Back to Journals » International Journal of Women's Health » Volume 17
A Qualitative Study on Barriers and Facilitators to Postpartum Cardiovascular Disease Risk Screening in Women with Hypertensive Disorders of Pregnancy: Perspectives from Patients and Healthcare Providers
Authors Zhang Y ![]() , Jiang Y, Sun S, Jiang L, Yu W, Hu J, Ji X
, Jiang Y, Sun S, Jiang L, Yu W, Hu J, Ji X
Received 23 September 2025
Accepted for publication 5 December 2025
Published 11 December 2025 Volume 2025:17 Pages 5329—5342
DOI https://doi.org/10.2147/IJWH.S569780
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Yan Zhang,1,* Yuyu Jiang,1,* Shijing Sun,1 Ling Jiang,1 Wei Yu,2 Jun Hu,3 Xiuming Ji1
1Department of Nursing, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou, People’s Republic of China; 2Department of Obstetrics, Suzhou Women and Children’s Healthcare Hospital, Suzhou, People’s Republic of China; 3Department of Urology, Changshu No.2 People’s Hospital, Changshu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Hu, Department of Urology, Changshu No.2 People’s Hospital, No. 18 Taishan Road, Changshu, 215501, People’s Republic of China, Email [email protected] Xiuming Ji, Department of Nursing, The Affiliated Suzhou Hospital of Nanjing Medical University, No. 26 Daoqian Street, Suzhou, 215002, People’s Republic of China, Email [email protected]
Purpose: To explore the barriers and facilitators to postpartum cardiovascular disease (CVD) risk screening among women with hypertensive disorders of pregnancy (HDP) from both patient and healthcare provider perspectives, with the aim of informing clinical screening strategies, optimizing postpartum care services, and improving maternal health outcomes.
Patients and Methods: This study employed purposive sampling and was conducted between February and May 2025 at a tertiary hospital in Suzhou, Jiangsu Province, China. Semi-structured, one-on-one interviews were conducted with 15 women diagnosed with HDP at 3– 12 months postpartum. In addition, focus group interviews were held with nine healthcare providers from the obstetrics department and community health centers (CHCs, primary care facilities in China). A content analysis approach was used to analyze the qualitative data.
Results: Three themes and twelve subthemes emerged: (1) Limited perception of CVD risk, poor ability to screen and apply health information, fear-driven avoidance behavior, conflicting role priorities, and economic burden are individual barriers; (2) lack of guidance from healthcare providers, fragmented and unstandardized postpartum care system are system-level barriers; (3) family history of hypertension, emphasis on personal health, strong family support, and positive experience with past interventions are promoting factors that encourage women to get screened.
Conclusion: Postpartum CVD risk screening in women with HDP remains inadequate. Strengthening transitional care, integrating structured screening into postpartum guidelines, expanding insurance coverage, and enhancing digital health and provider training are essential to close clinical gaps and improve long-term cardiovascular outcomes.
Keywords: hypertensive disorders of pregnancy, cardiovascular disease, postpartum, barriers, facilitators, qualitative research
Introduction
Hypertensive disorders of pregnancy (HDP), encompassing preeclampsia/eclampsia, chronic hypertension, superimposed preeclampsia, and gestational hypertension, affect about 10% of pregnancies worldwide,1 with a prevalence of 5.22–5.57% in China and a rising trend.2 HDP substantially contributes to maternal and perinatal morbidity and mortality,3 predisposes women to recurrence in later pregnancies,4 and has lasting health implications. Approximately 30–40% of women with severe preeclampsia progress to chronic hypertension within the first year after delivery.5 Compared with women who remain normotensive during pregnancy, those with HDP have nearly a four-fold greater likelihood of developing chronic hypertension within 6–12 months postpartum and a two-to three-fold higher risk of cardiovascular disease (CVD) within 15 years.6,7 Elevated risks of diabetes8 and end-stage renal disease9 are also well documented, both of which significantly contribute to maternal CVD burden. The American Heart Association (AHA) classifies HDP as a major cardiovascular and cerebrovascular risk factor, and the 2019 AHA/American College of Cardiology guideline for primary prevention of CVD identifies preeclampsia as a risk-enhancing factor.10 Consequently, reducing cardiometabolic risks and safeguarding the long-term health of women with a history of HDP are an urgent priority in both clinical care and public health.
CVD risk screening includes risk biomarkers (blood pressure, lipid, and glucose levels), lifestyle-related factors (diet, physical activity, smoking, alcohol use, weight management, sleep, and mental health), and female-specific factors such as reproductive history.11 For women with HDP, routine postpartum follow-up and CVD risk screening are crucial for early identification of risk and for preventing, delaying, or controlling the onset and progression of CVD. The 2023 European Society of Hypertension Guidelines12 recommend annual evaluations with regular blood pressure monitoring and cardiovascular risk assessment for this population. In China, the Expert Consensus on Comprehensive Cardiovascular Risk Management in HDP13 advises assessments at 42 days, 8–12 weeks, 6 months, and 12 months postpartum, along with lifestyle counseling to mitigate long-term risk. Nevertheless, postpartum CVD risk screening in practice remains inadequate. A cohort of 566,059 women14 found that only 18% of those with HDP attended a postpartum follow-up within six months. Similarly, a Chinese study15 reported blood pressure follow-up rates of just 24.26% at 42 days and 50.37% at three months postpartum. Together, these findings underscore a major missed opportunity for postpartum counseling, risk screening, and intervention in this high-risk group.
In recent years, multiple studies16,17 have used quantitative methods to investigate postpartum follow-up and its determinants among women with HDP, while some have also examined patients’ needs and experiences regarding postpartum risk counseling. A Norwegian study18 found that women with HDP valued such counseling and were motivated to adopt healthier lifestyles. Research from Australia19 identified both barriers and facilitators to postpartum CVD prevention in primary care. Moreover, a meta-analysis revealed that women with HDP often have limited awareness of the association between HDP and future CVD risk, which restricts the adoption of health-promoting behaviors.20
In China, changes in reproductive policies and evolving attitudes toward childbirth have contributed to a rise in high-risk pregnancies, including HDP and gestational diabetes mellitus. Yet, clinical care remains largely centered on intrapartum management, with limited emphasis on postpartum CVD risk. Evidence on how Chinese women with HDP experience CVD risk screening during the first postpartum year is scarce. Gaining insight into these experiences is essential to identify facilitators that could enhance current practice and to reveal systemic gaps, thereby guiding the design of feasible interventions. Accordingly, this study sought to examine, from both patient and healthcare provider perspectives, the current practices, barriers, and facilitators of postpartum CVD risk screening among women with HDP, aiming to inform clinical strategies and improve long-term maternal health outcomes.
