Back to Journals » Patient Preference and Adherence » Volume 18
Older Adult Perspectives on Statin Continuation and Discontinuation in Primary Cardiovascular Disease Prevention: A Mixed-Methods Study
Authors Brunner L ![]() , Mooser B, Spinewine A, Rodondi N, Aubert CE
, Mooser B, Spinewine A, Rodondi N, Aubert CE
Received 26 July 2023
Accepted for publication 10 December 2023
Published 3 January 2024 Volume 2024:18 Pages 15—27
DOI https://doi.org/10.2147/PPA.S432448
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Laureline Brunner,1 Blandine Mooser,1,2 Anne Spinewine,3,4 Nicolas Rodondi,1,2 Carole Elodie Aubert1,2
1Institute of Primary Health Care (BIHAM), University of Bern, Bern, Switzerland; 2Department of General Internal Medicine, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland; 3Université catholique de Louvain, Louvain Drug Research Institute, Clinical Pharmacy Research Group, Brussels, Belgium; Department of Pharmacy, Centre Hospitalier Universitaire (CHU) UCL Namur, Yvoir, Belgium; 4Clinical Pharmacy Research Group, Louvain Drug Research Institute, Université Catholique de Louvain, Brussels, Belgium
Correspondence: Carole Elodie Aubert, Department of General Internal Medicine, Inselspital, Bern University Hospital, University of Bern, Anna-von-Krauchthal Weg 7, Bern, CH-3010, Switzerland, Tel +41 31 632 03 98, Email [email protected]
Background and Purpose: Evidence for statin use for primary cardiovascular disease prevention in older adults is limited. When evidence on risk-benefit profile of a medication is uncertain, using it or not becomes a preference-sensitive decision. We aimed to assess and explore patient perspectives on continuation and discontinuation of statins used for primary cardiovascular prevention in older adults.
Patients and Methods: We used a convergent mixed-methods design, conducting in parallel a survey among 47 patients and three focus groups (FGs) with 14 patients total. We recruited patients aged ≥ 65 years and taking a statin for primary cardiovascular prevention. The survey and FGs aimed to assess and explore patient experiences of statin use, and views on statin continuation and discontinuation, including patient decision-making. Quantitative and qualitative data were first analyzed separately – descriptive statistics for quantitative data and thematic analysis for qualitative data – and then integrated to create metainferences, using joint displays.
Results: Forty-one percent of patients (N=19) were reluctant to discontinue the statin, whereas 22% (N=10) were willing to try discontinuing it. A reason to continue the statin was its perceived necessity, while self-estimated low cardiovascular risk and wish to reduce medication burden were given as reasons to discontinue it. Lack of expertise assumed by the patients to decide about statin continuation or discontinuation, uncertainty about statin indication, and fear of having a cardiovascular event after discontinuation made many patients uncertain about deciding to continue or discontinue the statin. In this context, 70% (N=33) would rather have their physician choose for them, and 94% (N=44) would continue taking the statin for as long as their physician told them to do so.
Conclusion: This study highlights factors that influence patient willingness to continue or discontinue statins, patient uncertainty about statin continuation or discontinuation, and the important role physicians play in the decision-making process.
Keywords: barriers, facilitators, primary care providers, statins
Introduction
Statins are among the most frequently prescribed chronic medications in older adults, and their prescription rates have increased in recent years.1–3 While benefits of statins for secondary cardiovascular disease (CVD) prevention are well demonstrated,4 evidence for their benefits in primary CVD prevention is weaker, particularly among older adults.5,6 Only 8% of participants enrolled in statin trials on primary CVD prevention were aged 75 years or older, and no statistically significant benefit was found for adults older than 70 years of age.6,7 Despite this lack of evidence, statins are more frequently prescribed for primary CVD prevention in older rather than in younger adults.8 Statins are also associated with adverse drug events (ADEs), such as muscle pain, myopathy, acute renal failure, or liver dysfunction, which might decrease quality of life.9
When evidence is uncertain about the benefits of a medication, to continue taking it or not becomes a preference-sensitive decision.10,11 As such, the American Heart Association recommends accounting for patient priorities of care, and using shared decision-making between patients and clinicians when addressing statin use for primary CVD prevention.5,12 However, little is known about older patient perspectives regarding statin continuation and discontinuation when used for primary CVD prevention.
A previous qualitative study on older patient perspectives on deprescribing showed that older adults taking a statin in primary CVD prevention feared a cardiovascular event if they discontinued the statin.13 An enquiry and a Q-methodology study showed, however, that older adults were willing to discontinue the statin if their physician said it was possible,14,15 or if they had a low self-estimated CVD risk.15 Another qualitative study focusing on deprescribing in patients with life-limiting illnesses found that patients mostly thought that discontinuing the statin would result in fewer symptoms and better quality of life.16
Hence, previous literature showed that older adults may have conflicting views on statin deprescribing. However, most studies approached statin discontinuation as part of broader deprescribing explorations/enquiries and focused neither on statin specifically nor on primary CVD prevention. We might expect different patient perspectives when focusing on this medication class used in primary CVD prevention.
Thus, the present study aimed at specifically assessing and exploring the perspectives of older adults on continuation and discontinuation of statins prescribed for primary CVD prevention. We hypothesized that fear of experiencing a cardiovascular event after discontinuation and involvement of primary care physicians would be critical factors influencing older adult views about statin continuation and discontinuation.
Methods
Design
We used a convergent mixed-methods research design,17 conducting in parallel a survey and focus groups (FGs). This specific design was used to provide a complementary and thorough exploration of patient perspectives regarding statin continuation and discontinuation.
Setting and Participants
We included patients aged ≥65 years (defined as “older adults” in the literature),18 taking a statin for primary CVD prevention and able to speak and understand German. Patients with cognitive impairment or taking a statin for secondary CVD prevention were excluded. Criteria to define primary and secondary CVD prevention are provided in Additional file 1. We screened for eligible patients during their hospitalization at the Department Of General Internal Medicine of Bern University Hospital between February and May 2022 and recruited them by phone after hospital discharge. All participants were asked to complete the survey. Participation in the FGs was based on individual availability and willingness. Participation was voluntary and all patients provided written consent.
