Back to Journals » International Journal of General Medicine » Volume 18
A Study of the Correlation Between the Inflammatory Index and Disease Activity in Ulcerative Colitis
Authors Chenfei Z, Ainiwaer Z, Xiaoling H
Received 9 July 2025
Accepted for publication 19 November 2025
Published 29 November 2025 Volume 2025:18 Pages 7143—7152
DOI https://doi.org/10.2147/IJGM.S552515
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Gopal Krishna Dhali
Zhang Chenfei, Zubiyan Ainiwaer, Huang Xiaoling
Xinjiang Uygur Autonomous Region People’s Hospital, Urumqi, Xinjiang Uygur Autonomous Region, People’s Republic of China
Correspondence: Huang Xiaoling, Email [email protected]
Objective: To analyze the level of systemic immune-inflammatory index (SII) in patients with ulcerative colitis (UC) and assess its relationship with disease activity.
Methods: This study included 616 UC patients and 211 healthy controls. Disease activity was assessed using the modified Mayo score, categorizing patients into remission (n=115) and active (n=501) groups, with the latter further stratified into mild, moderate, and severe activity. We compared multiple inflammatory indices—including SII, neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), neutrophil percentage-albumin ratio (NPAR), and others—between groups. Spearman correlation and ROC curve analyses were used to evaluate their associations with disease activity and predictive value for active and severe UC.
Results: SII, NLR, PLR, NPAR, and several other indices were significantly higher in the UC group than controls, while lymphocyte-to-monocyte ratio (LMR) and LHR were lower (all P< 0.05). Most indices were also elevated in active versus remission UC (P< 0.05), and showed significant differences across severity subgroups (P< 0.05), with SII, NLR, NPAR, NHR, and MHR increasing with severity. Spearman analysis revealed positive correlations between these markers and disease activity/severity (P< 0.001). ROC analysis demonstrated significant predictive value for active and severe UC (AUC> 0.60, P< 0.001), with NPAR exhibiting the highest efficacy (AUC=0.854).
Conclusion: SII, NLR, PLR, NPAR, and other inflammatory indices are useful non-invasive biomarkers for assessing UC disease activity and severity, with NPAR showing the strongest predictive performance.
Keywords: ulcerative colitis, systemic immune-inflammatory index, disease activity, biomarkers
Introduction
Inflammatory bowel disease (IBD) is a global disease characterized by chronic inflammation of the gastrointestinal tract, with ulcerative colitis (UC) and Crohn’s disease (CD) as its two common subtypes. The incidence of UC has been increasing in Asia in recent years, and China has become the country with the highest incidence of UC among Asian countries. The pathogenesis of UC may be related to genetics, geographic environment, dietary habits, breastfeeding, intestinal flora, smoking, etc. The clinical course of UC is variable, characterized by recurrent episodes of relapse and remission,1 and the main manifestations can be divided into intestinal manifestations (eg, recurrent diarrhea, mucous pus and blood stools) and extraintestinal manifestations. The prolonged intestinal inflammation brings serious physical and mental burdens to patients, and most of the related treatments work by suppressing inflammation, and long-term immunosuppressive therapy increases the infectious and tumor burden of systemic diseases,2 so effective and timely disease monitoring, choosing the appropriate treatment plan, maintaining long-lasting disease remission, and decreasing the risk of hospitalization and surgery appear to be of vital importance.