Materials and Methods
Study Design
This study adopted a descriptive qualitative design,21 which is particularly suitable for research areas with limited prior knowledge. This approach allows for an in-depth exploration of participants’ subjective experiences without the constraints of rigid theoretical frameworks. For this research, HDP patients and medical staff as would be selected as interview subjects to explore the barriers and promoting factors of postpartum CVD risk screening in patients. The study was conducted and reported in accordance with the Standards for Reporting Qualitative Research (SRQR) guidelines.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Affiliated Suzhou Hospital of Nanjing Medical University (No. K-2025-185-K01). The researchers strictly adhered to the principles of voluntary participation and confidentiality, and formal interviews commenced only after participants provided written informed consent, which included permission for the use of anonymized responses and direct quotations in publications. All participants were assigned unique identification codes (eg, patients: P1, P2; healthcare providers: N1, N2) to replace personal identifiers in interview transcripts and analyses. Any incidental references to third parties during the interviews were edited prior to data analysis. Access to the raw data was restricted solely to the research team.
Researcher Characteristics and Reflexivity
All interviews were conducted by the first author, a Master’s-trained nurse with formal training in qualitative research methods and clinical experience in high-risk pregnancy care. During data collection, the first author maintained a reflexive journal to document personal assumptions and potential biases and to examine how these factors might influence interview interactions and data interpretation.
Participants
Purposive sampling was used to recruit postpartum women with HDP from the outpatient clinic of a tertiary hospital in Suzhou, Jiangsu Province, China, between February and May 2025, as well as healthcare providers from obstetrics, cardiology, and community health centers. Patients were recruited via clinician referrals and notices posted on the outpatient bulletin board. Recruitment materials clearly outlined participants’ rights and responsibilities and provided contact information for the research team.
Inclusion/Exclusion Criteria
Inclusion criteria for patients were: (1) HDP as the discharge diagnosis; (2) age ≥ 20 years; (3) 3–12 months postpartum; and (4) fully conscious and able to articulate their perspectives clearly. Exclusion criteria included: (1) cognitive impairment; (2) severe postpartum complications or other major physical illnesses; and (3) current pregnancy.
Inclusion criteria for healthcare providers were: (1) a bachelor’s degree or higher; (2) ≥7 years of work experience; (3) direct involvement in obstetric wards or community healthcare; and (4) good communication and expression skills. Exclusion criteria included staff on study leave, sick leave, or otherwise not actively working.
Sampling
During patient sampling, the principle of maximum variation was applied, considering differences in age, educational level, gestational age at delivery, and family history of hypertension. This strategy aimed to ensure a representative sample and enhance the diversity of the data. The sample size was based on the principle of data saturation, that is, the interviews ended when no new themes emerged during the time of data analysis.
Research Process
Development of the Interview Guide
The interview guides were initially developed through literature review and internal discussions within the research team. Prior to formal interviews, pilot interviews were conducted with four postpartum women with HDP and three healthcare providers who met the inclusion criteria. Insights from the pilot interviews were used to refine the guides, and data from the pilot interviews were excluded from the final analysis. The revised guides were validated by two experts in qualitative research methods, resulting in the finalized interview guides for both HDP patients and healthcare providers.
The finalized patient interview guide included the following questions: (1) Are you aware that HDP may have long-term effects on cardiovascular health postpartum? Through which sources did you obtain this information? (2) What methods do you currently use to monitor your cardiovascular health after delivery? (3) How important do you think postpartum cardiovascular risk screening is in preventing future CVD? (4) What are the reasons for participating or not participating in CVD risk screening during the postpartum period? (5) Are there any barriers that limit your decision to undergo CVD risk screening, or are there factors that encourage you to participate? (6) Do your family, friends, or other relevant individuals support your engagement in postpartum cardiovascular risk screening? How do their attitudes influence your decision? (7) Based on your experience, what changes do you think are needed to improve postpartum CVD risk screening for women with HDP?
The finalized interview guide for healthcare providers included the following questions: (1) Based on your clinical experience, how do you perceive the postpartum cardiovascular risk in women with HDP? (2) In your practice, do you proactively monitor the cardiovascular health of these patients after delivery? If so, how do you implement this? If not, what are the reasons? (3) How is postpartum CVD risk screening conducted for HDP patients in your hospital or community setting? How is it implemented? (4) What factors facilitate or hinder the performance of postpartum cardiovascular risk screening for HDP patients in clinical practice? (5) In your opinion, which aspects of postpartum CVD risk screening need improvement?
Data Collection
Patient interviews were conducted individually, face-to-face, using a semi-structured format. Participants were contacted in advance to schedule interviews, which took place in private, quiet rooms to ensure a comfortable and natural environment. Before the interviews, the study purpose, procedures, and confidentiality measures were explained, and written informed consent was obtained. Each interview lasted 30–40 minutes and was audio-recorded, with concurrent note-taking that captured participants’ expressions, demeanor, and tone. The interviewer encouraged participants to express themselves fully, avoided leading questions or interruptions, and clarified ambiguous statements through probing, follow-up questions, or paraphrasing to ensure the accuracy and completeness of the data.
Healthcare provider data were collected through a single focus group comprising nine participants. The first author served as the moderator, assisted by a graduate student and supervised by an experienced nursing researcher. The focus group was held in a private room, and participants provided consent for audio recording. The moderator introduced relevant guidelines and expert consensus, explained the study purpose, and facilitated discussion based on the interview guide. All opinions were treated without judgment. The session concluded once data saturation was achieved, ie, when no new codes or themes emerged.
Data Analysis
Interview data were coded, organized, and synthesized using NVivo 11. Directed content analysis was applied to systematically analyze and integrate the data.22 The analytical procedure was as follows: Two researchers (Y.Z. and Y.J.) repeatedly read the interview transcripts to achieve immersion and gain a comprehensive understanding of the content. Line-by-line analysis was conducted to identify meaningful statements, followed by open coding. Similar or related codes were compared and grouped to gradually develop themes and subthemes. Themes, subthemes, and codes were clearly defined, and representative examples were extracted from the data. Finally, the findings were returned to participants for member checking to verify the accuracy and credibility of the identified content.