Sample Size
Survey
As we expected recruitment to be difficult and response rate limited in this older mostly frail recently hospitalized patient population, and as we aimed to provide attitudinal findings to be expanded by qualitative data, rather than to generalize survey data (see Mixed Methods Analysis),19,20 we conducted an explorative study by planning a convenience sample of 50 patients. As we also expected a high withdrawal due to the nature of the survey population, we purposefully planned to recruit 50% more patients.
Focus Groups
We used convenience sampling to recruit available patients meeting our inclusion criteria.21 Accounting for difficult recruitment of older patients for FGs (especially during the COVID-19 pandemic), we did not aim to reach theoretical saturation but rather to conduct three FGs with five to seven patients each. A member of a patient organization (“Patientenstelle Basel” – www.basel.patientenstelle.ch) was also involved, as data have shown that including such persons can be fruitful in medication-related research.22
Data Collection
The survey and FGs aimed to assess and explore patient experiences of statin use, and views on statin continuation and discontinuation, including decision-making. The quantitative data aimed to provide general patient attitudes towards statin continuation and discontinuation to be expanded by qualitative data.19,20
The survey and FG guide are available in Additional files 2 and 3.
Survey
The survey was developed based on the revised Patient Attitudes Towards Deprescribing (rPATD) questionnaire, a tool that was validated for older adults.23 The relevant rPATD questions were adapted to statin use. Additional and related questions were created based on a systematic review of barriers and facilitators to deprescribing cardiovascular medications conducted by the authors.24 The survey included 27 5-point Likert scale questions (1 = “completely agree”, 2 = “agree”, 3 = “don’t know”, 4 = “agree”, 5 = “completely disagree”), as well as free-text questions, so that patients could express additional opinions or concerns. The survey questions were revised by experts in mixed methods and deprescribing guidelines (see acknowledgement section). The survey was pilot-tested with three patients meeting the inclusion criteria, in order to ensure the questions were clear and easy to understand for the target population. A formal content and face validation were out of the scope of our study and therefore not conducted. The time required to complete the survey was approximately 30 minutes. The survey was sent to patients in paper format, along with an informed consent form, a short sociodemographic questionnaire (including questions on age, gender and number of years of statin use), and a prepaid return envelope. In addition, we extracted information on comorbidities and long-term medications from patient files at Bern University Hospital. Patients were asked to complete the survey on their own but could contact the research team in case of uncertainties. Patients were considered to have withdrawn from the study if they had not completed the survey after two telephone reminders. Patients received 20 Swiss francs as financial compensation for completing the survey.
Focus Groups
The FG guide was developed based on the aforementioned systematic review of barriers and facilitators to deprescribing cardiovascular medications,24 as well as on needs to facilitate decision-making.25 The FG guide was also revised by experts in mixed-methods and deprescribing guidelines. FGs were conducted in person by CEA and LB at Bern University Hospital between April and May 2021, lasted 45 to 60 minutes, and were recorded and then transcribed as verbatim. FG participants were asked to complete the survey before participating in the FGs. Participants were financially compensated for their participation (100 Swiss francs for the patient representative, 50 Swiss francs for the patients).
Data Analysis
Quantitative and qualitative data were first analyzed separately and then integrated to create metainferences (see Mixed Methods Analysis).
Quantitative Analysis
We used descriptive statistics to report the answers to the quantitative questions of the survey. We described percentages, distinguishing 3 categories for ease of interpretation: agreeing (combining 1 = “completely agree” and 2 = “agree” on the 5-point Likert scale), neutral (3 = “don’t know” on the 5-point Likert scale), and disagreeing (combining 4 = “disagree” and 5 = “completely disagree” on the 5-point Likert scale). We performed the analyses using Stata version 16.0 (StataCorp, College Station, TX, 2015).
Qualitative Analysis
FGs and free-text survey answers were analyzed using an inductive approach, ie allowing codes to emerge during analysis.26 Thematic analysis was chosen to identify common themes across FGs.27 FGs were coded independently by two authors (CEA and LB) to increase coding reliability. Consensus on categories and themes created from the coding was reached through discussion. Relevant quotes were translated from German into English. Coding was conducted using MAXQDA2020 software for qualitative analysis (VERBI Software, Berlin, Germany).
Mixed Methods Analysis
We used joint displays to integrate quantitative and qualitative results. This approach merges both data in a single table or figure to ensure a more distinct and nuanced comparison of the results and to draw metainferences.20 Quantitative and qualitative data can confirm (the two data sources essentially confirm each other), complement (the two data sources illustrate different, non-conflicting interpretations), expand (the two data sources provide both a central overlapping, as well as a broader non-overlapping interpretation), or contradict (the two data sources lead to conflicting interpretations) each other.20 The joint displays were created in an iterative process.20
Results
Patient Flow and Characteristics
Among 198 patients contacted, 89 accepted to complete the survey, with 15 also participating in the FGs. Finally, 47/89 (53%) patients completed the survey, and 14 of those 47 patients also participated in the FGs (one patient revoked participation). We conducted three FGs with, respectively, five (FG1: P1-P5), four (FG2: P6-P9), and five patients (FG3: P10-P14). A member of the patient organization was present in each FG. Patient recruitment process and reasons for withdrawal are presented in Additional file 4. Mean participant age was 73 years old and 51% of patients (N=24) had been taking a statin ≥5 years. Patient sociodemographic characteristics are presented in Additional file 5.
Patient Perspectives on Statin Continuation and Discontinuation
Quantitative Results
The following sections present the most important quantitative findings, grouped into three categories and represented in Figure 1. The percentages of agreement to all survey questions are presented in Additional file 6.
