inflammation. The Montreal Cognitive Assessment (MoCA)25 will be used to assess global cognitive function. Total scores range from 0 to 30, with higher scores indicating better cognitive performance. The Pittsburgh Sleep Quality Index (PSQI)26 will be used to assess sleep quality over the previous month. Total scores range from 0 to 21, with higher scores indicating poorer sleep quality. The Zung Self-rating Anxiety Scale (SAS)27 and Zung Self-rating Depression Scale (SDS)28 will be used to assess anxiety and depressive symptoms, respectively, with higher scores indicating more severe symptoms. In addition, changes in ACT score from baseline to weeks 8 and 12 will be analyzed as secondary outcomes to evaluate the persistence of treatment effects after the intervention period.
MRI Data Acquisition
MRI scans will be performed using a 3.0 Tesla Siemens scanner (Siemens, Munich, Germany). High-resolution T1-weighted images and resting-state functional MRI data will be acquired using standardized parameters at the Imaging Center of Chengdu Fifth People’s Hospital, Sichuan, China. The scanning parameters are detailed below:
- High-resolution three-dimensional T1-weighted: repetition time (TR)/echo time (TE) = 1900ms/2.26ms; voxel size = 1 × 1 × 1 mm3; matrix size = 256 × 256; and field of view (FOV) = 256 × 256 mm2.
- Resting-state functional MRI: TR/TE = 2000ms/30ms; voxel size = 3.75 × 3.75 × 5 mm3; flip angle = 90°; matrix = 64 × 64, slice thickness = 5 mm, total volume = 240 and FOV = 240 × 240 mm2.
Participants will be instructed to maintain regular routines for 24 hours before scanning and to avoid caffeine, smoking, and sleep deprivation. Before scanning, participants will rest for 30 minutes in a quiet environment. During scanning, they will be instructed to remain still, keep their eyes closed, and avoid deliberate cognitive activity.
Safety Assessment
All adverse events (AEs) will be recorded throughout the study, including their onset, duration, severity, and management. Potential AEs include subcutaneous hemorrhage, infection, and pain related to acupuncture. The relationship between AEs and the intervention will be assessed. Serious adverse events will be reported promptly to the ethics committee.
Safety outcomes will include the incidence, type, severity, duration, management, and relatedness of adverse events and serious adverse events. Safety analyses will be conducted using the safety set, defined as all randomized participants who receive at least one treatment session. Adverse events will be summarized by treatment group using frequencies and percentages. Between-group comparisons of adverse event incidence will be performed using the chi-square test or Fisher’s exact test, as appropriate. Serious adverse events and intervention-related adverse events will be described individually.
Data Management
Data will be collected and stored by independent outcomes assessor via the case report form, with subsequent entry into electronic data acquisition system. To ensure data integrity, two research associates will conduct a double check, and only principal investigators have the access to the full dataset. Following study completion, the data management will be locked up, and unable to be modified. The evidence-based medicine center of the CDUTCM is responsible for monitoring the study and data every 3 months and will make the final decision to terminate the trial.
Quality Control
To ensure study quality and reproducibility, the protocol has been reviewed by experts in acupuncture, statistics, methodology, and neuroimaging. All study personnel will receive standardized training prior to trial initiation.
Sample Size
The sample size was determined by considering both the clinical primary outcome and the neuroimaging component of the trial. For the clinical primary outcome, the primary endpoint is the between-group difference in the change in ACT score from baseline to week 4. A 3-point difference in the ACT was used as the target clinically meaningful effect.29 To adopt a conservative assumption, the pooled standard deviation was set at 4 points. With a two-sided α of 0.05 and 80% power, this calculation requires approximately 29 participants per group. For the neuroimaging component, this study is designed to explore treatment-related changes in brain function. Assuming a moderate-to-large standardized effect size of 0.75 for exploratory fMRI outcomes, with a two-sided α of 0.05 and 80% power, approximately 29 participants per group are required.30 This sample size is also consistent with methodological considerations suggesting that neuroimaging studies generally require sample sizes in the range of approximately 20–30 participants per group to improve statistical stability and reproducibility.31,32 Therefore, both the clinical endpoint calculation and the neuroimaging-based estimation support a target of approximately 29 evaluable participants per group. Thus, to account for a potential dropout rate of 20%, a total of 72 participants is planned to be recruited.