Results
A total of 15 postpartum women with HDP and 9 healthcare providers participated in the interviews. Participants were assigned unique identifiers: patients were coded as P1 to P15, and healthcare providers as N1 to N9. The mean age of patients was 30.9 years (SD = 4.8), and that of healthcare providers was 40.4 years (SD = 6.4). Tables 1 and 2 summarize the demographic characteristics of the patients and healthcare providers, respectively. Table 3 outlines the themes and subthemes, supported by illustrative quotes and interpretations.
 |
Table 1 Demographic and Clinical Characteristics of Postpartum Women with HDP (n=15) |
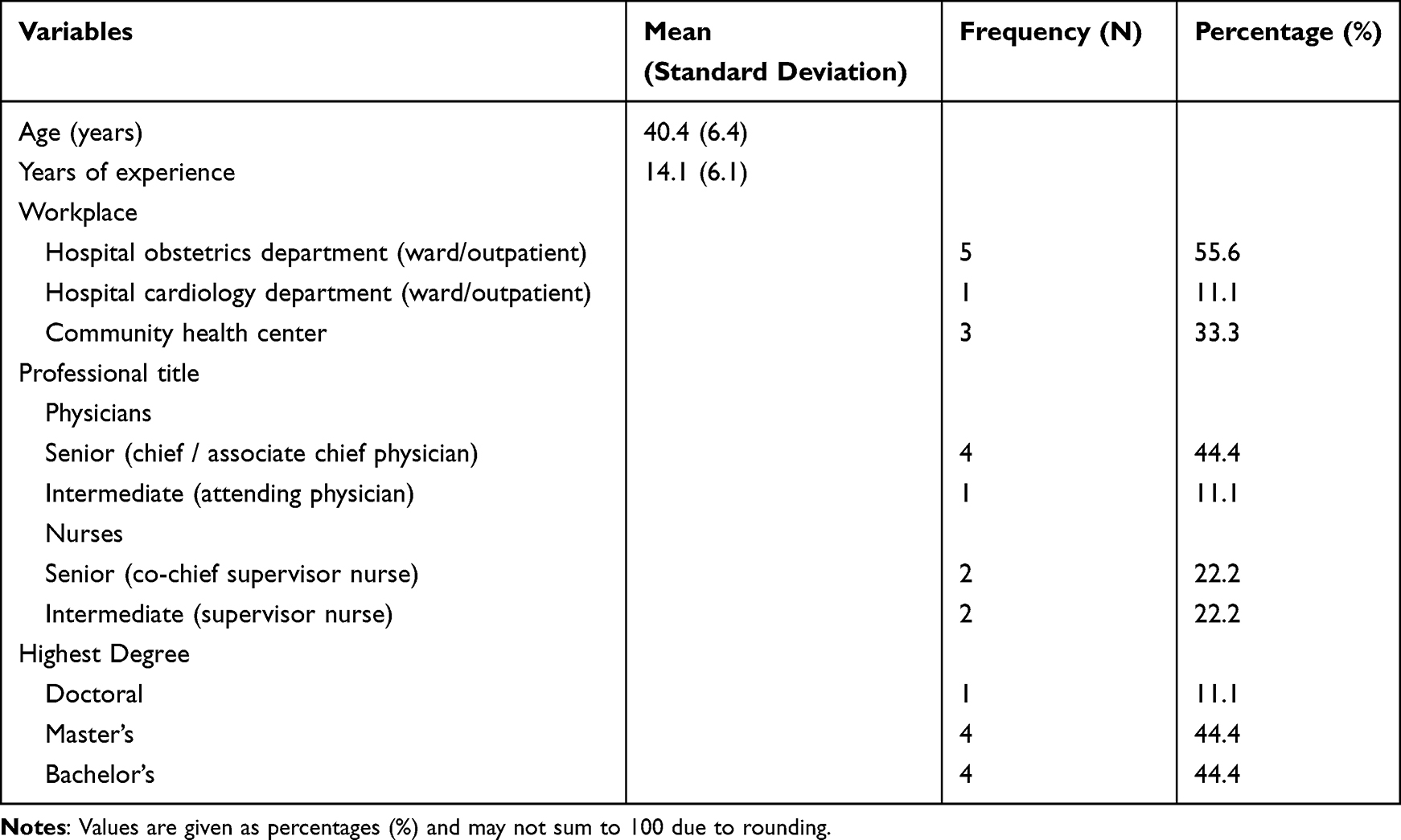 |
Table 2 Characteristics of Participating Healthcare Providers (n=9) |
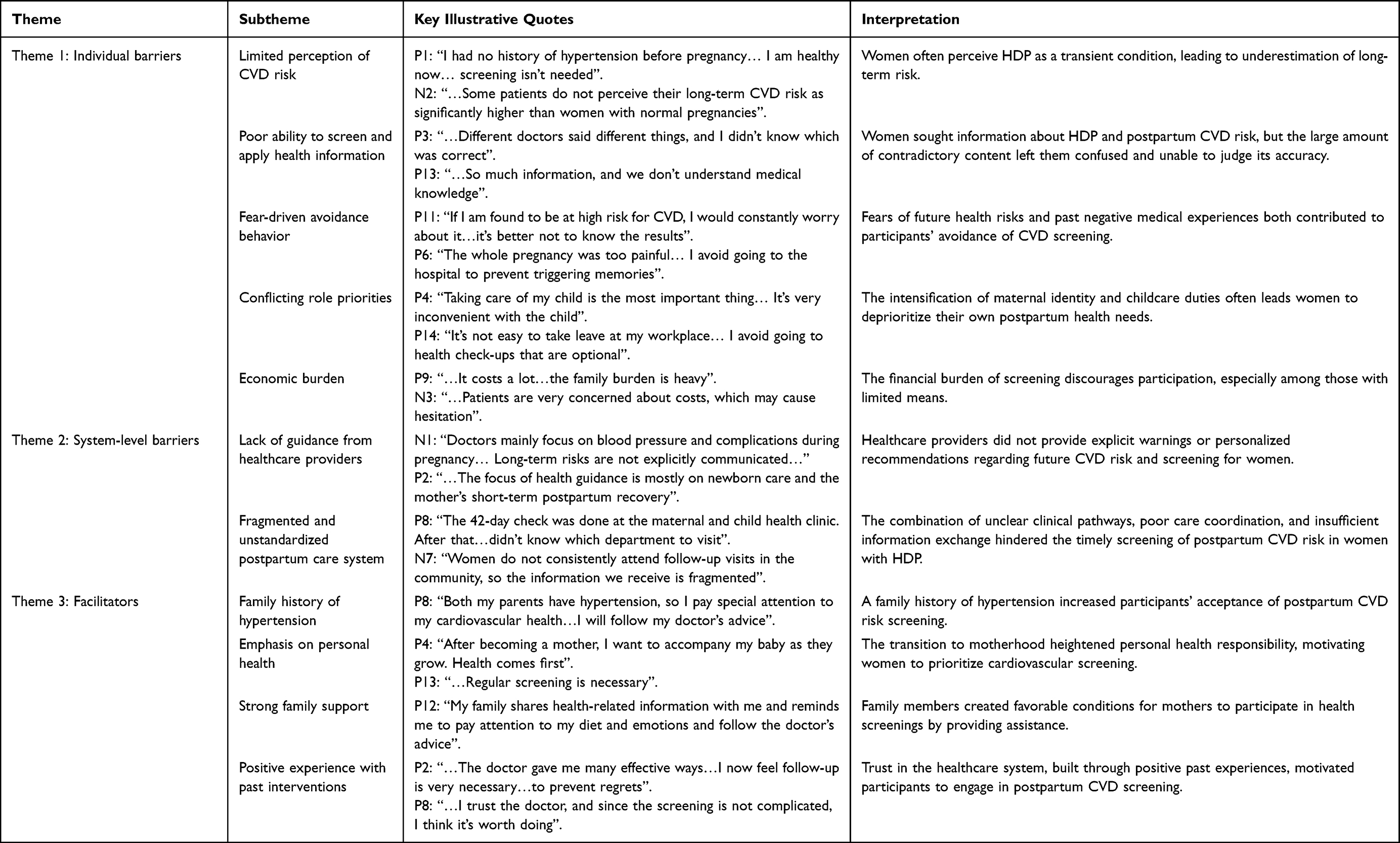 |
Table 3 Barriers and Facilitators to Postpartum CVD Risk Screening: Themes, Subtheme, Key Illustrative Quotes, and Interpretations |
Theme 1: Individual Barriers
Limited Perception of CVD Risk
Some participants perceived HDP and preeclampsia as transient, pregnancy-related conditions, believing that the risk disappears after delivery rather than recognizing them as independent risk factors for future CVD. Consequently, they considered postpartum screening or follow-up unnecessary.