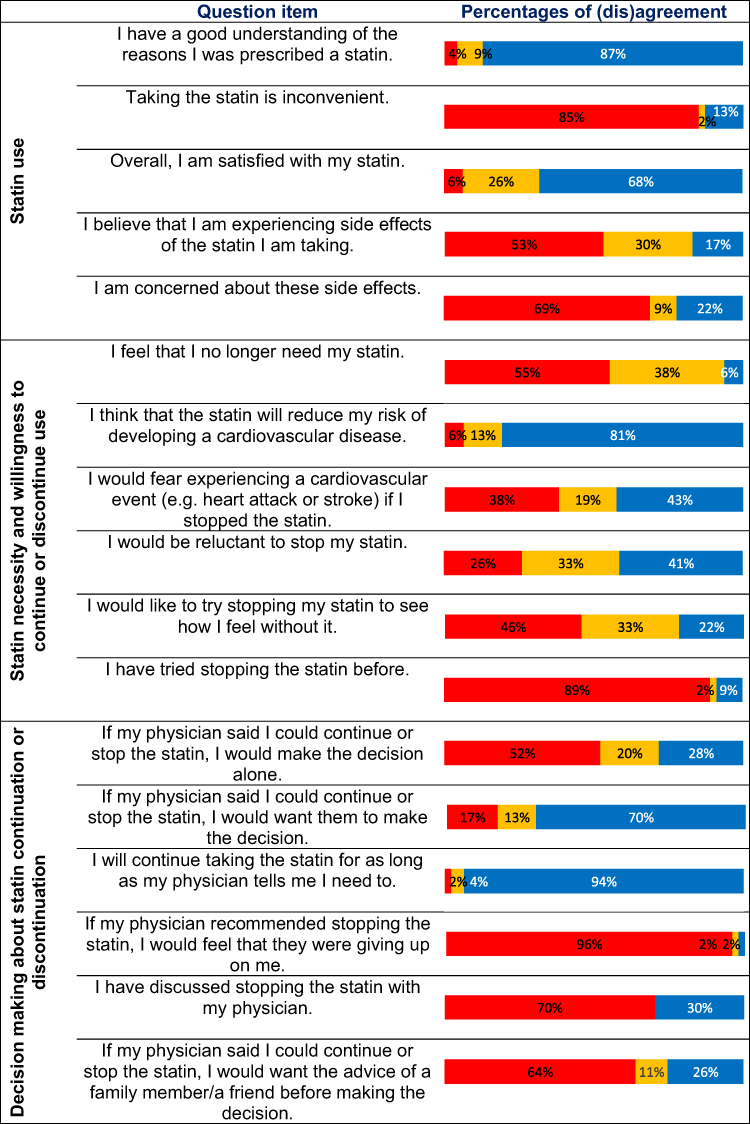 |
Figure 1 Most important quantitative findings. Notes: Percentage of (dis)agreement showing complete disagreement and disagreement combined (in red), “don’t know” (in orange), and agreement and complete agreement combined (in blue). |
Statin Use
Most surveyed patients (87%, N=41) understood why they were prescribed a statin. Eighty-five percent of patients (N=40) did not find statin use inconvenient, and 68% (N=32) reported being satisfied with the statin. Seventeen percent of patients (N=8) reported experiencing statin ADEs, while 30% (N=14) did not know if they were experiencing any ADEs. Most patients (69%, N=31) were not concerned by statin ADEs.
Statin Necessity and Willingness to Continue or Discontinue Use
Fifty-five percent of patients (N=26) felt that they needed their statin, and 81% (N=38) thought that their statin provided them with CVD protection. However, almost as many patients did (43%, N=20) and did not (38%, N=18) fear experiencing a cardiovascular event if they discontinued the statin. Forty-one percent of patients (N=19) were reluctant to discontinue the statin, whereas 22% (N=10) were willing to try discontinuing it to see how they would feel without it. Thirty-three percent of survey patients (N=15) were undecided about continuing or discontinuing the statin. Only 9% of patients (N=4) had already tried discontinuing it.
Decision Making About Statin Continuation or Discontinuation
When presented with the possibility to choose to either continue or discontinue the statin, half of the patients (52%, N=24) reported not wanting to decide on their own. Seventy percent of patients (N=33) would rather have their physician choose for them, and 94% (N=44) stated that they would continue taking the statin for as long as their physician told them to do so. However, ninety-six percent of patients (N=45) indicated they would not feel abandoned if their physician proposed to discontinue the statin. Only 30% of patients (N=14) had already discussed statin discontinuation with their physician. Sixty-four percent of patients (N=30) did not want to involve family members or friends in the decision-making process.
Qualitative results
Theme 1: Knowledge of the Reason for Statin Use
Patients showed different levels of understanding of the reason they were taking a statin. Most patients could explain the reasons they were prescribed a statin. As presented in Table 1, possible reasons to take the statin were having high cholesterol levels or atherosclerosis. However, some patients did not know or were unsure of the reason for their statin prescription.