Previously, the goal of treatment for UC disease was to focus on clinical palliation, including alleviation of symptoms of acute exacerbations, reduction of complications, and improvement of quality of life. However, limiting to clinical remission was not a significant improvement in the course of the disease, and in the long run the inflammation of the mucosa could not be cured, which increased the risk of intestinal stenosis, colon cancer, and surgical treatment.3 With better understanding of the disease, mucosal healing has been found to be associated with steroid-free remission of the disease as well as long-term remission, but the definition of mucosal healing in UC remains controversial,4 and LEMMENSB et al found that tissue biopsies from 14% of patients with MH still detected histologic activity,5 so that the intestinal mucosa of patients with UC who have attained MH may still be histologically inflamed. With the research of biologics related to the treatment of UC, we found that histological remission (HR) can reduce the recurrence rate, surgery rate and cancer probability of the disease and improve the prognosis of UC, which led to the concept of deep remission (DR).6
The selection of inflammatory indices in this study was based on their established roles in reflecting distinct yet complementary pathways of inflammation and immunity, coupled with their routine availability and cost-effectiveness. Established markers such as the systemic immune-inflammatory index (SII), neutrophil-to-lymphocyte ratio (NLR), and platelet-to-lymphocyte ratio (PLR) integrate multiple cellular components of the immune response and have demonstrated prognostic value in chronic inflammatory and neoplastic conditions.7,8 Their application in UC is grounded in the central roles of neutrophil infiltration, adaptive immune dysregulation, and platelet-mediated pro-inflammatory signaling in its pathogenesis.9,10 Building upon the rationale for composite indices, we specifically introduced the neutrophil percentage-albumin ratio (NPAR) to synergistically capture both the intensity of the innate immune response (via neutrophil percentage) and the systemic nutritional and synthetic reserve (via serum albumin). This dual-component design addresses key pathological features of active UC: sustained neutrophilic inflammation often leads to elevated neutrophil counts, while chronic inflammation and intestinal protein loss frequently result in hypoalbuminemia. Albumin itself also possesses anti-inflammatory and antioxidant properties, and its decrease may exacerbate inflammation. The combination into a single ratio may therefore offer a more holistic view of disease burden than either component alone. Furthermore, the proven utility of similar ratios, such as the C-reactive protein-to-albumin ratio (CAR), in predicting outcomes in cancer and inflammatory diseases, provided a strong precedent for investigating NPAR’s potential in UC.
Other investigated indices, including the inflammation-biomarker composite index (IBI), systemic inflammatory response index (SIRI), neutrophil-to-platelet ratio (NPR), and ratios involving lipoproteins (NHR, MHR, LHR), were included to provide a comprehensive comparison and explore the potential influence of lipid metabolism on UC-related inflammation. Therefore, in this paper, the authors tried to explore the correlation between SII, NLR, PLR, IBI, LMR, SIRI, NPR, NHR, MHR, LHR and UC mucosal histologic activity, as well as the value of its application as a simple and easy-to-use UC disease monitoring.
Subjects and Methods
Study Type
Retrospective comparative trial
Time and Place
The trial was completed from January 2020 to December 2022 in the Department of Gastroenterology of Xinjiang Uygur Autonomous Region People’s Hospital.
Inclusion Criteria
① Clinical data of the included subjects were all relatively complete; ② All of them were diagnosed with ulcerative colitis after comprehensive evaluation of clinical, laboratory examination, imaging examination, endoscopy and histopathological examination; ③ Passed through the Ethics Committee of Xinjiang Uygur Autonomous Region People’s Hospital, which has been examined and approved by NO: KY20241201105. All study subjects had signed the informed consent for drug use.
Exclusion Criteria
① Those who were previously diagnosed as digestive system tumor; ② Those who are now infected with other infectious diseases at the same time; ③People ≤18 years old and ≥70 years old, as well as pregnant or lactating women; ④Excluding diseases that may affect platelets, ALB, CRP, such as renal diseases, liver diseases, rheumatic diseases, blood-related diseases, active infections; ⑤ People who used drugs such as immunosuppressants, biologics, or hormones in the last 3 months; ⑥ People who were infected with other infectious or non-infectious colitis.
Grouping Criteria and Definitions
A. Grouping criteria: the disease activity of UC patients was assessed according to the modified Mayo score, with a Mayo score ≤2 and no single sub-score >1 defined as clinical remission, a single sub-score >1 as non-remission, and a Mayo score >2 as active (of which 3–5 was mild activity, 6–10 was moderate activity, and 11–12 was severe activity). Based on the modified Mayo score, 616 UC patients were divided into 115 cases in the remission group and 501 cases in the active group (206 cases in the mild activity group, 178 cases in the moderate activity group, and 117 cases in the severe activity group).
B. Inflammatory indices: ①Systemic immune inflammatory index formula (SII): platelet count×neutrophil count/lymphocyte count; ②NLR:Neutrophil/lymphocyte ratio; ③PLR:Platelet/lymphocyte ratio; ④LMR:Lymphoid mononuclear ratio; ⑤NPR:Neutrophil to platelet ratio; ⑥SIRI:Systemic inflammatory response index; ⑦NPIR. Neutrophil percentage (%) × 100/albumin; ⑧ IBI: C-reactive protein × neutrophils/lymphocytes; ⑨ NHR: neutrophils/high-density lipoprotein cholesterol; ⑩MHR: monocytes/high-density lipoprotein cholesterol; LHR: lymphocytes/ high-density lipoprotein cholesterol; and so on.
