Back to Journals » International Journal of General Medicine » Volume 17
Predictive Value of MHR and NLR for Ulcerative Colitis Disease Activity
Authors Liu T ![]() , Qin Z
, Qin Z ![]() , Yang Z, Feng X
, Yang Z, Feng X ![]()
Received 1 November 2023
Accepted for publication 18 January 2024
Published 27 February 2024 Volume 2024:17 Pages 685—692
DOI https://doi.org/10.2147/IJGM.S446723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Tian Liu, Zhenkun Qin, Zhiyue Yang, Xiaoling Feng
Division of General Practice, The Fifth Affiliated Hospital of Xinjiang Medical University, Urumqi, People’s Republic of China
Correspondence: Xiaoling Feng, Division of General Practice, The Fifth Affiliated Hospital of Xinjiang Medical University, No. 118, Henan West Road, Urumqi, Xinjiang Uygur Autonomous Region, 830011, People’s Republic of China, Email [email protected]
Background: Numerous non-invasive serologic tests are available to diagnose and monitor ulcerative colitis (UC), but their accuracy levels are limited. Thus, there is a pressing need for a serologic biomarker with higher precision for clinical practice. This study aims to evaluate the predictive capacity of monocyte/HDL ratio (MHR) and neutrophil/lymphocyte ratio (NLR) for UC disease activity.
Patients and Methods: We conducted a retrospective analysis of 81 UC patients and 77 age- and sex-matched healthy controls. UC patients were categorized into active and inactive groups based on the Mayo score. The Mayo endoscopic subscore classified them into mild-to-moderate and severe UC groups.
Results: The optimal cut-off values for diagnosing UC were 0.34 for MHR (85.7% sensitivity, 76.0% specificity, 88.9% positive predictive value, 70.4% negative predictive value) and 2.49 for NLR (66.1% sensitivity, 88.0% specificity, 92.5% positive predictive value, 53.7% negative predictive value). The optimal MHR and NLR cut-off values to differentiate between mild-to-moderate UC and severe UC were 0.38 (92.9% sensitivity, 56.6% specificity, 53.1% positive predictive value, 93.7% negative predictive value) and 3.46 (71.4% sensitivity, 88.7% specificity, 76.9% positive predictive value, 85.5% negative predictive value), respectively.
Conclusion: NLR and MHR are simple yet effective biological predictors of disease activity in UC patients.
Keywords: ulcerative colitis, monocyte/HDL ratio, neutrophil/lymphocyte ratio, disease activity
Introduction
Ulcerative colitis (UC) is a chronic inflammatory bowel disease of unknown etiology, characterized by inflammation extending from the rectum to the colon’s mucosal and submucosal layers.1 Evaluating intestinal inflammation is critical for UC disease management.2 While endoscopy and pathologic biopsy are standard methods for assessing UC clinical and endoscopic disease activity, they are invasive and associated with potential risks. Non-invasive tests, such as white blood cell (WBC) count, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and fecal calprotectin (FC), are commonly used but have limited accuracy.3–5 To meet clinical demands, various inflammatory markers derived from serologic indices have been developed.
Monocytes and neutrophils are crucial components of innate immunity and play a significant role in the development of UC. Similarly, lymphocytes are involved in the pathology of UC. Some UC patients exhibit an elevation in circulating neutrophils and monocytes along with a reduction in lymphocyte levels.6 Additionally, HDL cholesterol is involved in anti-oxidant and anti-inflammatory processes, and lower HDL cholesterol levels are associated with UC disease activity.7 Torun et al8 observed that elevated neutrophil/lymphocyte ratio (NLR) can predict disease activity in UC patients. The monocyte/HDL ratio (MHR) combines pro- and anti-inflammatory processes and may be useful in determining disease activity in UC patients. It is worth noting that NLR and MHR are cost-effective, noninvasive biomarkers of inflammation calculated from complete blood count and high-density lipoprotein levels. Previous studies have shown their utility in assessing systemic inflammation in various conditions, including infections, neoplasms, and cardiovascular disease.9–12 This study evaluated the value of MHR and NLR as biomarkers of UC disease activity.
Material and Methods
Patient Selection
This single-center retrospective cross-sectional study included a total of consecutive patients with UC and age-sex-matched healthy controls admitted to the Fifth Affiliated Hospital of Xinjiang Medical University between January 2019 and December 2022. The healthy controls were recruited from subjects who underwent colonoscopy at our hospital and had normal results. All patients underwent a complete colonoscopy and laboratory testing. Medical history data, including sex, age, disease duration, disease extension, surgical history, personal history, drug history, colonoscopy, and laboratory findings, were extracted from the hospital’s electronic medical records. Exclusion criteria include serious cardiovascular diseases, infectious diseases, malignant neoplasms, and other major systemic diseases.