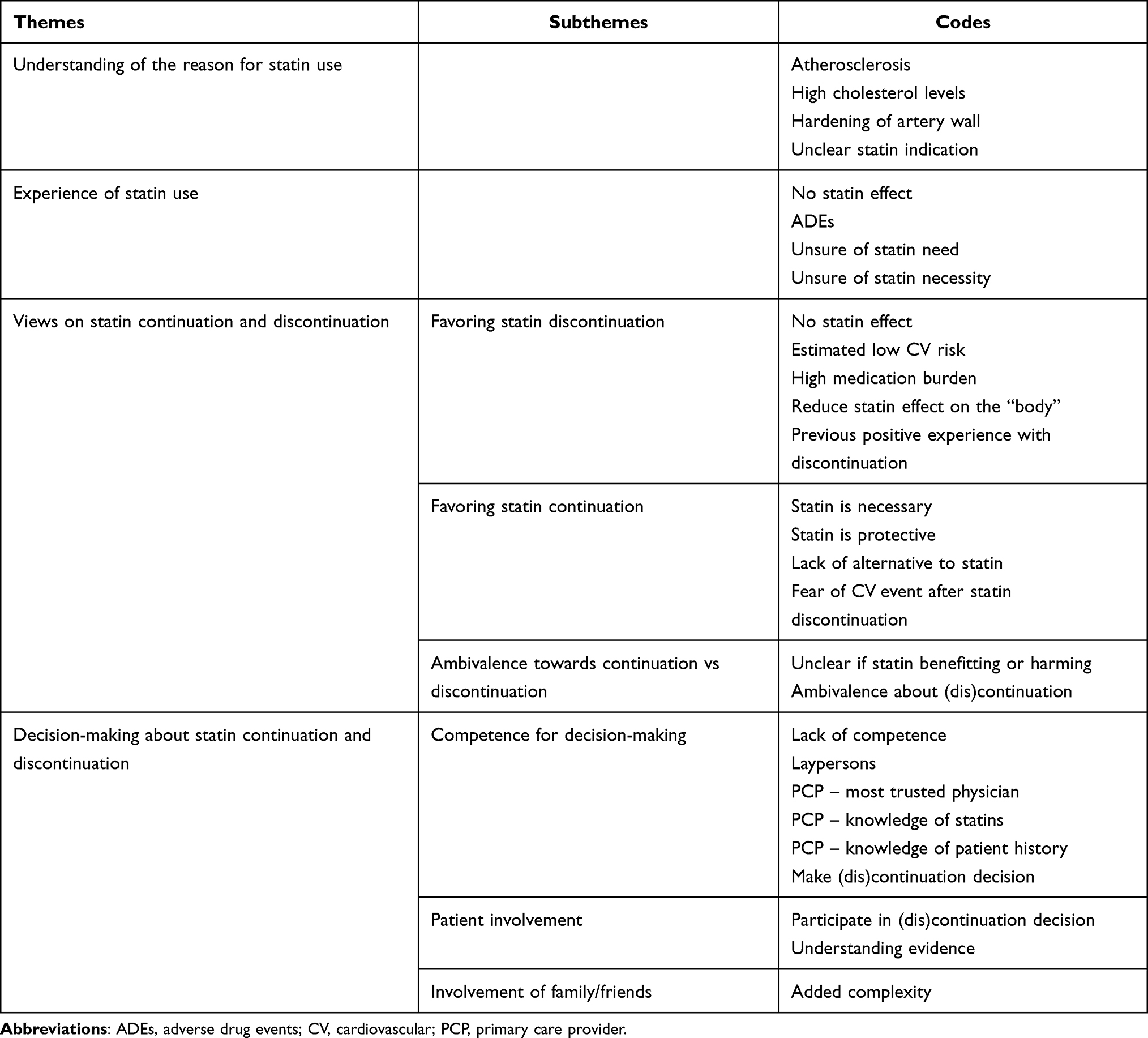 |
Table 1 Summary of Focus Group Categories, Themes and Main Codes |
Theme 2: Experience of Statin Use
Patients experienced statin use differently. Many patients explained not feeling any positive or negative effect of the statin. Others, however, explained experiencing ADEs, although they were not necessarily sure that they came from statin use. Patients unsure about their statin indication were also unsure about whether their statin was needed or helping them.
Theme 3: Views on Statin Continuation and Discontinuation
Subtheme 1 – Favoring statin discontinuation: Patients not feeling any statin effect (positive or negative) were more willing to discontinue the statin. Patients were also more willing to discontinue the statin when they self-estimated their CVD risk as low, had a high medication burden or wished to reduce statin effects on their “body”. A previous positive experience with statin discontinuation (not noticing any difference) also increased patient willingness to discontinue the statin.
Subtheme 2 – Favoring statin continuation: Patients perceiving the statin as necessary or protective were more willing to continue the statin. Patients who felt they lacked an alternative to statin to reduce cholesterol levels or who feared a cardiovascular event following statin discontinuation were also more willing to continue taking it.
Subtheme 3 – Ambivalence towards continuation vs discontinuation: Feeling unsure about their statin indication made patients ambivalent about wanting to continue or discontinue their statin, as it was not clear to them if they were benefiting from or being harmed by it.
Theme 4: Decision-Making About Statin Continuation and Discontinuation
Subtheme 1 – Competence for decision-making: Most patients thought that they lacked the competence to independently decide to continue or discontinue the statin. As such, patients relied on their physician, and especially their primary care physician (PCP), for decision-making. Patients emphasized the role played by their PCPs rather than by specialists, as they not only had knowledge about statins but also knew their other diseases and medications well.
Subtheme 2 – Patient involvement: Some patients stated that their PCP should independently decide whether to continue or discontinue the statin, while others wanted to be presented the evidence about statin continuation and discontinuation and actively participate in the decision. These patients also wanted their PCP to provide them with a plan to ensure safe discontinuation. Patients who wanted their PCP to decide emphasized that they would not feel abandoned by their PCP if they chose to discontinue the statin.
Subtheme 3 – Involvement of family/friends: Patients rejected the idea of involving family members or friends in the decision-making process, as they feared adding complexity to the decision.
Mixed-Methods Results
In the following sections, we present only the survey items for which we could draw meaningful inferences with the qualitative data. We created the joint displays to show 1) patient experience of statin use; 2) patient views on statin continuation and discontinuation; 3) patient involvement and physician role in station continuation or discontinuation decisions. For each subsection, attitudinal findings (ie quantitative results) and reflective quotes (ie qualitative results) are presented in the joint display, while metainferences between qualitative and quantitative data are presented in the text. We found mostly expanding, but also confirming and contradictory data.
Patient Experience of Statin Use
Qualitative data confirmed and expanded quantitative data by showing that patients indeed understood the reasons they were prescribed a statin and could explain these reasons (eg high cholesterol levels, Figure 2A). Qualitative analysis also provided expanding information by showing a possible reason why patients might feel unsure of the reason they were prescribed a statin, ie not understanding its indication, which might relate to a patient-physician miscommunication.
