Back to Journals » International Journal of Women's Health » Volume 17
A Review on the Applications of Artificial Intelligence for Diagnosing and Treating Cervical Cancer
Received 6 July 2025
Accepted for publication 17 October 2025
Published 29 October 2025 Volume 2025:17 Pages 3955—3970
DOI https://doi.org/10.2147/IJWH.S551976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Yuzhang Wu,1,2 Aihong Wang3
1Department of Telecommunications Engineering and Management, Beijing University of Posts and Telecommunications, Beijing, People’s Republic of China; 2Queen Mary University of London, London, UK; 3Department of Obstetrics and Gynaecology, The Second Affiliated Hospital of Shandong First Medical University, Tai’an, Shandong, People’s Republic of China
Correspondence: Aihong Wang, Department of Obstetrics and Gynaecology, The Second Affiliated Hospital of Shandong First Medical University, Tai’an, Shandong, People’s Republic of China, Email [email protected]
Abstract: Cervical cancer (CC) is a malignant gynaecological tumour that poses a serious threat to the lives of patients worldwide. CC is the second-most common-cancer in women located in developing countries, following breast cancer. Therefore, given the persistently high incidence and mortality rates of CC, it is necessary to explore better diagnostic and treatment methods for this disease so that prevention and treatment strategies can be improved. As a science that develops computer programs to simulate, enhance, and extend human behaviours, artificial intelligence (AI) offers new possibilities for achieving this goal. In recent years, AI has shown considerable potential for accurately screening, diagnosing and treating cancer. For CC, the rapid development of AI provides new possibilities for performing early screening and achieving precise clinical diagnoses and treatments. This review is focused on the current state of research regarding the application of AI for the early screening, precise clinical diagnosis, and treatment of CC, as well as the challenges we will face in the future.
Keywords: artificial intelligence, deep learning, cervical cancer, screening, diagnosis, treatment
Introduction
Artificial intelligence (AI) is an interdisciplinary subject that is based on computer science and integrates biology, psychology, mathematics, philosophy and linguistics. AI involves the use of artificial methods and technologies to develop intelligent machines or systems, thereby simulating, extending and expanding human intelligence and achieving intelligent behaviours, such as understanding natural language, recognizing images, reasoning, and learning. In recent years, AI has become a popular branch of computer science. AI methods can be divided into four main categories: (1) pattern recognition, in which various forms of information presented by different objects and phenomena are analysed and processed, thus enabling their classification, evaluation and description;1 (2) machine learning (ML), in which the learning behaviour of the human brain is simulated and the knowledge framework is reorganized to improve the performance of the developed program;2 (3) data mining, in which relevant algorithms are used based on multiple databases to eliminate redundancy and extract key information fragments;3 and (4) intelligent algorithms, which apply specialized methods to solve specific problems, with ML and deep learning (DL) as the main approaches for achieving AI. ML is a subset of AI, whereas DL, which is a subset of ML, enables the automatic extraction of features and the processing of large, complex datasets. For example, convolutional neural networks (CNNs) are widely used in DL. A basic CNN consists of sequential layers, each of which applies a differentiable function to pass data to the next layers. Typically, CNNs include five main types of layers: convolutional, batch normalization, nonlinear mapping, pooling, and fully connected layers. Stacking these layers forms a complete CNN that can be fine-tuned for completing specific tasks4 (Figure 1). Through CNNs, convolutional operations and model training enable the application of AI in the medical field. Therefore, integrating AI with healthcare can significantly improve disease diagnoses and treatments.
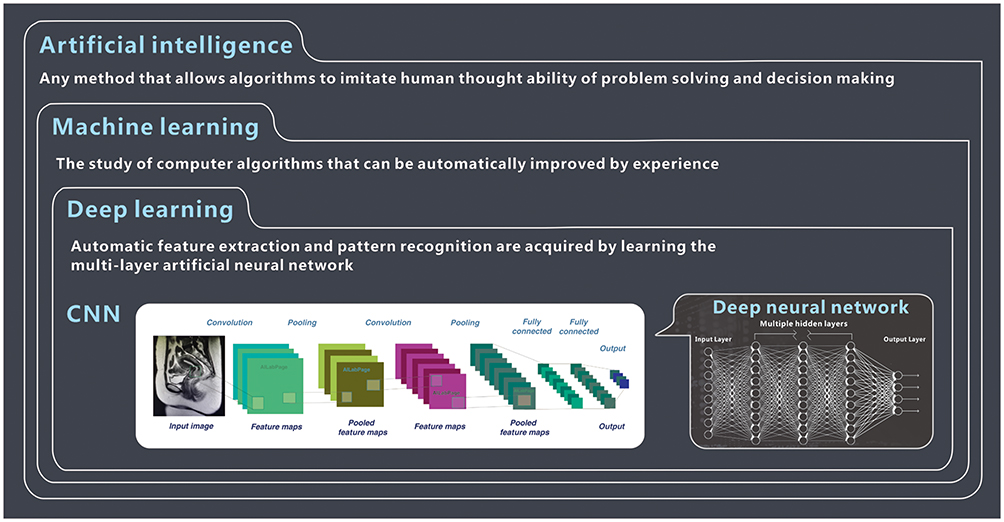 |
Figure 1 Main methods for achieving AI, ML and DL are the main methods for achieving AI. ML is a subset of AI, and DL is a subset of ML. CNNs are widely used in DL scenarios. The area selected by the green mark is the cervix of a cervical cancer patient. ML, machine learning; DL, deep learning; CNN, convolutional neural networks. |
Owing to the production of large amounts of medical data, an increasing number of medical fields have begun to use AI to assist in screening, diagnosing, treating and predicting prognoses for various diseases.3 As a result, AI has been successfully applied in image analysis scenarios, such as radiology and pathology, and for rapidly collating electronic medical records, optimizing the care trajectories experienced by chronic disease patients, etc. AI has become an important tool for accurately diagnosing diseases and designing better treatment plans. These methods have greatly improved diagnostic and treatment methods and increased the efficiency of diagnoses and treatments.5 Currently, malignant tumours are receiving increasing attention because of their increasing incidence and poor survival rates. Therefore, an increasing number of researchers are exploring the use of AI-related methods to optimize their treatment processes. AI has assumed a major role in diagnosing and treating malignant tumours, such as lung cancer,6 glioblastomas,7,8 breast cancer9 and prostate cancer.10 After a period of development, AI has paved a bright path for the continuing development of diagnostic and treatment methods and provides exciting opportunities for achieving precision oncology. Furthermore, the impact of AI on gynaecological oncology has also gradually received increasing amounts of attention.