Statistical Analysis
Clinical Data Analysis
Continuous variables will be presented as mean (standard deviation) or median (interquartile range) and analyzed using independent t-tests or Mann–Whitney U-tests as appropriate. Categorical variables will be summarized as frequencies (percentages) and analyzed using chi-square or Fisher’s exact tests.
The primary outcome, defined as the change in ACT score from baseline to week 4, will be analyzed using analysis of covariance, with treatment group as the fixed factor and baseline ACT score as the covariate. Model assumptions, including linearity, normality of residuals, homogeneity of variance, and influential observations, will be assessed. If substantial violations are identified, appropriate data transformation, robust standard errors, or nonparametric sensitivity analyses will be considered, rather than replacing the primary analysis model. Longitudinal changes in repeated outcomes measured at baseline, week 4, week 8, and week 12 will be analyzed using linear mixed-effects models, with fixed effects for group, time, and group-by-time interaction and a random intercept for participants. This model will be used for secondary longitudinal analyses, including ACT changes at weeks 8 and 12 and other repeated patient-reported outcomes.
All analyses will adhere to the intention-to-treat principle. Independent statistician will conduct these analyses using either R (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria) or SPSS (version 26.0; IBM Corp., Armonk, NY, USA). A two-sided p value of <0.05 will be designated as statistically significant. For handling missing data, the multiple imputation method will be applied under the assumption that data are missing at random. Comparisons for the secondary outcomes are considered exploratory and will not be adjusted.
MRI Data Analysis
Functional MRI data will undergo preprocessing via fMRIPrep (version 1.5.3), encompassing procedures including co-registration, brain extraction, brain tissue segmentation, spatial normalization, unwarping, and skull-stripping. Subsequent to this minimal preprocessing, several analytical approaches will be implemented in MATLAB 2021b (MathWorks Inc., Natick, MA, USA) to examine the cerebral responses to acupuncture treatment. These will include calculations of the amplitude of low-frequency fluctuation, seed-based functional connectivity, large-scale functional brain network analysis, and dynamic connectivity analyses. Finally, Pearson correlation analyses will be employed to quantify the relationships between alterations in brain activity and improvements in clinical outcomes within each study group.
Relevant potential confounders, including baseline clinical characteristics, medication use, and head motion parameters in MRI analyses, will be documented and considered in sensitivity or exploratory analyses where appropriate.
Discussion
Asthma remains a major global public health challenge, characterized by substantial morbidity and a significant burden on healthcare systems. Despite the widespread use of guideline-recommended pharmacological therapies, optimal asthma control remains difficult to achieve in a considerable proportion of patients.33 Real-world evidence suggests that only a small fraction of patients achieve well-controlled asthma, highlighting persistent unmet clinical needs.34 In addition, concerns regarding long-term medication use, particularly corticosteroids, continue to affect treatment adherence and patient acceptance.35 These limitations have stimulated growing interest in complementary and integrative therapeutic approaches. The present study is designed to evaluate the efficacy and safety of acupuncture for persistent asthma using a rigorously designed randomized, sham-controlled trial, while simultaneously exploring its central mechanisms through neuroimaging. By integrating clinical outcomes with objective physiological and neuroimaging measures, this study aims to provide more comprehensive and mechanistic evidence than previous investigations.
This trial incorporates several methodological features that enhance its scientific rigor. First, the inclusion of a predefined MCID for the primary outcome strengthens both the clinical relevance and interpretability of the results.36 This approach ensures that observed effects are not only statistically significant but also clinically meaningful. The use of an MCID-based framework is intended to distinguish clinical relevance from statistical significance. The interpretation of the trial findings will consider both the estimated effect size and its clinical relevance, rather than relying solely on p values. Second, the study employs a combination of PROMs and objective physiological indicators. While the ACT and AQLQ capture patient-centered outcomes, objective measures such as FEV1 and FeNO provide complementary assessments of lung function and airway inflammation.37 This multidimensional evaluation framework improves the robustness of efficacy assessment and addresses a major limitation of previous studies that relied predominantly on subjective outcomes. Third, the integration of neuroimaging represents a key innovation. Resting-state functional MRI allows for the investigation of functional brain alterations associated with acupuncture, providing an opportunity to bridge clinical effects with underlying neural mechanisms.