P1:I had no history of hypertension before pregnancy. My blood pressure increased in late pregnancy and was controlled with medication. By the third day after delivery, my blood pressure returned to normal, and I am healthy now. There may be some risk, but I do not think I will develop cardiovascular disease, so screening is not needed.
P5:During the 42-day postpartum check, my blood pressure was within the normal range. There’s no need to spend extra money on additional screening.
N2:I tell my patients that postpartum follow-up and CVD risk screening are important. However, in my experience, very few actually undergo screening. Some patients do not perceive their long-term CVD risk as significantly higher than women with normal pregnancies, and some think I am exaggerating. Even those with pre-existing hypertension before pregnancy often have low risk awareness.
P9:Although I have hypertension, I usually have no symptoms. Conditions like coronary heart disease or heart failure only appear when people get older, right?
Poor Ability to Screen and Apply Health Information
A few participants reported that they had searched for or consulted information regarding HDP and postpartum CVD risk screening. However, faced with a large volume of often contradictory information, they experienced confusion and difficulty evaluating its accuracy and relevance. As a result, the information remained at the “knowledge” level but did not translate into actionable behavior.
P3:I looked online to see if I should have a follow-up. Different doctors said different things, and I did not know which was correct. In the end, I just measured my blood pressure at home and occasionally went to the hospital or community for screening.
P13:There is so much information, and we do not understand medical knowledge, so it’s hard to tell what’s right or wrong.
Fear-Driven Avoidance Behavior
Some participants avoided CVD screening and discussions due to the fear of being identified as high-risk, which would require long-term follow-up and lifestyle changes.
P11:If I am found to be at high risk for CVD, I would constantly worry about it, which adds a lot of stress. I feel it’s better not to know the results.
P15:As long as I go to the hospital, there are always various problems. If I do not get checked, there will not be any issues. Sometimes you cannot fully trust what doctors say.
Some healthcare providers noted that negative experiences during delivery or postpartum care led women to avoid returning to hospitals or community health centers.
P6:The whole pregnancy was too painful. My baby stayed in the hospital for so long. I try not to recall that period. Within this year, unless the baby needs it, I avoid going to the hospital to prevent triggering memories.
N8:If patients have experienced one or two difficult medical encounters, they are indeed resistant to subsequent healthcare visits.
Conflicting Role Priorities
During the early postpartum period, maternal role identity often reaches its peak, and personal health needs are frequently placed secondary to the well-being of the infant and family. For employed women, work and childcare occupy most of their time, leading to the indefinite postponement or neglect of self-care activities, such as scheduling appointments or attending follow-ups.
P4:Taking care of my child is the most important thing. If I go out for a check-up, it takes at least half a day. Sometimes the results are not ready, and I have to go again the next day. It’s very inconvenient with the child.
P14:It’s not easy to take leave at my workplace. Unless the child is sick or there’s an urgent family matter, I avoid going to health check-ups that are optional.
Economic Burden
Direct medical costs (eg, registration fees, examination fees, and medications) and potential indirect costs (eg, transportation expenses and lost wages) together constitute an economic barrier to participation in screening, particularly for those with limited financial resources.
P9:Every time I go to the hospital, it costs a lot. Various examination fees are expensive, and medications are not cheap. Now I also have to take care of my child, so the family burden is heavy.
P10:If this screening requires blood tests or an ultrasound, it costs at least several hundred yuan, all out-of-pocket. Only my husband earns money in our family, so I have to consider the finances.
N3:Some postpartum HDP patients have abnormal blood pressure, lipids, or glucose. As a physician, I need to inform them of potential health risks and the need for regular monitoring, but patients are very concerned about costs, which may cause hesitation.
Theme 2: System-Level Barriers
Lack of Guidance from Healthcare Providers
This study found that some healthcare providers did not provide explicit warnings or personalized recommendations regarding future CVD risk and screening for women after delivery and during subsequent follow-up.
N1:Doctors mainly focus on blood pressure and complications during pregnancy and hospitalization after delivery. Long-term risks are not explicitly communicated to the mothers. If the mother or family members ask about monitoring or medication afterward, we usually suggest consulting internal medicine or visiting community institutions.
N5:During discharge follow-up, we ask about the mother’s blood pressure recovery and breastfeeding status, but we do not proactively tell them to undergo regular CVD risk screening. Mainly, we are not confident in this area of knowledge, and if we say something incorrect, it may lead to disputes.
P2:Whether at the delivery hospital or the community health center, the focus of health guidance is mostly on newborn care and the mother’s short-term postpartum recovery. There was no detailed explanation about long-term CVD risks and regular screening.
P14:Maybe the doctors and nurses briefly mentioned it during my hospitalization, but I was physically weak, and the environment was noisy. They could not go into detail, and I do not remember anything about it.
Fragmented and Unstandardized Postpartum Care System
Both women and healthcare providers described the postpartum care system as fragmented, lacking a structured pathway for cardiovascular follow-up among women with a history of HDP. After completing the routine 42-day postpartum check, many women felt abruptly “disconnected” from the healthcare system, uncertain about where to seek ongoing CVD risk assessment or which department was responsible for their care. Even when women attempted to seek follow-up, logistical barriers such as complex or poorly synchronized appointment systems further impeded engagement.