Cervical cancer (CC), as a kind of gynaecological oncology, represents a major malignancy with serious implications for patient health and survival. With advances in computational technologies, artificial intelligence (AI) has been progressively applied to enhance the accuracy of diagnosis and the effectiveness of treatment in CC (Figure 2).
 |
Figure 2 AI has been applied in medical treatment cases, from tumours to gynaecological oncology and then to CC. |
According to the Global Cancer Epidemiology Database (GLOBOCAN) 2020 data released by the World Health Organization (WHO), CC ranks fourth among all cancers in terms of their global incidence and mortality rates among females.11 Eighty-five percent of cases occur in developing countries; in these countries, CC is one of the leading causes of cancer deaths in women. These data indicate that the threat posed by CC to patients’ lives should not be underestimated and that a comprehensive response plan is necessary. CC has become a great burden on society. AI is being applied in all aspects of the diagnosis, treatment, prognosis and follow-up processes undergone by CC patients (Table 1). Its application has led to new optimization solutions for CC.12
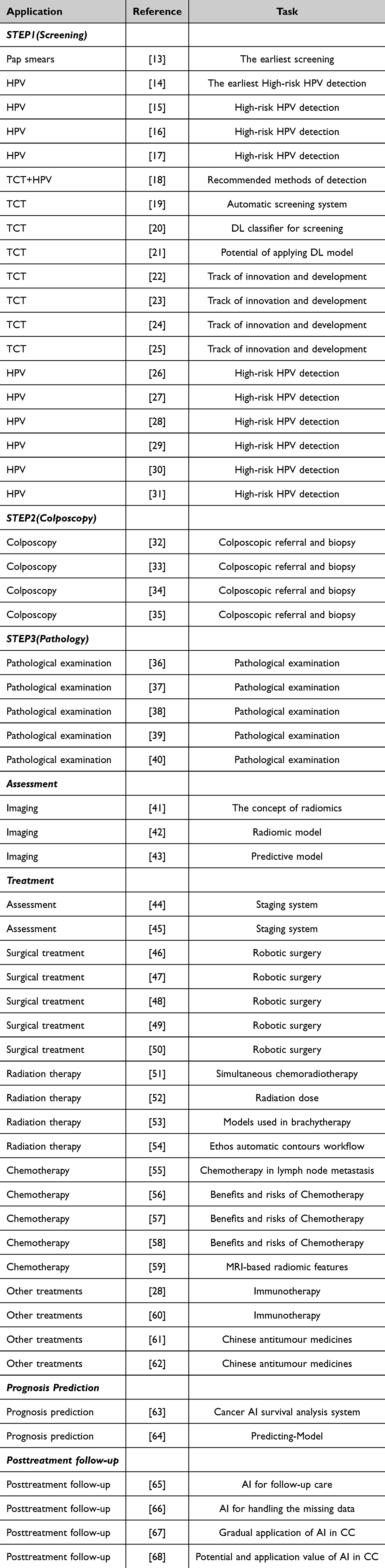 |
Table 1 Summary of Key Papers on the application of AI in CC. |
AI Combined with Early CC Screening and Diagnosis
The early detection of cancer, accurate cancer diagnosis, tumour classification, and tumour staging are key determinants of treatment decisions and patient outcomes. Cancer screening helps reduce the mortality rates of some common cancers.69,70 The treatment of precancerous lesions leads to a reduced incidence of invasive cancers.71 The most successful example of screening is the identification of precancerous lesions, such as the identification of adenomatous polyps via colorectal cancer screening and cervical intraepithelial neoplasia (CIN) via CC screening. CIN refers to a group of cervical lesions that are closely associated with invasive CC. CC screening is an effective method for detecting precancerous lesions and early-stage cancer. Screening, colposcopic referral and biopsy, and pathology confirmation are the three steps of the CC screening process (Figure 3). Through screening, cancerous and precancerous changes can be identified at an early stage, enabling timely diagnoses and treatments, which leads to better therapeutic outcomes.
 |
Figure 3 The three steps of the CC screening process: screening, colposcopic referral and biopsy, and pathology confirmation. TCT, Thinprep Cytologic Test; HPV, Human papilloma virus; NILM, Negative for intraepithelial lesion or malignancy; LSlL, Low-grade squamous intraepithelial lesion; HSIL, High-grade squamous intraepithelial lesion; CC, Cervical cancer; CIN, Cervical intraepithelial neoplasia. |
AI and Screening of CC
Screening is the first step of the whole three-step CC screening process. Many developed countries have implemented cytology-based screening programs since the middle of the 20th century, and the incidence of CC has been greatly reduced. A long period of sufficient development has been observed with respect to traditional CC screening. In 1941, Papanicolaou13 used Pap smears to conduct CC screening for the first time. In the 1990s, more sensitive and specific liquid-based thin-layer cytology examinations were used for CC screening purposes. Since Professor Howson14 discovered that human papillomavirus (HPV) can cause CC, HPV detection methods have also attracted attention. In 2012, the CC screening programs announced by the American Cancer Society (ACS), the US Preventive Services Task Force (USPSTF), and the American College of Obstetricians and Gynaecologists (ACOG) clearly defined the use of cytological examinations and combined screening methods. Over the years, the guidelines for the screening and treatment of cervical precancerous lesions have been continuously updated. Numerous studies have confirmed the practicability of HPV detection via CC screening.15–17 However, because not all types of CC are directly related to HPV infections, whether a cytological examination is justified or not needs to be weighed against its advantages and disadvantages, accounting for the patient’s financial situation, wishes, family history of tumours, and geographical and ethnic differences to achieve individualized screening. Therefore, high-risk HPV genotyping and liquid-based cytology are still widely recommended methods that are used worldwide.18 Recently, AI-based methods have greatly improved the efficiency of the inspection process and have advanced screening.
AI and Cytology Examination (Liquid-Based Thin-Layer Cytology Examination (TCT))
Cytology examination is one of the main CC screening methods. AI improves the accuracy of cytology examinations. After years of development and optimization, compared with traditional therapies, AI has demonstrated superiority in terms of diagnosing CC. In 1992, the United States developed the first commercial automatic screening system, ie, PAPNET.19 This innovation has attracted the attention of researchers worldwide, opening the door to AI-assisted cytological screening. The application of AI in TCT screening cases has subsequently become increasingly widespread. The employed methods are being continually improved to further enhance the advantages of AI in TCT examinations. For example, Wentzensen et al20 developed a DL classifier for the p16/Ki-67 double staining (DS) of cytology sections and used the biopsy-based gold standard for training. In addition, they developed a new image analysis platform based on DL in 2021, and after testing and verifying the platform in a large sample population, it was found that, compared with manual film reading, AI film reading had similar sensitivity rates and higher specificity (P<0.001). Compared with the methods that were widely used at that time, the new method demonstrated the potential of applying AI to assisted screening. Subsequently, Kanavati et al21 developed a DL model that could classify full-slide images of cytological samples. The research results revealed the reliability of this model for determining whether cytological images were derived from tumours or nontumours. Compared with previous methods, this finding further demonstrated the potential of applying DL to assisted screening. With the development of the economy and the increase in the level of investment, AI technology has gradually entered the fast track of innovation and development in the medical field.22 Owing to scientific and technological progress, the sensitivity of the CNN selected by Sanyal et al23 to identify abnormal lesions reached 95.63%, and the negative predictive value of the network reached 99.19%. Cao et al24 proposed a new DL method named the attention-based feature pyramid network, and the accuracy of this method reached 90.91%. Bao et al25 trained a supervised DL algorithm based on 188,542 digital cytological images in 2020 and evaluated its ability to detect CC or precancerous lesions. Different studies have shown the importance of AI in clinical settings. After undergoing repeated validations, the technology has become increasingly mature. Currently, some hospitals are already using AI-based screening technology, and the associated methods continue to be refined.