Statistical Analysis
All data were analyzed using SPSS 26.0 statistical software for data analysis. Data were processed and plotted using Graphpad prim 6.0 software. Shapiro–Wilk (S-W) test was used to analyze the normality of the data distribution; normally distributed numerical variables were expressed as (x±s), otherwise they were expressed as median interquartile range; for ordered or nominal variables, the rate of descriptions or composition ratio was described; the comparison of two groups of normally distributed measurements was done by T-test, and the comparison of non-normally distributed numerical variables was done by Mann–Whitney U-test; the comparison among multiple groups was done by one-way ANOVA; ROC curve analysis was used to determine the normal distribution of each group. Comparisons were made using one-way ANOVA; ROC curve analysis was used to determine the optimal cutoff value, sensitivity, and specificity of each test, and to calculate the area of the curve at the 95% confidence interval, Youden’s index; binary logistic regression models were used to determine the ROC curves for the parametric joint test; Spearman correlation analysis was used to determine the correlation between the parameters of interest. Two-sided tests were used, and P<0.05 was considered statistically significant.
Results
Analysis of the Number of Participants
827 cases of UC patients were included, and they were divided into 2 groups according to their diseases, 616 cases in the UC group and 211 cases in the control group, all of which entered the outcome analysis without shedding data.
Comparison of General Clinical Data and Laboratory Results Between Subjects in the UC Group and the Control Group
SII, NLR, PLR, NPAR, IBI, SIRT, NPR, NHR, and MHR of patients in the UC group were significantly higher than those in the control group, and LMR and LHR were significantly lower than those in the control group (P<0.05), and the differences in the rest of the indexes of the subjects in the two groups were not statistically significant (P>0.05). See Table 1.
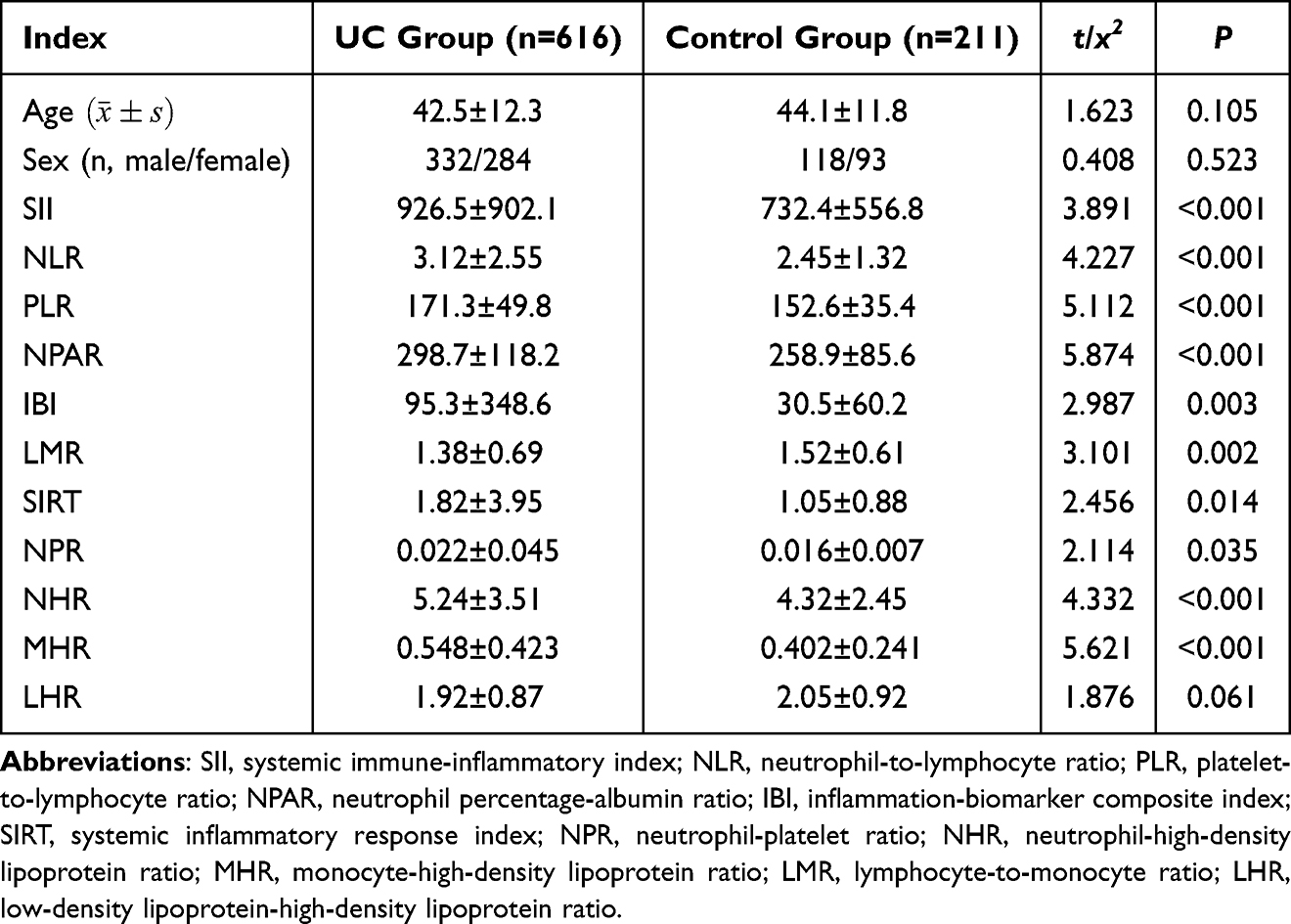 |
Table 1 Comparison of General Clinical Data and Laboratory Test Results Between UC Group and Control Group |
Comparison of Laboratory Findings Between UC Patients in the Active and Remission Groups
SII, NLR, PLR, NPAR, IBI, LMR, NPR, NHR and MHR of patients in the active group were significantly higher than those of the remission group, SIRT was significantly lower than that of the remission group (P<0.05), and there was no statistical significance in comparing the LHR of patients in the two groups (P>0.05). See Table 2.
 |
Table 2 Comparison of Laboratory Test Results Between Active and Remission Groups of UC Patients |
Comparison of Laboratory Findings in Patients with UC of Different Severity