Evaluation of Clinical and Endoscopic Disease Activities
Clinical activity in UC patients is assessed using the Mayo score, which includes stool frequency, rectal bleeding, endoscopic findings, and physician’s global assessment.13 Using this classification system, patients with UC were classified as mild, moderate, or severe. We classified individuals with Mayo score ≤ 2 and no sub-scale score > 1 were considered to be in the inactive group. Patients with Mayo scores of mild, moderate or severe disease were categorized into the active group. The Mayo endoscopic subscore is used to evaluate endoscopic activity in patients with ulcerative colitis.14 The Mayo endoscopic subscore can be divided into 3 levels. Score 0 as normal or healed mucosa. Score 1 as mild inflammation, erythema, decreased vascular patterns, and mild friability. Score 2 as moderate inflammation with loss of vascular patterns, marked erythema, erosions, and friability. Score 3 as severe inflammation with ulceration and spontaneous bleeding. Based on the results of the score, UC patients can be divided into a mild-to-moderate group (score 0–2) and a severe group (score 3).
Blood Analysis Methods
WBC, neutrophils, monocytes, and lymphocytes were determined using the Sysmex XN3100 (Kobe, Japan). High-density lipoprotein cholesterol (HDL-C) levels were assessed with the Beckman Coulter AU5831 automatic biochemical analyzer (California, USA). CRP was assayed with Getein 1600 (Jiangsu, China) and ESR was detected by the Mindray LBY-XC 40B (Shenzhen, China). NLR and MHR were calculated by dividing the absolute neutrophil count by the absolute lymphocyte count and the absolute monocyte count by HDL-C, respectively.
Statistical Analysis
We conducted data analysis and management using IBM SPSS 26.0 software and MedCalc 13.0 software. Continuous variables were expressed as either mean ± standard deviation (SD) or median (interquartile range), while discrete variables were presented as numbers and percentages. The normality of continuous variables was assessed through the Kolmogorov–Smirnov test. For normally distributed variables, we applied the independent t-test. Whereas the Mann–Whitney U-test was utilized for non-normally distributed continuous variables. The comparison of discrete variables was performed using the χ2 test. To evaluate the predictive accuracy of all inflammatory indicators in assessing disease activity, we employed Receiver Operating Characteristic (ROC) curves. These curves allowed us to identify optimal cut-off values and provided corresponding sensitivity, specificity, negative predictive value, positive predictive value, and the area under curve (AUC). Differences in AUCs were assessed using DeLong’s test and P-values were adjusted for Bonferroni correction. A P-value <0.05 was considered statistically significant.
Results
Comparison of Characteristics Between UC Patients and Healthy Controls
In our study, we analyzed 81 UC patients and 77 healthy individuals (see Figure 1). The UC group consisted of 60.5% males, with an average age of 49.8±14.1 years. The control group had 54.5% males, with an average age of 50.1±10.8 years. No statistically significant differences in age or sex were observed between the two groups (P > 0.05). NLR levels were significantly higher in UC patients than in healthy controls [2.48 (1.64–4.01) vs 1.55 (1.24–1.94) (P < 0.001)]. Similarly, MHR levels were significantly higher in UC patients than in healthy controls [0.44 (0.31–0.65) vs 0.31 (0.25–0.41) (P < 0.001)]. Detailed demographic and laboratory characteristics of UC patients and healthy controls are presented in Table 1.