AI and HPV DNA Detection
High-risk HPV detection is another main CC screening method. Persistent infection with high-risk HPV is a necessary condition for HPV-related CC to develop. HPV16 and HPV18 infections account for approximately 71% of CC cases and are associated with the highest carcinogenesis risks,26,27 whereas the other HPV subtypes (HPV31, HPV33, HPV45, HPV52, and HPV58) account for approximately 19% of all CC cases.28 The detection of high-risk HPV has become one of the main CC screening methods, especially in HPV-related CC screening scenarios. Conducting large-scale HPV screening incurs a significant expense; therefore, research and innovations related to detection are important for reducing the global burden. Accordingly, followed by increased AI applications, an increasing number of CC prevention programs have used HPV testing as a primary screening tool.29 To automatically forecast HPV integration sites by learning environmental features, an attention-based DL model named DeepHPV was developed by Tian R et al.30 To train this model, a total of 3608 known HPV integration sites were applied, and 584 reviewed sites were used as the testing dataset. This study showed that DeepHPV can provide new insights into HPV integration preferences and mechanisms with the help of AI.30 In addition, via DL-based microholography, real-time high-risk HPV 16 or 18 detection can also be realized.31 In terms of detecting HPV 16 and 18 DNA from cell lines, this HPV DNA assay exhibited good sensitivity and specificity. Compared with the traditional method, with the help of AI this approach was 120-folder faster. This method provides a more efficient and convenient tool for detecting HPV. Currently, the tool greatly improves the efficiency of HPV screening while ensuring high accuracy. Research is still ongoing in various regions, and it is believed that the application prospects for future cervical screening methods are promising.
AI and the Diagnosis of CC
Diagnostic colposcopy and directed biopsy are key components of CC screening programs. Additionally, the traditional clinical diagnosis process requires clinicians to analyse medical images, such as computed tomography (CT), magnetic resonance (MR), and positron emission tomography (PET) images, on the basis of their professional knowledge and clinical experience. This process is time-consuming and involves subjectivity and limitations. The emergence of AI has changed this situation. In the field of image recognition, AI is objective, efficient, and rapid, and its advantages in diagnostic scenarios are gradually becoming evident.
AI and Colposcopy
Colposcopic referral and biopsy constitute the second step of the whole three-step CC screening process. The unprecedented progress achieved in AI has led to synergistic effects for DL and digital colposcopy, which provides an opportunity for developing automatic image-based diagnosis methods. Improving the accuracy and popularization of technology based on the traditional methods has become an important research topic for gynaecologists and engineering technologists worldwide. Xu et al32 trained a CNN on 1,000 cervical images, achieving an accuracy of 88.91% in terms of identifying precancerous lesions, with a sensitivity of 87.83% and specificity of 90.0%. Mercy et al33 developed a portable electronic colposcope based on DL from a clinical dataset consisting of 200 cases, which yielded a sensitivity of 81.3% and specificity of 78.6% with respect to distinguishing between normal and abnormal lesions, achieving an overall accuracy of 80.0%. These studies indicate that AI-assisted electronic colposcopy systems have the potential to serve as auxiliary diagnostic tools, thereby enhancing the diagnostic capabilities of physicians. Subsequently, Hu et al34 performed an automated visual assessment of cervical images captured by a contemporary digital camera. This study involved a population-based longitudinal cohort consisting of 9406 women aged 18–94 years in Guanacaste, Costa Rica, who were followed up for 7 years (1993–2000). Multiple cervical screening methods were used, and precancers were confirmed via histopathology. This program can be used to apply AI to cervical colposcopy, which will be helpful for effectively achieving immediate cervical screening, including in remote areas. Notably, AI technology can offer better solutions than can the traditional methods. AI effectively reduces the dependence on doctors and decreases their workloads. Therefore, an AI-related automated colposcopy workflow can create a new CC screening model and eventually accelerate the elimination of CC worldwide.35 AI applications in colposcopy have been piloted in some hospitals, and it is believed that AI can serve clinical work more widely in the future.
AI and Pathological Examinations
Pathology confirmation is the third step of the whole three-step CC screening process. The unprecedented progress achieved in ML has made synergy between AI and digital pathology possible. The integration of digital slides into pathology workflows, advanced algorithms and computer-aided diagnostic technology has expanded the horizons of pathologists beyond the microscopic level, and this strategy can truly utilize and integrate knowledge that goes beyond the limits and boundaries of humans.36 In addition, some studies have incorporated AI and ML tools into clinical oncology, focused on the development of biomarkers, and discussed some challenges associated with the use of AI, thus proposing potential future precision oncology opportunities.37 The traditional role of pathologists in terms of providing accurate diagnoses or assessing biomarkers for producing companion diagnostics may be enhanced by AI-driven analytical tools in terms of precision, reproducibility, and scale.38 Cho et al39 developed and validated models that can automatically classify CIN on the basis of histological examinations. The performances of two pretrained CNN models were evaluated and compared with those of pathologists. A total of 1106 images acquired from 588 patients were included in the test dataset. The authors concluded that the use of digital histological images is a promising tool for diagnosing CIN lesions.
Thus, the application of AI can help pathologists quickly identify lesion areas, avoid missed diagnoses, and attain improved diagnostic efficiency. In addition, An H et al developed an AI model based on HE slices that can directly predict P16-positive regions and high-grade squamous intraepithelial lesions (HSILs). The model can accurately distinguish between HSILs and low-grade squamous intraepithelial lesions (LSILs). The accuracy of the model was comparable to that of professional pathologists and even exceeded the accuracy of some doctors with low seniority levels. Additionally, we believe that this model has great potential as an auxiliary diagnostic tool. It can not only significantly improve the accuracy of diagnoses but also save time and costs during the diagnosis process.40 In summary, AI has considerable potential for clinical applications in pathology and is a reliable method for achieving precision medicine. Related research is ongoing in major hospitals, and it is believed that in the future, AI will be applied clinically, thus enabling CC patients to benefit from these studies.
AI and CC Imaging
Owing to the superior capabilities of AI in image processing, AI is playing an increasingly significant role in the evaluation and treatment of CC. AI has been applied in the medical imaging, treatment, posttreatment and follow-up stages (Figure 4). After a pathological diagnosis is obtained, imaging data can be integrated to initially determine the stage of the disease, thus enabling a precise treatment to be implemented based on the stage of the lesion.
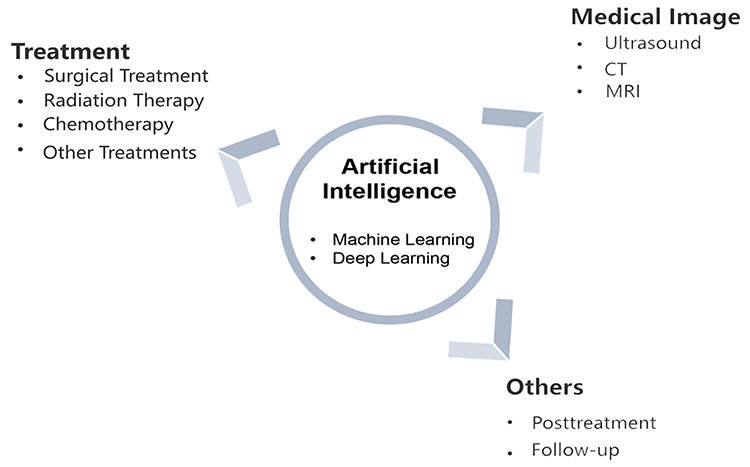 |
Figure 4 The applications of AI in medical imaging, treatment, posttreatment and follow-up. |
Ultrasound, CT, and MRI are the most commonly employed imaging methods. The concept of radiomics was first proposed by Gillies et al,41 who emphasized the extraction of information from imaging data to achieve tumour segmentation, feature extraction, and model development. AI is good at automatically identifying complex patterns and providing quantitative evaluations of imaging data, thus showing great potential for helping doctors obtain more accurate and repeatable results. Multiple studies have used this type of radiomics. For example, Yan et al42 conducted a study involving 190 eligible patients who were randomly divided into a training group (100 patients) and a validation group (90 patients). A radiomic model was then developed via logistic regression, and the model integrated handcrafted features, deep features, and squamous cell carcinoma antigen (SCC-Ag) levels. The performance of the model was evaluated and validated, with a focus on its calibration, discriminative ability, and clinical utility. The results indicated that the proposed radiomic model could effectively identify preoperative lymph node metastasis (LNM) in early-stage cutaneous squamous cell carcinoma (CSCC) patients, outperforming analyses executed based solely on SCC-Ag levels. This model represents a significant advancement regarding the identification of LNM in early CSCC patients by combining radiomic features with SCC-Ag levels. In addition, Dong et al43 conducted a study that included a cohort consisting of 226 pathologically confirmed operable CC patients from two academic medical institutions between December 2014 and November 2017. This dataset was randomly divided into a training set containing 176 patients and an independent testing set including 50 patients. Five radiomic features were selected to establish a radiomic signature, which was then combined with the preoperative tumour histology and grades of the patients. Baseline logistic regression (LRM) models and support vector machine (SVM) models were established for comparison purposes. The conclusion drawn from this study is that DL was utilized to create a comprehensive predictive model that incorporated the preoperative CT images, tumour histology, and grades of CC patients. Notably, the organic integration of AI and medical imaging-assisted diagnosis has led to the emergence of new radiomic methods, which quantify major diseases such as tumours by extracting a vast number of features from images, demonstrating significant clinical value.