P8:The 42-day check was done at the maternal and child health clinic. After that, I wanted to undergo CVD risk screening but did not know which department to visit. I ended up scheduling an appointment with obstetrics, and the doctor then referred me to cardiology.
P12:I prefer to go back to the hospital where I registered during my pregnancy, but I need to book an appointment in advance. Sometimes I forget to do so, or I cannot get a suitable time slot. It would be better if the hospital information system could provide reminders.
Healthcare providers similarly highlighted inconsistencies and ambiguity in postpartum care responsibilities. Obstetricians, cardiologists, and community health workers lacked clear role delineation, with no standardized mechanisms for transitioning patients from one setting to another. Providers also noted that postpartum visits in maternal and child health clinics predominantly focused on lactation and pelvic floor rehabilitation, with little attention given to cardiovascular risk assessment or related counseling.
N1:In practice, we do not even see the results of the 42-day postpartum check. Beyond that, the patient is no longer under obstetrics. Cardiology or community healthcare institutions should take over this work.
N6:In maternal and child health clinics, most consultations are about breastfeeding or pelvic floor rehabilitation. We have never received inquiries about CVD risk screening, and we have not provided related education or risk communication.
Fragmentation was further compounded by poor coordination and limited information exchange between tertiary hospitals and community health service centers. Many women doubted whether community hospitals had the capacity to conduct CVD screening or provide appropriate follow-up, leading them to bypass primary care entirely.
P4:Our community hospital is very basic, with only a few doctors. If some examinations or treatments cannot be done there, I still have to go to a tertiary general hospital. It’s better to go to the big hospital directly from the start.
Community providers also expressed challenges due to fragmented clinical information and inconsistent follow-up attendance.
N7:Women do not consistently attend follow-up visits in the community, so the information we receive is fragmented, and community management is somewhat disorganized.
N9:There is poor linkage between community hospitals and the maternity hospitals where women delivered. We cannot access pregnancy and delivery information, which makes it difficult to follow up on postpartum care for women with HDP.
Overall, these accounts illustrate a fragmented and unstandardized postpartum care system, in which unclear pathways, poor coordination, and inadequate information sharing collectively hindered timely postpartum CVD risk screening for women with HDP.
Theme 3: Facilitators
Family History of Hypertension
Several participants with a family history of hypertension highlighted how this background influenced their acceptance of postpartum CVD risk screening, shaping their perceptions and motivating behavior change.
P3:My grandmother died of coronary heart disease, and my blood pressure was already abnormal before pregnancy. This preterm birth experience made me more aware of the importance of blood pressure control, so I monitor my blood pressure regularly and consult doctors about medication use.
P8:Both my parents have hypertension, so I pay special attention to my cardiovascular health. Developing preeclampsia was a warning for me. I will follow my doctor’s advice and undergo regular screening for early detection and intervention.
Emphasis on Personal Health
Following childbirth, which was described as a major life transition, some participants demonstrated a heightened sense of personal health responsibility. This awareness motivated them to prioritize time and resources for postpartum CVD risk screening.
P4:After becoming a mother, I want to accompany my baby as they grow. Health comes first, so no matter how busy I am with work, I make time to visit the hospital.
P13:After giving birth, I felt my body was much weaker than before. With age, health problems will arise, so regular screening is necessary. Cardiovascular diseases are so common nowadays.
Strong Family Support
Participants highlighted the importance of family members, particularly spouses and parents, in facilitating health-promoting behaviors. Emotional encouragement and practical support, such as childcare assistance or accompaniment to medical visits, were described as critical enablers of postpartum CVD risk screening.
P10:My husband takes my health seriously. He takes responsibility for caring for our child and reminds me to attend check-ups on time.
P12:My family shares health-related information with me and reminds me to pay attention to my diet and emotions and follow the doctor’s advice.
Positive Experience with Past Interventions
Positive past experiences, such as timely detection of health problems during prenatal check-ups and subsequent effective interventions, strengthened participants’ belief in the value of screening. These experiences motivated them to engage in postpartum CVD risk screening.
P2:During my prenatal check-up, I was told that my blood sugar was high. The doctor gave me many effective ways to control it, which helped me avoid gestational diabetes. I now feel follow-up is very necessary—if screening identifies risks, adjustments can be made in time to prevent regrets.
P8:At my 3-month postpartum visit, my body mass index was found to be 31.4 kg/m2, which is considered obese. The doctor advised me to control my weight through diet and exercise. I trust the doctor, and since the screening is not complicated, I think it’s worth doing.
Discussion
This study represents the first qualitative investigation in China to examine the barriers and facilitators to postpartum CVD risk screening among women with HDP, integrating perspectives from both patients and healthcare providers. Three overarching themes emerged: individual-level barriers, system-level barriers, and facilitators. These findings indicate that postpartum screening behaviors are shaped by a complex interplay of cognitive, emotional, social, and organizational factors, rather than being solely the result of individual choice. Understanding these determinants is crucial for developing interventions that effectively enhance postpartum cardiovascular health in this high-risk population.
At the individual level, insufficient risk perception and limited capacity to access, filter, and apply health information are major barriers. Most women with HDP did not recognize the link between elevated blood pressure during pregnancy and long-term cardiovascular risk, which contributed to low awareness and neglect of postpartum screening, consistent with Roth et al.23 Even when patients actively sought information, the specialized nature and volume of medical content made it challenging for those without a medical background to distinguish credible guidance from misinformation. This often resulted in indecision, delays, or avoidance of screening. In China, patients generally perceive information from higher-level hospitals as the most credible and trustworthy,24 highlighting the importance of authoritative guidance in promoting adherence to recommended follow-up practices. However, our findings indicate that healthcare providers often placed limited emphasis on postpartum CVD screening, exhibited inconsistent knowledge regarding relevant procedures, and lacked confidence in patient education. In some cases, providers failed to proactively inform women about long-term CVD risks. Addressing this gap requires providing healthcare professionals with accessible resources, evidence-based training, and opportunities to update knowledge on postpartum CVD risk management. Clinicians should also recognize their critical role in promoting lifelong health, enhance their professional responsibility, and actively engage in patients’ health throughout the reproductive life course. These efforts can improve patients’ understanding of their own health, strengthen their ability to interpret and apply health information, and ultimately increase participation in postpartum CVD risk screening.