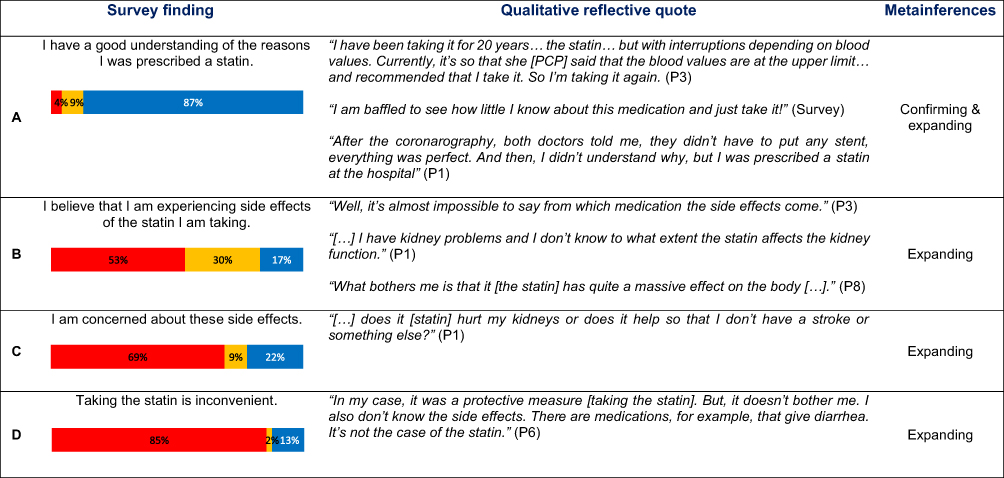 |
Figure 2 Patient experience of statin use. Notes: Percentage of (dis)agreement showing complete disagreement and disagreement combined (in red), “don’t know” (in orange), and agreement and complete agreement combined (in blue).. Figure 2 contains sub-figures (A–D). |
Qualitative data also expanded quantitative data about statin ADEs, with patients reporting having some symptoms but being unsure that they were statin ADEs (eg renal failure) (Figure 2B). These patients were thus unsure if they were really benefiting from the statin (Figure 2C). Qualitative data also expanded quantitative data as they inferred a possible connection between inconvenience of statin use and ADEs: lack of ADEs potentially means finding statin use not or less inconvenient (Figure 2D).
Patient Views on Statin Continuation and Discontinuation
Qualitative data expanded quantitative data by showing how patients linked their perceived necessity of the statin with their willingness to continue taking it or not, and providing reasons why patients thought they did (eg no alternative to the statin, atherosclerosis, Figure 3A) or did not (eg low perceived CVD risk, lack of feeling of statin effect, Figure 3B) need their statin. Furthermore, they showed that some patients were willing to discontinue their statin to reduce their medication burden, independently of its necessity (Figure 3C). Qualitative data also expanded quantitative data by linking patient indecisiveness about statin continuation or discontinuation with a potential lack of understanding of the indication for statin use (Figure 3C).
 |
Figure 3 Patient views on statin continuation and discontinuation. Abbreviations: CV, cardiovascular; TIA, transient ischemic attack. Notes: Percentage of (dis)agreement showing complete disagreement and disagreement combined (in red), “don’t know” (in orange), and agreement and complete agreement combined (in blue). Figure 3 contains sub-figures (A–D). |
In the qualitative phase, most patients expressed fear of having a cardiovascular event if they discontinued their statin, and some even accepted to endure statin ADEs if it meant reducing their risk of having a cardiovascular event. This somewhat contradicts quantitative data, which showed an almost equal proportion of patients fearing and respectively not fearing a cardiovascular event after statin discontinuation (Figure 3D).
Patient Involvement and Physician Role in Statin Continuation or Discontinuation Decision
Quantitative and qualitative data confirmed each other as they both showed patient reluctance to decide about statin continuation or discontinuation and the important role physicians played in decision-making (Figure 4A–4C). They also both highlighted patient reluctance to involve family or friends in decision-making (Figure 4D). Qualitative data were also expanding as they showed the reasons for patient reluctance to decide about statin continuation or discontinuation (eg lacking medical expertise, especially in regard to fearing a cardiovascular event following statin discontinuation, Figure 4B). Qualitative data also expanded quantitative data by showing that patients especially valued involvement of their PCP in the decision-making process and could provide the reasons of their trust in their PCPs (eg knowing their medical history well or PCP expertise, Figure 4A and 4B). Qualitative data also showed that, although some patients trusted their physician, they were not willing to discontinue the statin without discussing it first and getting information (ie engaging in shared-decision making, Figure 4B). Furthermore, qualitative data showed that the level of trust patients put in their physicians seemed to influence the level of involvement they wanted in decision-making (Figure 4B). Qualitative data were also expanding by showing how patients wanted their physician to ensure them a safe discontinuation, mostly through a monitoring of cholesterol levels and a possible statin restart (Figure 4B).