Currently, AI is widely used in image processing systems in major hospitals, and related research is ongoing both domestically and internationally, with continuous improvements achieved with regard to application methods. It is believed that in the future, this technology can be better applied and used in medical treatment cases.
AI and CC Treatments
The personalization of CC treatments is guided by International Federation of Gynecology and Obstetrics (FIGO) staging. Currently, CC staging is based on the internationally standardized 2018 staging system with the TNM classification scheme as a reference.44 The main treatment options for CC include surgery, radiotherapy, chemotherapy and immunotherapy. Radical hysterectomy or pelvic lymphadenectomy is often used for early CC. However, advanced CC is associated with higher incidence rates of lymph node metastasis, local recurrence, and distant recurrence. It may be difficult to remove all tumours with normal tissue margins; therefore, radiotherapy and chemotherapy are used for treatment purposes.45
AI and Surgical Treatments
Surgery is an important treatment for CC. Robotic surgery, as a method of treatment that is assisted by AI, is a major innovation regarding the clinical application of AI. The US Food and Drug Administration approved the use of the da Vinci surgical robot for gynaecological surgery in 2005.46 In 2006, Sert B M et al47 reported the world’s first robotic radical hysterectomy performed for CC. With medical advancements, CC surgery has increasingly shifted toward minimally invasive approaches, marking a transitional progression from open surgery to laparoscopic procedures. In 2015, Sinno A K et al48 reported the world’s first robotic less-invasive surgery (R-LESS), ie, radical hysterectomy, for stage-IB1 CC, confirming its feasibility. In 2018, Vizza E et al49 reported 20 cases of extensive hysterectomy and pelvic lymphadenectomy performed via a single-port robot, with its average surgical time and blood loss comparable to those of multiport robots, indicating the feasibility and safety of this approach for treating early-stage CC. Additionally, Liu et al50 searched the MEDLINE, Cochrane Library, and Embase databases as well as the Journal of Robotic Surgery up to December 30, 2015, to identify controlled trials and observational studies that evaluated the superiority of robotic surgery over the traditional treatment methods for CC. Compared with open surgery, robotic surgery is more beneficial for CC patients in terms of their hospital stay lengths, complication rates, blood loss rates and blood transfusion effects. Compared with traditional surgical methods, robotic surgery has demonstrated significant advantages. Through research, evaluations, and improvements, robotic surgery has now been implemented in some hospitals. AI provides comprehensive and multilevel assistance for implementing surgical treatments. The existing technologies are already able to aid our surgical procedures, and in the future, AI will play an even more significant role in surgeries.
AI and Radiation Therapy
Radiation therapy is another important method for treating CC. All stages of CC can be treated with radiation therapy, especially stages IB3 and IVA. Simultaneously performing chemoradiotherapy in combination with therapy can be considered as an initial treatment.51 To ensure the effectiveness of this treatment, the radiation dose should be sufficient. Additionally, maximizing the protection of adjacent normal tissues and reducing the side effects of radiotherapy are necessary so that the quality of life experienced by patients can be improved.52 In recent years, great progress has been made regarding the use of AI in the field of radiation therapy, and ML and neural network models are now widely used in all aspects of brachytherapy. For example, Kerkhof et al53 significantly reduced the irradiated volumes of the bladder, rectum, small intestine, and sigmoid colon, which received 20–45 Gy during the definitive CC treatment through weekly MRI-guided adaptive radiotherapy. Additionally, MRI-based online adaptive radiotherapy technology has been applied in clinical settings. Furthermore, AI-based software that can automatically delineate anatomical target structures and define the location, size and shape of the radiation beam has been developed. The advantages of the proposed technique include improved treatment accuracy, as well as reduced time (from weeks to minutes) and human resource requirements for radiation therapy. In another example, Zhang Y et al54 compared the dosimetric results acquired from automatic oART plans and supervised oART plans to evaluate target volumes and organ-at-risk (OAR) dose changes. The treatments were replanned using the Ethos automatic contour workflow without manual contouring. They concluded that, for CC, the accuracy of automatic plans is clinically acceptable It is evident that AI, through advantages such as personalized treatment plans, automated processes, and real-time monitoring, fully leverages its supportive functions to increase the effectiveness and safety of CC radiotherapy. This procedure has been carried out in some hospitals, and it is believed that it will be more widely used in the future so that patients can receive better treatments.
AI and Chemotherapy
Chemotherapy is also one of the main methods for treating CC. Chemotherapy is particularly recommended for patients with external pelvic metastasis or patients with recurrent disease who are not suitable for radiotherapy or surgery. A retrospective analysis was conducted on the National Cancer Database including a total of 3053 postoperative patients in the early CC stage with high-risk factors. We can conclude that, compared with pure radiotherapy, concurrent chemoradiotherapy can significantly improve patient prognoses, especially for patients with lymph node metastasis.55 Chemotherapy plays an important role in improving the prognoses of advanced-stage gynaecologic cancer patients and lowering the risk of relapse in early-stage disease cases; nevertheless, balancing the benefits and risks of this approach remains challenging.56–58 Therefore, it is important to conduct pretreatment evaluations and avoid unnecessary chemotherapy. In a study conducted by Sun et al,59 a total of 275 patients with locally advanced CC (LACC) receiving neoadjuvant chemotherapy (NACT) were enrolled from eight hospitals and allocated to training and testing sets (at a 2:1 ratio) to investigate whether MRI-based pretreatment radiomic features could predict the clinical responses of LACC patients to NACT. The authors concluded that, compared with the previously developed methods, MRI-based radiomic features have the potential to predict the responses of LACC patients to NACT before treatment and can be used to identify appropriate targets for NACT and avoid unnecessary treatments. This study demonstrated the significant value of AI in chemical applications. AI assistance provides strong evidence for the selection and adjustment of chemotherapy plans, allowing for thorough analyses to be conducted through comprehensive evaluations and helping to reduce the frequency of unnecessary treatments for patients. Currently, this application is still in the research stage, and we hope that it will be better applied in clinical settings in the future.