The differences in SII, NLR, PLR, NPAR, IBI, LMR, SIRT, NPR, NHR and MHR in patients with UC of different severity groups were statistically significant (P<0.05). SII, NLR, PLR, NPAR, IBI, SIRT, NHR and MHR were sequentially increased in patients in the mild activity group, moderate activity group and severe activity group; LMR level was higher in patients in the mild activity group and moderate activity group than that in the severe activity group (P<0.05), and there was no statistically significant difference in the comparison of LHR level among the three groups (P>0.05). See Table 3.
 |
Table 3 Comparison of Laboratory Test Results of UC Patients with Different Severity |
Correlation Analysis of Each Serological Index with UC Disease Activity and Severity of Active Phase
The results of Spearman correlation analysis showed that SII, NLR, PLR, NPAR, IBI, LMR, SIRT, NHR, and MHR were positively correlated with UC disease activity and the severity of the active phase of UC (P<0.001). See Table 4.
 |
Table 4 The Serum Markers Were Correlated with the Disease Activity and Severity of UC Spearman Related Analysis |
Predictive Efficacy of Each Inflammatory Index for Active UC and Severe UC
The results of ROC curve analysis showed that SII, NLR, PLR, NPAR, IBI, LMR, SIRT, NHR, and MHR all had some predictive value for active UC [area under the ROC curve (AUC) >0.60, P<0.001], with NPAR having the largest AUC; SII, NLR, PLR, NPAR, IBI, LMR, SIRT, NHR and MHR all had some predictive value for severe UC (P<0.001), with NPAR having the largest AUC. See Tables 5 and 6.
 |
Table 5 ROC Curve Analysis of the Predictive Indicators of Active UC |
 |
Table 6 ROC Curve Analysis Results of Various Inflammatory Indicators Predicting Severe UC |
Discussion
This study compared the value of various inflammatory markers in assessing the disease activity and severity of active ulcerative colitis (UC), and found that NPAR had the greatest predictive value for active UC and severe UC. Compared with IBI and SIRT, ROC curve analysis indicated that NPAR had the best predictive value for distinguishing the disease activity of UC. UC is a chronic inflammatory disease that can cause persistent inflammation of the intestinal mucosa. Many patients have mild disease activity that is self-limiting, but a considerable number of patients experience severe activity accompanied by serious complications. Effective drug treatment can alleviate symptoms and reduce the mortality rate of severe patients. Therefore, determining the disease activity of UC is crucial for assessing patient condition, adjusting treatment plans, and guiding disease prognosis. Although endoscopy has become the gold standard for assessing the disease activity of UC patients, it is an invasive method and may also increase the risk of UC activity recurrence and cause major complications such as perforation. Therefore, further research is needed into a non-invasive method for judging the disease activity of UC.