A major strength of this study lies in its mechanistic framework based on the lung–brain axis. Although asthma has traditionally been conceptualized as a peripheral inflammatory airway disease, accumulating evidence indicates that central nervous system processes play a critical role in its pathophysiology. Neuroimaging studies have demonstrated structural and functional brain alterations in patients with asthma, which are associated with disease severity and symptom burden.16,17,38 In addition, neural pathways involving the brainstem, thalamus, and cortical regions contribute to the regulation of airway function and perception of respiratory symptoms.18 Acupuncture is known to exert modulatory effects on central neural networks, including regions involved in sensory processing, autonomic regulation, and emotional modulation.19 Previous studies have suggested that acupuncture can alter functional connectivity patterns and that these changes may correlate with clinical improvements.39 Therefore, it is biologically plausible that acupuncture may alleviate asthma symptoms by modulating the lung–brain axis, influencing both physiological and perceptual components of the disease. However, direct evidence linking acupuncture-induced brain changes to clinical outcomes in asthma remains limited. By combining neuroimaging with clinical assessments, this study is expected to provide novel insights into whether central modulation represents a key mechanism underlying the therapeutic effects of acupuncture. However, direct evidence linking acupuncture-induced brain changes to clinical outcomes in asthma remains limited. By combining neuroimaging with clinical assessments, this study is expected to provide novel insights into whether central modulation represents a key mechanism underlying the therapeutic effects of acupuncture.
If the findings of this study demonstrate clinically meaningful improvements in asthma control, they may support the integration of acupuncture as an adjunctive therapy in asthma management. This could be particularly relevant for patients with suboptimal control, medication intolerance, or concerns regarding long-term pharmacotherapy. Second, demonstrating a mechanistic link between acupuncture‑induced brain changes and asthma symptom control would strengthen the rationale for targeting the lung‑brain axis in respiratory medicine. Third, the identification of specific neuroimaging biomarkers may enable a precision medicine approach, helping to identify which asthma patients are most likely to benefit from acupuncture. Several limitations should be acknowledged. First, the 4-week treatment period is designed primarily to assess short-term treatment effects, and the 8-week follow-up can provide only preliminary information on durability. Asthma is a chronic disease, and longer treatment and follow-up periods may be required to determine sustained clinical efficacy. Second, neuroimaging changes observed over this timeframe should be interpreted cautiously, as some treatment-related neural adaptations may require longer periods to stabilize. Third, although the sham acupuncture procedure is designed to improve blinding and reduce specific needling effects, non-penetrating sham acupuncture may still induce sensory and contextual responses and therefore may not be completely inert.
In summary, this randomized, sham-controlled, single-blind neuroimaging trial is designed to evaluate the efficacy and safety of acupuncture as an adjunctive intervention for patients with persistent asthma and to explore potential central mechanisms related to the lung–brain axis. If the trial demonstrates clinically meaningful benefits and acceptable safety, the findings may help identify selected patient groups who could benefit from adjunctive acupuncture and may provide preliminary neuroimaging evidence to guide future mechanism-informed and individualized studies. These potential implications remain conditional on the trial results and should be confirmed in larger, multicenter studies with longer follow-up.
Trial Status
The recruitment began on April 15, 2025, and is anticipated to end on June 30, 2027.
Abbreviations
ACT, Asthma Control Test; AEs, adverse events; AQLQ, Asthma Quality of Life Questionnaire; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FeNO, fractional exhaled nitric oxide; FOV, field of view; GINA, Global Initiative for Asthma; MCID, minimal clinically important difference; MoCA, Montreal Cognitive Assessment; MRI, magnetic resonance imaging; PROMs, patient-reported outcome measures; PSQI, Pittsburgh Sleep Quality Index; QoL, quality of life; RCT, randomized controlled trial; SAS, Zung Self-rating Anxiety Scale; SDS, Zung Self-rating Depression Scale; TCM, traditional Chinese medicine.