AI and Other Treatments
The optimal treatment for a patient with recurrent CC should be selected on the basis of the patient’s health status, site of recurrence and/or metastasis, degree of metastasis, and first treatment measure. In a prior study, for patients with large primary tumours, the probability of pelvic recurrence or the persistence of pelvic lesions was greater than that for patients with distant metastasis.28 In this group of patients, the efficacy of combination drugs was superior to that of single drugs. Other drugs, such as the antiangiogenic agent bevacizumab and immune checkpoint inhibitors (PD-1/PD-L1 antibodies), can also be used. The applicability of AI in immunotherapy has been explored by researchers; for example, Li et al60 suggested that cancer immunotherapy is a method for controlling and eliminating tumours by reactivating the cancer immune cycle of the body and restoring its antitumour immune response. Their review offered a glimpse of the current AI applications in immunotherapy. We increasingly believe that these advancements will eventually make their way into the clinical setting, pushing AI forwards in the field of oncology.
Furthermore, the meridians of traditional Chinese medicine (TCM) are important theoretical guides for clinical antitumour treatments. Some studies have determined the intrinsic properties or meridian classifications of phytochemicals in Chinese herbal medicine (CHM) on the basis of AI tools. Researchers built ShennongAlpha, which is an AI-driven sharing and collaboration platform for the intelligent curation, acquisition, and translation of natural medicinal material knowledge.61
It is challenging to use existing technologies to characterize complex molecular structures with high heterogeneity. Chinese antitumour medicines are closely related to the lung, liver, stomach, and spleen meridians. These herbs exhibit different properties when used to treat several cancers. Certain types of cancers, such as ovarian cancer, bladder cancer, and CC, can occur simultaneously.62 Research related to the applicability of AI in other treatments is ongoing. We believe that in the future, AI-based TCM and other related diagnostic and treatment methods may also be applied and promoted for diagnosing and treating CC.
AI and Prognosis Prediction
With the extensive applications of AI in clinical practice, AI plays a key role in analysing diverse healthcare data to identify early signs of disease. Researchers are attempting to apply AI to predict the prognoses of CC patients. For example, Liang et al63 constructed a novel AI-based cancer survival analysis system to predict the individual death risk curves of CC patients receiving different treatments. The examined dataset (n = 14,946) was downloaded from the Surveillance Epidemiology and End Results database. Three types of algorithms were used to develop prognostic models for determining the cancer-specific survival outcomes of patients with cervical carcinoma. Mortality percentages at specific time points could be provided by this system, and the actual benefits provided by different treatments could be explored; these results could then be used to determine individualized treatments. In addition, Guo et al64 studied and developed an ML model for predicting the survival and recurrence rates of CC. These authors retrospectively collected data from 2006 to 2017 in four hospitals. Compared with the traditional models, their ML model might be a better analysis method for predicting the prognoses of CC patients because it can simultaneously predict survival rates and site-specific recurrence events. In addition, the novel calculator can provide helpful information for clinicians and develop personalized follow-up plans and treatment strategies. Although the applications of AI are still in the research stage, it is evident that AI has significant potential for predicting the prognoses of CC patients, thus providing a new impetus for its optimization.
AI and Posttreatment Follow-Ups
Studies have shown that patients receiving pelvic radiation therapy have developed radiation-induced second tumours,65 especially at radiation sites near the cervix (eg, the colon and rectum/anus). These patients should therefore be carefully monitored and closely followed for long periods. Both domestic and international research has shown that AI has advantages in follow-up care. For example, Guo et al64 retrospectively collected data on CC patients from 2006 to 2017 in four hospitals. The value of the variables in terms of predicting survival or recurrence was analysed via multivariate Cox, principal component, and K-means clustering analyses. The predictive performances of eight ML models were compared with those of logistic or Cox models. The authors studied and developed an ML model for predicting the survival rate and site-specific recurrence events of CC patients. This novel network calculator can provide useful information for clinicians and help them develop personal postoperative follow-up plans and further treatment strategies. Since missing data seriously affect the performance of ML models, Aljrees66 conducted a study to address the key challenge associated with handling missing data to achieve high accuracy. This work represents a valuable contribution to CC detection, which should eventually be aimed at reducing the impact of this disease on women’s health and the health care system. Notably, the application of AI in follow-up care has led to great convenience for patients. The current research, both domestically and internationally, continues to involve optimizing usage methods. At present, this application is still in the research stage. In the future, AI will surely be better applied in clinical settings to serve patients.
The diagnosis and treatment of CC is a worldwide problem. CC is one of the main diseases that threatens women’s health. Especially in low- and middle-income countries, its incidence and mortality rates remain high. To address this challenge, AI is rapidly becoming an important tool for improving the quality and efficiency of CC screening methods.
With the gradual application of AI in the diagnosis and treatment of CC,67 it has demonstrated great potential and application value in the prevention and early diagnosis of CC.68 Further research should support the development of AI methods for CC screening, including in low- and middle-income countries with limited resources. The application of AI in the diagnosis and treatment of CC is expected to have broader prospects.
Discussion
AI is a computer-based system that simulates human intelligence and is capable of performing tasks that normally require human intelligence, including perception, reasoning, learning, and natural language processing.72 ML is a subset of AI and the current mainstream AI training method, which uses algorithms to make computers learn from data.73 DL is a further subfield of ML that involves the use of deep neural networks (DNNs) to model complex patterns; the keys to DNNs are their multilayer connections among neurons, activation functions, and backpropagation mechanisms.74 However, AI is not “intelligent” in the strictest sense of the word (ie, in comparison with human intelligence). AI does not aim to allow machines to perform human intelligence tasks; thus, the machines do not think and cannot develop simple thoughts. Therefore, AI can only play a supporting role in the application process.
In the medical field, computer vision is important, and models based on CNNs play a crucial role in DL, especially in computer vision tasks.75 Furthermore, CNNs play an indispensable role in medical AI. A CNN is used to carry out convolutional operations, and then, computers are trained by a relevant model to realize the application of AI in the medical field. Thus, the deep integration of AI technology and the medical industry can greatly improve the diagnoses and treatments of many diseases. CC is a major global health problem, and AI technology has been widely used in the screening, diagnosis, treatment and prognosis of CC,12 breast cancer,76 lung cancer,6 prostate cancer77 and other cancers. However, AI technology still faces many challenges in practical applications. The first problem concerns data quality control.78 High-quality data are the key to research and development tasks. Although a large amount of clinical image data has been accumulated, it is difficult to guarantee the normalization, authenticity and accuracy of the data collection problem. The second problem involves data management.79 The annotation of image data requires considerable energy from pathologists. In the future, it will be necessary to establish multiple standardized data platforms for managing data systems. The third problem is the issue of AI compatibility. Clinical cervical cytology products are numerous, possess uneven quality, have different staining schemes, and entail diverse production methods; however, they also involve different scanner parameters, different types of colposcopy equipment, different descriptive terms and other issues. The fourth problem relates to diagnostic performance. Although AI systems are better at diagnosing cancer than primary colposcopists are, misdiagnoses and missed diagnoses can still result from the diagnostic process.80 The fifth problem is that the image classification performance of AI models needs to be further improved. For newly built models, before applying and promoting, a series of prospective clinical studies are urgently needed to verify their results. The sixth problem involves ethics. The interpretation of the diagnostic results produced by AI models often involves multiple fields, such as medical ethics, laws and regulations, and issues including how to ensure the privacy and security of patient data also need to be further clarified. Therefore, before DL tools can be clinically implemented, some ethical issues need to be resolved, thus enabling multiple parties to jointly learn through AI models while abiding by ethical rules.2
AI is being applied to the full-scale management process of CC, including screening, colposcopy, biopsy, pathological examination, diagnosis, treatment, prognosis, and follow-up care. In future studies, DL technology can be applied to multimodal CC data. Through the new multimodal feature fusion method, multimodal features can complement each other, and the tasks of classifying and diagnosing CC and precancerous lesions can be effectively improved. It is hoped that the government AI-assisted diagnosis system can achieve greater reliability, higher quality, more powerful management capabilities, stronger security, higher compatibility, and higher stability in the future to become suitable for various types of equipment and have better generalizability and clinical performance. The application of AI for the diagnosis and treatment of CC (Figure 5) is a promising future endeavour. Certainly, this plan still requires the government to increase its level investment and supervision, medical institutions to conduct in-depth research and improve the levels of diagnoses and treatments, and the people to trust and participate in these subjects.