The Value of Inflammatory Indicators in the Diagnosis and Disease Activity Assessment of UC
In this study, the Systemic Immune-Inflammation Index (SII) was significantly higher in the ulcerative colitis (UC) group than in the control group (926.5 ± 902.1 vs 732.4 ± 556.8, P < 0.001), consistent with the findings of Gui’s study.11 The mechanism may be related to platelet activation promoting microthrombus formation in the intestinal mucosa and neutrophil infiltration.12 However, the predictive area under the curve (AUC) of SII in this study (0.812 for active stage and 0.786 for severe stage) was higher than the 0.75 reported by Takač et al,13 which may be due to a larger sample size and stricter inclusion criteria. The Neutrophil-to-Lymphocyte Ratio (NLR) was elevated in the UC group (3.12 ± 2.55 vs 2.45 ± 1.32, P < 0.001), consistent with previous meta-analysis results (pooled odds ratio = 2.34).14 The increased Platelet-to-Lymphocyte Ratio (PLR) (171.3 ± 49.8 vs 152.6 ± 35.4, P < 0.001) supports the hypothesis that platelets exacerbate mucosal damage by releasing pro-inflammatory factors such as PF4 and PDGF.15 Notably, the predictive AUC of PLR for the active stage in this study (0.753) was lower than Alper et al’s 0.82,16 potentially reflecting the impact of population heterogeneity on the results. This study is the first to propose NPAR (Neutrophil Percentage to Albumin Ratio) as a biomarker for UC, with a diagnostic efficacy (AUC = 0.854) significantly superior to traditional indicators. This finding is supported by two aspects: the elevated neutrophil percentage is positively correlated with the endoscopic severity of UC (r = 0.62, P < 0.001);17 hypoalbuminemia (<35 g/L) is an independent risk factor for hospitalization in UC patients (hazard ratio = 2.1).18 The dual-dimensional characteristics of NPAR may explain its superiority, but its clinical application requires multicenter validation.
Dynamic Monitoring of Disease Activity and Severity
This study systematically analyzed the value of inflammatory markers in assessing disease activity in ulcerative colitis (UC), revealing that both SII (906.3 ± 918.2 vs 743.6 ± 549.9, P < 0.001) and NLR (2.94 ± 2.44 vs 2.68 ± 1.47, P < 0.001) were significantly elevated during active disease, consistent with Li et al’s findings based on fecal calprotectin for disease activity stratification.19 However, LMR exhibited a paradoxical increase during active disease (1.42 ± 0.71 vs 1.39 ± 0.55, P < 0.001), potentially related to differential lymphocyte recovery rates between remission and active phases, necessitating further validation through lymphocyte subset analysis.20 Across mild-to-severe UC, SII (653.5 → 1148.4), NLR (2.35 → 3.76), and NPAR (153.7 → 194.0) all showed significant incremental trends (all P < 0.001), highly consistent with Mules et al’s Mayo score-based stratification study.21 Notably, PLR was slightly lower in severe UC (301.1 ± 143.2) compared to moderate UC (318.3 ± 128.7), potentially reflecting increased platelet consumption, a phenomenon also reported in sepsis studies.22 Meanwhile, LMR significantly decreased in severe UC (1.21 ± 0.66 vs 1.57 ± 0.71, P < 0.001), corroborating Ning et al’s finding that LMR < 1.5 predicts steroid resistance (OR = 3.2),23 likely due to monocyte differentiation into pro-inflammatory M1 macrophages amplifying the inflammatory cascade.24 These findings suggest that SII and NPAR could serve as reliable biomarkers for UC disease activity and severity, while the dynamic changes in LMR require further investigation through immune subset analysis to clarify its clinical application value in therapeutic decision-making.
Interpretation of Specific Biomarker Dynamics
The observation of an elevated Lymphocyte-to-Monocyte Ratio (LMR) during active disease, though seemingly counter-intuitive given the typical lymphopenia in inflammation, warrants further mechanistic interpretation. This phenomenon may be attributed to a complex, phase-dependent dynamic of lymphocyte subsets. In the early or moderately active stages of UC, a relative preservation or even transient increase in certain lymphocyte populations (eg, activated effector cells) might occur, potentially outpacing a more stable monocyte count, leading to a higher LMR.20 This pattern could differ significantly in severe disease, where our data indeed showed a declining LMR trend, likely reflecting eventual lymphocyte exhaustion and a pronounced monocyte/macrophage activation.24 This non-linear dynamic underscores the complexity of the immune response in UC and suggests that LMR’s utility might be context-dependent, requiring careful interpretation alongside clinical severity.