Data Sharing Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Ethics Statement
This trial will be conducted in accordance with the Declaration of Helsinki. Research ethics approval has been obtained from the Ethics Committee of Teaching Hospital of Chengdu University of TCM (No.2024KL-188). Following a detailed discussion of the study’s potential benefits and risks, all participants will give voluntary written informed consent prior to their inclusion.
Acknowledgments
We would like to express our gratitude to all the researchers who have participated and will participate in this study.
Author Contributions
Yangke Mao: Investigation, writing-original draft preparation, writing-review & editing. Pan Zhang: Conceptualization, writing-original draft preparation. Zilei Tian: Investigation, validation. Ling Huang: Visualization, investigation. Siyi Yu: Formal analysis. Zhaoxuan He: Validation. Zaiyi Luo: Data Curation. Ziyi Chen: Validation. Ruyi Zhao: Investigation. Xiaohui Dong: Writing-review & editing, funding acquisition. Jing Gao: Project administration, writing-review & editing. Fang Zeng: Conceptualization, writing-review & editing, funding acquisition. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This current study is supported by the Young Scientists Fund of the National Natural Science Foundation of China (No.82505762), the Sichuan Natural Science Foundation Program (No.2024NSFSC1860, 2025ZNSFSC1849), TCM Special Project of Meishan Science and Technology Guidance Program (No.2024ZDYY02), and the Sichuan Province Tianfu Qingcheng Program. The funding organizations had no involvement in any aspect of the research, including its design, conduct, statistical analysis, data interpretation, or the preparation and submission of the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Melén E, Zar HJ, Siroux V, et al. Asthma inception: epidemiologic risk factors and natural history across the life course. Am J Respir Crit Care Med. 2024;210(6):737–13. doi:10.1164/rccm.202312-2249SO
2. Chinn S, Luczynska C, Jarvis D, et al. Variations in the prevalence of respiratory symptoms, self-reported asthma attacks, and use of asthma medication in the European Community Respiratory Health Survey (ECRHS). Eur Respir J. 1996;9(4):687–695. doi:10.1183/09031936.96.09040687
3. Stern J, Pier J, Litonjua AA. Asthma epidemiology and risk factors. Semin Immunopathol. 2020;42(1):5–15. doi:10.1007/s00281-020-00785-1
4. Heaney LG, Robinson DS. Severe asthma treatment: need for characterising patients. Lancet. 2005;365(9463):974–976. doi:10.1016/S0140-6736(05)71087-4
5. Xia T, Qiu H, Yu B, et al. Cost-related medication nonadherence in US adults with asthma: the national health interview survey, 2013-2020. Ann Allergy Asthma Immunol. 2023;131(5):606–613.e5. doi:10.1016/j.anai.2023.07.013
6. Menzies-Gow A, Bafadhel M, Busse WW, et al. An expert consensus framework for asthma remission as a treatment goal. J Allergy Clin Immunol. 2020;145(3):757–765. doi:10.1016/j.jaci.2019.12.006
7. Rayner DG, Ferri DM, Guyatt GH, et al. Inhaled reliever therapies for asthma: a systematic review and meta-analysis. JAMA. 2025;333(2):143–152. doi:10.1001/jama.2024.22700
8. Nwaru BI, Ekström M, Hasvold P, Wiklund F, Telg G, Janson C. Overuse of short-acting β 2 -agonists in asthma is associated with increased risk of exacerbation and mortality: a nationwide cohort study of the global SABINA programme. Eur Respir J. 2020;55(4):1901872. doi:10.1183/13993003.01872-2019