 |
Figure 5 AI is being applied throughout the entire process of diagnosing and treating CC. |
Conclusions
In conclusion, early detection, early diagnosis, accurate classification and early treatment are key factors for reducing the mortality of CC. Although many problems and challenges remain, AI has exhibited considerable potential for accurately screening and diagnosing cancer and guiding treatments. Collaborative networks within and between hospitals might give a method to integrate AI into clinical practice. On November 17, 2020, the WHO released the “Global Strategy to Accelerate the Elimination of Cervical Cancer”. AI has excelled in image analysis tasks and will soon play an important role in improving the implementation of CC screening, management, and follow-up schemes. It is believed that in the future, with the joint efforts of the government, medical institutions and patients, AI will open a new chapter in modern diagnosis and treatment method, play a major role in standardizing the diagnosis and treatment processes applied to CC, and eventually accelerate the global elimination of this disease.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Deo RC. Machine learning in medicine. Circulation. 2015;132(20):1920–1930. PMID: 26572668; PMCID: PMC5831252. doi:10.1161/CIRCULATIONAHA.115.001593
2. Wu WT, Li YJ, Feng AZ, et al. Data mining in clinical big data: the frequently used databases, steps, and methodological models. Mil Med Res. 2021;8(1):44. PMID: 34380547; PMCID: PMC8356424. doi:10.1186/s40779-021-00338-z
3. Chen ZH, Lin L, Wu CF, Li CF, Xu RH, Sun Y. Artificial intelligence for assisting cancer diagnosis and treatment in the era of precision medicine. Cancer Commun. 2021;41:1100–1115. doi:10.1002/cac2.12215
4. Krizhevsky A, Sutskever I, Hinton GE, Simoncelli EP. Imagenet classification with deep convolutional neural networks. Adv Neural Inf Process Syst. 2012;25:3113–3121.
5. Miller DD, Brown EW. Artificial intelligence in medical practice: the question to the answer? Am J Med. 2018;131:129–133. doi:10.1016/j.amjmed.2017.10.035
6. Avanzo M, Stancanello J, Pirrone G, et al. Radiomics and deep learning in lung cancer. Strahlenther Onkol. 2020;196(10):879–887. doi:10.1007/s00066-020-01625-9
7. Way GP, Sanchez-Vega F, La K, et al. Machine learning detection of pancancer as pathway activation in cancer Genome Atlas. Cell Rep. 2018;23:172–180. doi:10.1016/j.celrep.2018.03.046
8. Itakura H, Achrol AS, Mitchell LA, et al. Magnetic resonance image features identify glioblastoma phenotypes subtypes with distinct molecular pathway activities. Sci Transl Med. 2015;7:303ra138. doi:10.1126/scitranslmed.aaa7582
9. Guo J, Hu J, Zheng Y, Zhao S, Ma J. Artificial intelligence: opportunities and challenges in the clinical applications of triple-negative breast cancer. Br J Cancer. 2023;128:2141–2149. doi:10.1038/s41416-023-02215-z
10. Ström P, Kartasalo K, Olsson H, et al. Artificial intelligence for diagnosis and grading of prostate cancer in biopsies: a population-based, diagnostic study. Lancet Oncol. 2020;21:222–232. doi:10.1016/S1470-2045(19)30738-7
11. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
12. Shen WC, Chen SW, Wu KC, et al. Prediction of local relapse and distant metastasis in patients with definitive chemoradiotherapy-treated cervical cancer by deep learning from 18F-fluorodeoxyglucose positron emission tomography/computed tomography. Eur Radiol. 2019;29:6741–6749. doi:10.1007/s00330-019-06265-x
13. Papanicolaou GN, Traut HF. The diagnostic value of vaginal smears in carcinoma of the uterus. 1941. Arch Pathol Lab Med. 1997;121(3):211–224. PMID: 9111103.
14. Zur Hausen H. Papillomaviruses and cancer: from basic studies to clinical application. Nat Rev Cancer. 2002;2(5):342–350. PMID: 12044010. doi:10.1038/nrc798
15. Bhatla N, Singhal S. Primary HPV screening for cervical cancer. Best Pract Res Clin Obstet Gynaecol. 2020;65:98–108. doi:10.1016/j.bpobgyn.2020.02.008
16. Zhang J, Zhao Y, Dai Y, et al. Effectiveness of high-risk human papillomavirus testing for cervical cancer screening in China: a multicentre, open-label, randomized clinical trial. JAMA Oncol. 2021;7(2):263–270. doi:10.1001/jamaoncol.2020.6575
17. Li ZF, Jia XH, Feng X, et al. Comparison of primary cytology, primary HPV testing and co-testing as cervical cancer screening for Chinese women: a population-based screening cohort. BMJ Open. 2022;12(10):e063622. doi:10.1136/bmjopen-2022-063622
18. Zhang S, Xu H, Zhang L, Qiao Y. Cervical cancer: epidemiology, risk factors and screening. Chin J Cancer Res. 2020;32:720–728. doi:10.21147/j.issn.1000-9604.2020.06.05
19. Mango LJ. Computer-assisted cervical cancer screening using neural networks. Cancer Lett. 1994;77(2–3):155–162. doi:10.1016/0304-3835(94)90098-1
20. Wentzensen N, Lahrmann B, Clarke MA, et al. Accuracy and efficiency of deep-learning-based automation of dual stain cytology in cervical cancer screening. J Natl Cancer Inst. 2021;113(1):72–79. doi:10.1093/jnci/djaa066
21. Kanavati F, Hirose N, Ishii T, et al. A deep learning model for cervical cancer screening on liquid-based cytology cimens in whole slide images. Cancers. 2022;14(5):1159. doi:10.3390/cancers14051159
22. Rajpurkar P, Chen E, Banerjee O, et al. AI in health and medicine. Nat Med. 2022;28(1):31–38. doi:10.1038/s41591-021-01614-0
23. Sanyal P, Barui S, Deb P, et al. Performance of a convolutional neural network in screening liquid based cervical cytology smears. J Cytol. 2019;36(3):146–151. doi:10.4103/JOC.JOC_201_18
24. Cao L, Yang J, Rong Z, et al. A novel attention-guided convolutional network for the detection of abnormal cervical cells in cervical cancer screening. Med Image Anal. 2021;73:102197. doi:10.1016/j.media.2021.102197
25. Bao H, Bi H, Zhang X, et al. Artificial intelligence-assisted cytology for detection of cervical intraepithelial neoplasia or invasive cancer: a multicenter, clinical-based, observational study. Gynecol Oncol. 2020;159(1):171–178. doi:10.1016/j.ygyno.2020.07.099
26. Waxman AG, Chelmow D, Darragh TM, et al. Revised terminology for cervicalhistopathology and its implications for management of high-grade squamousintraepithelial lesions of the cervix. Obstetrics Gynecol. 2012;120(6):1465–1471. doi:10.1097/AOG.0b013e31827001d5