Fear emerged as a critical emotional barrier influencing postpartum screening behaviors. Some women avoided CVD screening to mitigate psychological stress associated with potentially unfavorable results (“fear of results”) or due to previous traumatic birth experiences (“trauma-related avoidance”). This avoidance behavior represents a protective psychological mechanism rather than disregard for health. Postpartum posttraumatic stress disorder (PTSD), defined as a mental disorder arising after exposure to traumatic events during pregnancy or postpartum, including complications, traumatic births, or high neonatal risk,25 has been shown to be associated with heavy medical histories, previous gynecological disorders, and preeclampsia.26 Consistently, some women in our study deliberately avoided settings, personnel, or situations related to childbirth, which hindered follow-up. According to the fear-avoidance model, adverse medical experiences may trigger catastrophic thinking, hypervigilance, and excessive fear, which prompt avoidance as a coping strategy. Over time, such avoidance can lead to unfavorable health outcomes, which further reinforce fear, creating a vicious cycle.27 Healthcare providers should carefully assess women’s psychological status during the perinatal period, deliver humanistic care, and improve the overall childbirth and healthcare experience. Simultaneously, they should provide clear, accurate, and feasible strategies for postpartum CVD risk management to reduce psychological burden, correct misconceptions, and break the fear-avoidance cycle.
System-level barriers centered around fragmented and unstandardized postpartum care system. Our findings suggest that women’s difficulties stem not from two independent problems, but from a single overarching issue—fragmented postpartum care system—characterized by unclear pathways, poor referral coordination, and lack of information continuity across healthcare settings. Similar challenges have been reported in England, where fragmented systems compromise postpartum care.28 Establishing standardized, integrated transitional care models is urgently needed, with clearly defined pathways for transferring care from obstetrics to cardiology or community hospitals.29 Effective integration requires information sharing and bidirectional referral mechanisms between tertiary hospitals and community health centers, clear delineation of responsibilities, service content, and follow-up timing among different providers, as well as investment in medical infrastructure at the community level to ensure continuous, high-quality postpartum care.
Current risk prediction tools, including the Prediction for ASCVD Risk in China (China-PAR) model, have limitations in evaluating CVD risk among women with HDP.30 Future research should focus on developing tailored, digitalized postpartum CVD screening and assessment tools that incorporate obstetric factors, biomarkers, and other relevant clinical parameters.31,32 Mobile health technologies and app-based reminders could enhance access, adherence, and engagement, providing convenient platforms for remote monitoring and individualized health education.33
Socioeconomic and role-related factors also influenced screening behaviors. Postpartum women often experience a role transition in which maternal and family responsibilities take precedence over personal health needs, resulting in missed follow-up appointments.34 Financial burdens further exacerbate these barriers; although some Chinese cities include the postpartum 42-day check-up in insurance coverage, long-term CVD risk screening remains largely out-of-pocket.35 Policy-level interventions could include integrating postpartum CVD risk screening into national public health programs, expanding insurance coverage, and aligning maternal follow-up with infant care and vaccination schedules to reduce logistical and financial barriers. Concurrently, healthcare providers should deliver tailored education to strengthen awareness of early CVD risk detection and motivate high-risk women to engage in preventive care.
Facilitators of postpartum CVD risk screening included a family history of hypertension, strong family support, heightened attention to personal health, and historically perceived benefits of prior interventions. A family history of hypertension serves as a salient risk cue, significantly enhancing patients’ risk perception and motivation for screening.36 Family support–through shared childcare responsibilities, financial assistance, reminders, and emotional encouragement—provides practical and psychological resources that promote adherence.37 Positive experiences from prior medical interventions foster trust in healthcare systems, enhance perceived benefits of preventive actions, and reinforce proactive health behaviors, consistent with the Health Belief Model.38 Integrating family-centered health education, shared decision-making, and clear communication of benefits during the perinatal period can strengthen intrinsic motivation and convert the postpartum period into a critical window for CVD prevention.
A comparative synthesis showed both convergence and divergence. Both groups recognized limited awareness of long-term CVD risk and acknowledged gaps in postpartum health communication. Patients and providers also described the postpartum care pathway as fragmented, characterized by unclear referral routes, poor coordination between tertiary hospitals and community health centers, and inconsistent follow-up. However, notable differences emerged. Patients emphasized confusion from inconsistent health information, fear-driven avoidance, logistical difficulties with appointments, and low confidence in community-level care. In contrast, providers highlighted institutional role ambiguity, lack of standardized referral mechanisms, and insufficient training in postpartum CVD risk management. Providers often attributed missed follow-up to poor patient adherence, whereas patients cited emotional distress and trauma-related avoidance. These differences show that patients and providers perceive the same system through distinct lenses, underscoring the need for integrated strategies that enhance both patient navigation and provider workflow.
Practical Implications
Building on these barriers and facilitators, our findings provide several practical directions for strengthening postpartum CVD risk management among women with HDP in China. First, incorporating standardized CVD risk assessments into routine postpartum visits—such as the 42-day review and scheduled follow-ups at 3, 6, and 12 months—and establishing clear transition protocols between obstetric, cardiology, and community services may help reduce care fragmentation and improve continuity. Second, implementing brief, structured counseling at discharge and enhancing provider training on long-term CVD risks could address persistent gaps in patient awareness and inconsistent guidance identified in this study. Third, digital health tools, including app-based reminders, home blood pressure and weight monitoring, and interoperable electronic platforms linking tertiary hospitals with community health centers, may facilitate timely follow-up, improve information flow, and reduce logistical barriers for postpartum women. Finally, policy efforts to subsidize essential CVD screening tests and integrate family-centered education—leveraging the strong role of spouses and caregivers—could further promote adherence to risk monitoring and support sustainable cardiovascular prevention during the postpartum period.
Limitations
This study has several limitations. First, the interviews were conducted exclusively with women with HDP and healthcare providers from a single tertiary hospital in China, which may limit the generalizability of the findings. Second, the study only tracked postpartum CVD risk screening behaviors within 3–12 months after delivery. Over time, women’s role adaptation, psychosocial stress levels, and health priorities may change, potentially influencing their engagement in CVD risk screening. Third, considering regional variations in cultural background, economic conditions, and healthcare service delivery across China, our findings may not fully capture the diversity of experiences in other settings. Fourth, one patient participant had a healthcare professional background (nurse), which may have influenced the way she interpreted or articulated her postpartum screening experiences; however, her responses were analyzed in the same manner as those of other patient participants, and no disproportionate impact on theme development was observed. Fifth, although rigorous procedures were followed, potential researcher bias cannot be completely excluded, as the interviewer was also involved in data analysis. To minimize this risk, theme development and coding decisions were discussed within the research team, and discrepancies were resolved through consensus. Finally, as the interviews were conducted in Mandarin and subsequently translated into English for reporting, translation bias may have occurred. This risk was mitigated through bilingual review and cross-checking of translated excerpts to ensure accuracy and preserve meaning. Therefore, future studies should consider conducting multicenter, larger-sample investigations across different provinces to explore barriers and facilitators to postpartum CVD risk screening among women with HDP at various stages after delivery and within diverse healthcare service models. Such research could provide more comprehensive and regionally representative evidence to inform tailored interventions and policy development.