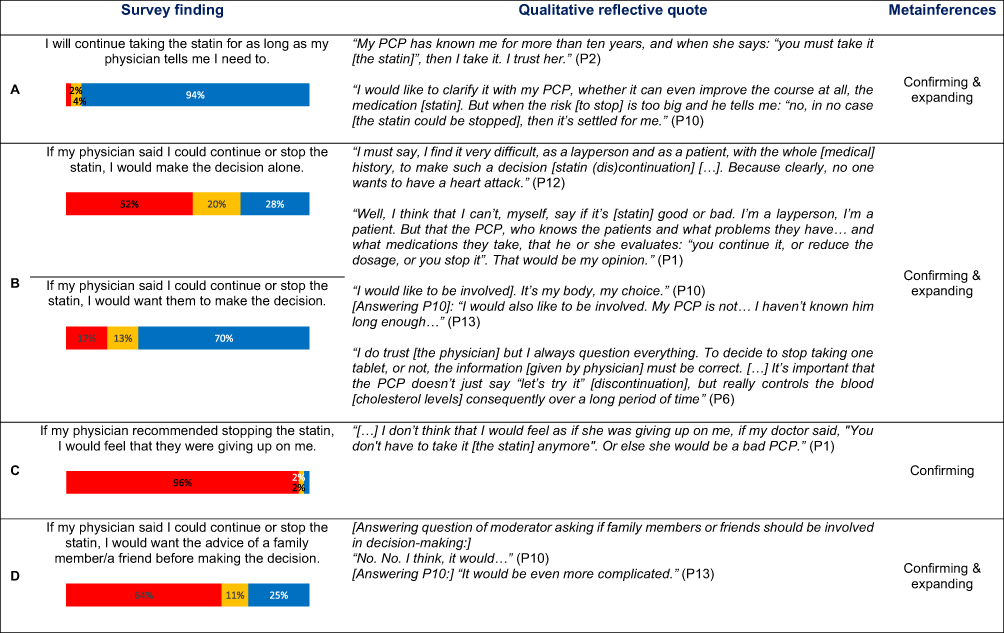 |
Figure 4 Patient involvement and physician role in statin continuation or discontinuation decision. Abbreviation: PCP, primary care physician. Notes: Percentage of (dis)agreement showing complete disagreement and disagreement combined (in red), “don’t know” (in orange), and agreement and complete agreement combined (in blue). Figure 4 contains sub-figures (A–D). |
Discussion
This study reveals important findings about patient perspectives regarding decision-making about statin continuation and discontinuation in primary CVD prevention in older adults. On the one hand, patients who saw their statin as protective or were focused on keeping low cholesterol levels were more willing to continue taking it. On the other hand, patients who thought they had a low CVD risk or who wished to reduce their medication burden or statin ADEs were more willing to discontinue it. Lack of expertise perceived by the patients to decide about statin continuation or discontinuation, uncertainty about statin indication, and fear of having a cardiovascular event after discontinuation, made many patients uncertain about deciding on their own to continue or discontinue the statin. In this context, patient trust in their PCP to support and guide decision-making emerged as central, while family or friend involvement was not desired.
The mixed-methods section showed that perception of statin necessity, or lack thereof, influenced patient willingness to continue or discontinue their statin. This factor was already highlighted in previous studies about deprescribing cardiovascular medications.15,28–30 In fact, patients viewing their cardiovascular medication as more than a necessity (ie an obligation) were more willing to continue it,28,29 while patients with a low self-perceived CVD risk deemed their cardiovascular medication less necessary and were more willing to discontinue it.15,28 Our mixed-methods analysis also showed that patients having statin ADEs could perceive that they were not benefiting from it and that those who did not have ADEs might find taking the statin less inconvenient. Previous studies about deprescribing cardiovascular medications also showed that ADEs played an important role in patient willingness to continue or discontinue the medication.31–34 Patients whose quality of life was reduced by the medication were unsure about its benefit and more willing to discontinue it.31,33 However, patients tended to put ADEs in perspective, balancing them against the reasons to take the medication (ie perceived benefit).32 Furthermore, patients who did not have any ADEs and did not feel any effect of the medication – as could happen with the statin – were unwilling to discontinue it.34
Interestingly, although patients could cite factors influencing their willingness to continue or discontinue their statin, many were uncertain about wishing to continue or discontinue it if they were given the choice as shown by the confirming metainference in the mixed-methods section. A critical factor highlighted in the FGs was the fear of experiencing a cardiovascular event after statin discontinuation. Interestingly, the inferences showed a discordance between the qualitative and the quantitative data, where most patients felt protected by their statin but half of them were not afraid of a cardiovascular event after discontinuation. Concordant to our qualitative results, many studies about patient-reported barriers and facilitators to deprescribing cardiovascular medications found that fear about possible consequences of discontinuing a cardiovascular medication made patients uncertain or afraid to discontinue it.13,28–31,33 As the cardiovascular medications of interest of these studies were often antidiabetics, antihypertensives or beta-blockers, we can hypothesize that patients might be more uncertain or afraid to discontinue a medication that subjectively improves their health (eg less dizziness under beta-blockers) as opposed to a medication whose effect they do not physically feel, although they might theoretically know that it protects them.
In the context of patient uncertainty about statin continuation or discontinuation in primary CVD prevention, both the quantitative and qualitative data showed the key role that patients assigned to their PCPs to support them in decision-making, or even to decide for them. The importance of PCPs in patient decision-making about deprescribing cardiovascular medications was highlighted in previous studies that showed that patients particularly trusted their PCPs since they knew them well,15,28 and that some patients depended on their PCP for decision-making.30 Furthermore, concordant with our results, previous studies found that a majority of older patients would be willing to discontinue a medication, including statins, if their physician said it was possible.14,35 However, patients showed different attitudes towards their own implication in decision-making about continuation or discontinuation, as suggested by our mixed-methods results and demonstrated in a previous study. Indeed, some patients might think they lack expertise to make a decision regarding statin continuation or discontinuation, and would thus refer decisions to healthcare providers.36 Furthermore, while patients should be informed about medication changes, some might desire, while others might refuse, to have an active role in decision-making.36
The main strength of this study is its mixed methods design, which allowed for a complementary exploration and highlighted older adults’ main perspectives on statin continuation and discontinuation. However, the recruitment of patients from a single hospital and the small sample size limit the validity of the triangulation of the quantitative and the qualitative data, as well as the generalizability of the results. Nevertheless, recruiting such patients is challenging and collecting their insights still brings important new knowledge. Another limitation is the lack of formal validation of the survey. However, most of our survey questions were adapted from or related to the rPATD, which is a tool validated for older adults, and the survey was revised by experts in mixed-methods and deprescription guidelines. The survey was also pilot-tested by patients.
Clinical Implications
Our study has several clinical implications. First, patient answers on willingness to continue or discontinue the statin show the importance of regularly assessing patient perspectives such as fear, sense of necessity, statin effects, and how these influence patient willingness to continue or discontinue their statin. Second, discussions about statin continuation or discontinuation should occur with physicians in whom patients trust. Patients should be informed about their medication indication, along with the current evidence on its efficacy and benefits, since medication intake should be acceptable to patients and concordant with their individual goals of care. Third, when considering statin continuation or discontinuation, it is important that trusted physicians evaluate the level of involvement in decision-making wished by each patient. To support patients wanting to actively participate in decision-making, physicians must be provided with tools (eg patient decision aids) to adequately convey and discuss the risks and benefits of the different options and to guide the discontinuation process and follow-up after discontinuation so that patients feel safe.