27. World Health Organization. Human papillomavirus vaccines: WHO positionpaper, May 2017-recommendations. Vaccine. 2017;35(43):5753–5755. doi:10.1016/j.vaccine.2017.05.069
28. Bhatla N, Aoki D, Sharma DN, et al. Cancer of the cervix uteri:2021 update. Int J Gynaecol Obstet. 2021;155(Suppl 1):28–44. doi:10.1002/ijgo.13865
29. Marth C, Landoni F, Mahner S, McCormack M, Gonzalez-Martin A, Colombo N. Cervical cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28:iv72–83. doi:10.1093/annonc/mdx220
30. Tian R, Zhou P, Li M, et al. DeepHPV: a deep learning model to predict human papillomavirus integration sites. Brief Bioinform. 2021;22(4):bbaa242. PMID: 33059369. doi:10.1093/bib/bbaa242
31. Pathania D, Landeros C, Rohrer L, et al. Point-of-care cervical cancer screening using deep learning-based microholography. Theranostics. 2019;9(26):8438–8447. PMID: 31879529; PMCID: PMC6924258. doi:10.7150/thno.37187
32. Xu T, Zhang H, Huang X, et al. Multimodal deep learning for cervical dysplasia diagnosis. In:
33. Asiedu MN, Simhal A, Chaudhary U, et al. Development of algorithms for automated detection of cervical pre-cancers with a low-cost, point-of-care, pocket colposcope. IEEE Trans Biomed Eng. 2019;66(8):2306–2318. PMID: 30575526; PMCID: PMC6581620. doi:10.1109/TBME.2018.2887208
34. Hu L, Bell D, Antani S, et al. An observational study of deep learning and automated evaluation of cervical images for cancer screening. J Natl Cancer Inst. 2019;111:923–932. doi:10.1093/jnci/djy225
35. Xue P, Ng MTA, Qiao Y. The challenges of colposcopy for cervical cancer screening in LMICs and solutions by artificial intelligence. BMC Med. 2020;18:169. doi:10.1186/s12916-020-01613-x
36. Niazi MKK, Parwani AV, Gurcan MN. Digital pathology and artificial intelligence. Lancet Oncol. 2019;20:e253–61. doi:10.1016/S1470-2045(19)30154-8
37. Bera K, Schalper KA, Rimm DL, Velcheti V, Madabhushi A. Artificial intelligence in digital pathology - new tools for diagnosis and precision oncology. Nat Rev Clin Oncol. 2019;16:703–715. doi:10.1038/s41571-019-0252-y
38. Baxi V, Edwards R, Montalto M, Saha S. Digital pathology and artificial intelligence in translational medicine and clinical practice. Mod Pathol. 2022;35:23–32. doi:10.1038/s41379-021-00919-2
39. Cho BJ, Kim JW, Park J, et al. Automated diagnosis of cervical intraepithelial neoplasia in histology images via deep learning. Diagnostics. 2022;12(2):548. PMID: 35204638; PMCID: PMC8871214. doi:10.3390/diagnostics12020548
40. An H, Ding L, Ma M, et al. Deep learning-based recognition of cervical squamous interepithelial lesions. Diagnostics. 2023;13(10):1720. PMID: 37238206; PMCID: PMC10217662. doi:10.3390/diagnostics13101720
41. Gillies RJ, Anderson AR, Gatenby RA, et al. The biology underlying molecular imaging in oncology:from genome to anatome and back again. Clin Radiol. 2010;65:517–521. doi:10.1016/j.crad.2010.04.005
42. Yan L, Yao H, Long R, et al. A preoperative radiomics model for the identification of lymph node metastasis in patients with early-stage cervical squamous cell carcinoma. Br J Radiol. 2020;93(1116):20200358. PMID: 32960673; PMCID: PMC7715994. doi:10.1259/bjr.20200358
43. Dong T, Yang C, Cui B, et al. Development and validation of a deep learning radiomics model predicting lymph node status in operable cervical cancer. Front Oncol. 2020;10:464. doi:10.3389/fonc.2020.00464
44. Olawaiye AB, Baker TP, Washington MK, Mutch DG. The new (Version 9) American Joint Committee on Cancer tumor, node, metastasis staging for cervical cancer. CA Cancer J Clin. 2021;71(4):287–298. PMID: 33784415. doi:10.3322/caac.21663
45. Kokka F, Bryant A, Olaitan A, et al. Hysterectomy with radio⁃therapy or chemotherapy or both for women with locally advanced cervi⁃ cal cancer. Cochrane Database Syst Rev. 2022;8(8):CD010260. doi:10.1002/14651858.CD010260.pub3
46. Lee PS, Bland A, Valea FA, et al. Robotic-assisted laparoscopic gynecologic procedures in a fellowship training program. J Soc Laparoendosc Surg. 2009;13(4):467–472. doi:10.4293/108680809X12589998403921
47. Sert BM, Abeler VM. Robotic-assisted laparoscopic radical hysterectomy (Piver type III) with pelvic node dissection—case report. Eur J Gynaecol Oncol. 2006;27(5):531–533.
48. Sinno AK, Tanner EJ. Robotic laparoendoscopic single site radical hysterectomy with sentinel lymph node mapping and pelvic lymphadenectomy for cervical cancer. Gynecol Oncol. 2015;139(2):387. doi:10.1016/j.ygyno.2015.08.012
49. Vizza E, Chiofalo B, Cutillo G, et al. Robotic single site radical hysterectomy plus pelvic lymphadenectomy in gynecological cancers. J Gynecol Oncol. 2018;29(1):e2. doi:10.3802/jgo.2018.29.e2
50. Liu Z, Li X, Tian S, Zhu T, Yao Y, Tao Y. Superiority of robotic surgery for cervical cancer in comparison with traditional approaches: a systematic review and meta-analysis. Int J Surg. 2017;40:145–154. doi:10.1016/j.ijsu.2017.02.062
51. Monk BJ, Tewari KS, Koh WJ. Multimodality therapy for locally advanced cervical carcinoma:state of the art and future directions. J Clin Oncol. 2007;25(20):2952–2965. doi:10.1200/JCO.2007.10.8324
52. Pötter R, Tanderup K, Schmid MP, et al. MRIguided adaptive brachytherapy in locally advanced cervical cancer (EMBRACE-I):a multicentre prospective cohort study. Lancet Oncol. 2021;22(4):538–547. doi:10.1016/S1470-2045(20)30753-1
53. Kerkhof EM, Raaymakers BW, van der Heide UA, van de Bunt L, Jürgenliemk-Schulz IM, Lagendijk JJ. Online MRI guidance for healthy tissue sparing in patients with cervical cancer: an IMRT planning study. Radiother Oncol. 2008;88(2):241–249. PMID: 18490068. doi:10.1016/j.radonc.2008.04.009
54. Zhang Y, Wang G, Chang Y, et al. Prospects for daily online adaptive radiotherapy for cervical cancer: auto-contouring evaluation and dosimetric outcomes. Radiat Oncol. 2024;19(1):6. PMID: 38212767; PMCID: PMC10785518. doi:10.1186/s13014-024-02398-6
55. Trifiletti DM, Swisher-McClure S, Showalter TN, et al. Postoperative chemoradiation therapy in high-risk cervical cancer:re-evaluating the findings of Gynecologic Oncology Group Study 109 in a large, population-based cohort. Int J Radiat Oncol Biol Phys. 2015;93(5):1032–1044. doi:10.1016/j.ijrobp.2015.09.001
56. Lheureux S, Braunstein M, Oza AM. Epithelial ovarian cancer: evolution of management in the era of precision medicine. CA Cancer J Clin. 2019;69(4):280–304. doi:10.3322/caac.21559