Conclusions
Postpartum engagement in CVD risk screening among women with HDP is critical for maintaining long-term cardiovascular health. This qualitative study, incorporating perspectives from both patients and healthcare providers, provides an in-depth understanding of the barriers faced by women in undergoing CVD risk screening, including insufficient risk perception, fear and psychological stress, economic constraints, and fragmented or inconsistent follow-up processes. Additionally, the study identifies key facilitators and practical recommendations to promote postpartum screening. These findings offer valuable insights for designing educational and behavioral interventions targeting patients, families, and healthcare professionals, with the ultimate goal of improving CVD screening uptake and the implementation of risk management strategies. Future interventions should focus on enhancing patients’ awareness and understanding of CVD risk, strengthening coordinated care between hospitals and community services, integrating family involvement, and providing broader social support to optimize postpartum cardiovascular health outcomes.
Acknowledgments
We are grateful for all the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Gusu Health Talent Program Research Project of Suzhou (Grant No. GSWS2023061); the Suzhou Key Medical Disciplines Construction Project under (Grant No. SZFCXK202101); the Suzhou Municipal Health Commission, Key Project of Science and Technology Program (Grant No. ZDXM2024011).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Thomopoulos C, Brguljan J, Cífková R, Persu A, Kreutz R. Mild chronic hypertension in pregnancy: to treat or wait? Blood Press. 2022;31(1):121–124. doi:10.1080/08037051.2022.2077698
2. Hypertensive Disorders in Pregnancy Study Group, Chinese Society of Obstetrics and Gynecology. Guidelines for diagnosis and management of hypertensive disorders in pregnancy (2020). Chin J Obstet Gynecol. 2020;55(4):227–238. doi:10.3760/cma.j.cn112141-20200114-00039
3. Hirshberg A, Srinivas SK. Epidemiology of maternal morbidity and mortality. Semin Perinatol. 2017;41(6):332–337. doi:10.1053/j.semperi.2017.07.007
4. Kinshella MW, Omar S, Scherbinsky K, et al. Maternal dietary patterns and pregnancy hypertension in low- and middle-income countries: a systematic review and meta-analysis. Adv Nutr. 2021;12(6):2387–2400. doi:10.1093/advances/nmab057
5. Benschop L, Duvekot JJ, Versmissen J, van Broekhoven V, Steegers EAP, Roeters van Lennep JE. Blood pressure profile 1 year after severe preeclampsia. Hypertension. 2018;71(3):491–498. doi:10.1161/HYPERTENSIONAHA.117.10338
6. Ackerman-Banks CM, Grechukhina O, Spatz E, et al. Seizing the window of opportunity within 1 year postpartum: early cardiovascular screening. J Am Heart Assoc. 2022;11(8):e024443. doi:10.1161/JAHA.121.024443
7. Rayes B, Ardissino M, Slob EAW, Patel KHK, Girling J, Ng FS. Association of hypertensive disorders of pregnancy with future cardiovascular disease. JAMA Network Open. 2023;6(2):e230034. doi:10.1001/jamanetworkopen.2023.0034
8. Lailler G, Fosse-Edorh S, Lebreton E, et al. Impact of different types of hypertensive disorders of pregnancy and their duration on incident post-partum risk of diabetes mellitus: results from the French nationwide study CONCEPTION. Diabetes Metab. 2024;50(5):101564. doi:10.1016/j.diabet.2024.101564
9. Piccoli GB, Torreggiani M, Schwotzer N, et al. Kidney health outcomes of hypertensive disorders of pregnancy. Nat Rev Nephrol. 2025;21(10):671–686. doi:10.1038/s41581-025-00977-8
10. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596–e646. doi:10.1161/CIR.0000000000000678
11. Arnott C, Patel S, Hyett J, Jennings G, Woodward M, Celermajer DS. Women and cardiovascular disease: pregnancy, the forgotten risk factor. Heart Lung Circ. 2020;29(5):662–667. doi:10.1016/j.hlc.2019.09.011
12. Mancia G, Kreutz R, Brunström M, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens. 2023;41(12):1874–2071. doi:10.1097/HJH.0000000000003480
13. Chinese Society of Cardiology, Chinese Medical Association; Editorial Board of Chinese Journal of Cardiology. Expert consensus on the comprehensive cardiovascular risk management of hypertensive disorders in pregnancy. Chin J Cardiol. 2025;53(3):235–246. doi:10.3760/cma.j.cn112141-20200114-00039
14. Lewey J, Levine LD, Yang L, Triebwasser JE, Groeneveld PW. Patterns of postpartum ambulatory care follow-up care among women with hypertensive disorders of pregnancy. J Am Heart Assoc. 2020;9(17):e016357. doi:10.1161/JAHA.120.016357
15. Li J, Zhou Q, Wang Y, et al. Risk factors associated with attendance at postpartum blood pressure follow-up visit in discharged patients with hypertensive disorders of pregnancy. BMC Pregnancy Childbirth. 2023;23(1):485. doi:10.1186/s12884-023-05780-6
16. Levine LD, Nkonde-Price C, Limaye M, Srinivas SK. Factors associated with postpartum follow-up and persistent hypertension among women with severe preeclampsia. J Perinatol. 2016;36(12):1079–1082. doi:10.1038/jp.2016.137
17. Wilcox A, Levi EE, Garrett JM. Predictors of non-attendance to the postpartum follow-up visit. Matern Child Health J. 2016;20(Suppl1):22–27. doi:10.1007/s10995-016-2184-9
18. Sandsæter HL, Horn J, Rich-Edwards JW, Haugdahl HS. Preeclampsia, gestational diabetes and later risk of cardiovascular disease: women’s experiences and motivation for lifestyle changes explored in focus group interviews. BMC Pregnancy Childbirth. 2019;19(1):448. doi:10.1186/s12884-019-2591-1
19. Slater K, Taylor R, McLaughlin K, Pennell C, Collins C, Hutchesson M. Barriers and facilitators to cardiovascular disease prevention following hypertensive disorders of pregnancy in primary care: cross-sectional surveys. Nutrients. 2023;15(17):3817. doi:10.3390/nu15173817
20. Liu X, Wang L, Du Z, et al. The women’s cardiovascular disease risk perception after hypertensive disorders of pregnancy: a qualitative meta-synthesis. Midwifery. 2025;140:104203. doi:10.1016/j.midw.2024.104203
21. Lindgren BM, Lundman B, Graneheim UH. Abstraction and interpretation during the qualitative content analysis process. Int J Nurs Stud. 2020;108:103632. doi:10.1016/j.ijnurstu.2020.103632