9. García-Marcos L, Chiang C-Y, Asher MI, et al. Asthma management and control in children, adolescents, and adults in 25 countries: a global asthma network Phase I cross-sectional study. Lancet Glob Health. 2023;11(2):e218–e28. doi:10.1016/S2214-109X(22)00506-X
10. Yeh GY, Horwitz R. Integrative medicine for respiratory conditions: asthma and chronic obstructive pulmonary disease. Med Clin North Am. 2017;101(5):925–941. doi:10.1016/j.mcna.2017.04.008
11. Wang L, Hu X, Geng L, et al. Multi-effective characteristics and advantages of acupuncture in COVID-19 treatment. Acupunct Herbal Med. 2023;3(2):83–95. doi:10.1097/HM9.0000000000000062
12. Chan HHL, Ng T. Traditional Chinese Medicine (TCM) and allergic diseases. Curr Allergy Asthma Rep. 2020;20(11):67. doi:10.1007/s11882-020-00959-9
13. Pai HJ, Azevedo RS, Braga ALF, et al. A randomized, controlled, crossover study in patients with mild and moderate asthma undergoing treatment with traditional Chinese acupuncture. Clinics. 2015;70(10):663–669. doi:10.6061/clinics/2015(10)01
14. Yutong J, Lingtao WU, Yanglu G, Chong X, Binyan YU, Lihua X. Long-term efficacy of point application therapy on different acupoints and durations in the treatment of asthma: a randomized controlled trial. J Tradit Chin Med. 2023;43(1):146–153. doi:10.19852/j.cnki.jtcm.2023.01.013
15. Choi J-Y, Jung H-J, Kim J-I, et al. A randomized pilot study of acupuncture as an adjunct therapy in adult asthmatic patients. J Asthma. 2010;47(7):774–780. doi:10.3109/02770903.2010.485665
16. Rosenkranz MA, Dean DC, Bendlin BB, et al. Neuroimaging and biomarker evidence of neurodegeneration in asthma. J Allergy Clin Immunol. 2022;149(2):589–598.e6. doi:10.1016/j.jaci.2021.09.010
17. Su Y, Xu J, Zhu Z, et al. Brainstem Dbh+ neurons control allergen-induced airway hyperreactivity. Nature. 2024;631(8021):601–609. doi:10.1038/s41586-024-07608-5
18. Blackwell VK, Van Goor JJ, Prescott SL. The airway-brain axis: connecting breath, brain, and behavior. Cell Rep. 2025;44(9):116239. doi:10.1016/j.celrep.2025.116239
19. Cai R-L, Shen G-M, Wang H, Guan -Y-Y. Brain functional connectivity network studies of acupuncture: a systematic review on resting-state fMRI. J Integr Med. 2018;16(1):26–33. doi:10.1016/j.joim.2017.12.002
20. Chan A-W, Boutron I, Hopewell S, et al. SPIRIT 2025 statement: updated guideline for protocols of randomized trials. JAMA. 2025;334(5):435–443. doi:10.1001/jama.2025.4486
21. Hopewell S, Chan A-W, Collins GS, et al. CONSORT 2025 statement: updated guideline for reporting randomised trials. Lancet. 2025;405(10489):1633–1640. doi:10.1016/S0140-6736(25)00672-5
22. MacPherson H, Altman DG, Hammerschlag R, et al. Revised Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. J Evid Based Med. 2010;3(3):140–155. doi:10.1111/j.1756-5391.2010.01086.x
23. Jia CE, Zhang HP, Lv Y, et al. The asthma control test and asthma control questionnaire for assessing asthma control: systematic review and meta-analysis. J Allergy Clin Immunol. 2013;131(3):695–703. doi:10.1016/j.jaci.2012.08.023
24. Bateman ED, Esser D, Chirila C, et al. Magnitude of effect of asthma treatments on asthma quality of life questionnaire and asthma control questionnaire scores: systematic review and network meta-analysis. J Allergy Clin Immunol. 2015;136(4):914–922. doi:10.1016/j.jaci.2015.03.023
25. Islam N, Hashem R, Gad M, et al. Accuracy of the montreal cognitive assessment tool for detecting mild cognitive impairment: a systematic review and meta-analysis. Alzheimers Dement. 2023;19(7):3235–3243. doi:10.1002/alz.13040
26. Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2016;25:52–73. doi:10.1016/j.smrv.2015.01.009
27. Zung WWK. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