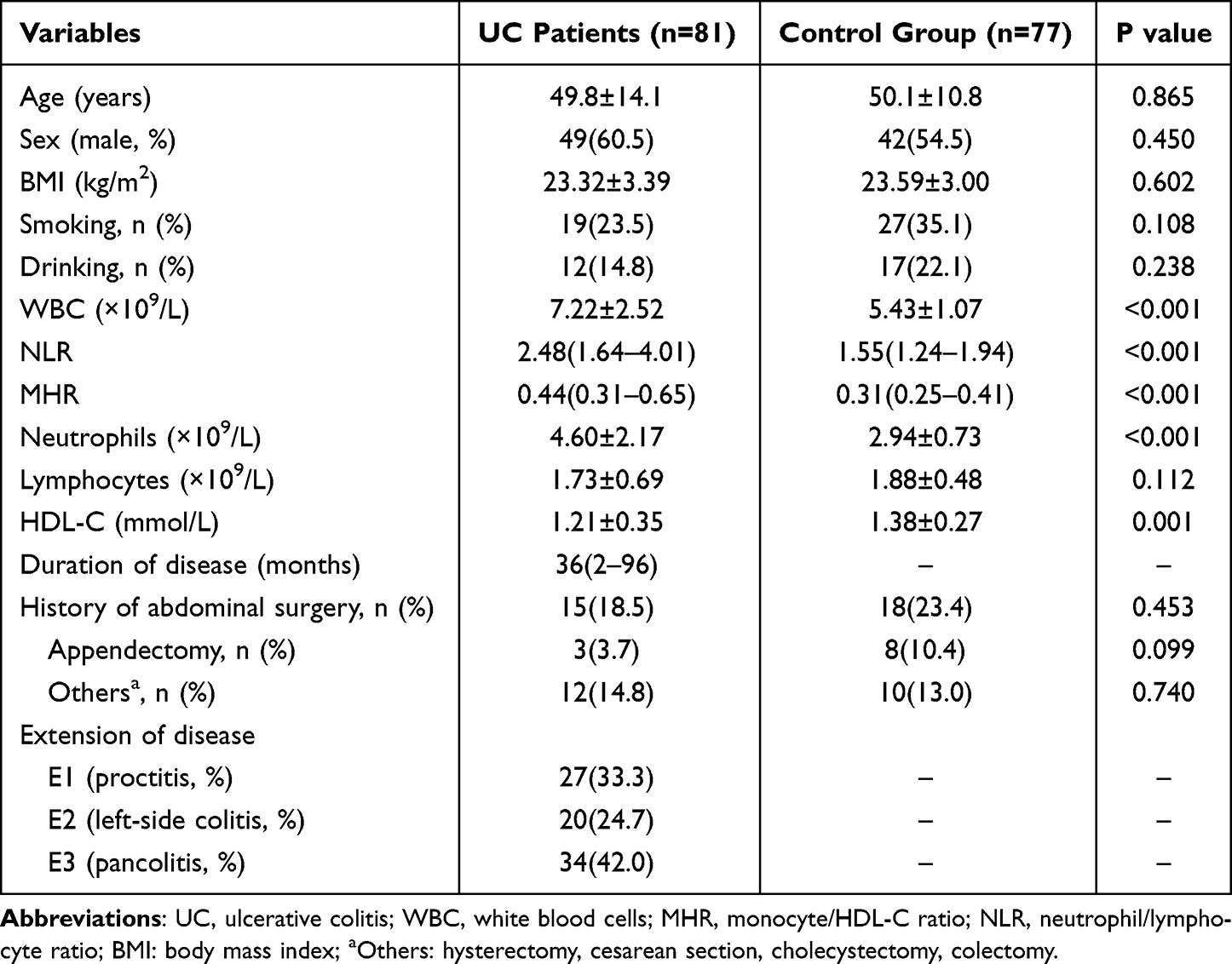 |
Table 1 Demographic and Laboratory Characteristics of UC Patients and Healthy Controls |
 |
Figure 1 Flow chart of study participants. Abbreviation: UC, ulcerative colitis. |
Comparison of Laboratory Indicators Between Active and Inactive UC Patients
Significantly higher levels of WBC, CRP, ESR, NLR, and MHR were observed in active UC patients compared to inactive UC patients. NLR levels in active and inactive UC were 3.04 (2.05–4.67) and 1.68 (1.28–2.34), respectively (P < 0.001). MHR values in active and inactive UC were 0.55 (0.39–0.75) and 0.31 (0.22–0.35), respectively (P < 0.001) (Table 2).
 |
Table 2 Comparison of Laboratory Indicators Between Active and Inactive UC |
Comparison of Laboratory Indicators Between Mild-to-Moderate and Severe UC Patients
Patients with severe UC exhibited significantly increased values of WBC, CRP, ESR, NLR, and MHR compared to those with mild-to-moderate UC. NLR levels in severe and mild-to-moderate UC were 4.28 (2.81–6.19) and 2.10 (1.40–2.62), respectively (P < 0.001). MHR values in severe and mild-to-moderate UC were 0.63 (0.45–1.16) and 0.35 (0.29–0.51), respectively (P < 0.001) (Table 3).