22. Rogo EJ. Exploring qualitative research. J Dent Hyg. 2024;98(4):56–61.
23. Roth H, LeMarquand G, Henry A, Homer C. Assessing knowledge gaps of women and healthcare providers concerning cardiovascular risk after hypertensive disorders of pregnancy-a scoping review. Front Cardiovasc Med. 2019;6:178. doi:10.3389/fcvm.2019.00178
24. Ruan Y, Luo J, Lin H. Why do patients seek diagnose dis-accordance with hierarchical medical system related policies in tertiary hospitals? A qualitative study in Shanghai from the perspective of physicians. Front Public Health. 2022;10:841196. doi:10.3389/fpubh.2022.841196
25. Meili X, Sasa H, Ying H, Lijuan Z, Guanxiu T, Jun L. Prevalence of postpartum post-traumatic stress disorder and its determinants in Mainland China: a systematic review and meta-analysis. Arch Psychiatr Nurs. 2023;44:76–85. doi:10.1016/j.apnu.2023.04.007
26. Martínez-Vazquez S, Rodríguez-Almagro J, Hernández-Martínez A, Delgado-Rodríguez M, Martínez-Galiano JM. Long-term high risk of Postpartum Post-Traumatic Stress Disorder (PTSD) and associated factors. J Clin Med. 2021;10(3):488. doi:10.3390/jcm10030488
27. Varangot-Reille C, Pezzulo G, Thacker M. The fear-avoidance model as an embodied prediction of threat. Cogn Affect Behav Neurosci. 2024;24(5):781–792. doi:10.3758/s13415-024-01199-4
28. O’Connor S, Tilston G, Jones O, et al. Acceptability of data linkage to identify women at risk of postnatal complication for the development of digital risk prediction tools and interventions to better optimise postnatal care, a qualitative descriptive study design. BMC Med. 2024;22(1):276. doi:10.1186/s12916-024-03489-7
29. Berhie SH, Little SE, Shulkin J, Seely EW, Nour NM, Wilkins-Haug L. Redesigning care for the management of postpartum hypertension: how can Ob-Gyns and primary care physicians partner in caring for patients after a hypertensive pregnancy? Am J Perinatol. 2024;41(S01):e1352–e1356. doi:10.1055/s-0043-1764207
30. Yang X, Li J, Hu D, et al. Predicting the 10-year risks of atherosclerotic cardiovascular disease in Chinese Population: the China-PAR Project (Prediction for ASCVD Risk in China). Circulation. 2016;134(19):1430–1440. doi:10.1161/CIRCULATIONAHA.116.022367
31. Jacobsen DP, Røysland R, Strand H, et al. Circulating cardiovascular biomarkers during and after preeclampsia: crosstalk with placental function? Pregnancy Hypertens. 2022;30:103–109. doi:10.1016/j.preghy.2022.09.003
32. Staff AC, Costa ML, Dechend R, Jacobsen DP, Sugulle M. Hypertensive disorders of pregnancy and long-term maternal cardiovascular risk: bridging epidemiological knowledge into personalized postpartum care and follow-up. Pregnancy Hypertens. 2024;36:101127. doi:10.1016/j.preghy.2024.101127
33. Aquino M, Munce S, Griffith J, Pakosh M, Munnery M, Seto E. Exploring the use of telemonitoring for patients at high risk for hypertensive disorders of pregnancy in the antepartum and postpartum periods: scoping review. JMIR mHealth uHealth. 2020;8(4):e15095. doi:10.2196/15095
34. Rossiter C, Henry A, Roberts L, et al. Optimising mothers’ health behaviour after hypertensive disorders of pregnancy: a qualitative study of a postnatal intervention. BMC Public Health. 2022;22(1):1259. doi:10.1186/s12889-022-13590-2
35. Zafar U, Suleman M, Butt MN, et al. Financial and treatment compliance challenges among diabetic patients: a cross-sectional study from Pakistan. Cureus. 2025;17(2):e78856. doi:10.7759/cureus.78856
36. Dalfrà MG, Burlina S, Del Vescovo GG, Anti F, Lapolla A. Adherence to a follow-up program after gestational diabetes. Acta Diabetol. 2020;57(12):1473–1480. doi:10.1007/s00592-020-01564-y
37. Nguyen AP, Mai LAT, Spies LA, Carriveau KL. Interventions for family support in cardiometabolic disease: an integrative review. Nurs Open. 2023;10(9):5797–5812. doi:10.1002/nop2.1858
38. Mohammadkhah F, Shamsalinia A, Rajabi F, Afzali Hasirini P, Khani Jeihooni A. The effect of educational intervention in the prevention of cardiovascular diseases in patients with hypertension with application of health belief model: a quasi-experimental study. JRSM Cardiovasc Dis. 2023;12:20480040231212278. doi:10.1177/20480040231212278
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Barriers and Facilitators to Successful Intensive Adherence Counseling in Rural Northern Uganda: An Exploratory Interview with HIV-Positive Clients Using the COM-B Framework
Beja H, Daisy N, Edek MT, Kobusinge V, Akaki O, Owachgiu IO, Udho S
HIV/AIDS - Research and Palliative Care 2022, 14:553-563
Published Date: 21 November 2022
Barriers and Facilitators to Health-Care Provider Payment Reform – A Scoping Literature Review
Ndayishimiye C, Tambor M, Dubas-Jakóbczyk K
Risk Management and Healthcare Policy 2023, 16:1755-1779
Published Date: 7 September 2023
Planning for Hospital Discharge for Older Adults in Uganda: A Qualitative Study Among Healthcare Providers Using the COM-B Framework
Owokuhaisa J, Schwartz JI, Wiens MO, Musinguzi P, Rukundo GZ
Journal of Multidisciplinary Healthcare 2023, 16:3235-3248
Published Date: 2 November 2023
Older Adult Perspectives on Statin Continuation and Discontinuation in Primary Cardiovascular Disease Prevention: A Mixed-Methods Study
Brunner L, Mooser B, Spinewine A, Rodondi N, Aubert CE
Patient Preference and Adherence 2024, 18:15-27
Published Date: 3 January 2024
Healthcare Professionals’ Perspectives on Perinatal Mental Health Care in the United Arab Emirates: A Qualitative Study of Barriers and Facilitators at the Patient, Family, and Societal Levels
ElKhalil R, Bayoumi R, Menon P, Qurniyawati E, Ahmed LA, Al-Rifai RH, Masuadi E, Elbarazi I
International Journal of Women's Health 2026, 18:597512
Published Date: 11 June 2026