Conclusion
This study provides valuable insights on older adult perspectives on statin continuation and discontinuation in primary CVD prevention, highlighting factors that might influence willingness to continue or discontinue statins, uncertainty about statin continuation or discontinuation, and the importance of PCPs in the decision-making process.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Ethical approval was waived by the Human Research Ethics Committee of the Canton of Bern, Switzerland (Req-2020-03065), as the study did not fall under the Human Research Act. Our study complies with the Declaration of Helsinki.
All participants in this study provided written consent.
Consent for Publication
Participant informed consent included publication of anonymized responses.
Acknowledgments
The authors want to thank the different experts in mixed methods and deprescribing, who critically revised the survey and focus group guide, along with the Qualitative & Mixed Methods Learning Lab of the University of Michigan for providing us with the opportunity to present our results and receive critical feedback during its Works-In-Progress session.
Author Contributions
AS, CEA, LB and NR designed the study. CEA and LB collected the data. CEA and LB analyzed the data. BM participated in the execution of the study. BM, CEA and LB lead the drafting of the article. NR and AS critically reviewed the article. CA and NR supervised the whole study. All authors reviewed and gave feedback as well as final approval for the article submission and resubmission. All authors agree to take responsibility and be accountable for the contents of the article. All authors agreed on the journal choice for the article submission.
Funding
LB and NR were partly supported by a grant from the Swiss National Science Foundation (Grant IICT 33IC30-193052). CEA was supported by the Swiss National Science Foundation (Grant PZ00P3 201672). This project and LB were supported by a grant from the College of General Internal Medicine (Switzerland).
Disclosure
The authors declare that they have no competing interests.
References
1. O’Keeffe AG, Nazareth I, Petersen I. Time trends in the prescription of statins for the primary prevention of cardiovascular disease in the United Kingdom: a cohort study using the health improvement network primary care data. Clin Epidemiol. 2016;8:123–132. doi:10.2147/CLEP.S104258
2. Gu Q, Paulose-Ram R, Burt VL, Kit BK. Prescription cholesterol-lowering medication use in adults aged 40 and over: United States, 2003–2012. NCHS Data Brief. 2014;177:1–8.
3. Canadian Institute for Health Information. Drug use among seniors in Canada; 2016. Available from: https://www.cihi.ca/sites/default/files/document/drug-use-among-seniors-2016-en-web.pdf.
4. Afilalo J, Duque G, Steele R, Jukema JW, de Craen AJ, Eisenberg MJ. Statins for secondary prevention in elderly patients: a hierarchical Bayesian meta-analysis. J Am Coll Cardiol. 2008;51(1):37–45. doi:10.1016/j.jacc.2007.06.063
5. Grundy SM, Stone NJ, Bailey AL, et al. for the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082–e143. doi:10.1161/CIR.0000000000000625
6. Armitage J, Baigent C, Barnes E; Cholesterol Treatment Trialists’ Collaboration. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. Lancet. 2019;393(10170):407–415. doi:10.1016/S0140-6736(18)31942-1
7. Byrne P, Cullinan J, Smith SM. Statins for primary prevention of cardiovascular disease. BMJ. 2019;367:l5674. doi:10.1136/bmj.l5674
8. Chokshi NP, Messerli FH, Sutin D, Supariwala AA, Shah NR. Appropriateness of statins in patients aged >/=80 years and comparison to other age groups. Am J Cardiol. 2012;110(10):1477–1481. doi:10.1016/j.amjcard.2012.06.058
9. Hippisley-Cox J, Coupland C. Unintended effects of statins in men and women in England and Wales: population based cohort study using the QResearch database. BMJ. 2010;340:c2197. doi:10.1136/bmj.c2197
10. Holmes HM, Todd A. The role of patient preferences in deprescribing. Clin Geriatr Med. 2017;33(2):165–175. doi:10.1016/j.cger.2017.01.004
11. Linsky A, Meterko M, Bokhour BG, Stolzmann K, Simon SR. Deprescribing in the context of multiple providers: understanding patient preferences. Am J Manag Care. 2019;25(4):192–198. doi:10.7326/0003-4819-140-10-200405180-00009
12. van der Ploeg MA, Floriani C, Achterberg WP, et al. Recommendations for (Discontinuation of) Statin treatment in older adults: review of guidelines. J Am Geriatr Soc. 2020;68(2):417–425. doi:10.1111/jgs.16219
13. Pickering AN, Hamm ME, Dawdani A, et al. Older patient and caregiver perspectives on medication value and deprescribing: a qualitative study. J Am Geriatr Soc. 2020;68(4):746–753. doi:10.1111/jgs.16370
14. Qi K, Reeve E, Hilmer SN, Pearson S-A, Matthews S, Gnjidic D. Older peoples’ attitudes regarding polypharmacy, statin use and willingness to have statins deprescribed in Australia. Int J Clin Pharm. 2015;37(5):949–957. doi:10.1007/s11096-015-0147-7
15. Luymes CH, Boelhouwer NJ, Poortvliet RK, de Ruijter W, Reis R, Numans ME. Understanding deprescribing of preventive cardiovascular medication: a Q-methodology study in patients. Patient Prefer Adherence. 2017;11:975–984. doi:10.2147/PPA.S131625
16. Tjia J, Kutner JS, Ritchie CS, et al. Perceptions of statin discontinuation among patients with life-limiting illness. J Palliat Med. 2017;20(10):1098–1103. doi:10.1089/jpm.2016.0489
17. Pluye P, Hong QN. Combining the power of stories and the power of numbers: mixed methods research and mixed studies reviews. Annu Rev Public Health. 2014;35(1):29–45. doi:10.1146/annurev-publhealth-032013-182440
18. Pazan F, Wehling M. Polypharmacy in older adults: a narrative review of definitions, epidemiology and consequences. Eur Geriatr Med. 2021;12(3):443–452. doi:10.1007/s41999-021-00479-3
19. Setia MS. Methodology series module 5: sampling strategies. Indian J Dermatol. 2016;61(5):505–509. doi:10.4103/0019-5154.190118
20. Fetters MD. Developing a joint display. In: Fargotstein LJA, Todorovic-Arndt L, editors. The Mixed Methods Research Workbook: Activities for Designing, Implementing, and Publishing Projects. California (USA): SAGE Publications, Inc.; 2019:193–210.