 |
Table 3 Comparison of Laboratory Indicators Between Mild-to-Moderate and Severe UC Patients |
Comparison of Diagnostic Accuracy of NLR and MHR in Predicting Clinical Activity in UC
Figure 2A shows the ROC curves for NLR, MHR, CRP, ESR, and WBC. The optimal NLR cut-off value for predicting clinical UC activity was 2.49, with a sensitivity of 66.1%, specificity of 88.0%, positive predictive value (PPV) of 92.5%, and negative predictive value (NPV) were 53.7%. For MHR, the optimal cut-off value was 0.34, with a sensitivity of 85.7%, specificity of 76.0%, PPV of 88.9%, and NPV of 70.4% (Table 4). Notably, the AUC of MHR was higher than that of WBC (P=0.005), but there was no statistical difference between the AUCs of NLR and MHR (P=0.483) (Table 5).
 |
Table 4 Comparing the Diagnostic Accuracy of Biomarkers in Predicting Clinical Activity in UC |
 |
Table 5 Comparisons of Biomarkers in Active Vs Inactive UC and Mild to Moderate Vs Severe UC |
 |
Figure 2 (A) shows that Receiver Operating Characteristic (ROC) curves for NLR, MHR, ESR, CRP, and WBC predict clinical activity in UC; (B) shows that ROC curves for NLR, MHR, ESR, CRP, and WBC predict endoscopic activity in UC. Abbreviations: UC, ulcerative colitis; WBC, white blood cells; MHR, monocyte to HDL-C ratio; NLR, neutrophil to lymphocyte ratio; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate. |
Comparing the Diagnostic Accuracy of NLR and MHR in Predicting Endoscopic Activity in UC
Figure 2B displays the ROC curves for NLR, MHR, CRP, ESR, and WBC. For predicting endoscopic UC activity, the optimal NLR cut-off value of 3.46, with a sensitivity of 71.4%, specificity of 88.7%, PPV of 76.9%, and NPV of 85.5%. The optimal MHR cut-off value for endoscopic severe UC was 0.38, with a sensitivity of 92.9%, specificity of 56.6%, PPV of 53.1%, and NPV of 93.7% (Table 6). Similar to the clinical activity analysis, the AUCs of NLR and MHR were not statistically different (P=1.000) (Table 5).
 |
Table 6 Comparing the Diagnostic Accuracy of Biomarkers in Predicting Endoscopic Activity in UC |
Discussion
In this study, we assessed the accuracy of NLR and MHR in predicting clinical and endoscopic activity in UC and compared their diagnostic value. Our findings revealed significant elevations in NLR and MHR in UC patients compared to healthy controls. NLR and MHR have good predictive ability for both clinical and endoscopic activity in patients with UC.
UC is a chronic inflammatory disease affecting the colorectal region, characterized by alternating periods of activity and remission. Evaluating UC severity involves clinical signs, laboratory indices, endoscopy, and histopathology.15 Mucosal healing, defined as the endoscopic resolution of UC’s erosions and ulcers, is a crucial treatment target for ulcerative colitis. Therefore, assessing endoscopic activity is essential for UC management.16 While endoscopy and histopathology play a crucial role in evaluating clinical and endoscopic UC activity, it’s important to consider the complications and contraindications associated with endoscopy. Non-invasive tests provide a convenient, rapid, and cost-effective means of diagnosing and assessing UC disease activity.17 This study aimed to evaluate the accuracy of NLR, and MHR in predicting clinical and endoscopic UC activity.
Clinical markers commonly used to measure UC disease activity include WBC, CRP, and ESR. However, these markers often lack sensitivity and specificity.5,18 NLR is a maker that responds to systemic inflammation and is widely employed in various diseases, such as cardiovascular disease, neoplastic disease, and rheumatic immune disease.12,19,20 A study by Wei et al found that MHR correlates well with CRP and has predictive value for systemic inflammation.21 Additionally, MHR is associated with an increased risk of cardiovascular events in patients with chronic kidney disease.22 Our study revealed that elevated NLR and MHR levels are associated with UC disease activity, offering valuable insights for clinicians assessing disease severity.