Regarding the superior predictive performance of NPAR, its enhanced accuracy likely stems from its unique biological composition, integrating two fundamental pathological pathways. The neutrophil percentage component directly reflects the intensity of acute neutrophilic inflammation and mucosal infiltration, a hallmark of UC flare-ups.17 Concurrently, serum albumin serves as a synthetic marker of the host’s systemic nutritional and inflammatory status; hypoalbuminemia in UC results from a combination of cytokine-driven suppression of hepatic synthesis, increased catabolism, and intestinal protein loss. Albumin itself also possesses anti-inflammatory and antioxidant properties.14 Therefore, NPAR simultaneously quantifies the level of innate immune activation (numerator) and the body’s reserve capacity to counteract inflammation and maintain homeostasis (denominator). This dual capture of the “insult” and the “host response” provides a more holistic reflection of disease burden than markers reflecting a single dimension, such as fecal calprotectin (primarily neutrophilic inflammation) or albumin alone. This integrative nature likely underpins its robust AUC compared to other indices.
Predictive Efficacy and Clinical Transformation of Inflammatory Indicators
NPAR demonstrated superior predictive performance for active UC, achieving an AUC of 0.843 (sensitivity 81.5%, specificity 76.8%), outperforming both CRP (AUC = 0.72)25 and fecal calprotectin (AUC = 0.89).26 While fecal biomarkers offer higher specificity, NPAR’s convenience as a blood-based test makes it more suitable for outpatient screening. For predicting severe UC, NPAR achieved an AUC of 0.854, comparable to the established anti-TNFα treatment failure risk model (AUC = 0.82).27 A combined predictive model incorporating MHR (AUC = 0.791) showed potential, such as: Risk Score = 0.4 × NPAR + 0.3 × MHR, which has already demonstrated preliminary success in Crohn’s disease (improving sensitivity by 15%)28. Notably, UC patients exhibited impaired lymphocyte reactivity with dysfunctional responses at both peripheral and mucosal levels, despite the lack of statistically significant differences in peripheral blood lymphocyte counts compared to controls in this study. These findings collectively indicate that NPAR effectively reflects host immune and inflammatory status, highlighting the critical roles of immune responses and inflammation in UC pathogenesis and progression. Consequently, NPAR demonstrates superior diagnostic capability for active UC compared to other inflammatory markers.
Limitations of the Article
This study has several limitations that should be considered. First, its single-center, retrospective design may introduce potential selection bias and limit the generalizability of the findings. Although our research team meticulously collected data to ensure integrity, unmeasured confounding factors inherent to retrospective analyses cannot be fully excluded. Second, the sample size, while substantial, remains relatively limited, which may affect the statistical power for certain subgroup analyses. Therefore, our results should be interpreted as preliminary, and further validation through large-scale, multicenter, prospective studies is essential to confirm the clinical utility of these inflammatory indices, particularly NPAR.
Conclusion
This study confirmed that SII, NLR, PLR, NPAR, IBI, LMR, SIRT, NHR, and MHR can non-invasively assess the activity and severity of UC, among which NPAR showed the best diagnostic efficacy. Future multi-center studies are needed to verify its clinical applicability and explore integration with genomic/microbial analysis.
Abbreviations
SII, Systemic immune-inflammatory index; NLR, Neutrophil/lymphocyte ratio; PLR, Platelet/lymphocyte ratio; NPAR, Neutrophil percentage-albumin ratio; IBI, Inflammation-biomarker composite index; SIRT, Systemic inflammatory response index; NPR, Neutrophil-platelet ratio; NHR, Neutrophil-high-density lipoprotein ratio; MHR, Monocyte-high-density lipoprotein ratio; LMR, Lymphocyte/monocyte ratio; LHR, Low-density lipoprotein-high-density lipoprotein ratio.