21. Sandelowski M. Sample size in qualitative research. Res Nurs Health. 1995;18(2):179–183. doi:10.1002/nur.4770180211
22. Rach C, Lukas J, Müller R, Sendler M, Simon P, Salloch S. Involving patient groups in drug research: a systematic review of reasons. Patient Prefer Adherence. 2020;14:587–597. doi:10.2147/PPA.S232499
23. Reeve E, Low LF, Shakib S, Hilmer SN. Development and validation of the revised patients’ Attitudes Towards Deprescribing (rPATD) questionnaire: versions for older adults and caregivers. Drugs Aging. 2016;33(12):913–928. doi:10.1007/s40266-016-0410-1
24. Brunner L, Rodondi N, Aubert CE. Barriers and facilitators to deprescribing of cardiovascular medications: a systematic review. BMJ Open. 2022;12(12):e061686. doi:10.1136/bmjopen-2022-061686
25. AM O’Connor. The things that are important to me when making a decision about tamoxifen; 1999. Available from: https://decisionaid.ohri.ca/docs/develop/Tools/Values_tamoxifen.pdf.
26. Burnard P, Gill P, Stewart K, Treasure E, Chadwick B. Analysing and presenting qualitative data. Br Dent J. 2008;204(8):429–432. doi:10.1038/sj.bdj.2008.292
27. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15(3):398–405. doi:10.1111/nhs.12048
28. Luymes CH, van der Kleij RM, Poortvliet RK, de Ruijter W, Reis R, Numans ME. Deprescribing potentially inappropriate preventive cardiovascular medication: barriers and enablers for patients and general practitioners. Ann Pharmacother. 2016;50(6):446–454. doi:10.1177/1060028016637181
29. Jansen J, McKinn S, Bonner C, Muscat DM, Doust J, McCaffery K. Shared decision-making about cardiovascular disease medication in older people: a qualitative study of patient experiences in general practice. BMJ Open. 2019;9(3):e026342. doi:10.1136/bmjopen-2018-026342
30. van Bussel E, Reurich L, Pols J, Richard E, Moll van Charante E, Ligthart S. Hypertension management: experiences, wishes and concerns among older people-A qualitative study. BMJ Open. 2019;9(8):e030742. doi:10.1136/bmjopen-2019-030742
31. Crutzen S, Baas G, Abou J, et al. Barriers and enablers of older patients to deprescribing of cardiometabolic medication: a focus group study. Front Pharmacol. 2020;11:1268. doi:10.3389/fphar.2020.01268
32. Benson J, Britten N. What effects do patients feel from their antihypertensive tablets and how do they react to them? Qualitative analysis of interviews with patients. Fam Pract. 2006;23(1):80–87. doi:10.1093/fampra/cmi081
33. Goyal P, Requijo T, Siceloff B, et al. Patient-reported barriers and facilitators to deprescribing cardiovascular medications. Drugs Aging. 2020;37(2):125–135. doi:10.1007/s40266-019-00729-x
34. van Middelaar T, Ivens SD, van Peet PG, et al. Prescribing and deprescribing antihypertensive medication in older people by Dutch general practitioners: a qualitative study. BMJ Open. 2018;8(4):e020871. doi:10.1136/bmjopen-2017-020871
35. Rozsnyai Z, Jungo KT, Reeve E, et al. What do older adults with multimorbidity and polypharmacy think about deprescribing? The LESS study - A primary care-based survey. BMC Geriatr. 2020;20(1):435. doi:10.1186/s12877-020-01843-x
36. Weir K, Nickel B, Naganathan V, et al. Decision-making preferences and deprescribing: perspectives of older adults and companions about their medicines. J Gerontol B Psychol Sci so Sci. 2018;73(7):e98–e107. doi:10.1093/geronb/gbx138
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Barriers and Facilitators to Successful Intensive Adherence Counseling in Rural Northern Uganda: An Exploratory Interview with HIV-Positive Clients Using the COM-B Framework
Beja H, Daisy N, Edek MT, Kobusinge V, Akaki O, Owachgiu IO, Udho S
HIV/AIDS - Research and Palliative Care 2022, 14:553-563
Published Date: 21 November 2022
Factors Influencing ART Adherence Among Persons Living with HIV Enrolled in Community Client-Led Art Delivery Groups in Lira District, Uganda: A Qualitative Study
Isabirye R, Opii DJ, Opio Ekit S, Kawomera A, Lokiru L, Isoke R, Ssenkaali J, Puleh SS
HIV/AIDS - Research and Palliative Care 2023, 15:339-347
Published Date: 15 June 2023
Barriers and Facilitators to Health-Care Provider Payment Reform – A Scoping Literature Review
Ndayishimiye C, Tambor M, Dubas-Jakóbczyk K
Risk Management and Healthcare Policy 2023, 16:1755-1779
Published Date: 7 September 2023
Barriers and Facilitators to Utilization of Community Drug Distribution Points Among People Living with HIV in Bushenyi District, South-Western Uganda: A Qualitative Study
Oyet D, Niyonzima V, Akol G, Onyait E, Twinomugisha D, Kawala Wambera D, Wakida EK, Obua C
HIV/AIDS - Research and Palliative Care 2023, 15:633-640
Published Date: 16 October 2023
Planning for Hospital Discharge for Older Adults in Uganda: A Qualitative Study Among Healthcare Providers Using the COM-B Framework
Owokuhaisa J, Schwartz JI, Wiens MO, Musinguzi P, Rukundo GZ
Journal of Multidisciplinary Healthcare 2023, 16:3235-3248
Published Date: 2 November 2023