Neutrophils play a pivotal role in the inflammatory response to UC. When the intestinal epithelium is damaged in UC patients, neutrophils are recruited to the site of inflammation. However, they also produce large quantities of reactive oxygen species, proteases, proinflammatory cytokines, and mediators that contribute to tissue damage.23 Previous studies have shown that lymphocytic infiltration reduces circulating lymphocytes, it lead the absolute number of lymphocytes is reduced in patients with active UC compared to normal subjects.6,24 In our study, we observed a significant difference in peripheral neutrophil counts between UC patients and healthy controls. However, although the mean peripheral lymphocyte count was lower in UC patients, there was no statistically significant difference between UC patients and healthy controls. The mononuclear phagocyte systems, consisting of macrophages and dendritic cells, are involved in the pathogenesis process of inflammatory bowel disease (IBD). Inflammatory conditions cause blood monocytes to enter the intestinal mucosa, differentiating into macrophages, which interrupts the normal differentiation of mononuclear phagocytes. This disruption leads to the accumulation of pro-inflammatory macrophages, which produce substantial pro-inflammatory cytokines, triggering intestinal inflammation. Studies have also indicated that patients with IBD have altered lipid profiles compared to healthy individuals, marked by lower levels of HDL-C and higher levels of low-density lipoprotein cholesterol (LDL-C) levels.7 HDL-C plays a crucial role in regulating innate and adaptive immune responses by modulating cholesterol bioavailability in immune cells.25 Our study found that UC patients exhibited significantly higher HDL-C levels than healthy controls.
Our study demonstrates the strong predictive value of NLR and MHR for both clinical and endoscopic UC activity. However, the difference between them was not statistically significant. Therefore, we propose combining NLR and MHR for diagnosing UC disease activity. Our results suggest that MHR has the highest AUC for discriminating between UC patients and healthy controls, while NLR has the highest AUC for distinguishing between severe UC and mild-to-moderate UC.
However, our study possesses certain limitations. It was conducted retrospectively at a solitary medical center and relied on a relatively small sample of UC patients. Furthermore, the data extraction was based on historical medical records from the hospital information system, and blood tests as well as endoscopies were not conducted simultaneously. Lastly, the study lacks external validation.
Conclusion
The study concluded that the levels of NLR and MHR were significantly higher in clinically active UC. Furthermore, the elevated levels of NLR and MHR served as predictors of endoscopic activity in UC patients. These assays could serve as a useful guide for assessing UC activity and mucosal damage, particularly when endoscopy is not feasible due to its easy application and affordability. We assert that NLR and MHR are indeed vital instruments for rapidly assessing UC clinical and endoscopic activity.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethical Statement
The study was approved by the hospital ethics committee of the Fifth Affiliated Hospital of Xinjiang Medical University (NO. XYDWFYLSH-2023-037). The study was retrospective in nature, maintained the confidentiality of all patient information, and has not adversely affect the health and rights of patients. Therefore, the committee waived the requirement for informed consent. The research adheres to the principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kucharzik T, Koletzko S, Kannengiesser K, Dignass A. Ulcerative colitis-diagnostic and therapeutic algorithms. Dtsch Arztebl Int. 2020;117(33–34):564–574. doi:10.3238/arztebl.2020.0564
2. Ge C, Lu Y, Shen H, Zhu L. Monitoring of intestinal inflammation and prediction of recurrence in ulcerative colitis. Scand J Gastroenterol. 2022;57(5):513–524. doi:10.1080/00365521.2021.2022193
3. Nardone OM, Shivaji UN, Ferruzza V, Ghosh S, Iacucci M. Soluble blood markers of mucosal healing in inflammatory bowel disease: the future of noninvasive monitoring. Inflamm Bowel Dis. 2020;26(6):961–969. doi:10.1093/ibd/izz226
4. Ricciuto A, Griffiths AM. Clinical value of fecal calprotectin. Crit Rev Clin Lab Sci. 2019;56(5):307–320. doi:10.1080/10408363.2019.1619159
5. Cioffi M, Rosa AD, Serao R, Picone I, Vietri MT. Laboratory markers in ulcerative colitis: current insights and future advances. World J Gastrointest Pathophysiol. 2015;6(1):13–22. doi:10.4291/wjgp.v6.i1.13
6. Giuffrida P, Corazza GR, Di Sabatino A. Old and new lymphocyte players in inflammatory bowel disease. Dig Dis Sci. 2018;63(2):277–288. doi:10.1007/s10620-017-4892-4
7. Liu Z, Tang H, Liang H, et al. Dyslipidaemia is associated with severe disease activity and poor prognosis in ulcerative colitis: a retrospective cohort study in China. Nutrients. 2022;14:15.