Data Sharing Statement
To analyze the level of systemic immunoinflammatory index (SI) in patients with ulcerative colitis (UC) and to assess its relationship with disease activity, so the dataset analyzed in this study is not publicly available but is available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
We confirm that all experiments were performed in accordance with the Declaration of Helsinki. The study was approved by the Ethical Committee of the Xinjiang Uygur Autonomous Region People’s Hospital, NO: KY20241201105. Each patient provided written informed consent before participating in the study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
Tianshan Talent Project, “The study of TAK-242 affecting macrophages and regulatory T cells by modulating the JAK2/STAT3 signaling pathway to alleviate ulcerative colitis.” ID:TSYC202301A040.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ng SC, et al. Incidence and phenotype of inflammatory bowel disease in Asia: a multicenter population-based study. Lancet Gastroenterol Hepatol. 2018;3(10):677–688. PMID: 30115544.
2. Liu JZ, Duecker K, Maack MC, et al. Genome-wide association study of ulcerative colitis in han chinese reveals genetic risk loci and pathways. Nat Commun. 2019;10(1):5427. PMID: 31776354. doi:10.1038/s41467-019-13417-6
3. Ananthakrishnan AN, et al. Dietary patterns and risk of inflammatory bowel disease: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 18(7):1459–1472. PMID: 31676300.
4. Ordás I, Eckmann L, Talamini M, et al. Ulcerative colitis. Lancet. 2012;380(9853):1606–1619. doi:10.1016/S0140-6736(12)60150-0
5. SColombel JF, Ricciuto A, Lewis A, et al. STRIDE-II: an Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD). Gastroenterology. 2021;160(5):1570–1583. PMID: 33359090. doi:10.1053/j.gastro.2020.12.031
6. Bryant RV, et al. Histologic healing is associated with reduced risk of disease progression in ulcerative colitis. Gastroenterology. 2019;156(4):965–977. PMID: 30529583.
7. Chen JH, et al. Platelet activation promotes mucosal inflammation in ulcerative colitis. Inflamm Bowel Dis. 2019;25(5):859–867. PMID: 30517652.
8. Zhang Y, et al. Systemic immune-inflammation index predicts disease severity in ulcerative colitis. J Crohns Colitis. 2020;14(3):331–338. PMID: 31630145.
9. Torun S, et al. Neutrophil-to-lymphocyte ratio in ulcerative colitis: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 31(7):742–747. PMID: 30720417.
10. Yamamoto T, Goyal P, Agarwal A, et al. C-reactive protein to albumin ratio correlates with disease activity and poor prognosis in ulcerative colitis. Sci Rep. 2021;11(1):16236. PMID: 34373474. doi:10.1038/s41598-021-95758-1
11. Gui X, Bazarova A, Del Amor R, et al. ICaSSO Histologic Remission Index (PHRI) in ulcerative colitis: development of a novel simplified histological score for monitoring mucosal healing and predicting clinical outcomes and its applicability in an artificial intelligence system. Gut. 2022;71(5):889–898. doi:10.1136/gutjnl-2021-326376
12. Cherfane CE, Gessel L, Cirillo D, et al. Monocytosis and a low lymphocyte to monocyte ratio are effective biomarkers of ulcerative colitis disease activity. Inflamm Bowel Dis. 2015;21(8):1769–1775. doi:10.1097/MIB.0000000000000427
13. Takač B, Mihaljević S, Glavaš-Obrovac L, et al. Interactions among interleukin-6, c-reactive protein and interleukin-6 (−174) g/c polymorphism in the pathogenesis of crohn’s disease and ulcerative colitis. Acta Clin Croat. 2020;59(1):67–80. doi:10.20471/acc.2020.59.01.09
14. Motwani KK, Alizadeh M, Abutaleb A. et al. correlation between serum and fecal biomarkers and patient-reported outcomes in patients with crohn’s disease and ulcerative colitis. Dig Dis Sci. 2024;69(6):2154–2163. doi:10.1007/s10620-024-08421-w
15. Restellini S, Chao CY, Martel M, et al. Clinical parameters correlate with endoscopic activity of ulcerative colitis: a systematic review. Clin Gastroenterol Hepatol. 2019;17(7):1265–1275.e8. doi:10.1016/j.cgh.2018.12.021
16. Alper A, Zhang L, Pashankar DS. Correlation of erythrocyte sedimentation rate and c-reactive protein with pediatric inflammatory bowel disease activity. J Pediatr Gastroenterol Nutr. 2017;65(2):e25–e27. doi:10.1097/MPG.0000000000001444
17. Parkes G, Ungaro RC, Danese S, et al. Correlation of mucosal healing endpoints with long-term clinical and patient-reported outcomes in ulcerative colitis. J Gastroenterol. 2023;58(10):990–1002. doi:10.1007/s00535-023-02013-7
18. Yüksel O, Helvaci K, Başar O, et al. An overlooked indicator of disease activity in ulcerative colitis: mean platelet volume. Platelets. 2009;20(4):277–281. doi:10.1080/09537100902856781
19. Xiaotong L, Lijuan H. Correlation analysis between systemic immune inflammation index and disease activity of ulcerative colitis. Int J Digestive Dis. 2022;42(05):289–293.