57. Oseledchyk A, Leitao MM, Konner J, et al. Adjuvant chemotherapy in patients with stage I endometrioid or clear cell ovarian cancer in the platinum era: a surveillance, epidemiology, and end results cohort study, 2000–2013. Ann Oncol. 2017;28(12):2985–2993. doi:10.1093/annonc/mdx525
58. Huang H, Feng YL, Wan T, et al. Effectiveness of sequential chemoradiation vs concurrent chemoradiation or radiation alone in adjuvant treatment after hysterectomy for cervical cancer: the STARS Phase 3 randomized clinical trial. JAMA Oncol. 2021;7(3):361–369. doi:10.1001/jamaoncol.2020.7168
59. Sun C, Tian X, Liu Z, et al. Radiomic analysis for pretreatment prediction of response to neoadjuvant chemotherapy in locally advanced cervical cancer: a multicentre study. EBioMedicine. 2019;46:160–169. doi:10.1016/j.ebiom.2019.07.049
60. Li T, Li Y, Zhu X, et al. Artificial intelligence in cancer immunotherapy: applications in neoantigen recognition, antibody design and immunotherapy response prediction. Semin Cancer Biol. 2023;91:50–69. doi:10.1016/j.semcancer.2023.02.007
61. Yang Z, Yin Y, Kong C, et al. ShennongAlpha: an AI-driven sharing and collaboration platform for intelligent curation, acquisition, and translation of natural medicinal material knowledge. Cell Discov. 2025;11(1):32. PMID: 40169534; PMCID: PMC11961663. doi:10.1038/s41421-025-00776-2
62. Zhang S, Zhang X, Du J, Wang W, Pi X. Multi-target meridians classification based on the topological structure of anti-cancer phytochemicals using deep learning. J Ethnopharmacol. 2024;319:117244. doi:10.1016/j.jep.2023.117244
63. Liang J, He T, Li H, Guo X, Zhang Z. Improve individual treatment by comparing treatment benefits: cancer artificial intelligence survival analysis system for cervical carcinoma. J Transl Med. 2022;20:293. doi:10.1186/s12967-022-03491-8
64. Guo C, Wang J, Wang Y, et al. Novel artificial intelligence machine learning approaches to precisely predict survival and site-specific recurrence in cervical cancer: a multi-institutional study. Transl Oncol. 2021;14:101032. doi:10.1016/j.tranon.2021.101032
65. Chaturvedi AK, Kleinerman RA, Hildesheim A, et al. Second cancers after squamous cell carcinoma and adenocarcinoma of the cervix. J Clin Oncol. 2009;27(6):967–973. doi:10.1200/JCO.2008.18.4549
66. Tong W, Eric L, Zhao F, Basu P, Qiao Y. Cancer biology & medicine. Cancer Biol Med. 2024;21(10):864–879. doi:10.20892/j.issn.2095-3941.2024.0198
67. Liu L, Liu J, Su Q, Chu Y, Xia H, Xu R. Performance of artificial intelligence for diagnosing cervical intraepithelial neoplasia and cervical cancer: a systematic review and meta-analysis. EClinicalMedicine. 2024;80:102992. PMID: 39834510; PMCID: PMC11743870. doi:10.1016/j.eclinm.2024.102992
68. Aljrees T. Improving prediction of cervical cancer using KNN imputer and multi-model ensemble learning. PLoS One. 2024;19:e0295632. doi:10.1371/journal.pone.0295632
69. Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365:395–409.
70. Byers T, Wender RC, Jemal A, Baskies AM, Ward EE, Brawley OW. The American cancer society challenge goal to reduce US cancer mortality by 50% between 1990 and 2015: results and reflections. CA Cancer J Clin. 2016;66:359–369. doi:10.3322/caac.21348
71. Corley DA, Jensen CD, Marks AR, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014;370:1298–1306. doi:10.1056/NEJMoa1309086
72. McCarthy J, Minsky ML, Rochester N, et al. A proposal for the dartmouth summer research project on artificial intelligence, August 31, 1955. AI Magazine. 2006;27(4):12.
73. Samuel AL. Some studies in machine learning using the game of checkers. IBM J Res Develop. 1959;3(3):210–229. doi:10.1147/rd.33.0210
74. LeCun Y, Bottou L, Bengio Y, et al. Gradient-based learning applied to document recognition. Proc IEEE. 1998;86(11):2278–2324. doi:10.1109/5.726791
75. Kadhim YA, Khan MU, Mishra A. Deep learning-based computer-aided diagnosis (CAD): applications for medical image datasets. Sensors. 2022;22:8999. doi:10.3390/s22228999
76. Balkenende L, Teuwen J, Mann RM. Application of deep learning in breast cancer imaging. Semin Nucl Med. 2022;52(5):584–596. doi:10.1053/j.semnuclmed.2022.02.003
77. Munir K, Elahi H, Ayub A, et al. Cancer diagnosis using deep learning:a bibliographic review. Cancers. 2019;11(9):1235. doi:10.3390/cancers11091235
78. Obermeyer Z, Emanuel EJ. Predicting the future-big data, machine learning, and clinical medicine. N Engl J Med. 2016;375(13):1216–1219. doi:10.1056/NEJMp1606181
79. Bi WL, Hosny A, Schabath MB, et al. Artificial intelligence in cancer imaging: clinical challenges and applications. CA Cancer J Clin. 2019;69(2):127–157. doi:10.3322/caac.21552
80. Li JB, Jiang ZF. Establishment and its application of Chinese society of clinical oncology artificial intelligence system (CSCO AI). Zhonghua Yi Xue Za Zhi. 2020. 100(6):411–415. [Chinese]. PMID: 32146762. doi:10.3760/cma.j.issn.0376-2491.2020.06.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nanotechnology: A Promising Approach for Cancer Diagnosis, Therapeutics and Theragnosis
Dessale M, Mengistu G, Mengist HM
International Journal of Nanomedicine 2022, 17:3735-3749
Published Date: 26 August 2022
Updated Perspectives on the Diagnosis and Management of Onychomycosis
Falotico JM, Lipner SR
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1933-1957
Published Date: 15 September 2022
A Post-International Gastrointestinal Cancers’ Conference (IGICC) Position Statements
Yalcin S, Lacin S, Kaseb AO, Peynircioğlu B, Cantasdemir M, Çil BE, Hurmuz P, Doğrul AB, Bozkurt MF, Abali H, Akhan O, Şimşek H, Sahin B, Aykan FN, Yücel İ, Tellioğlu G, Selçukbiricik F, Philip PA
Journal of Hepatocellular Carcinoma 2024, 11:953-974
Published Date: 29 May 2024
Automatic Real-Time Detection and Diagnosis of Liver Tumor with Ultrasound

Wu CH, Sheu JC, Chou PL, Lee J, Nien HC
Journal of Hepatocellular Carcinoma 2025, 12:1599-1611
Published Date: 23 July 2025
Artificial Intelligence in the Diagnosis and Management of Pulmonary Tuberculosis: A Review of Current Applications and Future Perspectives
Ou Y, Zhang Q, Meng C, Zhou X, Na M, Yu Z, Ma W, Huang C
Therapeutics and Clinical Risk Management 2026, 22:596651
Published Date: 31 March 2026