28. Zung WK. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch Gen Psychiatry. 1965;13(6):508–515. doi:10.1001/archpsyc.1965.01730060026004
29. Schatz M, Kosinski M, Yarlas AS, Hanlon J, Watson ME, Jhingran P. The minimally important difference of the Asthma Control Test. J Allergy Clin Immunol. 2009;124(4):719–723.e1. doi:10.1016/j.jaci.2009.06.053
30. Desmond JE, Glover GH. Estimating sample size in functional MRI (fMRI) neuroimaging studies: statistical power analyses. J Neurosci Methods. 2002;118(2):115–128. doi:10.1016/S0165-0270(02)00121-8
31. Pajula J, Tohka J. How many is enough? Effect of sample size in inter-subject correlation analysis of fMRI. Comput Intell Neurosci. 2016;2016:2094601. doi:10.1155/2016/2094601
32. Szucs D, Ioannidis JP. Sample size evolution in neuroimaging research: an evaluation of highly-cited studies (1990–2012) and of latest practices (2017–2018) in high-impact journals. Neuroimage. 2020;221:117164. doi:10.1016/j.neuroimage.2020.117164
33. Beasley R, Braithwaite I, Semprini A, Kearns C, Weatherall M, Pavord ID. Optimal asthma control: time for a new target. Am J Respir Crit Care Med. 2020;201(12):1480–1487. doi:10.1164/rccm.201910-1934CI
34. Nathan RA, Thompson PJ, Price D, et al. Taking aim at asthma around the world: global results of the asthma insight and management survey in the Asia-Pacific Region, Latin America, Europe, Canada, and the United States. J Allergy Clin Immunol Pract. 2015;3(5):734–742.e5. doi:10.1016/j.jaip.2015.04.013
35. Caminati M, Vaia R, Furci F, Guarnieri G, Senna G. Uncontrolled asthma: unmet needs in the management of patients. J Asthma Allergy. 2021;14:457–466. doi:10.2147/JAA.S260604
36. Wang Y, Devji T, Carrasco-Labra A, et al. A step-by-step approach for selecting an optimal minimal important difference. BMJ. 2023;381:e073822. doi:10.1136/bmj-2022-073822
37. Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (F e NO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi:10.1164/rccm.9120-11ST
38. Carrol D, Busse WW, Frye CJ, et al. Regional brain structural alterations in reward and salience networks in asthma. Brain Behav Immun. 2025;126:80–97. doi:10.1016/j.bbi.2025.01.028
39. Wang F-X, Jin L-W. Research on the Mechanism and application of acupuncture therapy for asthma: a review. J Asthma Allergy. 2024;17:495–516. doi:10.2147/JAA.S462262
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
Evaluating the Efficacy and Underlying Mechanisms of Acupuncture for Chronic Subjective Tinnitus Using Functional Near-Infrared Spectroscopy: Study Protocol for a Randomized Controlled Trial
Hu H, Lin X, Fang L, Li Y, Gao H
Journal of Pain Research 2023, 16:3367-3378
Published Date: 4 October 2023
Clinical Efficacy and Safety of a Modified Moxibustion Therapy for Low Back Pain in Lumbar Disc Herniation: A Two-Center, Randomized, Controlled, Non-Inferiority Trial
Xue K, Wang X, Xiao C, Zhang N, Liu M, Fu J, Cui J
Journal of Pain Research 2024, 17:1853-1865
Published Date: 23 May 2024
A Pilot Study for Effectiveness and Safety of Adjunctive Pharmacopuncture to Acupuncture Treatment for Rotator Cuff Diseases: A Pragmatic Randomized Controlled Trial
Cha HJ, Han CH, Jeon JH, Jeong JK, Jung IC, Yang C, Kang BK, Kim MJ, Choi YE, Kim YI
Journal of Pain Research 2024, 17:2203-2221
Published Date: 24 June 2024
Exploration of Key Brain Regions Involved in Acupuncture and Moxibustion Analgesia: An Imaging-Based Study
He L, Zhou R, Hou S, Huang D, Zhao X, Wang M, Huang M, Yin T, Yin H, Yu S
Journal of Pain Research 2025, 18:2051-2067
Published Date: 15 April 2025