20. Bossuyt P, Bisschops R, Vermeire S, et al. Variability in the distribution of histological disease activity in the colon of patients with ulcerative colitis. J Crohns Colitis. 2021;15(4):603–608. doi:10.1093/ecco-jcc/jjaa206
21. Mules TC, Swaminathan A, Hirschfeld E, et al. The impact of disease activity on psychological symptoms and quality of life in patients with inflammatory bowel disease-results from the Stress, Anxiety and Depression with Disease Activity (SADD) Study. Aliment Pharmacol Ther. 2022;55(2):201–211. doi:10.1111/apt.16616
22. Walmsley RS, Ayres RC, Pounder RE, et al. A simple clinical colitis activity index. Gut. 1998;43(1):29–32. doi:10.1136/gut.43.1.29
23. Ning L, Li S, Gao J, et al. Tenascin-C Is increased in inflammatory bowel disease and is associated with response to infliximab therapy. Biomed Res Int. 2019;2019:1475705. doi:10.1155/2019/1475705
24. Solem CA, EV L, Tremaine WJ, Harmsen WS, Zinsmeister AR, Sandborn WJ. Tremaine WJ, et al. Correlation of C-reactive protein with clinical, endoscopic, histologic, and radiographic activity in inflammatory bowel disease. Inflamm Bowel Dis. 2005;11(8):707–712. doi:10.1097/01.MIB.0000173271.18319.53
25. Oikonomou KA, Kapsoritakis AN, Theodoridou C, et al. Neutrophil gelatinase-associated lipocalin (NGAL) in inflammatory bowel disease: association with pathophysiology of inflammation, established markers, and disease activity. J Gastroenterol. 2012;47(5):519–530. doi:10.1007/s00535-011-0516-5
26. Masoodi I, Kochhar R, Dutta U, et al. Fecal lactoferrin, myeloperoxidase and serum C-reactive are effective biomarkers in the assessment of disease activity and severity in patients with idiopathic ulcerative colitis. J Gastroenterol Hepatol. 2009;24(11):1768–1774. doi:10.1111/j.1440-1746.2009.06048.x
27. Xu M, Cen M, Chen X, et al. Correlation between serological biomarkers and disease activity in patients with inflammatory bowel disease. Biomed Res Int. 2019;2019:6517549. doi:10.1155/2019/6517549
28. Tan Y, Guan Y, Sun Y, et al. Correlation of intestinal mucosal healing and tight junction protein expression in ulcerative colitis patients. Am J Med Sci. 2019;357(3):195–204. doi:10.1016/j.amjms.2018.11.011
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Identification of Critical Modules and Biomarkers of Ulcerative Colitis by Using WGCNA
Yuan Y, Li N, Fu M, Ye M
Journal of Inflammation Research 2023, 16:1611-1628
Published Date: 17 April 2023
Predictive Value of MHR and NLR for Ulcerative Colitis Disease Activity
Liu T, Qin Z, Yang Z, Feng X
International Journal of General Medicine 2024, 17:685-692
Published Date: 27 February 2024
Predictive Value of Albumin to Fibrinogen Ratio and CALLY Index for Diagnosis of Ulcerative Colitis and Mucosal Healing After Vedolizumab Treatment
Su K, Xiao S, Wang M, Wang K, Fan Q, Sha S, Cheng Y, Liu X, Shi H
Journal of Inflammation Research 2025, 18:589-600
Published Date: 14 January 2025
Identification of Senescence-Related Genes for the Prediction of Ulcerative Colitis Based on Interpretable Machine Learning Models
Ma J, Chen C, Wang N, Fang T, Liu Y, He P, Dong W
Journal of Inflammation Research 2025, 18:3431-3447
Published Date: 10 March 2025
Ulcerative Colitis: Advances in Pathogenesis, Biomarkers, and Therapeutic Strategies
Bu S, Cheng X, Chen M, Yu Y
Pharmacogenomics and Personalized Medicine 2025, 18:219-238
Published Date: 5 September 2025