8. Torun S, Tunc BD, Suvak B, et al. Assessment of neutrophil-lymphocyte ratio in ulcerative colitis: a promising marker in predicting disease severity. Clin Res Hepatol Gastroenterol. 2012;36(5):491–497. doi:10.1016/j.clinre.2012.06.004
9. Yin X, Wu L, Yang H, Yang H. Prognostic significance of neutrophil-lymphocyte ratio (NLR) in patients with ovarian cancer: a systematic review and meta-analysis. Medicine. 2019;98(45):e17475. doi:10.1097/MD.0000000000017475
10. Ganjali S, Gotto AM, Ruscica M, et al. Monocyte-to-HDL-cholesterol ratio as a prognostic marker in cardiovascular diseases. J Cell Physiol. 2018;233(12):9237–9246. doi:10.1002/jcp.27028
11. Adir A, Braester A, Natalia P, et al. The role of blood inflammatory markers in the preoperative diagnosis of acute appendicitis. Int J Lab Hematol. 2023;46(1):58–62. doi:10.1111/ijlh.14163
12. Lin N, Li J, Yao X, et al. Prognostic value of neutrophil-to-lymphocyte ratio in colorectal cancer liver metastasis: a meta-analysis of results from multivariate analysis. Int J Surg. 2022;107:106959. doi:10.1016/j.ijsu.2022.106959
13. Pabla BS, Schwartz DA. Assessing severity of disease in patients with ulcerative colitis. Gastroenterol Clin North Am. 2020;49(4):671–688. doi:10.1016/j.gtc.2020.08.003
14. Ruscio MD, Cedola M, Mangone M, Brighi S. How to assess endoscopic disease activity in ulcerative colitis in 2022. Ann Gastroenterol. 2022;35(5):462–470. doi:10.20524/aog.2022.0732
15. Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2019;114(3):384–413. doi:10.14309/ajg.0000000000000152
16. Boal Carvalho P, Cotter J. Mucosal healing in ulcerative colitis: a comprehensive review. Drugs. 2017;77(2):159–173. doi:10.1007/s40265-016-0676-y
17. Lin H, Bai Z, Wu Q, et al. Inflammatory indexes for assessing the severity and disease progression of ulcerative colitis: a single-center retrospective study. Front Public Health. 2022;10:851295. doi:10.3389/fpubh.2022.851295
18. Mosli MH, Zou G, Garg SK, et al. C-reactive protein, fecal calprotectin, and stool lactoferrin for detection of endoscopic activity in symptomatic inflammatory bowel disease patients: a systematic review and meta-analysis. Am J Gastroenterol. 2015;110(6):802–819; quiz 820. doi:10.1038/ajg.2015.120
19. Yang Y, Xu Y, Wang J, Zhai X, Jiang H. Predictive efficacy of neutrophil-to-lymphocyte ratio for long-term prognosis in new onset acute coronary syndrome: a retrospective cohort study. BMC Cardiovasc Disord. 2020;20(1):500. doi:10.1186/s12872-020-01773-x
20. Fu H, Qin B, Hu Z, et al. Neutrophil- and platelet-to-lymphocyte ratios are correlated with disease activity in rheumatoid arthritis. Clin Lab. 2015;61(03+04/2015):269–273. doi:10.7754/clin.lab.2014.140927
21. Wei XB, Chen F, Huang JL, et al. Novel risk biomarker for infective endocarditis patients with normal left ventricular ejection fraction - monocyte to high-density lipoprotein cholesterol ratio. Circ J. 2017;82(1):283–288. doi:10.1253/circj.CJ-17-0427
22. Kanbay M, Solak Y, Unal HU, et al. Monocyte count/HDL cholesterol ratio and cardiovascular events in patients with chronic kidney disease. Int Urol Nephrol. 2014;46(8):1619–1625. doi:10.1007/s11255-014-0730-1
23. Drury B, Hardisty G, Gray RD, Ho GT. Neutrophil extracellular traps in inflammatory bowel disease: pathogenic mechanisms and clinical translation. Cell Mol Gastroenterol Hepatol. 2021;12(1):321–333. doi:10.1016/j.jcmgh.2021.03.002
24. Selby W, Jewell D. T lymphocyte subsets in inflammatory bowel disease: peripheral blood. Gut. 1983;24(2):99–105. doi:10.1136/gut.24.2.99
25. Catapano AL, Pirillo A, Bonacina F, Norata GD. HDL in innate and adaptive immunity. Cardiovasc Res. 2014;103(3):372–383. doi:10.1093/cvr/cvu150
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Study of the Correlation Between the Inflammatory Index and Disease Activity in Ulcerative Colitis
Chenfei Z, Ainiwaer Z, Xiaoling H
International Journal of General Medicine 2025, 18:7143-7152
Published Date: 29 November 2025